")
Back to Journals » International Journal of General Medicine » Volume 15
Factors Affecting Quality of Life in Hemodialysis Patients
Authors Yonata A , Islamy N, Taruna A, Pura L
Received 31 May 2022
Accepted for publication 22 August 2022
Published 12 September 2022 Volume 2022:15 Pages 7173—7178
DOI https://doi.org/10.2147/IJGM.S375994
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Ade Yonata,1 Nurul Islamy,2 Ahmad Taruna,1 Lukman Pura1
1Department of Internal Medicine, Faculty of Medicine, Lampung University–Abdul Moelok Hospital, Lampung, Indonesia; 2Department of Obstetry Ginecology, Faculty of Medicine, Lampung University–Abdul Moelok Hospital, Lampung, Indonesia
Correspondence: Ade Yonata, Department of Internal Medicine, Faculty of Medicine, Lampung University, Jl. Prof. Soemantri Brojonegoro No. 1, Bandar Lampung, 35145, Indonesia, Tel/Fax +62721 7691197, Email [email protected]
Background: Hemodialysis is one of the main therapies for patients with end-stage renal disease. Quality of life is essential in the management of chronic kidney disease (CKD) patients undergoing hemodialysis. Factors that influence the quality of life in hemodialysis patients must be identified.
Purpose: This research evaluated the quality of life in CKD patients undergoing hemodialysis and determined factors affecting the quality of life.
Patients and Methods: This study used an analytical survey method with a cross-sectional design. The Subjective Global Assessment (SGA) questionnaire was used to evaluate nutritional status, and the KDQOL-SFTM questionnaire was used to evaluate quality of life. The bivariate statistical test applied was the Student’s t-test or the Mann–Whitney U-test. Multivariate analysis was done using logistic regression.
Results: The total number of hemodialysis patients in the study was 124. Their median age was 44 years. The patients consisted of 66 (53%) men and 58 (47%) women. Overall, 84 patients had good quality of life (67.7%), and 40 (32.3%) reported poor quality of life. Our study showed a relationship between economic status and quality of life (p = 0.029) and between the number of comorbid factors and quality of life (p = 0.014). No relationship was found between nutritional status and quality of life (p = 0.121). Multivariate analysis using logistic regression analysis showed that the number of comorbidities was a significant factor in quality of life (p = 0.004, OR = 3.4 [1.67– 7.46]).
Conclusion: The majority of hemodialysis patients had good quality of life. Logistic regression analysis found that the number of comorbidities was a significant factor in the quality of life of hemodialysis patients. Comorbidities in hemodialysis patients must be managed to improve their quality of life.
Keywords: comorbid, quality of life, hemodialysis
Introduction
Chronic kidney disease is defined as kidney damage or a glomerular filtration rate (GFR) of less than 60 mL/min/1.73 m2 for at least three months. Regardless of the underlying etiology, once the loss of nephrons and reduction in functional kidney mass reach a certain point, the remaining nephrons initiate an irreversible sclerosis process, leading to a progressive decrease in GFR.1,2
Treatment of chronic renal failure is divided into two stages: conservative management and renal replacement therapy. The most frequently given kidney replacement therapy is hemodialysis, followed by continuous ambulatory peritoneal dialysis.3–5
Quality of life is an individual’s perception of their position in life in the context of their culture, value system, and relationship to life goals, expectations, standards, and other related matters. Quality of life is an increasingly important factor in the assessment of the management of chronic kidney disease patients undergoing hemodialysis.6,7
Several studies have shown a decreased quality of life and increased depression in the hemodialysis patient population.8–10 Poor quality of life itself is also reported to increase complications such as depression and malnutrition and even increase mortality.11 Several factors such as anemia, age, duration of hemodialysis, number of comorbid diseases, and number of medications are known to be factors related to the quality of life of hemodialysis patients.12,13
Little research exists on the quality of life of hemodialysis patients in Indonesia, especially using multivariate analysis. Therefore, we performed this study to describe the quality of life of hemodialysis patients and determine the independent factors associated with poor quality of life in Indonesian patients with hemodialysis.
