Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
Effectiveness of Community Nurse-Led Intervention in Managing Older Adults with Multimorbidity: A Systematic Review of Randomized Controlled Trials
Authors Rahmat R, Haroen H, Juniarti N ![]() , Sari SP
, Sari SP ![]() , Rinawan FR
, Rinawan FR
Received 23 June 2025
Accepted for publication 17 September 2025
Published 3 October 2025 Volume 2025:18 Pages 6373—6389
DOI https://doi.org/10.2147/JMDH.S548950
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr David C. Mohr
Rahmat Rahmat,1,2 Hartiah Haroen,3 Neti Juniarti,3 Sheizi Prista Sari,3 Fedri Ruluwedrata Rinawan4
1Doctoral Nursing Program, Faculty of Medicine, Universitas Padjadjaran, Sumedang, West Java, Indonesia; 2Nursing Department, Faculty of Health Sciences, Universitas Aisyiyah, Bandung, West Java, Indonesia; 3Community Nursing Department, Faculty of Nursing, Universitas Padjadjaran, Sumedang, West Java, Indonesia; 4Public Health Department, Faculty of Medicine, Universitas Padjadjaran, Sumedang, West Java, Indonesia
Correspondence: Rahmat Rahmat, Doctoral Nursing Program, Faculty of Medicine, Universitas Padjadjaran, Sumedang, West Java, Indonesia, Tel +62 857 9753 2991, Email [email protected]
Background: Multimorbidity is highly prevalent among older adults and poses significant challenges to healthcare systems globally, especially in low and middle-income countries. Nurse-led interventions are considered a promising strategy for addressing the complexity of care required for older adults with multiple chronic conditions.
Purpose: This systematic review aimed to synthesize empirical evidence on the effectiveness of nurse-led interventions in improving health outcomes among older adults with multimorbidity.
Methods: A systematic literature search was conducted across five major databases (PubMed, CINAHL, ScienceDirect, Scopus and Taylor & Francis) without time restriction. Randomized controlled trials (RCTs) focusing on nurse-led interventions in older adults with two or more chronic conditions were included. The methodological quality of studies was assessed using the Risk of Bias assessment. Data were extracted and synthesized qualitatively.
Results: A total of nine RCTs met the inclusion criteria. The interventions varied in design, setting, and duration. The interventions were categorized into three themes: (1) nursing care transitions, (2) strengthening self-management programs, and (3) integrated collaborative care. Community nurse-led interventions have consistently demonstrated effectiveness in improving physical function, chronic disease management capacity, medication adherence and knowledge, and perceptions of service quality and coordination. This intervention also contributed to a reduction in readmission rates, use of home care services, and length of stay in a secondary care facility.
Conclusion: Nurse-led interventions demonstrate strong potential in supporting older adults with multimorbidity by enhancing self-management capacity, optimizing care transitions, and improving intersectoral coordination. To maximise impact, future implementation in developing countries like Indonesia should consider cultural adaptability, primary care readiness, and system sustainability.
Keywords: nurse-led intervention, older adults, multicomorbidity, self-management, quality of life
Introduction
Multimorbidity in the elderly has become a global challenge, with a prevalence reaching more than 65% in the population aged 65 years and above. Globally, a review using data from 2000 to 2021 revealed that the prevalence of multimorbidity has exceeded 45%.1 A previous review analyzed data from 126 peer-reviewed studies involving nearly 15.4 million people (32.1% were men) from 54 countries. The overall global prevalence of multimorbidity was 37.2%, with the highest prevalence in South America (45.7%), followed by North America (43.1%), Europe (39.2%), and Asia (35.0%).1 In Indonesia, the prevalence of multimorbidity in the population aged 40 years and above is reported to be slightly more than 20% and shows an increase as the population ages.2–4 A previous study reported that 44.4% of the elderly population in Indonesia had multimorbidity.5 This condition increases the risk of repeated hospitalization and the burden of health costs and creates complexity in care coordination due to interactions between diseases and complicated treatment regimens.6
Multimorbidity refers to a condition in which an individual experiences two or more chronic diseases simultaneously, significantly impacting their overall health and necessitating comprehensive medical management.7 This condition consequently results in higher healthcare utilization and increased medical expenses.8 At the same time, the complexities and risks associated with polypharmacy and patient management also intensify.9 Unfortunately, resources to effectively address these challenges remain limited, particularly in low- and middle-income countries.
Multimorbidity can be prevented by targeting and managing factors associated with multimorbidity in health interventions. Previous studies in lower-income countries have identified factors influencing multimorbidity.3,5,10,11 Some factors that have been identified include age, socio-economic status, unhealthy diet, lack of physical activity, smoking, and genetic factors.5,10,11 Given the strong association between lifestyle and the development of multimorbidity, behaviour-based interventions and health education will be key in reducing the prevalence of this problem.
Community-based interventions with a more personalized and evidence-based approach are needed to address this issue. One approach that can be applied is a nurse-led intervention.12,13 Nurses play a vital role in health education, monitoring medical conditions, and providing the support needed to improve adherence to treatment and healthier lifestyle changes.14 Previous reviews have shown that nurse-led interventions, including case management or transitional care interventions, with advanced practice nurses, support for self-management of conditions, and emphasis on continuity of care are effective in improving the quality of life and self-management of patients with multimorbidities.6
Several studies have explored various forms of nursing interventions for managing elderly patients with multimorbid conditions. However, to date, no systematic review has comprehensively synthesized the findings from these studies to provide an integrated picture of the effectiveness of nursing interventions, especially in the context of community care. Previous reviews have been conducted, but they have differed in focus—both in terms of population characteristics (eg, including a general adult age group) and the heterogeneity of the study designs analysed, which limits the generalizability of the results obtained.6 Furthermore, most previous reviews examined literature with a limited publication span, with the most recent publication only up to 2020.6
The development of community-based nursing intervention models and approaches over the last five years has experienced significant acceleration, along with an increasing focus on integrated primary health care. Therefore, this review aims to synthesise the latest empirical evidence on nurse-led interventions in community settings, homes, or transitions from hospital to community care in older adults with multimorbidity. This effort is expected to yield a deeper and more focused understanding, supporting evidence-based nursing practice in the community and encouraging the development of policies responsive to the needs of older adults with complex health conditions.
Materials and Methods
Study Design
This systematic review was conducted following the methodological framework outlined in the Cochrane Handbook for Systematic Reviews of Interventions and adhered to the reporting standards set by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.15,16
Eligibility Criteria
This systematic review was structured based on the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines to explore the effectiveness of nurse-led interventions in managing older adults with multimorbidity in the community.15 The formulation of the research question and selection criteria for included studies were guided by the PICO framework (Population, Intervention, Comparison, Outcome), as outlined below:
P (Population): Older adult with multimorbidity
I (Intervention): Nurse-led interventions delivered in community, home-based care, home care or transitional care settings
C (Comparison): Standard care or Usual Care
O (Outcome): Health-related outcomes, including but not limited to quality of life, medication adherence, self-management capacity, hospital readmission rates, and patient-reported experiences of care
Studies were excluded if they lacked full-text access, were published in languages other than English, or were classified as secondary research (eg, reviews, editorials, commentaries). Only original research articles employing a randomized controlled trial (RCT) design, published in English with full-text availability, and explicitly focused on nurse-led interventions targeting older adults with multiple chronic conditions were included. Nurse-led intervention is defined as an intervention in which a nurse takes the lead role in planning, organizing, directing, and facilitating the intervention, and where the nurse’s contribution is substantial to its delivery and outcomes. While some included studies involved multidisciplinary teams, only those in which nurses had a primary and significant leadership role in the intervention were classified as nurse-led.
