Back to Journals » Journal of Pain Research » Volume 19
Auricular Acupoint Selection Patterns for Knee Osteoarthritis Pain Relief: A Systematic Review and Data Mining Analysis
Authors Li Y ![]() , Zhang X, Liu M, Wang Y, Shen Z, Shan Y
, Zhang X, Liu M, Wang Y, Shen Z, Shan Y ![]()
Received 17 September 2025
Accepted for publication 13 January 2026
Published 21 January 2026 Volume 2026:19 568124
DOI https://doi.org/10.2147/JPR.S568124
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Houman Danesh
Yawen Li,1,2 Xinyue Zhang,2 Mengnan Liu,1,2 Yin Wang,2 Zhongming Shen,1 Yawei Shan1,2
1Department of Nursing, Guanghua Hospital Affiliated to Shanghai University of Traditional Chinese Medicine, Shanghai, People’s Republic of China; 2School of Nursing, Shanghai University of Traditional Chinese Medicine, Shanghai, People’s Republic of China
Correspondence: Yawei Shan, Department of Nursing, Guanghua Hospital Affiliated to Shanghai University of Traditional Chinese Medicine, No. 1508, Yan’an West Road, Shanghai, 200050, People’s Republic of China, Tel +86 17601260156, Email [email protected] Zhongming Shen, Department of Nursing, Guanghua Hospital Affiliated to Shanghai University of Traditional Chinese Medicine, No. 1508, Yan’an West Road, Shanghai, 200050, People’s Republic of China, Tel +86 13918892898, Email [email protected]
Objective: To systematically evaluate randomized controlled trials of auricular therapy for knee osteoarthritis pain and to explore acupoint selection patterns using data mining techniques.
Methods: Eleven Chinese and English databases were searched from inception to September 1, 2025. Eligible randomized controlled trials were screened and assessed for methodological quality. Descriptive statistics, frequency analysis, association rule mining, and hierarchical cluster analysis were applied to identify commonly used auricular points and their combinations.
Results: Thirty-six studies involving 3,105 participants were included. Study quality was moderate, with frequent shortcomings in blinding and allocation reporting. The most frequently used acupoints were Shenmen (TF4), Xi (AH4), Jiaogan (AH6a), Pizhixia (AT4), Gan (CO12), and Shen (CO10). Association rule analysis showed Shenmen (TF4)–Pizhixia (AT4) as the most frequent co-occurring pair (support = 97.22%), while Neifenmi (CO18)–Shenshangxian (TG2p) and Shenmen (TF4)–Shenshangxian (TG2p) exhibited the strongest association (lift = 3.15). Cluster analysis identified three synergistic groups: Cluster 1: Shenmen (TF4), Xi (AH4), Jiaogan (AH6a), and Pizhixia (AT4), linked to nerve regulation; Cluster 2: Gan (CO12) and Shen (CO10), associated with zang-fu organ function; and Cluster 3: Yidan (CO11), Xin (CO15), Fei (CO14), Pi (CO13), and Sanjiao (CO17), functioning as adjunctive regulators.
Conclusion: Auricular therapy for knee osteoarthritis pain relief shows promising patterns in acupoint selection that align with both Traditional Chinese Medicine and neurophysiological mechanisms. Despite encouraging results, interpretation should be cautious due to methodological limitations, protocol heterogeneity, and the exploratory nature of data mining. Future research should include rigorously designed, preregistered RCTs with standardized intervention protocols and transparent reporting to validate these findings and evaluate clinical effectiveness.
Keywords: osteoarthritis of knee, auricular therapy, acupoint selection, traditional Chinese medicine, pain management, systematic review, data mining
Introduction
Knee osteoarthritis (KOA), categorized as “Knee Bi” or “Bone Bi” in Traditional Chinese Medicine (TCM), a degenerative whole-joint disorder affecting not only the articular cartilage but also all joint tissues, including subchondral bone, menisci, synovium, ligaments, and the infrapatellar fat pad.1–3 Globally, KOA is the most common form of osteoarthritis, with an estimated 595 million individuals affected by osteoarthritis in 2020.4 The prevalence of KOA is especially high among individuals aged over 40, and it is projected to increase by 74.9% by 2050.4 Key risk factors include aging, obesity, joint injury, genetic predisposition, and mechanical overload.5 As a predominant symptom, chronic knee pain substantially impairs both physical functionality and psychological well-being, profoundly compromising patients’ quality of life. Approximately 25% of adults over 55 experience recurrent knee pain annually, with 15% suffering from activity limitations due to pain.6,7
Conventional treatment approaches for KOA-related pain include both pharmacological and non-pharmacological strategies. Nonsteroidal anti-inflammatory drugs (NSAIDs) remain a cornerstone of pharmacologic therapy, offering effective pain relief and anti-inflammatory effects.8,9 However, their use is often limited by adverse effects such as gastrointestinal discomfort, hepatic and renal impairment, and elevated cardiovascular risks.10,11 For patients with comorbidities like peptic ulcers or liver dysfunction, the risks of pharmacological treatment may outweigh the benefits, prompting the need for safer, effective, and integrative alternatives.12
Auricular therapy, an integral component of TCM, is based on the principle that the ear reflects the body’s internal organs through a network of meridians. As noted in the “Ling Shu Kou Wen”, the ear is viewed as the convergence site of the Zong Mai (major meridians), forming the theoretical foundation of auricular therapy.13 This modality includes techniques such as filiform needle acupuncture, pellet pressure, electroacupuncture, and massage. It is characterized by simplicity, safety, and convenience, and is widely adopted in clinical practice, particularly in pain management, substance addiction, insomnia, and anxiety.14,15 Contemporary research has revealed that auricular point stimulation can modulate spinal gate control mechanisms and central analgesic pathways, promoting the release of endogenous opioids and enhancing pain thresholds.13,16
A growing body of primary research supports the efficacy of auricular therapy in relieving KOA-associated pain. For instance, randomized controlled trials (RCTs) have shown that auricular therapy significantly reduces knee pain and improves function in KOA patients.17,18 Moreover, systematic reviews have confirmed the analgesic benefits of auricular therapy for musculoskeletal conditions.19,20 However, these reviews tend to focus on efficacy and mechanisms of action rather than on patterns of acupoint selection, which remains heterogeneous across studies. Variability in auricular point selection often based on practitioners’ experience or patient-reported pain locations can lead to inconsistent clinical outcomes.15 To date, there has been no comprehensive analysis aimed at identifying the most commonly used and potentially effective auricular points for KOA pain management.
The rationale for using auricular acupoints in KOA is grounded in both TCM theory and modern neurophysiology. According to TCM holographic somatotopic mapping, the ear reflects the entire body,15 with the knee region specifically corresponding to the “Xi” area (AH4), enabling targeted modulation of knee-related pathology. Furthermore, KOA is categorized as “Bi Zheng” (painful obstruction syndrome), and acupoint selection aims not only to alleviate pain (for instance, via Shenmen (TF4)) but also to address the root cause by regulating zang-fu organ function (for instance, using Shen (CO10) to tonify the Kidney, which governs bones). From a contemporary biomedical perspective, the external ear is richly innervated by branches of the vagus, trigeminal, facial, and glossopharyngeal nerves, and stimulation of these points can modulate nociceptive signaling via spinal and supraspinal pathways, engaging mechanisms such as gate control and endogenous opioid release.13,16 The convergence of these traditional and neurophysiological mechanisms provides a theoretical basis for using auricular acupoints to alleviate KOA-related pain and improve function.