Research Methods
This study used an analytical survey method with a cross-sectional design. Its purpose was to assess the quality of life and the factors that influence it in patients with chronic renal failure undergoing hemodialysis therapy at Dr. Abdul Moeloek Hospital. Sampling in this study was conducted using a consecutive technique. All eligible confirmed hemodialysis patients (>3 months hemodialysis duration, literate, and able to understand Bahasa Indonesia) who were consecutively enrolled for treatment at the study sites from June to August of 2021 were included in the study. Patients with physical or cognitive limitations that prevented them from being able to answer questions were excluded. Data were collected from the participants’ medical records and completed questionnaires.
This study was conducted in accordance with the principles of the Declaration of Helsinki. All protocols used throughout were approved by the Dr. Abdul Moeloek Hospital Ethics Committee. All patients provided informed consent and were given the opportunity to refuse participation.
All patients were given the KDQOL-SF™ questionnaire. All general dimensions and kidney domains were scored. The score scale is 0–100 per domain, where higher scores correspond to better quality of life. For all dimensions and domains, a mean score of less than 60 was considered poor quality of life, and a mean score of more than or equal to 60 was considered good quality of life.
The questionnaire used to evaluate nutritional status was the Subjective Global Assessment (SGA). The rank of SGA is determined on the basis of subjective weighting by clinician. The economic status parameter was based on income per month. Income per month of less than two million IDR was classified as low economic status, income between two and four million IDR as middle economic status, and income over four million IDR as good economic status. The categories were based on the regional minimum salary and the Central Agency of Statistics of Indonesia.
