Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 18
Are We Missing the Opportunity to Disseminate GOLD Recommendations Through AECOPD Discharge Letters?
Authors Vukić Dugac A ![]() , Vergles M, Škrinjarić Cincar S
, Vergles M, Škrinjarić Cincar S ![]() , Bulat Kardum L, Lampalo M
, Bulat Kardum L, Lampalo M ![]() , Popović-Grle S
, Popović-Grle S ![]() , Ostojić J
, Ostojić J ![]() , Tokić Vuksan-Ćusa T
, Tokić Vuksan-Ćusa T ![]() , Vrbica Ž
, Vrbica Ž ![]() , Lozo Vukovac E
, Lozo Vukovac E ![]() , Tudorić N
, Tudorić N
Received 16 February 2023
Accepted for publication 19 May 2023
Published 26 May 2023 Volume 2023:18 Pages 985—993
DOI https://doi.org/10.2147/COPD.S408307
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jill Ohar
Andrea Vukić Dugac,1,2 Mirna Vergles,3 Sanda Škrinjarić Cincar,4 Ljiljana Bulat Kardum,5 Marina Lampalo,1 Sanja Popović-Grle,1,2 Jelena Ostojić,6 Tatjana Tokić Vuksan-Ćusa,7 Žarko Vrbica,8,9 Emilija Lozo Vukovac,10 Neven Tudorić11
1Clinic for Respiratory Diseases, University Hospital Centre Zagreb, Zagreb, Croatia; 2School of Medicine, University of Zagreb, Zagreb, Croatia; 3Department of Pulmonology, Clinical Hospital Dubrava, Zagreb, Croatia; 4Faculty of Medicine, University of Osijek, Osijek, Croatia; 5Department of Pulmonology, Clinical Hospital Centre Rijeka, Rijeka, Croatia; 6Pulmonary Outpatient Clinic, Special Hospital for Pulmonary Diseases, Zagreb, Croatia; 7Department of Internal Medicine, Karlovac General Hospital, Karlovac, Croatia; 8Department of Internal Medicine, Dubrovnik General Hospital, Dubrovnik, Croatia; 9University Study Programme Nursing, University of Dubrovnik, Dubrovnik, Croatia; 10Department of Pulmonology, University Hospital Split, Split, Croatia; 11Pulmonary Outpatient Clinic, St. Catherine Specialty Hospital, Zagreb, Croatia
Correspondence: Neven Tudorić, St. Catherine Specialty Hospital, Branimirova Ul. 71E, Zagreb, 10000, Croatia, Tel +385915832449, Email [email protected]
Introduction: Acute exacerbations in chronic obstructive pulmonary disease (AECOPD) lead to poor outcomes and increased burden for patients and healthcare systems. The Global Initiative for COPD (GOLD) includes specific recommendations for AECOPD interventions, discharge criteria, and follow-up. Aligning the AECOPD discharge letters (DL) with GOLD guidelines could facilitate dissemination of recommendations among general practitioners (GPs).
Purpose: This study was conducted to assess the compliance of DL with the GOLD recommendations in Croatia.
Methods: Pre-pandemic DL of patients presenting for AECOPD to emergency room (ER) were analyzed and stratified by clinical decision to hospitalize (HDL) or discharge patients for outpatient treatment (ERDL). Experienced pulmonologists checked the information from DL against guidelines by using online study-specific questionnaires.
Results: In total, 225 HDL and 368 ERDL were analyzed. In most cases, the GOLD ABCD categories (85% HDL, 92% ERDL) or the spirometry-based degree of severity (90% HDL, 91% ERDL) were not included. The number of AEs in the previous year was recorded, but the specific frequent exacerbator phenotype not explicitly stated. The AE phenotype was included in two thirds of HDL and one third of ERDL. The blood eosinophil count was frequently available, but not considered decision-relevant information. Adjustments of previous maintenance therapy, mostly escalation, were recommended in 58.4% HDL and 27.9% ERDL, respectively. Education on proper use of inhalers was recommended only in 15.6% of HDL. Smoking cessation measures were advised in 23.1% HDL and 7.9% ERDL; pulmonary rehabilitation in 35.6% HDL and 0.8% ERDL. Early follow-up was frequently advised (> 50%), but rarely appointed.
Conclusion: Significant deficiencies in compliance with the GOLD guidelines were identified, translating into a missed opportunity for GPs to become acquainted with GOLD recommendations. These findings emphasize the necessity to increase compliance with guidelines first at specialist level and consequent standardization of DL.
Keywords: COPD, GOLD guidelines, acute exacerbation, discharge record
Introduction
For decades, chronic obstructive pulmonary disease (COPD) has been placed among the leading causes of morbidity and mortality worldwide.1–3 Given the widespread exposure to risk factors for COPD, aging population and no disease modifying treatments, the COPD burden is expected to further increase.4,5 On these grounds, the Global Initiative for Chronic Obstructive Lung Disease (GOLD) was founded in 1998 aiming to provide clinicians with systematic, scientifically sound recommendations for COPD management.6 The first GOLD report was published in 2001 and has been updated regularly since.6,7 This comprehensive state of the art document, also used in Croatia, provides an evidence-based framework for the outpatient and inpatient management of COPD patients.
The adoption of GOLD recommendations in clinical practice is challenging and significantly variable: in Germany, most lung specialists increased their adherence to updated guideline recommendations over time,8 but other reports across Europe were less enthusiastic.9–12 Moreover, the adoption of GOLD guidelines seems to be particularly insufficient in primary healthcare.13–18 These studies indicated that misdiagnosis, poor use of spirometry, insufficient symptom evaluation, and misalignment of treatment regimens with GOLD recommendations are common and primarily explained by the lack of awareness of the GOLD initiative.16,17 Non-adherence to guidelines has been shown to have significant negative repercussions on patients’ outcomes and healthcare systems.19,20 For many countries,21 including Croatia, where the basic care for patients with COPD is the task of family practitioners, these findings become particularly important.
