Back to Journals » Nature and Science of Sleep » Volume 17

Task-Shifting from Acupuncturists to Nurses in Delivering Acupuncture/Acupressure or Supervising Patient Self-Administered Acupressure for Sleep Management: Is It Feasible?
Authors Zhao FY ![]() , Zhang WJ, Chow CM
, Zhang WJ, Chow CM ![]() , Lee YX
, Lee YX ![]() , Xu P, Ho YS, Fu QQ
, Xu P, Ho YS, Fu QQ ![]() , Conduit R
, Conduit R ![]()
Received 8 August 2025
Accepted for publication 27 October 2025
Published 7 November 2025 Volume 2025:17 Pages 2887—2900
DOI https://doi.org/10.2147/NSS.S556267
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Valentina Alfonsi
Fei-Yi Zhao,1– 4,* Wen-Jing Zhang,4,* Chin Moi Chow,3,5,* Yuan Xin Lee,4 Peijie Xu,6 Yuen-Shan Ho,7 Qiang-Qiang Fu,8 Russell Conduit2
1Department of Nursing, School of International Medical Technology, Shanghai Sanda University, Shanghai, 201209, People’s Republic of China; 2School of Health and Biomedical Sciences, RMIT University, Bundoora, VIC, 3083, Australia; 3Sydney School of Health Sciences, Faculty of Medicine and Health, The University of Sydney, Camperdown, NSW, 2050, Australia; 4Shanghai Municipal Hospital of Traditional Chinese Medicine, Shanghai University of Traditional Chinese Medicine, Shanghai, 200071, People’s Republic of China; 5Sleep Research Group, Charles Perkins Centre, The University of Sydney, Camperdown, NSW, 2050, Australia; 6School of Computing Technologies, RMIT University, Melbourne, VIC, 3000, Australia; 7School of Nursing, Faculty of Health and Social Sciences, The Hong Kong Polytechnic University, Hong Kong SAR, People’s Republic of China; 8Yangpu Hospital, School of Medicine, Tongji University, Shanghai, 200090, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yuen-Shan Ho, School of Nursing, Faculty of Health and Social Sciences, The Hong Kong Polytechnic University, Hong Kong SAR, People’s Republic of China, Tel +852 2766-6410, Fax +852 2364-9663, Email [email protected] Qiang-Qiang Fu, Yangpu Hospital, School of Medicine, Tongji University, Shanghai, 200090, People’s Republic of China, Tel + 86 021-6569 0520, Fax + 86 021-6569 6249, Email [email protected]
Abstract: Acupuncture and acupressure are widely used for managing self-reported impaired sleep quality and duration. However, outside East Asia, access is often limited due to a shortage of trained acupuncturists and minimal reimbursement under national health insurance systems, leading to treatment discontinuation or inaccessibility driven by “Financial Toxicity.” This prompts a critical yet underexplored inquiry: can advanced practice nurses serve as alternative providers to deliver acupuncture/acupressure for managing these common sleep complaints, thereby improving accessibility, expanding treatment coverage, and lowering consultation costs? This comprehensive mini-review synthesizes current evidence to assess the feasibility of this promising and innovative acupuncturist-nurse task-shifting paradigm and outlines key preparatory steps for its pilot implementation.
Keywords: traditional chinese medicine, TCM nursing, sleep disorder, sleep disturbance, insomnia, complementary and alternative medicine
Background
Prevalence, Health Impact, and Psychological Interventions for Impaired Sleep Quality and Duration
Sleep disturbance constitutes a widespread and consequential public health concern in contemporary 24-hour societies.1 In Australia, 33–45% of adults report inadequate sleep duration or poor sleep health.2 Data from the US National Health and Nutrition Examination Survey (NHANES) indicate that 30.5% of adults experience at least one hour of sleep debt, 29.8% report sleep initiation/maintenance difficulties, and 27.2% suffer from excessive daytime sleepiness.3 Approximately 25% of adults in New Zealand are affected by chronic sleep problems.2 A broad range of sleep disturbances—from impaired sleep quality to reduced duration—has been associated with adverse health outcomes and increased all-cause mortality,4 including cardiovascular (eg, coronary artery disease, myocardial infarction, stroke),5 metabolic (eg, diabetes, obesity),5 psychiatric (eg, major depressive disorder, schizophrenia, post-traumatic stress disorder),6 as well as higher rates of serious motor vehicle accidents.7
Insomnia represents the most prevalent sleep disturbance.8 Its hallmark features, insufficient sleep duration and poor sleep quality, cause substantial distress and impair daily functioning.9 Impaired sleep quality and duration are also widespread among individuals with chronic diseases, even when formal diagnostic criteria for insomnia are not met. For example, non-restorative sleep and poor sleep quality are frequent complaints in rheumatoid arthritis patients and are associated with greater functional disability.10 Likewise, insufficient and poor-quality sleep are common in chronic kidney disease (CKD), contributing to disease progression and increased mortality among patients receiving maintenance dialysis.11 Cognitive-behavioral therapy for insomnia (CBTi) is established as a first-line treatment in insomnia management.9 Beyond insomnia, CBT has demonstrated efficacy in enhancing sleep quality and alleviating associated symptoms—such as depression, anxiety, and fatigue—across diverse chronic diseases, including the aforementioned rheumatoid arthritis12 and CKD.13
Nurses represent the largest professional group within the global healthcare workforce, prompting multiple countries to investigate their potential to lead or participate in CBT dissemination efforts.14 UK clinical data reveal that trained mental health nurses provide CBT with equivalent efficacy to psychiatrists and psychologists for comparable patient populations while demonstrating superior cost-effectiveness.14 A 2023 study published in The Lancet demonstrated that primary care nurses, following appropriate training, effectively administered brief, manualized sleep restriction therapy, yielding medium-to-large and sustained reductions in insomnia severity.15
Accessibility Challenges in Acupuncture and Its Non-Invasive Counterparts
Beyond CBT, acupuncture16 and acupressure17 are also favored by individuals with sleep disturbances who seek non-pharmacological therapies. Both stimulate specific acupoints on the body to achieve therapeutic benefits and are primary treatment approaches used by acupuncturists in clinical settings. Acupuncture involves inserting fine needles into acupoints,18 whereas acupressure applies manual pressure to acupoints using fingers/knuckles/thumbs or other tools.19 Despite their shared theoretical foundation, they differ in complexity, invasiveness, and accessibility, influencing their clinical adoption.
Acupuncture: Costly Expertise and Limited Access
Acupuncture is a sophisticated therapeutic procedure requiring precise execution to ensure both safety and efficacy.20 Despite its popularity, access faces multiple barriers. The primary challenge lies in the extensive training required to become a licensed acupuncturist: in East Asian countries such as Korea,21 China,22 and Japan,23 practitioners must complete four to six years of undergraduate education and pass rigorous national licensure examinations. While this lengthy training ensures competency, it also constrains the number of qualified providers. Outside East Asia, few universities offer full-time undergraduate programs in acupuncture or traditional Chinese medicine (TCM), and acupuncture is not yet fully integrated into many local healthcare systems—further diminishing its accessibility.
