Back to Journals » Journal of Inflammation Research » Volume 18
The Relationship Between IL-6 and IL-10 Expression Levels and the Prognosis in B-Cell Non-Hodgkin Lymphoma Patients Treated with R-CHOP
Authors Dong Q, Lin W, Yu S, Qin Y, Jia C, Wang N, Xiu W, Shan W, Dong M, Liu D
Received 3 April 2025
Accepted for publication 5 September 2025
Published 25 October 2025 Volume 2025:18 Pages 14791—14804
DOI https://doi.org/10.2147/JIR.S532323
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Felix Marsh-Wakefield
Quan Dong,1,* Wenxin Lin,1,* Saihui Yu,1 Yuxin Qin,1 Chuiming Jia,2 Na Wang,3 Wei Xiu,4 Weiqi Shan,5 Mei Dong,1,* Duo Liu1,*
1Department of Pharmacy, Harbin Medical University Cancer Hospital, Harbin, 150086, People’s Republic of China; 2Hematology Department, Harbin Medical University Cancer Hospital, Harbin, 150086, People’s Republic of China; 3Department of Science and Education, Heilongjiang Provincial Hospital, Harbin, 150036, People’s Republic of China; 4Department of Pharmacy, Heilongjiang Forest Industry General Hospital, Harbin, 150040, People’s Republic of China; 5Department of Gastrointestinal Medical Oncology, Harbin Medical University Cancer Hospital, Harbin, 150086, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Duo Liu, Department of Pharmacy, Harbin Medical University Cancer Hospital, Harbin, 150086, People’s Republic of China, Email [email protected] Mei Dong, Department of Pharmacy, Harbin Medical University Cancer Hospital, Harbin, 150086, People’s Republic of China, Email [email protected]
Purpose: To explore the relationship between the expression of IL-6 and IL-10 in the blood of B-cell non-Hodgkin lymphoma (B-NHL) patients and their survival time and adverse reactions.
Methods: The study collected and analyzed blood samples from 488 patients with B-NHL treated with rituximab (94 serum samples, 394 plasma samples) as well as plasma samples from 202 healthy subjects, along with relevant clinical information. Expression levels of IL-6 and IL-10 in the blood were measured using enzyme-linked immunosorbent assay (ELISA).
Results: The expression of IL-6 in the plasma of B-NHL patients was significantly higher than those in healthy subjects (P < 0.001). Patients with low IL-6 expression (serum) had longer Event Free Survival (EFS) compared to those with high IL-6 expression (P = 0.011). Patients with low IL-10 expression (plasma) had longer Progression Free Survival (PFS) (P = 0.009) and EFS (P = 0.027) compared to those with high IL-10 expression. For patients with collected serum samples, non-GCB have shorter PFS (P = 0.027) and EFS (P = 0.03) than GCB patients. The COX proportional hazards regression model results suggest that elevated plasma IL-10 levels (P = 0.008) and advanced stage (P < 0.001) are risk factors for PFS in B-NHL patients.
Conclusion: The expression of IL-6 and IL-10 in the blood can serve as important biomarkers for predicting the prognosis of rituximab in patients with B-NHL.
Keywords: IL-6, IL-10, rituximab, B-NHL, prognosis
Introduction
Non-Hodgkin lymphoma (NHL) is among the top ten malignant tumors in terms of both incidence and tumor-related mortality.1 Among these, B-NHL is the most common form of non-Hodgkin lymphoma.2
Rituximab combined with cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP) chemotherapy regimen is the first-line treatment for Diffuse large B-cell lymphoma (DLBCL).3 But 30–40% patients still experience treatment failure or relapse due to the heterogeneity DLBCL.4 The IPI score and gene expression profile-based disease classification are currently widely used methods for evaluating disease prognosis, but they do not account for poor treatment responses in some patients.5 There is a lack of reliable prognostic indicators for lymphoma.
The presence of cytokines in the tumor microenvironment affects various stages of tumor progression, including initiation, proliferation, promotion of tumor cell transformation, angiogenesis, invasion, inhibition of apoptosis, immune surveillance, drug resistance, and metastasis.6 The growth of tumors is regulated by the host’s immune system, and interleukins play a crucial role in modulating immune responses.7
IL-6 has a wide range of biological effects, primarily participating in immune functions, inflammatory responses, and influencing hematopoietic functions.8–10 IL-6 can promote tumor cell proliferation and survival by activating signaling pathways such as the JAK/STAT3 pathway.11,12 Previous studies have found that DLBCL patients who have high serum IL-6 expression tend to have shorter PFS and lower complete remission (CR) rates.13 However, other studies have not identified an association.14
IL-10 is a multifunctional immune regulatory factor that can modulate the immune balance and inflammatory state in the body.15 Due to the dual functions of IL-10 in both immunosuppression and immune stimulation, it can promote tumor growth while also exerting anti-tumor effects.16,17 Studies have shown that serum IL-10 levels in NHL patients are significantly higher than those in healthy subjects.18,19 However, other studies have found that the plasma levels of IL-6 and IL-10 did not change significantly in patients treated with the R-CHOP regimen.20,21 Some studies have not found a correlation between IL-6, IL-10, and prognostic parameters in NHL patients.14,22 There is only one study in China examining the correlation between serum cytokine concentrations and the prognosis of DLBCL patients treated with rituximab. This study found that high serum levels of IL-10 indicate a poorer therapeutic outcome, while no correlation was found between serum IL-6 and patient prognosis.23
Therefore, this study aims to investigate the relationship between the levels of IL-6 and IL-10 in the blood of Chinese B-NHL patients and their survival time as well as adverse reactions during rituximab treatment, with the goal of screening reliable biomarkers that can predict the survival time of B-NHL patients.
Materials and Methods
Main Experimental Reagents
The IL-6 enzyme-linked immunosorbent assay kit (JL14113) and IL-10 enzyme-linked immunosorbent assay kit (JL19246) used in this study were purchased from Shanghai Jianglai Biological Technology Co., Ltd. The detection ranges are as follows: IL-6 (3.12–200 pg/mL) and IL-10 (0.78–50 pg/mL). The kits include a 96-well plate pre-coated with antibody, protein standards, 100× concentrated biotin-labeled antibody, universal diluent (BSA), 20× washing buffer (PBST), 100× concentrated enzyme conjugate, substrate (TMB), and diluted sulfuric acid stop solution.