This review therefore seeks to address this gap by applying data mining techniques to systematically identify and characterize patterns of auricular acupoint selection for KOA pain relief in published clinical studies. Our primary objectives are to (1) identify the most frequently used auricular acupoints, (2) analyze their combination patterns and synergistic relationships, and (3) explore functional groupings of acupoints through cluster analysis. This descriptive mapping of current practices aims to inform the development of standardized, evidence-informed protocols for future research.
Materials and Methods
Study Design and Registration Status
The methodology of this systematic review was aligned with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) reporting guidelines.21 As an exploratory hypothesis-generating study without planned meta-analyses of clinical outcomes, prospective registration was not pursued in databases such as PROSPERO. Nonetheless, all methodological steps, including literature search strategies, inclusion/exclusion criteria, data extraction, and analysis plans, were prospectively documented during the review conduct and are detailed within this article to ensure transparency.
Eligibility Criteria
Inclusion Criteria: (1) Participants (P): Participants had a confirmed diagnosis of KOA, consistent with both Western and TCM diagnostic criteria.1,10 (2) Intervention (I): The intervention involved auricular therapy—either as a standalone approach or in combination with other therapies—adhering to the principles outlined in Auricular Diagnosis and Therapy.22 (3) Comparison (C): Control groups receiving sham auricular therapy, no intervention, wait-list care, or conventional standard care. (4) Outcomes (O): The primary outcome was pain and assessments employed validated instruments such as the Visual Analogue Scale (VAS) and the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC). (5) Study design (s): Study design was restricted to randomized controlled trials (RCTs).
Exclusion Criteria: (1) Participants had undergone knee replacement surgery, presented with acute KOA due to trauma or strenuous activity, or had other significant pain disorders. (2) The outcome is unclear or literature on the ineffectiveness of auricular acupuncture. (3) The intervention protocol for auricular therapy was inadequately described. (4) Studies not published in either Chinese or English. (5) Duplicate publications, in which case the most recent or comprehensive version was retained.
Search Strategy
A comprehensive literature search was conducted in the following databases from inception through September 1, 2025: Chinese National Knowledge Infrastructure (CNKI, https://www.cnki.net), Wanfang Data Knowledge Service Platform (Wanfang, http://www.wanfangdata.com.cn), Vip Journal Integration Platform (VIP, http://qikan.cqvip.com/), China Biomedical Literature Database (SinoMed, http://www.sinomed.ac.cn/), Chinese Medical Association Publishing House (CMAPH, http://www.yiigle.com/), China TCM Database (http://cintmed.cintcm.com/cintmed/main.html), PubMed, Web of Science, Embase, Scopus, Cochrane Library, and CINAHL.
The search strategy combined subject headings and free-text terms related to KOA and auricular therapy. The keywords used were: (“knee osteoarthritis” OR “knee arthritis” OR “gonarthritis” OR “arthritic knee”) AND (“auricular therapy” OR “auricular acupressure” OR “auricular seed” OR “auricular point sticking” OR “magnetic beads auricular point” OR “ear acupuncture”). Search terms were adapted to suit the syntax of each database. A sample PubMed search strategy is provided in Supplementary Table 1.
Study Selection
All identified citations were imported into EndNote 21.0 for deduplication. Two reviewers independently screened titles and abstracts according to the eligibility criteria. Full texts of potentially relevant studies were retrieved and evaluated in detail. Discrepancies were resolved through discussion, and if needed, a third reviewer provided arbitration.
Data Extraction
Data were extracted independently by two reviewers using a standardized Excel 2016 form. Extracted items included: study title, first author, publication year, auricular point names, syndrome classification, intervention details (experimental and control groups), and outcome measures.
Auricular point names were standardized according to the Nomenclature and Location of Auricular Points,23 and syndrome classifications followed the 2023 Guidelines for Integrated TCM-WM Diagnosis and Treatment of KOA.1,24 Data consistency and accuracy were confirmed via a double-checking process.
Quality Assessment
The risk of bias for each included RCT was independently assessed by two reviewers using the Cochrane Risk of Bias 2.0 (ROB 2.0) tool, in accordance with the Cochrane Handbook for Systematic Reviews of Interventions.25 Any disagreements were resolved through discussion with a third reviewer.
Data Analysis
Data Preparation and Construction
A structured dataset was constructed for data mining based on the acupoint prescriptions extracted from each included study. Acupoint Coding by Excel 2016, and “co-occurrence” was defined as two or more acupoints being used together within the same intervention arm of a single study. Each unique study intervention arm was treated as one transaction or case in the dataset. Then the data was organized into a binary matrix where each row represented a study intervention arm, and each column represented a specific auricular acupoint. A value of “1” indicated the presence of that acupoint in the prescription for that particular study arm, while a value of “0” indicated its absence. This matrix served as the foundational input for all subsequent analyses.
Association Rule Mining
Association rule mining was performed using the Apriori algorithm within IBM SPSS Modeler 18.0 to identify significant co-occurrence patterns among auricular acupoints and set a minimum support threshold of >30% and a minimum confidence of ≥80%. Rules with a lift (lift) <1 were excluded. The choice of algorithm parameters was based on both statistical considerations and clinical interpretability: (1) Support (>30%): This threshold was set to ensure that the identified acupoint combinations appeared in a sufficiently large proportion of the included studies, reflecting highly prevalent and stable patterns of clinical practice rather than occasional or potentially random occurrences. (2) Confidence (≥80%): This high threshold was chosen to ensure that the generated association rules were highly reliable. A confidence of ≥80% indicates that when the antecedent acupoint was used, the consequent acupoint was also used in at least 80% of those cases, suggesting a strong predictive relationship and clinical co-application. (3) Lift (>1): This metric measures the degree of dependence between the antecedent and consequent. A lift value greater than 1 indicates that the two acupoints are positively correlated and co-occur more frequently than would be expected if they were independent. Rules with lift <1, indicating negative or neutral correlations, were excluded as non-meaningful.
These parameter settings collectively ensure that the reported rules are both frequent (high support), reliable (high confidence), and non-random (lift >1), providing clinically relevant and robust insights into acupoint selection patterns. Rules of the form “Antecedent-Consequent” were generated. Only rules passing all the above thresholds were considered statistically meaningful and clinically relevant for interpretation. Due to the exploratory nature of pattern discovery and the lack of built-in multiple comparison correction functionality in SPSS Modeler, the initial analysis employed support, confidence, and lift metrics to identify potential patterns. To rigorously control the false discovery rate (FDR), the list of all generated rules and their associated metrics were exported. The Benjamini-Hochberg procedure was then applied externally using R 4.4.2 to adjust the p-values derived from the confidence metrics, with an FDR threshold set at q < 0.05. A visual network diagram was generated to display the interrelationships among frequently co-occurring acupoints.
