Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
The Effectiveness of a Self-Management-Based Nutritional Promotion Program on Food Consumption Knowledge, Behaviors, and Quality of Life of Patients Undergoing Hemodialysis
Authors Maytharit B, Wungrath J, Ong-artborirak P ![]() , Chautrakarn S
, Chautrakarn S ![]()
Received 7 January 2026
Accepted for publication 1 April 2026
Published 14 April 2026 Volume 2026:19 591842
DOI https://doi.org/10.2147/JMDH.S591842
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr David C. Mohr
Bowornjit Maytharit,1 Jukkrit Wungrath,2 Parichat Ong-artborirak,3 Sineenart Chautrakarn1
1Faculty of Public Health, Chiang Mai University, Chiang Mai, 50200, Thailand; 2ASEAN Institute for Health Development, Mahidol University, Nakhon Pathom, 73170, Thailand; 3Department of Research and Medical Innovation, Faculty of Medicine Vajira Hospital, Navamindradhiraj University, Bangkok, 10300, Thailand
Correspondence: Sineenart Chautrakarn, Faculty of Public Health, Chiang Mai University, 239, Huay Kaew Road, Muang District, Chiang Mai, Thailand, 50200, Tel +6653942503, Fax +6653942525, Email [email protected]
Background: Patients undergoing hemodialysis (HD) often experience food consumption and nutritional challenges that affect their health outcomes and quality of life (QoL). Traditional nutritional education alone may be insufficient to promote sustainable behavioral change. The self-management concept, which emphasizes patients’ active involvement in managing their health, has been insufficiently applied among HD patients in Thailand.
Purpose: This study evaluated the effectiveness of a nutritional promotion program in improving the QoL of HD patients, based on the self-management concept of Creer (2000).
Methods: A quasi-experimental design was employed with 110 HD patients recruited from two dialysis centers in Sakon Nakhon Province, Thailand. Participants were equally allocated to experimental (n = 55) and control (n = 55) groups. The experimental group received a 12-week nutritional promotion program based on the self-management concept of Creer (2000), which consisted of individual face-to-face education, group-based educational content via the LINE application, individualized tele-counseling, and group discussions, while the control group received standard care. Data were collected using the Kidney Disease Quality of Life-Short Form (KDQOL-SF™), version 1.3, and analyzed using descriptive statistics and repeated measures ANOVA.
Results: The results indicated no significant differences in demographic characteristics or baseline mean QoL scores between groups. The experimental group showed significant improvements in food consumption knowledge, food consumption behaviors, and QoL (p < 0.05) across time points compared with the control group.
Conclusion: The nutritional promotion program grounded in Creer’s (2000) self-management framework, integrating individualized education, structured group-based LINE content, individualized tele-counseling, and group discussions, effectively improved food consumption knowledge, food consumption behaviors, and QoL in HD patients. The program strengthened patients’ capacity for self-regulation of food consumption behaviors and enhanced their overall well-being. These findings underscore the potential of hybrid, self-management-based nutritional interventions as a patient-centered approach to improving key outcomes in HD care.
Keywords: nutritional promotion program, quality of life, hemodialysis, self-management, food consumption knowledge, food consumption behaviors
Introduction
Chronic kidney disease (CKD) has emerged as a major global public health concern, characterized by progressive and irreversible impairment of renal function. According to the Global Burden of Disease Study 2017, CKD accounted for 1.2 million deaths worldwide, representing a 41.5% increase in mortality since 1990.1 Moreover, an estimated 697.5 million people were affected by CKD globally, with the prevalence increasing by 29.3% across all age groups during the same period. The World Health Organization (WHO) reported that kidney diseases have risen from the nineteenth to the ninth leading causes of death globally, accompanied by an estimated 95% increase in mortality between 2000 and 2021.2 This steady upward trend underscores the urgent need for effective management strategies to address the disease and its consequences.
In Thailand, CKD is similarly recognized as a pressing national health challenge. The prevalence of CKD stages 3–5 among adults has been reported at approximately 8.45%, with higher rates observed in the northern and northeastern regions of the country.3,4 For patients who progress to end-stage renal disease (ESRD), renal replacement therapy (RRT) is indispensable for survival. The three main methods of RRT, which include peritoneal dialysis (PD), hemodialysis (HD), and kidney transplantation (KT), have distinct benefits and limitations. Among these methods, HD is the most commonly utilized in Thailand. This utilization pattern is associated, in part, with the national health policy under the Universal Coverage Scheme, which enables eligible ESRD patients to access either PD or HD services free of charge through shared decision-making with their nephrologists.5
Although HD sustains life, it does not provide a definitive cure. Patients undergoing long-term HD face multiple burdens that extend beyond the biological aspects of renal failure. These include persistent complications, food consumption and fluid restrictions, frequent hospital visits, and significant psychosocial challenges. The studies have shown that patients receiving HD are at high risk of depression, anxiety, and diminished QoL due to the chronic nature of the therapy and the disruptions it imposes on daily living.6–9 Furthermore, economic burdens associated with treatment costs, transportation, and reduced productivity compound the physical and emotional stress experienced by patients.10,11
Malnutrition is a common complication among patients with ESRD, particularly those receiving HD, and is a major contributor to morbidity and mortality.12,13 Its multifactorial causes include pre-dialysis food consumption restrictions, appetite loss, and increased catabolism during dialysis. Non-adherence to recommended food consumption guidelines often results in inadequate intake of essential nutrients, including vitamins, minerals, and energy.14 However, barriers such as limited dietary knowledge, insufficient access to dietitians, and cultural or socioeconomic constraints impede optimal nutritional care.15 Therefore, effective nutritional management is essential in HD to prevent malnutrition and related complications.