Experimental Subjects
Inclusion and Exclusion Criteria for the Study
The patients included in this study were all treated at the Harbin Medical University Cancer Hospital, with admission dates ranging from April 2021 to January 2024. All patients received R-CHOP or R-CDOP as the initial treatment regimen. This study collected blood samples from 488 patients with B-BHL and plasma samples from 202 healthy controls. To accurately reflect the biological characteristics of patients at the start of treatment, the blood samples were collected within one year after the initial chemotherapy. The inclusion criteria were: (1) patients with a diagnosis of B-NHL confirmed by histopathology; (2) treatment regimens included rituximab; (3) patients whose lymphoma was a primary cancer; (4) patients with no liver, kidney, or heart function impairment, and with normal granulocyte counts. The exclusion criteria were: (1) patients receiving only palliative care; (2) patients who are pregnant or nursing; (3) patients who did not use rituximab during treatment.
Demographic Characteristics and Clinicopathological Information
The treatment regimen for each cycle of the enrolled patients was obtained from the medical records management system of Harbin Medical University Cancer Hospital. Epidemiological information was recorded, including patient name, age, medical record number, height and weight, gender, ethnicity, smoking and alcohol history, and family history of cancer. The collected pathological parameters include the clinical stage of the tumor, germinal center origin, pathological classification, liver and kidney function, and adverse reactions. Detailed information on disease progression was also recorded, such as admission and discharge times, disease progression status, time of death, and immunohistochemical markers, which were included in the analysis as covariates, and cell origin determined according to the Hans method. This study protocol was approved by the Ethics Committee of Harbin Medical University, and all participants provided written informed consent. To ensure patient privacy, all personal information and data collected for the experiment were anonymized. The ethics approval number for this study is KY2021-39.
Treatment Regimen
All B-NHL patients included in this study received a regimen containing rituximab.
Adverse Reactions and Survival Time
The adverse reactions among the patients included in this study mainly consist of liver and kidney function abnormalities, gastrointestinal reactions, fever, fatigue, and myelosuppression, among others. Adverse reactions are assessed every four cycles. PFS is defined as the time from the start of chemotherapy to disease progression, recurrence, or death. EFS is defined as the time from the start of treatment to disease progression, recurrence, death, the occurrence of severe adverse reactions, change in medication regimen, or initiation of salvage therapy. For the first 2 years, follow up every 3 months, and then every 6 months thereafter.
Statistical Analysis
The statistical analysis was conducted using SPSS 26.0 software. The practice evaluation of adverse reactions in this study adopts the Common Terminology Criteria for Adverse Events standard 5.0 (CTCAE 5.0). The Shapiro–Wilk (S-W) test was used to assess the normality of the experimental results. For the comparison of non-normally distributed data between two groups, the Wilcoxon rank-sum test was applied, and the data are presented as medians. For normally distributed data, a t-test was used to compare the two groups. This study focused on PFS and EFS as the primary endpoints. Survival curves were constructed using the Kaplan-Meier method. The relationship between the expression levels of IL-6 and IL-10 and the adverse reactions in common B-NHL patients was explored using Logistic regression analysis. The Cox proportional hazards model was employed for both univariate and multivariate analyses, assessing the factors influencing the survival period of B-NHL patients. A P-value of less than 0.05 was considered to indicate statistical significance in the group differences.
Results
Basic Information of B-NHL Patients
The study included blood samples from 488 patients with B-NHL, consisting of 394 plasma samples and 94 serum samples. The average age of all B-NHL patients was 57.8 years. Among them, 170 patients (36.8%) were aged 65 or older, while 318 patients (63.2%) were under 65 years old. 246 men, 242 women. A total of 179 patients (36.7%) were in Ann Arbor stage I–II, 278 patients (60.0%) were in stage III–IV, and staging information could not be obtained for 31 patients. Additionally, 76 patients (15.6%) experienced grade III or higher bone marrow suppression. During the treatment, 236 (48.4%) individuals encountered varying degrees of systemic adverse reactions, including fatigue, interstitial pneumonia, severe allergic reactions, gastrointestinal responses, bone marrow suppression, and liver and kidney impairment. Among them, 92 individuals (18.9%) experienced systemic adverse reactions of grade III or higher. For detailed information, Supplementary Table 1.
The patients included in this study primarily have: DLBCL, Follicular Lymphoma (FL), Marginal Zone Lymphoma (MZL), Chronic Lymphocytic Leukemia/Small Lymphocytic Lymphoma (CLL/SLL), Mantle-Cell Lymphoma (MCL), among others. There were 344 patients with DLBCL, and their information is as follows: the average age was 59.3 years, with 133 patients aged 65 and over (38.7%), and 211 patients under 65 (61.3%). There were slightly more male patients than female (male: female = 175:169). Ann Arbor stage I–II patients numbered 137 (39.8%), stage III–IV patients numbered 184 (53.5%), and the remaining patients had no staging information (6.7%). There were 142 patients (41.3%) with the Germinal Center B-cell (GCB) subtype and 182 patients (52.9%) with the non-Germinal Center B-cell (non-GCB) subtype, while the remaining 20 patients (6.7%) have no staging information. Seventy patients (20.3%) experienced grade III or higher systemic adverse reactions, among whom 57 patients (15.7%) developed grade III or higher bone marrow suppression following treatment. This study also included 74 FL, 12 MZL, 32 MCL, and other B-NHL patients. For detailed information, Supplementary Table 2.
Relationship Between IL-6 and IL-10 Expression Levels and the Survival Time of B-NHL Patients
Relationship Between IL-6 Levels and the Survival Time of B-NHL Patients
In this study, plasma samples from a total of 394 B-NHL patients were collected, the median follow-up time was 22 months. The IL-6 concentration displayed a non-normal distribution according to the S-W test. Among the patients, 229 cases (57.6%) had undetectable levels (0 ng/mL), with the median being 0. This study divides B-NHL patients into high expression and low expression groups based on the median concentration of IL-6 (0 ng/mL) as the cutoff value. We did not find a correlation between the plasma IL-6 levels and PFS or EFS in patients with B-NHL.
