")
Back to Journals » Patient Preference and Adherence » Volume 16
Quality of Life and Adherence to Healthcare Services During the COVID-19 Pandemic: A Cross-Sectional Analysis
Authors Hassan SUN , Zahra A , Parveen N , Khatoon F , Bangi NA, Hosseinzadeh H
Received 12 June 2022
Accepted for publication 26 August 2022
Published 13 September 2022 Volume 2022:16 Pages 2533—2542
DOI https://doi.org/10.2147/PPA.S378245
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Johnny Chen
Sehar-un-Nisa Hassan,1 Aqeela Zahra,2 Nuzhat Parveen,3 Fahmida Khatoon,2 Naseer Ahmad Bangi,4 Hassan Hosseinzadeh5
1Department of Public Health, College of Public Health and Health Informatics, University of Ha’il, Ha’il, 81451, Saudi Arabia; 2Department of Family and Community Medicine, College of Medicine, University of Ha’il, Ha’il, 81451, Saudi Arabia; 3Department of Obstetrics and Gynecology, College of Medicine, University of Ha’il, Ha’il, 81451, Saudi Arabia; 4Department of Respiratory Therapy, College of Medical Rehabilitation Sciences, Taibah University, Madinah, 42353, Saudi Arabia; 5School of Haelth and Society, University of Wollongong, Wollongong, NSW, Australia
Correspondence: Aqeela Zahra, Department of Family and Community Medicine, College of Medicine, University of Ha’il, Ha’il, 81451, Saudi Arabia, Tel +966583675414, Email [email protected]
Purpose: To determine the relationship of various domains of quality of life (QoL) with healthcare adherence during the COVID-19 pandemic in Saudi Arabia.
Methods: The study sample comprised 795 participants among which 203 had a current diagnosis of any major NCDs, including cardiovascular diseases, diabetes mellitus, asthma, chronic pulmonary diseases, and chronic psychiatric illnesses and a control group of 592 participants who had no NCD. Participants completed an online survey questionnaire which obtained data on socio-demographic variables, types of NCDs, and healthcare adherence during the year 2020, the period during which Saudi Arabia underwent the first two waves of the COVID-19 pandemic. World Health Organization Quality of Life (WHOQOL-BREF) assessed the QoL in four domains physical, psychological, social and environmental and used standard scores in the analysis. GraphPad Prism 5 and SPSS 25V were employed for the statistical analysis. Bar graphs and frequency distribution tables present descriptive data. Bivariate and multivariate logistic regression analyses were computed to determine the significance of the relationship between QoL and healthcare adherence.
Results: Almost equal proportions of participants with NCDs (n=109/203; 54%) and without NCDs (n=327/592; 55%) demonstrated nonadherence to their regular healthcare during the COVID-19 pandemic (χ 2=0.14; p=0.71). Patients with NCDs experienced lower quality of life in the psychological, social and environmental domains of QoL (p< 0.05). Results from the multivariate regression analysis showed that female gender (AOR=1.52; p< 0.05) psychological QoL (AOR=1.99; p< 0.05), social QoL (AOR=1.98; p< 0.05) and environmental QoL (AOR=1.95; p< 0.05) significantly relate with adherence to healthcare.
Conclusion: Psychological, social and environmental may influence healthcare adherence among patients with NCDs during pandemics and should be focused on while devising future healthcare policy and interventions.
Keywords: quality of life, COVID-19 pandemic, healthcare, adherence, non-communicable diseases, behaviors
Introduction
Quality of Life (QoL) is now considered a distinct but crucial factor that is associated with physical health and determines the overall functioning in various aspects of life.1 The term QoL in relation to the health of individuals was conceptualized by World Health Organization (WHO) and it encompasses a person’s state of well-being from the physical health domain to various other domains of life such as psychological, social, environmental, and spiritual well-being.2 This definition of the QoL construct provides a comprehensive picture of individual well-being because health is less likely to be experienced in isolation from other domains of wellness.3 In a traditional biomedical model, the QoL was primarily interpreted as optimal physical functioning, whereas subsequent models incorporated mental health, social well-being, satisfaction with economic conditions and fulfilment of life goals as markers of QoL.4 Patients suffering from Non-Communicable Diseases (NCDs) such as cardiovascular diseases, diabetes mellitus, asthma, chronic pulmonary diseases, and chronic psychiatric illnesses are vulnerable to poor quality of life.5,6 NCDs impact the daily life functioning of individuals reducing their quality of life and according to some estimates it accounts for 74% of global mortality.7 The management of illness usually requires adherence to prescribed treatment as well as lifestyle changes. Patients are often required to undergo extensive medical examinations and compliance to treatment regimen to maintain health and functioning.