In Thailand, nutritional education for patients undergoing hemodialysis is commonly provided by healthcare professionals during routine clinical care, focusing on dietary restrictions and appropriate nutrient intake. However, such education is often delivered primarily through conventional knowledge-based counseling, which may have limitations in promoting sustained dietary behavioral change. Consequently, traditional nutrition education approaches may have limited effectiveness in supporting long-term adherence, leading to an increased interest in self-management-oriented interventions. This recognition has encouraged the development of theory-based approaches that promote patient empowerment and self-regulation. The concept of self-management, as proposed by Creer (2000), emphasizes patients’ active participation in managing their health through goal selection, information collection, information processing and evaluation, decision-making, action, and self-reaction.16 This concept has been successfully applied in chronic diseases such as diabetes, hypertension, and asthma, demonstrating improved disease control and QoL.17–20 However, limited research has applied this framework to nutritional interventions for HD patients. In Thailand, evidence on self-management-based nutritional interventions for HD patients remains particularly limited.
In response, this study developed and evaluated a nutritional promotion program grounded in Creer’s self-management concept, delivered through multimodal strategies that included individual face-to-face education, group-based health education delivered via the LINE application through videos and infographics, individualized tele-counseling via LINE, and group discussions. This comprehensive approach was designed to enhance patients’ food consumption knowledge, strengthen their self-management skills, and improve adherence to recommended food consumption practices, ultimately contributing to better nutritional status and overall QoL. The study’s findings are expected to provide evidence-based guidance for healthcare professionals in implementing contextually-appropriate interventions that promote improved QoL among HD patients.
Materials and Methods
Study Design, Setting, and Samples
This quasi-experimental study was conducted from July to December 2024. Participants were patients with ESRD stage 5 who were undergoing HD at two hemodialysis centers in Sakon Nakhon Province, Thailand. Sakon Nakhon is a province in northeastern Thailand. In terms of demographic and socioeconomic context, the area is considered rural. It is quite comparable to other rural areas in Thailand in terms of population characteristics and socioeconomic background.
The inclusion criteria were patients undergoing HD aged between 20 and 70 years, who had been receiving treatment for at least three months, were able to consume meals, and could communicate effectively in Thai without any communication impairments. In addition, participants were required to be accessible via mobile phone with the LINE application and to provide informed consent before enrollment. Participants were excluded if they had major debilitating comorbidities, including congestive heart failure (stage III or IV), terminal malignancy, acquired immunodeficiency syndrome (AIDS), psychiatric disorders, dementia, or other severe conditions that could adversely affect food consumption.
The sample size was calculated using G*Power software based on the difference between two independent means (two groups) as the statistical test, with a one-tailed test, a statistical power of 0.80, an alpha level of 0.05, and an effect size of 0.50. The required sample size was determined to be 51 participants per group. To account for potential attrition during the study, the sample size was increased by 10%. Consequently, each group comprised 56 participants. The experimental group (n = 56) received the nutritional promotion program, whereas the control group (n = 56) received standard care.
This study employed purposive selection of study sites. Two HD centers were purposively chosen based on pragmatic considerations, feasibility of data collection, and contextual similarity. The participants in both the experimental group and control group were HD patients who received dialysis services at two different HD centers in Sakon Nakhon Province. The participants in the experimental group had no contact with those in the control group, as they were situated in different HD centers. One HD center was assigned to the experimental group, while the other was assigned to the control group. Therefore, the participants in the control group received only standard care, whereas those in the experimental group received the nutritional promotion program. Following site selection, eligible participants were recruited using consecutive sampling during the study period.
Research Instrument
The research instruments consisted of four components, developed based on a review of the relevant literature.
The first section was a demographic questionnaire for HD patients, which included questions about age, gender, marital status, education level, occupation status, monthly income, health scheme, person responsible for food preparation, duration of HD, and frequency of HD each week.
The second questionnaire was a food consumption knowledge test, which consisted of 17 items related to dietary knowledge specific to HD patients, including foods that should be consumed and foods that should be avoided. All items were presented as true or false. Scoring was based on correctness: a correct response received a score of one, while an incorrect response received a zero.
The third questionnaire was a food consumption behavior questionnaire. It consisted of 23 items related to commonly consumed food types, ingredients used in food preparation, and frequency of food consumption. Responses were measured using a five-point rating scale based on the Likert scale concept, including never, rarely, sometimes, often, and always.
The content validity of the food consumption knowledge questionnaire and the food consumption behavior questionnaire was assessed by a panel of three experts, including a nutrition specialist, a nephrologist, and a health behavior specialist. The reliability of both instruments was evaluated through pilot testing among 30 HD patients with characteristics similar to those of the study participants. The reliability of both tools was assessed through pilot testing on 30 HD patients with characteristics similar to those of the research participants. The reliability value for the food consumption knowledge questionnaire was 0.64, as measured by the Kuder-Richardson formula (KR-20), whereas the Cronbach’s alpha coefficient for the food consumption behavior questionnaire was 0.83.
The final section of the questionnaire was the Kidney Disease Quality of Life-Short Form (KDQOL-SF™) version 1.3.21,22 The generic core includes 36 items across eight dimensions: physical function (10 items), role-physical (4 items), pain (2 items), general health (5 items), emotional well-being (5 items), role-emotional (3 items), social function (2 items), energy/fatigue (4 items), and an overall health rating item. The disease-specific core includes 43 items covering 11 dimensions: symptom/problem list (12 items), effects of kidney disease (8 items), burden of kidney disease (4 items), work status (2 items), cognitive function (3 items), quality of social interaction (3 items), sexual function (2 items), sleep (4 items), social support (2 items), dialysis staff encouragement (2 items), and patient satisfaction (1 item). Scores for all subscales are transformed to a range between 0 and 100, with higher scores indicating better QoL. The overall quality of life is summarized into three composite scores: PCS (Physical Component Summary), MCS (Mental Component Summary), and KDCS (Kidney Disease Component Summary).