Among the 94 patients from whom serum samples were taken, the median follow-up time was 35 months. The IL-6 concentration was also found to be non-normally distributed (P < 0.001). When using the median (8.077 pg/mL) as the cut-off value, a significant difference in the mean EFS was observed between the IL-6 low expression group and the IL-6 high expression group (P = 0.011) (Figure 1 and Table 1). It is worth further studying that, through analysis, there is a significant difference between plasma IL-6 levels and serum IL-6 levels.
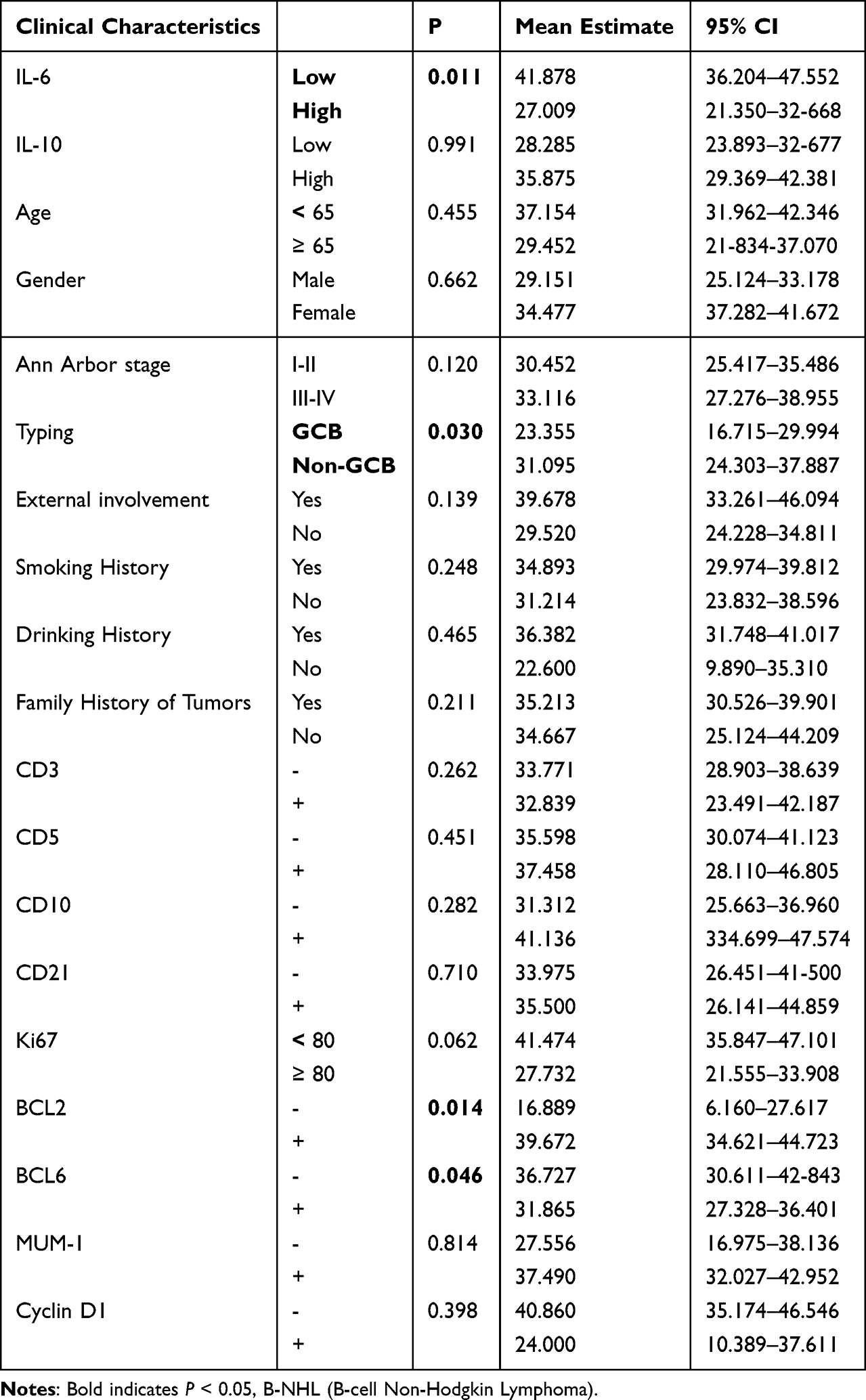 |
Table 1 Factors Influencing EFS in Patients with B-NHL Treated with Rituximab |
 |
Figure 1 Kaplan-Meier curve showing the correlation between serum IL-6 levels and EFS in B-NHL patients treated with rituximab. |
The results of the subgroup analysis indicate that among patients who provided serum samples, males with low IL-6 expression had significantly longer PFS (P = 0.006, Supplementary Figure 1A) and EFS (P = 0.003, Supplementary Figure 1B) compared to those males with high IL-6 expression. However, for female patients, there was no significant difference in PFS (P = 0.741) and EFS (P = 0.330). Patients with a BMI between 18.5 and 28 and low IL-6 expression experienced longer EFS (P = 0.017, Supplementary Figure 1D) compared to those with high IL-6 expression, although there was no significant difference in PFS (Supplementary Figure 1C and Supplementary Table 3).
No correlation was found between plasma IL-6 levels and patient survival time.
Relationship Between IL-10 Levels and the Survival Time of B-NHL Patients
In the patients from whom plasma samples were collected, the IL-10 concentration was found to be non-normally distributed according to the S-W test. B-NHL patients were divided into high expression and low expression groups using the IL-10 concentration median (6.48 ng/mL) as the cut-off value. The PFS for patients in the IL-10 low expression group was significantly longer than that of the IL-10 high expression group (P = 0.007, Figure 2A and Table 2). Similarly, there was a significant difference in EFS between IL-10 high expression and low expression groups (P = 0.032, Figure 2B and Table 3).