Educational programs and local, concise guidelines based on GOLD have been cited in the literature as modalities to improve their uptake in primary care.13,17 Also, simpler solutions like automated tools assisting physicians in generating discharge recommendations using GOLD guidelines for patients admitted with acute exacerbations of their COPD have been explored, showing effectiveness in real-life that translated to improved patient’s care.22
To see to what extent the discharge letters (DL) issued for acute exacerbations in COPD (AECOPD) in Croatian hospitals follow the GOLD recommendations, we conducted this medical chart review study. To evaluate the adherence to GOLD recommendations, we checked the inclusion in the discharge records of specific information such as disease severity, outcomes, phenotype, inhaler treatments, and technique.
Methods
Study Design
This was a retrospective, observational study assessing the discharge records generated in emergency room (ER) or following hospitalization in 5 major academic teaching hospitals and 3 county hospitals in Croatia, in the pre-pandemic period October 2019 and February 2020. Based on the clinical decision to hospitalize or discharge the patients for outpatient treatment following the presentation to ER, the DL were classified into hospital DL (HDL) or ERDL. Consecutive HDL and ERDL were analyzed using questionnaires specifically designed by the authors of the present study. Only data from completely filled questionnaires were analyzed. Experienced hospital pulmonologists reviewed the DL and completed the study on-line questionnaires (Supplementary Tables 1 and 2). The GOLD in use at the time of the study design was GOLD 2019.23
The study complies with the Declaration of Helsinki and its conduct was approved by the Ethics Committees of all participating hospitals (University Hospital Centre Zagreb, Zagreb; Clinical Hospital Dubrava, Zagreb; University Hospital Osijek, Osijek; Clinical Hospital Centre Rijeka, Rijeka; University Hospital Split, Split; Special Hospital for Pulmonary Diseases, Zagreb; Karlovac General Hospital, Karlovac; Dubrovnik General Hospital, Dubrovnik). No information allowing patient identification was collected. No informed consent was required because anonymized data from electronic medical records were used.
Study Questionnaires
The questionnaires collected data on patient demographics (sex, age), ER admission details (referral pathway, healthcare practitioner performing the initial examination in the ER and referral diagnosis), smoking status, COPD severity, comorbidities, previous COPD treatment, spirometry (history and forced expiratory volume [FEV1]), exacerbation history (previous 12 months before the current episode, previous AECOPD, and frequent exacerbator phenotype), current exacerbation details (symptoms, investigations performed, blood eosinophils information, treatment in ER), and other specific data (COPD stage, AE severity, AE etiology, blood eosinophils, probable phenotype of AE and education on inhaler use, treatments recommended at discharge and general recommendations made).