No restrictions were placed on the publication year to ensure a comprehensive and longitudinal perspective. This approach enabled the inclusion of a broad range of studies, allowing for the identification of emerging trends, early intervention models, and a comparative evaluation of traditional and contemporary nurse-led strategies in enhancing health outcomes for older adults with multimorbidity.
Search Strategy
A systematic literature search was conducted across four major electronic databases: PubMed, CINAHL, ScienceDirect, Scopus, and Taylor and Francis, with the search completed on April 17, 2025. The search strategy utilized a combination of controlled vocabulary and free-text terms to ensure comprehensive coverage of relevant studies. The following keyword string was employed: (nurse-led intervention) OR (nursing intervention) AND (multimorbidity) OR (comorbidities)) OR (multiple chronic condition)) OR (polymorbidity) AND (aged[MeSH Terms]) (older adult[MeSH Terms]) OR (elderly[MeSH Terms]) AND health-related outcome OR clinical outcome. In addition to the database search, a hand search was conducted by screening the reference lists of all included studies and relevant systematic reviews on similar topics. This was done to identify any additional eligible studies that may not have been captured through the electronic database search.
To enhance the sensitivity and specificity of the search, MeSH (Medical Subject Headings) terms were applied, and relevant synonyms were incorporated to further refine the search. Boolean operators “AND” and “OR” combined search terms, expanding or narrowing the results as needed. Since each database has its indexing system and advanced search functionalities, the search syntax was carefully adapted to align with each platform’s specific requirements and thesaurus terms. More details regarding search strategy can be seen in Supplementary Table 1.
Study Selection and Risk of Bias Assessment
All authors independently selected eligible studies. During the initial screening phase, duplicates were identified and removed using Mendeley reference management software. Following this, titles, abstracts, and full-text articles were reviewed to assess their relevance to the research objectives and to apply the predefined inclusion and exclusion criteria. In the final appraisal stage, each included article underwent a rigorous quality assessment using the RoB 2.0.17
The authors (R.R and F.R.R) independently evaluated the risk of bias for the randomised controlled trials (RCTs) included in this review using the Cochrane Risk of Bias (RoB) 2 tool to ensure methodological rigour and minimise assessment bias. RCT studies consist of five RoB domains, including (1) randomization process, (2) deviation from the intended intervention, (3) missing outcome data, (4) outcome measurement, and (5) selection of reported outcomes.17 RoB is defined as “high”, “low”, “some concern”, or “no information” for each domain. All authors then discussed and reviewed discrepancies in the assessment results to determine the decision.
Data Extraction and Analysis
The first and second authors (R.R and H.H) initially conducted data extraction and verified it with the remaining authors to ensure consistency and accuracy. For this systematic review, a structured data extraction table was employed to comprehensively capture and summarize all relevant findings aligned with the research focus. The table included detailed information on study characteristics, intervention types, and key outcomes.
The data analysis process began with systematically organising extracted data into tabular form, facilitating clear visualisation and comparison across studies. Each included article was carefully examined to extract pertinent variables, including study design, population characteristics, intervention components, duration, and measured outcomes. Following the extraction, all authors collaboratively reviewed and interpreted the findings, providing narrative descriptions and analytical insights based on the synthesised data. To ensure the reliability of the extracted information and reduce the risk of bias or data omission, the final step involved a thorough cross-checking of all included studies. This verification process aimed to enhance the overall rigour and transparency of the review methodology.
Results
Study Selection
A systematic search for articles was conducted across five major electronic databases: PubMed (n = 240), ScienceDirect (n = 751), Scopus (n = 406), CINAHL (n = 4156), and Taylor & Francis (n = 565). A total of 6.118 articles were identified from all of these databases. Of these, 1.270 duplicate articles were removed before screening, leaving 4848 articles to proceed to the title and abstract screening stage.
After initial screening, 4.817 articles were excluded because they did not meet the predetermined inclusion criteria. Thirty-one articles were continued to the full-text search stage, and all were successfully accessed (no reports were not retrieved). Furthermore, 31 articles were assessed for eligibility, but 25 articles were excluded for several reasons, including the participants used in the study were heterogeneous in age (n = 15), the study design was not appropriate (n = 7), and the intervention did not involve nurses (n = 3).
In addition to the electronic database search, the hand-searching method was conducted, which successfully identified three additional articles. All three articles were accessible and deemed suitable for inclusion in the review. Thus, nine articles were included in this review, comprising six articles retrieved from the electronic database search and three from the hand search (See Figure 1).
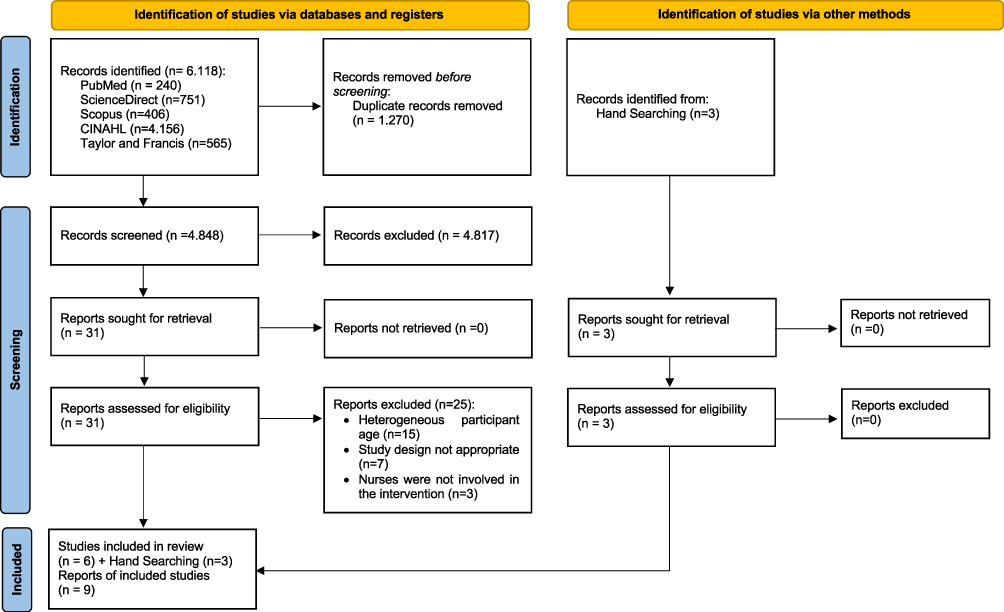 |
Figure 1 PRISMA Flow Diagram adapted from Page MJ, McKenzie JE, Bossuyt PM et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. Creative Commons.15 |
Characteristic of the Study
Based on the analysis of Table 1, all nine included studies employed a Randomised Controlled Trial (RCT) design. The majority of studies were conducted in Canada (n = 5),18–22 the United States of America (n = 2),23,24 one study in China,12 and one in Hong Kong.25 All studies examined the effectiveness of nurse-delivered interventions in older adults with multimorbidity, generally defined as individuals aged 65 years and older with two or more chronic disease conditions. Sample sizes in each study varied from 59 to 904 participants (see Table 1).