The COVID-19 pandemic presented unique challenges to every segment of the population and worse for the people suffering from NCDs. The extensive and prolonged quarantine measures compromised the quality of life of people in several ways. Many patients with chronic illnesses evaded healthcare services and did not follow-up with medication reconciliation either out of fear to get the infection, or delayed appointments due to the extra burden on healthcare services.8 The literature demonstrated that stress experienced by people during COVID-19 has considerably obstructed adherence with medical treatment, which has consequences among patients with comorbidity and poor health conditions.9
Literature supports most patients with NCDs need regular medical care and attention. For instance, a study reported that patients with coronary heart diseases and ischemic diseases of the lower extremities undergo long-term therapeutic interventions, uninterrupted medical attention and support from healthcare services.10 QoL assessment is conducted as a part of their treatment progress to monitor the impacts of their disease on various domains of QoL and guide intervention that focuses on enhancing their functioning in various areas of life. However, the lockdown measures prevented patients with chronic health problems from carrying out routine checkup and healthcare behaviors such as walk, exercise and physiotherapy.11 Additionally, low social support and economic difficulties also appeared as significant risk factors during the pandemic to worsen their health problems.12 A recent study from Korea demonstrated that various social, behavioral, psychological, and physical health-related factors were related with QoL in patients with chronic illnesses.13 Moreover, it stated that health-promoting behavior significantly predict quality of life in patients, and psychological factors such as enhanced self-esteem, social factors such as social support and behavioral factors that is adherence to planned action of health behaviors significantly account for health and well-being in these individuals.13
Current studies from Saudi Arabia and other parts of the world have demonstrated COVID-19 pandemic has both short-term and long-term impacts on the QoL of people.14,15 People with NCDs are particularly prone to a secondary incidence of depression, and the non-availability of appropriate healthcare services is likely to have negative consequences on the patient health outcomes.16 Untreated anxiety and depression significantly impact disease prognosis and increase the risk of disease-related complications in patients with NCDs.17 Findings from one study reported that a number of patients with chronic diseases experienced both physical and psychological problems during the COVID-19 outbreak,18 and this was anticipated to markedly increase thereafter and thus may worsen psychiatric symptoms such as agitation, mania, psychosis, or severe depression.19 A study based upon conviction of mental health professionals reported that the possibility of developing various anxiety disorders due to the COVID-19 pandemic in different populations ranged between 42% to 60% and those who are in 50 to 70 years of age have maximum probability of experiencing anxiety as an impact of COVID-19 pandemic.20
Non-adherence to healthcare among healthy population and patients with NCDs was primarily due to the fear of catching infection and a generalized anxiety linked with immense coverage of pandemic and associated morbidity in media.21 Most patients with NCDs were reluctant to seek healthcare which led to additional challenges of delayed care such as prolonged consumption of health resources due to long stays in intensive care.22 Seeking appropriate healthcare is crucial for people who are suffering from NCDs during health crisis such as pandemics, and ignorance in this aspect is likely to worsen their health conditions with an additional burden on healthcare providers and caregivers due to these illnesses.
The current study therefore aims at assessing the relationship of various domains of quality of life (QoL) with healthcare adherence amoung patients with NCDS, during the COVID-19 pandemic in Saudi Arabia.
Gaps in Literature and Study Context
In most previous research studies, the quality of life has been investigated either as impact on illness or to determine the positive impacts of treatment outcomes on life of patients with chronic illnesses.10,23 However, there is no study which investigated the predictive role of various domains of QoL in adherence to healthcare during health crisis periods such as epidemics or pandemics. A study from China demonstrated positive association of perceived social support on adherence to regimen in patients with hypertension.24 Nonetheless, to date there is lack of literature about association of physical, psychological, social and environment domains of QoL with healthcare behavior during prolonged global crisis events.
The present study intended to assess how physical, psychological, social and environmental quality of life domains relate to uptake of healthcare services in healthy population and people with NCDs. Keeping in view the panic situation during COVID-19 pandemic and other environmental circumstances such as social distancing and quarantine measures which were strictly applied in Saudi Arabia. The rationale for this study aligns with the prevention and promotion perspectives in the field of public health. The assessment of QoL of patients will help to identify the domains which negatively influenced the utilization of healthcare services, and that will guide the planning of provision of healthcare services during health crisis situations. This information will be useful to ascertain the vulnerability of people for non-compliance with healthcare due to the poor quality of life and the planning of public health interventions.
Materials and Methods
Study Design, Sample, and Procedures
A cross-sectional survey research design was employed because it was the most viable option to collect the data on study variables during the COVID-19 pandemic. The target population for the study was a sample of patients with NCDs recruited from the community and a control group without NCDs. According to prior epidemiological studies, the prevalence rates for NCDs in KSA is around 30%,25 therefore the estimated sample size for this group was about 196 patients and for control group 315 participants by choosing 95% Confidence Interval (CI)24 with margin of error 5%. The sample size used in this analysis after data cleaning were of 203 patients who had a current diagnosis of any NCD, and a sample of 592 participants without NCDs.
The data for this study were collected in November and December 2020 and the study area was restricted to the Ha’il region in the Kingdom of Saudi Arabia. Out of thirteen provinces in Saudi Arabia, Ha’il is the 8th largest province which is sprawled over 103,887 km square and by population it is the 9th largest region.
The data was collected through online survey questionnaire which was distributed by professional colleagues on various online platforms. The first screen on the questionnaire introduced study goals and screening questions to assess whether a prospective participant met the inclusion/exclusion criteria. The inclusion criterion which were (1) adult with age 18 years and above (2) residing in Saudi Arabia and (3) able to read and complete an online self-report online survey. The exclusion criterion was (1) below the age of 18 years (2) not living in KSA during the pandemic (3) any limitation which did not allow to complete the self-report online survey questionnaire. Those who meet the study inclusion criteria were asked for informed consent and requested to fill in online survey questionnaire which was concurrently displayed on the screens in both English and Arabic language.
