Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
Sociodemographic Determinants of Hospitalized Exacerbations in Exposure-Defined COPD Phenotypes: A Nationwide Prospective Cohort Study in China
Authors Zheng Z, Tang X, Li W, Niu H ![]() , Dong F
, Dong F ![]() , Yan J, Shi M, Cui Y, Huang T, Han Z, Peng Y, Su R
, Yan J, Shi M, Cui Y, Huang T, Han Z, Peng Y, Su R ![]() , Wang C, Russell RE
, Wang C, Russell RE ![]() , Yang T, Huang K
, Yang T, Huang K ![]()
Received 10 March 2026
Accepted for publication 25 May 2026
Published 5 June 2026 Volume 2026:21 606977
DOI https://doi.org/10.2147/COPD.S606977
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Zijing Zhou
Zhoude Zheng,1– 3 Xingyao Tang,2,4 Wei Li,2 Hongtao Niu,2 Fen Dong,2 Jisong Yan,2 Minghui Shi,2,4 Yanan Cui,2 Tingting Huang,2 Zhifa Han,2 Yaodie Peng,1,2 Rui Su,1,2 Chen Wang,2,5 Richard EK Russell,3,* Ting Yang,1,2,* Ke Huang2,*
1Peking University China-Japan Friendship School of Clinical Medicine, Beijing, People’s Republic of China; 2National Center for Respiratory Diseases; State Key Laboratory of Respiratory Health and Multimorbidity; National Clinical Research Center for Respiratory Diseases; Institute of Respiratory Medicine, Chinese Academy of Medical Sciences; Department of Pulmonary and Critical Care Medicine, Center of Respiratory Medicine, China-Japan Friendship Hospital, Beijing, People’s Republic of China; 3King’s Centre for Lung Health, School of Immunology and Microbial Sciences, Faculty of Life Sciences and Medicine, King’s College London, London, UK; 4Capital Medical University China-Japan Friendship School of Clinical Medicine, Beijing, People’s Republic of China; 5School of Population Medicine and Public Health, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ting Yang; Ke Huang, Email [email protected]; [email protected]
Purpose: Chronic obstructive pulmonary disease (COPD) a major cause of morbidity, hospitalization, and healthcare burden worldwide and is increasingly recognized as a heterogeneous syndrome with diverse environmental and socioeconomic determinants. We aimed to identify phenotype-specific determinants of hospitalized exacerbations and annual total length of hospital stay (LHS) in smoking and non-smoking COPD.
Patients and Methods: We analyzed 3,913 COPD patients from a nationwide multicenter prospective cohort in China, stratified by smoking status. Hospitalized exacerbations at baseline and during one-year follow-up, as well as LHS, were assessed. Multivariable logistic regression and ordinal logistic regression models were used to estimate adjusted odds ratios (ORs) for hospitalized exacerbations and annual total LHS within each subgroup.
Results: Among 3,913 participants, 1,709 (43.7%) had non-smoking COPD and 2,204 (56.3%) had smoking-related COPD. During follow-up, 28.0% of non-smokers and 29.9% of smokers experienced hospitalized exacerbations. Rural residence, larger household size, and prior hospitalizations in the preceding year were consistently associated with hospitalized exacerbations and longer annual total LHS in both groups. Biomass exposure was independently associated with hospitalized exacerbations among non-smoking patients but not among smokers after full adjustment. Low body mass index (BMI) was associated with increased risk in non-smoking COPD. Findings were consistent across baseline and prospective analyses, as well as binary and ordinal outcome models.
Conclusion: In China, rural residence, larger household size, and prior exacerbation history were common determinants of hospitalized exacerbations and longer annual total LHS in patients with COPD, while biomass exposure and low BMI exerted stronger effects in non-smoking COPD.
Keywords: COPD, acute exacerbation, hospitalization, biomass exposure, non-smoking COPD, prospective cohort
Introduction
Chronic obstructive pulmonary disease (COPD) is a leading cause of respiratory morbidity worldwide and poses a substantial public health burden.1 According to the China Pulmonary Health study, COPD affects approximately 13.7% of individuals aged over 40 years in China.2,3 In addition to its high prevalence, COPD contributes significantly to healthcare utilization, hospitalization, and socioeconomic burden.1,4 Increasing evidence suggests that COPD is a heterogeneous syndrome influenced by complex interactions between environmental, socioeconomic, and host-related factors rather than a single smoking-related disease entity.5
Although cigarette smoking is the primary cause, non-smoking COPD represents a substantial proportion of disease burden globally.6 Biomass exposure, air pollution, and occupational hazards have all been implicated in COPD development among never-smokers.7,8 Globally, an estimated 4–16% of COPD cases arise in never-smokers, while studies from China have reported substantially higher proportions.6,9–11 These observations highlight considerable heterogeneity of COPD and suggest that distinct exposure pathways may shape disease characteristics and progression.
Previous studies have described variations in clinical and radiological features across exposure-defined COPD phenotypes.12–14 Non-smoking COPD has been associated with biomass exposure, tuberculosis-related lung damage, and airway-predominant changes, whereas tobacco-related COPD more frequently demonstrates emphysema-dominant patterns.14–16 Chinese cohort studies have further reported differences in symptom profiles, childhood respiratory history, and body mass index among patients with differing exposure backgrounds.17,18 Collectively, these findings support the concept that COPD encompasses diverse phenotypes driven by distinct environmental and host-related factors rather than a uniform smoking-related disorder.
Acute exacerbations of COPD (AECOPD), particularly those requiring hospitalizations, are major drivers of morbidity, mortality, and healthcare utilizations. Prolonged length of hospital stay (LHS) further amplifies healthcare burden and costs.19,20 Previous studies have identified associations between exacerbation risk and factors such as air pollution, occupational exposures, damp housing conditions, smoking history, and comorbidities.21–24 Recent work has highlighted that lower income, smoking history, damp living conditions, and job exposures increase exacerbation risk.25–27 Prior exacerbation history has also been consistently associated with future hospitalization risk.28 However, many previous studies have focused primarily on clinical variables, involved relatively small sample sizes, or lacked longitudinal follow-up. Moreover, evidence remains limited regarding sociodemographic and environmental determinants of hospitalized exacerbations and healthcare utilization within exposure-defined COPD phenotypes, particularly among non-smoking patients with COPD.
To address this gap, we analyzed data from a large national multicenter prospective cohort in China. By stratifying patients according to smoking status, we aimed to characterize sociodemographic and environmental determinants of hospitalized AECOPD and annual total LHS within each exposure-defined subgroup. Rather than directly contrasting smoking and non-smoking COPD, this approach seeks to clarify phenotype-specific risk structures that may inform more tailored prevention and management strategies.
Methods
Participants
The Enjoy Breathing Program is a nationwide prospective cohort study involving participants predominantly recruited from healthcare institutions across 17 provinces (or equivalent) in mainland China among adults aged ≥40 years, the details of which have been described previously.29,30 Patients with COPD were diagnosed according to spirometry with post-bronchodilator forced expiratory volume in 1 second to forced vital capacity (FEV1/FVC) ratio of less than 0.7. We analyzed data from 3,913 patients with COPD with one-year follow-up enrolled in the Enjoy Breathing Program. Figure 1 shows the participant selection process. Detailed methods are provided in the Supplementary Methods.
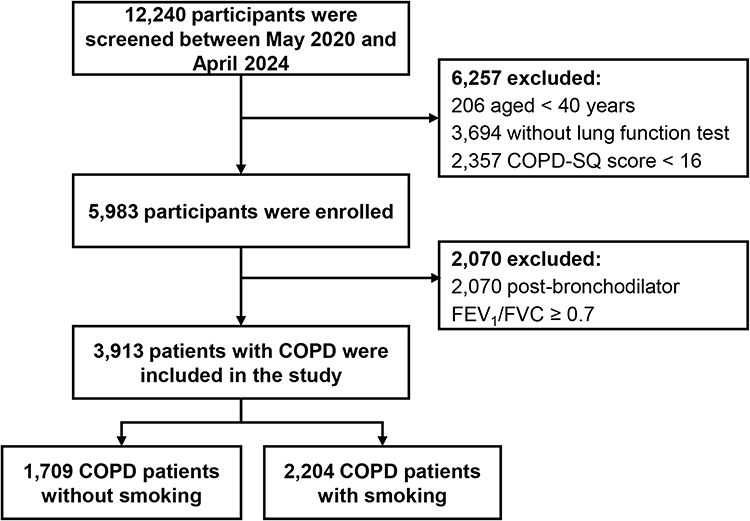 |
Figure 1 Flowchart of participant inclusion. A total of 12,240 individuals were screened between May 2020 and April 2022. After excluding participants based on age (<40 years), absence of lung function tests, and low COPD-SQ scores (<16), 5983 participants were enrolled. Among them, 2,070 were excluded due to a post-bronchodilator FEV1/FVC ≥ 0.7. The final study sample included 3913 COPD patients, comprising 1,709 non-smokers and 2204 smokers. |
The study was registered on www.ClinicalTrials.gov in March 2020 with the ID NCT04318912. Ethical approval was granted by the China-Japan Friendship Hospital (approval number: 2019–41-k29), and all participants gave written informed consent to participate. The study was carried out following the ethical guidelines of the Declaration of Helsinki.