Cluster Analysis
Hierarchical cluster analysis (HCA) was performed using IBM SPSS Statistics V27.0 to group acupoints based on their co-occurrence patterns across studies. The squared Euclidean distance was used as the distance metric to quantify the dissimilarity between acupoints. The between-groups linkage method (average linkage) was employed to define the distance between clusters. The final number of clusters was determined by examining the dendrogram and the agglomeration schedule coefficients to identify a meaningful stopping point that yielded clinically interpretable groups. And the cluster solution was selected as it provided clear differentiation and alignment with TCM theory.
Results
Characteristics and Quality of Included Studies
A total of 299 studies were initially identified through systematic searches. After removing duplicates and applying the inclusion and exclusion criteria, 36 RCTs were included in the final analysis.18,26–60 The study selection process is illustrated in Figure 1, and the basic characteristics of the included studies are summarized in Supplement Table 2.
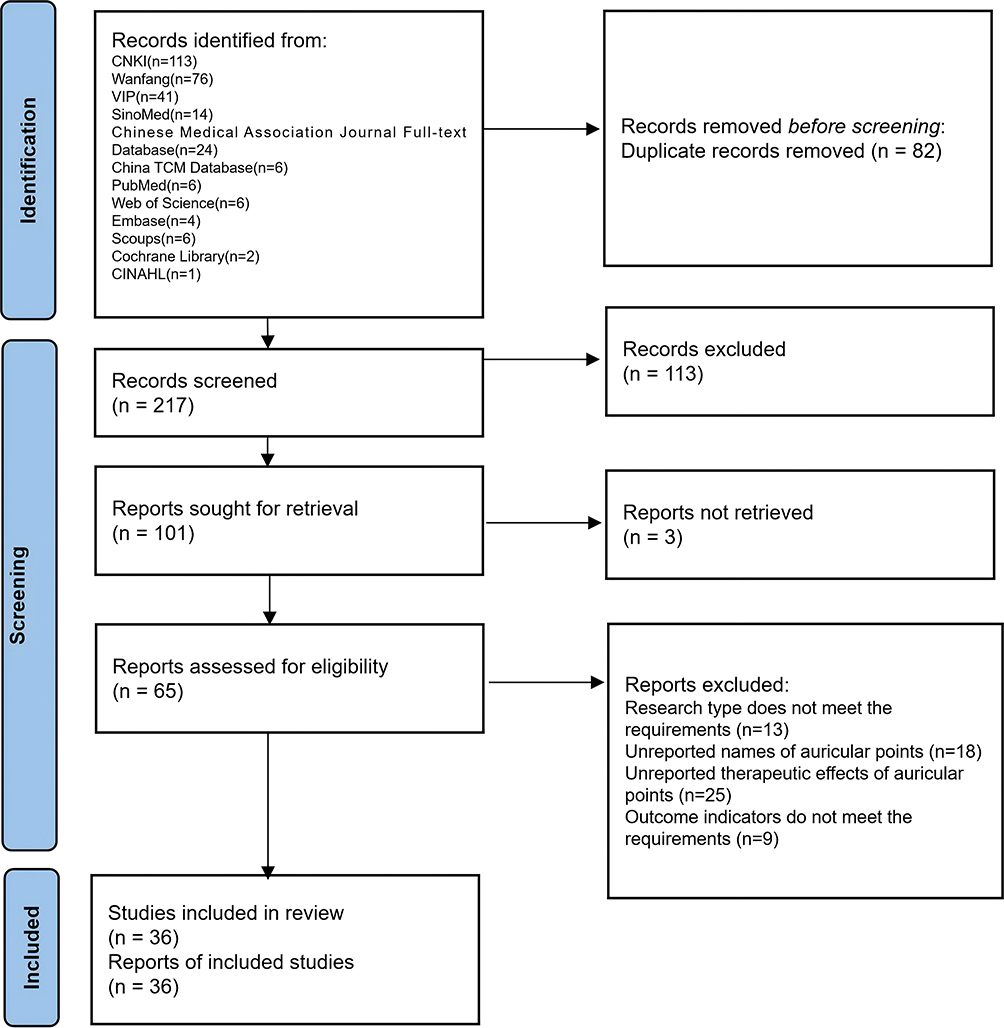 |
Figure 1 PRISMA flow diagram identification of studies via databases and registers to show the results of the searches. |
Among the 36 included studies, most reported the use of random allocation but lacked detailed descriptions of the randomization procedures (30 of 36). Due to the nature of auricular acupuncture interventions, blinding of participants and practitioners was generally not feasible. While data completeness was acceptable in most studies, none explicitly reported blinding of outcome assessors, potentially increasing the risk of detection bias. The risk of bias assessment for each study is presented in Supplement Figures 1 and 2, using the Cochrane ROB 2.0 tool.
Intervention Characteristics
Auricular therapy was the primary intervention in all 36 studies. Of these, 31 studies incorporated combination therapies, such as moxibustion therapy, external application of Chinese herbs, tuina (massotherapy), or oral TCM formulations (Table 1). Among these, moxibustion combined with auricular therapy was the most commonly reported protocol.
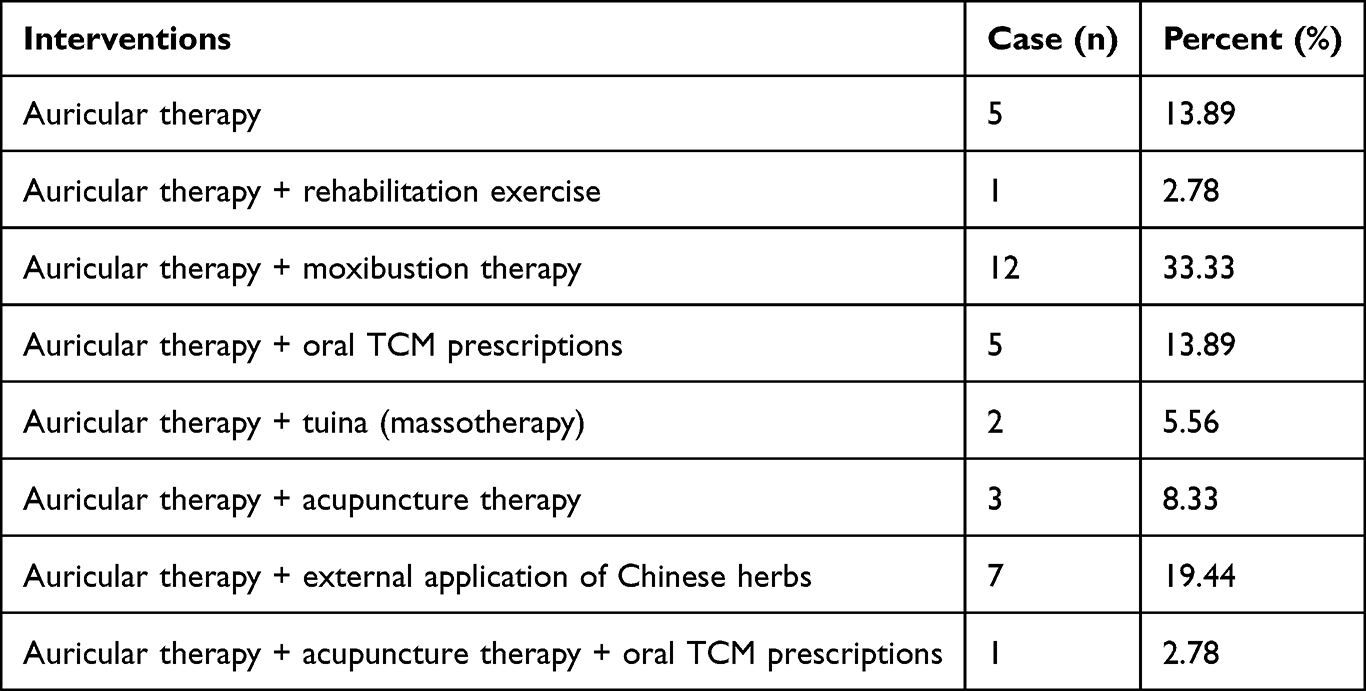 |
Table 1 Intervention Measures of Auricular Therapy for Alleviating Pain in Patients with Knee Osteoarthritis (n=36) |
Syndrome Differentiation and Common Auricular Acupoints
Of the included studies, 19 (52.78%) reported syndrome classification based on the 2023 edition of the Guidelines for Integrated TCM and Western Medicine Diagnosis and Treatment of Knee Osteoarthritis. Excess syndromes were more prevalent (13 studies, 36.11%), with damp-cold obstruction being the most frequent (12 studies, 33.33%). Deficiency syndromes were identified in 6 studies (16.66%), including liver-kidney deficiency (3 studies, 8.33%) and qi-blood deficiency (3 studies, 8.33%). Commonly used auricular points for all studies included and each syndrome type are detailed in Figure 2 and Supplement Table 3 for more details in the figure.