Study Variables and Questionnaire
The first part of the study questionnaire included data on the demographic background of participants that included gender, age, education, and marital status. The next part required participant to indicate whether they are suffering from any of the listed NCDs. To assess adherence to healthcare, participants were asked a close-ended question with Yes/No categories about utilization of healthcare/medical services for regular medical follow-up during the year 2020, when Saudi Arabia experienced the first and second wave of the COVID-19 pandemic.
The quality of life was assessed by a reliable and valid QoL measure known as World Health Organization quality of life (WHOQOL-BREF).26,27 This tool is a standard measure to assess various domains of QoL namely physical, social, psychological, and environmental. The measure is comprised of 26 items which are distributed over five domains excluding two questions which assess general health status and overall satisfaction with life. The items on the scale are rated on a 5-point Likert Scale and higher scores on the scale indicate a better QoL in the specific domain whereas a low score indicates poor QoL experienced by respondents in a particular domain of life. Previous psychometric validations of the tool have shown acceptable levels of its reliability and validity.28 The Cronbach Alpha values based on data collected in this study sample on all four domains lie in the range between 0.78–0.84.
Ethical Approval
The ethical review and approval for the study was conducted by the Institutional Review Board of the University of Ha’il, approval letter H-2021–29, and the study was completed by following the rules and guidelines of consent, beneficence, non-maleficence, and right to withdraw as mentioned in the Declaration of Helsinki.
Statistical Analysis
All statistical analyses were done using GraphPad Prism v.5 and presented in bar graphs and IBM SPSS25 and results are presented in tables. Discrete/categorical variables were reported as percentages and numerical counts and continuous variables were reported using descriptive statistics as mean, median, standard deviation, and range. Statistical tests were applied to determine the bivariate association of demographic variables with outcome variable and a multiple logistic regression analyses were applied to determine association of QoL with healthcare adherence after adjusting for the effect of gender, age and education.