Bivariate analysis was used to determine the relationship between variables using statistical tests. The bivariate statistical test used was the Student’s t-test or Mann–Whitney U-test. All variables in which p < 0.25 in bivariate analysis underwent multivariate analysis using logistic regression.
Results
This study included 124 chronic kidney disease patients undergoing hemodialysis. The demographic and clinical characteristics of the patients are shown in Table 1. Their median age was 44 years, with a minimum age of 21 years and a maximum age of 69 years. The patients consisted of 66 (53%) men and 58 (47%) women. The duration of hemodialysis ranged from one to 12 years, with a median of five years.
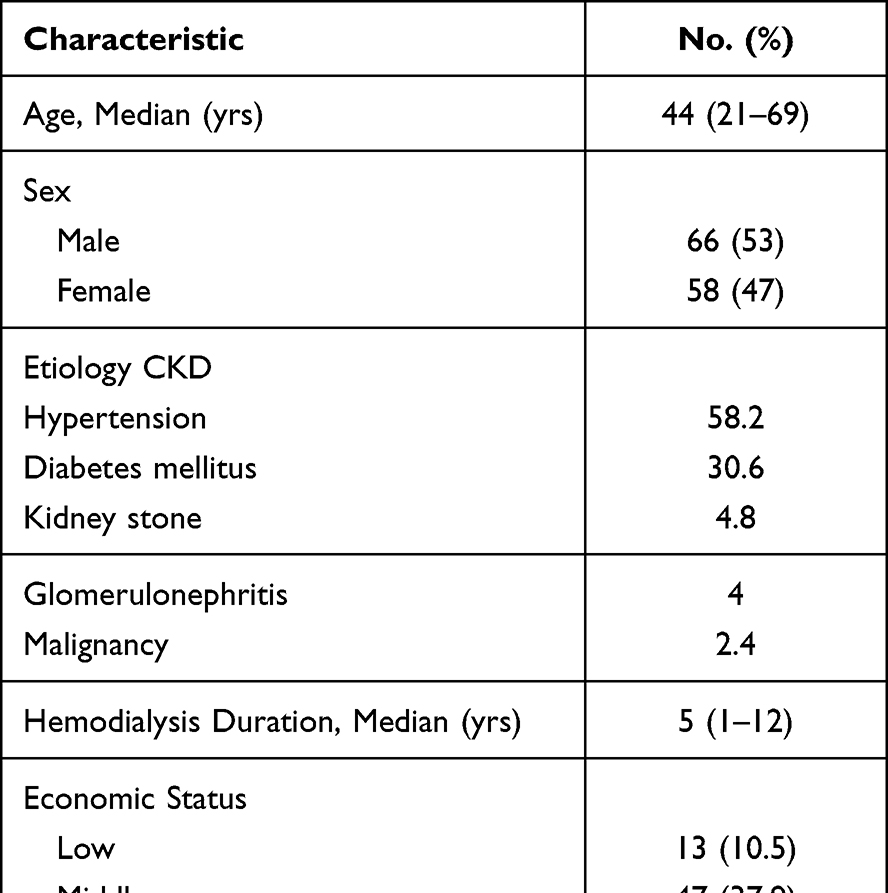 |
Table 1 Baseline Characteristics of Hemodialysis Patients |
The majority of patients in this study (64; 51.6%) had a good economic status, with a family income of greater than four million IDR. Most of the hemodialysis patients (79; 63.7%) had two comorbidities, 22.5% had one comorbidity, and 13.8% had more than three comorbidities. The comorbid conditions assessed were cardiac disease, diabetes, hypertension, cerebrovascular disease, non-autoimmune arthritis, eye disease, autoimmune disease, COPD, gastrointestinal disease, and malignancy. The most common comorbidity was hypertension, followed by cardiac disease (data not shown). Around 36.3% of hemodialysis patients had good nutritional status, and 49.1% had moderate nutritional status. Only 14.6% of hemodialysis patients were malnourished.
