Back to Journals » OncoTargets and Therapy » Volume 19
Sintilimab-Induced Sequential Multi-System Severe Immune-Related Adverse Events in an Elderly Patient with Esophageal Squamous Cell Carcinoma: A Case Report and Literature Review
Authors Xia X, Yu T, Sun H, Li J, Liu F, Zhu X
Received 9 March 2026
Accepted for publication 30 June 2026
Published 9 July 2026 Volume 2026:19 606668
DOI https://doi.org/10.2147/OTT.S606668
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Sanjay Singh
Xi Xia,1,* Ting Yu,1,* Hui Sun,1 Jian Li,1 Fengjun Liu,1 Xin Zhu2
1Department of Infectious Diseases, Affiliated Hospital of North Sichuan Medical College, Nanchong, Sichuan, People’s Republic of China; 2Department of Otorhinolaryngology and Head & Neck Surgery, Affiliated Hospital of North Sichuan Medical College, Nanchong, Sichuan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xin Zhu, Department of Otorhinolaryngology and Head & Neck Surgery, Affiliated Hospital of North Sichuan Medical College, Nanchong, Sichuan, People’s Republic of China, Email [email protected]
Abstract: Immune checkpoint inhibitors (ICIs) can induce a spectrum of immune-related adverse events (irAEs), yet sequential, multi-organ severe irAEs remain uncommon and challenging to manage. We present a 78-year-old male patient with esophageal squamous cell carcinoma, suspected to have developed continuous, life-threatening irAEs involving the liver, bone marrow, and lungs after receiving sintilimab combined with chemotherapy. All events were successfully controlled through glucocorticoid treatment and multidisciplinary collaboration support. However, it should be noted that during the tapering of steroids, existing irAE symptoms may worsen or new adverse reactions may occur. This case emphasizes that sintilimab may trigger a severe, sequential multi-system irAEs, potentially suggesting a progressive breakdown of immune tolerance, though direct evidence is lacking. It highlights the critical need for prolonged, vigilant multi-organ monitoring in elderly patients receiving ICIs, especially in combination regimens, and suggests that sustained immunomodulation may be required to control subsequent irAEs even after initial toxicity resolution.
Keywords: immune checkpoint inhibitors, immune-related adverse events, sintilimab, immune-mediated hepatotoxicity, haematological immune-related adverse events, checkpoint inhibitor-related pneumonitis
Introduction
Cancer remains a major challenge in global public health. According to the Global Cancer Statistics 20221 and the China Report on Nutrition and Chronic Disease Status 2025, the incidence of cancer continues to rise. Immune checkpoint inhibitors (ICIs) have significantly improved outcomes in various solid tumors and hematologic malignancies.2 However, they may disrupt immune tolerance and lead to immune‑related adverse events (irAEs).3 ICIs primarily include monoclonal antibodies targeting programmed death-1 (PD-1)/programmed death-ligand 1 (PD-L1) and cytotoxic T-lymphocyte-associated antigen-4 (CTLA-4).4
Among patients treated with PD‑1/PD‑L1 inhibitors, the overall incidence of irAEs is approximately 66–70%, with grade ≥3 severe events accounting for about 14%.5,6 irAEs can affect any organ; cutaneous, gastrointestinal, and endocrine toxicities are relatively common, whereas pneumonitis, myocarditis, neurological toxicity, nephritis, and hematologic toxicity are less frequent but can be life‑threatening.5,6 Notably, the time of onset and resolution vary considerably across different organ systems – irAEs may appear weeks to months after treatment initiation and can even occur after drug discontinuation.7 When two or more organs are involved, it is defined as multi‑organ irAE, which accounts for approximately 20–30% of all irAE cases.8,9 Studies suggest that patients with multi‑organ injury are predominantly male, aged 33 to 75 years, and most events occur during the first or second cycle of ICI exposure.10 Multi‑organ irAEs can be simultaneous or sequential; about 16% of patients with solid tumors receiving PD‑1/PD‑L1 inhibitors develop involvement of more than one organ system,11 and the proportion is even higher in patients receiving anti‑CTLA‑4 inhibitors or combination ICI therapy.12 Common multi‑organ combinations include cardiac + neurological, cardiac + pulmonary, thyroid + pituitary, cardiac + hepatic, and gastrointestinal + cutaneous.12–14 Compared with single‑organ irAEs, multi‑organ irAEs are generally more severe, have a worse prognosis, and respond less favorably to high‑dose glucocorticoids.12
Esophageal squamous cell carcinoma (ESCC) is a common malignancy in China and other high‑incidence regions of Asia. PD‑1/PD‑L1 inhibitors have brought new hope for ESCC patients, especially those with chemotherapy resistance or recurrent/metastatic disease.15 However, not all ESCC patients derive benefit; the therapeutic efficacy is highly dependent on pre‑existing immune cell infiltration within the tumor microenvironment (TME), particularly the density and function of CD8⁺ T cells.16 The TME of ESCC exhibits pronounced immunosuppressive features, and recent basic research has uncovered several key regulatory pathways. For example, NME4 suppresses the NFκB2‑CCL5 axis, limiting CD8⁺ T cell infiltration into the tumor parenchyma, thereby creating a “cold tumor” phenotype.17 Chemotherapy resistance further aggravates immune evasion: in 5‑fluorouracil (5‑FU)‑resistant ESCC cells, ADAM10 is markedly upregulated, which cleaves membrane‑bound PD‑L1 and releases soluble PD‑L1, impairing the recruitment and cytotoxic function of CD8⁺ T cells.18 Metabolically, lactate efflux mediated by monocarboxylate transporter 4 (MCT4) leads to acidification of the TME and is closely associated with the infiltration of CD8⁺ T cells, M2 macrophages, and neutrophils, thereby influencing patient prognosis.19 Moreover, PIK3CA, a frequently mutated oncogene in ESCC, can alter the infiltration pattern of CD4⁺ T cell subsets and is linked to resistance to p38/JNK pathway inhibitors.20 Together, these mechanisms constitute a complex network of immune escape in ESCC and also provide a molecular basis for both the response to immunotherapy and the development of irAEs. By blocking immune checkpoints, PD‑1 inhibitors can partially reverse the above immunosuppression and re‑activate T cells to attack tumors. However, this non‑specific immune enhancement may also damage normal tissues, leading to irAEs;21 in some patients, severe and even life‑threatening multi‑organ involvement occurs.
Sintilimab, a domestic PD‑1 inhibitor, is widely used in clinical practice. Although it shows efficacy both as monotherapy and in combination with chemotherapy, its irAE incidence is relatively high, warranting special attention to the risk in elderly patients.22–26 To date, reports of sintilimab‑induced sequential, severe multi‑organ irAEs are scarce. We report a case of a 78-year-old male with ESCC who was suspected to develop sequential immune-mediated hepatotoxicity, aplastic anemia-like immune-mediated bone marrow suppression, and checkpoint inhibitor-related pneumonia caused by sintilimab combined with chemotherapy. We describe the clinical course and management strategies, aiming to provide clinical references for the management of such severe irAEs.