Results
Respondents who endorsed suffering from any of the listed NCDs were of 203 patients with NCDs and included 592 respondents without NCDs. Table 1 compares frequency distribution of participants who were suffering from NCDs with control group across demographic variables. For gender, age, education and on adherence to healthcare the differences were non-significant across gender, age and education categories. Almost equal proportions of participants with NCDs (109/203; 54%) and without NCDs (327/592; 55%) demonstrated non-adherence to their regular healthcare during the COVID-19 pandemic (χ2=0.14; p=0.71). Results from the multivariate regression analysis showed that female participants were more likely to show non-adherence with medical care during the pandemic (AOR=1.52; p<0.05) (Table 2).
 |
Table 1 Frequency, Percentage Values, and Chi-Square Analysis on the Demographic Characteristics of Participants (n=795) |
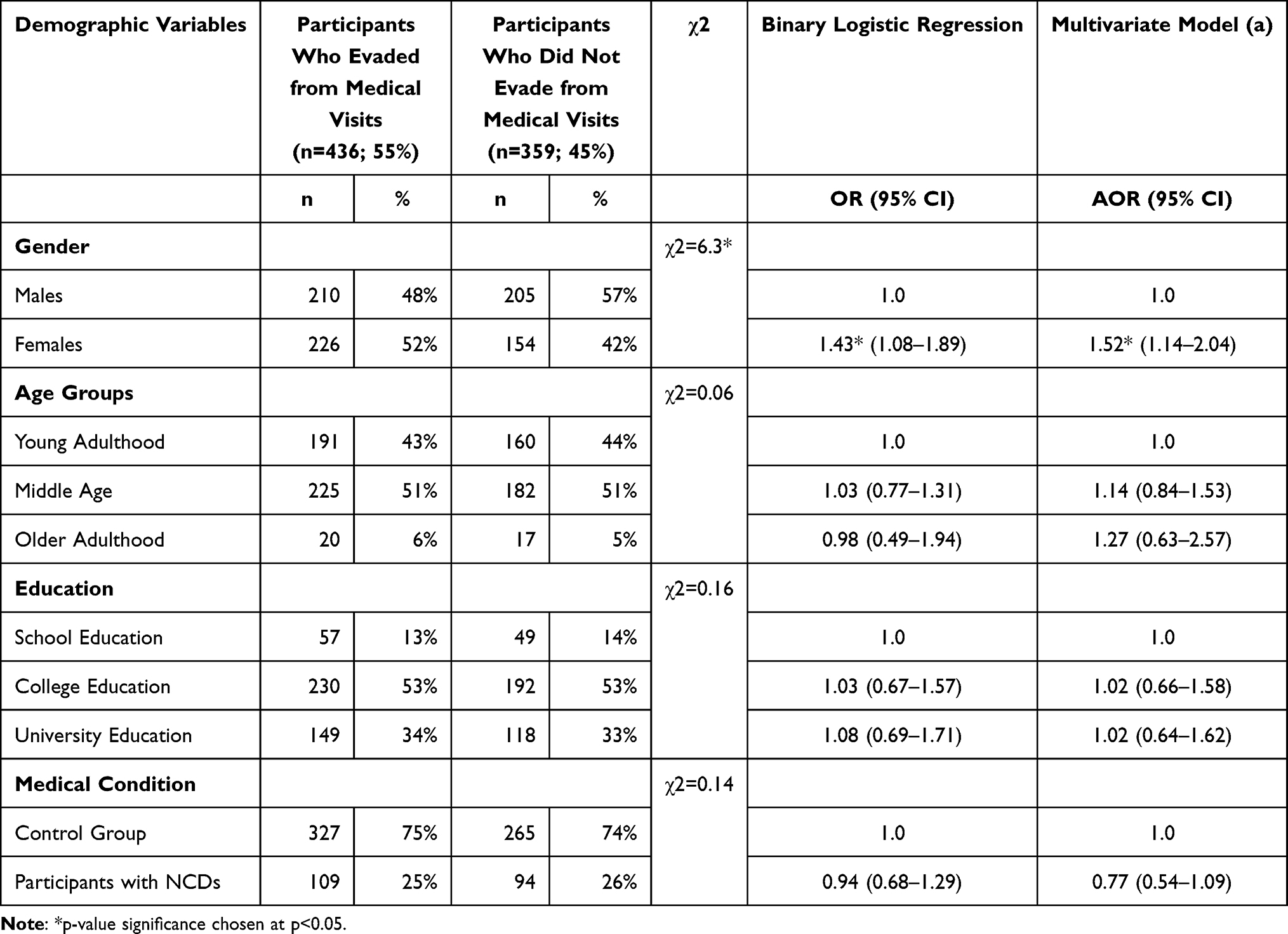 |
Table 2 Chi-Square Test χ2 and Logistic Regression for Assessing Relationship Between Independent Variables with Adherence to Healthcare (n=795) |
The inspection of Figure 1 shows that patients with NCDs who adhere with medical care during the pandemic had lowest mean score on Psychological QoL (M=44.4; SD=17.0) followed by Environmental QoL (M=40.8; SD=18.0). Patients with NCDs also experienced lower Social QoL (M=42.9; SD=14.6) as compared to those without NCDS (M=57.5; SD= 20.2).
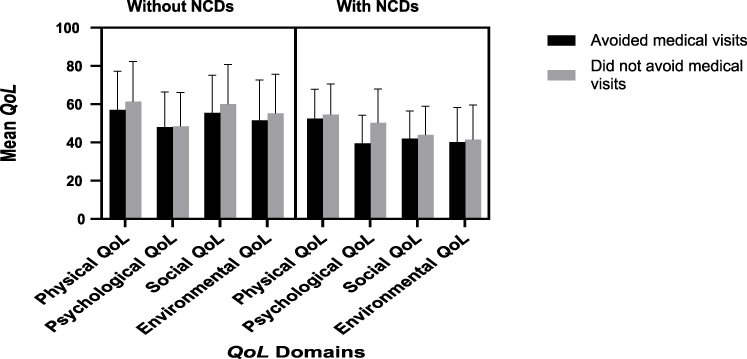 |
Figure 1 Mean scores on four domains of QoL of participants with NCDs and control group and those who adhere or not adhere with medical care (n=795). |
The inspection of results from t-test shows that mean differences on all domains of QoL between participants with NCDs and without NCDs were statistically significant at p<0.05 as well as there were statistically significant difference on domains of QoL who adhere and did not adhere with medical care were statistically significant at p<0.05 between patients who adhere and did not adhere with medical care were statistically significant at p<0.05 (Table 3). Poor psychological QoL (AOR=1.99; p<0.05), social QoL (AOR=1.98; p<0.05) and environmental QoL (AOR=1.95; p<0.05) significantly predict non-adherence with healthcare (Table 3).