Most patients in the study reported good quality of life (84; 67.7%), and only 40 (32.3%) reported poor quality of life. No relationship was found between age and quality of life (p = 0.082) or from the unpaired t-test analysis between the duration of hemodialysis and quality of life (p = 0.075). Our study showed a relationship between economic status and quality of life (p= 0.029) and between number of comorbidities and quality of life (p = 0.014) in bivariate analysis. No relationship existed between nutritional status and quality of life, as shown in Table 2 (p = 0.121).
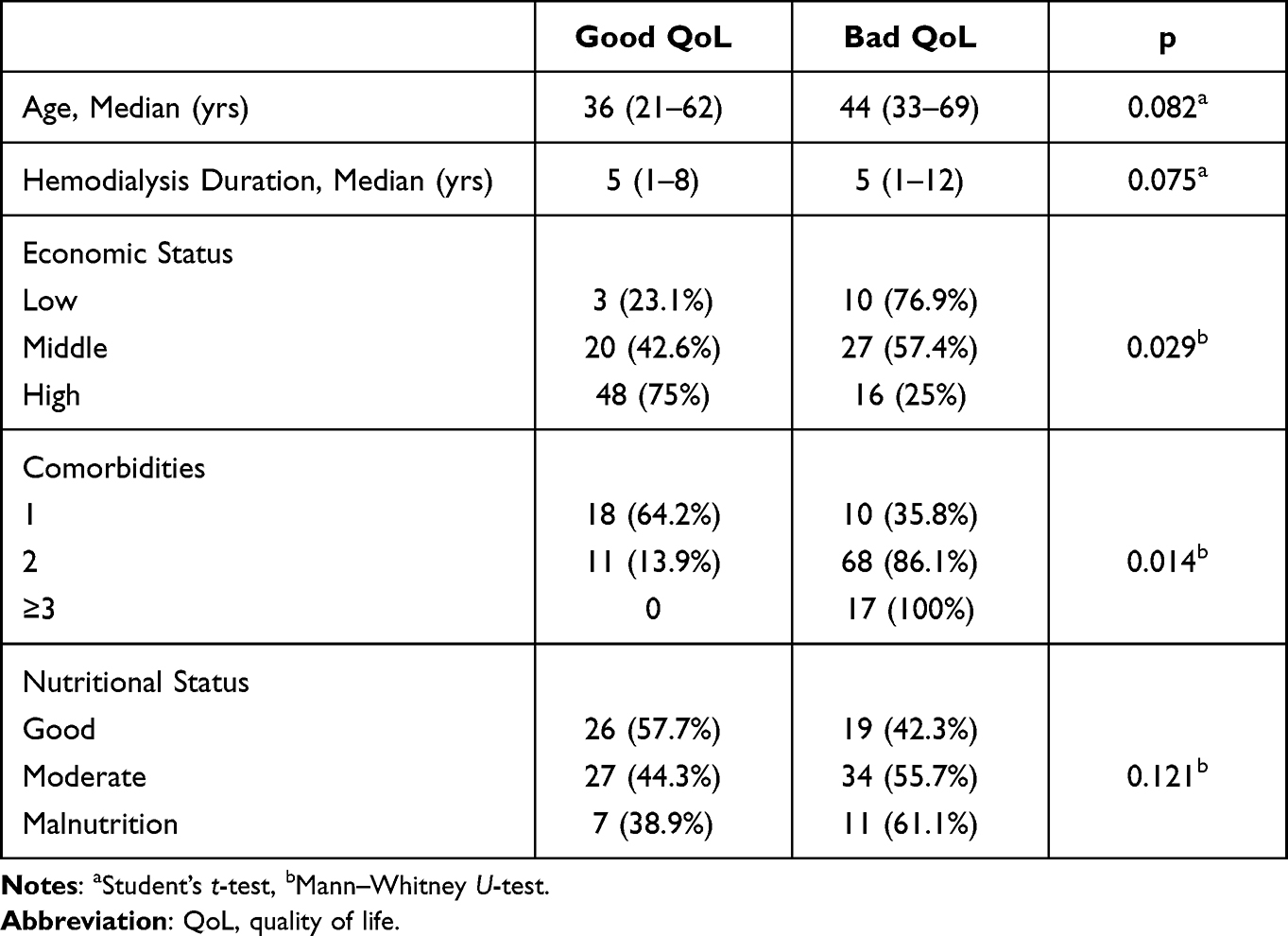 |
Table 2 Bivariate Analysis of Quality of Life in Hemodialysis Patients |
From the bivariate results, we found several variables with p < 0.25: economic status (p = 0.029), number of comorbidities (p = 0.014), and nutritional status (p = 0.121). These three variables were then analyzed using multivariate logistic regression analysis. The multivariate logistic regression analysis can be seen in Table 3. Our multivariate analysis showed that comorbidity was a statistically significant factor (p = 0.004; OR = 3.4 [1.67–7.46]).
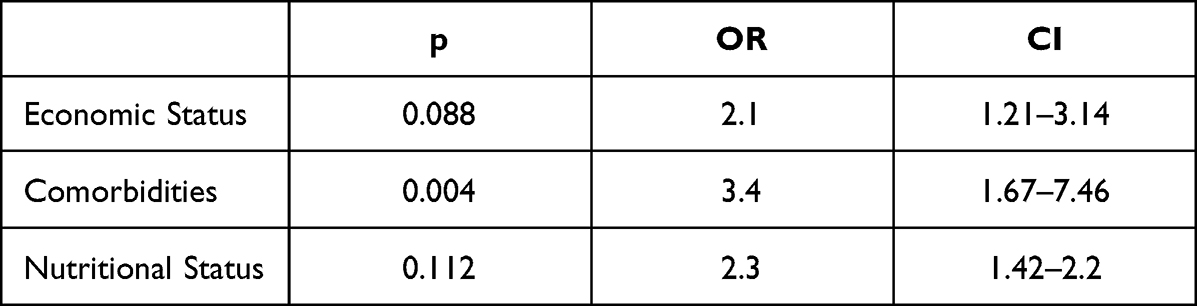 |
Table 3 Multivariate Analysis of Quality of Life in Hemodialysis Patients |
Discussion
In our study, the majority of hemodialysis patients had good quality of life. This was different from other studies that showed decreased quality of life in hemodialysis patients.8,9 This difference could be because of differences in the population characteristics. In our sample, the median age was 44 (21–69) years. Many of our patients were younger compared to the other studies. The duration of hemodialysis in our study was also longer, with a median of 5 years (1–12 years). Most of our patients had already adapted to hemodialysis and their general health mostly had already stabilized, and the most severe hemodialysis patients had already died.