Case Report
A 78-year-old male was first hospitalized on February 13, 2025, with a chief complaint of “yellowing of skin and sclera for 5 days.”
Past History and Oncologic Treatment
Cancer Diagnosis and Surgery: Presented in November 2024 with “dysphagia and chest discomfort for over 1 week.” Gastroscopy and biopsy confirmed lower esophageal squamous cell carcinoma. On November 15, 2024, he underwent “thoracoscopic-laparoscopic combined esophagectomy with cervical esophagogastric anastomosis and lymph node dissection.” Pathology: (Esophagus) moderately to well-differentiated squamous cell carcinoma, invading the superficial muscularis propria, with no definite perineural invasion observed. No cancer involvement was found at the esophageal and gastric resection margins. Metastatic cancer was found in 2 of 5 perigastric lymph nodes, 2 of 3 lymph nodes in Group 8, 2 of 2 lymph nodes in Group 16, 3 of 4 lymph nodes in Group 17, and 1 of 2 paralaryngeal lymph nodes along the left recurrent laryngeal nerve. No metastatic cancer was seen in 1 lymph node of Group 7, 1 lymph node of 8u, or 3 paralaryngeal lymph nodes along the right recurrent laryngeal nerve. AJCC pTNM staging (2017, 8th edition): pT2N2Mx (Figure 1). Postoperative recovery was uneventful.
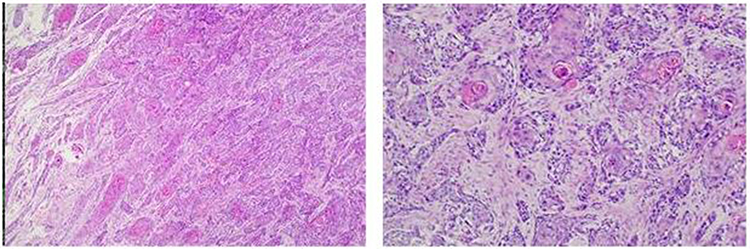 |
Figure 1 (Esophagus) moderately to well-differentiated squamous cell carcinoma, invading the superficial muscularis propria, with no definite perineural invasion observed. No cancer involvement was found at the esophageal and gastric resection margins. Metastatic cancer was found in 2 of 5 perigastric lymph nodes, 2 of 3 lymph nodes in Group 8, 2 of 2 lymph nodes in Group 16, 3 of 4 lymph nodes in Group 17, and 1 of 2 paralaryngeal lymph nodes along the left recurrent laryngeal nerve. No metastatic cancer was seen in 1 lymph node of Group 7, 1 lymph node of 8u, or 3 paralaryngeal lymph nodes along the right recurrent laryngeal nerve. AJCC pTNM staging (2017, 8th edition): pT2N2Mx. |
Immunotherapy Combined with Chemotherapy:
Cycle 1 (Dec 26, 2024): Sintilimab (weight≥60 kg, the dosage is 200 mg). 200mg (day 1) + Albumin-bound paclitaxel (125mg/m2) 210mg (day 1) + Nedaplatin (60–75mg/m2) 34mg (days 1–3), IV infusion, q3w.27 Pre-chemotherapy liver function (Dec 25, 2024) was normal. The patient’s body weight during antitumor therapy was 61 kg, with a body surface area of 1.68 m2.
Cycle 2 (Jan 19, 2025): Same regimen. Pre-chemotherapy liver function (Jan 17, 2025): ALT 121 U/L, AST 43 U/L.
Personal and Family History
- Smoking: >50 years, 20 cigarettes/day.
- Alcohol: >40 years, 100–150 mL liquor/day.
- Family History: Father died of esophageal cancer; brother diagnosed with esophageal cancer (post-operative >10 years, alive).
First Hospital Admission (Feb 13, 2025)
Chief Complaint: Yellowing of skin and sclera for 5 days.
Physical Examination: Weight: 48kg, Poor nutritional status, hepatic facies. Severe jaundice of skin, mucous membranes, and sclera. No liver palms, spider angiomata, petechiae, or ecchymoses. No other significant positive findings.
Key Investigations (Feb 11, 2025):
CBC (complete blood counts):WBC (White blood cell) 6.43×109/L, RBC (red blood cell) 3.30×1012/L, platelets (PLT) 262×109/L, hemoglobin (Hb) 102g/L.
Liver Function: ALT (Alanine aminotransferase)254U/L, AST (Aspartate aminotransferase) 176U/L, ALP (Alkaline phosphatase) 850U/L, GGT (Gamma-glutamyl transferase) 816U/L, TB (Total bilirubin) 385.6μmol/L, DB (Direct bilirubin) 259.0μmol/L, TBA (Total Bile acids) 296.6μmol/L.
Viral Hepatitis and Autoimmune Liver Disease Antibodies: Negative.
Coagulation function: Normal.
Abdominal Ultrasound: Hepatic cyst, hyperechoic hepatic nodule (0.7cm,nature indeterminate); gallbladder poorly visualized; right renal cyst; enlarged prostate; ascites.
Preliminary Diagnosis:
- Liver dysfunction, etiology undetermined: Drug-induced liver injury? Other?
- Post-operative lower esophageal squamous cell carcinoma (pT2N2Mx), mediastinal lymph node metastasis.
First Hospitalization Course
Phase 1 (Feb 13–19, 2025, Oncology Department)
Treatment: Magnesium isoglycyrrhizinate (150 mg/d IV), Reduced glutathione (1.8 g/d IV), Prednisone acetate (45 mg/d PO, 0.94 mg/kg/day).
Clinical Change (Feb 14):CBC showed PLT 59×109/L, Hb 87g/L. Recombinant human thrombopoietin (15,000 IU/d SC) was added.
Liver function showed no significant improvement. Transferred to Infectious Diseases Department after consultation.
Phase 2 (Feb 19–Apr 4, 2025, Infectious Diseases Department)
Hepatoprotective & Glucocorticoid Therapy: Ademetionine (1.0 g/d IV), Reduced glutathione (1.2 g/d IV), Magnesium isoglycyrrhizinate (200 mg/d IV), Methylprednisolone (40 mg/d IV, 0.83mg/kg/day, Feb 19–28). Supplemented with acid suppression, potassium replacement, albumin infusion, etc.
After the above treatment, the liver function indexes gradually decreased. From Feb 28, the hormone was changed to prednisone acetate orally and gradually reduced (see Figure 2 for details of dose adjustment and changes in liver function indicators).