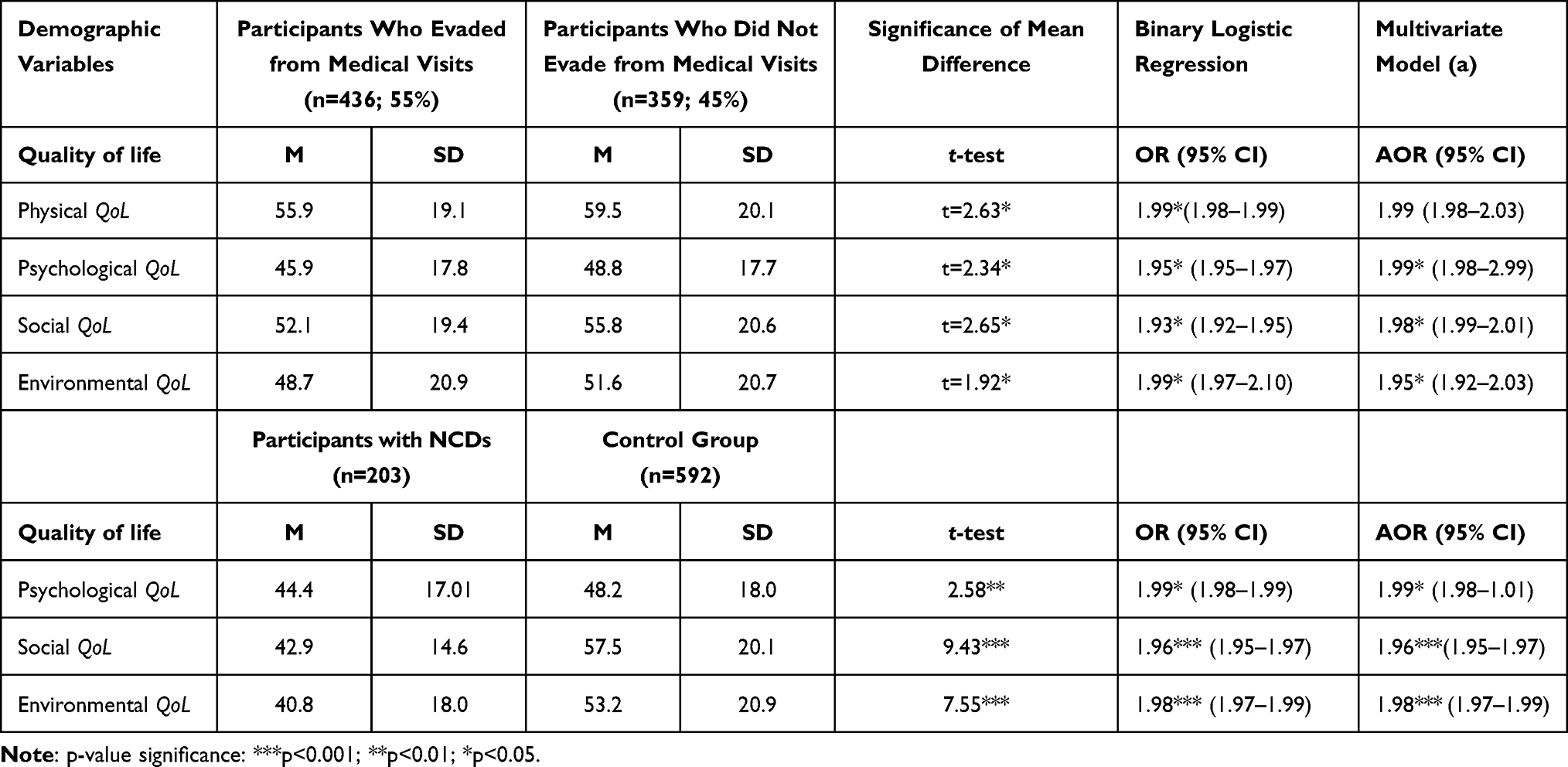 |
Table 3 Significance of Mean Differences and Logistic Regression for Assessing Relationship Between QoL and Adherence to Healthcare (n=795) |
Discussion
Findings validate lack of adherence with regular medical care in patients with NCDs during the COVID-19 pandemic in Saudi Arabia. This finding aligns with other global studies which showed that patients with chronic illnesses skipped medical care or less likely to utilize healthcare services as high as up to 39%29 and prior evidence also approve that follow-up visits to physicians reduced by around 10% during the pandemic and this is likely to impact physical and mental health of patients with other illnesses.30 Keeping in view that over fifty percent of patients with chronic health conditions in this study avoided obligatory medical care during the pandemic, this is a concerning issues and calls for attention of health policy workers.
Our study demonstrated the predictive role of various domains of QoL during the pandemic with healthcare behaviors of patients and compared it with control group and thus distinguishes from previous research studies which inspected the impact of ill health on the quality of life during the pandemic.31 Findings demonstrate that patients with NCDs experienced lower psychological, social and environmental QoL as compared to those without NCDs and they were also less likely to adhere with their medical care. In this way, we were able to demonstrate how despite of physical health problems, psychological, social and environmental domains of QoL during the pandemic period influence people’s healthcare behaviors. They were reluctant to seek healthcare services despite when they needed it out of fear and distress that was pervasive during the pandemic.32 The items on psychological quality of life assessed levels of satisfaction, ability to concentrate and experience of psychological symptoms such as low mood, anxiety, and depression. Patients who experienced such symptoms likely to show non-adherence with healthcare during the pandemic and previous literature support that symptoms of anxiety and depression impact healthcare behaviors of patients.33 These findings validate the need of psychosocial support for patients with NCDs that may help them to follow-up with their healthcare needs.