 |
Table 2 Factors Affecting PFS in Patients (plasma) with B-NHL Treated with Rituximab |
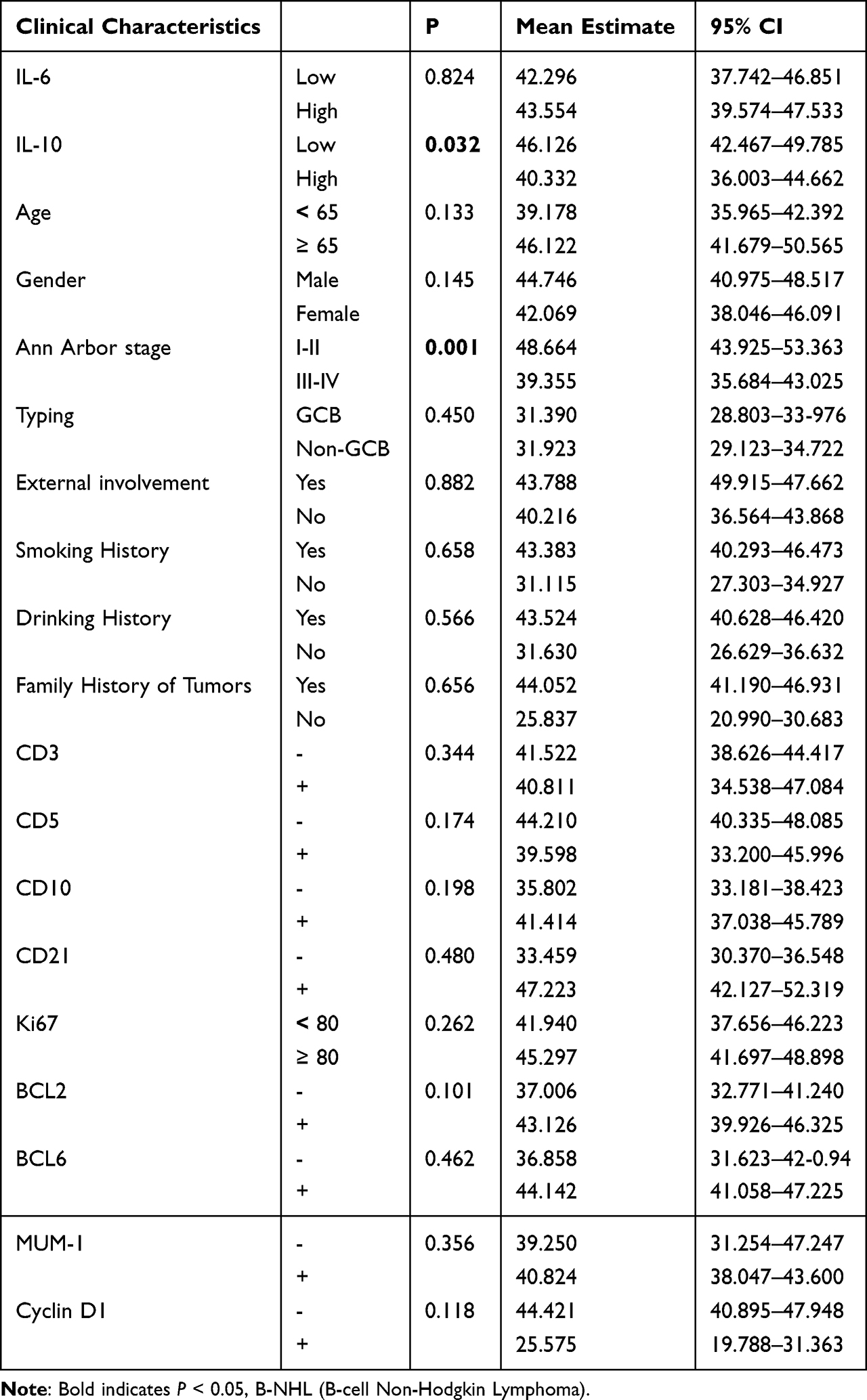 |
Table 3 Factors Affecting EFS in Patients with B-NHL Treated with Rituximab |
 |
Figure 2 Kaplan-Meier curve illustrating the correlation between plasma IL-10 levels and PFS (A) and EFS (B) in B-NHL patients treated with rituximab. |
Among the 94 patients from whom serum samples were collected, the IL-10 concentration was also non-normally distributed (P < 0.001) based on the K–S test. Using the median IL-10 concentration (13.69 ng/mL) as the cut-off value, yet no significant differences in PFS or EFS were observed between patients in the IL-10 high expression and low expression groups. There is no statistically significant difference between plasma IL-10 levels and serum IL-10 levels.
Subgroup analysis results indicate that male B-NHL patients, who have low plasma IL-10 expression, experience longer PFS (P = 0.026, Supplementary Figure 2A) and EFS (P = 0.032, Supplementary Figure 2B) compared to those with high IL-10 expression. Among patients under the age of 65, those with low plasma IL-10 expression also have longer PFS (P = 0.012, Supplementary Figure 2C) and EFS (P = 0.024, Supplementary Figure 2D) than those with high IL-10 expression. In female patients or those aged 65 and above, there was no significant difference in PFS or EFS between the high and low plasma IL-10 expression groups. Among patients without extranodal involvement (P = 0.024, Supplementary Figure 3A), with a BMI ≥ 28 (P = 0.01, Supplementary Figure 3B), or with non-germinal center (P = 0.044, Supplementary Figure 3C), the low plasma IL-10 expression group showed a significant increase in PFS compared to the high IL-10 expression group.
In the patients from whom serum samples were collected, the concentration of IL-10 also displayed a non-normal distribution according to the S-W test (P < 0.001). Based on the median value (13.69 pg/mL), B-NHL patients were divided into high expression and low expression groups. No correlation was found between serum IL-10 levels and patient survival time.
Apart from IL-6 and IL-10 expression levels, the Kaplan-Meier survival curve results indicate that in the plasma group of patients, those with advanced stages III/IV had shorter PFS (P < 0.001, Supplementary Figure 4A) and EFS (P = 0.001, Supplementary Figure 4B) compared to those in the early stages I/II (Table 2 and Table 3). Among patients from whom serum samples were collected, those with non-GCB had shorter PFS (P = 0.027, Supplementary Figure 4C) and EFS (P = 0.03, Supplementary Figure 4D) compared to those with GCB patients (Tables 1 and 4).
 |
Table 4 Factors Affecting PFS in Patients (serum) with B-NHL Treated with Rituximab |
Due to limited conditions, this study could only collect plasma samples from the healthy control group, and there was a significant difference in plasma IL-6 levels between the healthy control group and B-NHL patients (P < 0.001).
