Back to Journals » Clinical Ophthalmology » Volume 19
Proinflammatory Tear Cytokines in Human Adenoviral Keratoconjunctivitis and Clinical Eye Severity
Authors Santacruz Valdés C, Ponce-Rosas ER, Jimenez-Martinez MC
Received 20 September 2024
Accepted for publication 20 January 2025
Published 11 February 2025 Volume 2025:19 Pages 439—448
DOI https://doi.org/10.2147/OPTH.S497111
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Concepción Santacruz Valdés,1 Efrén Raúl Ponce-Rosas,2 Maria C Jimenez-Martinez3,4
1Department of Cornea and Refractive Surgery, Institute of Ophthalmology “Conde de Valenciana”, Mexico City, Mexico; 2Subdivision of Family Medicine, Department of Postgraduates, Faculty of Medicine, National Autonomous University of México, Mexico City, Mexico; 3Department of Immunology and Research Unit, Institute of Ophthalmology “Conde de Valenciana”, Mexico City, Mexico; 4Department of Biochemistry, Faculty of Medicine, National Autonomous University of Mexico, Mexico City, Mexico
Correspondence: Maria C Jimenez-Martinez, Email [email protected]
Introduction: Acute adenoviral conjunctivitis is a disease with mild to severe clinical manifestations. Animal models have provided insight into the role of the innate immune system in clinical damage, but the human immune response at the ocular surface remains poorly understood. Therefore, this study aimed to establish the relationship between tear cytokine levels and disease severity in patients with epidemic keratoconjunctivitis (EKC).
Methods: Fourteen consecutive patients with EKC, confirmed with HAdV8 infection, were included. Ocular characteristics were documented, and each patient’s eye was classified as having more or less severe disease. After tear sampling, levels of cytokines IL-8, IL-6, IL-1b, IL-10, IL-12, and TNF-a were measured using a cytometric bead array.
Results: Our results showed the expression of proinflammatory cytokines in EKC-affected eyes. IL-6, IL-8, and IL-12 significantly correlated with the total clinical ophthalmological score. In the more severely affected eyes, IL-8 and IL-6 significantly correlated with conjunctival hyperemia, and IL-6 correlated with conjunctival swelling. In the less severely affected eyes, inflammatory response, conjunctival hyperemia, and conjunctival hemorrhages were significantly correlated with IL-12 and TNF-a, and ocular discharge was significantly correlated with all tear cytokines. IL-10 was detected in both eyes, suggesting a possible regulatory counterbalance.
Discussion: This study offers novel insights into the pathophysiology of human adenoviral keratoconjunctivitis and its association with clinical data.
Plain Language Summary: Despite the clinical significance of adenoviral keratoconjunctivitis, most studies have concentrated on defining its genotype. Similarly, knowledge of the molecular basis of adenoviral conjunctivitis comes from animal models or cellular lines. Prior to our work, the human immune response at the ocular surface during adenovirus conjunctivitis was poorly understood. Our study described the clinical features of the disease based on severity and found significant correlations between proinflammatory tear cytokines and clinical signs. The results of this study provide new insights into the pathophysiology of adenoviral keratoconjunctivitis and a potential new approach to diagnosis and prompt treatment.
Keywords: tear cytokines, adenovirus infection, keratoconjunctivitis, IL-1b, IL-6, IL-8, IL-10, IL-12, TNF-a
Introduction
Human adenovirus (HAdV) is a highly infectious pathogen capable of arresting all mucosal tissues including the ocular surface, and inducing illness via severe respiratory, gastrointestinal, and genitourinary infections.1,2 Adenovirus is highly contagious and is the leading cause of infectious conjunctivitis worldwide.2 They can induce outbreaks in enclosed environments such as hospitals, schools, or military institutions due to direct hand-to-hand or eye-to-hand transmission, resulting in large economic losses due to missed work.3 Adenoviral conjunctivitis usually manifests as acute viral follicular conjunctivitis, epidemic keratoconjunctivitis (EKC), pharyngoconjunctival fever (PCF), or chronic/relapsing adenoviral conjunctivitis.4 EKC is the most severe ocular infection caused by HAdV. Among the seven groups of HAdV (A-G), adenovirus group D (−8, −19, and −37) affects the conjunctiva, and cornea inducing severe prolonged inflammation in the form of EKC.3,5
The adenoviral disease begins after an incubation period of 5–10 days in one eye as an acute follicular or pseudomembranous/membranous conjunctivitis. After 2 or 3 days, diffuse epithelial keratitis may be present, and after one week, focal areas of subepithelial infiltrates may appear, compromising vision quality due to astigmatism and corneal aberrations, which may persist over time.1,4,6,7 About 7–10 days after the commencement of the acute phase of conjunctivitis, subepithelial nummular corneal opacities appear, inducing halos, and in some cases, blurred vision, which rarely may persist for years.6,8 Characteristics of the disease include significant edema of the plica, caruncle, and conjunctiva, of variable severity. Edematous lid swelling could be accompanied by pseudoptosis due to inflammation and is frequently seen in the primarily affected eye. Similar but usually milder manifestations commonly appear after two to seven days in the second eye and may remain unnoticed. Characteristic symptoms include tearing, foreign body sensation, itching, pain, and photophobia as a result of punctate epithelial corneal lesions.8
After adenoviral infection, replication occurs in ocular surface epithelial cells, followed by interleukin (IL) 8 expression in corneal stromal cells.9 Fibroblast-like stromal keratocytes may respond to adenovirus by expressing numerous pro-inflammatory mediators, including Monocyte Chemoattractant Protein-1 (MCP-1), IL-6, and Interferon-gamma Inducible Protein 10 (IP-10)10 Despite our understanding of the immune response after adenoviral infection in animal models, the production of cytokines during acute adenoviral infection and its relationship to disease severity has not been explored in humans. Therefore, our study aims to identify the cytokine profile during acute (epidemic) adenovirus conjunctivitis and its correlation with clinical disease severity.