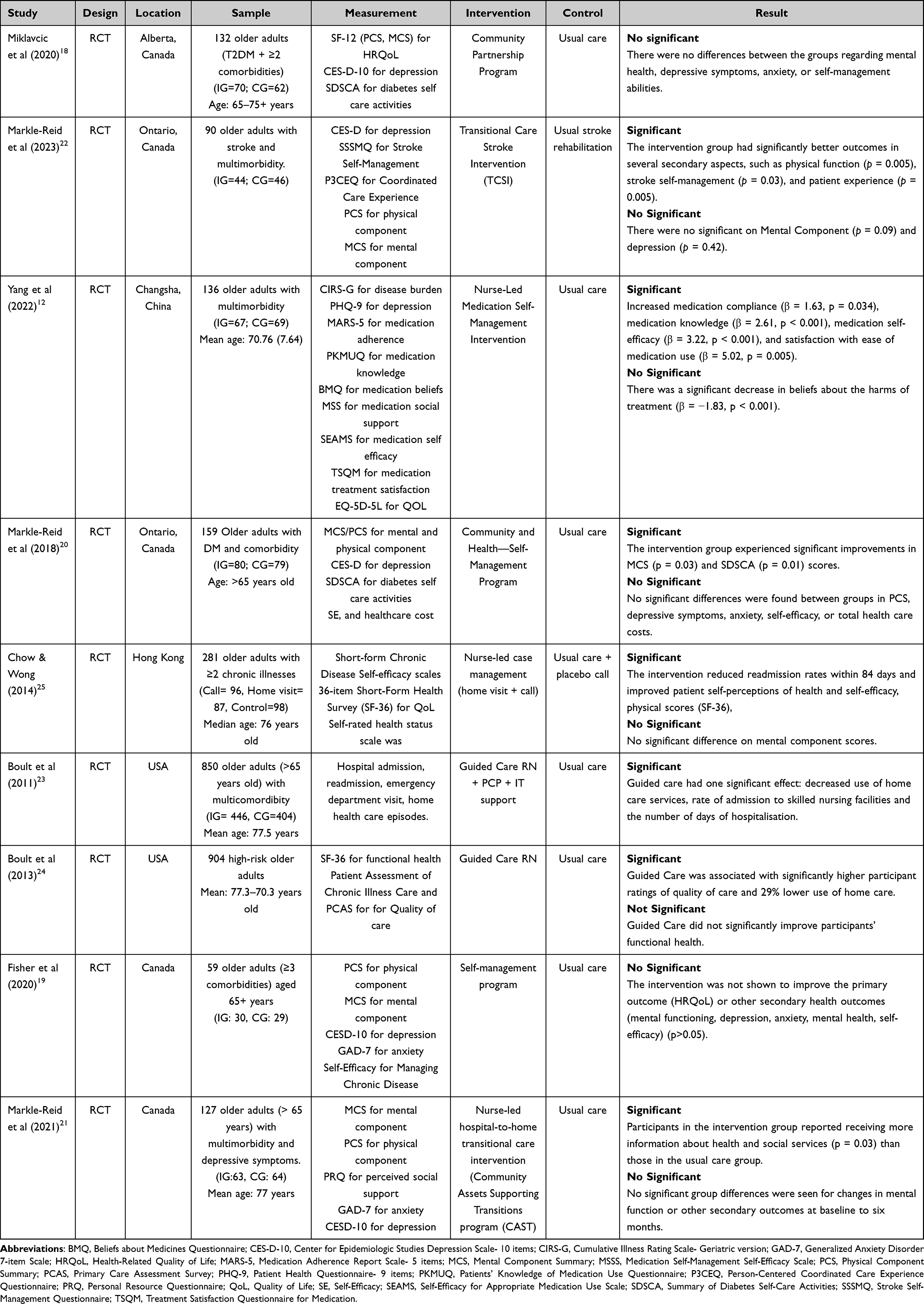 |
Table 1 Characteristics of Study |
Various measurement instruments were used in nine studies to assess the outcomes of nurse-led interventions for older adults with multimorbidity. Some of the most frequently used measurement instruments were the PCS (Physical Component Summary) and MCS (Mental Component Summary), which are part of quality-of-life questionnaires such as the SF-12 and SF-36, used to evaluate participants’ physical and mental health status. Additionally, the CES-D-10 (Center for Epidemiologic Studies Depression Scale - 10-item version) was used to assess the level of depressive symptoms. In contrast, the SDSCA (Summary of Diabetes Self-Care Activities) was explicitly used in the context of diabetic patients to assess self-care activities.
In stroke-related studies, the Stroke Self-Management Questionnaire (SSSMQ) was used to assess the self-management ability of post-stroke patients, and the Person-Centered Coordinated Care Experience Questionnaire (P3CEQ) was used to evaluate patient experiences of coordinated and patient-centred care. Several other studies also adopted medication-focused measurement tools, such as the Medication Adherence Report Scale (MARS-5) to measure medication adherence, the Patients’ Knowledge of Medication Use Questionnaire (PKMUQ) to assess patient knowledge about medication use, and the Beliefs about Medicines Questionnaire (BMQ) to measure patient beliefs about the medications they are undergoing.
Self-efficacy measurement is also an important component in intervention evaluation, as seen in the use of the Self-Efficacy for Appropriate Medication Use Scale (SEAMS) and the Medication Self-Management Self-Efficacy Scale (MSSS), both of which assess patients’ self-confidence in managing and using medications appropriately. Meanwhile, the Treatment Satisfaction Questionnaire for Medication (TSQM) measures patient satisfaction with the treatment received. Several studies also assess general quality of life through the QoL (Quality of Life) indicator and measure anxiety levels using the GAD-7 (Generalized Anxiety Disorder Scale-7).
Risk of Bias Assessment Results of Included Studies
Most of the studies fell into the category of some concern,18–22,25 and three were in the high-risk category.12,23,24 All studies showed weaknesses in domain D2 (deviation from intended intervention), where most did not explain in detail any deviations from the intervention that had been designed (see Figure 2). In general, the weaknesses found were mostly in the inappropriateness or lack of reporting on the intervention implementation process, data collection of outcomes, and the possibility of bias in reporting the reported results. Meanwhile, most studies showed a low-risk assessment in domains D4 (bias in the measurement of the outcome) and D5 (bias in the selection of the reported result), which indicated that the measurement of outcomes and data reporting were generally carried out appropriately and validly.