The Relationship Between Immunohistochemical Expression and Survival Time in B-NHL Patients
All the patients included in this study were CD20(+) and were treated with rituximab. We conducted statistical analysis on the expression of nine common immunohistochemical markers that may affect 488 patients with B-NHL and analyzed their correlation with the survival time of B-NHL patients. Statistical results indicate that among patients who provided serum samples, Patients with BCL6 (-) had a longer EFS compared with those with BCL6 (+) (P = 0.046, Table 2). Patients with BCL2 (-) had a shorter PFS (P = 0.020) and EFS (P = 0.014) compared to BCL2 (+) patients (Tables 2). No significant difference was observed among patients who provided plasma samples.
The results of the subgroup analysis combining immunohistochemical markers with IL-6 and IL-10 indicate that among patients from whom serum samples were collected, those with BCL2 (+) and low IL-6 expression had significantly longer PFS (P = 0.021) and EFS (P = 0.005) compared to those with high IL-6 expression. In patients with BCL2 (-), there was no significant difference in PFS (P = 0.539) and EFS (P = 0.624) between those with low and high IL-6 expression. Patients with CD3 (-) (P = 0.029), CD3 (+) (P = 0.008), CD5 (+) (P = 0.038), or Mum-1 (+) (P = 0.024) and low IL-6 expression had longer EFS compared to those with high IL-6 expression.
The serum levels of IL-10 do not have a predictive effect on the patient’s survival duration. In patients from whom plasma samples were collected, those with low expression of IL-10 exhibited significantly prolonged PFS compared to patients with high IL-10 expression when characterized by CD3(-) (P = 0.005), CD5(-) (P = 0.002), CD21(-) (P = 0.021), BCL6(+) (P = 0.010), Mum-1(-) (P = 0.017), CyclinD1(-) (P = 0.030), or Ki-67 expression < 80% (P = 0.012). Similarly, patients with low IL-10 expression had significantly extended EFS compared to those with high expression when characterized by CD3(-) (P = 0.011), CD5(-) (P = 0.013), CD21(-) (P = 0.026), BCL6(+) (P = 0.043), or CyclinD1(-) (P = 0.040).
In conclusion, the expression of serum IL-6 and plasma IL-10, combined with immunohistochemical markers, can predict the treatment outcome of B-NHL.
The Relationship Between IL-6, IL-10 Expression Levels and Adverse Reactions in B-NHL Patients
In this study, we collected information on adverse reactions occurring in 488 B-NHL patients during treatment with rituximab. The main adverse reactions included bone marrow suppression, fatigue, fever, digestive system reactions, interstitial pneumonia, cardiac toxicity, and other systemic adverse effects. Among the patients from whom plasma samples were collected, 191 experienced adverse reactions. Of these, 83 patients (43.5%) had grade III or above systemic adverse reactions, and 68 patients (33.0%) experienced grade III bone marrow suppression. Fever symptoms were noted in 20 patients (10.5%), interstitial pneumonia in 15 patients (7.9%), gastrointestinal reactions such as nausea and vomiting in 14 patients (7.3%), and cardiac toxicity-related adverse reactions in 4 patients (2.1%). Through logistic regression analysis, we did not find a correlation between high expression levels of IL-6 and IL-10 in plasma or serum samples and the occurrence of Grade III or higher severe adverse reactions.
Cox Regression Analysis of Factors Affecting Survival Time in B-Cell Non-Hodgkin Lymphoma
To assess the impact of various variables on PFS and EFS in B-NHL patients, we established a Cox proportional hazards model to analyze the influence of IL-6 and IL-10 expression, age, gender, and other factors on patient survival. Univariate analysis results indicated that high serum IL-6 expression significantly shortened the EFS of B-NHL patients (HR = 2.212, 95% CI: 1.170–4.184, P = 0.015) (Supplementary Table 5); additionally, B-NHL patients with non-germinal centers had shorter PFS (HR = 0.385, 95% CI: 0.154–0.962, P = 0.037) and EFS (HR = 0.375, 95% CI: 0.149–0.943, P = 0.041) compared to those with germinal centers (Supplementary Tables 5 and 6). High levels of IL-10 in plasma are factors that shorten PFS (HR = 1.731, 95% CI: 1.152–2.602, P = 0.008) and EFS (HR = 1.480, 95% CI: 1.028–2.130, P = 0.035) in patients with B-NHL (Supplementary Tables 7 and 8). Additionally, patients in advanced stages (III, IV) experience shorter PFS (HR = 2.247, 95% CI: 1.404–3.597, P < 0.001) and EFS (HR = 1.974, 95% CI: 1.300–2.998, P = 0.001) compared to those in early stages (I–II) of B-NHL (Supplementary Tables 7 and 8). Multivariate Cox regression further indicates that high plasma IL-10 expression and advanced stage are indicators of poor prognosis for B-NHL treated with rituximab. Patients with low IL-10 expression in B-NHL have a longer PFS compared to those with high IL-10 expression (HR = 1.730, 95% CI: 1.152–2.602, P = 0.008). Furthermore, patients in the early stages have significantly extended PFS (HR = 2.179, 95% CI: 1.360–3.490, P = 0.001) and EFS (HR = 1.933, 95% CI: 1.272–2.937, P = 0.002) compared to those in the advanced stages.
Discussion
This study aims to analyze the impact of IL-6 and IL-10 expression levels on the survival time and adverse reactions of B-NHL patients treated with rituximab. The study found that, compared to healthy subjects, B-NHL patients had significantly elevated plasma IL-6 levels. Patients with elevated serum IL-6 levels had a shorter EFS; those with elevated plasma IL-10 levels had shorter PFS and EFS. Furthermore, elevated plasma IL-10 levels and advanced stages were risk factors for PFS in B-NHL patients, while advanced stages were risk factors for EFS in B-NHL patients.