Materials and Methods
Patients
Fourteen consecutive patients with untreated epidemic keratoconjunctivitis, diagnosed clinically and confirmed by of HAdV8 infection via polymerase-chain reaction (PCR), were included in the study. Informed consent was obtained from all patients to perform a complete ophthalmological evaluation before obtaining tear samples and clinical photographs. The Investigation, Biosecurity, and Ethics Committees of the Institute of Ophthalmology ¨Conde de Valenciana Foundation” (CC-04-2007) in Mexico City approved the study, assuring compliance with the Declaration of Helsinki.
Clinical Evaluation
A complete medical-ophthalmologic history was performed, and clinical signs were identified using a slit lamp (Carl Zeiss, Meditec Inc., Dublin, CA, USA). Ocular signs such as eyelid involvement, conjunctival hyperemia, conjunctival hemorrhages, discharge, swelling, inflammatory response, and corneal involvement in either eye were recorded in each patient. To establish the most and least severely affected eye, the severity of each sign was classified on a scale of 0 to 4, where 0 = None, 1 = Mild, 2 = Moderate, 3 = Severe, and 4 = Very Severe. The sum of all signs per eye was obtained to get a final score. Clinical descriptions of signs with an assigned grade of severity are shown in Table 1. The eye with the higher score was identified as the most affected eye (MAE), and the contralateral eye as the less affected eye (LAE). The total clinical ophthalmological score per patient was obtained with the sum of both eyes. Representative clinical photographs for each grade are presented in Figure 1. All cases were documented by clinical photography. The evolution time was considered from the onset of the symptoms until tear sampling. All patients in this study presented bilateral adenoviral infection. No additional microbial infections were identified at the time of sampling.
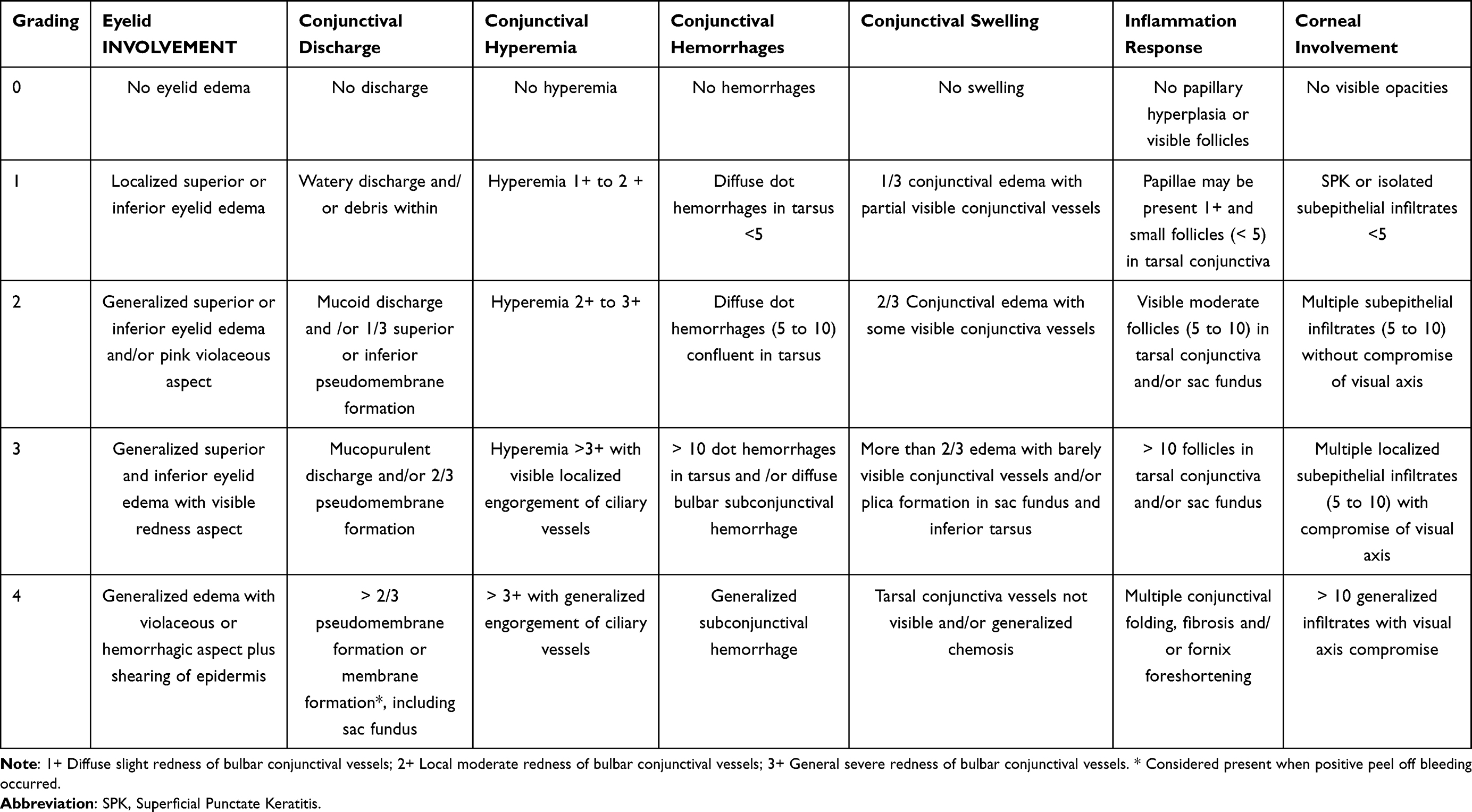 |
Table 1 Adenoviral Conjunctivitis Grade of Severity Classification |
 |
Figure 1 Grade based on severity of signs in adenoviral keratoconjunctivitis. The severity of each sign was evaluated on a scale of 0 to 4. For each eye, the sum of signs indicated severity. The eye with the higher score was identified as the most affected eye (MAE) and the contralateral eye as the less affected eye (LAE). |
Tear Samples and Determination of Soluble Cytokines in Tears