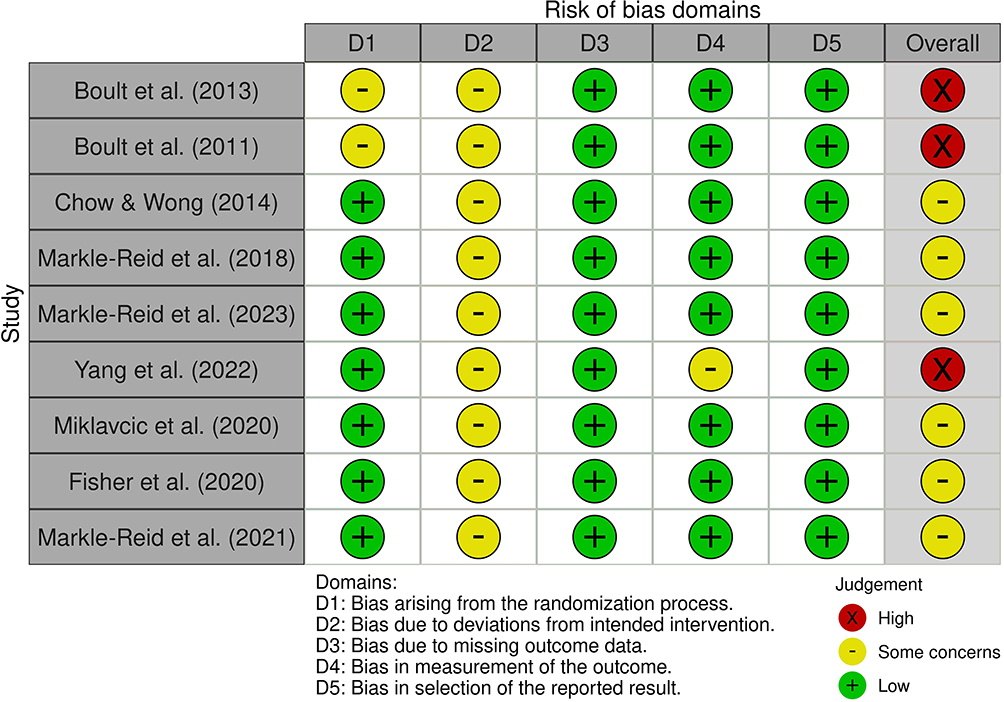 |
Figure 2 Risk of Bias Assessment of Included Studies.12,18–25 |
Characteristics of Nurse-Led Intervention
Based on the analysis of the nine studies included in this review, all interventions were conducted by nurses (nurse-led interventions) with variations in context and strategies tailored to the needs of elderly patients with multimorbidity (see Table 2). The role of the family, intervention setting, educational media and content, and duration and form of follow-up were key elements that differentiated the approaches between studies.12,18–25
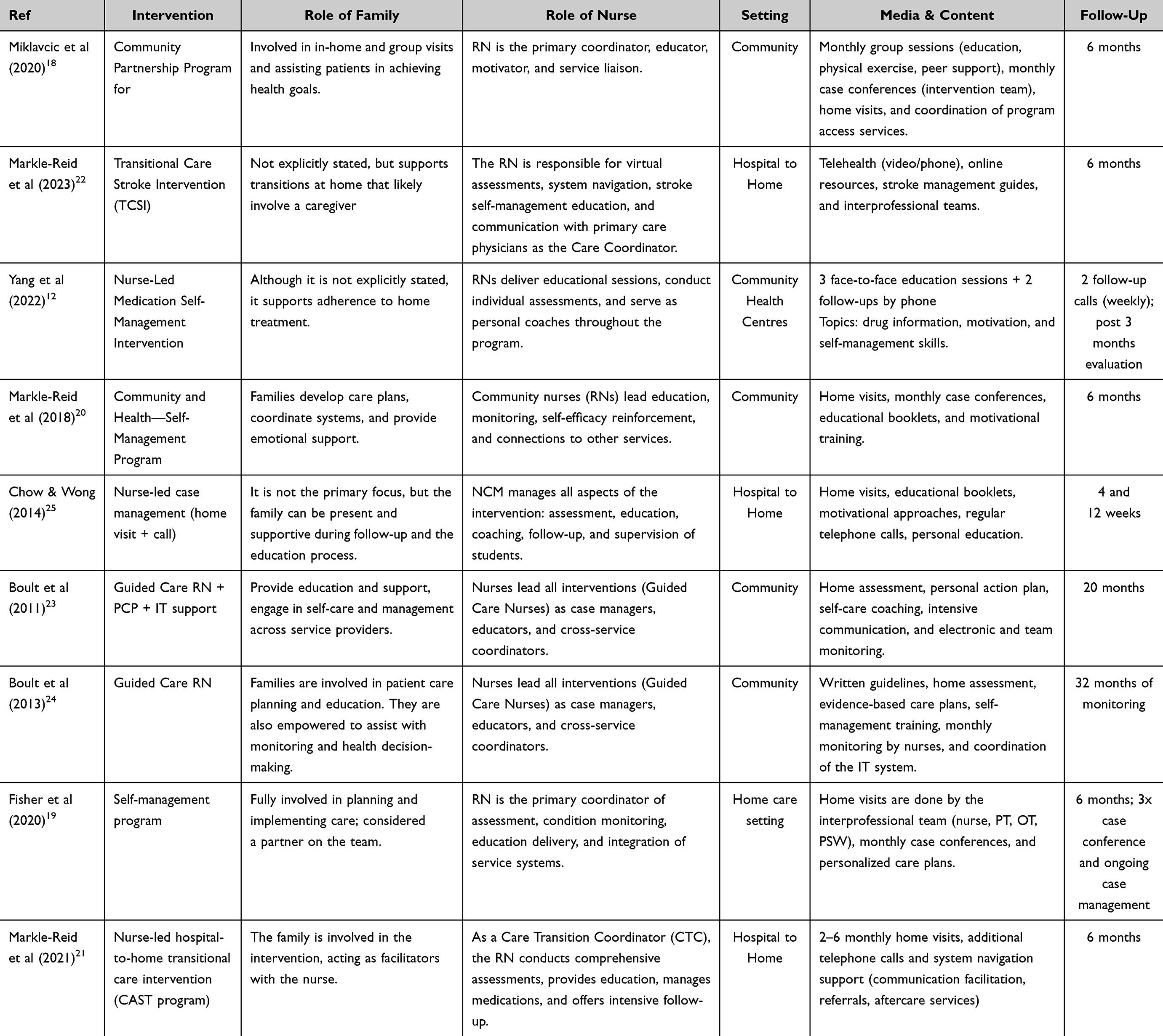 |
Table 2 Characteristics of Intervention |
In terms of family roles, the involvement of family members varies across studies. In some studies, such as Markle-Reid et al (2018) and Markle-Reid et al,20,21 the family plays an active role in the care planning process, emotional support, and facilitation of communication between the patient and the health care system. A study by Boult et al (2013) also showed that families were trained to support chronic disease management and were actively involved in care assessment and communication.24 In contrast, some studies did not explicitly involve families in the intervention, such as Yang et al (2022) and Miklavcic et al,12,18 where the primary focus is patient empowerment through education and peer support.
Regarding the intervention settings, the majority of the studies were conducted in the context of community or hospital-to-home transition. For example, Chow & Wong (2014) and Markle-Reid et al (2023) emphasized a transitional approach, focusing on home visits and using telehealth and telephone calls.22,25 On the other hand, community-based interventions are highlighted in studies such as Boult et al (2011) and Fisher et al (2020), which involve home assessments, self-management training, and regular multidisciplinary case conferences.19,23
In terms of media and content, the approaches used are very diverse, ranging from face-to-face educational sessions, as conducted in the study by Yang et al (2022), to the use of written guides, educational booklets, and information technology (IT) systems as in Boult et al12,24 Several studies also used telephone and video calls as a medium for follow-up and communication, reflecting the adoption of technology in supporting continuity of care.
The intervention duration ranged from 3 months to 32 months for follow-up. Studies with short durations, such as Chow & Wong,25 conducted follow-up at weeks 4 and 12, while long-term studies, such as Boult et al,24 included 32 months of monitoring with periodic evaluation by nurses using an evidence-based approach and an electronic monitoring system.