Financial burden compounds the issue. In most countries, acupuncture is rarely covered by national health insurance, leaving patients to pay out-of-pocket.24 Even with partial coverage, costs remain high. In the US, for instance, 75% of patients pay entirely out-of-pocket, and among those with insurance, two-thirds still bear at least half the cost.25 In Washington, D.C., the median fees for initial and follow-up acupuncture visits are $145 USD and $85 USD, respectively.25 Similarly, in the UK26 and Australia,27 limited reimbursement leads to comparable financial strain. The high cost frequently leads to treatment discontinuation, a phenomenon some studies term “Financial Toxicity” in acupuncture recipients.24
These challenges underscore the need to explore alternative approaches to improve the accessibility of acupuncture services, given their inherent complexity and resource demands.
Acupressure: Lower-Barrier Implementation for Wider Accessibility
Acupressure offers a simpler alternative to acupuncture for managing sleep disturbances. Unlike acupuncture’s muscle tissue penetration, acupressure applies pressure to the skin surface using fingers or instruments. While potentially less potent than needle stimulation,19 its non-invasive nature and technical simplicity enhance safety and accessibility for both practitioners and patients. Numerous studies have demonstrated its successful use in clinical settings for managing patient-reported sleep impairments28,29 and other health conditions.30 Moreover, for individuals interested in acupuncture but deterred by needle phobia, acupressure presents a viable option.24
Compared to acupuncture, acupressure is easier to learn. Beyond licensed acupuncturists, many studies document successful administration by various healthcare professionals including nurses,28 midwives,31 physiotherapists,32 and occupational therapists.33 Patients can also self-apply acupressure for sleep-related symptom relief.34,35 These advantages—operational simplicity and ease of dissemination—make acupressure particularly valuable in resource-limited areas with scarce acupuncturists, thereby broadening treatment availability for affected populations.
Objective, Rationale, and Framework of This Narrative Mini-Review
Accessibility Barriers and Potential Solutions
As outlined in the Background, acupuncture and acupressure are widely used non-pharmacological TCM approaches for sleep management. However, outside East Asia, the scarcity of licensed acupuncturists and the high out-of-pocket costs within Western healthcare systems limit patient access to these therapies. Nurses, the largest group of healthcare professionals, may provide a feasible solution. Task-shifting these interventions from acupuncturists to nurses could enhance accessibility and affordability for patients with sleep disturbances—a strategy that remains underexplored.
Aim, Scope, and Delimitations of This Mini-Review
This mini-review aims to evaluate the feasibility of integrating acupuncture and acupressure into nursing practice for managing patient-reported impaired sleep quality and duration—specifically, whether these interventions can be task-shifted from licensed acupuncturists to trained nurses. To address this objective, we (1) synthesize current evidence on the effectiveness and safety of nurse-delivered acupuncture and acupressure, and (2) discuss potential implementation challenges—including policy and technical barriers—and necessary strategic preparations.
The scope is limited to acupuncture and acupressure applied in contexts comparable to CBTi, targeting sleep impairments associated with primary or secondary insomnia or other chronic conditions. Distinct sleep disorders such as breathing-related sleep disorders, sleep-related movement disorders, and parasomnias are excluded because their pathophysiological mechanisms differ fundamentally from the sleep maintenance and quality issues central to this review. This exclusion ensures a focused and coherent scope.
Research Paradigm and Reporting Framework
This review adopts a narrative synthesis approach. While systematic reviews are required to follow rigorous reporting standards such as the PRISMA statement, no equivalent framework exists specifically for narrative reviews. Therefore, this study referred to the Scale for the Assessment of Narrative Review Articles (SANRA)36 to guide its structure and enhance the comprehensiveness and reporting quality of the synthesis.
Task-Shifting in Integrative Care: Rationale for Evolving Nursing Scope-of-Practice
Expanding the Nursing Role Through Task-Shifting
Task-shifting—delegating clinical responsibilities from physicians to nurses or other non-physician providers—has emerged globally as a solution to workforce shortages and the rising demand for affordable, high-quality care, particularly for patients with chronic and multimorbid conditions.37 A survey across 39 countries revealed that 69% had implemented task-shifting to varying extents, reflecting a global shift toward expanding nurses’ scope-of-practice in primary care.38
Evidence demonstrates that adequately trained advanced practice nurses (APNs) can deliver care comparable to or superior to that of physicians.38 A Cochrane review found that nurse-delivered care for selected acute and chronic physical conditions yielded comparable or better health outcomes than care provided by primary care physicians, with higher patient satisfaction and ratings. Nurses also achieved greater patient engagement through longer consultation durations and increased adherence to follow-up visits.39
In mental health care, another systematic review confirmed that nurses, when properly trained and supervised, can effectively deliver psychological services in resource-limited settings lacking specialists.40
These findings highlight the potential of nurses to bridge critical care gaps, including in areas like sleep management where accessibility challenges persist.
Conceptual Synergy Between Acupuncture/Acupressure and Modern Nursing: A Foundation for Integrative Practice
Our literature search found no policy-oriented studies, reviews, or commentaries addressing task-shifting from Traditional Chinese/Korean Medicine (TC/KM) practitioners/acupuncturists to nurses, underscoring both the novelty of this study and the need for further investigation in this area.
The prospects for such a task-shifting model appear promising for three key reasons:
First, growing evidence supports the integration of Complementary and Alternative Medicine approaches into nursing care due to their limited side effects compared to conventional biomedical treatments.41
Second, CBT is a highly complex and procedurally cumbersome therapeutic modality that goes beyond discrete techniques; it involves integrating cognitive-behavioral theory with individualized case conceptualization, maintaining structured therapeutic direction, fostering curiosity in problem exploration, and sustaining a strong therapeutic alliance.42 In contrast, acupuncture and acupressure involve more streamlined procedures and shorter session durations, making them more suitable for task-shifting and application in resource-constrained settings.
Third, three core conceptual synergies between acupuncture/acupressure and modern nursing philosophy provide a theoretical foundation for integration:
- Individualized and patient-centered care: Acupuncture and acupressure rely on syndrome differentiation,43 tailoring acupoint selection and stimulation methods based on each patient’s unique symptoms and response.44 This dynamic adaptation is regarded as a person-centered therapeutic strategy,44 which parallels nursing’s patient-centered philosophy and clinical workflow, reinforcing nurses’ professional autonomy.41
- Holistic philosophy: Both acupuncture/acupressure and nursing adopt holistic frameworks, interpreting symptoms as human responses to environmental interactions and informing diagnosis through symptom analysis.41,45
- Patient empowerment: Nurse-guided self-administered acupressure fosters a sense of personal responsibility empowering patients to manage their own symptoms and enhance their health literacy.46 This approach aligns with nursing’s focus on promoting self-efficacy and internal health locus of control.47
Clinical Evidence for Nurse-Led Acupuncture/Acupressure for Sleep Disturbance: From Direct Delivery to Patient Self-Administration
To assess the efficacy and safety of nurse-led acupuncture/acupressure in managing sleep disturbances, a systematic search was conducted across three databases: Cochrane CENTRAL, EMBASE (via Ovid), and MEDLINE (via PubMed). Inclusion criteria comprised (1) qualitative or quantitative investigations examining nurse-led acupuncture/acupressure interventions for sleep disturbances, with a primary focus on impaired sleep quality and duration; (2) required outcome measures assessing subjective sleep quality using validated instruments such as the Pittsburgh Sleep Quality Index (PSQI), Insomnia Severity Index, or sleep logs, or qualitative descriptions of patients’ sleep experiences; Studies incorporating objective measures such as total sleep time (TST), sleep onset latency (SOL), or wake after sleep onset (WASO) recorded via polysomnography or actigraphy were also eligible but not mandatory; (3) no restrictions on publication date or study location; and (4) publication in English. The search strategy and key terms are detailed in Appendix 1.