Study Intervention
The nutritional promotion program comprised a set of activities designed to promote the nutritional status and appropriate food consumption of patients undergoing HD. The program was developed by the researcher based on a review of the relevant literature and was grounded in the self-management concept of Creer (2000).16 It consisted of the following components: 1) Goal selection involved providing patients with essential knowledge before they set personal goals aimed at maintaining appropriate nutritional status. The educational content included information on CKD and dietary recommendations suitable for patients undergoing HD, delivered through face-to-face sessions and a take-home dietary handbook developed specifically for HD patients. In addition, the LINE application was utilized as a supplementary platform for delivering nutritional education; 2) Information collection, which involved maintaining a daily dietary intake record and self-monitoring; 3) Information processing and evaluation, which involved taking the data obtained from the information collection to determine how to adjust food consumption behavior to meet defined criteria or goals; 4) Decision making, which involves selecting appropriate foods for the disease based on the information gathered and evaluated; 5) Action, which referred the implementation of the plan through self-management in selecting foods appropriate for the disease.; and 6) Self-reaction, which referred to the patient’s self-assessment to determine whether their food intake aligns with the proper dietary plan for their condition. Complementing face-to-face education sessions and group discussions, the program also utilized the LINE application as a platform for delivering nutritional education to patients undergoing HD through video clips and infographics, as well as for providing tele-counseling. These strategies served as key components in supporting follow-up and monitoring patients’ adherence to dietary recommendations.
The experimental group received a 12-week nutritional promotion program based on the self-management concept of Creer (2000). Education was provided by the researcher once a week throughout the 12-week intervention period, with each session lasting approximately 30–50 minutes, depending on the content and learning activities. The intervention was designed to support the six key processes of self-management: goal selection, information collection, information processing and evaluation, decision making, action, and self-reaction. These processes guided the structure and implementation of all intervention activities. The program consisted of individual face-to-face education, group-based educational content delivered via the LINE application, individualized tele-counseling, and group discussions. The educational content in this intervention was based on information from the Clinical Practice Recommendation for Nutritional Management in Adult Kidney Patients 2018 by the Society of Parenteral and Enteral Nutrition of Thailand in collaboration with the Nephrology Society of Thailand.23
The control group did not receive any specific intervention during the 12-week study period. Participants continued their standard care according to the routine dietary recommendations provided by their healthcare professionals. To ensure ethical considerations, after completion of the study, the nutritional promotion program was also provided to the control group in the same manner as that received by the intervention group.
Data Collection
In the experimental group, food consumption knowledge, food consumption behavior, and QoL were assessed using the KDQOL-SF version 1.3 at three time points: baseline, 12 weeks after completion of the intervention program, and 16 weeks. Similarly, these outcomes in the control group were assessed using the same instrument at the corresponding time points: baseline, week 12, and week 16. The study flow and data collection process for both groups are illustrated in Figure 1.
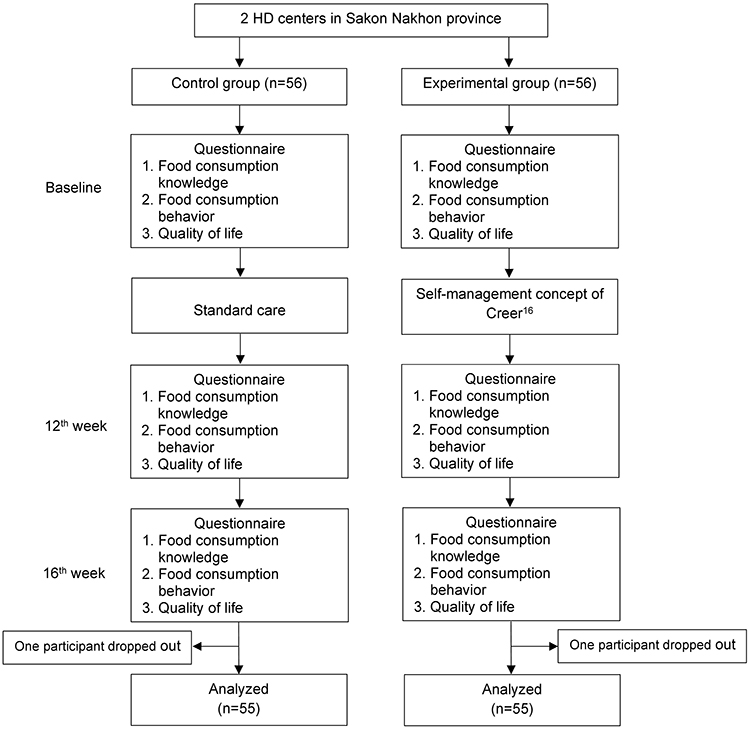 |
Figure 1 Data Collection Flowchart. |
Data Analysis
Data were analyzed by SPSS Version 29. Group differences in baseline demographic characteristics were examined using Chi-square tests or Fisher’s exact test. A repeated measures ANOVA was conducted to assess the effects of the nutritional promotion program over time (baseline, week 12, and week 16). A Bonferroni test was applied to identify which pairs of time points or groups showed significant differences. All statistical tests were conducted with a significance level set at p = 0.05.