Tear samples were taken from each patient’s eye by applying 20mL of sterile saline solution to the ocular surface and immediately recovering tear fluid via a sterile capillary, following the methodology reported in.11 All tear samples were taken from 9:00 am to 12:00 am before scraping conjunctiva for laboratory diagnosis. The cytokines IL-1 β, IL-6, IL-8, IL-10, IL-12p70, and Tumor Necrosis Factor alfa (TNF-α) were identified using a Human Inflammation Cytokine kit (BD Biosciences, San Jose, CA, USA) and were measured using cytometry bead arrays according to the manufacturer’s instructions (BD Biosciences) and analyzed using flow cytometry (FACS Calibur, Biosciences, Franklin Lakes, NJ, USA). Kit detection limits were as follows: IL-1β, 7.2 pg/mL; IL-6, 2.5 pg/mL; IL-8, 3.8 pg/mL; IL-10, 3.3 pg/mL; IL-12p70, 1.9 pg/mL; and TNF-α, 3.7 pg/mL. The upper limit for all cytokines was 2500 pg/mL.
Laboratory Confirmation of Adenovirus Infection
The sample was collected by scraping the lower conjunctival sac using a calcium alginate swab (Eurotubo, S.A., Spain), and then placed in a transport medium containing 50 mg/mL gentamicin, 500 U/mL penicillin-streptomycin, 1 mg/mL fungizone, and 5% bovine serum albumin in Hank’s buffer (Gibco, Invitrogen Ltd., USA). Subsequently, all samples were processed at the clinical laboratory of the Institute of Ophthalmology “Conde de Valenciana” using the methodology described by Mejía-Lopez12 to identify adenovirus 8 infection through PCR.
Statistical Analysis
Parametric distribution was assessed using the Shapiro–Wilk test, comparisons between the more and less severely affected eyes were performed using the Mann–Whitney U-Test, and the Spearman test was used to assess correlations. GraphPad Prism 9 (GraphPad Software Inc., La Jolla, CA, US) and SPSS 22 (IBM Corporation, Armonk, NY, US) were used for statistical analysis. In all cases, p<0.05 was considered statistically significant. A colorblind-proof design is used in the bar graphs to represent the results.
Results
Demographics, Ocular Characteristics, and Clinical Background of Patients With Acute Adenovirus Conjunctivitis
The mean age of patients with adenovirus conjunctivitis was 47 ± 16 years (n = 14; nine women (64.2%) and five men (35.7%)). The evolution time since symptoms onset was 8.5 ± 5.0 days. The relevant medical history of patients is shown in Table 2 and more detailed in supplementary Table 1. The severity distributions in the affected eyes are depicted in supplementary Table 2. Score evaluation per sign and the affected eye is depicted in Figure 2.