The questionnaire collecting data from HDL included additional details on the current hospitalization for AE (reasons for hospital admission, unit, and duration of hospitalization, pharmacological and non-pharmacological interventions and procedures, blood eosinophils, and hospitalization outcome).
Data Analysis
Descriptive statistics was used for data analysis. Categorical variables are presented as numbers and proportions (%), and continuous as mean and standard deviation (SD) or median and interquartiles (IQR) depending on the type of distribution. Statistical analysis was performed using MedCalc® Statistical Software version 20.027 (MedCalc Software Ltd, Ostend, Belgium; https://www.medcalc.org; 2022).
Results
In total, 593 DL with AECOPD as initial diagnosis were included in this analysis: 368 (62.1%) ERDL and 225 (37.9%) HDL. Except for the type of referral (almost half of hospitalized patients were brought by ambulance, while one third of the patients treated in the ER were referred via GPs), the rest of patients’ characteristics were similar among groups (Table 1).
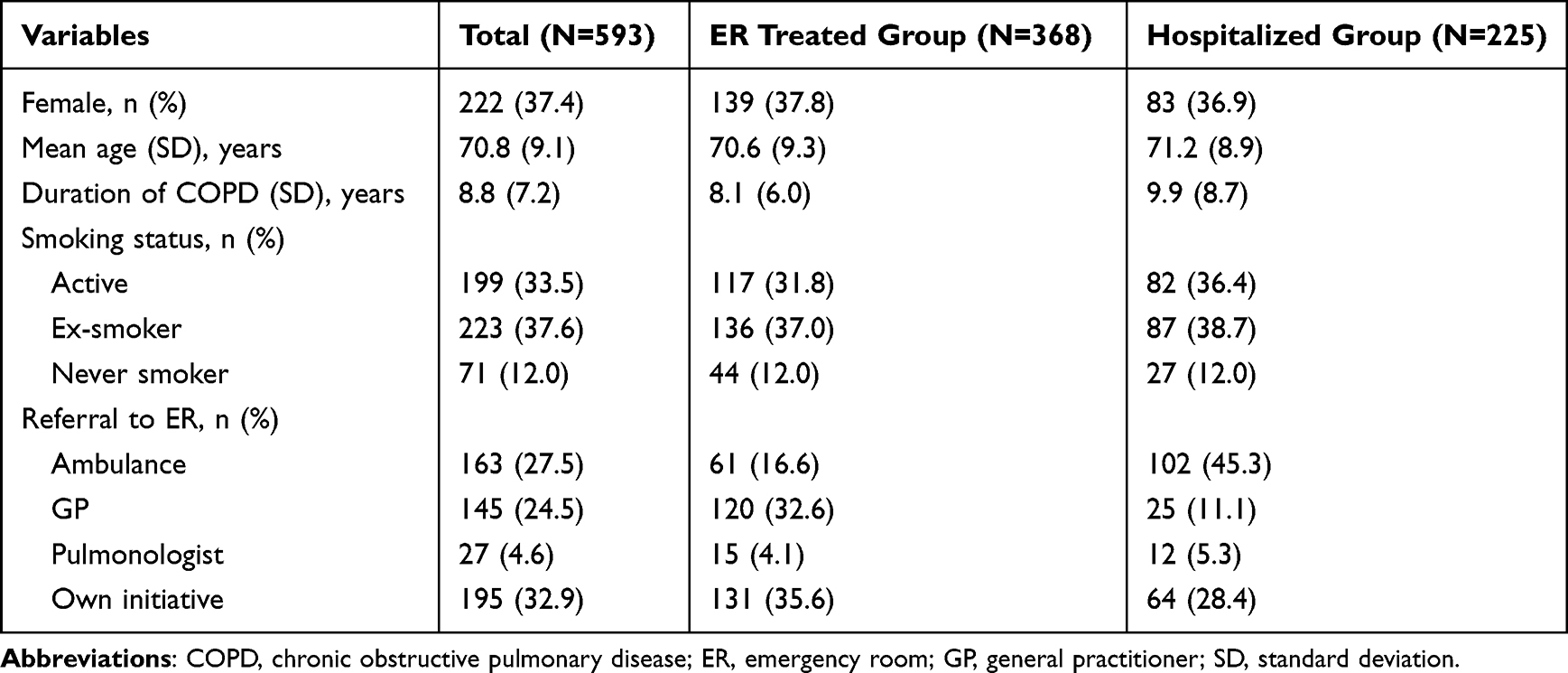 |
Table 1 Characteristics of the Study Population |
The degree of severity (GOLD grades 1–4) and the ABCD category designation had a low reporting rate (<15% in HDL and <10% in ERDL) (Table 2). The severity of COPD as part of the final discharge diagnosis was stated in 25.8% of HDL and only 5.7% of ERDL. The number of AEs in the previous year was stated in around one third of HDL and ERDL. The phenotype of the frequent exacerbator (FE) was not explicitly specified in any DL; however, based on available data about AEs in the previous year, 33.3% of the hospitalized patients and 19.6% of those discharged from ER, respectively, could have been classified as having FE phenotype (ie, at least 2 AEs in the previous year). The severity of current AECOPD was rarely pointed out in the leading discharge diagnosis, especially in ERDL. In the ERDL, the AE etiology (phenotype) was reported in 33.7% of ERDL and 62.2% HDL. Using the data reported, the AE phenotype could be determined in almost all HDL.
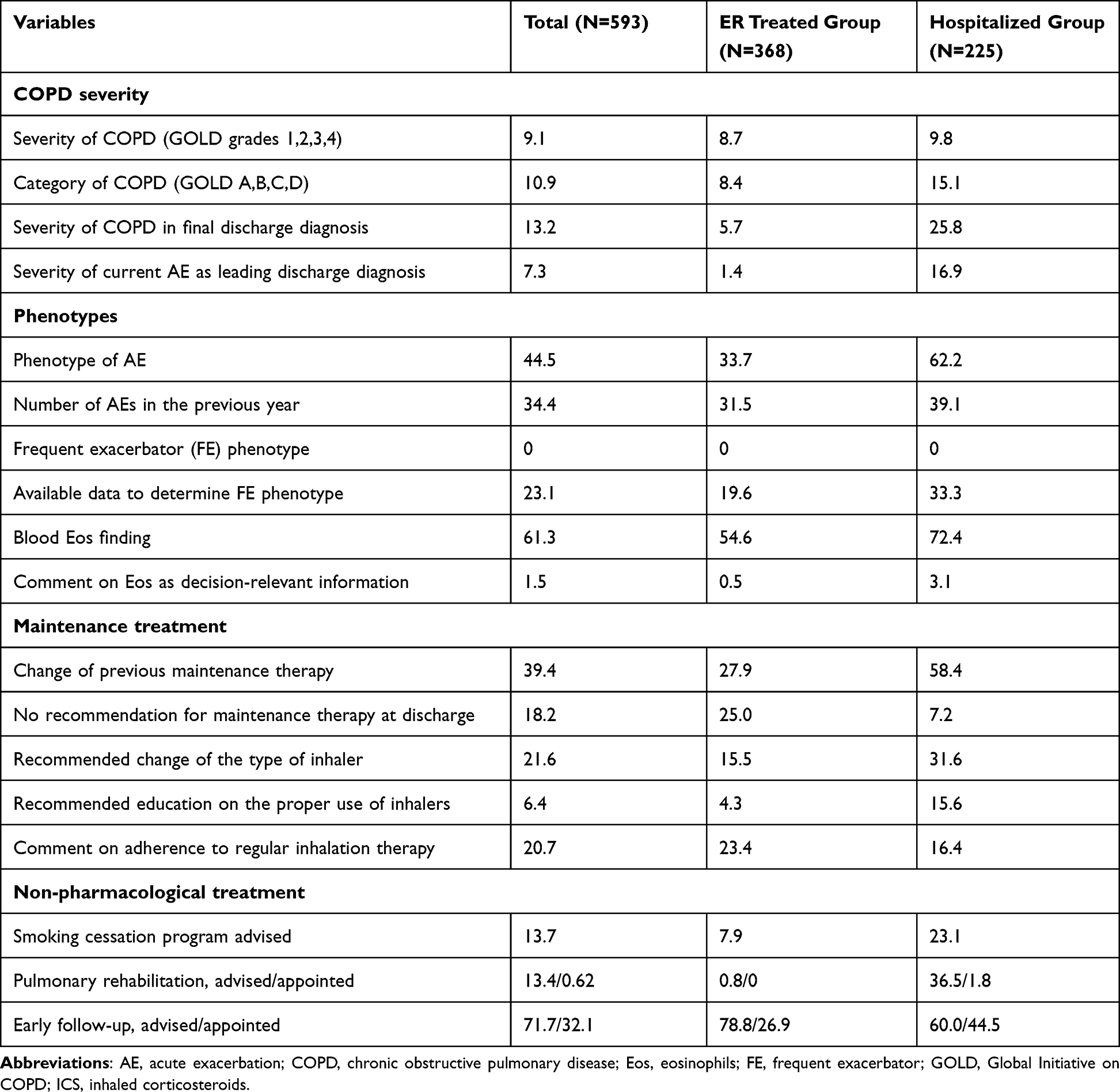 |
Table 2 Specific Items of Interest Stated in Discharge Letters and Used to Assess the Adherence to the GOLD Recommendations. All Results are Expressed as Percentages (%) |
The number of blood eosinophils (Eos) was frequently specified, but eosinophilia was rarely pointed out as important information. The median Eos count was 34 (IQR 0–116.5) cells/μL in hospitalized patients (43.6% <100 Eos, 15.3% 100–300 Eos, and 6.1% >300 Eos), and 107 (IQR 30–130) cells/μL (22.6% <100 Eos, 38.4% 100–300 Eos, and 17.9% >300 Eos) in patients discharged from ER.