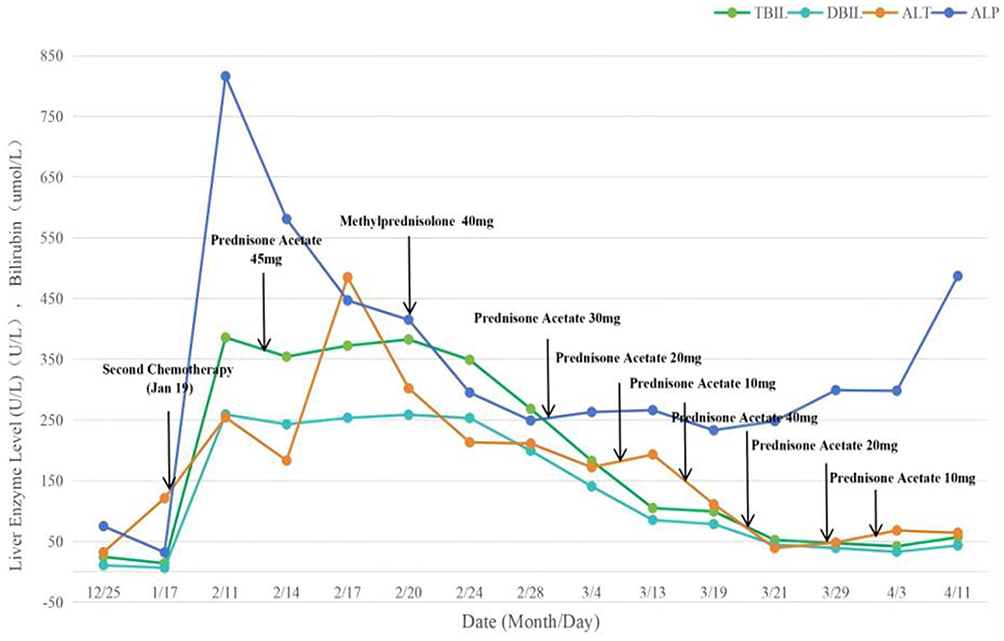 |
Figure 2 Relationship between changes in liver function and hormone dosage adjustment. After addition of glucocorticoid (methylprednisolone 40mg/day) therapy, the patient’s liver function gradually recovered, and no rebound occurred during the tapering of glucocorticoids. |
Hematological Toxicity Progression (Mar 13):
CBC: WBC 3.79×109/L,RBC 1.39×1012/L, Hb 44g/L, PLT 172×109/L.
Fecal occult blood test: negative
Reticulocytes: Absolute count 0.0009×1012/L (extremely low), Percentage 0.070%.
Hematology Consultation: Suspected pure red cell aplasia? Treated with red blood cell transfusions (Mar 14, 16, 20).
Bone Marrow Failure Syndrome & Intensified Therapy (From Mar 18):
Mar 18 CBC: WBC 1.11×109/L,RBC 1.32×1012/L, Hb 43g/L, PLT 47×109/L.
Hematopoietic Support: Human granulocyte colony-stimulating factor (100 μg/d SC), Recombinant human interleukin-11 (3 mg/d SC) (Mar 19–25).
Bone Marrow Examination:
- Morphology: Hypocellular marrow (suggesting possible dilution).
- Biopsy: Minimal marrow tissue, rare hematopoietic elements (Figure 3).
- Repeat Hematology Consultation: Suspected bone marrow failure syndrome. Recommended intensified immunosuppression (Prednisone: 0.5–1mg/kg/day,Cyclosporine: 3–5mg/kg/day). Due to concerns about the hepatotoxicity of cyclosporine, it was decided to withhold its initiation. Instead, the dose of prednisone was adjusted to 20mg orally twice daily (0.83mg/kg/day) on March 20.
- Outcome:Gradual trilineage recovering.Discharged improved on Apr 4, 2025, on prednisone acetate 10mg orally once daily (Changes in glucocorticoid dosage and corresponding hematological parameters are presented in Figure 4).
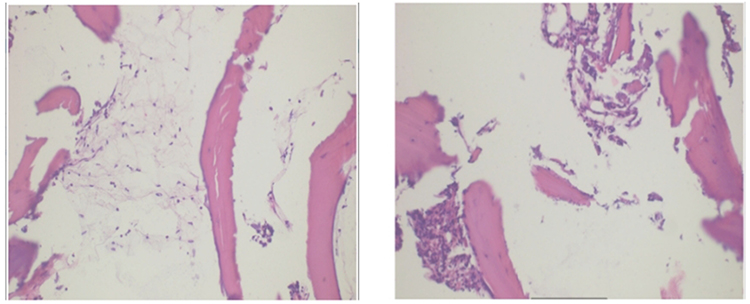 |
Figure 3 Bone marrow: The main bone tissue is fragmented, and only a very small amount of hematopoietic tissue is seen inside. |
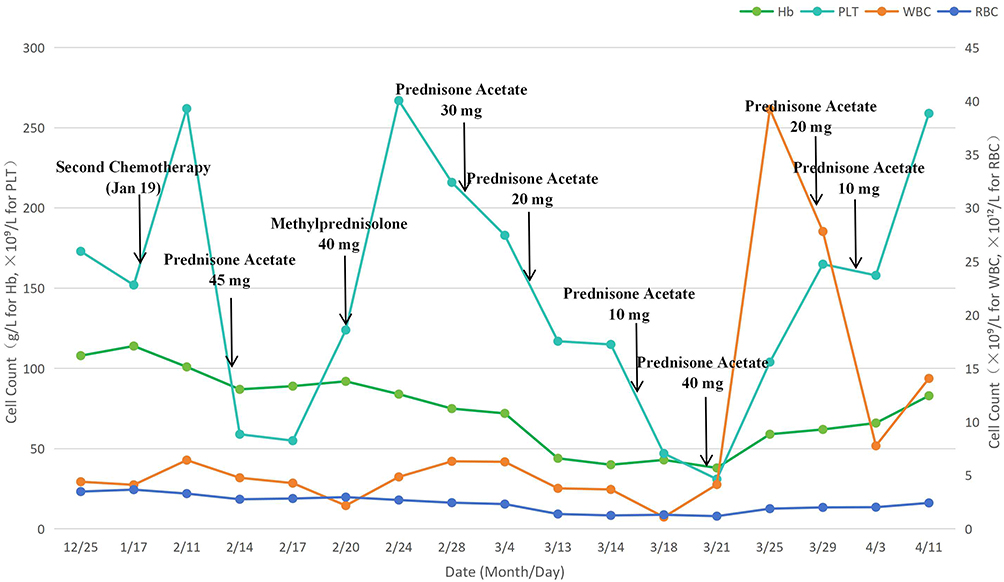 |
Figure 4 Relationship between changes in complete blood count and hormone dosage adjustment. When the patient began to experience a decrease in platelets, the addition of platelet-raising drugs and glucocorticoid treatment gradually restored the platelet count to normal. However, during the tapering of glucocorticoids, progressive severe pancytopenia occurred. The patient was given red blood cell transfusions, human granulocyte colony-stimulating factor, human interleukin-11, and intensified immunosuppressive therapy (prednisone acetate increased to 40 mg/day), after which the three blood cell lineages gradually recovered. |
Readmission (Apr 11, 2025)
Chief Complaint:Fever and dyspnea for 1 day.