IL-6 is a multifunctional immunoregulatory cytokine produced by various cells, playing a crucial role in the occurrence and development of NHL.14,24 Hind et al reported that the IL-6 signaling complex is a key driver of DLBCL progression, which includes the IL-6/STAT3 signaling axis and the inactivating mutations of the negative regulator of IL-6 signaling, suppressor of cytokine signaling 1 (SOCS1), negatively affecting the prognosis of DLBCL patients.25 The study indicates that NHL patients with higher serum IL-6 levels have shorter PFS, consistent with related findings from Spain.13 Additional research from Turkey, Croatia, and Egypt shows that IL-6 levels in NHL and DLBCL patients are significantly elevated compared to healthy individuals.14,26,27 Furthermore, the study from Croatia suggests that patients with elevated IL-6 levels (IL-6 ≥ 28 pg/mL) have shorter 3-year and 5-year survival rates, as well as OS, and a lower CR rate.26 However, the study from Turkey found no correlation between serum IL-6, IL-10 concentrations, and prognostic parameters.14
IL-10 is a multifunctional anti-inflammatory cytokine produced by immune cells. Numerous studies have shown that IL-10 promotes the proliferation of tumor B lymphocytes, affects the body’s immune surveillance, and thereby participates in the immune regulation of lymphoma.28–32 Additionally, rituximab can downregulate the anti-apoptotic IL-10 autocrine/paracrine loop, reduce IL-10 levels and make therapeutic agents more sensitive to NHL cells.33 Currently, there is still controversy regarding the relationship between IL-10 levels and prognostic parameters like survival in NHL patients. Previous reports have indicated that serum IL-10 levels in NHL patients are significantly higher than in control groups.19,34–36 Studies from Croatia (IL-10 ≥ 20.2 pg/mL) and France (IL-10 ≥ 31.5 pg/mL) have shown that patients with high IL-10 expression have shorter OS and lower CR rates, suggesting a poorer treatment response.37,38 However, some studies have not found an effect of IL-10 levels on treatment outcomes in NHL patients.14,21,22 Currently, there are only two studies using plasma samples that investigate the relationship between IL-10 expression and prognosis in lymphoma patients. Both studies have found that high levels of IL-10 (IL-10 ≥ 35 or 26 pg/mL) in patients’ plasma are indicative of shorter PFS or EFS, consistent with the results of this study.19,34
In this study, the results for patients from whom serum and plasma samples were collected differed, which may be related to the differences in composition between serum and plasma. Plasma is the liquid component of blood. Serum is the liquid portion remaining after the blood has undergone the coagulation process. During blood coagulation, certain proteins, such as fibrinogen, are converted into fibrin and form a clot, so serum does not contain clotting factors. Under inflammatory conditions, levels of interleukins (such as IL-6) are significantly elevated. The liver increases the synthesis of fibrinogen, antithrombin, C-reactive protein, and other related proteins, thereby indirectly participating in the coagulation process.39–41 At the same time, certain coagulation factors (such as coagulation factor Xa) can promote immune cells (such as macrophages and lymphocytes) to release various interleukins, such as IL-6 and IL-8, by activating protease-activated receptors (PARs).42,43 Subgroup analysis results indicate that among male patients, those with high serum IL-6 expression and high plasma IL-10 expression have shorter PFS and EFS, whereas no significant differences were observed in female patients. Studies suggest that there are significant gender differences in immune responses; typically, women’s immune systems respond more vigorously to pathogens, while men’s responses are weaker. This may be related to estrogen promoting the production of certain types of interleukins (such as IL-4, IL-5, IL-6), ultimately leading to greater variability in interleukin levels in female patients due to physiological and pathological states and individual hormone levels. Consequently, the ability of interleukin levels to predict treatment outcomes in female patients is relatively poor.44,45
In addition, this study still has many limitations. By the statistical cutoff date, the number of deaths among the enrolled patients was small, which made it impossible to calculate the overall survival time of the patients. It also indicated that the median follow-up period was short, which imposed restrictions on the survival analyses. Due to the limitations of the case system, we were unable to obtain relevant information such as patients’ LDH levels, PS ECOG, IPI and remission rates. This study did not find a correlation between the expression levels of IL-6 and IL-10 and the occurrence of adverse reactions in patients, which may be related to the preventive medication used during the patients’ treatment process. Besides, different lymphoma subtypes limit the generalizability of the findings. In the future, we will continue to expand the sample size and focus on research involving DLBCL patients.
The research on blood IL-6 and IL-10 as prognostic factors in NHL patients is limited with the types of samples collected and outcomes being inconsistent. This may be related to differences in patient populations, lifestyle habits, types of samples collected, and detection methods. This study is a retrospective analysis. Due to the limitations of the case system, the response rates of all patients after front-line treatment could not be obtained. There are only two studies on the correlation between plasma IL-10 expression levels and the prognosis of lymphoma patients. However, IL-6 was not included in the study.19,34 Most studies are conducted in Europe and North America and do not specify treatment regimens for patients. A retrospective study conducted in China found that patients with elevated IL-6 or IL-10 levels (IL-6 ≥ 4.5 or IL-10 ≥ 5.0 pg/mL) had shorter survival times and higher recurrence rates, similarly without specific treatment plans.5 Another study considered IL-6 only, but did not specify treatment plans.46 Yet another study, which included the above two inflammatory factors, found that only the serum IL-10 levels (IL-10 ≥ 11.74 pg/mL) was correlated with the mortality rate of DLBCL patients. No correlation was found between serum IL-6 concentration levels and the treatment efficacy or survival time of the patients.23 Due to the limited sample size of the enrolled patients, further multicenter large-sample studies are needed in the future to explore this correlation.
In summary, this study found a relationship between the expression levels of IL-6 and IL-10 in the blood of patients and the survival time and adverse reactions in B-NHL patients treated with rituximab. The findings will provide new insights and a theoretical foundation for individualized dosing of rituximab in the treatment of B-NHL patients.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author (Duo Liu) upon reasonable request.
Ethical Approval
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (Ethics Committee of Harbin Medical University (HMUIRB20160004)) and with the Helsinki Declaration of 1975, as revised in 2000. Informed consent was obtained from all patients for being included in the study. The study complies with the Declaration of Helsinki.
Informed Consent
Informed consent was not required for this study.
Acknowledgments
This study was supported by National Natural Science Foundation of China (No. 82003775), Heilongjiang Provincial Natural Science Foundation of China (YQ2024H025), Young Talents of Basic Research in Universities of Heilongjiang Province (YQJH2024138), Haiyan Foundation of Harbin Medical University Cancer Hospital (JJZD2024-11), and Talent Project established by Chinese Pharmaceutical Association Hospital Pharmacy department (No. CPA-Z05-ZC-2023-003).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no potential conflicts of interest in this work.