Overall, around 10% of patients (12.0% of hospitalized and 8.4% of patients discharged from ER) were not receiving any COPD medication prior to hospital/ER admission. Adjustments of previous maintenance therapy were often recommended in hospitalized patients, mainly escalation to triple therapy (TT) and reductions of inhaled corticosteroids/long-acting beta-agonists (ICS/LABA), LAMA (long-acting muscarinic antagonists) and LABA/LAMA recommendations (Figure 1A). In patients discharged from ER, adjustments of previous therapy were less frequent, with reductions in ICS/LABA and LABA/LAMA and increases in TT recommendations at discharge (Figure 1B). Overall, one fifth (18.2%) of DL had no treatment recommendations (7.2% of HDL, and 25.0% of ERDL).
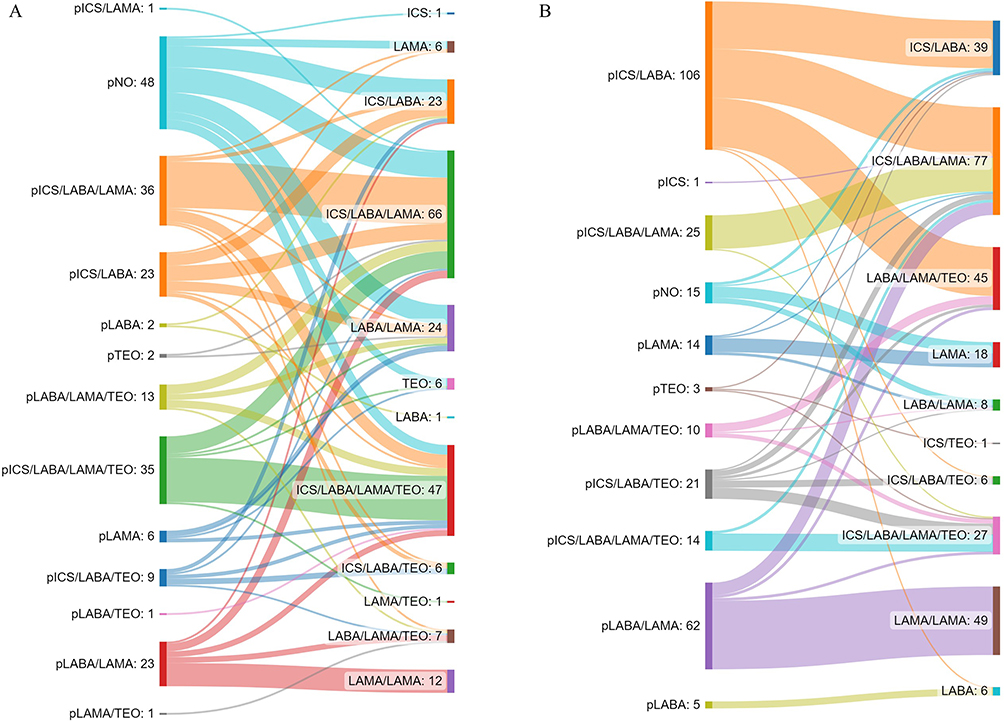 |
Figure 1 Changes made at discharge in maintenance treatment recommendations. (A) Hospitalized patients; (B) patients discharged from emergency room. Abbreviations: ICS, inhaled corticosteroids; LABA, long-acting beta-agonists; LAMA, long-acting muscarinic agonists. Note: Patients who received LAMA + LABA/ICS or LABA/LAMA + ICS concomitantly were included in the triple therapy group. |
The type of inhaler used was indicated in 50.7% of HDL and 68.7% of ERDL, while the change of the type of inhaler was suggested in a third of HDL and 15.5% of ERDL, respectively. The inhalation technique was recorded as checked in one fifth of hospitalized patients (18.7%), and education on the proper use of inhalers was recommended in 15.6% of patients. Education on the proper use of inhalers was suggested only in 4.3% of discharge letters.