Following screening, 14 eligible studies were included (Appendix 2) and categorized by service delivery model: one group comprised studies where nurses directly performed acupuncture/acupressure, while the other consisted of studies where patients self-administered acupressure under nurse supervision. Key findings from both modalities were extracted and summarized in Table 1 and Table 2, and the collective evidence was critically analyzed.
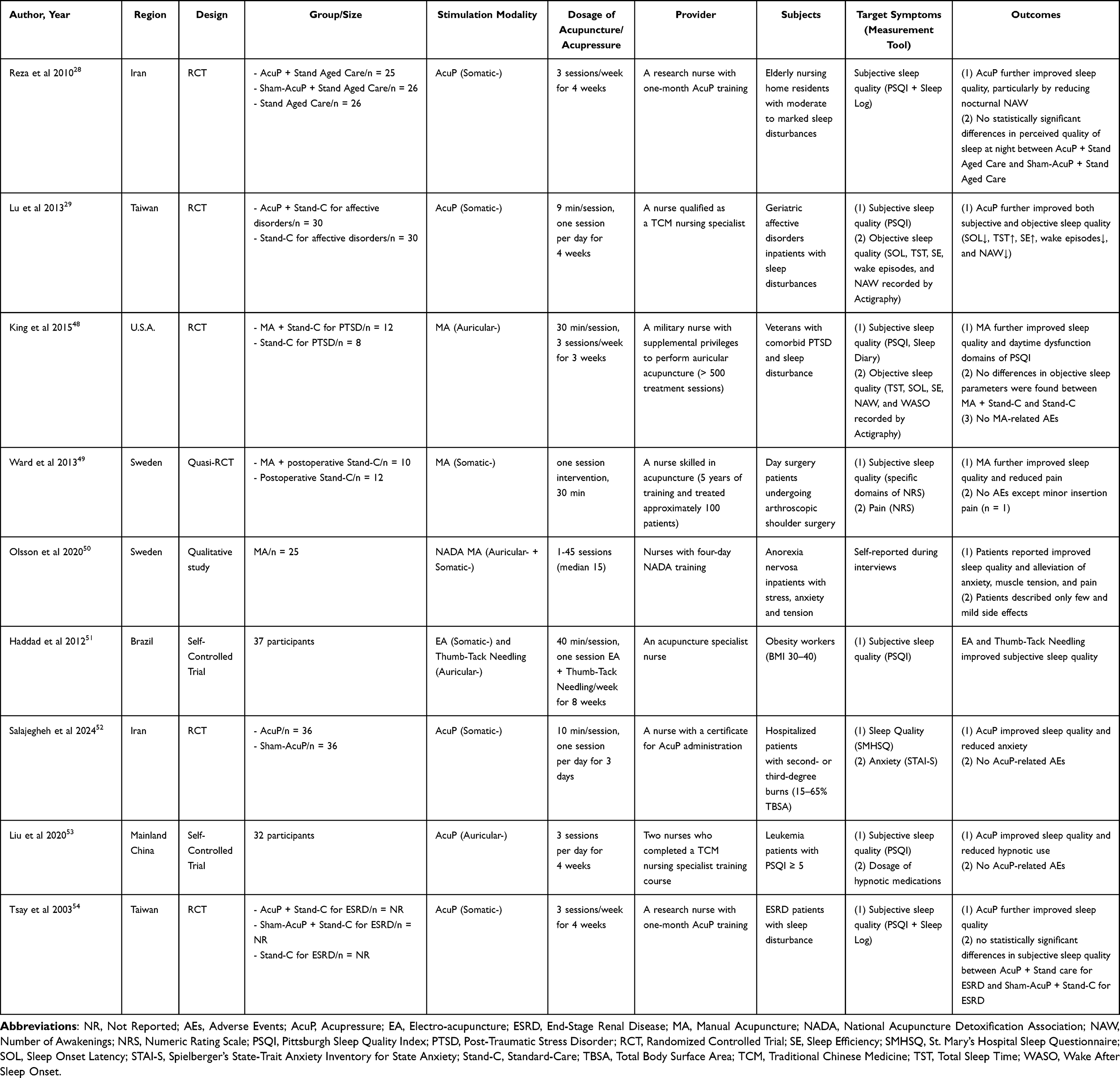 |
Table 1 Characteristics of Clinical Trials on Nurse-Delivered Acupuncture/Acupressure for Sleep Management |
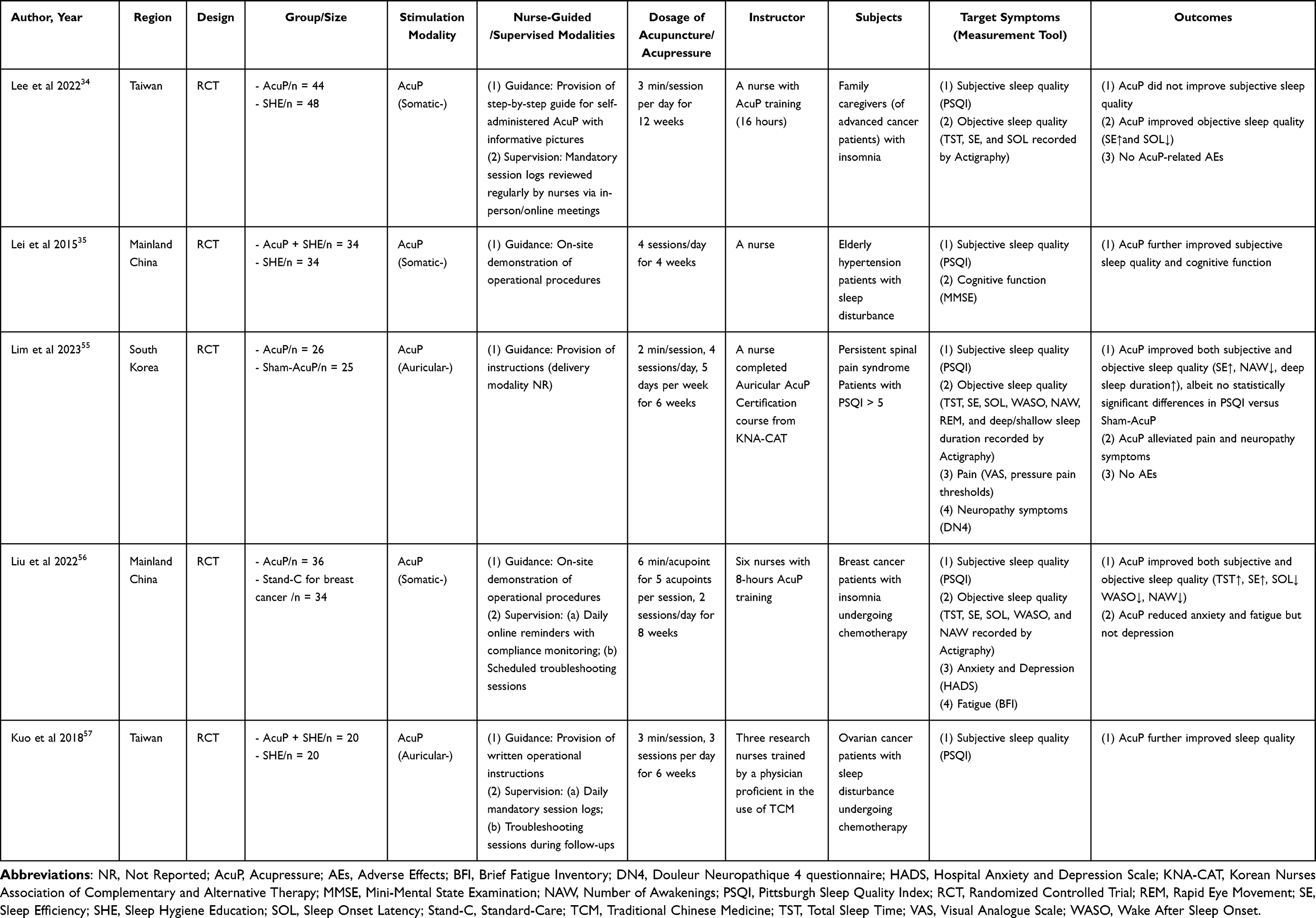 |
Table 2 Characteristics of Clinical Trials on Nurses-Guided/Supervised Patient Self-Administered Acupressure for Sleep Management |
Clinical Evidence Concerning Nurse-Delivered Acupuncture/Acupressure in Sleep Management
Nurse-delivered acupuncture has demonstrated results for managing sleep disturbances across diverse populations, though trial data remains limited. A US randomized controlled trial (RCT) on veterans with comorbid post-traumatic stress disorder and sleep disturbances found that nine sessions of nurse-delivered acupuncture significantly improved subjective sleep quality and reduced daytime dysfunction, with no reported adverse events.48 Qualitative interviews embedded in the RCT further revealed high patient acceptance and satisfaction, citing improved sleep, relaxation, and reduced musculoskeletal pain and headaches.58 All treatments were administered by a military nurse with two years of acupuncture experience.48,58 In Sweden, a trial with 10 patients undergoing arthroscopic shoulder surgery found that a 30-minute acupuncture session delivered by a registered nurse (RN) improved postoperative pain and sleep quality compared to non-acupuncture controls. Only minor needle-insertion discomfort was reported.49 Another Swedish qualitative study on anorexia nervosa patients reported improved sleep quality and reduced anxiety following nurse-administered acupuncture, even after discontinuing hypnotics. Participants expressed interest in more individualized acupuncture treatment and continuation beyond the study.50 In Brazil, a trial on obese workers found that nurse-delivered acupuncture reduced PSQI scores by three points,51 reaching the threshold for minimal clinically important difference for sleep improvement59 (See Table 1).