Results
The characteristics of participants are summarized in Table 1. The control and experimental groups were comparable in terms of gender, age, marital status, education, occupation, income, health insurance coverage, food preparation responsibility, duration of hemodialysis, and frequency of dialysis sessions, with no statistically significant differences observed between the groups at baseline (p > 0.05). Overall, most participants were middle-aged (mean age = 53.58 ± 13.31 years in the control group and 49.85 ± 11.91 years in the experimental group), married, unemployed, and covered by the Universal Coverage Scheme (UCS). More than half had completed primary education, had no income, and had been undergoing hemodialysis for over three years, with the majority receiving treatment three times per week.
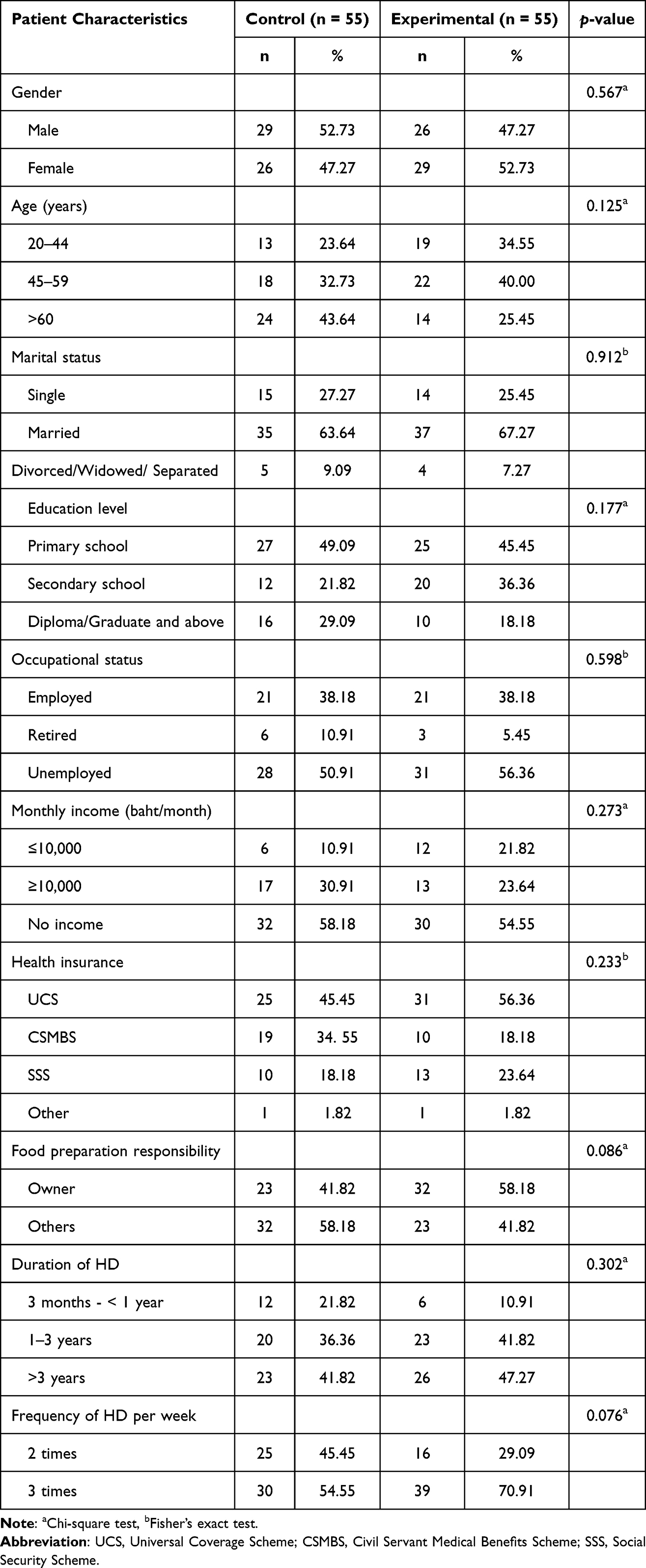 |
Table 1 Comparison of Demographic Characteristics Between the Control and the Experimental Groups |
The effects of the nutritional promotion program are presented in Table 2. Repeated measures ANOVA demonstrated significant effects on food consumption knowledge, food consumption behavior, and QoL domains, including physical, kidney disease-specific, and total QoL scores (p < 0.05), with a marginally significant effect observed for mental health (p = 0.057). A time-dependent effect was also observed across all outcomes (p < 0.05).
 |
Table 2 Repeated Measures ANOVA of Study Outcomes Over Time in the Control and Experimental Groups |
Pairwise comparisons demonstrated significant improvements in the experimental group across food consumption knowledge, food consumption behavior, and all QoL domains from baseline to weeks 12 or 16 following participation in the nutritional promotion program (p < 0.05). No significant between-group differences were observed at baseline; however, the experimental group showed significantly higher scores than the control group at weeks 12 and 16 for food consumption knowledge, physical and mental components, kidney disease-specific, and total QoL (p < 0.05). The results are presented in Table 3.