Pulmonary rehabilitation was recommended in one third of hospitalized patients and <1% of patients discharged from ER, but only 4 hospitalized patients (<2%) received an appropriate referral for scheduled rehabilitation. Although rarely recommended, vaccination was advised only in case of hospitalized patients (8.9% against influenza, 1.8% against pneumococcus). Early follow-up (2-week) was advised in two thirds of HDL, and a referral was issued in almost half of these patients (44.5%). In ERDL, the 4-week control was recommended in most patients (78.8%), of whom 26.9% received an appropriate referral.
Discussion
To our knowledge, this is the first structured evaluation of discharge records conducted in Croatia in patients with COPD presenting to emergency departments, specifically designed to evaluate adherence to the GOLD recommendations.6,23 In this data set, we assessed information on items that GOLD considers particularly important for the appropriate management of COPD: airflow limitation severity and grades’ categorization, frequency of AEs, proper COPD phenotyping, and appropriate prescribing of inhaled treatments, mainly ICS. The results of this study, like some others, showed a significant lack of adherence to GOLD AECOPD recommendations in use at that time.22,24,25
Previous and current GOLD reports require categorization of COPD based on spirometry, severity of symptoms, and exacerbations frequency, which was neglected by most of DL assessed in this study.6,23 Data on previous spirometry (FEV1) were often missing, as well as notes on spirometry eventually performed during hospitalization. Although not currently recommended, spirometry during hospitalization in clinically stabilized patients may provide useful data, especially when compared with post-discharge outpatient spirometry.26–28
Exacerbations have always been a crucial component of the risk assessment in COPD patients. Given their clinical relevance, more emphasis is placed on exacerbations in the 2023 GOLD edition, and the ABCD assessment tool has been revised to ABE tool.6 It is recognized that rate of subsequent exacerbations is accelerated by each past exacerbation, therefore the prompt recognition of AEs is of utmost importance for adequate management and consequent reduction of negative consequences.29 Frequent exacerbators are characterized by more severe symptoms, increased frequency of hospitalizations, and faster disease progression.30 Identification of these patients and timely introduction of the maintenance therapy that includes ICS should be clinical priority.31 The number of AEs was reported only in one third of DL, while none stated explicitly the phenotype of frequent exacerbator. The severity of the AECOPD was also rarely noted. Although hospitalization itself may imply the gravity of the event, the severity of current AE as the leading reason for admission was included only in one third of HDL.
GOLD emphasizes a favorable response to ICS-containing maintenance therapy in patients with an increased number of blood eosinophils, especially in those with concomitant increased risk of AE.32–35 The number of eosinophils in peripheral blood was reported in most DL, but the finding was extremely rarely emphasized in the records, despite the high number of patients with significant eosinophilia (>300 Eos/μL).
In a substantial proportion of patients, previous maintenance therapy was escalated mostly to TT (ICS/LABA/LAMA), although TT was suggested in less than half of discharged patients. Previous reports showed the benefits of prompt introduction of TT after AECOPD as compared to TT delayed start, ie, significant reduction of exacerbations and healthcare costs.36,37 Reducing exacerbations is a key factor in decreasing COPD-related deaths, and current GOLD edition includes evidence supporting TT as the only pharmacotherapy reducing mortality.6 In our data set, we noticed that methylxanthines, which are not the mainstay of respiratory maintenance therapy, were often used and not further discontinued at discharge, although all inhaled COPD drugs are available in Croatia. It is generally accepted, and clearly stated in GOLD, that ICS are overutilized in all categories of COPD patients, and a more targeted use of ICS is recommended based on documented benefits of ICS withdrawal.6,38 We could not assess the relevance of withdrawal rate in our study because ICS weaning is usually performed in an outpatient setting. Surprisingly, we identified that no treatment recommendation was given at discharge in 7% of HDL and 25% of ERDL. Consequently, GPs had not received any specialist opinion on post-AECOPD maintenance therapy for one fifth of patients.
We also analyzed the adequacy of recommendations on non-pharmacological measures. Smoking cessation was documented to reduce mortality in patients with COPD, also having the greatest capacity to influence the natural history of the disease.6 With effective resources, long-term quitting success rates of up to 25% could be achieved.38 Therefore, smoking cessation recommendations should be part of every discharge plan,6,39,40 but it was advised only in a quarter of discharge notes, with poor rates of appointments for smoking cessation services. Similarly, pulmonary rehabilitation (PR) helps improve exercise capacity and quality of life in COPD patients by reducing fatigue and dyspnea.41 In our dataset, one third of DL further recommended PR, and only 4 patients were provided actual referrals. Comparably low rates of referral to PR have been reported in other studies.42 Vaccination against influenza and pneumococcus was advised even less, only in 10% of overall DL, although the finding is comparable to other reports.22,25
Finally, GOLD emphasizes the importance of follow-up visits after an AECOPD event. Missing the 30-day follow-up visit to pulmonologist was associated with a significantly increased risk for ER visit and re-admission within 3 months from discharge.43,44 Even though many DL included recommendations for early follow-up, only a few patients received an appropriate referral.