References
1. Siegel RL, Miller KD, Wagle NS, Jemal A. Cancer statistics, 2023. Ca-Cancer J Clin. 2023;73(1):17–48. doi:10.3322/caac.21763
2. Meng X, Min Q, Wang JY. B cell lymphoma. Adv Exp Med Biol. 2020;1254:161–181. doi:10.1007/978-981-15-3532-1_12
3. China Anti-cancer Association Lymphoma Committee. Clinical practice guideline for lympoma in China (2021 Edition). Zhonghua zhong liu za zhi. 2021;43(7):707–735. doi:10.3760/cma.j.cn112152-20210516-00382
4. Jamil MO, Mehta A. Diffuse large B-cell lymphoma: prognostic markers and their impact on therapy. Expert Rev Hematol. 2016;9(5):471–477. doi:10.1586/17474086.2016.1146584
5. Bao C, Gu J, Huang X, You L, Zhou Z, Jin J. Cytokine profiles in patients with newly diagnosed diffuse large B-cell lymphoma: IL-6 and IL-10 levels are associated with adverse clinical features and poor outcomes. Cytokine. 2023;169:156289. doi:10.1016/j.cyto.2023.156289
6. Shang GS, Liu L, Qin YW. IL-6 and TNF-α promote metastasis of lung cancer by inducing epithelial-mesenchymal transition. Oncol Lett. 2017;13(6):4657–4660. doi:10.3892/ol.2017.6048
7. Murdaca G, Paladin F, Orsi A, Gangemi S. Interleukin-31: a Pro-inflammatory oriented cytokine. Front Biosci. 2025;30(6):37462. doi:10.31083/FBL37462
8. Hirano T. IL-6 in inflammation, autoimmunity and cancer. Int Immunol. 2021;33(3):127–148. doi:10.1093/intimm/dxaa078
9. Jones SA, Jenkins BJ. Recent insights into targeting the IL-6 cytokine family in inflammatory diseases and cancer. Nat Rev Immunol. 2018;18(12):773–789. doi:10.1038/s41577-018-0066-7
10. Grebenciucova E, VanHaerents S. Interleukin 6: at the interface of human health and disease. Front Immunol. 2023;14:1255533. doi:10.3389/fimmu.2023.1255533
11. Huang B, Lang X, Li X. The role of IL-6/JAK2/STAT3 signaling pathway in cancers. Front Oncol. 2022;12:1023177. doi:10.3389/fonc.2022.1023177
12. Johnson DE, O’Keefe RA, Grandis JR. Targeting the IL-6/JAK/STAT3 signalling axis in cancer. Nat Rev Clin Oncol. 2018;15(4):234–248. doi:10.1038/nrclinonc.2018.8
13. Dlouhy I, Filella X, Rovira J, et al. High serum levels of soluble interleukin-2 receptor (sIL2-R), interleukin-6 (IL-6) and tumor necrosis factor alpha (TNF) are associated with adverse clinical features and predict poor outcome in diffuse large B-cell lymphoma. Leukemia Res. 2017;59:20–25. doi:10.1016/j.leukres.2017.05.014
14. Guney N, Soydinc HO, Basaran M, et al. Serum levels of interleukin-6 and interleukin-10 in Turkish patients with aggressive non-Hodgkin’s lymphoma. Asian Pac J Cancer Prev. 2009;10(4):669–674.
15. Iyer SS, Cheng G. Role of interleukin 10 transcriptional regulation in inflammation and autoimmune disease. Crit Rev Immunol. 2012;32(1):23–63. doi:10.1615/critrevimmunol.v32.i1.30
16. Rallis KS, Corrigan AE, Dadah H, et al. Cytokine-based cancer immunotherapy: challenges and opportunities for IL-10. Anticancer Res. 2021;41(7):3247–3252. doi:10.21873/anticanres.15110
17. Oft M. IL-10: master switch from tumor-promoting inflammation to antitumor immunity. Cancer Immunol Res. 2014;2(3):194–199. doi:10.1158/2326-6066.CIR-13-0214
18. Huo J, Fu L, Jin M, Li Z, Zhang M. IL-10 contributes to gemcitabine resistance in extranodal NK/T-cell lymphoma cells via ABCC4. Invest New Drug. 2022;40(3):537–545. doi:10.1007/s10637-022-01224-8
19. Lech-Maranda E, Bienvenu J, Michallet AS, et al. Elevated IL-10 plasma levels correlate with poor prognosis in diffuse large B-cell lymphoma. Eur Cytokine Netw. 2006;17(1):60–66.
20. Epeldegui M, Lee JY, Martínez AC, et al. Predictive value of cytokines and immune activation biomarkers in AIDS-related non-hodgkin lymphoma treated with rituximab plus infusional EPOCH (AMC-034 trial). Clin Cancer Res. 2015;22(2):328–336. doi:10.1158/1078-0432.CCR-14-0466
21. Fabre-Guillevin E, Tabrizi R, Coulon V, et al. Aggressive Non-Hodgkin’s lymphoma: concomitant evaluation of interleukin-2, soluble interleukin-2 receptor, interleukin-4, interleukin-6, interleukin-10 and correlation with outcome. Leukemia Lymphoma. 2006;47(4):603–611. doi:10.1080/10428190500361029
22. Ozdemir F, Aydin F, Yilmaz M, et al. The effects of IL-2, IL-6 and IL-10 levels on prognosis in patients with aggressive Non-Hodgkin’s Lymphoma (NHL). J Exp Clin Cancer Res. 2004;23(3):485–488.
23. Man Y, Ge CQ, Li ZZ, Yang TH, Wang YJ. Expression and prognostic value of cytokines in patients with newly diagnosed diffuse large B-Cell lymphoma. Zhongguo Shi Yan Xue Ye Xue Za Zhi. 2023;31(4):1050–1055. doi:10.19746/j.cnki.issn.1009-2137.2023.04.019