Our results demonstrated that female patients were more likely to forgo medical follow-up for their disease conditions during the COVID-19 pandemic as compared to male patients. This somewhat corroborates with the findings from a study which investigated healthcare behaviors among rural women during the pandemic and reported that women living with their children reduced their visits to healthcare providers by 1.9 times.34 Our findings thus validate that pandemic may increase the gender-based health disparities. The possible explanations for such differences are either socioeconomic conditions because women are less likely to hold employment and health insurance which were found to be significant factors in evading healthcare during the pandemic35 or it could be due to psychological factors such as increased vulnerability to experience stress and anxiety symptoms.36 A study of Iranian women with diagnosis of breast cancer reported increased levels of anxiety and distress experienced by women during the outbreak.37
Although our study did not demonstrate significant differences in healthcare avoidance among patients in different age groups and educational background, there is some evidence from a previous study which obtained data from Singapore and reported that middle-aged and older age patients with NCDs reduced use of medical care by 23% to 49% during the COVID-19 pandemic.30 A cross-sectional study from South Korea also identified that both people from general population and clinical populations prevented seeking healthcare during the COVID-19 pandemic and socio-demographic factors such as gender, age and financial conditions were significantly associated with evading healthcare which may have intensify health impacts of such crisis.38
One factor that might have impact on people non-adherence to medical care could be knowledge as there were lots of misinformation and insufficient knowledge about the COVID-19 virus in year 2020. Our study finding also confirmed the predictive role of environmental quality of life in non-adherence to healthcare during the COVID-19 pandemic in patients with chronic illness. The environmental quality of life relates with access to information, access to healthcare services and feeling of safety in outer physical environment. All these aspects of environmental quality of life were compromised during the COVID-19 pandemic and influenced the healthcare behaviors of patients with NCDs. A study of older American adults demonstrated that around one-fifth of patients avoided visiting medical centers and healthcare avoidance was significantly associated with risk perceptions.39 Previous research has also demonstrated that poor health education in the communities is a major factor in non-compliance.40 In Saudi Arabia, to minimize the direct contact with healthcare centers and to improve the access to healthcare, Saudi government took several initiatives such as expansion of telemedicine services to the community during the pandemic. However, access to such services was restricted in rural areas and mainly people living in urban areas benefitted from this alternative source of healthcare. A study from Portugal in the late phase of the COVID-19 pandemic reported that unclear information and perception of people about less effective protective measures in healthcare institutions were found to be related with escaping needed healthcare by patients and other people during the pandemic.41 The recent literature underscores the need to understand various factors that may influence quality of healthcare provision through telemedicine. For instance, patients with physical injuries and surgical treatment may require direct physical examination. Moreover, there are several ambiguities related to legal and ethical issues in field of telehealth services that may influence quality of care and health outcomes should be thoroughly reviewed and addressed while policy formulation to expand telemedicine.42 Another qualitative study assessed patients’ attitudes towards health technology who underwent joint replacement surgery and monitored through sensors installed in home environment. Patients demonstrated acceptance towards this monitoring system and needed support from social network during this period to operate and maintain the smart home system.43 This also aligns with other study findings which revealed that social quality of life is an important factor in adherence to medical care during the pandemic. Social life particularly in collectivist societies such as Saudi Arabia is important dimension of everyday life. The strict social distancing measures implemented during the pandemic has several repercussions on the social life of people in communities which have influences on their overall functioning. The impact of social quality of life in healthcare behaviors of patients with chronic illnesses has been reported in previous literature. For instance, a study from China demonstrated that community organizations are important source of social support, and they can help the patients gain health information and improve treatment adherence.24 Our study findings underscore the crucial role of QoL as a predictor of healthcare adherence. Considering these factors will ensure that patients with chronic health conditions could access and avail necessary medical care.
Study has some significant policy implications such as Saudi Arabia implemented a prolonged lockdown during the pandemic, and it is therefore necessary to have clear policy guidelines and course of appropriate actions to prevent adverse health consequences due to delay in the essential medical treatments for patients with NCDs. Such policies will ensure that patients with chronic conditions could access and avail necessary medical treatments during such health crisis situations. Interventions should focus on vulnerable populations such as women to prevent the irreversible loss associated with delayed care. Most patients avoided healthcare because they rely on media for information, and in current times misinformation is usually propagated through social media and internet, therefore, it is imperative that there should be clear health education to handle such issues. There should be focus on raising public awareness and urging patients to access needed healthcare to avoid the health risks associated with such medical care avoidance. Psychological support and improving environmental health should be the focus of public health interventions during health crises.
Study Limitations and Future Research
Findings need to be interpreted keeping in view some limitations such as data was primarily obtained from a self-report online survey, thus sample only comprises of participants who are active users of online technology, and this also suggests that rates of healthcare avoidance may be higher than reported in current analysis. The study used the data collected through an online survey method thus some of the potential biases such as self-report bias are inherent in the study. Besides we relied on the information given by the participants regarding adherence to healthcare and institutional or insurance data were not used. Moreover, data was collected during the time when the levels of generalized fear and anxiety related to COVID-19 infection were high in Saudi Arabia, and patients with chronic illnesses avoided such visits as a preventive course of action because visits to hospitals may expose them to catch infection. This is assumed because of poor psychological quality of life of patients. However, to draw valid inferences, future research should collect data about specific reasons why patients skipped medical care. There is also a need for population-based studies to obtain conclusive evidence about the impact of the pandemics on health care behaviors in patients with other illnesses to determine the role of social, economic, and cultural factors.
Conclusion
The assessment of the relationship of quality of life with healthcare avoidance provides a unique perspective to understand quality of life as predictor of healthcare utilization during the COVID-19 pandemic. Psychological, social and environmental quality of life appeared to be low among patients with NCDs during the pandemic and they appeared as significant factors associated with medical care avoidance, thus focus of interventions should be to enhance these aspects of health for patients with chronic illnesses. The study findings provide useful insight to understand and address quality of life factor that may hinder adherence to healthcare during health crisis periods such as pandemic.