History of Present Illness:Symptoms began 1 week post-discharge after catching a cold: fever (Tmax 38.6°C), chills, and progressive dyspnea.
Physical Examination:Poor mental status. Mild jaundice of skin, mucous membranes, and sclera. Bilateral moist rales audible (more prominent on right).
Key Investigations (Apr 11, 2025):
- CBC: WBC 14.07×109/L, RBC 2.43×1012/L,Hb 83g/L, PLT 259×109/L.
- Liver Function: ALT 64U/L, AST 40U/L, ALP 487U/L, GGT 570U/L, TB 56.9μmol/L, DB 43.3μmol/L, TBA 85.3μmol/L.
- Arterial Blood Gas (oxygen via nasal cannula): PaO2 64mmHg, PaCO2 28mmHg, SpO2 89.0%.
- Infection Markers: PCT 12.757ng/mL; β-D-glucan 980pg/mL; GM test 0.21.
Second Hospitalization Course
Initial Treatment (Apr 11–13):
- Patient declined chest CT, Fiberoptic bronchoscopy, NGS analysis of Bronchoalveolar lavage fluid.
- Empirical Antibiotics: Piperacillin-tazobactam (4.5g q8h IV).
- Respiratory Support: High-flow nasal cannula oxygen therapy.
- Dyspnea did not improve.
Treatment Adjustment (From Apr 13):
- Upgrading of antibiotic therapy: Imipenem-cilastatin (1.0 g q8h IV, Apr 13–22).
- Glucocorticoids: Methylprednisolone 40 mg/d IV (Apr 13–14).
- Clinical Deterioration:Dyspnea worsened, oxygenation declined (HFNC, FiO275%, SpO2 86%).
Further Adjustment (From Apr 15):
- Antifungal: Fluconazole (loading dose 400mg, then 200 mg/d IV, Apr 15–27) (due to elevated β-D-glucan).
- Glucocorticoids Increased: Methylprednisolone 40 mg q12h IV (80 mg/d total, Apr 15–27).
- Linezolid added (600 mg q12h PO, Apr 19–22).
Imaging examination and Multidisciplinary Consultation (Apr 20):
Chest CT: interstitial pneumonia in both lung, predominantly involving the upper lobes and the right middle lobe, along with scattered pulmonary bullae. (Figure 5).
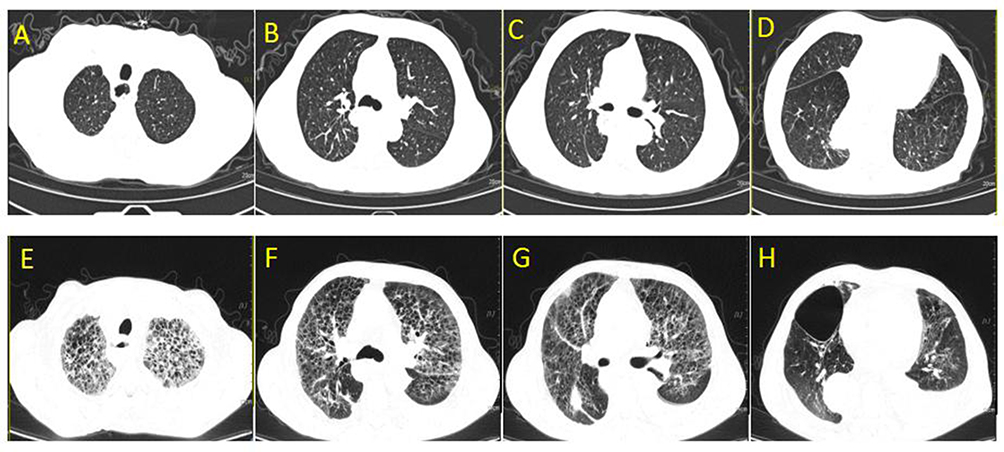 |
Figure 5 (A–D) shows chest CT images at different levels of the patient’s chest prior to initiating antitumor therapy. Chest CT scan (December 24,2024): The lung markings show slight increase and disorder, with increased radiolucent areas and scattered small cystic hypoconvsitutes. Scattered patchy and linear density-increasing shadows are observed in the posterior basal segments of both lower lobes and the dorsal segment of the right lower lobe. The right pleura shows localized thickening, with a small amount of pleural effusion. (E–H) shows chest CT images at different levels of the patient’s chest during the onset of dyspnea following two rounds of antitumor therapy. Chest CT scan (April 20,2025): The lung markings show slight increase and disorder, with honeycomb-like changes in the upper lobes and middle lobe of the right lung. Increased radiolucent areas and scattered cystic hypoconvsitutes are present, with larger ones located in the anterior basal segment of the right lower lobe (approximately 7.3×5.3cm). Small pleural effusions are observed bilaterally, predominantly on the left side. Scattered patchy and linear density-increasing shadows are seen in the lower lobes of both lungs, accompanied by partial consolidation in the right lower lobe. Bilateral pleural thickening is noted. |
Sputum general bacterial, acid-fast bacilli, and Candida smear: squamous epithelial cells <10/LPF, white blood cells <25/LPF, no Candida detected, no acid-fast bacilli detected, no intracellular bacteria detected; sputum general bacterial and Haemophilus culture and identification: normal flora growth, no Haemophilus influenzae detected;
Combined with history (ICI use, sequential irAEs):Immune-related pneumonitis considered likely.
Oncology Consultation Recommendation: Increase methylprednisolone to 2mg/kg/d (96mg/d), consider methylprednisolone 1g/d pulse for 3 days if necessary; slow taper after symptom control (total duration 1–2 months); consider adding mycophenolate mofetil or infliximab if inadequate response.
Respiratory department consultation: Considering interstitial lung fibrosis,Cannot rule out drug-induced, it is recommended to add hydrocortisone 100 mg once daily.
Outcome:Symptoms and oxygenation gradually improved. Glucocorticoid dose was not adjusted (maintained at methylprednisolone 80 mg/d). Discharged improved on April 27, 2025.
The entire disease course of the patient, including the timeline of immune-related adverse events and the corresponding management measures, can be seen in Figure 6.