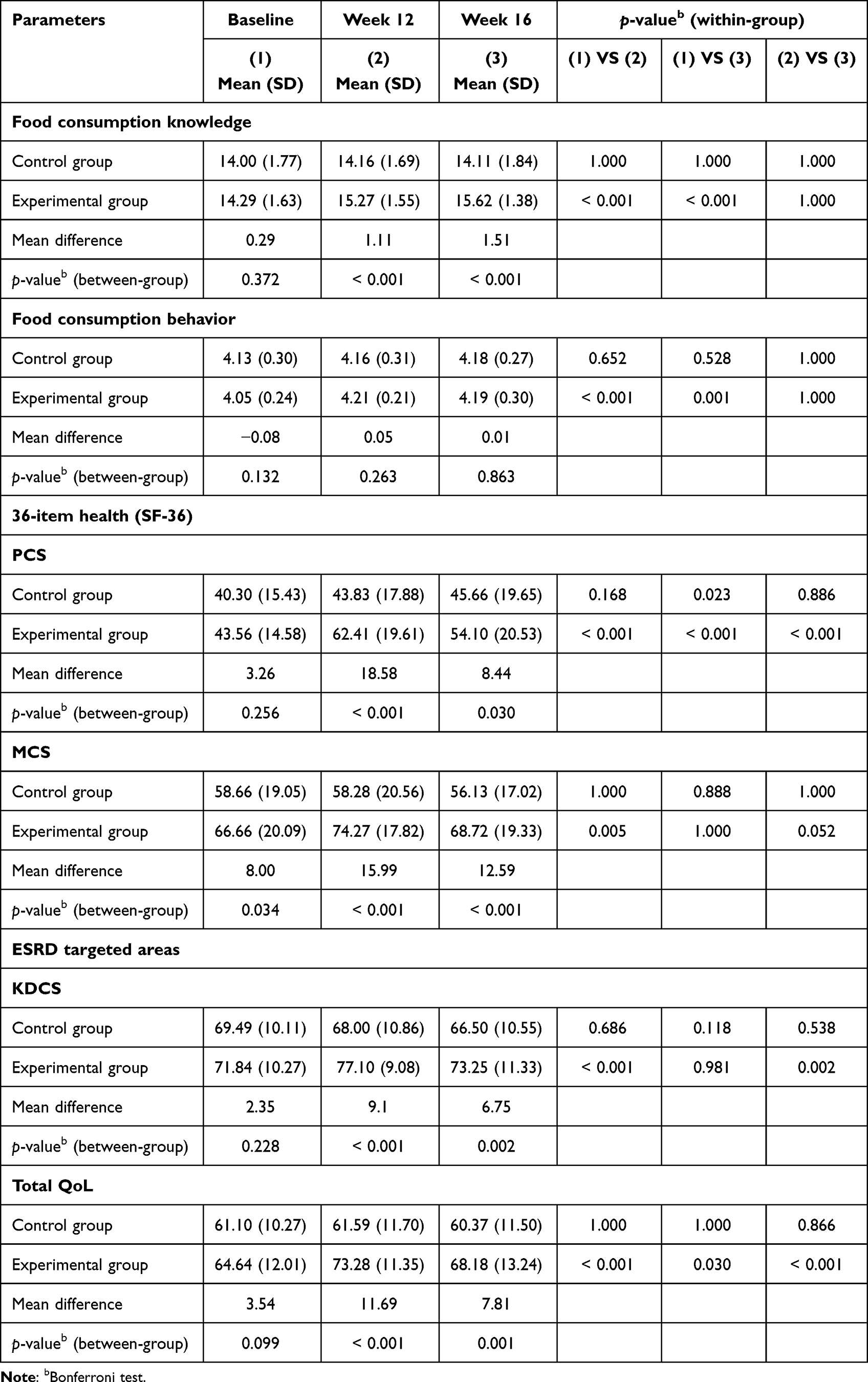 |
Table 3 Comparison of Study Outcomes Between the Control and Experimental Groups at Baseline, Week 12, and Week 16 |
Discussion
The present study demonstrated statistically significant improvements in food consumption knowledge, food consumption behavior, and QoL among patients undergoing HD who received the nutritional promotion program. All outcomes showed substantial gains from baseline to post-intervention in the experimental group, whereas the control group exhibited minimal or negligible changes over time. These findings indicate that the structured, multimodal intervention grounded in Creer’s (2000) self-management framework16 effectively enhanced patients’ capacity to regulate their food consumption practices and contributed to improved health-related QoL.
Improvements in food consumption knowledge can be explained through the preparatory role of knowledge within Creer’s self-management concept. According to Creer (2000), goal selection, the first formal step in self-management, can occur only when patients have acquired an adequate understanding of their illness and its management. Such knowledge forms the cognitive foundation for subsequent processes, enabling individuals to interpret information, anticipate consequences, and participate effectively in health-related decision-making.
In the present study, this foundation was strengthened through individualized face-to-face education, structured educational materials delivered via the LINE application, and individualized tele-counseling. These multimodal strategies provided repeated exposure to key dietary principles and allowed patients to clarify uncertainties in real time. The resulting improvements in food consumption knowledge are consistent with evidence from a systematic review showing that nutrition education significantly enhances nutritional and food consumption knowledge among HD patients.24 Moreover, evidence from a randomized controlled trial has demonstrated that educational interventions significantly improve both dietary knowledge and adherence among HD patients.25 These gains in food consumption knowledge established the essential cognitive groundwork for subsequent self-management processes, thereby supporting the progression toward the improvements in food consumption behaviors observed in this study.
Improvements in food consumption behavior can be interpreted through the intermediate processes of Creer’s (2000) self-management framework, particularly information processing and evaluation, decision making, action, and self-reaction. As patients acquired sufficient food consumption knowledge, they became more capable of appraising their eating patterns, identifying inconsistencies with renal dietary recommendations, and making appropriate adjustments. The program supported these processes by offering structured guidance on food selection, food-exchange principles, portion regulation, and essential renal dietary considerations, including sodium, potassium, phosphorus, protein, and fluid restriction, which were reinforced through LINE-based educational materials and individualized tele-counseling.