 |
Figure 2 Schematic diagrams of commonly used auricular points across all included studies and by syndrome type. (a) The distribution and frequency of auricular acupoints in auricular therapy to alleviate pain in patients with KOA. (b) The distribution and frequency of auricular acupoints in KOA with Dampness-cold obstruction syndrome. (c) The distribution and frequency of auricular acupoints in KOA with Dampness-heat obstruction syndrome. (d) The distribution and frequency of auricular acupoints in KOA with Deficiency of liver and kidney. (e) The distribution and frequency of auricular acupoints in KOA with Qi-blood weakness syndrome. The red triangular indicator represents the sympathetic point, which is not directly visible in the frontal view but is located on the inner side of the ear, highlighting the importance of a comprehensive examination of the ear’s anatomy for accurate point identification. The frequency data for each acupoint is presented in Supplement Table 3. Notes: (I) Frontal view of auricular zones and point locations. II. Inner side view of auricular zones and point locations. The embedded table provides the occurrence frequency of each acupoint. Adapted from Reference.23 Each acupoint is identified by a unique combination of letters and numbers or letters and subscripts, which correspond to specific regions and locations on the ear. |
Association Rule Analysis of Auricular Acupoint Combinations
Association rule mining was conducted to uncover significant acupoint partnerships. As detailed in the Methods section, we employed stringent parameters (support >30%, confidence ≥80%, lift >1) to identify robust and clinically prevalent combinations. The analysis included second- to sixth-order rules derived from the 36 studies. A total of 147 valid rules were generated. (1) The rule with the highest support was Shenmen (TF4)–Pizhixia (AT4) (support=97.22%). (2) The rule with the highest lift were Neifenmi (CO18)–Shenshangxian (TG2 p) and Neifenmi (CO18) and Shenmen (TF4)–Shenshangxian (TG2 p) (lift=3.15); (3) 72 rules demonstrated 100% confidence.
The q-value (the Benjamini-Hochberg procedure applied to adjust the p-values derived from the confidence metrics) of 46 rules, after being corrected by FDR, are less than 0.05 (listed in Supplement Table 4). Frequently observed combinations included: (1) Six-point set: Jiaogan (AH6 a), Gan (CO12), Pizhixia (AT4), Xi (AH4), Shenmen (TF4)––Shen (CO10) (case=11, support=30.56%, confidence=100.00%, lift=1.57, q<0.001); (2) Five-point set: Gan (CO12), Pizhixia (AT4), Xi (AH4), Shenmen (TF4)–Shen (CO10) (case=14, support=38.59%, confidence=100.00%, lift=1.57, q<0.001); (3) Four-point set: Gan (CO12), Xi (AH4), Shenmen (TF4)–Shen (CO10) (case=19, support=52.78%, confidence=100.00%, lift=1.09, q<0.001); (4) Three-point set: Pizhixia (AT4), Xi (AH4)–Shenmen (TF4) (case=23, support=63.89%, confidence=100.00%, lift=1.03, q<0.001); (5) Two-point set: Shenmen (TF4)–Pizhixia (AT4) (case=28, support=77.78%, confidence=100.00%, lift=1.03, q<0.001). The network of point selection is illustrated in Figure 3.
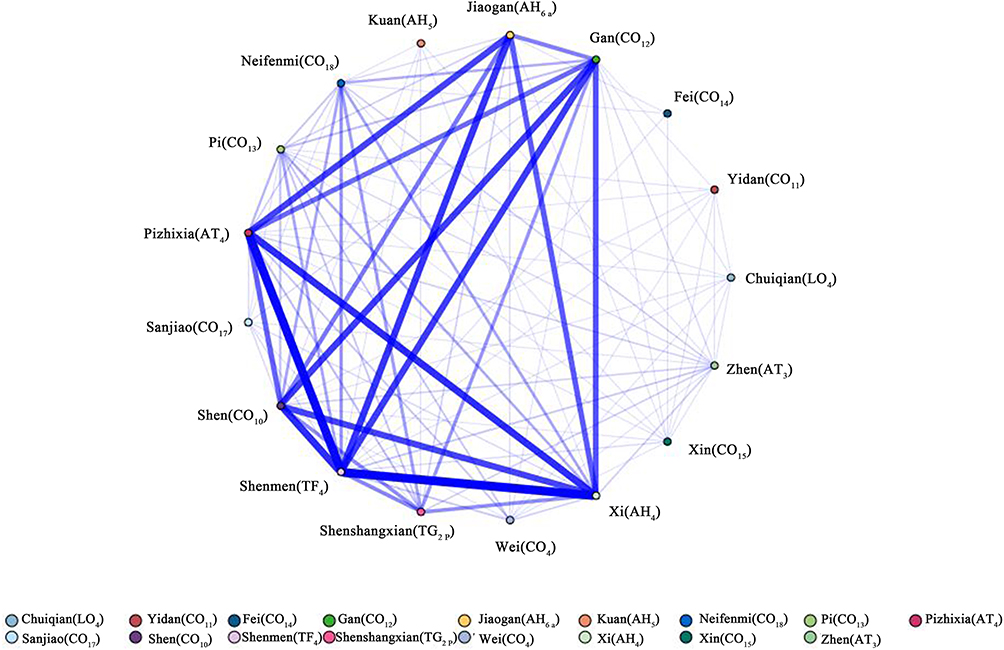 |
Figure 3 Network relationship diagram of auricular acupoint selection for pain relief in patients with knee osteoarthritis. Notes: The thickness of the line indicates the strength of the correlation between the two points; Each acupoint is identified by a unique combination of letters and numbers or letters and subscripts, which correspond to specific regions and locations on the ear. |
Cluster Analysis of Auricular Acupoints
A hierarchical cluster analysis was performed using SPSS Statistics 27.0 to categorize the 17 acupoints based on similarity. The resulting dendrogram (Figure 4) demonstrated three distinct clusters with good intra-cluster similarity and inter-cluster dispersion, consistent with clinical practice. The clusters were: (1) Cluster 1: Shenmen (TF4), Xi (AH4), Pizhixia (AT4), Jiaogan (AH6a); (2) Cluster 2: Gan (CO12), Shen (CO10); (3) Cluster 3: Chuiqian (LO4), Yidan (CO11), Xin (CO15), Fei (CO14), Kuan (AH5), Sanjiao (CO17), Zhen (AT3), Pi (CO13), Wei (CO4), Neifenmi (CO18), Shenshangxian (TG2 p).