Category of Nurse-Led Intervention
This review groups the various intervention models into three main categories (see Table 3). This classification is based on the primary focus, delivery mechanism, and level of nurse involvement in the patient care process. These categories reflect the complexity of the nurse’s role and show how nurse-led interventions can be tailored to different contexts and patient needs. The three main categories of nurse-led interventions in this review are as follows:
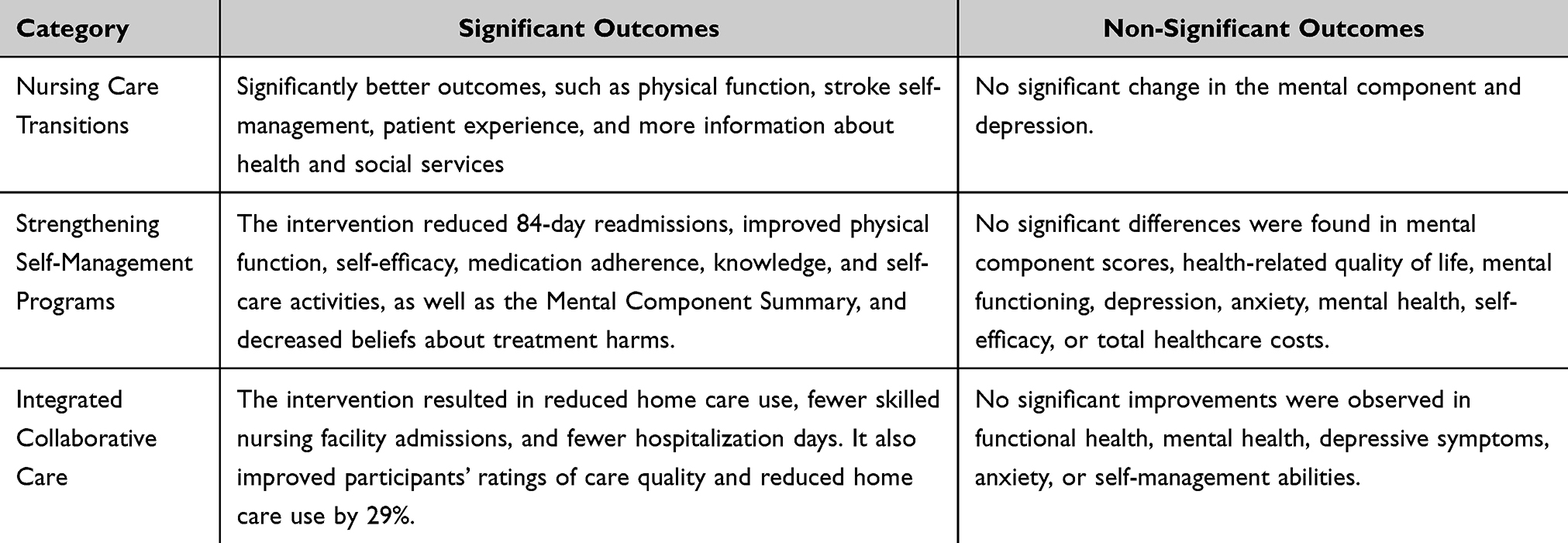 |
Table 3 The Outcomes Based on Intervention Category |
Category I: Nursing Care Transitions
Interventions in this category focus on supporting patients as they transition from hospital to home or community, aiming to reduce readmissions, improve continuity of care, and enhance post-hospitalization support.
The first care transition intervention was conducted in the study by Markle-Reid et al (2023), specifically focusing on stroke patients with several other comorbidities.22 This complex intervention is delivered over 6 months and designed to help patients adjust to life after discharge from the hospital. The intervention is delivered by an interprofessional team, including nurses, physical therapists, occupational therapists, social workers, and speech-language pathologists. Each patient receives support through a phone call after discharge, up to six virtual visits (phone or video), and ongoing support from a care coordinator who helps navigate the healthcare system.22 In addition, patients are given access to the My Stroke Recovery Journey online site to help them understand how to care for themselves and access the needed services. Throughout the process, the team regularly discusses care plans in monthly conferences to tailor each patient’s care plan to their specific needs. This approach emphasizes the importance of involving patients and families in decision-making and care planning.22
A similar intervention was also conducted by the same authors (Markle-Reid et al, 2023), namely Markle-Reid et al (2021), in an elderly population with multimorbidity and depressive symptoms.21 This transitional care program is called Community Assets Supporting Transitions (CAST) and lasts 6 months. In this intervention, nurses serve as Care Transition Coordinators, conducting home visits, making phone calls, and providing support to help individuals navigate the healthcare system.21 They assisted patients with symptom management, medication adjustments, problem-solving therapy, and connecting patients to community services. Participants in the intervention group received an average of three home visits and other support. Although the primary outcomes (mental and physical functioning) did not differ significantly from the control group, patients in the intervention group felt more informed about health and social services. Additionally, a trend toward increased perceived social support was observed, although it was not statistically significant.21
Category II: Strengthening Self-Management Program
In this category, interventions aim to enhance the patient’s and/or family’s ability to manage chronic conditions independently, encompassing medication management, lifestyle modifications, and informed health decision-making.
A nurse-led intervention (nursing case management) aimed at improving self-management through self-efficacy was conducted by Chow and Wong (2014).25 The program uses an empowerment and self-management approach, with home visits and/or phone call-based interventions conducted by expert nurses assisted by nursing students. The intervention lasts 4 weeks and begins with a pre-discharge assessment by nurses using the Omaha system.25 During the intervention, patients are educated, supported, and encouraged to set goals with their caregivers regarding their health care. The intervention is individually tailored to each patient’s needs.25 The final telephone call in the fourth week post-discharge was to remind patients about adherence behaviours and motivate and support them before the intervention ended.25
Yang et al (2022) also conducted a self-management program led by nurses.12 The intervention lasted 6 weeks, including three face-to-face educational sessions and two follow-up phone calls. The educational sessions included information on medications, motivational techniques to improve adherence, and medication management skills. The intervention was based on the Information-Motivation-Behavioural Skills (IMB) model. The study concluded that brief interventions, such as this, were beneficial in the short term; however, continued support and longer-term interventions were necessary for more lasting results.12
The same strengthening Self-Management program was also carried out by Fisher et al,19 where the Intervention is delivered by an interprofessional team (nurse, physical/occupational therapist, care coordinator, personal support worker) and includes home visits, monthly case conferences, and active case management. The primary focus of the intervention is to empower patients and their families, strengthen their ability to manage chronic conditions, and coordinate comprehensive care. This approach employs a holistic, patient-centred care model that emphasises team collaboration and patient and family involvement in developing the care plan.19
Markle-Reid et al (2018) implemented a 6-month community-based self-management program for older adults with type 2 diabetes and two or more other chronic diseases.20 An interprofessional team delivered the intervention of nurses, dietitians, community program coordinators (such as from the YMCA), and peer volunteers. Over six months, participants received up to three home visits from a nurse or dietitian to provide education and direct support tailored to their specific condition. In addition, participants were included in monthly group wellness sessions involving service providers from the diabetes education centre, community partners, and peer volunteers. These activities provided information and motivation and created a space for sharing experiences among patients.20 Then, to ensure continuity of care, the providers also hold monthly case conferences to discuss the participant’s progress, review individual needs, and adjust the care plan. The entire process is actively coordinated by the nurse who acts as the care leader and liaison between the participant, family, and the health care system.20
Category III: Integrated Collaborative Care
This category encompasses interventions that emphasize partnerships among nurses, healthcare teams, and communities, as well as the active role of nurses in integrating cross-sector services to ensure continuity of care and promote patient empowerment.