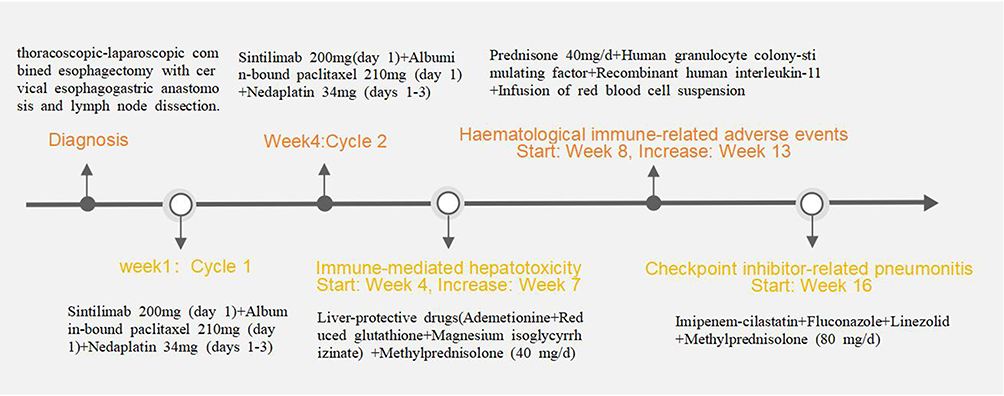 |
Figure 6 The timeline of immune checkpoint inhibitor therapy and its immune-related adverse events, along with corresponding management measures. |
Discussion
This patient had no prior history of hepatitis or hematologic disease, with normal baseline CBC and liver function before chemotherapy. Following sintilimab combined with albumin-bound paclitaxel and nedaplatin, he sequentially developed liver injury, severe myelosuppression, and interstitial pneumonitis. Hepatotoxicity, which developed in the fourth week following the commencement of immunotherapy and reached its peak by the seventh week, was gradually ameliorated with a combination of hepatoprotective and corticosteroid therapy. Hematological toxicity first appeared at week 8 (decreased hemoglobin, platelets), transiently improved with thrombopoietin and glucocorticoids, but relapsed during the glucocorticoid reduction, progressing to severe pancytopenia (predominantly hemoglobin and platelet decline, with extremely low reticulocytes). By week 13, this manifested as aplastic anemia-like immune-mediated myelosuppression. Treatment with interleukin-11, granulocyte colony-stimulating factor, and increased glucocorticoid dose led to gradual trilineage recovery, with no recurrence during subsequent tapering. Interstitial pneumonitis presented at week 16 (fever, dyspnea), with chest CT showing diffuse bilateral interstitial changes, improving after glucocorticoid dose escalation combined with broad-spectrum antibiotics. These toxic reactions are characterized by sequential and multi-system involvement, suggesting that they may be associated with anti-tumor treatment.
Analysis of the Three Therapeutic Agents
Nedaplatin: A second-generation platinum agent exerting anti-tumor effects by interfering with DNA replication.28 The peak incidence of adverse reactions occurred within 30 minutes and during the 2- to 14-day period.29 Common reactions like systemic hypersensitivity and associated dermatological, respiratory, or cardiovascular symptoms are immediate, while myelosuppression and hepatotoxicity are delayed, the management primarily involves targeted supportive measures, including leukocyte and platelet boosters as well as hepatoprotective agents, which are generally effective in mitigating these toxicities.30 Both the hematological toxicity and interstitial pneumonia in this case notably fell outside the typical time window for nedaplatin toxicity. Specifically, myelosuppression occurred at week 8 (and relapsed during steroid taper), whereas interstitial pneumonia developed as late as week 16.
Albumin-bound Paclitaxel:This formulation enhances tumor uptake and concentration of paclitaxel.31 Adverse effects include hematologic toxicity, alopecia, fatigue, neurotoxicity, cardiotoxicity, hepatorenal toxicity, and gastrointestinal reactions,32,33 which usually resolve rapidly upon discontinuation or dose reduction.34 Its myelosuppression is dose-dependent and limiting, typically occurring 8–10 days post-chemotherapy and resolving quickly after stopping or reducing the dose.35 In this patient, myelosuppression not only manifested with a notably delayed onset (at week 8) but also persisted and progressed to aplastic anemia-like immune-mediated myelosuppression after drug discontinuation, which is inconsistent with its typical toxicity profile.
Sintilimab:As a recombinant fully human IgG4 PD-1 monoclonal antibody, sintilimab-induced irAEs are distinct from traditional chemotherapy toxicities, characterized by delayed onset, prolonged duration, and potential persistence post-discontinuation.36,37 The delayed presentation of liver injury, myelosuppression, and pneumonitis (weeks 4, 8, and 16, respectively), the relapse of myelosuppression during steroid taper, and the protracted course support irAEs. Based on the Naranjo adverse drug reaction probability scale (Table 1),38 the association score between sintilimab and each adverse event was 6 (probable).