This multimodal reinforcement helped patients translate knowledge into practice, regulate daily food choices, and monitor adherence more effectively. These improvements align with evidence demonstrating that self-management interventions enhance adherence to appropriate food consumption practices and promote favorable behavioral outcomes among patients with ESRD. Jeentae26 reported improvements in phosphorus control behaviors following participation in a self-management program, whereas Doungpibool27 observed significant gains in eating behavior scores after implementing a 24-week behavioral self-management intervention. Advancements in mobile health technologies have further expanded the use of application-based and messaging-based interventions to support food consumption behavior change among patients with chronic illnesses, including those receiving HD. Such tools offer convenient, real-time access to nutritional information, personalized reminders, and channels for ongoing follow-up, thereby facilitating sustained adherence to dietary recommendations. The use of LINE-based educational reinforcement and tele-counseling in the present program reflects these principles. Consistent evidence further supports the effectiveness of these approaches. Kim and Cho28 demonstrated that an online community-based dietary self-care program improved dietary behaviors and physiological indicators in HD patients, while Saengyo29 found that combining LINE-based education with tele-counseling enhanced caregivers’ nutritional knowledge and dietary management behaviors for HD patients. Collectively, these findings indicate that integrating self-management principles with digital reinforcement strategies, particularly LINE-based education and tele-counseling, can effectively promote positive dietary behavior change among HD patients, as evidenced in the present study.
Improvements in QoL observed in this study can be understood through the successive self-management processes outlined in Creer’s framework, wherein enhanced food consumption knowledge supports more effective behavioral regulation and may contribute to more favorable self-reported health perceptions. As patients acquired adequate food consumption knowledge and translated this knowledge into appropriate food consumption behaviors, they became more capable of making informed dietary decisions and managing dietary restrictions with greater confidence. The enhanced food consumption knowledge likely strengthened patients’ confidence in managing dietary restrictions and supported more informed decision-making in daily food choices. These mechanisms were reflected in the study’s findings, which revealed notable improvements in total QoL as well as PCS, MCS, and KDCS scores, with the most pronounced gains emerging at week 12 and maintained through week 16. Improved food consumption behaviors may also have contributed to more stable symptom experiences and enhanced perceptions of daily functioning as patients applied dietary recommendations more consistently. Furthermore, sustained engagement with LINE-based educational reinforcement and individualized tele-counseling provided continuous guidance and support, thereby supporting psychological well-being and dialysis-related experiences, as reflected in higher MCS and KDCS scores.
These findings are consistent with previous research indicating that self-management interventions positively influence QoL in HD populations. Lee et al30 reported significant improvements in both physical and mental QoL domains following a structured self-management program, whereas El-Etreby and El-Monshed31 observed broad enhancements across multiple QoL subscales after implementing a similar intervention. Further supporting evidence comes from technology-assisted self-management research. Pack and Lee32 found that mobile-based health coaching enhanced self-efficacy and QoL among HD patients, emphasizing the value of digital platforms for reinforcing self-management skills. Chae and Kim33 demonstrated that a mobile self-management application grounded in social cognitive theory improved PD-related knowledge, health behaviors, albumin and hemoglobin levels, and health-related QoL across symptoms and daily activity. Similarly, Li et al34 showed that integrating wearable technologies, a health management platform, and social media tools such as LINE enhanced self-efficacy, self-management behaviors, and overall QoL among individuals with CKD undergoing long-term dialysis. Collectively, these findings indicate that the QoL improvements observed in this study likely resulted from the synergistic effects of enhanced food consumption knowledge, strengthened behavioral regulation, and ongoing digital reinforcement, all of which supported successive self-management processes consistent with Creer’s model. Through the integration of face-to-face education, LINE-based digital support, and individualized tele-counseling, the program facilitated a continuous cycle of knowledge acquisition, behavioral adjustment, and improved health perceptions, ultimately contributing to the QoL among patients undergoing HD.
The findings of this study demonstrate that combining Creer’s self-management framework with digital nutritional support provides a practical and effective approach to enhancing food consumption knowledge, improving food consumption behaviors, and ultimately promoting QoL among patients undergoing HD. The blended model integrating face-to-face education, group discussion, LINE-based reinforcement, and tele-counseling activated key self-management processes and proved both effective and clinically feasible. In addition, facilitator factors such as age, income, and educational level may be relevant to self-management. However, as baseline characteristics were comparable between the groups, these factors were unlikely to have substantially confounded the observed outcomes. Policy implications highlight the viability of incorporating digital self-management tools into routine HD care as a scalable, low-cost strategy for enhancing long-term patient outcomes. In practice, similar multimodal interventions may strengthen dietary adherence and reduce nutrition-related complications across diverse care settings. Overall, these results position technology-enhanced self-management as a sustainable and adaptable pathway for advancing patient-centered nutritional care and guiding future innovations in HD service delivery.
Limitations
This study has several limitations. First, the study was conducted in HD centers within a single province, which may limit the generalizability of the findings to other regions or healthcare settings. Second, the follow-up period was relatively short, restricting the ability to determine whether the improvements in QoL observed after the intervention can be sustained over the long term. Third, the QoL was assessed using a self-reported questionnaire, which may be influenced by recall bias, response bias, or subjective interpretation of the items. Self-reported measures may also be affected by social desirability and may not fully capture objective clinical changes. Future research should consider incorporating objective clinical indicators alongside self-reported measures to enhance accuracy and provide a more comprehensive assessment of patients’ health outcomes. In addition, future studies should involve more diverse clinical environments and employ longer follow-up durations to better examine the long-term effects of self-management–based nutritional interventions on the QoL of patients undergoing HD.