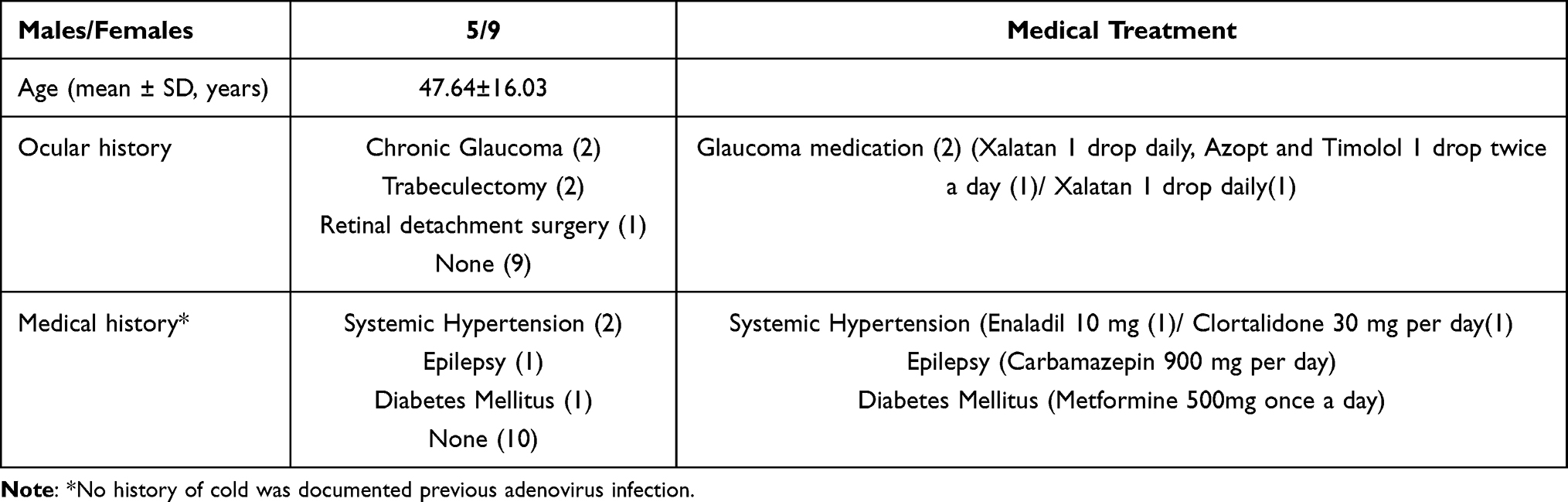 |
Table 2 Demographics and Clinical History of Patients With Acute Adenoviral Keratoconjunctivitis |
 |
Figure 2 Severity Score per sign in EKC-affected eyes. Scored severity by sign presentation in the total affected eyes (A), the less affected eyes (LAE) (B), and the most affected eyes (MAE) (C). Differential distribution was observed according to severity score and the clinical evaluation. |
The Proinflammatory Cytokines IL-8, IL-6, IL-1β, IL-12, and TNF-a Were Detected in Tears of Patients With Acute Adenoviral Conjunctivitis
All proinflammatory cytokines were detected in both eyes, to a slightly greater extent in the more severely affected eye (see Table 3). Cytokine expression was then evaluated by the fold of change in MAE/LAE; IL-10 and IL-12 showed the greatest interocular difference in expression, but this difference was not statistically significant (Figure 3). Tear cytokine expression per affected eye is depicted in supplementary Table 3.
 |
Table 3 Tear Cytokine Levels in Acute Adenoviral Conjunctivitis |
 |
Figure 3 Tear cytokines in patients with adenoviral keratoconjunctivitis. Levels of cytokines IL-1b, IL-6, IL-18, IL-10, and TNF-a were measured in the most affected eyes (MAE) and the less affected eyes (LAE) (A) Fold increase (interocular difference) per cytokine (MAE vs LAE) p-values are shown (B). Fold increase was obtained by dividing the average level of each cytokine in the MAE by that in the LAE. Most differences were found in IL-10 and IL-12. The dotted line indicates MAE/LAE quotient equal to 1 (zero interocular difference). |
Correlations Between Clinical Data and Tear Cytokines
Correlations between tear cytokine levels and disease severity are shown in Tables 4, 5, and Supplementary Table 4. Total Score correlated with IL-12 (r = 0.3552, p = 0.0345), IL-6 (0.3387, 0.0453), and IL-8 (0.3913, p = 0.024) (See Supplementary Table 4). In the most affected eyes, eyelid involvement and conjunctival swelling (CS) correlated with IL-10; CS also correlated with IL-6 (see Table 4). In the less affected eyes, inflammatory response, conjunctival hyperemia, and conjunctival hemorrhages were significantly correlated with IL-12 and TNF-a, while ocular discharge was significantly correlated with all tear cytokines (see Table 5). Interestingly, TNF-α correlations with evolution time and patient age were significant in the less affected eyes (Table 5).