Nurse-delivered acupressure has also shown significant benefits. An Iranian RCT demonstrated that elderly patients with moderate-to-severe insomnia experienced a 5.04-point reduction in PSQI scores after four weeks of nurse-administered acupressure, outperforming sham-acupressure groups.28 Additional clinical evidence confirmed such benefits extend to secondary sleep disturbances in diverse conditions, including affective disorders,29 unintentional second- or third-degree burns,52 leukemia,53 and end-stage renal disease (ESRD).54 Particularly noteworthy are actigraphy-documented outcomes in affective disorder patients, showing extended TST, improved sleep efficiency, and reduced SOL, alongside decreased nocturnal awakenings and wake episodes29 (See Table 1).
Clinical Evidence Concerning Nurse-Guided and Supervised Patient Self-Administered Acupressure in Sleep Management
Studies also support the feasibility of nurse-guided patient self-administered acupressure for sleep management. For instance, Lee et al found that family caregivers of advanced cancer patients with insomnia improved sleep efficiency and reduced SOL—measured by actigraphy—through self-acupressure under a nurse’s supervision, though PSQI scores showed no significant change. No adverse events were reported, supporting the well-tolerated safety profile of this approach34 (See Table 2).
Four RCTs further confirmed the benefits of nurse-guided/supervised self-acupressure in patients experiencing sleep disturbances secondary to hypertension,35 persistent spinal pain syndrome,55 breast cancer,56 and ovarian cancer.57 In addition to enhancing subjective and/or objective sleep quality, participants also reported improvements in comorbid symptoms, such as anxiety,56 fatigue,56 pain,55 and cognitive impairment35 (See Table 2).
Diversity of Interventions and Clinical Implications
It is important to note that the studies summarized in Table 1 and Table 2 exhibited considerable clinical heterogeneity across multiple domains. Key variations included intervention type (eg, manual or electro-acupuncture, somatic or auricular acupressure), treatment protocols (eg, acupoints selection, treatment dosage), and participant populations (eg, primary or post-operative insomnia sufferers, patients with hypertension or ESRD reporting significant sleep impairments, and cancer survivors with chemotherapy-induced sleep disturbances). Substantial differences were also observed in the training and experience of nurses delivering or supervising the treatments. This diversity underscores the high flexibility and real-world applicability of nurse-led acupuncture and acupressure, supporting their potential for broad implementation across diverse clinical settings and patient groups. Nonetheless, such variability also highlights the necessity for future studies to adopt more standardized designs to isolate core active components and establish optimized treatment parameters.