Conclusion
This study demonstrates that a nutritional promotion program grounded in Creer’s (2000) self-management framework, integrating individualized face-to-face education, structured group-based LINE educational content, individualized tele-counseling, and group discussions, with reinforcement provided through digital formats, effectively improves food consumption knowledge, food consumption behaviors, and QoL among patients undergoing HD. These findings highlight the feasibility and scalability of hybrid nutritional interventions as patient-centered strategies for routine HD care. Incorporating digital self-management support into standard practice may enhance continuity of guidance, reduce nutrition-related risks, and promote long-term adherence.
Ethics Approval
This study was reviewed and approved by the Research Ethics Committee of Chiang Mai University’s Faculty of Public Health (ET007/2567) on February 29, 2024, and the Human Research Ethics Committee of Sakon Nakhon Hospital (SKNH No.012/2567) on June 27, 2024. Prior to any study procedures being used in the study, all subjects provided written informed consent. The study was carried out in accordance with the ethical principles outlined in the Declaration of Helsinki, as well as the International Conference on Harmonization’s (ICH) Good Clinical Practice (GCP) guidelines, and all applicable regulatory requirements regarding data protection were met permanently.
Acknowledgments
The authors sincerely thank the Hemodialysis Center, Tanom Tai Center at Sakon Nakhon Hospital, Thailand, for their cooperation during data collection. We also extend our gratitude to all participants for their valuable contributions to this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bikbov B, Purcell CA, Levey AS; Collaboration GBDCKD. Global, regional, and national burden of chronic kidney disease, 1990–2017: a systematic analysis for the global burden of disease study 2017. Lancet. 2020;395(10225):709–14. doi:10.1016/S0140-6736(20)30045-3
2. World Health Organization. The top 10 causes of death [Internet]. World Health Organization. Available from: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death.
3. Ong-Ajyooth L, Vareesangthip K, Khonputsa P, Aekplakorn W. Prevalence of chronic kidney disease in Thai adults: a national health survey. BMC Nephrol. 2009;10(1):35. doi:10.1186/1471-2369-10-354
4. Ingsathit A, Thakkinstian A, Chaiprasert A, et al. Prevalence and risk factors of chronic kidney disease in the Thai adult population: thai SEEK study. Nephrol Dial Transplant. 2010;25(5):1567–1575. doi:10.1093/ndt/gfp669
5. National Health Security Office. NHSB gives nod to reimbursement payment for kidney patients opting for HD [Internet]. National Health Security Office. Available from: https://eng.nhso.go.th/view/1/home/IN%20DEPTH/407/EN-US.
6. Marthoenis M, Syukri M, Abdullah A, et al. Quality of life, depression, and anxiety of patients undergoing hemodialysis: significant role of acceptance of the illness. Int J Psychiatry Med. 2021;56(1):40–50. doi:10.1177/0091217420913382
7. Al Naamani Z, Gormley K, Noble H, Santin O, Al Maqbali M. Fatigue, anxiety, depression and sleep quality in patients undergoing haemodialysis. BMC Nephrol. 2021;22(1):157. doi:10.1186/s12882-021-02349-3
8. Alshelleh S, Alhawari H, Alhouri A, Abu-Hussein B, Oweis A. Level of depression and anxiety on quality of life among patients undergoing hemodialysis. Int J Gen Med. 2023;16:1783–1795. doi:10.2147/IJGM.S406535
9. Al-Nashri F, Almutary H. Impact of anxiety and depression on the quality of life of haemodialysis patients. J Clin Nurs. 2022;31(1–2):220–230. doi:10.1111/jocn.15900
10. Bello AK, Okpechi IG, Levin A, et al. An update on the global disparities in kidney disease burden and care across world countries and regions. Lancet Glob Health. 2024;12(3):e382–e395. doi:10.1016/S2214-109X(23)00570-3
11. Mohd Fadzli NFA, Mohd Rasani AA, Keng SL. Assessing the financial burden of hemodialysis treatment in Malaysia. Belitung Nurs J. 2021;7(6):529–534. doi:10.33546/bnj.1804
12. Bashardoust B, Gavami M, Maleki N, Doustkami H, Habibzadeh S. Mortality and nutritional status in patients undergoing hemodialysis. Shiraz E-Med J. 2015;16(2). doi:10.17795/semj20076
13. Rashid I, Sahu G, Tiwari P, et al. Malnutrition as a potential predictor of mortality in chronic kidney disease patients on dialysis: a systematic review and meta-analysis. Clin Nutr. 2024;43(7):1760–1769. doi:10.1016/j.clnu.2024.05.037
14. Ikizler TA, Burrowes JD, Byham-Gray LD, et al. KDOQI clinical practice guideline for nutrition in CKD: 2020 update. Am J Kidney Dis. 2020;76(3 Suppl 1):S1–S107. doi:10.1053/j.ajkd.2020.05.006
15. Cupisti A, Brunori G, Di Iorio BR, et al. Nutritional treatment of advanced CKD: twenty consensus statements. J Nephrol. 2018;31(4):457–473. doi:10.1007/s40620-018-0497-z
16. Creer TL. Self-management of chronic illness. In: Boekaerts M, Pintrich PR, Zeidner M, editors. Handbook of Self-Regulation. San Diego, CA: Academic Press; 2000:601–629. doi:10.1016/B978-012109890-2/50047-0
17. McManus RJ, Mant J, Bray EP, et al. Telemonitoring and self-management in the control of hypertension (TASMINH2): a randomised controlled trial. Lancet. 2010;376(9736):163–172. doi:10.1016/S0140-6736(10)60964-6
18. Norris SL, Lau J, Smith SJ, Schmid CH, Engelgau MM. Self-management education for adults with diabetes: a meta-analysis of the effect on glycemic control. Diabetes Care. 2002;25(7):1159–1171. doi:10.2337/diacare.25.7.1159
19. Ritklar L, Wattana C, Kitipawong P. Effects of a self-management program on self-management behaviors, dyspnea, activities of daily living, and quality of life among patients with congestive heart failure. Nurs J. 2012;39(1):64–76.