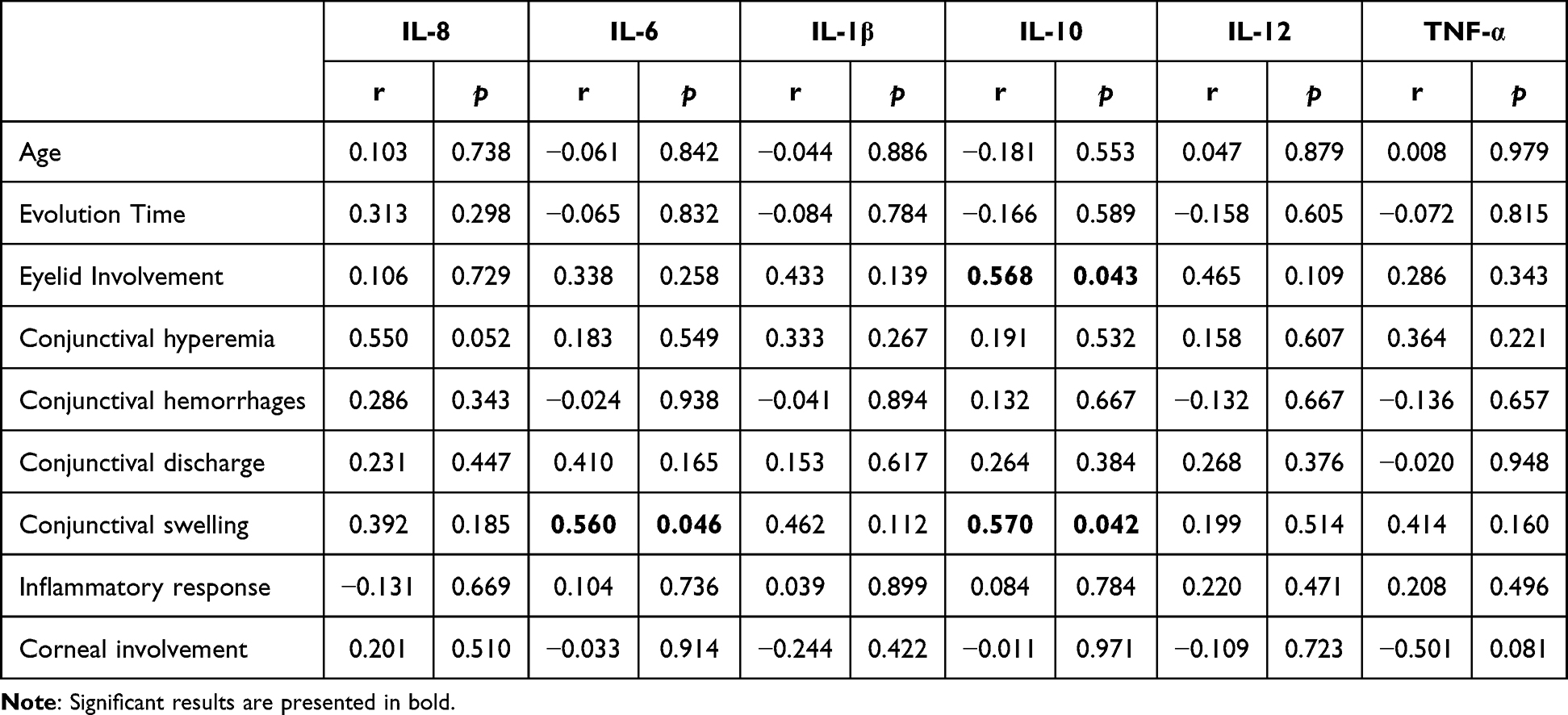 |
Table 4 Correlation Matrix Between Clinical Data and Tear Cytokines in the Most Affected Eyes |
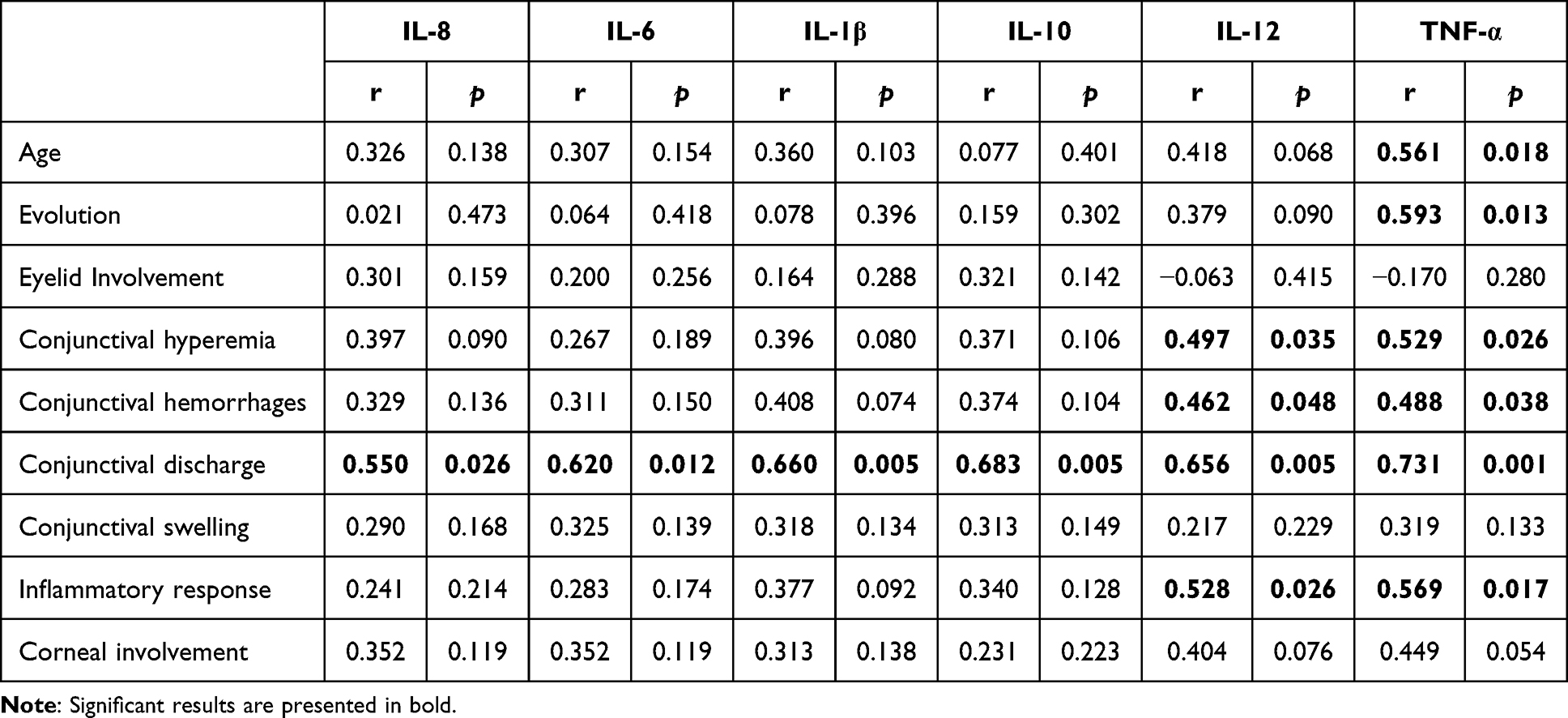 |
Table 5 Correlation Matrix Between Clinical Data and Tear Cytokines in the Less Affected Eyes |
Discussion
Adenoviruses are spread globally by droplets and smears of contaminated bodily fluids that enter through the nose, throat, and conjunctiva. This work aimed to study proinflammatory mediators in epidemic keratoconjunctivitis to understand the pathophysiological mechanisms involved in clinical ophthalmological changes. In accordance with our hypothesis, all proinflammatory tear cytokines were detected in both eyes. Several years ago, Chodosh et al9 suggested that infected human corneal stromal fibroblasts were able to generate IL-8 after infection with AdV19; similarly, porcine corneal cells infected with AdV 37 are capable of inducing IL-8 mRNA.13 IL-8 is a chemokine involved in the cellular homing of neutrophils; in the eye, IL-8 has been involved in several diseases, such as allergies, uveitis, glaucoma,14 and microbial infections.11,15 Regarding proinflammatory cytokines in the healthy ocular surface, some studies have demonstrated that IL-6 and IL-8 are present in tears but at very low concentrations.16–18 Our results suggest a relevant role of IL-8 and IL-6 in adenoviral conjunctivitis; however, the lack of healthy controls limits our conclusions. It is important to note that IL-8 and IL-6 are key molecules involved in inflammation and have been reported in dry eye,19 microbial keratitis,11 allergic conjunctivitis,20 and keratoconus.21 These reports reinforce the positive and significant association between the inflammatory response, conjunctival hyperemia, hemorrhages, and proinflammatory tears cytokines observed in our work.
The presence of IL-10 and IL-12 in EKC patients’ tears has several biological implications. IL-12 has a variety of functions, such as induction of Th1 immune response, increased effectiveness against viral infection, and promotion of local inflammation.22 The involvement of IL-12 in pathological conditions has been reported in herpetic keratitis15 and diabetic retinopathy.23 Its presence in chronic conditions implies a role in sustaining local inflammation as well as participation in long-term ophthalmological clinical changes associated with corneal adenoviral infections, such as subepithelial infiltrates. In contrast, IL-10 has anti-inflammatory and anti-angiogenic properties in ocular tissues such as the conjunctiva and cornea;24 therefore, their expression might be associated with a failed attempt to avoid inflammation at the ocular surface. Further studies would be necessary to address IL-10 function in EKC.