24. Salles G, Coiffier B. Inherited cytokine response and risk of lymphoma. Lancet Oncol. 2006;7(1):3–4.
25. Hashwah H, Bertram K, Stirm K, et al. The IL-6 signaling complex is a critical driver, negative prognostic factor, and therapeutic target in diffuse large B-cell lymphoma. Embo Mol Med. 2019;11(10):e10576. doi:10.15252/emmm.201910576
26. Nacinović-Duletić A, Stifter S, Dvornik S, Skunca Z, Jonjić N. Correlation of serum IL-6, IL-8 and IL-10 levels with clinicopathological features and prognosis in patients with diffuse large B-cell lymphoma. Int J Lab Hematol. 2008;30(3):230–239. doi:10.1111/j.1751-553X.2007.00951.x
27. el-Far M, Fouda M, Yahya R, el-Baz H. Serum IL-10 and IL-6 levels at diagnosis as independent predictors of outcome in Non-Hodgkin’s lymphoma. J Physiol Biochem. 2004;60(4):253–258. doi:10.1007/BF03167070
28. Moore KW, de Waal Malefyt R, Coffman RL, O’Garra A. Interleukin-10 and the interleukin-10 receptor. Annu Rev Immunol. 2001;19:683–765. doi:10.1146/annurev.immunol.19.1.683
29. Levast B, Li Z, Madrenas J. The role of IL-10 in microbiome-associated immune modulation and disease tolerance. Cytokine. 2014;75(2):291–301. doi:10.1016/j.cyto.2014.11.027
30. Contasta I, Pellegrini P, Berghella AM, Adorno D. Cell cycle control in cellular homeostasis during the immune response: interactions between TH1, TH2 cytokines, and Bcl2 and p53 molecules. Cancer Biother Radio. 2001;16(1):63–71. doi:10.1089/108497801750096069
31. Ruella M, Kenderian S, Shestova O, et al. Novel chimeric antigen receptor T cells for the treatment of hodgkin lymphoma. Blood. 2014;124(21):806. doi:10.1182/blood.v124.21.806.806
32. Mocellin S, Marincola F, Rossi CR, Nitti D, Lise M. The multifaceted relationship between IL-10 and adaptive immunity: putting together the pieces of a puzzle. Cytokine Growth F R. 2004;15(1):61–76. doi:10.1016/j.cytogfr.2003.11.001
33. Alas S, Bonavida B. Rituximab inactivates signal transducer and activation of transcription 3 (STAT3) activity in B-non-Hodgkin’s lymphoma through inhibition of the interleukin 10 autocrine/paracrine loop and results in down-regulation of Bcl-2 and sensitization to cytotoxic drugs. Cancer Res. 2001;61.
34. Gupta M, Han JJ, Stenson M, et al. Elevated serum IL-10 levels in diffuse large B-cell lymphoma: a mechanism of aberrant JAK2 activation. Blood. 2012;119(12):2844–2853. doi:10.1182/blood-2011-10-388538
35. Xiu B, Lin Y, Grote DM, et al. IL-10 induces the development of immunosuppressive CD14(+)HLA-DR(low/-) monocytes in B-cell non-Hodgkin lymphoma. Blood Cancer J. 2015;5:e328. doi:10.1038/bcj.2015.56
36. Lech-Maranda E, Bienvenu J, Broussais-Guillaumot F, et al. Plasma TNF-alpha and IL-10 level-based prognostic model predicts outcome of patients with diffuse large B-Cell lymphoma in different risk groups defined by the international prognostic index. Arch Immunol Ther Ex. 2010;58(2):131–141. doi:10.1007/s00005-010-0066-1
37. Duletić-Nacinović A, Stifter S, Marijić B, et al.. Serum IL-6, IL-8, IL-10 and beta2-microglobulin in association with international prognostic index in diffuse large B cell lymphoma. Tumori J. 2008;94 (4), 511. doi:10.1177/030089160809400412.
38. Lech-Maranda E, Baseggio L, Bienvenu J, et al. Interleukin-10 gene promoter polymorphisms influence the clinical outcome of diffuse large B-cell lymphoma. Blood. 2003;103(9):3529–3534. doi:10.1182/blood-2003-06-1850
39. Wilhelm G, Mertowska P, Mertowski S, et al. The crossroads of the coagulation system and the immune system: interactions and connections. Int J Mol Sci. 2023;24(16). doi:10.3390/ijms241612563
40. Chen XF, Wu J, Zhang YD, et al. Role of SOCS3 in enhanced acute-phase protein genes by neonatal macrophages in response to IL-6. J Microbiol Immunol. 2019;54(2):206–212. doi:10.1016/j.jmii.2019.05.005
41. Kishimoto T. IL-6: from its discovery to clinical applications. International Immunol. 2010;22(5):347–352. doi:10.1093/intimm/dxq030
42. Ossovskaya VS, Bunnett NW. Protease-activated receptors: contribution to physiology and disease. Physiol Rev. 2004;84(2):579–621. doi:10.1152/physrev.00028.2003
43. Ghazizadeh S, Khoshnoodi J, Dace SH, Lentz SR. Factor Xa: a new role in inflammation. Thrombosis. Research. 2014;134(3):641–645.
44. Takahashi T, Iwasaki A. Sex differences in immune responses. Science. 2021;371(6527):347–348. doi:10.1126/science.abe7199
45. Chakraborty B, Byemerwa J, Krebs T, Lim F, Chang CY, McDonnell DP. Estrogen receptor signaling in the immune system. Endocr Rev. 2023;44(1):117–141. doi:10.1210/endrev/bnac017
46. Zhao S, Bai N, Cui J, Xiang R, Li N. Prediction of survival of diffuse large B-cell lymphoma patients via the expression of three inflammatory genes. Cancer Med. 2016;5(8):1950–1961. doi:10.1002/cam4.714
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Safety and Efficacy of Rituximab-Based Regimen in Atypical Membranous Nephropathy: A Single Center Retrospective Cohort Study
Liu Y, Zhang S, Hu R, Li C, Chen G, Shi X, Liu Y, Zheng K, Li H, Wen Y, Li X, Li X, Xia P, Qin Y
International Journal of General Medicine 2023, 16:1983-1993
Published Date: 23 May 2023
Proinflammatory Tear Cytokines in Human Adenoviral Keratoconjunctivitis and Clinical Eye Severity
Santacruz Valdés C, Ponce-Rosas ER, Jimenez-Martinez MC
Clinical Ophthalmology 2025, 19:439-448
Published Date: 11 February 2025
Based on the Dual Pathway of Interaction-Mediated NF-κB in Cell Apoptosis and Immune Inflammation to Study the Effect of Danzhi Xiaoyao Powder on the Learning and Cognitive Ability of AD Model Rats
Wang HP, Li MC, Yang J, Zhou J, Meng ZP, Hu YY, Lyu YJ, Chen YQ, Han YM, Pei WL
Degenerative Neurological and Neuromuscular Disease 2025, 15:41-64
Published Date: 14 April 2025