20. Ruengkajorn O, Kittiwatanapaisan W. The effectiveness of self-management program on self-management behavior and asthma controlled level in asthma patient at Ranode Hospital, Songkhla Province. J Nurs Sci Health. 2011;34(3):11–21.
21. Hays RD, Kallich JD, Mapes DL, et al. Kidney Disease Quality of Life–Short Form (KDQOL-SF™) Version 1.3: A Manual for Use and Scoring. RAND; 1997.
22. Homjean K. Reliability and validity of the Thai version of the kidney disease quality of life-short form questionnaire [master’s thesis]. Chulalongkorn University; 2009.
23. The Society of Parenteral and Enteral Nutrition of Thailand; The Nephrology Society of Thailand. Clinical Practice Recommendation for Nutritional Management in Adult Kidney Patients B.E. 2561 (2018). Bangkok: The Society of Parenteral and Enteral Nutrition of Thailand; 2018. Revised 2020.
24. Ouirdani M, Boutib A, Azizi A, et al. Impact of nutrition education on various health-related components of hemodialysis patients: a systematic review. Healthcare. 2024;12(12):1197. doi:10.3390/healthcare12121197
25. Dsouza B, Prabhu R, Unnikrishnan B, et al. Effect of educational intervention on knowledge and level of adherence among hemodialysis patients: a randomized controlled trial. Global Health Epidemiol Genom. 2023;2023:4295613. doi:10.1155/2023/4295613
26. Jeentae H. The effect of self-management program on phosphorus control behavior and blood phosphorus level of end-stage kidney disease undergoing hemodialysis at Inburi Hospital. J Environ Educ Med Health. 2025;10(1):620–629.
27. Doungpibool P. The development of self-management skills on eating behaviors for delayed chronic kidney disease in CKD clinic Watphleng Hospital. J Res Health Improv Qual Life. 2022;2(3):13–24.
28. Kim H, Cho MK. Development and effectiveness of dietary self-care promotion program using online community for hemodialysis patients: a pilot randomized controlled trial. Asian Nurs Res. 2025;19(2):126–135. doi:10.1016/j.anr.2025.01.007
29. Saengyo S, Rerkkasem K, Wungrath J. Effectiveness of a LINE application together with telephone-based consultation and education program on the dietary knowledge and behavior among caregivers of end-stage renal disease patients on hemodialysis. Malays J Public Health Med. 2023;23(2):282–290. doi:10.37268/mjphm/vol.23/no.2/art.2214
30. Lee JE, Kim HJ, Lee MJ, et al. Comparison of dietary intake patterns in hemodialysis patients by nutritional status: a cross-sectional analysis. Kidney Res Clin Pract. 2020;39(2):202–212. doi:10.23876/j.krcp.20.037
31. El-Etreby RR, AHE-S E-M. Effect of self-management program on quality of life for patients with chronic kidney disease. Am J Nurs Res. 2019;7(4):657–663. doi:10.12691/ajnr-7-4-27
32. Pack S, Lee J. Randomised controlled trial of a smartphone application-based dietary self-management program on haemodialysis patients. J Clin Nurs. 2021;30(5–6):840–848. doi:10.1111/jocn.15627
33. Chae YJ, Kim HS. Effects of a mobile application on improving self-management of adult patients receiving peritoneal dialysis: a randomized controlled trial. Jpn J Nurs Sci. 2024;21(1):e12555. doi:10.1111/jjns.12555
34. Li WY, Chiu FC, Zeng JK, et al. Mobile health app with social media to support self-management for patients with chronic kidney disease: prospective randomized controlled study. J Med Internet Res. 2020;22(12):e19452. doi:10.2196/19452
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Factors Affecting Quality of Life in Hemodialysis Patients
Yonata A, Islamy N, Taruna A, Pura L
International Journal of General Medicine 2022, 15:7173-7178
Published Date: 12 September 2022
Quality of Life and Adherence to Healthcare Services During the COVID-19 Pandemic: A Cross-Sectional Analysis
Hassan SUN, Zahra A, Parveen N, Khatoon F, Bangi NA, Hosseinzadeh H
Patient Preference and Adherence 2022, 16:2533-2542
Published Date: 13 September 2022
Level of Depression and Anxiety on Quality of Life Among Patients Undergoing Hemodialysis
Alshelleh S, Alhawari H, Alhouri A, Abu-Hussein B, Oweis A
International Journal of General Medicine 2023, 16:1783-1795
Published Date: 10 May 2023
The Association Between Lifestyle and All-Cause Mortality in Patients Undergoing Maintenance Hemodialysis: A 3-year Prospective, Observational Study
Zhang L, Zhang S, Tang X
Journal of Multidisciplinary Healthcare 2025, 18:1721-1729
Published Date: 20 March 2025
Effectiveness of Community Nurse-Led Intervention in Managing Older Adults with Multimorbidity: A Systematic Review of Randomized Controlled Trials
Rahmat R, Haroen H, Juniarti N, Sari SP, Rinawan FR
Journal of Multidisciplinary Healthcare 2025, 18:6373-6389
Published Date: 3 October 2025