Potential Mechanisms of Acupuncture/Acupressure in Alleviating Sleep Disturbance
Numerous studies have investigated the mechanisms by which acupuncture improves sleep disturbances, using molecular biology18 and neuroimaging techniques.60 Somatic acupuncture/acupressure appears to enhance sleep quality by activating the parasympathetic nervous system, increasing autonomic responses, and reducing psychological stress.61,62 In contrast, auricular stimulation stabilizes the autonomic nervous system by simultaneously activating the parasympathetic and inhibiting the sympathetic branches, thereby diminishing sleep disturbances and reducing reliance on sedatives.63
In the context of insomnia, acupuncture’s therapeutic actions may involve the modulation of brain-derived neurotrophic factors, inflammatory cytokines, the hypothalamic–pituitary–adrenal axis, neurotransmitters, and gut microbiota.18 Additionally, acupuncture may alter the activity of key brain regions, notably within the default mode network, including the frontal lobe and precuneus.60 Our previous review offers a detailed summary of these mechanisms for further reference.18 Another systematic review concluded that acupuncture can mitigate the effects of sleep deprivation by restoring sleep homeostasis and modulating the associated negative emotions and cognitive deficits. This is achieved by enhancing the activity intensity in the default network, precuneus anterior lobe, cingulate gyrus, and other related brain regions, as well as by strengthening the connectivity between the frontal and temporal lobes and reinforcing synchronized neural network interactions.64
Advancing Nurse-Led Acupuncture/Acupressure: Challenges and Strategic Preparation
Evidence Gaps and Research Priorities
While existing clinical trial evidence generally supports the efficacy of nurse-led acupuncture/acupressure in improving sleep outcomes, most are constrained by limited sample sizes and a lack of sham-controls, complicating attribution of observed benefits to specific treatment effects versus nonspecific placebo responses. Furthermore, inadequate assessment during intervention and limited medium- to long-term follow-up obscure the onset and sustainability of therapeutic effects. Even among the few sham-controlled RCTs, some did not detect statistically significant differences between verum and sham interventions.28,55 These limitations underscore the need for larger, rigorously designed multicenter trials incorporating sham-controls, frequent early assessments, and extended follow-up to accurately evaluate true efficacy, time of onset, and sustainability of nurse-led acupuncture/acupressure. Nesting qualitative and cost-effectiveness analyses within these trials could also provide insights into (1) patients’ experiences and their perspectives on the task-shifting model from acupuncturists to nurses, and (2) the socioeconomic implications of this model, and thereby aiding policy development.
Additionally, systematic reviews and meta-analyses are warranted to separately appraise primary sleep disturbances and those secondary to somatic or psychological conditions. Such evidence would help clarify the magnitude of treatment response to nurse-administered acupuncture/acupressure across different subtypes of sleep disorders and support evidence-based nursing practices in diverse clinical settings.
Variations in Policy and Clinical Integration Pathways for Nurse-Delivered Acupuncture/Acupressure
Acupressure: High Cost-Effectiveness Warrants Further Promotion
Unlike the five-year or longer training required to qualify as a licensed TC/KM practitioner authorized to perform acupuncture/acupressure in China22 and South Korea,21 several reviewed studies document that even nurses without prior traditional medicine knowledge can acquire effective acupressure skills through brief training programs—as short as 8 hours.56 Clinical research from Iran and Brazil indicates that nurse-delivered acupressure is effective not only for impaired sleep quality and duration—the focus of this study—but also for conditions such as restless legs syndrome65 and obstructive sleep apnea.51 These findings substantiate the high cost-effectiveness of transitioning acupressure delivery from acupuncturists to RNs in sleep management.
Interestingly, this task-shifting paradigm has gained significant policy endorsement in China. To address physician shortages and care gaps, nurse-led clinics—modeled after those in developed countries—have been widely established.66 These include nurse-led TCM clinics, where APNs provide interventions, such as acupressure, Gua-Sha (a traditional East Asian technique involving press-stroking the skin with a smooth tool to elicit therapeutic petechiae), and moxibustion (a TCM method that involves burning Artemisia vulgaris on or near acupoints to apply heat and relieve symptoms).67 Our previous qualitative study found that Chinese APNs expressed strong interest in providing such care.67 Similarly, in Australia, many physicians and nurses are open to further training in acupressure, with nurses showing greater enthusiasm for clinical and educational application.27 This widespread receptiveness also supports the potential integration of acupressure—and possibly broader CAM content—into mainstream medical education curricula.27 Nevertheless, our prior findings also revealed that APNs in China seek more explicit standardized operational guidelines—encompassing syndrome differentiation methods, rationale for acupoint selection, and protocols for treatment frequency and duration—to guide the effective and safe delivery of TCM nursing techniques, including acupressure.67 Consequently, it is imperative to establish a multidisciplinary consensus among experts in TCM, nursing, and sleep medicine to develop specific clinical practice guidelines and consensus tailored to nurse-delivered acupressure for sleep management.
In addition, future research could explore the development and efficacy of public digital acupressure training platforms to assist in self-administered acupressure; however, the integration of initial nurse guidance and periodic supervision remains crucial to ensuring the safety of patients’ self-administered acupressure and their long-term adherence to it.
Acupuncture: Caution Remains Warranted Regarding Nurse Operational Authority
In contrast to acupressure, acupuncture, as an invasive procedure, is subject to considerable regional variation in regulatory standards. In Brazil, nurses are authorized to perform acupuncture under Resolution No. 585/2018.68 In the US, states such as Arizona, Kentucky, and Washington include acupuncture within the scope-of-practice for APNs, contingent upon completion of at least 1905 hours of systematic training.69 The local Acupuncture Practice Acts also specifies that RNs and nurse practitioners are not eligible for reduced training requirements.69 In China and South Korea, acupuncture is legally restricted to licensed TC/KM practitioners, institutionalizing safety through rigorous licensure systems.21,22 Given these regulatory disparities, we maintain a cautious stance on nurses directly delivering acupuncture for sleep management. Korean scholars have noted that acupuncture-related traumatic adverse events outside Korea may stem from procedures performed by non-acupuncturists with varying training levels, including nurses, physicians, and physiotherapists.21 Therefore, before implementing task-shifting of acupuncture from acupuncturists to nurses, comprehensive evaluations of feasibility, safety, and effectiveness are needed, along with input from professional TC/KM practitioners.
In China, pilot programs in Anhui Province (Year 2018) and Shenzhen City (Year 2022) granted APNs limited prescribing authority.70 Drawing on this model, we propose that in the future, nurses might be allowed to perform limited acupuncture procedures under close supervision from licensed TCM practitioners and based on a clear TCM diagnosis and prescription. Such conditionally delegated authority could help delineate professional boundaries, reduce role ambiguity, and clarify the distinct contributions of each healthcare profession.
Conclusion
As the largest segment of the healthcare workforce with greater patient contact time than physicians in hospital settings, nurses are well positioned to supplement acupuncturists in delivering acupressure for managing patient-reported sleep impairments. Given the invasive nature of acupuncture and the potential safety risks associated with improper practice, the appropriateness of nurses performing acupuncture remains a matter of debate. While preliminary trials support the feasibility of this task-shifting model, significant methodological variations and inconsistent results highlight evidence gaps.
To advance nurse-led acupuncture and acupressure, we propose two key directions for research and policy: (1) For acupressure: rigorous large-scale RCTs, qualitative studies, and systematic reviews with meta-analyses are needed to objectively assess the effectiveness, treatment adherence, and patient satisfaction associated with nurse-led acupressure in sleep management. Additionally, the development of standardized training curricula, evaluation frameworks, and clinical practice guidelines is essential for supporting the implementation and broader dissemination of this innovative service delivery paradigm. (2) For acupuncture, comprehensive investigations into the feasibility of nurse-delivered acupuncture are warranted, considering the perspectives of nurses, patients, acupuncturists, and policymakers. Where consensus among stakeholders is reached, pilot programs involving limited nurse-administered acupuncture under the close supervision of licensed acupuncturists should be conducted and re-evaluated in accordance with national or regional health policies.