Institutional Review Board Statement
The study was reviewed by ethical review committee, University of Ha’il and approved by the university letter H-2021-29 and has been conducted in accordance with the Declaration of Helsinki.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Funding
This research was funded by the Deanship of Research at the University of Ha'il, grant number RG-21007.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Smith KW, Avis NE, Assmann SF. Distinguishing between quality of life and health status in quality of life research: a meta-analysis. Qual Life Res. 1999;8(5):447–459. doi:10.1023/A:1008928518577
2. Theofilou P. Quality of life: definition and measurement. Eur J Psychol. 2013;9(1):150–162. doi:10.5964/ejop.v9i1.337
3. Ratner PA, Johnson JL, Jeffery B. Examining emotional, physical, social, and spiritual health as determinants of self-rated health status. Am J Health Promot. 1998;12(4):275–282. doi:10.4278/0890-1171-12.4.275
4. Olsen JA, Misajon R. A conceptual map of health-related quality of life dimensions: key lessons for a new instrument. Qual Life Res. 2020;29(3):733–743. doi:10.1007/s11136-019-02341-3
5. Jankowska A, Golicki D. Self-reported diabetes and quality of life: findings from a general population survey with the Short Form-12 (SF-12) health survey. Arch Med Sci. 2021. doi:10.5114/aoms/135797
6. Piotrowicz E, Mierzynska A, Pencina M, et al. Quality of life in heart failure patients undergoing hybrid comprehensive telerehabilitation versus usual care results of TELEREH-HF randomized clinical trial. Eur Heart J. 2020;41(Supplement_2):ehaa946–3109.
7. Al-Noumani H, Al-Harrasi M, Al Zaabi O, Natarajan J. Predictors of health-related quality of life in patients with non-communicable diseases: a national cross-section study. Appl Nurs Res. 2022;64:151566. doi:10.1016/j.apnr.2022.151566
8. Splinter MJ, Velek P, Ikram MK, et al. Prevalence and determinants of healthcare avoidance during the COVID-19 pandemic: a population-based cross-sectional study. PLoS Med. 2021;18(11):e1003854. doi:10.1371/journal.pmed.1003854
9. Zhao C, Batio S, Lovett R, Pack AP, Wolf MS, Bailey SC. The relationship between COVID-19 related stress and medication adherence among high-risk adults during the acceleration phase of the US outbreak. Patient Prefer Adherence. 2021;15:1895. doi:10.2147/PPA.S310613
10. Tóthová V, Bártlová S, Dolák F, et al. Quality of life in patients with chronic diseases. Neuro Endocrinol Lett. 2014;35(Suppl 1):11–18.
11. de Boer DR, Hoekstra F, Huetink KIM, Hoekstra T, Krops LA, Hettinga FJ. Physical activity, sedentary behavior and well-being of adults with physical disabilities and/or chronic diseases during the first wave of the COVID-19 pandemic: a rapid review. Int J Environ Res Public Health. 2021;18(12):6342. doi:10.3390/ijerph18126342
12. Cugmas M, Ferligoj A, Kogovšek T, Batagelj Z. The social support networks of elderly people in Slovenia during the Covid-19 pandemic. PLoS One. 2021;16(3):e0247993. doi:10.1371/journal.pone.0247993
13. Han K, Lee P, Lee S, Park E. Factors influencing quality of life in people with chronic illness in Korea. J Nurs Scholarsh. 2003;35(2):139–144. doi:10.1111/j.1547-5069.2003.00139.x
14. Algahtani FD, Hassan S-N, Alsaif B, Zrieq R. Assessment of the quality of life during COVID-19 pandemic: a cross-sectional survey from the Kingdom of Saudi Arabia. Int J Environ Res Public Health. 2021;18(3):847. doi:10.3390/ijerph18030847
15. Bryson WJ. Long-term health-related quality of life concerns related to the COVID-19 pandemic: a call to action. Qual Life Res. 2021;30(3):643–645. doi:10.1007/s11136-020-02677-1
16. O’Dwyer MC, Meixner K, Albiac LC, et al. Health-related quality of life for people with acute and chronic illnesses during the COVID-19 pandemic. J Am Board Fam Med. 2021;34(3):509–521. doi:10.3122/jabfm.2021.03.200593
17. Wańkowicz P, Szylińska A, Rotter I. The impact of the COVID-19 pandemic on psychological health and insomnia among people with chronic diseases. J Clin Med. 2021;10(6):1206. doi:10.3390/jcm10061206
18. Wang Y, Duan Z, Ma Z, et al. Epidemiology of mental health problems among patients with cancer during COVID-19 pandemic. Transl Psychiatry. 2020;10(1):1–10. doi:10.1038/s41398-020-00950-y
19. Leite JS, Feter N, Caputo EL, et al. Managing noncommunicable diseases during the COVID-19 pandemic in Brazil: findings from the PAMPA cohort. Cien Saude Colet. 2021;26(3):987–1000. doi:10.1590/1413-81232021263.39232020
20. Kumar D, Bajaj G, Bhoria A, et al. The manifestation of anxiety as repercussion of COVID-19: a survey of medical practitioner’s opinion. Arab J Sci Eng. 2022;47(1):189–195. doi:10.1007/s13369-021-05686-5
21. Guo D, Han B, Lu Y, et al. Influence of the COVID-19 pandemic on quality of life of patients with Parkinson’s disease. Park Dis. 2020;2020:1216568. doi:10.1155/2020/1216568
22. Moroni F, Gramegna M, Ajello S, et al. Collateral damage: medical care avoidance behavior among patients with myocardial infarction during the COVID-19 pandemic. Case Rep. 2020;2(10):1620–1624. doi:10.1016/j.jaccas.2020.04.010