The severity score used in this study was developed to analyze the ophthalmological characteristics in EKC and their possible association with a specific proinflammatory tear cytokine. The score incorporates a few clinical variables (the most frequent clinical signs) to understand the involvement of some tear cytokines in clinical presentations. Van Gelder et al established a clinical score to evaluate the clinical presentation of human AdVE4 vs AdVD8. Like us, they classified symptoms and signs based on eye severity, including the worst seeing eye when bilateral involvement occurred. Although their data did not show statistically significant differences between groups, they proposed five signs and symptoms based on moderate or severe scores, implying that some clinical presentations could be influenced by the molecular basis of these two viral types.25 Our findings showed high variability between patients, and we did not find any cytokine profile associated directly with the clinical ophthalmological severity. The data dispersion in our results could be explained by sample size, lack of a standardized international system to evaluate clinical severity in adenovirus infection, lack of symptoms evaluation, differences in evolution time at tear sampling, age presentation, and comorbidities. Remarkably, the intra-group variability observed in our findings underscores the complexity of the relationship between cytokine profiles and the clinical severity of EKC. In this context, comorbidities such as glaucoma26 and diabetes27 have been reported to significantly alter tear cytokine profiles, modifying cytokine concentrations directly related to the viral infection. Another critical consideration is the possible influence of age and sex-related immunological variations; it is known that older patients may have different systemic cytokine profiles than younger individuals due to immunosenescence, and hormonal changes could affect the tear profile.28,29
In addition, molecular explanations for the variability in clinical phenotypes, such as viral load30 and cytokine polymorphisms, have also been proposed.31 The viral burden is associated with developing subepithelial infiltrates, while IL-6 polymorphisms are involved in several ocular inflammatory diseases. Furthermore, diurnal rhythms have been linked to tear cytokine variations;32 Uchino et al observed higher levels of proinflammatory cytokines (IL-6, IL-1b, and TNF-a) at 12:00 am than at 9:00 am. In our study, sampling was performed in this time range; thus, diurnal differences during tear collection could also explain the high variability observed in the EKC patients. Another limitation of our investigation was the methodology employed in tear sample collection; several authors have demonstrated that the detection of specific proteins may vary based on the method utilized; thus, the results could be interpreted cautiously.33–35
Although we did not find a characteristic cytokine profile that could describe a specific severity grade in adenoviral conjunctivitis, our work shows the involvement of IL-6, IL-8, and IL-12, in EKC. It is essential to highlight that these cytokines could contribute to the dysregulation of the local microenvironment, resulting in ocular surface damage and clinical appearance. More studies exploring the immunological basis of human adenoviral conjunctivitis will lead to new treatments for EKC by targeting proinflammatory cytokines.