Abbreviations
APN(s), Advanced Practice Nurse(s); CBT, Cognitive-Behavioral Therapy; CBTi, Cognitive-Behavioral Therapy for Insomnia; CKD, Chronic Kidney Disease; ESRD, End-Stage Renal Disease; NHANES, National Health and Nutrition Examination Survey; PSQI, Pittsburgh Sleep Quality Index; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses; RCT(s), Randomized Controlled Trial(s); RN(s), Registered Nurse(s); SANRA, Scale for the Assessment of Narrative Review Articles; SOL, Sleep Onset Latency; TC/KM, Traditional Chinese/Korean Medicine; TST, Total Sleep Time; WASO, Wake After Sleep Onset.
Data Sharing Statement
Data availability is not applicable as no new data was generated for this paper.
Author Contributions
Fei-Yi Zhao: Conceptualization, Investigation, Formal analysis, Funding acquisition, Writing – original draft. Wen-Jing Zhang: Investigation, Writing – review & editing. Chin-Moi Chow: Formal analysis, Writing – review & editing. Yuan Xin Lee: Formal analysis, Writing – review & editing. Peijie Xu: Data curation, Writing – review & editing. Yuen-Shan Ho: Conceptualization, Formal analysis, Writing – review & editing. Qiang-Qiang Fu: Validation, Formal analysis, Writing – review & editing. Russell Conduit: Conceptualization, Project administration, Writing – review & editing. All authors gave final approval of the version to be published, agreed on the journal to which the article was submitted, and agreed to be accountable for all aspects of the work.
Funding
This work was supported by the Scientific Research Fund Project of Shanghai Sanda University [2024BSZX03] to FY-Z.
Disclosure
The authors declare no competing interests.
References
1. Chattu VK, Manzar MD, Kumary S, Burman D, Spence DW, Pandi-Perumal SR. The global problem of insufficient sleep and its serious public health implications. Healthcare. 2018;7(1):1. doi:10.3390/healthcare7010001
2. Meaklim H, Jackson ML, Bartlett D, et al. Sleep education for healthcare providers: addressing deficient sleep in Australia and New Zealand. Sleep Health. 2020;6(5):636–650. doi:10.1016/j.sleh.2020.01.012
3. Di H, Guo Y, Daghlas I, et al. Evaluation of sleep habits and disturbances among US Adults, 2017-2020. JAMA Network Open. 2022;5(11):e2240788. doi:10.1001/jamanetworkopen.2022.40788
4. Grandner MA, Jackson NJ, Pigeon WR, Gooneratne NS, Patel NP. State and regional prevalence of sleep disturbance and daytime fatigue. J Clin Sleep Med. 2012;8(1):77–86. doi:10.5664/jcsm.1668
5. Grandner MA, Jackson NJ, Pak VM, Gehrman PR. Sleep disturbance is associated with cardiovascular and metabolic disorders. J Sleep Res. 2012;21(4):427–2869.2011.00990.x. doi:10.1111/j.1365-2869.2011.00990.x
6. Sun X, Liu B, Liu S, et al. Sleep disturbance and psychiatric disorders: a bidirectional Mendelian randomisation study. Epidemiol Psychiatr Sci. 2022;31:e26. doi:10.1017/S2045796021000810
7. Bioulac S, Micoulaud-Franchi J-A, Arnaud M, et al. Risk of motor vehicle accidents related to sleepiness at the wheel: a systematic review and meta-analysis. Sleep. 2018;41(7). doi:10.1093/sleep/zsy075
8. Drake CL, Roehrs T, Roth T. Insomnia causes, consequences, and therapeutics: an overview. Depress Anxiety. 2003;18(4):163–176. doi:10.1002/da.10151
9. Riemann D, Espie CA, Altena E, et al. The European insomnia guideline: an update on the diagnosis and treatment of insomnia 2023. J Sleep Res. 2023;32(6):e14035. doi:10.1111/jsr.14035
10. Luyster FS, Chasens ER, Wasko MC, Dunbar-Jacob J. Sleep quality and functional disability in patients with rheumatoid arthritis. J Clin Sleep Med. 2011;7(1):49–55.
11. Tan LH, Chen PS, Chiang HY, et al. Insomnia and poor sleep in CKD: a systematic review and meta-analysis. Kidney Med. 2022;4(5):100458. doi:10.1016/j.xkme.2022
12. Hewlett S, Ambler N, Almeida C, et al. Self-management of fatigue in rheumatoid arthritis: a randomised controlled trial of group cognitive-behavioural therapy. Ann Rheum Dis. 2011;70(6):1060–1067. doi:10.1136/ard.2010.144691
13. Shareh H, Hasheminik M, Jamalinik M. Cognitive behavioural group therapy for insomnia (CBGT-I) in patients undergoing haemodialysis: a randomized clinical trial. Behav Cogn Psychother. 2022;50(6):559–574. doi:10.1017/S1352465822000364
14. Yoshinaga N, Tanoue H, Hayashi Y. Naturalistic outcome of nurse-led psychological therapy for mental disorders in routine outpatient care: a retrospective chart review. Arch Psychiatr Nurs. 2022;40:43–49. doi:10.1016/j.apnu.2022.04.008
15. Kyle SD, Siriwardena AN, Espie CA, et al. Clinical and cost-effectiveness of nurse-delivered sleep restriction therapy for insomnia in primary care (HABIT): a pragmatic, superiority, open-label, randomised controlled trial. Lancet. 2023;402(10406):975–987.doi:10.1016/S0140–6736(23)00683–9.