 |
Figure 4 Auricular acupoint clustering dendrogram of auricular therapy for pain relief in patients with knee osteoarthritis. Notes: The red line in the figure represents the clustering divided at a distance scale of 12.5. Each acupoint is identified by a unique combination of letters and numbers or letters and subscripts, which correspond to specific regions and locations on the ear. |
Discussion
Key Findings
This review included 36 clinical studies on auricular acupoint therapy for KOA pain relief. The analysis revealed the following key findings: (1) High frequency of combined interventions: Most studies (31/36) applied auricular acupoint therapy in combination with moxibustion, external application of Chinese herbs, tuina (massotherapy), or oral TCM prescriptions. Among them, moxibustion was the most common adjunctive therapy. (2) Dominance of specific auricular acupoints: Shenmen (TF4), Xi (AH4), Pizhixia (AT4), Jiaogan (AH6 a), Shen (CO10), and Gan (CO12) were the top six most frequently used acupoints. (3) Syndrome differentiation-based application: Nearly half of the studies adopted syndrome differentiation per the “Guidelines for Integrated TCM and Western Medicine Diagnosis and Treatment of KOA (2023)”.24 The dampness-cold obstruction syndrome was the most common type. (4) Association rule and cluster analysis: The Shenmen (TF4)–Pizhixia (AT4) pair had the strongest support. Cluster analysis further grouped auricular points into three functional categories reflecting their synergistic roles in pain relief and organ modulation.
Status and Recommendations for Primary Study Design
Although 36 studies met the inclusion criteria, the overall methodological quality remains suboptimal. Randomization was poorly described, and no study implemented blinding for outcome assessors, which increases the risk of detection and reporting bias. These limitations are consistent with previous systematic reviews of acupuncture or auricular therapies.10,22 To improve future research quality, this study recommends: (1) Transparent randomization procedures: Clear documentation of random sequence generation and allocation concealment should be included. (2) Blinding of outcome assessors: While patient blinding is challenging in auricular therapy, assessor blinding remains feasible and important. (2) Use of standardized outcome measures: Pain scales, functional indices (for example WOMAC), and biomarkers should be consistently reported. The findings highlight the necessity for rigorously designed RCTs adhering to CONSORT and STRICTA guidelines.
Synergistic Effects of Moxibustion Combined with Auricular Therapy
In traditional Chinese medicine, moxibustion is used to warm meridians, dispel cold and dampness, relieve arthralgia, and restore yang.61 When combined with auricular therapy, its clinical efficacy is enhanced. Studies show that integrating moxibustion (with dried ginger cake) and auricular bean embedding improves joint function, reduces pain, shortens morning stiffness, and accelerates recovery in KOA patients compared to routine care.41,62 This combination also demonstrates better safety than moxibustion alone.62 A study involving 55 KOA patients with wind-cold-damp syndrome found that moxibustion (with bamboo ring and ginger cake) plus auricular therapy significantly relieved pain.28 These findings highlight the synergistic effect of the two therapies and reflect the holistic principles of TCM in addressing both root and symptom.
Patterns and Recommendations in Auricular Acupoint Selection
Auricular therapy is rooted in the holographic theory, where the ear is viewed as a microsystem reflecting the whole body.15 Acupoints such as Shenmen (TF4), Xi (AH4), and Jiaogan (AH6 a) are frequently selected due to their regulatory effects on the nervous and endocrine systems. Shenmen (TF4) is well-documented to calm the mind, relieve pain, and regulate cortical activity.19,63 Xi (AH4) stimulates local analgesia, while Pizhixia (AT4) inhibits pain signal transmission. Jiaogan (AH6 a) harmonizes the autonomic nervous system and is particularly effective in chronic pain conditions with underlying neurohumoral imbalance.64 Furthermore, syndrome differentiation plays a key role in personalized treatment. For dampness-cold obstruction syndrome, Shen (CO10) and Gan (CO12) are employed to warm yang and dispel cold-dampness, aligning with TCM’s theory of internal-external interaction.24 In deficiency syndromes, such as liver-kidney deficiency and qi-blood depletion, Shen (CO10), Pi (CO13), and Sanjiao (CO17) are used to tonify the root and restore systemic balance.
Based on association rule and cluster analysis, this study identified synergistic auricular acupoint pairings that enhance the therapeutic efficacy of auricular therapy for KOA. Among them, Shenmen (TF4)–Pizhixia (AT4) showed the highest support. Shenmen (TF4) calms the mind to relieve pain, while Pizhixia (AT4) promotes Qi and blood circulation; together they harmonize mind and body to achieve analgesic effect.63,65 From the TCM Zang-Xiang perspective, KOA is rooted in liver and kidney deficiency, which impairs tendon and bone function. Accordingly, the Gan (CO12)–Shen (CO10) pairing nourishes and strengthens these organs to restore balance. Cluster analysis further revealed three acupoint groups: (1) Regulatory core: Shenmen (TF4), Xi (AH4), Jiaogan (AH6 a), and Pizhixia (AT4), which relieve pain by calming the mind, regulating qi and blood, and promoting circulation; (2) Zang-fu reinforcement: Gan (CO12) and Shen (CO10), focusing on tonifying the liver and kidney to improve musculoskeletal function; and (3) Adjunctive functional group: a broader group including Yidan (CO11), Xin (CO15), Fei (CO14), Pi (CO13), and Sanjiao (CO17), which harmonize internal organ function to support qi-blood production and systemic balance.63,64,66 These findings reflect the integration of TCM’s holistic, syndrome-differentiation approach with neurophysiological mechanisms, supporting personalized and synergistic acupoint selection strategies for KOA pain management.