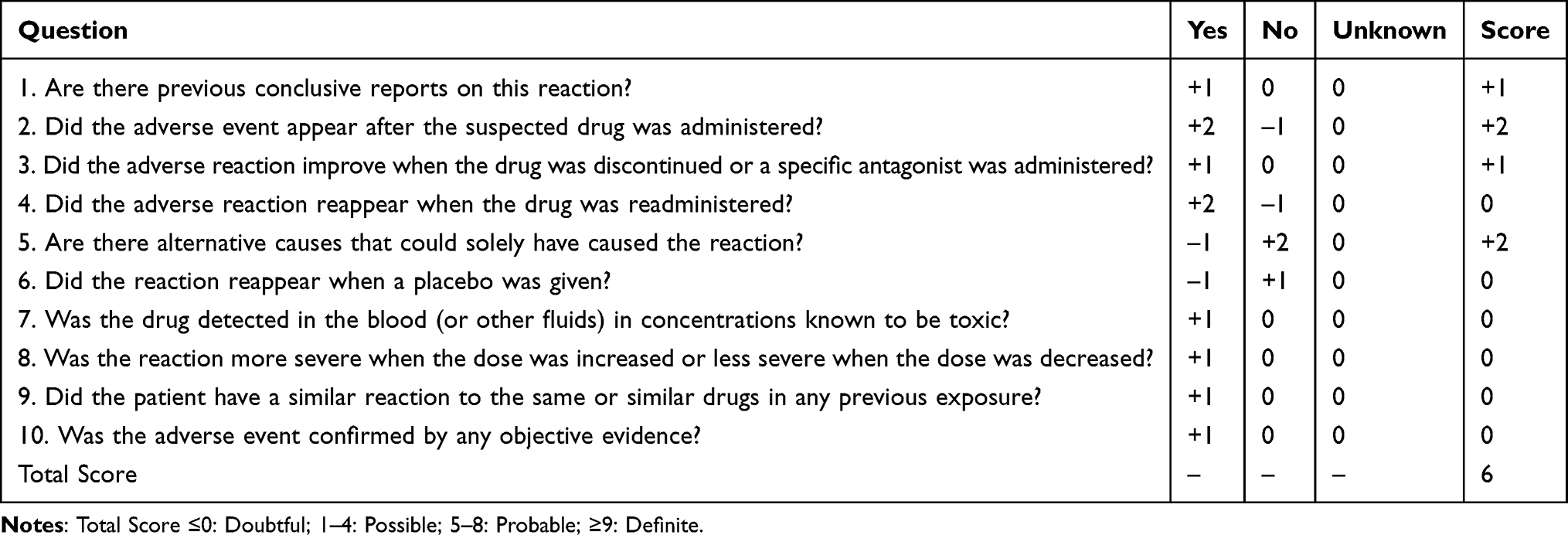 |
Table 1 Naranjo Adverse Drug Reaction (ADR) Probability Scale Scoring for This Case |
While sintilimab demonstrates significant anti-tumor efficacy,39 irAEs are inevitable Treatment-related adverse event rates exceed 58.0% with monotherapy, with ≥grade 3 events in 13%;8 combined with chemotherapy (pemetrexed + platinum), TRAE incidence reaches 99.6%, ≥grade 3 in 61.7%, with a 2.3% fatality rate.9 ADRs occur more frequently in middle-aged and elderly males, can arise 0–544 days post-initiation, with higher risk within the first 4 months.24–26 Currently, some case reports have reported that tumor patients receiving ICIs treatment (including PD-1 inhibitor combined with chemotherapy, or PD-1 inhibitor and CTLA-4 inhibitor) may develop severe consecutive irAEs involving multiple organ systems, and each irAE can occur at different time points, including after the interruption of immunotherapy.40–46
Ni CX and others reported a case of an elderly patient with metastatic pancreatic cancer who developed severe immune-related colitis after 2 months of treatment with sintilimab combined with gemcitabine, and then developed immune-related ureteritis again after 8 months of treatment, also suggesting that sintilimab can cause serious consecutive irAEs in multiple organ systems.40
Analysis of irAE Characteristics in This Case
Immune-mediated hepatotoxicity (IMH)
The incidence of sintilimab-related hepatitis is 9.5%,47 with a median time to first onset of 40 days (range: 13–362 days), and most cases resolve within 8–12 weeks after treatment initiation.48 The clinical presentations include hepatocellular, cholestatic, and mixed patterns, with the hepatocellular type accounting for 50% of cases.49 The pathogenesis of IMH involves T-cell subset imbalance and cytokine network dysregulation, characterized by expansion of effector T cells (Th1, Th17) and depletion of regulatory T cells (Tregs), leading to elevated pro-inflammatory cytokines (IL-2, IFN-γ, TNF) and reduced anti-inflammatory cytokines (IL-10, IL-35, TGF-β), as well as disruption of the crosstalk between innate and adaptive immunity. Elevated autoantibody levels enhance humoral autoimmune responses, and complement system activation directly contributes to hepatocyte injury.50 Genome-wide association studies have identified specific genetic loci associated with irAE development, suggesting the involvement of genetic factors, which may explain why only a subset of patients develop these events.51 Based on the R value (ALT/ALP ratio, R=0.79), the present case fits the cholestatic pattern. Guidelines suggest that such patients may have a poor response to glucocorticoids.52 Nevertheless, after treatment with glucocorticoids (initial regimen: prednisone acetate 45 mg), this patient showed improved liver function, with sustained recovery and no relapse during weekly tapering, indicating a favorable response to glucocorticoids.
Haematological immune-related adverse events (Haem-irAEs)
Current studies have shown a high incidence of sintilimab-related myelosuppression, reaching 67.06%, with grade III/IV severe events accounting for 86.47%; paclitaxel use and stage M tumor are independent risk factors for myelosuppression.53 Among patients receiving sintilimab plus chemotherapy, common hematologic toxicities include neutropenia, thrombocytopenia, anemia, and leukopenia.53,54 The incidence of immune-related thrombocytopenia is 1.5%, with a median time to onset of 1.9 months (range: 0.7–10.9 months) and a median duration of 0.6 months (range: 0.1–2.3 months).55 Collectively, the patient was at high risk for hematologic toxicity, initially presenting with thrombocytopenia and anemia, which subsequently progressed to aplastic anemia-like immune-mediated myelosuppression. The underlying mechanism may involve overproduction of pro-inflammatory cytokines (eg., IFN-γ, TNF-α) by activated T cells, which suppress hematopoietic stem/progenitor cell proliferation and promote their apoptosis.56 Activated CD8⁺ T cells can directly attack megakaryocytes, inhibiting their maturation and platelet production; pro-inflammatory cytokines such as IFN-γ and TNF-α may also enhance macrophage-mediated platelet phagocytosis. B cells can produce platelet-associated immunoglobulin G (PA-IgG), facilitating platelet destruction by splenic macrophages.57 ICIs may also enhance humoral autoimmunity, generating autoantibodies against erythrocytes and leading to immune hemolysis.58 When these mechanisms simultaneously affect multiple lineages (eg., aplastic anemia combined with thrombocytopenia and hemolysis), they are associated with global dysregulation of the T-cell, B-cell, and cytokine networks induced by ICIs, which aligns with the known pathogenesis of irAEs. The patient’s rapid response (within one week) to intensified steroid therapy and the absence of relapse during subsequent tapering support an immune-mediated mechanism.
Checkpoint inhibitor-related pneumonitis (CIP)
The incidence of sintilimab-related pneumonitis is 4.3%, with a median time to onset of 9.1 days (range: 0–369 days). Prior lung injury (eg., smoking, radiotherapy) is a risk factor;59 additionally, Asian ethnicity, advanced age (≥65 years),60 squamous cell carcinoma histology,61 and the use of PD-1 inhibitors62 are significantly associated with the development of CIP. Imaging findings are diverse, including patterns resembling organizing pneumonia, nonspecific interstitial pneumonia, hypersensitivity pneumonia, diffuse alveolar damage, and typical interstitial pneumonia, which may be accompanied by pleural thickening, pleural effusion, granulomas, or lymphadenopathy.63 The pathogenesis involves abnormal T-cell activity and proportions, reduced B-cell counts and function, alterations in the inflammatory cytokine profile (elevated IL-6, IL-17, TNF-α, and IFN-γ; decreased IL-8), autoimmune antibody changes, and complement activation by autoantibodies that exacerbates inflammation.64,65 In summary, the patient was at high risk for CIP, and the present case primarily presented with diffuse interstitial pneumonia and bullous lesions. These bullous lesions were not observed on chest CT before anticancer therapy and were considered treatment-related; according to previous literature, such lesions are relatively rare.