A cross-service collaborative intervention emphasising integrated collaborative care was conducted by Miklavcic et al (2020) through the Community Partnership Program.18 This intervention was targeted at older adults with type 2 diabetes and multimorbidity and lasted for 6 months. The program was led by an interprofessional team comprising a registered nurse (RN), a dietitian (RD), and a program coordinator from a community organisation.18 The intervention includes up to three home visits by an RN and/or RD, six monthly group sessions including health education, light exercise, shared meals, peer support, and monthly case conferences to discuss patient progress and needs. Throughout the program, the nurse serves as the care coordinator, working with the primary care team and community to connect patients to relevant health and social service resources.18
Boult et al (2011; 2013) also implemented a similar intervention through the Guided Care model, which places specially trained nurses (Guided Care Nurses) as working partners of 2 to 5 doctors in primary care practices.23,24 In this model, nurses provide eight core services: comprehensive home-based assessment, evidence-based care planning, regular symptom monitoring, interprofessional service coordination, care transitions, self-management training, caregiver support, and facilitation of access to community services. The intervention lasts over six months and utilizes information technology (IT) support to facilitate documentation and service coordination.23,24 The study found that patients in the program reported better quality of care and lower use of home care services than the control group. Additionally, there was a significant decrease in admissions to skilled nursing facilities and length of stay in the subgroup of patients with integrated insurance, such as Kaiser Permanente.23,24
Although the interventions were the same, the two studies had different focuses for evaluation.23,24 Boult et al (2011) evaluated the impact of Guided Care on health service utilization, such as frequency of hospitalizations, emergency department (ED) visits, skilled nursing care, and home care.23 The results showed a significant decrease in overall home healthcare use and a significant decrease in admissions and days at skilled nursing facilities among patients with integrated insurance (Kaiser Permanente). Meanwhile, Boult et al (2013) focused more on patient health function and perceptions of quality of care. This study showed that although there was no significant improvement in physical function, patients receiving Guided Care reported a significant increase in the quality of care received and lower home care use compared to the control group.24
Discussion
The findings of this review suggest that nurse-led interventions significantly contribute to improving certain aspects of health management in older adults with multimorbidity; however, the results are not always consistent across studies. In general, interventions that involve nurses in active roles as educators, care coordinators, and facilitators of patient empowerment demonstrate significant potential for enhancing self-efficacy, treatment adherence, self-management, and overall quality of life. The review divides interventions into three main categories: nursing care transitions, self-management strengthening, and integrated collaborative care.
Older adults with complex comorbid conditions are at high risk of experiencing adverse events and safety incidents soon after they are discharged from the hospital.26 Nursing care transitions is an important approach where interventions focus on the crucial transition phase from hospital to home.27,28 The role of nurses as care transition coordinators is to effectively navigate the service system, provide post-hospitalization education, and build communication between patients, families, and healthcare providers. The findings of this review support previous literature that emphasises the importance of transitional support in preventing rehospitalisation and facilitating patient adaptation to chronic health conditions.29 Previous studies showed that a nurse-led transitional approach can improve certain aspects such as physical function, patient experience of care, stroke self-management, and access to health care information.21,22 Nevertheless, alongside the positive findings, both studies reported no significant improvements in mental health components, including depression, anxiety, and perceived social support.21,22 These findings suggest that while nurse-led transitional care interventions may effectively address physical and informational needs during the post-discharge period, they may not be sufficient on their own to support the psychological and emotional well-being of older adults with complex health conditions.
Another aspect that is still challenging and needs to be considered in caring for elderly patients with multiple comorbidities is self-management. Several studies have reported that self-management of elderly patients with chronic diseases tends to be low to moderate.30–32 In Indonesia, the level of self-management of older adults with various chronic conditions, such as hypertension, is often less than optimal.33,34 The importance of self-management cannot be ignored, especially in the elderly with multiple comorbidities, because managing chronic diseases requires active patient involvement in monitoring symptoms, managing medications, maintaining a healthy lifestyle, and making daily decisions regarding their health conditions.34–36 Good self-management skills have been shown to correlate with improved quality of life, increased well-being, decreased frequency of hospitalizations, and lower mortality rates.35,37,38 Therefore, interventions to strengthen the self-management of elderly patients need to be carried out.
This review strengthens the self-management intervention category, focusing on improving patients’ ability to manage their health conditions independently. Education-based interventions show that empowerment through increased knowledge, medication management skills, and internal motivation can improve self-efficacy and adherence to therapy.12,19,25 Previous studies even added community and group support elements to the educational program, significantly strengthening patients’ sense of engagement and increasing consistency in self-care behaviours.20,25 The results of the study reported that there was an increase in self-efficacy, quality of life and self-management skills, as well as a decrease in depressive symptoms and clinical outcomes of patients.20,25 Nonetheless, evidence from several studies indicated that strengthening self-management interventions did not effectively reduce levels of depression, anxiety, or maladaptive beliefs regarding the harmfulness of treatment.12,19,20,25 These mixed findings suggest that while self-management interventions are promising in enhancing functional and behavioural outcomes, their impact on psychological dimensions remains limited. This discrepancy may be attributed to the fact that most interventions primarily target knowledge and behavioural change without incorporating tailored psychological support.
Nurses play a central role in facilitating self-management programs through various approaches, including home visits, telephone calls, educational sessions, and care coordination. Chow & Wong25 used an individual Omaha system-based empowerment approach that lasted 4 weeks. Meanwhile, Yang et al12 implemented the IMB model in a 6-week brief intervention emphasising medication management skills and behavioural motivation. Fisher et al (2020) and Markle-Reid et al (2018) demonstrated a more comprehensive intervention that integrated interprofessional teams, community-based approaches, and regular case conferences to support holistic, long-term management of chronic conditions. This approach increased patient self-efficacy and strengthened the role of family and community in supporting successful self-management.
The integrated collaborative care category emphasizes the importance of cross-sector integration and stakeholder synergy in supporting continuity of care for older adults with multiple comorbidities. Interventions in this category demonstrate the strategic role of nurses as clinical service providers, system navigators, and cross-service coordinators. Through the Community Partnership Program, Miklavcic et al (2020) showed how the synergy between health professionals (registered nurses and dietitians), community coordinators, and local service providers can create a holistic ecosystem of ongoing support.18 This intervention includes home visits and health education but also creates a social space to build peer support and increase patient engagement in managing their health. Furthermore, several previous studies developed a more complex Guided Care model, in which nurses with specialized training are integrated into primary care practices with 2–5 physicians, delivering eight core services that include multidimensional assessment, evidence-based care planning, self-management training, and care transition support.23,24 With the support of information technology to facilitate documentation and coordination, guide care interventions have significantly improved perceptions of quality of care and efficiency of health service use, especially in systems with integrated insurance.23,24
However, interventions within this category also demonstrated several statistically non-significant outcomes. For instance, the study by Miklavcic et al18 reported no significant differences in mental health, depression, anxiety, or self-management abilities between the intervention and control groups. Similarly, Boult et al24 found that the guided care intervention did not lead to meaningful improvements in patients’ functional health. These findings highlight the variability in effectiveness across studies and suggest that while strengthening self-management interventions may offer benefits in some domains, they may fall short in addressing more complex aspects of patient well-being. This underlines the importance of refining intervention designs to ensure they address both the physical and psychological needs of individuals with chronic conditions.
In addition to clinical effectiveness, several studies in this review also addressed aspects of cost-effectiveness, although this was not the primary focus of analysis. Markle-Reid et al (2018) reported that community-based nurse-led interventions did not significantly increase total healthcare costs, yet were able to maintain or improve quality of life without adding financial burden.20 The Guided Care model also demonstrated potential efficiency gains through reductions in home care utilization, admissions to skilled nursing facilities, and length of stay effects that translated into direct cost savings in systems with integrated insurance.23,24 Complementing these findings, data from Charline Mourgues showed that the cost of the intervention was €16,804.2, contributing to the performance of 747 additional preventive procedures at a cost of €30,184.8; the intervention was financially balanced when at least 37 patients followed the recommendations for each preventive procedure.39 These findings suggest that although quantitative evidence on cost-effectiveness remains limited and varies across contexts, nurse-led interventions have the potential to deliver good value.