Statistical Analysis
Descriptive statistics were used to summarize continuous variables as means ± standard deviation (SD) and categorical variables as frequencies. The Student’s t-test was used for continuous variables with normal distribution and equal variances; otherwise, the Mann–Whitney U-test was applied. The χ2 test was used for categorical variables, with Fisher’s exact test applied for small cell counts. Moreover, a one-way ANOVA was used for comparing continuous variables across multiple groups, and the Kruskal–Wallis test was applied for non-parametric data.
Univariable logistic regression analyses were performed for descriptive purposes. Then, covariates were selected a priori based on a directed acyclic graph (DAG) rather than on statistical significance in univariable analyses.31 The DAG was constructed based on existing literature and clinical knowledge to represent assumed relationships among sociodemographic factors, environmental exposures, baseline disease burden, COPD severity, treatment, and hospitalization outcomes (Supplementary Figure S1). Minimal sufficient adjustment sets were identified according to the DAG framework for estimating total effects of each exposure on hospitalized exacerbations and annual total LHS. Variables reflecting COPD severity (CAT score, mMRC, lung function/GOLD stage, and comorbidities) and treatment were considered downstream mediators or subject to indication bias and were therefore not adjusted for in the primary total-effect analyses.32 The causal analyses focused on sociodemographic and environmental exposures that precede disease progression, including body mass index (BMI), family size, residential setting, geographical region, biomass exposure, education level, employment status and prior COPD-related hospitalizations as an indicator of baseline disease risk. Therefore, covariates differed across exposure-specific models.
Multivariable logistic regression models were used to estimate adjusted odds ratios (ORs) for hospitalized exacerbations at baseline and during one-year follow-up. Ordinal logistic regression models were used to evaluate determinants of annual total LHS, categorized as 0, 1–10, 11–20, and ≥ 21 days. The proportional odds assumption for ordinal logistic regression was assessed before model fitting and was considered acceptable Annual total LHS categories were defined according to the overall distribution and mean hospitalization duration among hospitalized patients while ensuring clinically meaningful gradients of healthcare burden and adequate sample size within each category.
Based on the DAG framework, potential covariates were progressively adjusted in two models: Model 1 was adjusted for age and gender; and Model 2 was further adjusted for the covariates according to DAG results. Analyses were stratified by smoking status. Subgroup analyses according to age, sex, geographical region, and residence were descriptive in nature.
Analyses were conducted using complete-case data because loss to follow-up was minimal, with only three participants lacking follow-up information. Statistical analysis was conducted using GraphPad Prism (version 9.00), SPSS (version 23), and R (version 4.2.3). A two-tailed p-value < 0.05 was considered statistically significant.
Results
Characteristics of Non-Smoking and Smoking COPD Patients at Baseline
Among the 3913 participants with COPD included in the study, 1709 were non-smokers and 2204 were smokers (Figure 1). Non-smoking COPD patients were of similar age to their smoking counterparts (66.2 ± 12.2 years vs 67.0 ± 10.8 years) (Table 1). A substantial difference in sex distribution was observed between groups, with females comprising the majority of non-smoking COPD patients (66.8%) and males accounting for nearly all smoking COPD patients (96.7%) (P < 0.001) (Table 1). Compared to smokers with COPD, non-smokers with COPD were more likely to reside in northern, northeastern, and northwestern regions, have lower education levels, higher employment rates, less usage of therapies, higher rates of biomass exposure, and were less likely to have experienced exacerbations requiring hospitalizations in the past 12 months (Table 1).
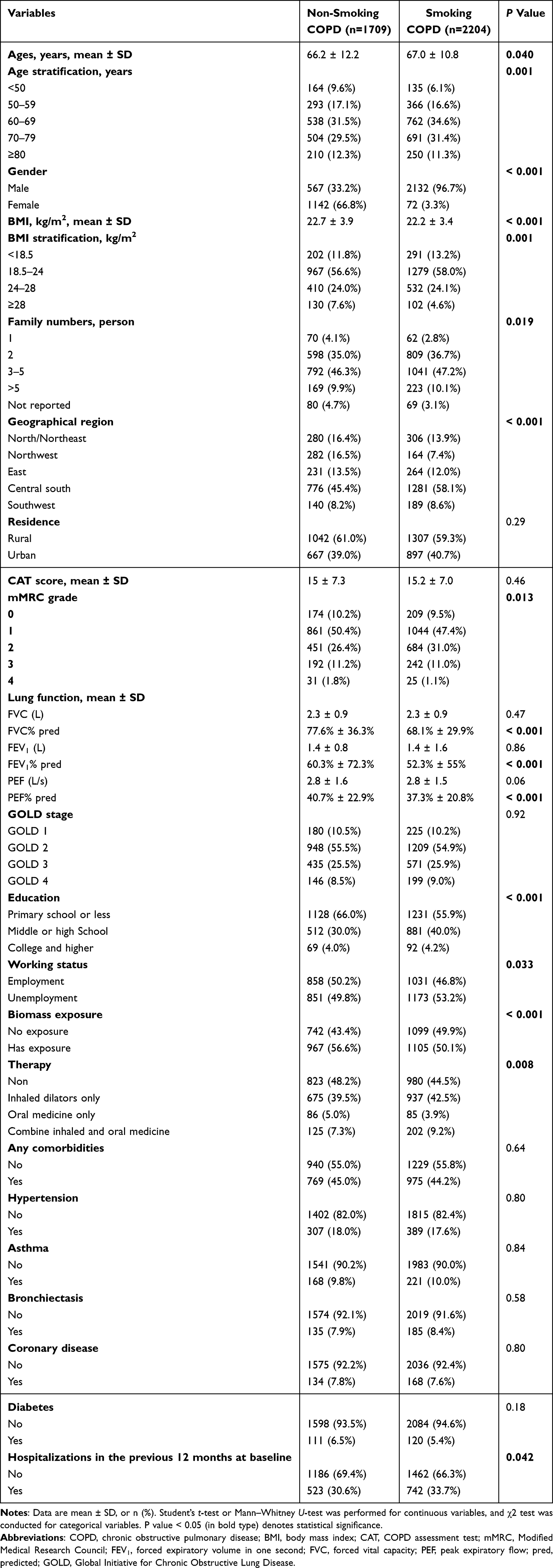 |
Table 1 Sociodemographic Characteristics in Non-Smoking and Smoking COPD Patients at Baseline |
To examine whether these characteristics distributions varied by age group, we then conducted age-stratified analyses (< 50, 50–59, 60–69, 70–79, and ≥ 80 years). The distributions of non-smokers and smokers across sociodemographic factors were significantly different across age subgroups (Supplementary Figure S2). In contrast, upset plots demonstrated broadly similar patterns of comorbidity clustering between non-smoking and smoking COPD patients at baseline (Supplementary Figure S3). In the non-smoking group, 23.1% had one comorbidity, 11.3% had two, and 1.2% had three or more, compared with 23.5%, 9.7%, and 2.0%, respectively, in the smoking group (Supplementary Figure S3).
Sociodemographic Characteristics for Hospitalized Exacerbation Prior 12-Month Hospitalized Exacerbation in Non-Smoking and Smoking COPD at Baseline
Supplementary Table S1 presents the baseline characteristics of COPD patients, stratified by smoking status and further divided according to the presence or absence of hospitalized acute exacerbations in the previous year. At baseline, 523 of 1709 (30.6%) non-smoking COPD patients experienced hospitalized exacerbations, compared to 742 of 2204 (33.7%) smoking patients. (Supplementary Table S1). Baseline characteristics differed significantly between patients with and without hospitalized exacerbations in both non-smoking and smoking COPD groups. In both populations, patients who experienced hospitalized exacerbations were older, had lower BMI, larger family size, and were more likely to reside in rural areas (all P < 0.001) (Supplementary Table S1). They also had higher symptom burden, reflected by higher CAT scores and mMRC grades, and were more frequently receiving inhaled therapies. In contrast, most lung function parameters, GOLD stage distribution, biomass exposure, and the prevalence of major comorbidities did not differ substantially between groups (Supplementary Table S1).