In general, the inaccuracy seen in AECOPD discharge notes and the lack of information continuity required in the transition of care result in worse patient outcomes, including a high re-admission rate.45 In this regard, various improvement measures have been proposed. For example, Epstein et al designed and successfully implemented a decision support tool to automatically generate discharge recommendations based on GOLD guidelines.22 These led to substantial improvements of recommendations for long-acting medications, smoking cessation, vaccination and pulmonologist check-up. Another attempt to optimize management after an AECOPD is to use care bundle, which is a set of structured evidence-based practices directed to improve patient outcomes in common chronic conditions.46 The most frequently used individual interventions were proper inhaler technique demonstrations, educational programs on self-management, assessments/referrals for PR, arrangement of outpatient follow-ups, and referrals to a smoking cessation program.47,48 Only few studies focused on COPD discharge care bundles in ER, probably due to complexity of management and pressure on clinicians’ to deliver acute medical care. However, adherence to a COPD care bundle in patients treated for an AE at ER was shown to significantly reduce 30-day ER re-visits.48 Reports of the effectiveness of hospital discharge care bundles are much more numerous, but not uniform in conclusions. In two single-center, randomized trials from USA and France, discharge care bundles proved insufficient to reduce the 30-day risk of re-admission, ER visits or death rate.49,50 On the other hand, two review studies reported that hospital discharge care bundles led to fewer re-admissions but did not significantly improve mortality or quality of life.46,47 Accordingly, GOLD states that no standards can be applied currently, and includes discharge criteria, and recommendations for early and late follow-ups after AECOPD.6
The retrospective nature of this study limits the generalizability of results. Perhaps more procedures, interventions, and recommendations were provided to patients, but not recorded in the discharge records. Although collected in a relatively short and specific pre-pandemic COVID-19 period, these data are the first structured nation-wide attempt to measure adherence to guidelines. The findings will serve as reference for initiating discussions at local level with the aim to improve care after AECOPD discharge. Standardizing DL and follow-up studies to measure their effectiveness are required.
Conclusion
We identified significant insufficiencies in the surveyed discharge records, which were not compliant with the GOLD guidelines. The lack of GOLD-based recommendations is concerning because it could jeopardize the continuity of care. This also translates into a missed opportunity for GPs to become familiar with and adhere to the GOLD recommendations. Our findings emphasize the necessity to increase compliance to guidelines first at specialist level, so that simple tools like discharge records can adequately contribute to improving COPD care.
Acknowledgments
This manuscript presents independent work by a panel of experts. The views and opinions expressed by the authors of this publication are their own and do not necessarily reflect the overall situation in any specific hospital. Medical writing support, which was in accordance with Good Publication Practice (GPP3) guidelines was provided by Professor Davor Plavec, MD, PhD (Zagreb, Croatia) and funded by AstraZeneca Croatia. Editorial assistance at various stages of the manuscript was provided by Ana Maria Iordan, MD, MSc (Bucharest, Romania), and funded by AstraZeneca Croatia. The logistical and medical writing support was funded by AstraZeneca Croatia.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lozano R, Naghavi M, Foreman K, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the global burden of disease study 2010. Lancet. 2012;380(9859):2095–2128. doi:10.1016/S0140-6736(12)61728-0
2. Ford ES. Trends in mortality from chronic obstructive pulmonary disease among adults in the United States. Chest. 2015;148(4):962–970. doi:10.1378/chest.14-2311.Trends
3. World Health Organization. Chronic obstructive pulmonary disease (COPD); 2020. Available from: https://www.who.int/news-room/fact-sheets/detail/chronic-obstructive-pulmonary-disease-(copd).
4. Adeloye D, Song P, Zhu Y, Campbell H, Sheikh A, Rudan I. Global, regional, and national prevalence of, and risk factors for, chronic obstructive pulmonary disease (COPD) in 2019: a systematic review and modelling analysis. Lancet Respir Med. 2022;10(5):447–458. doi:10.1016/S2213-2600(21)00511-7
5. Gross NJ, Barnes PJ. New therapies for asthma and chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2017;195(2):159–166. doi:10.1164/rccm.201610-2074PP
6. Global Initiative for Chronic Obstructive Lung Disease. Global Strategy for th eDiagnosis, management and prevention of chronic obstructive pulmonary disease (2023 Report); 2023. Available from: https://goldcopd.org/2023-gold-report-2/.
7. Rodriguez-Roisin R, Rabe KF, Vestbo J, Vogelmeier C, Agustí A. Global initiative for chronic obstructive lung disease (GOLD) 20th Anniversary: a brief history of time. Eur Respir J. 2017;50:1. doi:10.1183/13993003.00671-2017
8. Glaab T, Vogelmeier C, Hellmann A, Buhl R. Guideline-based survey of outpatient COPD management by pulmonary specialists in Germany. Int J COPD. 2012;7:101–108. doi:10.2147/COPD.S27887
9. Marmy JL, Diedrich JP, Cadus C, et al. Adherence to GOLD recommendations among Swiss pulmonologists and general practitioners. COPD J Chronic Obstr Pulm Dis. 2020;18(1):9–15. doi:10.1080/15412555.2020.1859469