Limitations
This study has several limitations inherent to systematic reviews and data mining approaches. First, the overall methodological quality of the included randomized controlled trials was suboptimal. Many studies lacked detailed descriptions of randomization methods, allocation concealment, blinding procedures and lack of research solely focusing on the use of ear points, which may introduce bias and limit the strength of the evidence. Second, there was considerable heterogeneity in intervention protocols, including variations in auricular point selection, stimulation methods, treatment duration, and outcome measures, making direct comparisons and meta-analysis difficult. Third, due to the descriptive nature of data mining techniques such as frequency and association rule analysis, causal relationships between specific auricular point combinations and clinical outcomes cannot be established. Future research should prioritize rigorously designed, multicenter RCTs with standardized intervention protocols and robust reporting standards to validate and extend these findings. In addition, while we employed FDR correction to enhance the robustness of our association rule findings, it is important to note that the p-values for these rules were approximations derived post-hoc. Future studies with pre-registered hypotheses could employ more specialized software packages designed for statistical inference in pattern mining. What’s more, our study is subject to selection bias. In seeking to identify patterns associated with positive outcomes, we intentionally focused on studies that reported efficacy. This approach inevitably excludes studies with null or negative findings, which may skew the perceived importance of certain acupoint combinations and limits the generalizability of our findings. Additionally, the generalizability of our findings may be influenced by the fact that the included studies were primarily conducted in China. Therefore, caution is warranted when extrapolating these results to other ethnic and cultural populations, and we provided English translations of abstract of the original Chinese articles in Supplement File 1.
Conclusion
This systematic review characterized patterns of auricular acupoint selection for KOA pain relief. Data mining revealed that commonly used points and combinations align with both TCM theory and neurophysiological mechanisms, suggesting that current clinical practice is largely consistent with established principles. However, methodological limitations and heterogeneity among the included trials preclude firm conclusions regarding efficacy, underscoring the need for rigorously designed studies with transparent randomization, assessor blinding, and standardized protocols.
Clinically, our findings support a stepped approach to point selection: begin with a core analgesic pair (Shenmen (TF4) and Xi (AH4), add Gan (CO12) and Shen (CO10) to address Liver and Kidney deficiency, and further individualize with adjunctive points based on syndrome differentiation (eg, Spleen and Stomach points for qi-blood deficiency). Future trials comparing these data-driven strategies will be essential to transition from descriptive mapping to clinical validation and evidence-based framework development.
Abbreviations
KOA, knee osteoarthritis; TCM, traditional Chinese medicine; NSAIDs, nonsteroidal anti-inflammatory drugs; RCTs, randomized controlled trials; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses, VAS, Visual Analogue Scale; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index; ROB, Risk of Bias.
Author Contributions
All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
This study is supported by the National Natural Science Foundation of China (72204165). The funding is not involved in study design, data collection, analysis, interpretation, manuscript writing, or the decision to publish.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Medicine CC. Guidelines for INTEGRATED TCM WM diagnosis and treatment of knee osteoarthritis(2023 edition). J Tradit Chin Orthopedics. 2023;35(06):1–13.
2. Sharma L. Osteoarthritis of the Knee. N Engl J Med. 2021;384(1):51–59. doi:10.1056/NEJMcp1903768
3. Battistelli M, Favero M, Burini D, et al. Morphological and ultrastructural analysis of normal, injured and osteoarthritic human knee menisci. Eur J Histochem. 2019;63(1). doi:10.4081/ejh.2019.2998
4. Steinmetz JD, Culbreth GT, Haile LM, Global. regional, and national burden of osteoarthritis, 1990-2020 and projections to 2050: a systematic analysis for the Global Burden of Disease Study 2021. Lancet Rheumatol. 2023;5(9):e508–e522. doi:10.1016/s2665-9913(23)00163-7
5. Gelber AC. Knee Osteoarthritis. Ann Intern Med. 2024;177(9):Itc129–itc144. doi:10.7326/annals-24-01249
6. Du X, Liu ZY, Tao XX, et al. Research progress on the pathogenesis of knee osteoarthritis. Orthop Surg. 2023;15(9):2213–2224. doi:10.1111/os.13809
7. Peat G, McCarney R, Croft P. Knee pain and osteoarthritis in older adults: a review of community burden and current use of primary health care. Ann Rheum Dis. 2001;60(2):91–97. doi:10.1136/ard.60.2.91
8. Jang S, Lee K, Ju JH. Recent updates of diagnosis, pathophysiology, and treatment on osteoarthritis of the knee. Int J Mol Sci. 2021;22(5):2619. doi:10.3390/ijms22052619
9. Gibbs AJ, Gray B, Wallis JA, et al. Recommendations for the management of Hip and knee osteoarthritis: a systematic review of clinical practice guidelines. Osteoarthritis Cartilage. 2023;31(10):1280–1292. doi:10.1016/j.joca.2023.05.015
10. Bannuru RR, Osani MC, Vaysbrot EE, et al. OARSI guidelines for the non-surgical management of knee, Hip, and polyarticular osteoarthritis. Osteoarthritis Cartilage. 2019;27(11):1578–1589. doi:10.1016/j.joca.2019.06.011
11. Bruyère O, Honvo G, Veronese N, et al. An updated algorithm recommendation for the management of knee osteoarthritis from the European Society for Clinical and Economic Aspects of Osteoporosis, Osteoarthritis and Musculoskeletal Diseases (ESCEO). Semin Arthritis Rheum. 2019;49(3):337–350. doi:10.1016/j.semarthrit.2019.04.008
12. Li LC, Ahmad MA, Hou TC, et al. Comparing the effects of computerized versus manual methods of identifying point-specific acupuncture as an adjunct to physiotherapy in the management of knee osteoarthritis: a randomized controlled trial protocol. PLoS One. 2025;20(1):e0313761. doi:10.1371/journal.pone.0313761
13. Guo K, Lu Y, Wang X, et al. Multi-level exploration of auricular acupuncture: from traditional Chinese medicine theory to modern medical application. Front Neurosci. 2024;18:1426618. doi:10.3389/fnins.2024.1426618
14. Hou PW, Hsu HC, Lin YW, Tang NY, Cheng CY, Hsieh CL. The history, mechanism, and clinical application of auricular therapy in Traditional Chinese Medicine. Evid Based Complement Alternat Med. 2015;2015:495684. doi:10.1155/2015/495684
15. Elliott T, Merlano Gomez M, Morris D, Wilson C, Pilitsis JG. A scoping review of mechanisms of auricular acupuncture for treatment of pain. Postgrad Med. 2024;136(3):255–265. doi:10.1080/00325481.2024.2333232
16. Moura CC, Chaves ECL, Chianca TCM, et al. Contribution of Chinese and French ear acupuncture for the management of chronic back pain: a randomised controlled trial. J Clin Nurs. 2019;28(21–22):3796–3806. doi:10.1111/jocn.14983
17. Lin Y, Wu Y, Zhou X, Shen B, Lv C. Observation of the therapeutic effect of auricular bean pressing on early knee osteoarthritis pain: a randomized controlled trial. J Back Musculoskelet Rehabil. 2023;36(4):815–822. doi:10.3233/bmr-220271
18. Zhang X, He B, Wang H, Sun X. Auricular acupressure for treating early stage of knee osteoarthritis: a randomized, sham-controlled prospective study. QJM. 2022;115(8):525–529. doi:10.1093/qjmed/hcab230
19. He J, Ma L, Zhou F, et al. The efficacy and safety of auricular point pressing therapy for knee osteoarthritis: a protocol for systematic review and meta-analysis. Medicine. 2022;101(15):e29098. doi:10.1097/md.0000000000029098
20. Li WX, Wu CQ, Feng W, et al. Acupuncture for rehabilitation after total knee arthroplasty: a systematic review and network meta-analysis. Int J Surg. 2025;111(1):1373–1385. doi:10.1097/js9.0000000000002006
21. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021:
22. Medicine SAoTC. Standardized manipulations of acupuncture and moxibustion—Part 3:Ear acupuncture. State Administration for Market Regulation CNSA. editor. 2021:12
23. Medicine SAO TC. Nomenclature and location of auricular points. In: State Administration for Market Regulation CNSA, editor. 2008.