Sociodemographic Correlates Associated with Prior 12-Month Hospitalized Exacerbation in Non-Smoking and Smoking COPD at Baseline
Univariable logistic regression analyses of all baseline variables for hospitalized AECOPD at baseline are presented in Supplementary Table S2. In multivariable analyses adjusted according to the prespecified DAG (Model 2), distinct and shared determinants of hospitalized exacerbations were observed between non-smoking and smoking COPD patients at baseline (Table 2). In non-smoking COPD, larger household size (3–5 members: OR = 2.55, [95% CI, 1.28–5.07]), rural residence (urban vs rural: OR = 0.52, [95% CI, 0.40–0.68]), specific geographical regions (East, Central south, and Southwest), and biomass exposure (OR = 1.47, [95% CI, 1.14–1.89]) were independently associated with hospitalized exacerbations (Table 2). Higher BMI categories were associated with reduced odds (Table 2).
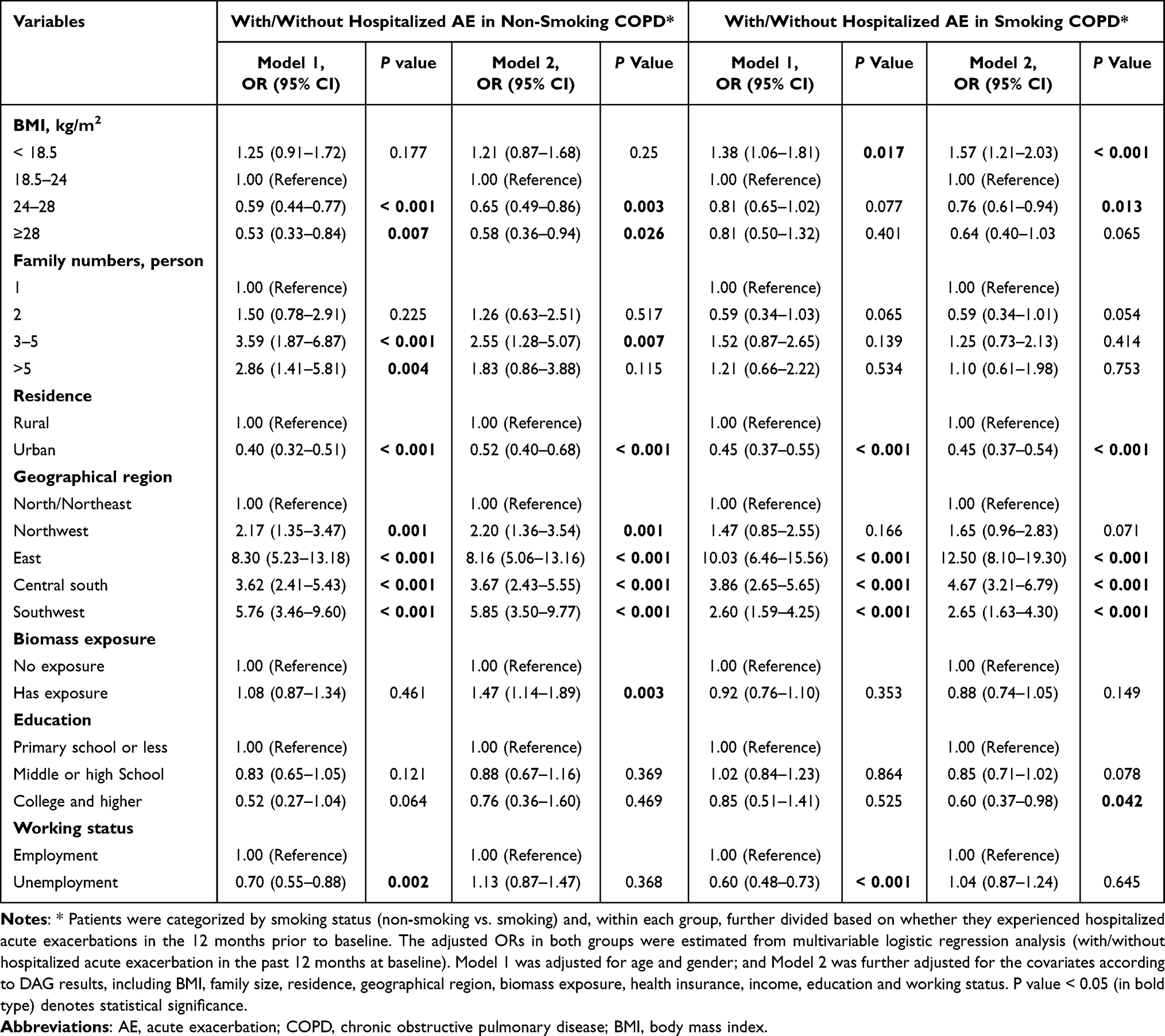 |
Table 2 Adjusted ORs for Factors Associated with Hospitalized Exacerbation Among COPD Patients at Baseline |
In smoking COPD, low BMI was associated with increased risk, whereas urban residence remained protective (OR = 0.45, [95% CI, 0.37–0.54]). Strong regional and residential effects were similarly observed. In contrast to non-smoking COPD, household size and biomass exposure were not independently associated after adjustment. Higher educational attainment (college or above) was associated with lower odds of hospitalizations in smoking COPD.
Sociodemographic Characteristics for Hospitalized Exacerbation in Non-Smoking and Smoking COPD in a 12-Month Follow-Up
Supplementary Table S3 presents the baseline characteristics of COPD patients, stratified by smoking status and further divided according to the presence or absence of hospitalized AE during one-year follow-up. During one-year follow-up, hospitalized exacerbations occurred in 28.0% of non-smoking and 29.9% of smoking COPD patients (Supplementary Table S3). In both groups, patients who experienced hospitalized exacerbations were older, had lower BMI, larger household size, and were more likely to reside in rural areas (all P < 0.001). Symptom burden was significantly higher among hospitalized patients, as evidenced by elevated CAT scores and mMRC grades (Supplementary Table S3). Interestingly, prior hospitalizations within the preceding 12 months were strongly associated with subsequent hospitalized exacerbations in both non-smoking and smoking COPD populations (P < 0.001) (Supplementary Table S3). In contrast, spirometry indices, GOLD stage, and most comorbidities showed no consistent differences between non-smoking and smoking COPD groups (Supplementary Table S3).
To descriptively explore hospitalization patterns according to smoking status across different populations, subgroup analyses were performed stratified by age, sex, geographical region, and residence (Figure 2). Hospitalization proportions generally increased with advancing age in both smoking and non-smoking COPD groups (Figure 2A). Different distributions according to sex were observed between the two groups, with smoking COPD predominantly occurring in males and non-smoking COPD including a larger proportion of females (Figure 2B). Geographical variation in hospitalization proportions was observed across regions in both groups, particularly in the East and Central South regions (Figure 2C). In addition, rural populations showed higher hospitalization proportions than urban populations in both smoking and non-smoking COPD (Figure 2D).