23. Flanagan S, Damery S, Combes G. The effectiveness of integrated care interventions in improving patient quality of life (QoL) for patients with chronic conditions. An overview of the systematic review evidence. Health Qual Life Outcomes. 2017;15(1):1–11. doi:10.1186/s12955-017-0765-y
24. Shen B, Guan T, Du X, Pei C, Zhao J, Liu Y. Medication adherence and perceived social support of hypertensive patients in China: a community-based survey study. Patient Prefer Adherence. 2022;16:1257–1268. doi:10.2147/PPA.S363148
25. Tyrovolas S, El Bcheraoui C, Alghnam SA, et al. The burden of disease in Saudi Arabia 1990–2017: results from the global burden of disease study 2017. Lancet Planet Health. 2020;4(5):e195–208. doi:10.1016/S2542-5196(20)30075-9
26. Skevington SM, Lotfy M, O’Connell KA. The World Health Organization’s WHOQOL-BREF quality of life assessment: psychometric properties and results of the international field trial. A report from the WHOQOL group. Qual Life Res. 2004;13(2):299–310. doi:10.1023/B:QURE.0000018486.91360.00
27. Khoshhal S, Al-Harbi K, Al-Mozainy I, et al. Assessment of quality of life among parents of children with congenital heart disease using WHOQOL-BREF: a cross-sectional study from Northwest Saudi Arabia. Health Qual Life Outcomes. 2019;17(1):1–8. doi:10.1186/s12955-019-1249-z
28. Dalky HF, Meininger JC, Al-Ali NM. The reliability and validity of the Arabic World Health Organization quality of life-BREF instrument among family caregivers of relatives with psychiatric illnesses in Jordan. J Nurs Res. 2017;25(3):224–230. doi:10.1097/JNR.0000000000000146
29. Baggio S, Vernaz N, Spechbach H, et al. Vulnerable patients forgo health care during the first wave of the Covid-19 pandemic. Prev Med. 2021;150:106696. doi:10.1016/j.ypmed.2021.106696
30. Ahn S, Kim S, Koh K. Changes in healthcare utilization, spending, and perceived health during COVID–19: a longitudinal study from Singapore. Spending, and Perceived Health during COVID–19: A Longitudinal Study from Singapore (August 7, 2020); 2020.
31. Algamdi MM. Assessment of post-COVID-19 quality of life using the quality of life index. Patient Prefer Adherence. 2021;15:2587. doi:10.2147/PPA.S340868
32. Alkhamees AA, Alrashed SA, Alzunaydi AA, Almohimeed AS, Aljohani MS. The psychological impact of COVID-19 pandemic on the general population of Saudi Arabia. Compr Psychiatry. 2020;102:152192. doi:10.1016/j.comppsych.2020.152192
33. Ganson KT, Weiser SD, Tsai AC, Nagata JM. Associations between anxiety and depression symptoms and medical care avoidance during COVID-19. J Gen Intern Med. 2020;35(11):3406–3408. doi:10.1007/s11606-020-06156-8
34. Glenister KM, Ervin K, Podubinski T. Detrimental health behaviour changes among females living in rural areas during the COVID-19 pandemic. Int J Environ Res Public Health. 2021;18(2):722. doi:10.3390/ijerph18020722
35. Anderson KE, McGinty EE, Presskreischer R, Barry CL. Reports of forgone medical care among US adults during the initial phase of the COVID-19 pandemic. JAMA Netw open. 2021;4(1):e2034882–e2034882. doi:10.1001/jamanetworkopen.2020.34882
36. Salari N, Hosseinian-Far A, Jalali R, et al. Prevalence of stress, anxiety, depression among the general population during the COVID-19 pandemic: a systematic review and meta-analysis. Global Health. 2020;16(1):1–11. doi:10.1186/s12992-019-0531-5
37. Choobin MH, Mirabolfathi V, Chapman B, Moradi AR, Grunfeld EA, Derakshan N. The impact of COVID-19 outbreak on emotional and cognitive vulnerability in Iranian women with breast cancer. Front Psychol. 2021;12:1695. doi:10.3389/fpsyg.2021.663310
38. Lee M, You M. Avoidance of healthcare utilization in South Korea during the coronavirus disease 2019 (COVID-19) pandemic. Int J Environ Res Public Health. 2021;18(8):4363. doi:10.3390/ijerph18084363
39. Lu P, Kong D, Shelley M. Risk perception, preventive behavior, and medical care avoidance among American older adults during the COVID-19 pandemic. J Aging Health. 2021;33(7–8):577–584. doi:10.1177/08982643211002084
40. Mebrahtu G, Moleki MM, Achila OO, Seyoum Y, Adnoy ET, Ovberedjo M. Antihypertensive medication adherence and associated factors: a cross-sectional analysis of patients attending a National Referral Hospital in Asmara, Eritrea. Patient Prefer Adherence. 2021;15:2619. doi:10.2147/PPA.S319987
41. Soares P, Leite A, Esteves S, et al. Factors associated with the patient’s decision to avoid healthcare during the COVID-19 pandemic. Int J Environ Res Public Health. 2021;18(24):13239. doi:10.3390/ijerph182413239
42. Montemurro N. Telemedicine: could it represent a new problem for spine surgeons to solve? Glob Spine J. 2022;12(6):1306–1307. doi:10.1177/21925682221090891
43. Grant S, Blom AW, Craddock I, Whitehouse M, Gooberman-Hill R. Home health monitoring around the time of surgery: qualitative study of patients’ experiences before and after joint replacement. BMJ Open. 2019;9(12):e032205. doi:10.1136/bmjopen-2019-032205.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.