Acknowledgments
We would like to thank Verónica Romero for her technical assistance.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was partially supported by “Conde de Valenciana Foundation” and Department of Biochemistry, Faculty of Medicine, UNAM.
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Garcia-Zalisnak D, Rapuano C, Sheppard JD, Davis AR. Adenovirus ocular infections: prevalence, pathology, pitfalls, and practical pointers. Eye Contact Lens. 2018;44:S1–S7. doi:10.1097/ICL.0000000000000226
2. Kosulin K. Intestinal HAdV infection: tissue specificity, persistence, and implications for antiviral therapy. Viruses. 2019;11:804. doi:10.3390/v11090804
3. Robinson CM, Singh G, Lee JY, et al. Molecular evolution of human adenoviruses. Sci Rep. 2013;3:1812. doi:10.1038/srep01812
4. Omari AA, Mian SI. Adenoviral keratitis: a review of the epidemiology, pathophysiology, clinical features, diagnosis, and management. Current Opinion Ophthalmol. 2018;29:365–372. doi:10.1097/ICU.0000000000000485
5. Shorter ES, Whiteside MM, Harthan JS, et al. Diagnostic accuracy of clinical signs, symptoms and point-of-care testing for early adenoviral conjunctivitis. Clin Exp Optometry. 2021;104:1–6. doi:10.1080/08164622.2021.1984180
6. Gouider D, Khallouli A, Maalej A, Khochtali S, Khairallah M. Role of anterior segment optical coherence tomography in monitoring epidemic keratoconjunctivitis. J Curr Ophthalmol. 2021;33:408. doi:10.4103/joco.joco_218_20
7. Jhanji V, Chan TCY, Li EYM, Agarwal K, Vajpayee RB. Adenoviral keratoconjunctivitis. Survey Ophthalmol. 2015;60:435–443. doi:10.1016/j.survophthal.2015.04.001
8. Jonas RA, Ung L, Rajaiya J, Chodosh J. Mystery eye: human adenovirus and the enigma of epidemic keratoconjunctivitis. Prog Retinal Eye Res. 2020;76:100826. doi:10.1016/j.preteyeres.2019.100826
9. Chodosh J, Astley RA, Butler MG, Kennedy RC. Adenovirus keratitis: a role for interleukin-8. Invest Ophthalmol Vis Sci. 2000;41:783–789.
10. Chodosh J. Human adenovirus type 37 and the BALB/c mouse: progress toward a restricted adenovirus keratitis model (an American Ophthalmological Society thesis). Trans Am Ophthalmol Soc. 2006;104:346–365.
11. Santacruz C, Linares M, Garfias Y, et al. Expression of IL-8, IL-6 and IL-1β in tears as a main characteristic of the immune response in human microbial keratitis. Int J mol Sci. 2015;16:4850–4864. doi:10.3390/ijms16034850
12. Melendez CP, Florentino MM, Martinez IL, Lopez HM. Outbreak of epidemic keratoconjunctivitis caused by adenovirus in medical residents. Mol Vis. 2009;15:557–562.
13. Ramke M, Lam E, Meyer M, Knipper A, Heim A. Porcine corneal cell culture models for studying epidemic keratoconjunctivitis. Mol Vis. 2013;19:614–622.
14. Ghasemi H, Ghazanfari T, Yaraee R, Faghihzadeh S, Hassan ZM. Roles of IL-8 in ocular inflammations: a review. Ocul Immunol Inflamm. 2011;19:401–412. doi:10.3109/09273948.2011.618902
15. Marino A, Pergolizzi S, Cimino F, et al. Role of herpes simplex envelope glycoprotein B and toll-like receptor 2 in ocular inflammation: an ex vivo organotypic rabbit corneal model. Viruses. 2019;11:819. doi:10.3390/v11090819
16. Lam H, Bleiden L, de Paiva CS, Farley W, Stern ME, Pflugfelder SC. Tear cytokine profiles in dysfunctional tear syndrome. Am J Ophthalmol. 2009;147:198–205.e1. doi:10.1016/j.ajo.2008.08.032
17. Landsend ECS, Utheim ØA, Pedersen HR, et al. the level of inflammatory tear cytokines is elevated in congenital aniridia and associated with meibomian gland dysfunction. Invest Ophthalmol Vis Sci. 2018;59:2197. doi:10.1167/iovs.18-24027
18. Jun AS, Cope L, Speck C, et al. Subnormal cytokine profile in the tear fluid of keratoconus patients. PLoS One. 2011;6:e16437. doi:10.1371/journal.pone.0016437
19. Roda M, Corazza I, Bacchi Reggiani ML, et al. Dry eye disease and tear cytokine levels-A meta-analysis. Int J mol Sci. 2020;21:E3111. doi:10.3390/ijms21093111
20. Salazar A, Casanova-Méndez I, Pacheco-Quito M, et al. Low expression of IL-10 in circulating bregs and inverted IL-10/TNF-α ratio in tears of patients with perennial allergic conjunctivitis: a preliminary study. Int J mol Sci. 2019;20:E1035. doi:10.3390/ijms20051035