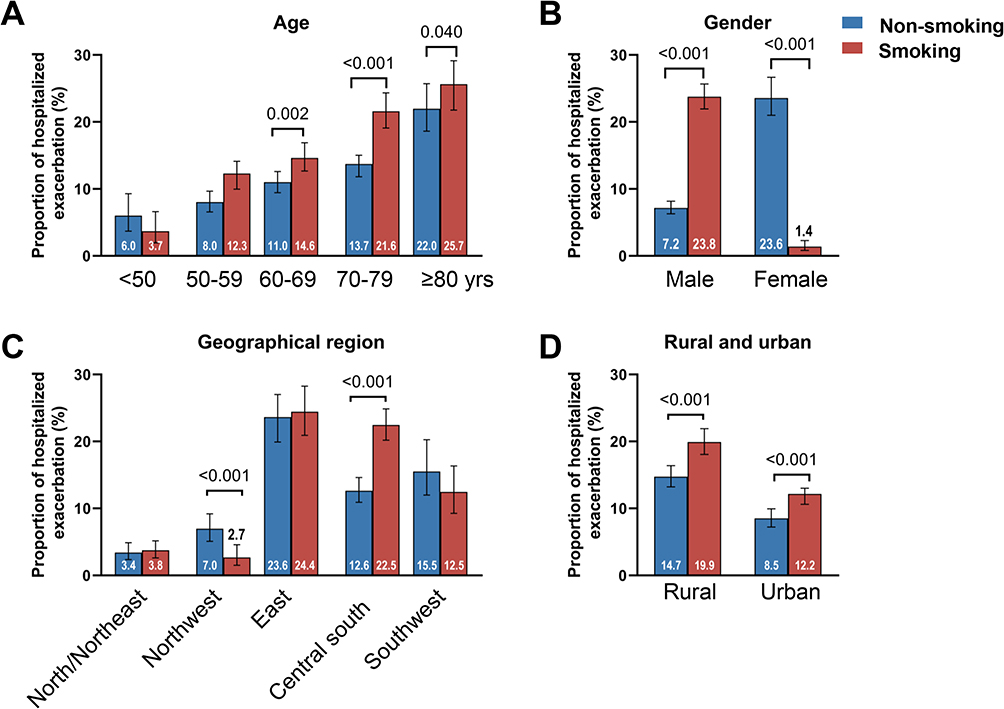 |
Figure 2 The proportion of hospitalized exacerbations in non-smoking and smoking COPD in specific subgroup analyses in a 12-month follow-up. The proportion of hospitalized exacerbation in non-smoking and smoking COPD in subgroup analyses of age (A), gender (B), geographical region (C), and rural and urban (D). The total population was divided into small subgroups based on age stratification (< 50, 50–59, 60–60, 70–79, ≥ 80 years), gender (male and female), geographical region (north/northeast, northwest, east, central south, and southwest), rural and urban, and the proportion was calculated for each subgroup. The Student’s t-test or the Mann–Whitney U-test was used for two-groups comparisons. The One-way ANOVA or the Kruskal–Wallis test was used for multi-groups comparisons. Annotation of the colors: dark red for the proportion of smoking status, dark blue for the proportion of non-smoking status. |
Sociodemographic Correlates of Hospitalized Exacerbation in Non-Smoking and Smoking COPD in a 12-Month Follow-Up
Univariable logistic regression analyses of all baseline variables for hospitalized AECOPD during one-year follow-up are presented in Supplementary Table S4. During one-year follow-up, distinct risk patterns were observed between non-smoking and smoking COPD patients (Table 3). In non-smoking COPD, lower BMI (< 18.5 kg/m2) was independently associated with an increased risk of hospitalized exacerbations, whereas overweight (BMI 24–28 kg/m2) and obesity (BMI ≥ 28 kg/m2) were associated with reduced risk. Larger family size (≥ 3 members) (from adjusted OR = 2.76 [1.26–6.02] to OR = 3.31 [1.44–7.64]), and living in the East (adjusted OR = 9.47 [5.49–16.32]), Central South (adjusted OR = 5.93 [3.64–9.66]), or Southwest regions (adjusted OR = 7.50 [4.19–13.42] were significantly associated with higher odds of hospitalizations (Table 3). Prior COPD-related hospitalizations at baseline were the strongest predictor of future hospitalized exacerbations (adjusted OR = 8.99, [95% CI, 6.82–11.85]) (Table 3). In contrast, Urban residence was associated with lower hospitalization risk (adjusted OR = 0.67 [0.51–0.87]). In smoking COPD, larger family size (from adjusted OR = 3.45 [1.65–7.20] to OR = 2.75 [1.25–6.03]) and geographical regions (from adjusted OR = 5.60 [3.27–9.60], OR =3.78 [2.35–6.08] to OR = 2.09 [1.16–3.80]) remained significant predictors. Urban residence was associated with lower hospitalization risk (adjusted OR = 0.54 [0.42–0.68]). Prior hospitalizations also strongly predicted subsequent exacerbations (adjusted OR = 7.79, [95% CI, 6.35–9.55]) (Table 3).
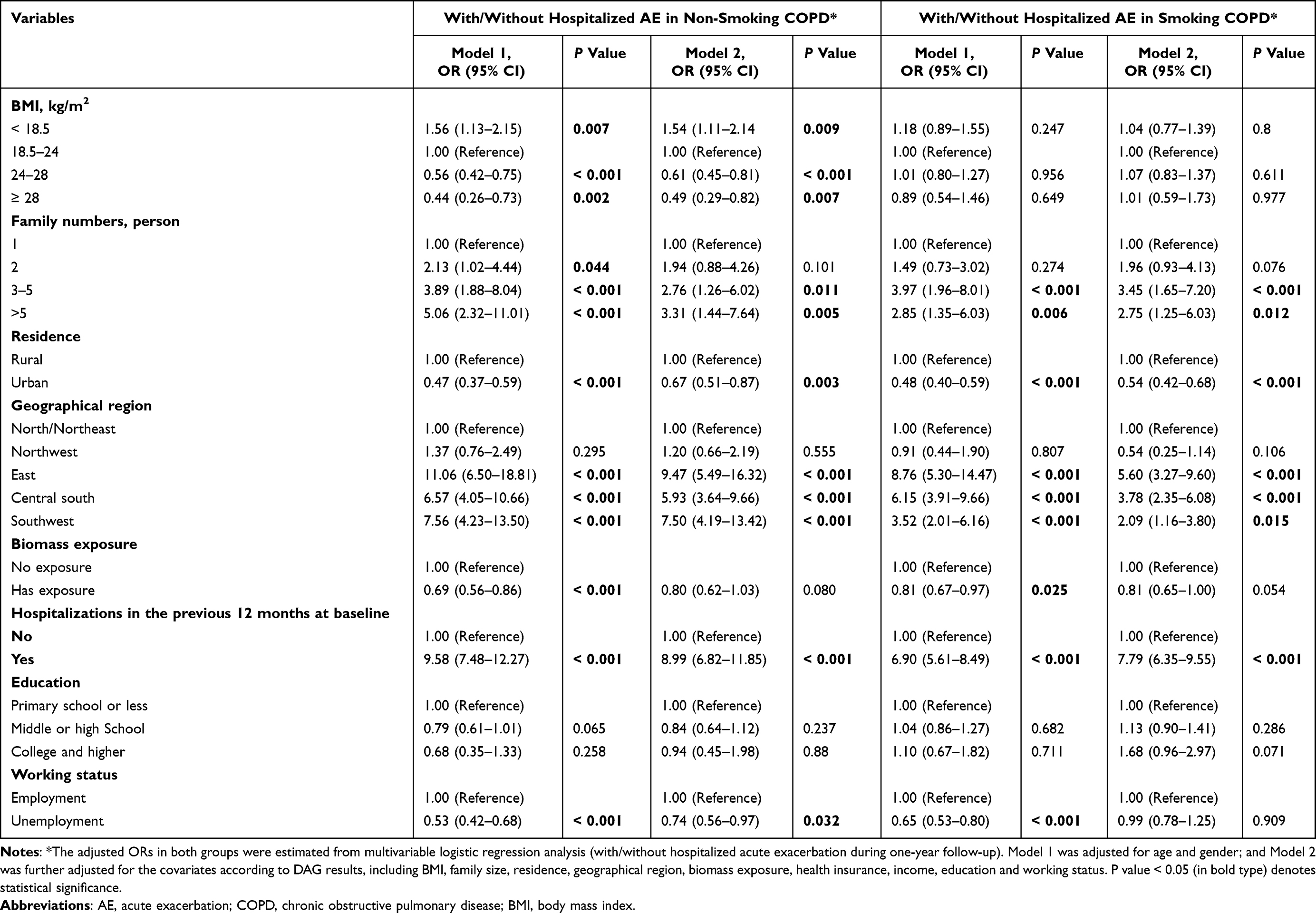 |
Table 3 Adjusted ORs for Factors Associated with Hospitalized Exacerbation Among COPD Patients During One-Year Follow-Up |
Regarding biomass exposure, a weaker association with hospitalized exacerbations was observed in crude analyses among non-smokers, and was no longer statistically significant after multivariable adjustment (adjusted OR = 0.80, [95% CI, 0.62–1.03]) (Table 3). Among smokers, biomass exposure showed a weaker and borderline association in the fully adjusted model (adjusted OR = 0.81, [95% CI, 0.65–1.00]) (Table 3).