Overall, the results of this review confirm that nurse-led interventions have great potential to improve care coordination, patient empowerment, and continuity of services for older adults with multimorbidity.12,13,40,41 Nurses act as clinical service providers and care navigators who bridge communication and collaboration between patients, families, and various health service sectors, thus ensuring responsive and holistic care integration. In developing countries such as Indonesia, implementing these intervention models must consider sociocultural determinants, human and technological resource limitations, and the readiness of the primary health care system. Contextual adaptation and cross-sector policy support are crucial to ensure that globally proven intervention approaches can be adopted sustainably and positively impact the quality of life of older adults with multiple chronic conditions.
Implication of This Study
This review underscores that community nurse-led interventions can deliver significant benefits for older adults with multimorbidity, including improvements in physical function, self-management skills, medication adherence, and patient experience of care, alongside potential reductions in healthcare utilization. From a public health perspective, such interventions can contribute to healthier ageing, decrease the burden of preventable hospitalizations, and optimize resource allocation critical priorities in ageing societies. For nursing practice, the findings support expanding the role of community and transitional care nurses as key coordinators and educators, integrating these models into primary care and community health frameworks. At the policy level, the evidence highlights the importance of investing in scalable, culturally adaptable, and cost-effective nurse-led programs to enhance equity in access and quality of care for older adults with complex health needs.
Strength and Limitation
This review demonstrates methodological rigour by adhering to the PRISMA guidelines and employing the Risk of Bias for quality appraisal. It provides a comprehensive synthesis of recent evidence, focusing solely on nurse-led interventions in older adults with multimorbidity —a population with increasingly complex care needs. The categorization of interventions into three conceptual themes enhances clarity and provides a structured framework for understanding the mechanisms of interventions. However, the findings are limited by heterogeneity in outcome measures, intervention formats, and durations across studies, which precluded meta-analysis. Furthermore, most included studies were conducted in high-income countries, which may limit their generalizability to low-resource settings. Some studies also exhibited methodological weaknesses, such as a lack of blinding and unclear allocation concealment, which could introduce potential bias.
Conclusion
This systematic review synthesized evidence from nine randomized controlled trials, categorizing nurse-led interventions into three primary models: (1) Nursing Care Transitions, (2) Strengthening Self-Management Programs, and (3) Integrated Collaborative Care. Across these studies, most interventions demonstrated statistically significant benefits in key health domains, including enhanced physical function, self-management capacity, patient experience, medication adherence, knowledge, and self-efficacy in medication use, as well as improvements in mental health scores and self-care activities among patients with diabetes. Additional outcomes included reductions in rehospitalization rates, decreased reliance on home care and skilled nursing facilities, and improved patient perceptions of care quality. However, several trials reported no significant effects on specific psychological outcomes such as depression, anxiety, mental functioning, and negative treatment-related beliefs, indicating that while nurse-led interventions are effective in improving physical and behavioural health outcomes, their influence on emotional and cognitive domains remains inconsistent and warrants further investigation.
Future research should explore culturally adapted models in resource-constrained settings and assess their long-term sustainability and cost-effectiveness. Policymakers and healthcare leaders are encouraged to invest in strengthening the roles of community and transitional care nurses, particularly in countries like Indonesia, where population ageing and chronic disease burdens are rapidly escalating. Nurse-led models offer a scalable and person-centred solution that aligns with goals for integrated primary healthcare and universal health coverage.
Acknowledgment
The author would like to thank Universitas Padjadjaran, Indonesian Education Scholarship, Center for Higher Education Funding and Assessment, and Indonesian Endowment Fund for Education.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Chowdhury SR, Chandra Das D, Sunna TC, Beyene J, Hossain A. Global and regional prevalence of multimorbidity in the adult population in community settings: a systematic review and meta-analysis. EClinicalMedicine. 2023;57:101860. doi:10.1016/j.eclinm.2023.101860
2. Husnayain A, Ekadinata N, Sulistiawan D, Chia-Yu Su E. Multimorbidity patterns of chronic diseases among Indonesians: insights from Indonesian national health insurance (INHI) sample data. Int J Environ Res Public Health. 2020;17(23). doi:10.3390/ijerph17238900
3. Hussain MA, Huxley RR, Al Mamun A. Multimorbidity prevalence and pattern in Indonesian adults: an exploratory study using national survey data. BMJ Open. 2015;5(12):e009810. doi:10.1136/bmjopen-2015-009810
4. Barnett K, Mercer SW, Norbury M, watt G, Wyke S, Guthrie B. Epidemiology of multimorbidity and implications for health care, research, and medical education: a cross-sectional study. Lancet. 2012;380(9836):37–43. doi:10.1016/S0140-6736(12)60240-2
5. Mahmudah NA, Tessma MK, Mahendradhata Y. Multimorbidity and its associated factors in Indonesia through universal health coverage scheme: a cross-sectional study based on national claims data. medRxiv. 2022;2009–2022.
6. McParland C, Johnston B, Cooper M. A mixed-methods systematic review of nurse-led interventions for people with multimorbidity. J Adv Nurs. 2022;78(12):3930–3951. doi:10.1111/jan.15427
7. World Health Organization. Technical Series on Safer Primary Care: Multimorbidity; 2016. Available from: https://www.who.int/publications/i/item/9789241511650.
8. Anindya K, Ng N, Atun R, et al. Effect of multimorbidity on utilisation and out-of-pocket expenditure in Indonesia: quantile regression analysis. BMC Health Serv Res. 2021;21(1):427. doi:10.1186/s12913-021-06446-9
9. Aggarwal P, Woolford SJ, Patel HP. Multi-morbidity and polypharmacy in older people: challenges and opportunities for clinical practice. Geriatr. 2020;5(4).
10. Mahwati Y. Determinants of multimorbidity among the elderly population in Indonesia. Kesmas. 2014;9(2):187–193.
11. Widyaningsih V, Premanawasti A, Sofia A, et al. Sociodemographic differences in multimorbidity: a closer look from indonesian family and life survey. In:
12. Yang C, Lee DTF, Wang X, Chair SY. Effects of a nurse-led medication self-management intervention on medication adherence and health outcomes in older people with multimorbidity: a randomised controlled trial. Int J Nurs Stud. 2022;134:104314. doi:10.1016/j.ijnurstu.2022.104314
13. Dougados M, Soubrier M, Perrodeau E, et al. Impact of a nurse-led programme on comorbidity management and impact of a patient self-assessment of disease activity on the management of rheumatoid arthritis: results of a prospective, multicentre, randomised, controlled trial (COMEDRA). Ann Rheum Dis. 2015;74(9):1725–1733. doi:10.1136/annrheumdis-2013-204733
14. Subiyanto P, Susilo CB. The role of community nurses in improving public health: strategies and implementation of educational programs. Oshada. 2024;1(August):29–44. doi:10.62872/sp67wd98
15. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372.