10. Palmiotti GA, Lacedonia D, Schino P, et al. Adherence to GOLD Italy.pdf; 2018:2455–2462.
11. Tzanakis N, Koulouris N, Dimakou K, et al. Classification of COPD patients and compliance to recommended treatment in Greece according to GOLD 2017 report: the RELICO study. BMC Pulm Med. 2021;21(1):1–9. doi:10.1186/s12890-021-01576-6
12. Rajnoveanu RM, Rajnoveanu AG, Ardelean AB, et al. Pulmonologists adherence to the chronic obstructive pulmonary disease gold guidelines: a goal to improve. Med. 2020;56(9):1–13. doi:10.3390/medicina56090422
13. Albitar HAH, Iyer VN. Adherence to global initiative for chronic obstructive lung disease guidelines in the real world: current understanding, barriers, and solutions. Curr Opin Pulm Med. 2020;26(2):149–154. doi:10.1097/MCP.0000000000000655
14. Surani S, Aiyer A, Eikermann S, et al. Adoption and adherence to chronic obstructive pulmonary disease GOLD guidelines in a primary care setting. SAGE Open Med. 2019;7:205031211984222. doi:10.1177/2050312119842221
15. Maniscalco M, Martucci M, Fuschillo S, de Felice A, D’Anna SE, Cazzola M. A case scenario study on adherence to COPD GOLD recommendations by general practitioners in a rural area of southern Italy: the “progetto PADRE”. Respir Med. 2020;170:105985. doi:10.1016/j.rmed.2020.105985
16. Yawn BP, Wollan PC. Knowledge and attitudes of family physicians coming to COPD continuing medical education. Int J COPD. 2008;3(2):311–317. doi:10.2147/copd.s2486
17. Sehl J, O’Doherty J, O’Connor R, O’Sullivan B, O’Regan A. Adherence to COPD management guidelines in general practice? A review of the literature. Ir J Med Sci. 2018;187(2):403–407. doi:10.1007/s11845-017-1651-7
18. Jochmann A, Neubauer F, Miedinger D, et al. General practitioners’ adherence to the COPD GOLD guidelines: baseline data from the Swiss COPD Cohort Study. Swiss Med Wkly. 2010;140:1–8. doi:10.4414/smw.2010.13053
19. Jiang YQ, Zhu YX, Chen XL, et al. Impact of adherence to GOLD guidelines on 6-minute walk distance, MRC dyspnea scale score, lung function decline, quality of life, and quality-adjusted life years in a Shanghai suburb. Genet Mol Res. 2015;14(3):8861–8870. doi:10.4238/2015.August.3.9
20. Mannino DM, Yu T-C, Zhou H, Higuchi K. GOLD-adherent prescribing and resource utilization journal.copdfoundation.org JCOPDF ©. J Copd F. 2015;2(3):223–235. doi:10.15326/jcopdf.2.3.2014.0151
21. Kayyali R, Odeh B, Frerichs I, et al. COPD care delivery pathways in five European Union countries: mapping and health care professionals’ perceptions. Int J COPD. 2016;11(1):2831–2838. doi:10.2147/COPD.S104136
22. Epstein D, Barak-Corren Y, Isenberg Y, Berger G. Clinical decision support system: a pragmatic tool to improve acute exacerbation of COPD discharge recommendations. COPD J Chronic Obstr Pulm Dis. 2019;16(1):18–24. doi:10.1080/15412555.2019.1593342
23. López-Campos JL, Soler-Cataluña JJ, Miravitlles M; Global Initiative for Chronic Obstructive Lung Disease (2019 Report). Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease 2019 report: future challenges. Arch Bronconeumol. 2020;56(2):65–67. goldcopd.org. doi:10.1016/j.arbr.2019.06.014
24. Fano V, D’Ovidio M, Del Zio K, et al. [The role of the quality of hospital discharge records on the comparative evaluation of outcomes: the example of chronic obstructive pulmonary disease (COPD)]. TT - Ruolo della qualita delle schede di dimissione ospedaliera nella valutazione co. Epidemiol Prev. 2012;36:172–179. Italian.
25. Migone C, O’Connor M, Kelly E, McDonnell TJ. Patients hospitalised with an acute exacerbation of COPD: is there a need for a discharge bundle of care? Ir Med J. 2015;108:9.
26. Rea H, Kenealy T, Adair J, Robinson E, Sheridan N. Spirometry for patients in hospital and one month after admission with an acute exacerbation of COPD. Int J COPD. 2011;6(1):527–532. doi:10.2147/COPD.S24133
27. Fernández-Villar A, Represas-Represas C, Mouronte-Roibás C, et al. Reliability and usefulness of spirometry performed during admission for COPD exacerbation. PLoS One. 2018;13(3):1–12. doi:10.1371/journal.pone.0194983
28. Loh CH, Genese FA, Kannan KK, Lovings TM, Peters SP, Ohar JA. Spirometry in hospitalized patients with acute exacerbation of COPD accurately predicts post discharge airflow obstruction. Chronic Obstr Pulm Dis. 2018;5(2):124–133. doi:10.15326/jcopdf.5.2.2017.0169
29. Suissa S, Dell’Aniello S, Ernst P. Long-term natural history of chronic obstructive pulmonary disease: severe exacerbations and mortality. Thorax. 2012;67(11):957–963. doi:10.1136/thoraxjnl-2011-201518
30. Hurst JR, Vestbo J, Anzueto A, et al. Susceptibility to exacerbation in chronic obstructive pulmonary disease. N Engl J Med. 2010;363(12):1128–1138. doi:10.1056/nejmoa0909883
31. McGarvey L, Lee AJ, Roberts J, Gruffydd-Jones K, McKnight E, Haughney J. Characterisation of the frequent exacerbator phenotype in COPD patients in a large UK primary care population. Respir Med. 2015;109(2):228–237. doi:10.1016/j.rmed.2014.12.006
32. Bafadhel M, McKenna S, Terry S, et al. Acute exacerbations of chronic obstructive pulmonary disease: identification of biologic clusters and their biomarkers. Am J Respir Crit Care Med. 2011;184(6):662–671. doi:10.1164/rccm.201104-0597OC
33. Miravitlles M, Calle M, Molina J, et al. Spanish COPD Guidelines (GesEPOC) 2021: updated Pharmacological treatment of stable COPD. Arch Bronconeumol. 2022;58(1):69–81. doi:10.1016/j.arbres.2021.03.005