Sociodemographic Characteristics for Annual Total LHS in Non-Smoking and Smoking COPD in 12-Month Follow-Up
When stratified by annual total LHS during follow-up as 0, 1–10, 11–20, and ≥ 20 days, a clear gradient pattern was observed in both non-smoking and smoking COPD patients (Supplementary Table S5). Increasing annual total LHS was associated with older age, larger household size, rural residence, and residence in the East and Central South regions in both groups (Supplementary Table S5). Similarly, prior hospitalizations within the previous 12 months showed a strong monotonic association with increasing annual total LHS in both groups (Supplementary Table S5).
Sociodemographic Correlates of Annual Total LHS in Non-Smoking and Smoking COPD in 12-Month Follow-Up
Univariable logistic regression analyses of all baseline variables for annual total LHS during one-year follow-up are presented in Supplementary Table S6. Findings from the ordinal logistic regression analyses of annual total LHS were largely consistent with those for hospitalized exacerbations, with regard to both non-smoking and smoking COPD groups during the 12-month follow-up (Table 4). Larger household size (from adjusted OR = 2.23 [1.02–4.88] to OR = 3.11 [1.37–7.08]), specific geographical regions (East: adjusted OR = 8.81 [5.16–15.05]; Central south: adjusted OR = 6.23 [3.82–10.14]; Southwest: adjusted OR = 6.31 [3.56–11.19]), and prior hospitalizations (adjusted OR = 7.66 [5.91–9.93]) were strongly associated with increasing annual total LHS in non-smoking COPD (Table 4). Urban residence was associated with lower hospitalization risk (adjusted OR = 0.69 [0.53–0.90]).
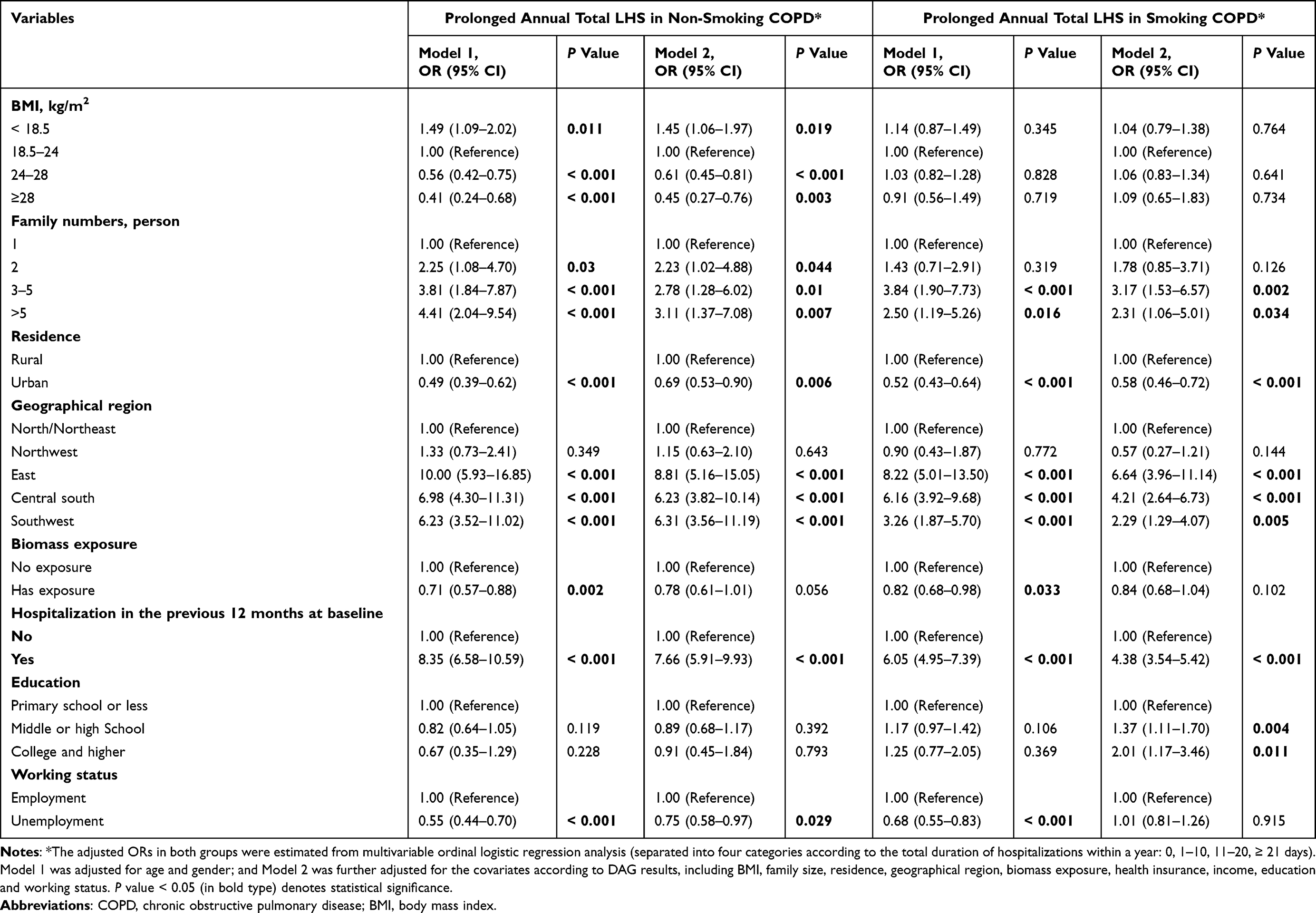 |
Table 4 Adjusted ORs for Factors Associated with Prolonged Annual Total LHS Among COPD Patients During One-Year Follow-Up |
Consistent patterns were also observed across these factors in smoking COPD. Low BMI remained significant among non-smoking COPD patients (adjusted OR = 1.45 [1.06–1.97]), whereas no independent association (adjusted OR = 1.04 [0.79–1.38]) was observed among smokers after adjustment (Table 4). Biomass exposure demonstrated borderline inverse associations that attenuated after full adjustment in both groups (Table 4).
Discussion
Summary of Main Findings
To the best of our knowledge, this study is the largest multicenter survey in China comprehensively demonstrating sociodemographic characteristics and risk factors for hospitalized AECOPD in non-smoking and smoking patients with COPD. Several important findings emerged from this study. First, specific geographical regions, rural residence, larger household size, and prior hospitalizations in the preceding year were consistently associated with both hospitalized exacerbations and longer annual total LHS in both groups. Second, heterogeneity was observed in the associations of biomass exposure and BMI, suggesting that environmental and host-related vulnerabilities may operate differently in smoking-related and non-smoking COPD phenotypes. Third, the consistency of findings across cross-sectional and prospective analyses strengthens the robustness of these associations.