24. Zeng L, Zhou G, Yang W, Liu J. Guidelines for the diagnosis and treatment of knee osteoarthritis with integrative medicine based on traditional Chinese medicine. Front Med. 2023;10:1260943. doi:10.3389/fmed.2023.1260943
25. Shuster JJ. Review of Cochrane handbook for systematic reviews for interventions, Version 5.1.0. Res Synthesis Method. 2011;(No.2):126–130.
26. Dong LL, Wei Z, Dong B, Ren K. Observation on clinical effect of “Shuang Zhou Therapy” in treating knee osteoarthritis. Acta Chin Med. 2020;35(4):875–880. doi:10.16368/j.issn.1674-8999.2020.04.195
27. Wang XH, Wang J, Zhang T, Liu JW, Xiu Q, Xie YS. The efficacy observe of the treatment of Jintiange combined with sticking magnetic beads on auricular points for knee osteoarthritis. J Front Med. 2020;10(18):26–28.
28. Li YY, Wang L, Zhou WY. Bamboo ring ginger moxibustion combined with auricular acupoint pressing in the treatment of knee osteoarthritis of wind-cold-dampness arthralgia syndrome. Chin Med M Distance Educ China. 2022;20(7):110–112. doi:10.3969/j.issn.1672-2779.2022.07.040
29. Zhou PY, Shen RY, Chen C. Effect of moxibustion combined with auricular point bean pressure in treating knee osteoarthritis of dampness-cold obstruction syndrome. Chin J Rural Med Pharm. 2022;29(1):12–13. doi:10.19542/j.cnki.1006-5180.005893
30. Shen JY, Jin HT, Xu TT, Tong PJ. Clinical study on the effect of bushen huoxue decoction combined with auricular therapy on knee osteoarthritis. J Emergency Traditional Chin Med. 2016;25(3):477–479. doi:10.3969/j.issn.1004-745X.2016.03.032
31. Li LH. Clinical Observation of Traditional Chinese Medicine DuHuoJiSheng Granule and Auricular Therapy in the Treatment of Knee Osteoarthritis. Doctoral dissertation. Guangzhou University of Chinese Medicine; 2011. 15:09.
32. Cheng G, Cheng W, Jiang YG. Controlled observation of clinical efficacy on knee osteoarthritis treated with auricular electroacupuncture and the isolated moxibustion with Lingxianherbal paste. Chin Acupunct Moxibustion. 2014;34(3):230–234. doi:10.13703/j.0255-2930.2014.03.008
33. Huang LG, Xiao LW. Clinical effect of auricular therapy in relieving knee osteoarthritis pain. Heilongjiang J Traditional Chinese Med. 2015;44(1):43.
34. Wang XR. A Clinical Observation of Auricular Application Pressure Analgesia Applied in Rehabilitation Training of Knee Osteoarthritis Patients with Kidney Deficiency Type. Master’s thesis. Fujian University of Traditional Chinese Medicine; 2017.
35. Wang J, Wang S, YJ W. Clinical observation on the treatment of knee osteoarthritis with auricular acupoint pressing beans combined with traditional Chinese medicine prescription and acupuncture. Guangming J Chin Med. 2019;34(6):917–919. doi:10.3969/j.issn.1003-8914.2019.06.043
36. Yu HY, Huang LJ, Zou F. Clinical effect of pressing beans at auricular points combined with traditional Chinese medicine Reyanbao on KOA patients. Contemp Med. 2021;27(29):55–57. doi:10.3969/j.issn.1009-4393.2021.29.022
37. Ma X, Sun SJ, Huo JF, Liang YL, Li XH. Observing the effect of auricular acupuncture combined with moxibustion on Lysholm knee score and VAS score in patients with knee osteoarthritis. J Sichuan Tradit Chin Med. 2015;33(7):175–177.
38. Li LH, Sun SJ, Zhang XP, Liang YL, Li XH. Influence of ear acupuncture and moxibustion on lysholm scales and VAS of the patients with knee osteoarthritis. Western J Tradit Chin Med. 2016;29(4):109–111. doi:10.3969/j.issn.1004-6852.2016.04.038
39. Sun SJ, Sun LJ, Liang YL, Sun LM, Li XH. Clinical research on moxibustion and auricular acupuncture treatment of patients with osteoarthritis of knee. Acta Chin Med. 2016;31(2):297–299.
40. Sun SJ, Sun LM, Huo JF, Li XH, Liang YL, Sun LH. Curative observation of applying auricular acupressure and moxibustion to treat 38 cases of yang deficiency, jtanfeng, et and cold type of knee osteoarthritis. J Sichuan Tradit Chin Med. 2014;2014(10):156–158.
41. Liu J, Xie Q. The effect of aconite cake separated moxibustion combined with auricular point bean embedding in the nursing of knee osteoarthritis. Chin Med Modern Distance Educ China. 2023;21(6):175–177. doi:10.3969/j.issn.1672-2779.2023.06.062
42. Zhou XL, Deng D, Shen B, Wu FM, Chen QD, Lin YY. Application of combing thumbtack needle with ear point pressing beans in knee osteoarthritis patients with syndrome of qi and blood weakness. Chin J Gen Pract. 2022;20(1):121–124. doi:10.16766/j.cnki.issn.1674-4152.002292
43. Liang LJ, Wang QF, Bie SG, Li JJ, Li JP. Clinical effect of press-needle combined with auricular pressure in the treatment of knee osteoarthritis. Chin J Practical Med. 2022;116–119. doi:10.3760/cma.j.cn115689-20220616-02568
44. Yang HM, Zheng BL. Clinical efficacy observation of shangkehuangshui external application and auricular point seed-pressing therapy in treating knee osteoarthritis with damp-heat accumulation type. J Guangzhou Univer Tradit Chin Med. 2020;37(6):1109–1114. doi:10.13359/j.cnki.gzxbtcm.2020.06.022
45. Huang WJ, Huang JF, Zhao K, Li ZM, Zhang ZY. Clinical observation of Shiquan Dabu decoction combined with auricular point therapy in the treatment of mild to moderate knee osteoarthritis syndrome of qi and blood weakness. Chin J Tradit Med Traumatol Orthopedics. 2017;25(3):40–42.