The Cornerstone of irAE Management: Glucocorticoids
Glucocorticoid regimens vary slightly depending on the organ system involved.
IMH
For grade G2, it is recommended to withhold ICIs and administer prednisone/methylprednisolone at 0.5–1 mg/kg/day, with slow tapering after clinical improvement (total course ≥4 weeks). For grades G3–G4, prednisone/methylprednisolone at 1–2 mg/kg/day is recommended,begin taper after recovery to ≤G1, complete over ≥1 month.Ursodeoxycholic acid (13–15 mg/kg/day) may be considered in cholestatic or mixed patterns.66,67 However, emerging studies have shown that more than two-thirds of patients with grade 3–4 ICI-induced liver injury do not require corticosteroids, and simple ICI withdrawal achieves a remission rate of 38%–50%. For patients without signs of liver failure, initial ICI discontinuation with supportive care is also feasible.68,69 Furthermore, prednisone at 0.5–0.8 mg/kg/day effectively controls most cases of ICI-induced liver injury, whereas higher doses (≥1.5 mg/kg/day) do not improve efficacy but increase the risk of adverse events.70–72 In our study, a dose of less than 1 mg/kg was used for treatment, and the patient’s liver function gradually recovered.
Haem-irAEs
For immune-related thrombocytopenia: grade G2 recommends withholding ICIs; if conventional treatment fails or no improvement is seen within 4–6 weeks, add prednisone/methylprednisolone at 1 mg/kg/day for 2–4 weeks, followed by tapering over 4–6 weeks. For grades G3–G4, prednisone/methylprednisolone at 1–2 mg/kg/day is recommended for 2–4 weeks.52,67 For aplastic anemia (pure red cell aplasia): severe to very severe cases recommend prednisone/methylprednisolone at 1–2 mg/kg/day until remission to non-severe status, followed by tapering over 4–8 weeks.67 However, one retrospective study noted that among patients with grade G2–G3 hematologic toxicities, none received systemic immunosuppressive therapy such as corticosteroids or intravenous immunoglobulin, nor was ICI therapy interrupted.73 In our study, a dose of less than 1 mg/kg was used for treatment, and the patient’s three blood cell lineages gradually recovered.
CIP
For grade G2, methylprednisolone at 1–2 mg/kg/day is recommended until symptoms improve to ≤G1, followed by gradual tapering over 4–6 weeks (eg., 5–10 mg weekly). For grades G3–G4, after excluding/covering infection (including atypical pathogens), methylprednisolone at 1–2 mg/kg/day is given and tapered over 6 weeks.66,67,74 Nevertheless, Masato Karayama summarized multiple real-world retrospective studies and clinical trial data and found that in clinical practice, the actual dose or duration of corticosteroid administration is often lower than guideline recommendations.62 In our study, the guideline‑recommended dose of 1–2 mg/kg was used for treatment, and the patient’s dyspnoea gradually resolved.
Currently, glucocorticoids are regarded as the cornerstone therapy for irAEs, with their specific regimen determined by the toxicity grade and whether the condition is life-threatening. Timely initiation of treatment is critical (delay beyond 5 days may compromise efficacy), and slow tapering (generally >4 weeks; 6–8 weeks or longer in severe cases) is essential for preventing recurrence, particularly in pneumonitis and hepatitis, where rapid tapering may exacerbate existing irAE symptoms or trigger new events.52 However, accumulating real-world evidence and clinical practice data indicate discrepancies between guideline recommendations and actual clinical practice. These differences suggest that current standardized, grade-based treatment protocols may overtreat some patients, thereby highlighting the necessity of individualized decision-making. Future prospective studies are warranted to identify which patients can be managed by immunotherapy discontinuation alone, which patients are suitable for low-dose corticosteroids, and whether further simplification or shortening of treatment duration is feasible, so as to maximize efficacy while minimizing corticosteroid-related adverse effects.
However, this study still has some limitations. First, when the patient presented with pancytopenia, bone marrow biopsy revealed extremely scant marrow tissue with rare hematopoietic elements, suggesting a possible bone marrow failure syndrome; however, this may also indicate insufficient bone marrow sampling. Second, at the time of CIP diagnosis, the patient had markedly elevated levels of procalcitonin (12.757 ng/mL) and β-D-glucan (980 pg/mL). Although sputum microbiological examination was negative, the patient refused fiberoptic bronchoscopy and BAL fluid NGS testing and concurrently received broad-spectrum antibiotics and antifungal therapy. Therefore, infectious etiologies—particularly fungal infection or Pneumocystis jirovecii pneumonia (PJP)—could not be fully excluded. Therefore, when diagnosing irAEs, thorough examinations should be performed to adequately rule out other possible etiologies, thereby minimizing diagnostic bias and identifying the underlying cause.
Conclusion
This case report suggests that sintilimab may induce sequential, multi-system (hepatic, hematopoietic, pulmonary), delayed-onset severe irAEs, including drug-induced liver injury (cholestatic pattern), aplastic anemia-like immune-mediated myelosuppression, and interstitial pneumonitis. In this elderly patient, the sequential occurrence of these events indicates that advanced age may increase the risk of such complex irAEs. Glucocorticoids formed the foundation of successful treatment in this case, supplemented by organ-specific supportive care. However, there are discrepancies between the dosage and treatment duration of glucocorticoids recommended in guidelines and those observed in actual clinical practice, necessitating further prospective studies for guidance. Clinicians should maintain a high index of suspicion for irAEs and implement long-term, multi-system monitoring in patients receiving sintilimab, particularly when combined with chemotherapy. Within a multidisciplinary framework, prompt, intensive, and individualized management strategies are crucial for the early recognition and effective management of such complex sequential irAEs, ultimately improving patient outcomes.
Abbreviations
ICIs, Immune checkpoint inhibitors; irAEs, immune-related adverse events; PD-1, programmed death-1; PD-L1, programmed death-ligand 1; CTLA-4, cytotoxic T-lymphocyte-associated antigen-4; CBC, complete blood counts; WBC, White blood cell; RBC, red blood cell; PLT, platelets; Hb, hemoglobin; AST, Aspartate aminotransferase; ALT, Alanine aminotransferase; ALP, Alkaline phosphatase; GGT, Gamma-glutamyl transferase; TB, Total bilirubin; DB, Direct bilirubin; TBA, Total Bile acids; ESCC, Esophageal squamous cell carcinoma; IMH, Immune-mediated hepatotoxicity; Haem-irAEs, Haematological immune-related adverse events; CIP, Checkpoint inhibitor-related pneumonitis; TME, tumor microenvironment.
Data Sharing Statement
The data that support the findings of this study are available on request from the first author.
Ethics Statement
This study was approved by the Medical Ethics Committee of the Affiliated Hospital of North Sichuan Medical College (approval number:2025ER464-1) and the case details have been approved for publication by the Affiliated Hospital of North Sichuan Medical College.