Distinct Characteristics in Smoking and Non-Smoking COPD
Non-smoking patients accounted for substantial amount of COPD patients. Although tobacco smoking is considered as a major risk factor for COPD, there are 25–45% of patients with COPD who have never smoked.6 Consistently, we found that about 43.7% of all non-smoking patients with COPD diagnosed using spirometry, aligned with previously reported proportion of 38.6%–50.4% in China.3,17 The rates in China were higher than those in Denmark (22%),10 Canada (27%),14 and Switzerland (29.3%).33 The discrepancy may due to unbalance of sociodemographic index (SDI): in countries with a high SDI, non-smoking causative factors contributed to 26% of COPD, at middle SDI quintiles 54.8%, at low-middle SDI was 63.9%, and at low SDI quintiles 71.2%.11,34
Increasing evidence suggests that non-smoking COPD represents a clinically meaningful entity, often associated with household air pollution, biomass exposure, and differing inflammatory or structural lung changes.18,33 The Chinese Epidemiological Survey of COPD (CESCOPD) including 644 nonsmokers and 1024 smokers, has suggested that non-smoking COPD were more likely to be female, having better lung function, with less chronic productive coughs and higher BMI but comparable dyspnea scores and age, compared with smokers with COPD.17 In line with previous studies, we found that marked baseline differences were observed between smoking and non-smoking COPD. As expected in the Chinese population, smoking COPD was overwhelmingly male, whereas non-smoking COPD included a substantially higher proportion of women.3 This sex distribution reflects national tobacco consumption patterns but also highlights the structural interdependence between smoking status, gender, occupational exposure, and socioeconomic background.35,36
Such heterogeneity justifies the stratified analytical approach adopted in this study. Previous analyses from the same national program identified four COPD clusters—young male smokers, biomass-exposed females, respiratory comorbidity, and elderly multimorbid patients—with poorer health-related quality of life observed in the latter two clusters.37 In contrast, the current study extends these findings by quantifying phenotype-specific risk factors for clinically important outcomes, including hospitalized exacerbations and annual total LHS. By stratifying analyses according to smoking status, we aimed to clarify risk structures within each exposure-defined phenotype rather than assuming a unified disease pathway.38
Shared Determinants of Hospitalized Exacerbations and LHS in Smoking and Non-Smoking COPD
In this study, we found that living in rural areas was an independent risk factor for hospitalized AECOPD and longer hospital stays in both smoking and non-smoking COPD patients. Moreover, for the first time, our findings have found that living in the East, Central South, or Southwest regions were significantly associated with higher odds of hospitalizations and longer LHS in both groups. These findings align with a previous Chinese study reporting regional and hospital-level variations in COPD exacerbation rates.39 Consistently, a large study conducted in low- and middle-Income countries demonstrated that household air pollution exposure is associated with a higher prevalence of COPD, especially among women and those resided in rural areas.40
In addition, we found that larger household size (≥ 3 members) was consistently associated with both hospitalized exacerbations and longer annual total LHS in both smoking and non-smoking COPD. This association persisted across cross-sectional and longitudinal analyses. Possible mechanisms include increased exposure to respiratory infections, delayed care-seeking in complex family structures, socioeconomic clustering, and caregiving burdens.41 Crowded living conditions may facilitate viral transmission, a known trigger of exacerbations.42 Consistently, Hermann et al found that children under five residing in larger households had a higher prevalence of fever.43 Additionally, household size may proxy underlying socioeconomic structure not fully captured by income or education. These findings underscore the importance of incorporating social environmental variables into COPD risk modelling beyond traditional clinical parameters.
A history of hospitalized exacerbation within the preceding year emerged as the strongest predictor of future hospitalizations and prolonged annual total LHS in both groups. This finding aligns with the well-established principle that exacerbation history is the most powerful predictor of future events, as reflected in GOLD risk stratification frameworks.44 Frequent exacerbators may exhibit a triad of persistent airway inflammation, impaired host defenses, and suboptimal adherence, leading to systemic inflammation, lung hyperinflation, and changes in airway microbiology.45 Importantly, the magnitude and consistency of this association across both smoking and non-smoking COPD suggest that exacerbation susceptibility represents a shared vulnerability pathway transcending exposure phenotype.
Distinct Risk Factors of Hospitalized Exacerbations and LHS in Non-Smoking COPD
Biomass exposure demonstrated differential patterns across smoking strata and analytical models. In non-smoking COPD, biomass exposure was independently associated with hospitalized exacerbations in baseline analyses, although the association became attenuated and no longer statistically significant after full adjustment in prospective analyses. Similar patterns were observed for annual total LHS. These findings remain broadly consistent with previous literature linking household air pollution to airflow limitation, chronic airway inflammation, and increased exacerbation risk.46 Mechanistically, biomass smoke contains particulate matter and toxic gases that induce oxidative stress and small airway remodeling-mechanisms that overlap with, but are not identical to those triggered by tobacco smoke.47 In contrast, among smoking COPD patients, biomass exposure showed weaker and borderline associations after multivariable adjustment, particularly in prospective analyses. This pattern should not be interpreted as a protective effect. Several explanations are plausible. First, the cumulative toxic burden of tobacco smoke may dominate the pathophysiological trajectory in smokers, reducing the detectable marginal contribution of biomass exposure.48 Second, biomass exposure may correlate with rural residence or socioeconomic factors, resulting in residual confounding after adjustment.49 Third, self-reported exposure may not capture duration or intensity, introducing non-differential misclassification.50 Overall, these findings suggest that biomass exposure may act as a more prominent etiological driver in non-smoking COPD, whereas its relative impact in smoking COPD may be may be partially obscured by tobacco-related injury.
Previous research has demonstrated that low BMI is a risk factor for the development of COPD and is also linked to poorer lung function and prognosis in patients with COPD.21,51 Suzuki et al found that weight loss were an independent risk factors for COPD exacerbations.21 In non-smoking COPD, low BMI (< 18.5 kg/m2) was independently associated with increased hospitalization risk and longer annual total LHS, while overweight and obesity appeared protective. This pattern is consistent with the so-called “obesity paradox” described in COPD cohorts, where underweight status correlates with worse outcomes,52 potentially due to reduced respiratory muscle strength, sarcopenia, and systemic inflammation.53
Interestingly, BMI was not independently associated with hospitalizations or annual total LHS in smoking COPD after full adjustment. It is possible that tobacco-related lung injury exerts a dominant influence on disease progression in smokers, diminishing the relative contribution of nutritional status.54 Alternatively, differences in body composition and systemic inflammatory burden between cigarette and biomass smoke-induced phenotypes may underlie this heterogeneity.55
Clinical and Public Health Implications
These findings have important clinical and public health implications. Identification of phenotype-specific determinants may facilitate more individualized prevention and management strategies in COPD. In particular, recognition of biomass exposure and low BMI as important risk factors in non-smoking COPD may improve risk stratification and healthcare resource allocation in vulnerable populations, especially in rural and low-resource settings. More broadly, our findings highlight the importance of incorporating environmental and sociodemographic determinants into COPD prevention frameworks beyond traditional smoking-related paradigms.
Strengths, Limitations, and Future Research Needs
This study has several notable strengths. First, it was based on a large nationwide multicenter prospective cohort, enhancing statistical power and representativeness across diverse regions of China. Second, both baseline and one-year follow-up data were integrated, enabling evaluation of both cross-sectional and prospective determinants of hospitalized exacerbations. Third, clinically meaningful outcomes, including hospitalized exacerbations and annual total LHS, were simultaneously assessed to comprehensively characterize healthcare burden. Fourth, stratified analyses according to smoking status allowed identification of phenotype-specific risk structures in smoking and non-smoking COPD. Fifth, a prespecified DAG-informed adjustment strategy strengthened causal interpretability and reduced inappropriate adjustment and overadjustment bias. Finally, It complements previous work from the same program that characterized COPD heterogeneity using cluster analysis.37
There are potential limitations in the present study. First, as an observational study, residual confounding from unmeasured socioeconomic, environmental, or occupational factors cannot be fully excluded. Detailed information regarding occupational dust exposure, household ventilation, healthcare accessibility, and treatment adherence was not comprehensively available. Second, hospitalization outcomes were partly based on self-report during follow-up interviews and may therefore be subject to recall or reporting bias, although medical records were reviewed when necessary to verify reported events. Third, although loss to follow-up was minimal, a small proportion of participants had incomplete follow-up data, which may introduce potential selection bias. Fourth, variables reflecting COPD severity and treatment may partially overlap with mediators within the causal pathway and were therefore not included in the primary total-effect models. Fifth, the follow-up period was limited to one year, and longer-term studies are warranted to identify sustained determinants of hospitalization burden. Sixth, part of the study period overlapped with the COVID-19 pandemic, which may have influenced healthcare utilization patterns and disease classification. Seventh, the non-smoking group included never-smokers, and we did not collect data on passive smoking exposure. This could lead to non-differential misclassification, potentially diluting the true differences between the two groups. Finally, findings derived from a Chinese population may not be fully generalizable to other healthcare settings or populations.
Conclusion
In this nationwide prospective cohort, rural residence, larger household size, and prior hospitalizations were consistently associated with hospitalized exacerbations and longer annual total LHS in both smoking and non-smoking COPD. Biomass exposure and lower BMI showed stronger associations in non-smoking COPD, highlighting phenotype-specific vulnerability patterns. These findings provide new evidence regarding determinants of healthcare burden across exposure-defined COPD phenotypes and support more targeted prevention strategies, particularly for non-smoking COPD.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author upon reasonable request. Data requests should include a brief description of the intended use and relevant research credentials. All data sharing will be conducted in accordance with applicable ethical guidelines and institutional policies.