34. Proboszcz M, Mycroft K, Paplinska-Goryca M, et al. Relationship between blood and induced sputum eosinophils, bronchial hyperresponsiveness and reversibility of airway obstruction in mild-to-moderate chronic obstructive pulmonary disease. COPD J Chronic Obstr Pulm Dis. 2019;16(5–6):354–361. doi:10.1080/15412555.2019.1675150
35. Hastie AT, Martinez FJ, Curtis JL, et al. Association of sputum and blood eosinophil concentrations with clinical measures of COPD severity: an analysis of the SPIROMICS cohort. Lancet Respir Med. 2017;5(12):956–967. doi:10.1016/S2213-2600(17)30432-0
36. Bogart M, Glassberg MB, Reinsch T, Stanford RH. Impact of prompt versus delayed initiation of triple therapy post COPD exacerbation in a US-managed care setting. Respir Med. 2018;145:138–144. doi:10.1016/j.rmed.2018.10.013
37. Mannino D, Bogart M, Germain G, et al. Benefit of prompt versus delayed use of single-inhaler fluticasone Furoate/Umeclidinium/ Vilanterol (FF/UMEC/VI) following a COPD exacerbation. Int J COPD. 2022;17:491–504. doi:10.2147/COPD.S337668
38. van Eerd EAM, van der Meer RM, van Schayck OCP, Kotz D. Smoking cessation for people with chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2016;2016:8. doi:10.1002/14651858.CD010744.pub2
39. Reis AJ, Alves C, Furtado S, Ferreira J, Drummond M, Robalo-Cordeiro C. COPD exacerbations: management and hospital discharge. Pulmonology. 2018;24(6):345–350. doi:10.1016/j.pulmoe.2018.06.006
40. Hopkinson NS, Englebretsen C, Cooley N, et al. Designing and implementing a COPD discharge care bundle. Thorax. 2012;67(1):90–92. doi:10.1136/thoraxjnl-2011-200233
41. Jácome C, Marques A. Pulmonary rehabilitation for mild COPD: a systematic review. Respir Care. 2014;59(4):588–594. doi:10.4187/respcare.02742
42. Jones SE, Green SA, Clark AL, et al. Pulmonary rehabilitation following hospitalisation for acute exacerbation of COPD: referrals, uptake and adherence. Thorax. 2014;69(2):181–182. doi:10.1136/thoraxjnl-2013-204227
43. Sharma G, Kuo YF, Freeman JL, Zhang DD, Goodwin JS. Outpatient follow-up visit and 30-day emergency department visit and readmission in patients hospitalized for chronic obstructive pulmonary disease. Arch Intern Med. 2010;170(18):1664–1670. doi:10.1001/archinternmed.2010.345
44. Rachel G, Amalia L, Kalcheim DO, Karp Erez MN, Maimon N. The association between hospital readmission and pulmonologist follow-up visits in patients with chronic obstructive pulmonary disease. Chest. 2015;148(2):375–381. doi:10.1378/chest.14-1453
45. Dummer J, Stokes T. Improving continuity of care of patients with respiratory disease at hospital discharge. Breathe. 2020;16(3):1–8. doi:10.1183/20734735.0161-2020
46. Ospina MB, Mrklas K, Deuchar L, et al. A systematic review of the effectiveness of discharge care bundles for patients with COPD. Thorax. 2017;72(1):31–39. doi:10.1136/thoraxjnl-2016-208820
47. Gómez-Angelats E, Sánchez C. Care bundles after discharging patients with chronic obstructive pulmonary disease exacerbation from the emergency department. Med Sci. 2018;6(3):63. doi:10.3390/medsci6030063
48. Zafar MA, Loftus TM, Palmer JP, et al. COPD care bundle in emergency department observation unit reduces emergency department revisits. Respir Care. 2020;65(1):1–10. doi:10.4187/respcare.07088
49. Jennings JH, Thavarajah K, Mendez MP, Eichenhorn M, Kvale P, Yessayan L. Predischarge bundle for patients with acute exacerbations of COPD to reduce readmissions and ED visits: a randomized controlled trial. Chest. 2015;147(5):1227–1234. doi:10.1378/chest.14-1123
50. Cousse S, Gillibert A, Salaün M, Thiberville L, Cuvelier A, Patout M. Efficacy of a home discharge care bundle after acute exacerbation of COPD. Int J COPD. 2019;14:289–296. doi:10.2147/COPD.S178147
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Fibrinogen, a Promising Marker to Evaluate Severity and Prognosis of Acute Exacerbation of Chronic Obstructive Pulmonary Disease: A Retrospective Observational Study
Sun W, Cao Z, Ma Y, Wang J, Zhang L, Luo Z
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:1299-1310
Published Date: 3 June 2022
Influences of Two FEV1 Reference Equations (GLI-2012 and GIRH-2017) on Airflow Limitation Classification Among COPD Patients
Wei D, Wang Q, Liu S, Tan X, Chen L, Tu R, Liu Q, Jia Y, Liu S
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2053-2065
Published Date: 2 September 2022
A Novel Metabolic Score for Predicting the Acute Exacerbation in Patients with Chronic Obstructive Pulmonary Disease
Peng L, You H, Xu MY, Dong ZY, Liu M, Jin WJ, Zhou C
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:785-795
Published Date: 5 May 2023
Paradigm Shift in the Treatment of Chronic Obstructive Pulmonary Disease Improves Patient Outcomes
Huang YJ, Wang KY, Chien WC, Chung CH, Kao LT, Kao S, Chian CF
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:1965-1972
Published Date: 17 June 2025
Sociodemographic Determinants of Hospitalized Exacerbations in Exposure-Defined COPD Phenotypes: A Nationwide Prospective Cohort Study in China
Zheng Z, Tang X, Li W, Niu H, Dong F, Yan J, Shi M, Cui Y, Huang T, Han Z, Peng Y, Su R, Wang C, Russell RE, Yang T, Huang K
International Journal of Chronic Obstructive Pulmonary Disease 2026, 21:606977
Published Date: 5 June 2026