21. Peyman A, Namgar M, Feizi A, Hakemi MG, Nasab FH, Pourazizi M. Interleukin-6 and tumor necrosis factor-α levels in tear film of Keratoconus patients. J Res Med Sci. 2021;26:75. doi:10.4103/jrms.jrms_35_21
22. Vignali DAA, Kuchroo VK. IL-12 family cytokines: immunological playmakers. Nat Immunol. 2012;13:722–728. doi:10.1038/ni.2366
23. Gverović Antunica A, Karaman K, Znaor L, Sapunar A, Buško V, Puzović V. IL-12 concentrations in the aqueous humor and serum of diabetic retinopathy patients. Graefes Arch Clin Exp Ophthalmol. 2012;250:815–821. doi:10.1007/s00417-011-1905-4
24. Ghasemi H, Ghazanfari T, Yaraee R, Owlia P, Hassan ZM, Faghihzadeh S. Roles of IL-10 in ocular inflammations: a review. Ocul Immunol Inflamm. 2012;20:406–418. doi:10.3109/09273948.2012.723109
25. Van Gelder RN, Akileswaran L, Nakamichi K, Stroman D. Molecular and clinical characterization of human adenovirus E4–associated conjunctivitis. Am J Ophthalmol. 2022;233:227–242. doi:10.1016/j.ajo.2021.10.028
26. Mravec Bencurova D, Vyborny P, Dankova P. Comparative analysis of tear cytokines in patients with glaucoma, ocular hypertension, and healthy controls. Int Ophthalmol. 2023;43:3559–3568. doi:10.1007/s10792-023-02763-6
27. Liu J, Shi B, He S, Yao X, Willcox MDP, Zhao Z. Changes to tear cytokines of type 2 diabetic patients with or without retinopathy. Mol Vis. 2010;16:2931–2938.
28. Micera A, Di Zazzo A, Esposito G, et al. Age-related changes to human tear composition. Invest Ophthalmol Vis Sci. 2018;59:2024. doi:10.1167/iovs.17-23358
29. Fernández I, Enríquez-de-Salamanca A, Portero A, García-Vázquez C, Calonge M, Herreras JM. Age- and sex-adjusted reference intervals in tear cytokine levels in healthy subjects. Appl Sci. 2021;11:8958. doi:10.3390/app11198958
30. Isik P, Harbiyeli II, Ozturk G, Erdem E, Yagmur M, Yarkin F. The relationship between clinical findings and viral load in adenoviral keratoconjunctivitis. Jpn J Infect Dis. 2022;75:592–596. doi:10.7883/yoken.JJID.2022.210
31. Ulhaq ZS, Soraya GV, Budu, Wulandari LR. The role of IL-6-174 G/C polymorphism and intraocular IL-6 levels in the pathogenesis of ocular diseases: a systematic review and meta-analysis. Sci Rep. 2020;10:17453. doi:10.1038/s41598-020-74203-9
32. Uchino E, Sonoda S, Kinukawa N, Sakamoto T. Alteration pattern of tear cytokines during the course of a day: diurnal rhythm analyzed by multicytokine assay. Cytokine. 2006;33:36–40. doi:10.1016/j.cyto.2005.11.013
33. Bachhuber F, Huss A, Senel M, Tumani H. Diagnostic biomarkers in tear fluid: from sampling to preanalytical processing. Sci Rep. 2021;11:10064. doi:10.1038/s41598-021-89514-8
34. Pieczyński J, Szulc U, Harazna J, Szulc A, Kiewisz J. Tear fluid collection methods: review of current techniques. Eur J Ophthalmol. 2021;31:2245–2251. doi:10.1177/1120672121998922
35. Lam SM, Tong L, Duan X, Petznick A, Wenk MR, Shui G. Extensive characterization of human tear fluid collected using different techniques unravels the presence of novel lipid amphiphiles. J Lipid Res. 2014;55:289–298. doi:10.1194/jlr.M044826
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Development of Biomarkers and Prognosis Model of Mortality Risk in Patients with COVID-19
Zhang Z, Tang L, Guo Y, Guo X, Pan Z, Ji X, Gao C
Journal of Inflammation Research 2024, 17:2445-2457
Published Date: 22 April 2024
Based on the Dual Pathway of Interaction-Mediated NF-κB in Cell Apoptosis and Immune Inflammation to Study the Effect of Danzhi Xiaoyao Powder on the Learning and Cognitive Ability of AD Model Rats
Wang HP, Li MC, Yang J, Zhou J, Meng ZP, Hu YY, Lyu YJ, Chen YQ, Han YM, Pei WL
Degenerative Neurological and Neuromuscular Disease 2025, 15:41-64
Published Date: 14 April 2025
The Relationship Between IL-6 and IL-10 Expression Levels and the Prognosis in B-Cell Non-Hodgkin Lymphoma Patients Treated with R-CHOP
Dong Q, Lin W, Yu S, Qin Y, Jia C, Wang N, Xiu W, Shan W, Dong M, Liu D
Journal of Inflammation Research 2025, 18:14791-14804
Published Date: 25 October 2025