Acknowledgments
The authors would like to thank the patients and doctors who were involved in Enjoying Breathing Program. We thank Prof. Mona Bafadhel for her valuable input and constructive discussions during the early stage of this study. In the preparation of this manuscript, the authors utilized ChatGPT-5.1 for language editing and to enhance readability. This paper has been uploaded to research gate as a preprint: https://www.researchgate.net/publication/393579997_Comparison_of_Sociodemographic_Determinants_for_Exacerbation-Related_Hospitalisation_in_Non-Smoking_and_Smoking_COPD_A_Nationwide_Prospective_Study_in_China.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was funded by Noncommunicable Chronic Diseases-National Science and Technology Major Project (2023ZD0506306, 2023ZD0506003), CAMS Innovation Fund for Medical Sciences (CIFMS) (2024-I2M-1-049, 2022-I2M-C&T-B-107), Social Development Project of Yunnan Province (202403AC100006) and Elite Medical Professionals Project of China-Japan Friendship Hospital (ZRJY2024-GG06), China Scholarship Council program (CSC202406010153).
Disclosure
All authors declare no competing interests in this work.
References
1. Vestbo J, Hurd SS, Agustí AG. et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med. 2013;187(4):347–17. doi:10.1164/rccm.201204-0596PP
2. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: 2024 report. 2024. Available from: https://goldcopd.org/.
3. Wang C, Xu J, Yang L, et al. Prevalence and risk factors of chronic obstructive pulmonary disease in China (the China Pulmonary Health [CPH] study): a national cross-sectional study. Lancet. 2018;391(10131):1706–1717. doi:10.1016/s0140-6736(18)30841-9
4. Iheanacho I, Zhang S, King D, Rizzo M, Ismaila AS. Economic Burden of Chronic Obstructive Pulmonary Disease (COPD): a Systematic Literature Review. Int J Chron Obstruct Pulmon Dis. 2020;15:439–460. doi:10.2147/copd.S234942
5. Martinez CH, Han MK. Contribution of the environment and comorbidities to chronic obstructive pulmonary disease phenotypes. Med Clin North Am. 2012;96(4):713–727. doi:10.1016/j.mcna.2012.02.007
6. Salvi SS, Barnes PJ. Chronic obstructive pulmonary disease in non-smokers. Lancet. 2009;374(9691):733–743. doi:10.1016/s0140-6736(09)61303-9
7. Gan WQ, FitzGerald JM, Carlsten C, Sadatsafavi M, Brauer M. Associations of ambient air pollution with chronic obstructive pulmonary disease hospitalization and mortality. Am J Respir Crit Care Med. 2013;187(7):721–727. doi:10.1164/rccm.201211-2004OC
8. Zhou Y, Zou Y, Li X, et al. Lung function and incidence of chronic obstructive pulmonary disease after improved cooking fuels and kitchen ventilation: a 9-year prospective cohort study. PLoS Med. 2014;11(3):e1001621. doi:10.1371/journal.pmed.1001621
9. Wheaton AG, Liu Y, Croft JB, et al. Chronic Obstructive Pulmonary Disease and Smoking Status - United States, 2017. MMWR Morb Mortal Wkly Rep. 2019;68(24):533–538. doi:10.15585/mmwr.mm6824a1
10. Thomsen M, Nordestgaard BG, Vestbo J, Lange P. Characteristics and outcomes of chronic obstructive pulmonary disease in never smokers in Denmark: a prospective population study. Lancet Respir Med. 2013;1(7):543–550. doi:10.1016/s2213-2600(13)70137-1
11. Yang IA, Jenkins CR, Salvi SS. Chronic obstructive pulmonary disease in never-smokers: risk factors, pathogenesis, and implications for prevention and treatment. Lancet Respir Med. 2022;10(5):497–511. doi:10.1016/s2213-2600(21)00506-3
12. Salvi SS, Brashier BB, Londhe J, et al. Phenotypic comparison between smoking and non-smoking chronic obstructive pulmonary disease. Respir Res. 2020;21(1):50. doi:10.1186/s12931-020-1310-9
13. Duarte-de-Araújo A, Teixeira P, Hespanhol V, Correia-de-Sousa J. Characterisation of morbidity in a COPD hospital cohort. Pulmonology. 2019;25(4):200–207. doi:10.1016/j.pulmoe.2019.02.010
14. Tan WC, Sin DD, Bourbeau J, et al. Characteristics of COPD in never-smokers and ever-smokers in the general population: results from the CanCOLD study. Thorax. 2015;70(9):822–829. doi:10.1136/thoraxjnl-2015-206938
15. Lamprecht B, McBurnie MA, Vollmer WM, et al. COPD in never smokers: results from the population-based burden of obstructive lung disease study. Chest. 2011;139(4):752–763. doi:10.1378/chest.10-1253
16. Choi JY, Kim JW, Kim YH, et al. Clinical Characteristics of Non-Smoking Chronic Obstructive Pulmonary Disease Patients: findings from the KOCOSS Cohort. Copd. 2022;19(1):174–181. doi:10.1080/15412555.2022.2053088
17. Zhou Y, Wang C, Yao W, et al. COPD in Chinese nonsmokers. Eur Respir J. 2009;33(3):509–518. doi:10.1183/09031936.00084408
18. Zhang J, Lin XF, Bai CX. Comparison of clinical features between non-smokers with COPD and smokers with COPD: a retrospective observational study. Int J Chron Obstruct Pulmon Dis. 2014;9:57–63. doi:10.2147/copd.S52416
19. Mei F, Dalmartello M, Bonifazi M, et al. Chronic obstructive pulmonary disease (COPD) mortality trends worldwide: an update to 2019. Respirology. 2022;27(11):941–950. doi:10.1111/resp.14328
20. Ruparel M, López-Campos JL, Castro-Acosta A, Hartl S, Pozo-Rodriguez F, Roberts CM. Understanding variation in length of hospital stay for COPD exacerbation: european COPD audit. ERJ Open Res. 2016;2(1):3. doi:10.1183/23120541.00034-2015
21. Suzuki M, Makita H, Ito YM, Nagai K, Konno S, Nishimura M. Clinical features and determinants of COPD exacerbation in the Hokkaido COPD cohort study. Eur Respir J. 2014;43(5):1289–1297. doi:10.1183/09031936.00110213
22. Pouwels SD, Nawijn MC, Bathoorn E, et al. Increased serum levels of LL37, HMGB1 and S100A9 during exacerbation in COPD patients. Eur Respir J. 2015;45(5):1482–1485. doi:10.1183/09031936.00158414
23. Zhou M, He G, Liu Y, et al. The associations between ambient air pollution and adult respiratory mortality in 32 major Chinese cities, 2006–2010. Environ Res. 2015;137:278–286. doi:10.1016/j.envres.2014.12.016
24. Madani NA, Carpenter DO. Patterns of Emergency Room Visits for Respiratory Diseases in New York State in Relation to Air Pollution, Poverty and Smoking. Int J Environ Res Public Health. 2023;20(4):3267. doi:10.3390/ijerph20043267
25. Williams PJ, Cumella A, Philip KEJ, Laverty AA, Hopkinson NS. Smoking and socioeconomic factors linked to acute exacerbations of COPD: analysis from an Asthma + Lung UK survey. BMJ Open Respir Res. 2022;9(1):1. doi:10.1136/bmjresp-2022-001290
26. Agboado G, Peters J, Donkin L. Factors influencing the length of hospital stay among patients resident in Blackpool admitted with COPD: a cross-sectional study. BMJ Open. 2012;2(5):2. doi:10.1136/bmjopen-2012-000869
27. Crisafulli E, Ielpo A, Barbeta E, et al. Clinical variables predicting the risk of a hospital stay for longer than 7 days in patients with severe acute exacerbations of chronic obstructive pulmonary disease: a prospective study. Respir Res. 2018;19(1):261. doi:10.1186/s12931-018-0951-4
28. Garcia-Aymerich J, Monsó E, Marrades RM, et al. Risk factors for hospitalization for a chronic obstructive pulmonary disease exacerbation. EFRAM study. Am J Respir Crit Care Med. 2001;164(6):1002–1007. doi:10.1164/ajrccm.164.6.2006012
29. Huang K, Zheng Z, Li W, et al. Sociodemographic correlates with prevalence of comorbidities in patients with chronic obstructive pulmonary disease: a study from a Chinese National Survey. Lancet Reg Health West Pac. 2024;42:100937. doi:10.1016/j.lanwpc.2023.100937
30. Jia C, Zhang C, Fang F, et al. Enjoying Breathing Program: a National Prospective Study Protocol to Improve Chronic Obstructive Pulmonary Disease Management in Chinese Primary Health Care. Int J Chron Obstruct Pulmon Dis. 2020;15:2179–2187. doi:10.2147/copd.S258479
31. Digitale JC, Martin JN, Glymour MM. Tutorial on directed acyclic graphs. J Clin Epidemiol. 2022;142:264–267. doi:10.1016/j.jclinepi.2021.08.001
32. Schisterman EF, Cole SR, Platt RW. Overadjustment bias and unnecessary adjustment in epidemiologic studies. Epidemiology. 2009;20(4):488–495. doi:10.1097/EDE.0b013e3181a819a1
33. Bridevaux PO, Probst-Hensch NM, Schindler C, et al. Prevalence of airflow obstruction in smokers and never-smokers in Switzerland. Eur Respir J. 2010;36(6):1259–1269. doi:10.1183/09031936.00004110