Gerasimoula et al found the total quality of life score to be higher in participants under 60 years old.14 Joshvi et al found that patients with chronic kidney disease on dialysis had five variables associated with lower quality of life: age, ethnicity, employment status, income, and duration of hemodialysis.7 These results are slightly different from our study, where age and duration of hemodialysis were not associated with quality-of-life scores. The discrepancy could be due to differences in the nature of the patient population: many patients in our hemodialysis unit have had chronic kidney disease from a young age, some even since childhood, due to autoimmune-related etiology such as primary glomerulonephritis or lupus nephritis. Some also develop hypertension at a young age with complications of the heart and blood vessels.
Our study revealed a relationship between economic status and quality of life (p= 0.029). Most hemodialysis patients had an income of over 4 million IDR. The Mann–Whitney U-test analysis of family income on quality of life revealed a significant relationship (p = 0.029) between low income and poor quality-of-life scores. These results are similar to those of Josi et al, which found low income to be an independent negative predictor of quality-of-life scores in hemodialysis patients.7 One reason for this link could be that even though all patients are covered for treatment by National Health Insurance, very low income generally affects all other aspects of their lives. Some patients complained about the cost of public transportation when the distance from their homes was far, as well as the need for costs if they had to be hospitalized for blood transfusions or other clinical problems.
Our study found a significant relationship between the number of comorbidities and the quality-of-life score (p = 0.014). A greater number of comorbidities predicted lower quality of life. This is understandable because generally, the greater the number of comorbidities, the more a patient’s health status deteriorates, affecting their physical, mental, and social status.
We found no relationship between nutritional status and quality of life. Research by Dwyer et al indicated that nutritional status affects the quality of life in hemodialysis patients. However, their study was slightly different from ours. In our study, the nutritional status used was based only on the SGA. In the study of Dwyer et al, the nutritional status was based on energy intake, serum creatinine, serum albumin, appetite, and BMI. Their study found that appetite, dietary energy intake, serum albumin, and serum creatinine were associated with Physical Component Scale quality scores.15
Comorbidity was found to be a factor that affected the quality of life of our hemodialysis patients (p = 0.004; OR = 3.4 [1.67–7.46]) in multivariate analysis. These results are similar to those obtained by Cha et al5 in their study in Korea, where the quality-of-life scores differed significantly based on the number of comorbidities (<0.001). Likewise, research conducted by Mandoorah et al in Saudi Arabia and Stojanovic et al in Serbia also found that comorbidities reduce patients’ quality of life.16,17
Our study has some limitations. We explored only a few factors affecting quality of life. We also only used SGA to determine nutritional status, rather than using other physical and laboratory results. Further multicenter studies with larger sample sizes and more quality of life variable factors might be needed.
Conclusion
Our study demonstrated that most of the hemodialysis patients had good quality of life. Logistic regression found that the number of comorbidities was a significant factor in quality of life for hemodialysis patients. Comorbidities in hemodialysis patients must be managed to improve their quality of life.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lamb EJ, Levey AS, Stevens PE. The Kidney Disease Improving Global Outcomes (KDIGO) guideline update for chronic kidney disease: evolution not revolution. Clin Chem. 2013;59(3):462–465. doi:10.1373/clinchem.2012.184259
2. Schnaper HW. Remnant nephron physiology and the progression of chronic kidney disease. Pediatr Nephrol. 2014;29(2):193–202. doi:10.1007/s00467-013-2494-8
3. Daugirdas JT, Depner TA, Inrig J, et al. KDOQI clinical practice guideline for hemodialysis adequacy: 2015 update. Am J Kidney Dis. 2015;66(5):884–930. doi:10.1053/j.ajkd.2015.07.015
4. Suzuki H, Hoshi H, Inoue T, Kikuta T, Tsuda M, Takenaka T. Combination therapy with hemodialysis and peritoneal dialysis. Contrib Nephrol. 2012;177:71–83.