16. Chiu HY, Hsieh YJ, Tsai PS. Acupuncture to reduce sleep disturbances in perimenopausal and postmenopausal women: a systematic review and meta-analysis. Obstet Gynecol. 2016;127(3):507–515. doi:10.1097/AOG.0000000000001268
17. Tan JB, Wang T, Zhao I, Polotan MJ, Eliseeva S. An evidence-based somatic acupressure intervention protocol for managing the breast cancer fatigue-sleep disturbance-depression symptom cluster: development and validation following the medical research council framework. Int J Environ Res Public Health. 2022;19(19):11934. doi:10.3390/ijerph191911934
18. Zhao FY, Spencer SJ, Kennedy GA, et al. Acupuncture for primary insomnia: effectiveness, safety, mechanisms and recommendations for clinical practice. Sleep Med Rev. 2024;74:101892. doi:10.1016/j.smrv.2023.101892
19. Schlaeger JM, Gabzdyl EM, Bussell JL, et al. Acupuncture and acupressure in labor. J Midwifery Womens Health. 2017;62(1):12–28. doi:10.1111/jmwh.12545
20. Yue JH, Li XL, Huang DH, et al. How to improve safety in acupuncture clinical practice? Med Acupunct. 2025;37(4):292–298. doi:10.1089/acu.2024.0128
21. Kim SA, Lee JS, Kim TH, Lee S, Lee JD, Kang JW. The reporting quality of acupuncture-related traumatic adverse events: a systematic review of case studies in Korea. BMC Complement Med Ther. 2024;24(1):120. doi:10.1186/s12906-024-04421-5
22. Lim MY, Huang J, Zhao B, Ha L. Current status of acupuncture and moxibustion in China. Chin Med. 2015;10:12. doi:10.1186/s13020-015-0041-1
23. Kawai M, Yamashita H, Furuse N, et al. Current status of licensing and education of acupuncture and moxibustion for physicians and acupuncturists/moxibustionists in Japan. Med Acupunct. 2025;37(1):43–49. doi:10.1089/acu.2024.0095
24. Zhao FY, Conduit R, Kennedy GA, et al. Why some embrace and others hesitate? A behavioral analysis of insomnia sufferers’ engagement with acupuncture treatment. World J Psych. 2025;15(5):105802. doi:10.5498/wjp.v15.i5.105802
25. Fan AY, Wang DD, Ouyang H, et al. Acupuncture price in forty-one metropolitan regions in the United States: an out-of-pocket cost analysis based on OkCopay.com. J Integr Med. 2019;17(5):315–320. doi:10.1016/j.joim.2019.06.003
26. Bishop FL, Barlow F, Coghlan B, Lee P, Lewith GT. Patients as healthcare consumers in the public and private sectors: a qualitative study of acupuncture in the UK. BMC Health Serv Res. 2011;11:129. doi:10.1186/1472-6963-11-129
27. Zhang NM, Daly D, Terblanche M, et al. Doctors’ and nurses’ attitudes of acupuncture and acupressure use in perioperative care: an australian national survey. Pain Manag Nurs. 2022;23(6):800–810. doi:10.1016/j.pmn.2022.08.008
28. Reza H, Kian N, Pouresmail Z, Masood K, Sadat Seyed Bagher M, Cheraghi MA. The effect of acupressure on quality of sleep in Iranian elderly nursing home residents. Complement Ther Clin Pract. 2010;16(2):81–85. doi:10.1016/j.ctcp.2009.07.003
29. Lu MJ, Lin ST, Chen KM, Tsang HY, Su SF. Acupressure improves sleep quality of psychogeriatric inpatients. Nursing Research. 2013;62(2):130–137. doi:10.1097/NNR.0b013e3182781524
30. Lee EJ, Frazier SK. The efficacy of acupressure for symptom management: a systematic review. J Pain Symptom Manage. 2011;42(4):589–603. doi:10.1016/j.jpainsymman.2011.01.007
31. Türkmen H, Turfan E Ç. The effect of acupressure on labor pain and the duration of labor when applied to the SP6 point: randomized clinical trial. Jpn J Nurs Sci. 2020;17(1):e12256. doi:10.1111/jjns.12256
32. Gonçalves AD, Poli GG, Silva CM, Beleza AC, Liebano RE. Therapeutic resources used by physiotherapists for the relief of labor pain: a cross-sectional study. Revista Brasileira de Ginecologia e Obstetrícia. 2024;46:e–rbgo99. doi:10.61622/rbgo/2024rbgo99
33. Knupp HM, Esmail S, Warren S. The use of complementary and alternative medicine (CAM) by Canadian occupational therapists. Occup Ther Int. 2009;16(1):6–24. doi:10.1002/oti.262
34. Lee KC, Chao YC, Lin YP, Wang HC. Effectiveness of self-administered acupressure for family caregivers of advanced cancer patients with insomnia: a randomized controlled trial. Cancer Nurs. 2022;45(1):E1–E9. doi:10.1097/NCC.0000000000000870
35. Lei XF, Chen XL, Lin JX, Bao AF, Tao XC. Clinical study on acupoint massage in improving cognitive function and sleep quality of elderly patients with hypertension. J Acupunc Tuina Sci. 2015;13(3):175–179. doi:10.1007/s11726-015-0845-7
36. Baethge C, Goldbeck-Wood S, Mertens S. SANRA-a scale for the quality assessment of narrative review articles. Res Integr Peer Rev. 2019;4:5. doi:10.1186/s41073-019-0064-8
37. Martínez-González NA, Djalali S, Tandjung R, et al. Substitution of physicians by nurses in primary care: a systematic review and meta-analysis. BMC Health Serv Res. 2014;14:214. doi:10.1186/1472-6963-14-214
38. Maier CB, Aiken LH. Task shifting from physicians to nurses in primary care in 39 countries: a cross-country comparative study. Eur J Public Health. 2016;26(6):927–934. doi:10.1093/eurpub/ckw098
39. Laurant M, van der Biezen M, Wijers N, Watananirun K, Kontopantelis E, van Vught AJ. Nurses as substitutes for doctors in primary care. Cochrane Database Syst Rev. 2018;7(7):CD001271. doi:10.1002/14651858.CD001271.pub3
40. Aurizki GE, Wilson I. Nurse-led task-shifting strategies to substitute for mental health specialists in primary care: a systematic review. Int J Nurs Pract. 2022;28(5):e13046. doi:10.1111/ijn.13046
41. Bousfield APS, Padilha MI, Bellaguarda MLR, et al. Nursing process as a potentializer of acupuncture practice. Escola Anna Nery. 2021;25:e20200148. doi:10.1590/2177-9465-EAN-2020-0148
42. Waltman S, Hall BC, McFarr LM, Beck AT, Creed TA. In-session stuck points and pitfalls of community clinicians learning CBT: qualitative investigation. Cognit Behav Pract. 2017;24(2):256–267. doi:10.1016/j.cbpra.2016.04.002
43. Wang L, Wu F, Zhao L, et al. Patterns of traditional Chinese medicine diagnosis in thermal laser acupuncture treatment of knee osteoarthritis. Evid Based Complement Alternat Med. 2013;2013:870305. doi:10.1155/2013/870305
44. Landgren K, Strand AS, Ekelin M, Ahlström G. Ear acupuncture in psychiatric care from the health care professionals’ perspective: a phenomenographic analysis. Issues Ment Health Nurs. 2019;40(2):166–175. doi:10.1080/01612840.2018.1534908
45. de Mello Pereira RD, Alvim NAT. Acupuncture to intervene in nursing diagnosis: assessment of nursing experts. Escola Anna Nery Revista de Enfermagem. 2025;20(4). doi:10.5935/1414-8145.20160084
46. Zhao FY, Xu P, Kennedy GA, et al. Home-based self-management using traditional Chinese medicine techniques: empowerment and risks in breast cancer survivors’ fulfillment of health-deviation self-care requisites. J Cancer Surviv. 2025. doi:10.1007/s11764-025-01808-2
47. Wang R, Zhou C, Wu Y, et al. Patient empowerment and self-management behaviour of chronic disease patients: a moderated mediation model of self-efficacy and health locus of control. J Adv Nurs. 2022;78(4):1055–1065. doi:10.1111/jan.15077
48. King HC, Spence DL, Hickey AH, Sargent P, Elesh R, Connelly CD. Auricular acupuncture for sleep disturbance in veterans with post-traumatic stress disorder: a feasibility study. Mil Med. 2015;180(5):582–590.doi:10.7205/MILMED–D–14–00451.