16. Riley RD, Moons KGM, Snell KIE, et al. A guide to systematic review and meta-analysis of prognostic factor studies. BMJ. 2019;364. doi:10.1136/bmj.k4597
17. Strene JAC, Page JS, Blencowe NS, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:1–8.
18. Miklavcic JJ, Fraser KD, Ploeg J, et al. Effectiveness of a community program for older adults with type 2 diabetes and multimorbidity: a pragmatic randomized controlled trial. BMC Geriatr. 2020;20(1):174. doi:10.1186/s12877-020-01557-0
19. Fisher K, Markle-Reid M, Ploeg J, et al. Self-management program versus usual care for community-dwelling older adults with multimorbidity: a pragmatic randomized controlled trial in Ontario, Canada. J Comorbidity. 2020;10:2235042X2096339. doi:10.1177/2235042X20963390
20. Markle-Reid M, Ploeg J, Fraser KD, et al. Community program improves quality of life and self-management in older adults with diabetes mellitus and comorbidity. J Am Geriatr Soc. 2018;66(2):263–273. doi:10.1111/jgs.15173
21. Markle-Reid M, McAiney C, Fisher K, et al. Effectiveness of a nurse-led hospital-to-home transitional care intervention for older adults with multimorbidity and depressive symptoms: a pragmatic randomized controlled trial. PLoS One. 2021;16(7 July):1–25. doi:10.1371/journal.pone.0254573
22. Markle-Reid M, Fisher K, Walker KM, et al. The stroke transitional care intervention for older adults with stroke and multimorbidity: a multisite pragmatic randomized controlled trial. BMC Geriatr. 2023;23(1):1–22. doi:10.1186/s12877-023-04403-1
23. Boult C, Reider L, Leff B, et al. The effect of guided care teams on the use of health services: results from a cluster-randomized controlled trial. Arch Intern Med. 2011;171(5):460–466. doi:10.1001/archinternmed.2010.540
24. Boult C, Leff B, Boyd CM, et al. A matched-pair cluster-randomized trial of guided care for high-risk older patients. J Gen Intern Med. 2013;28(5):612–621. doi:10.1007/s11606-012-2287-y
25. Chow SKY, Wong FKY. A randomized controlled trial of a nurse-led case management programme for hospital-discharged older adults with co-morbidities. J Adv Nurs. 2014;70(10):2257–2271. doi:10.1111/jan.12375
26. Coleman EA, Min SJ, Chomiak A, Kramer AM. Posthospital care transitions: patterns, complications, and risk identification. Health Serv Res. 2004;39(5):1449–1466. doi:10.1111/j.1475-6773.2004.00298.x
27. Couture V, Germain N, Côté É, et al. Transitions of care for older adults discharged home from the emergency department: an inductive thematic content analysis of patient comments. BMC Geriatr. 2024;24(1):1–17. doi:10.1186/s12877-023-04482-0
28. Murray LM, Laditka SB. Care transitions by older adults from nursing homes to hospitals: implications for long-term care practice, geriatrics education, and research. J Am Med Dir Assoc. 2010;11(4):231–238. doi:10.1016/j.jamda.2009.09.007
29. Fønss Rasmussen L, Grode LB, Lange J, Barat I, Gregersen M. Impact of transitional care interventions on hospital readmissions in older medical patients: a systematic review. BMJ Open. 2021;11(1):e040057. doi:10.1136/bmjopen-2020-040057
30. Cong Z, Huo M, Jiang X, Yu H. Factors associated with the level of self-management in elderly patients with chronic diseases: a pathway analysis. BMC Geriatr. 2024;24(1):1–10. doi:10.1186/s12877-024-04956-9
31. Han TC, Lin HS, Chen CM. Association between chronic disease self-management, health status, and quality of life in older Taiwanese adults with chronic illnesses. Healthc. 2022;10(4):609. doi:10.3390/healthcare10040609
32. Suarilah I, Lin CC. Factors influencing self-management among Indonesian patients with early-stage chronic kidney disease: a cross-sectional study. J Clin Nurs. 2022;31(5–6):703–715. doi:10.1111/jocn.15930
33. Prabasari NA. Self efficacy, self care management, and compliance in elderly with hypertension (phenomenological study). J Keperawatan Malang. 2021;6(1):1–10. doi:10.36916/jkm.v6i1.115
34. ALkautsar I, Kartinah K. The relationship between self management and blood pressure in elderly with hypertension in the Kartasura Health Center Area. Malahayati Nurs J. 2023;5(11):3686–3700. doi:10.33024/mnj.v5i11.9652
35. Sadeghi H, Mohammadi Shahbolaghi F, Hosseini M, Fallahi-Khoshknab M, Ghaedamini Harouni G. Factors associated with self-management in older adults with multiple chronic conditions: a qualitative study. Front Public Health. 2024;12:1412832.
36. Ersek M, Turner JA, McCurry SM, Gibbons L, Kraybill BM. Efficacy of a self-management group intervention for elderly persons with chronic pain. Clin J Pain. 2003;19(3):156–167. doi:10.1097/00002508-200305000-00003
37. Hu Q, Toonsiri C, Hengudomsub P. Factors affecting quality of life among older adults with hypertension in Wenzhou, China: a cross-sectional study. Belitung Nurs J. 2024;10(6):654–661. doi:10.33546/bnj.3565
38. Cramm JM, Hartgerink JM, de Vreede PL, et al. The relationship between older adults’ self-management abilities, well-being and depression. Eur J Ageing. 2012;9(4):353–360. doi:10.1007/s10433-012-0237-5
39. Mourgues C, Blanquet M, Gerbaud L, Soubrier M, Dougados M. Economic analysis of a nurse-led programme for comorbidities management of rheumatoid arthritis patients. Jt Bone Spine. 2018;85(5):573–576. doi:10.1016/j.jbspin.2017.09.009
40. Marsden E, Craswell A, Taylor A, et al. Nurse-led multidisciplinary initiatives to improve outcomes and reduce hospital admissions for older adults: the care coordination through emergency department, residential aged care and primary health collaboration project. Australas J Ageing. 2018;37(2):135–139. doi:10.1111/ajag.12526
41. Karam M, Chouinard MC, Poitras ME, et al. Nursing care coordination for patients with complex needs in primary healthcare: a scoping review. Int J Integr Care. 2021;21(1):1–21. doi:10.5334/ijic.5518
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
An Easy-to-Implement Clinical-Trial Frailty Index Based on Accumulation of Deficits: Validation in Zoster Vaccine Clinical Trials

Andrew MK, Matthews S, Kim JH, Riley ME, Curran D
Clinical Interventions in Aging 2022, 17:1261-1274
Published Date: 19 August 2022
Assessing the Impact of Community Health Coaching on Self-Management of Chronic Illness Among Older Adults: A Cross-Sectional Approach
Almutairi M, Almutairi AA, Alodhialah AM
Clinical Interventions in Aging 2025, 20:231-244
Published Date: 27 February 2025
A Systematic Review of Continuity of Care Strategies for Enhancing Diabetes Self-Management in Older Adults in Asian Countries
Sari CWM, Haroen H, Juniarti N, Amalia L, Pardosi JF
Journal of Multidisciplinary Healthcare 2025, 18:5441-5459
Published Date: 2 September 2025
Influence of 5A-Based Self-Regulated Nursing Intervention on Self-Care Capability and Well-Being Among PCI Recipients with Coronary Heart Disease
Wang H, Wang W, Zhang L
Journal of Multidisciplinary Healthcare 2026, 19:569413
Published Date: 6 January 2026
Oral Frailty and Its Impact on Elderly Quality of Life: A Scoping Review
Wulandari AB, Hidayat W, Zakiawati D
Clinical Interventions in Aging 2026, 21:549826
Published Date: 2 February 2026