5. Cha J, Han D. Health-related quality of life based on comorbid among patients with end-stage renal disease. Osong Public Health Res Perspect. 2020;11(4):194–200. doi:10.24171/j.phrp.2020.11.4.08
6. WHOQOL GROUP, T. Development of the World Health Organization WHOQOL-BREF quality of life assessment. Psychol Med. 1998;28(3):551–558. doi:10.1017/S0033291798006667
7. Joshi U, Subedi R, Poudel P, Ghimire PR, Panta S, Sigdel MR. Assessment of quality of life in patients undergoing hemodialysis using WHOQOL-BREF questionnaire: a multicenter study. Int J Nephrol Renovasc Dis. 2017;10:195–203. doi:10.2147/IJNRD.S136522
8. Yang F, Griva K, Lau T, et al. Health-related quality of life of Asian patients with end-stage renal disease (ESRD) in Singapore. Qual Life Res. 2015;24(9):2163–2171. doi:10.1007/s11136-015-0964-0
9. Kang GW, Lee IH, Ahn KS, Lee J, Ji Y, Woo J. Clinical and psychosocial factors predicting health-related quality of life in hemodialysis patients. Hemodial Int. 2015;19(3):439–446. doi:10.1111/hdi.12271
10. Khan A, Khan AH, Adnan AS, Sulaiman SAS, Mushtaq S. Prevalence and predictors of depression among hemodialysis patients: a prospective follow-up study. BMC Public Health. 2019;19(1):531. doi:10.1186/s12889-019-6796-z
11. Walters BA, Hays RD, Spritzer KL, Fridman M, Carter WB. Health-related quality of life, depressive symptoms, anemia, and malnutrition at hemodialysis initiation. Am J Kidney Dis. 2002;40(6):1185–1194. doi:10.1053/ajkd.2002.36879
12. Türk S, Guney I, Altintepe L, Tonbul Z, Yildiz A, Yeksan M. Quality of life in male hemodialysis patients, role of erectile dysfunction. Nephron Clin Pract. 2004;96:c21–C27. doi:10.1159/000075568
13. Zyoud SH, Daraghmeh DN, Mezyed DO, et al. Factors affecting quality of life in patients on haemodialysis: a cross-sectional study from Palestine. BMC Nephrol. 2016;17(1):44. doi:10.1186/s12882-016-0257-z
14. Gerasimoula K, Lefkothea L, Maria L, Victoria A, Paraskevi T, Maria P. QUALITY OF LIFE IN HEMODIALYSIS PATIENTS. Mater Sociomed. 2015;27(5):305–309. doi:10.5455/msm.2015.27.305-309
15. Dwyer JT, Larive B, Leung J, et al. Nutritional status affects quality of life in Hemodialysis (HEMO) Study patients at baseline. J Ren Nutr. 2002;12(4):213–223. doi:10.1053/jren.2002.35297
16. Mandoorah QM, Shaheen FA, Mandoorah SM, Bawazir SA, Alshohaib SS. Impact of demographic and comorbid conditions on quality of life of hemodialysis patients: a cross-sectional study. Saudi J Kidney Dis Tran. 2014;25(2):432–437. doi:10.4103/1319-2442.128613
17. Stojanovic M, Stefanovic V. Assessment of health-related quality of life in patients treated with hemodialysis in Serbia: influence of comorbidity, age, and income. Artif Organs. 2007;31(1):53–60. doi:10.1111/j.1525-1594.2007.00340.x
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.