49. Ward U, Nilsson UG. Acupuncture for postoperative pain in day surgery patients undergoing arthroscopic shoulder surgery. Clin Nurs Res. 2013;22(1):130–136. doi:10.1177/1054773812454136
50. Olsson A, Landgren K. Getting well is more than gaining weight - patients’ experiences of a treatment program for anorexia nervosa including ear acupuncture. Issues Ment Health Nurs. 2020;41(4):328–338. doi:10.1080/01612840.2019.1663567
51. Haddad ML, Medeiros M, Marcon SS. Sleep quality of obese workers of a teaching hospital: acupuncture as a complementary therapy. Rev Esc Enferm USP. 2012;46(1):82–88. doi:10.1590/s0080-62342012000100011
52. Salajegheh Z, Harorani M, Shahrodi M, et al. Effects of acupressure on sleep quality and anxiety of patients with second- or third-degree burns: a randomized sham-controlled trial. BMC Complement Med Ther. 2024;24(1):5. doi:10.1186/s12906-023-04292-2
53. Liu XR, Rana N, Wong NS, James C, Lu J, Xu X. The effect of auricular acupressure on sleep disturbance among patients with leukemia: a feasibility study. Holist Nurs Pract. 2020;34(2):103–112. doi:10.1097/HNP.0000000000000372
54. Tsay SL, Chen ML. Acupressure and quality of sleep in patients with end-stage renal disease--a randomized controlled trial. Int J Nurs Stud. 2003;40(1):1–7. doi:10.1016/s0020-7489(02)00019-6
55. Lim Y, Park H. The effects of auricular acupressure on low back pain, neuropathy and sleep in patients with persistent spinal pain syndrome (PSPS): a single-blind, randomized placebo-controlled trial. Int J Environ Res Public Health. 2023;20(3):1705. doi:10.3390/ijerph20031705
56. Liu Q, Wang C, Wang Y, et al. Mindfulness-based stress reduction with acupressure for sleep quality in breast cancer patients with insomnia undergoing chemotherapy: a randomized controlled trial. Eur J Oncol Nurs. 2022;61:102219. doi:10.1016/j.ejon.2022.102219
57. Kuo HC, Tsao Y, Tu HY, Dai ZH, Creedy DK. Pilot randomized controlled trial of auricular point acupressure for sleep disturbances in women with ovarian cancer. Res Nurs Health. 2018;41(5):469–479. doi:10.1002/nur.21885
58. King CH, Moore LC, Spence CD. Exploring self-reported benefits of auricular acupuncture among veterans with posttraumatic stress disorder. J Holist Nurs. 2016;34(3):291–299. doi:10.1177/0898010115610050
59. Zhao FY, Zheng Z, Fu QQ, et al. Acupuncture for comorbid depression and insomnia in perimenopause: a feasibility patient-assessor-blinded, randomized, and sham-controlled clinical trial. Front Public Health. 2023;11:1120567. doi:10.3389/fpubh.2023.1120567
60. Zang S, Chen Y, Chen H, Shi H, Zhou L. Effects of acupuncture on the brain in primary insomnia: a coordinate-based meta-analysis of fMRI studies. Front Neurol. 2023;14:1180393. doi:10.3389/fneur.2023.1180393
61. Waits A, Tang YR, Cheng HM, Tai CJ, Chien LY. Acupressure effect on sleep quality: a systematic review and meta-analysis. Sleep Med Rev. 2018;37:24–34. doi:10.1016/j.smrv.2016.12.004
62. Li YW, Li W, Wang ST, et al. The autonomic nervous system: a potential link to the efficacy of acupuncture. Front Neurosci. 2022;16:1038945. doi:10.3389/fnins.2022.1038945
63. Bang YY, Park H. Effects of auricular acupressure on the quality of sleep and anxiety in patients undergoing cardiac surgery: a single-blind, randomized controlled trial. Appl Nurs Res. 2020;53:151269. doi:10.1016/j.apnr.2020.151269
64. Guo X, Yang W, Wang Y, Ma S, Lu Q, Wang H. Study on acupuncture improving sleep deprivation comorbid with cognitive dysfunction based on rs-fMRI: a protocol for systematic review and meta-analysis. Medicine. 2023;102(14):e33490. doi:10.1097/MD.0000000000033490
65. Asgari F, Aghajani M, Nia SM. The effect of self-auriculotherapy on the severity of restless leg syndrome, sleep quality, and fatigue in hemodialysis patients: a randomized controlled clinical trial. Explore. 2025;21(5):103205. doi:10.1016/j.explore.2025.103205
66. Pu X, Malik G, Murray C. Nurses’ experiences and perceptions of running nurse-led clinics: a scoping review. Int J Nurs Pract. 2024;30(6):e13285. doi:10.1111/ijn.13285
67. Zhao FY, Kennedy GA, Gilbert J, et al. Career considerations in nurse-led traditional Chinese medicine clinics: a two-center qualitative study. Risk Manag Healthc Policy. 2024;17:1533–1546. doi:10.2147/RMHP.S465663
68. Melo GAA, Aguiar LL, Silva RA, et al. Effects of acupuncture in patients with chronic kidney disease: a systematic review. Revista Brasileira de Enfermagem. 2020;73(4):e20180784. doi:10.1590/0034-7167-2018-0784
69. Bleck RR, Gold MA, Westhoff CL. Training hour requirements to provide acupuncture in the United States. Acupunct Med. 2021;39(4):327–333. doi:10.1177/0964528420939576
70. Wu Y, Liu J, Fornah L, Yan Z, Meng L, Wu S. The attitudes of physicians toward nurse prescribing rights: a cross-sectional study. BMC Nurs. 2025;24(1):113. doi:10.1186/s12912-025-02756-z
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Assessment of Lumbar Spinal Stenosis as a Risk Factor for Development of Sleep Disorder: The Locomotive Syndrome and Health Outcome in Aizu Cohort Study (LOHAS)
Kobayashi H, Sekiguchi M, Otani K, Ono R, Nikaido T, Watanabe K, Kato K, Kobayashi Y, Yabuki S, Konno SI, Matsumoto Y
International Journal of General Medicine 2023, 16:5417-5424
Published Date: 22 November 2023
Relationship Between Insomnia and Continued Outpatient Treatment in Psychiatric Patients
Kamata Y, Takashio O, Sato R, Kawai H, Ishii H, Aoyagi K, Tomita A, Toda S, Iwanami A
Neuropsychiatric Disease and Treatment 2024, 20:697-723
Published Date: 27 March 2024
From Needles to Photons: Clinical Efficacy, Safety, and Mechanistic Insights of Laser Acupuncture in Insomnia Management
Zhao FY, Zhang WJ, Chow CM, Xu P, Yue LP, Ho YS, Fu QQ, Conduit R
Nature and Science of Sleep 2025, 17:3105-3114
Published Date: 2 December 2025
Auricular Acupoint Selection Patterns for Knee Osteoarthritis Pain Relief: A Systematic Review and Data Mining Analysis
Li Y, Zhang X, Liu M, Wang Y, Shen Z, Shan Y
Journal of Pain Research 2026, 19:568124
Published Date: 21 January 2026