46. Pang WX. Clinical Study on Treatment of Knee Osteoarthritis with Herbal Fumigation Combined with auricular acupressure by magnetic bead. Master’s thesis. Zhejiang University of Chinese Medicine; 2023.
47. Luo L, Li YH. Effect of traditional Chinese medicine directional medication combined with ear acupoint bean-pressing on 35 cases of knee osteoarthritis. Hunan J Tradit Chin Med. 2022;38(6):89–91. doi:10.16808/j.cnki.issn1003-7705.2022.06.027
48. Zhang HM, Wang XL, Liu X. Application of auricular pressing therapy of midnight-midday ebb flow Nazi method in nursing of knee osteoarthritis. J Clin Med Pract. 2024;28(5):122–125. doi:10.7619/jcmp.20232640
49. Li JY. Clinical observation of comprehensive treatment of knee osteoarthritis. J Pract Tradit Chin Med. 2022;38(1):113–114.
50. Wang XR, Zheng QK, Gan AF. Ear point seed embedding combined with exercise training was used to treat 30 cases of knee osteoarthritis of Yang deficiency and cold condensation type. Fujian J Trad Chinese Med. 2018;49(2):77–78. doi:10.13260/j.cnki.jfjtcm.011607
51. Chen BM, Wang LL, Chen XY. Nursing observation on the treatment of knee arthralgia with self-made fumigation and washing prescription combined with auricular point pressing. Smart Healthcare. 2021;7(23):171–173. doi:10.19335/j.cnki.2096-1219.2021.23.056
52. Zhao YJ, Zhang HF, Cui LK. Clinical study on juanbi tang combined with auricular point sticking for knee osteoarthritis of cold-dampness impediment type. New Chin Med. 2021;53(22):40–43. doi:10.13457/j.cnki.jncm.2021.22.011
53. Wei YY, Zhao YJ, Meng XH. Effect of massage combined with ear acupoint bean-pressing on knee osteoarthritis. Zhongguo Xiangcun Yiyao. 2023;30(19):12–13. doi:10.19542/j.cnki.1006-5180.2211-100
54. Sun LM, Sun SJ, Sun LH, et al. Auricular acupuncture combined with moxibustion in the treatment of knee osteoarthritis of Yang deficiency and cold condensation. J Hebei Tradit Chin Med Pharmacol. 2015;30(1):44–47. doi:10.16370/j.cnki.13-1214/r.2015.01.015
55. Li YX, Wei X. Effect of auricular acupuncture combined with acupoint application on bone metabolism inflammatory factors and pain in patients with knee osteoarthritis. Chin J Convalescent Med. 2023;32(12):1243–1246. doi:10.13517/j.cnki.ccm.2023.12.003
56. Xu C, Gao YN, Yang HS. Observations on the efficacy of needle warming therapy plus auricular point sticking and medication in treating knee osteoarthritis. Shanghai J Acupuncture Moxibustion. 2018;37(11):1286–1290. doi:10.13460/j.issn.1005-0957.2018.11.1286
57. Li LD, Sun SJ, Huo JF, Liang YL, Li XH. Clinical study on moxibustion and auricular acupressure for patients with knee osteoarthritis identified as yang deficiency-cold coagulation. J Traditional Chinese Med Pharm. 2015;21(17):50–52. doi:10.13862/j.cnki.cn43-1446/r.2015.17.018
58. Peng XF, Zhao C. Effect of auricular bean embedding on nocturnal rest pain in patients with knee osteoarthritis. Tradit Chin Med Rehab. 2014;5(10):141–142.
59. Wang Y, Jia XH, Lu Z, Wang ZF. Efficacy observation of ear point therapy in treating knee osteoarthritis and the effects on bone metabolism and inflammatory factors. Shanghai J Acupuncture Moxibustion. 2024;43(11):1170–1176. doi:10.13460/j.issn.1005-0957.2024.11.0001
60. Yang YQ, Liao AP, Lei SH, Huang YX. Exploring the application effect of traditional Chinese medicine nursing in patients with knee osteoarthritis treated with PRP injection. J Front Med. 2024;14(29):106–108.
61. Xin S, Liu J, Yang Z, Li C. Comparative effectiveness of moxibustion and acupuncture for the management of osteoarthritis knee: a systematic review and meta-analysis. Heliyon. 2023;9(7):e17805. doi:10.1016/j.heliyon.2023.e17805
62. Ma YY, Liu RR, Yin H, Liu MN. Nursing effect of aconite cake-separated moxibustion combined with ear point buried beans in the treatment of knee osteoarthritis. World Latest Med Informat. 2019;19(95):282. doi:10.19613/j.cnki.1671-3141.2019.95.188
63. Quan R, Zhou J, Jia Y, et al. Effects of ear seed acupressure at the subcortex,Shenmen (TF4) and adrenal gland points on pressure pain thresholds and pain tolerance in healthy individuals. Modern Chin Clin Med. 2023;30(06):17–20. doi:10.3969/j.issn.2095-6606.2023.06.004
64. Liu M, Tong Y, Chai L, et al. Effects of auricular point acupressure on pain relief: a systematic review. Pain Manag Nurs. 2021;22(3):268–280. doi:10.1016/j.pmn.2020.07.007
65. Xin W, Miao Y, Yu M, et al. Acupuncture provides short-term functional improvements and pain relief for patients after knee replacement surgery: a systematic review and meta-analysis. J Pain. 2024;25(12):104669. doi:10.1016/j.jpain.2024.104669
66. Wang ZW, Jin LF, Qi PK. Exploration of the therapeutic effect of warm acupuncture and moxibustion combined with massage on knee osteoarthritis based on the theory of “liver dominating tendon and kidney dominating bone”. China Med Pharm. 2024;14(06):34–38. doi:10.20116/j.issn2095-0616.2024.06.07
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Evidence Based Research on Medication Patterns in the Traditional Chinese Medicine Treatment of Tic Disorders: A Complete Review
Li B, Zhu J, Zhang B, Ling Z, Zhao Y, Leng W, Zhang Q, Zhou X
Neuropsychiatric Disease and Treatment 2025, 21:2001-2016
Published Date: 10 September 2025
Task-Shifting from Acupuncturists to Nurses in Delivering Acupuncture/Acupressure or Supervising Patient Self-Administered Acupressure for Sleep Management: Is It Feasible?
Zhao FY, Zhang WJ, Chow CM, Lee YX, Xu P, Ho YS, Fu QQ, Conduit R
Nature and Science of Sleep 2025, 17:2887-2900
Published Date: 7 November 2025
From Needles to Photons: Clinical Efficacy, Safety, and Mechanistic Insights of Laser Acupuncture in Insomnia Management
Zhao FY, Zhang WJ, Chow CM, Xu P, Yue LP, Ho YS, Fu QQ, Conduit R
Nature and Science of Sleep 2025, 17:3105-3114
Published Date: 2 December 2025
Acupuncture-Based Interventions for Sleep Outcomes in Patients with Postherpetic Neuralgia: A Systematic Review and Meta-Analysis
Zhang J, Zhang J, Chen J, Li Z, Liu X, Chen S
Journal of Pain Research 2026, 19:613776
Published Date: 19 June 2026