34. Institute for Health Metrics and Evaluation. GBD Compare. Available from:https://vizhub.healthdata.org/gbd-compare/.
35. King BA, Dube SR, Tynan MA. Current tobacco use among adults in the United States: findings from the National Adult Tobacco Survey. Am J Public Health. 2012;102(11):e93–e100. doi:10.2105/ajph.2012.301002
36. Zhang M, Yang L, Wang L, et al. Trends in smoking prevalence in urban and rural China, 2007 to 2018: findings from 5 consecutive nationally representative cross-sectional surveys. PLoS Med. 2022;19(8):e1004064. doi:10.1371/journal.pmed.1004064
37. Wang C, Yu F, Cao Z, et al. Exploring COPD Patient Clusters and Associations with Health-Related Quality of Life Using A Machine Learning Approach: a Nationwide Cross-Sectional Study. Engineering. 2025;50:220–228. doi:10.1016/j.eng.2025.05.005
38. Naito T, Inoue K, Namba S, et al. Machine learning reveals heterogeneous associations between environmental factors and cardiometabolic diseases across polygenic risk scores. Commun Med. 2024;4(1):181. doi:10.1038/s43856-024-00596-7
39. Yang T, Cai B, Cao B, et al. Exacerbation in patients with stable COPD in China: analysis of a prospective, 52-week, nationwide, observational cohort study (REAL). Ther Adv Respir Dis. 2023;17:17534666231167353. doi:10.1177/17534666231167353
40. Siddharthan T, Grigsby MR, Goodman D, et al. Association between Household Air Pollution Exposure and Chronic Obstructive Pulmonary Disease Outcomes in 13 Low- and Middle-Income Country Settings. Am J Respir Crit Care Med. 2018;197(5):611–620. doi:10.1164/rccm.201709-1861OC
41. Ponsonby AL, Couper D, Dwyer T, Carmichael A, Kemp A. Relationship between early life respiratory illness, family size over time, and the development of asthma and hay fever: a seven year follow up study. Thorax. 1999;54(8):664–669. doi:10.1136/thx.54.8.664
42. Aldridge RW, Pineo H, Fragaszy E, et al. Household overcrowding and risk of SARS-CoV-2: analysis of the Virus Watch prospective community cohort study in England and Wales. Wellcome Open Res. 2021;6:347. doi:10.12688/wellcomeopenres.17308.1
43. Badolo H, Bado AR, Hien H, Méda N, Susuman AS. Factors associated with mothers’ health care-seeking behaviours for childhood fever in Burkina Faso: findings from repeated cross-sectional household surveys. Glob Health Res Policy. 2022;7(1):37. doi:10.1186/s41256-022-00270-2
44. Worth H, Buhl R, Criée CP, Kardos P, Gückel E, Vogelmeier CF. In ‘real world’ patients with COPD, exacerbation history, and not blood eosinophils, is the most reliable predictor of future exacerbations. Respir Res. 2023;24(1):2. doi:10.1186/s12931-023-02311-x
45. Wedzicha JA, Brill SE, Allinson JP, Donaldson GC. Mechanisms and impact of the frequent exacerbator phenotype in chronic obstructive pulmonary disease. BMC Med. 2013;11:181. doi:10.1186/1741-7015-11-181
46. Shetty BSP, D’Souza G, Padukudru Anand M. Effect of Indoor Air Pollution on Chronic Obstructive Pulmonary Disease (COPD) Deaths in Southern Asia-A Systematic Review and Meta-Analysis. Toxics. 2021;9(4):85. doi:10.3390/toxics9040085
47. Pérez-Padilla R, Ramirez-Venegas A, Sansores-Martinez R. Clinical Characteristics of Patients With Biomass Smoke-Associated COPD and Chronic Bronchitis, 2004–2014. Chronic Obstr Pulm Dis. 2014;1(1):23–32. doi:10.15326/jcopdf.1.1.2013.0004
48. Camp PG, Ramirez-Venegas A, Sansores RH, et al. COPD phenotypes in biomass smoke- versus tobacco smoke-exposed Mexican women. Eur Respir J. 2014;43(3):725–734. doi:10.1183/09031936.00206112
49. Albadrani M. Socioeconomic disparities in mortality from indoor air pollution: a multi-country study. PLoS One. 2025;20(1):e0317581. doi:10.1371/journal.pone.0317581
50. van Smeden M, Lash TL, Groenwold RHH. Reflection on modern methods: five myths about measurement error in epidemiological research. Int J Epidemiol. 2020;49(1):338–347. doi:10.1093/ije/dyz251
51. Tang X, Lei J, Li W, et al. The Relationship Between BMI and Lung Function in Populations with Different Characteristics: a Cross-Sectional Study Based on the Enjoying Breathing Program in China. Int J Chron Obstruct Pulmon Dis. 2022;17:2677–2692. doi:10.2147/copd.S378247
52. Chittal P, Babu AS, Lavie CJ. Obesity paradox: does fat alter outcomes in chronic obstructive pulmonary disease? Copd. 2015;12(1):14–18. doi:10.3109/15412555.2014.915934
53. Kiss N, Prado CM, Daly RM, et al. Low muscle mass, malnutrition, sarcopenia, and associations with survival in adults with cancer in the UK Biobank cohort. J Cachexia, Sarcopenia Muscle. 2023;14(4):1775–1788. doi:10.1002/jcsm.13256
54. Chan SMH, Cerni C, Passey S, et al. Cigarette Smoking Exacerbates Skeletal Muscle Injury without Compromising Its Regenerative Capacity. Am J Respir Cell Mol Biol. 2020;62(2):217–230. doi:10.1165/rcmb.2019-0106OC
55. Golpe R, Martín-Robles I, Sanjuán-López P, et al. Differences in systemic inflammation between cigarette and biomass smoke-induced COPD. Int J Chron Obstruct Pulmon Dis. 2017;12:2639–2646. doi:10.2147/copd.S141068
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Fibrinogen, a Promising Marker to Evaluate Severity and Prognosis of Acute Exacerbation of Chronic Obstructive Pulmonary Disease: A Retrospective Observational Study
Sun W, Cao Z, Ma Y, Wang J, Zhang L, Luo Z
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:1299-1310
Published Date: 3 June 2022
Influences of Two FEV1 Reference Equations (GLI-2012 and GIRH-2017) on Airflow Limitation Classification Among COPD Patients
Wei D, Wang Q, Liu S, Tan X, Chen L, Tu R, Liu Q, Jia Y, Liu S
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2053-2065
Published Date: 2 September 2022
A Novel Metabolic Score for Predicting the Acute Exacerbation in Patients with Chronic Obstructive Pulmonary Disease
Peng L, You H, Xu MY, Dong ZY, Liu M, Jin WJ, Zhou C
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:785-795
Published Date: 5 May 2023
Are We Missing the Opportunity to Disseminate GOLD Recommendations Through AECOPD Discharge Letters?
Vukić Dugac A, Vergles M, Škrinjarić Cincar S, Bulat Kardum L, Lampalo M, Popović-Grle S, Ostojić J, Tokić Vuksan-Ćusa T, Vrbica Ž, Lozo Vukovac E, Tudorić N
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:985-993
Published Date: 26 May 2023
Prediction of Hospitalization and Mortality in Patients with Chronic Obstructive Pulmonary Disease with the New Global Initiative for Chronic Obstructive Lung Disease 2023 Group Classification: A Prospective Cohort and a Retrospective Analysis
Cheng W, Zhou A, Zeng Y, Lin L, Song Q, Liu C, Zhou Z, Peng Y, Yang M, Yang L, Chen Y, Cai S, Chen P
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:2341-2352
Published Date: 26 October 2023