Consent for Publication
The patient data were anonymized and no information in the manuscript could trace back to the individual in question. The patient agreed to publication and signed an informed consent form before the start of the study.
Acknowledgments
We would like to thank the patient and his family for authorizing publication of the present case.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74:229–14. doi:10.3322/caac.21834
2. Bagchi S, Yuan R, Engleman EG. Immune checkpoint inhibitors for the treatment of cancer: clinical impact and mechanisms of response and resistance. Annu Rev Pathol. 2021;16:223–249. doi:10.1146/annurev-pathol-042020-042741
3. de Miguel M, Calvo E. Clinical challenges of immune checkpoint inhibitors. Cance Cell. 2020;38:326–333. doi:10.1016/j.ccell.2020.07.004
4. Hossain MA. A comprehensive review of immune checkpoint inhibitors for cancer treatment. Int Immunopharmacol. 2024;126(Pt 2):111365. doi:10.1016/j.intimp.2023.111365
5. Lee DJ, Lee HJ, Farmer JR, Reynolds KL. Mechanisms driving immune-related adverse events in cancer patients treated with immune checkpoint inhibitors. Curr Cardiol Rep. 2021;23:98. doi:10.1007/s11886-021-01530-2
6. Yin Q, Wu L, Han L, et al. Immune-related adverse events of immune checkpoint inhibitors: a review. Front Immunol. 2023;14:1167975. doi:10.3389/fimmu.2023.1167975
7. Tang SQ, Tang LL, Mao YP, et al. The pattern of time to onset and resolution of immune-related adverse events caused by immune checkpoint inhibitors in cancer: a pooled analysis of 23 clinical trials and 8,436 patients. Cancer Res Treat. 2021;53:339–354. doi:10.4143/crt.2020.790
8. Shankar B, Zhang J, Naqash AR, et al. Multisystem immune-related adverse events associated with immune checkpoint inhibitors for treatment of non-small cell lung cancer. JAMA Oncol. 2020;6:1952–1956. doi:10.1001/jamaoncol.2020.5012
9. Kichenadasse G, Miners JO, Mangoni AA, Rowland A, Hopkins AM, Sorich MJ. Multiorgan immune-related adverse events during treatment with atezolizumab. J Natl Compr Canc Netw. 2020;18:1191–1199. doi:10.6004/jnccn.2020.7567
10. Yuan M, Han N, Shu L, Yan L, Tang H. Case report: multi-organ injuries induced by tislelizumab. Front Immunol. 2025;16:1508293. doi:10.3389/fimmu.2025.1508293
11. Olsson Ladjevardi C, Koliadi A, Rydén V, et al. Multiple immune-related adverse events secondary to checkpoint inhibitor therapy in patients with advanced cancer: association with treatment effectiveness. Front Oncol. 2024;14:1399171. doi:10.3389/fonc.2024.1399171
12. Wang D, Zhou Y, Li H, et al. Clinical characteristics and therapies of multi-organ immune related adverse events. Clin Exp Med. 2026;26:165. doi:10.1007/s10238-026-02052-3
13. Kuo AM, Kraehenbuehl L, King S, et al. Contribution of the Skin-Gut Axis to Immune-Related Adverse Events with Multi-System Involvement. Cancers. 2022;14:2995. doi:10.3390/cancers14122995
14. Wan G, Chen W, Khattab S, et al. Multi-organ immune-related adverse events from immune checkpoint inhibitors and their downstream implications: a retrospective multicohort study. Lancet Oncol. 2024;25:1053–1069. doi:10.1016/S1470-2045(24)00278-X
15. Li N, Sohal D. Current state of the art: immunotherapy in esophageal cancer and gastroesophageal junction cancer. Cancer Immunol Immunother. 2023;72:3939–3952. doi:10.1007/s00262-023-03566-5
16. Paijens ST, Vledder A, de Bruyn M, Nijman HW. Tumor-infiltrating lymphocytes in the immunotherapy era. Cell Mol Immunol. 2021;18:842–859. doi:10.1038/s41423-020-00565-9
17. Zheng S, He S, Liang Y, et al. NME4 suppresses NFκB2-CCL5 axis, restricting CD8+ T cell tumour infiltration in oesophageal squamous cell carcinoma. Immunology. 2024;173:408–421. doi:10.1111/imm.13838
18. Cai B, Feng X, Luo S, et al. 5-FU resistance facilitates immune evasion in esophageal squamous cell carcinoma through ADAM10-mediated PD-L1 shedding and tumour microenvironment remodelling. Immunology. 2026;177:170–184. doi:10.1111/imm.70038
19. Zheng S, Liu T, Li L, et al. Tumor-infiltrating lymphocyte signature in epithelial and stromal compartments of an esophageal squamous cell carcinoma acidic microenvironment mediated by MCT4. Pathol Res Pract. 2022;236:153954. doi:10.1016/j.prp.2022.153954
20. He S, Liu Q, Luo S, et al. Immune cell infiltration and drug sensitivity in PIK3CA-mutated esophageal squamous cell carcinoma: a TCGA database analysis. Hum Immunol. 2024;85:111167. doi:10.1016/j.humimm.2024.111167
21. Li L, Huang Y, Xue R, et al. T cell-mediated mechanisms of immune-related adverse events induced by immune checkpoint inhibitors. Crit Rev Oncol Hematol. 2025;213:104808. doi:10.1016/j.critrevonc.2025.104808
22. Zhang L, Mai W, Jiang W, Geng Q. Sintilimab: a promising anti-tumor PD-1 antibody. Front Oncol. 2020;10:594558. doi:10.3389/fonc.2020.594558
23. Yang Y, Wang Z, Fang J, et al. Efficacy and safety of sintilimab plus pemetrexed and platinum as first-line treatment for locally advanced or metastatic nonsquamous non-small cell lung cancer: a randomized, double-blind, Phase 3 study (ORIENT-11). J Thorac Oncol. 2020;15:1636–1646. doi:10.1016/j.jtho.2020.07.014
24. Li M, Qi YM, Xie YJ, Yu WW, Wang L, Li X. Analysis of 205 adverse drug reaction reports of sintilimab injection. Guide Chin Med. 2025;23:1–4. doi:10.15912/j.cnki.issn1671-8194.2025.08.001
25. Yu X, Zhou Y, Li Q, Cheng XF. Retrospective literature analysis of adverse reactions of four domestic PD-1 inhibitors. Chin J Clin Pharmacol Ther. 2024;29:887–898.
26. Zhao FF, Li M, Yang N, Mao LJ, Chen JX, Guo F. Literature analysis of adverse reactions induced by sintilimab. China Pharm. 2022;33:2012–2016.
27. Chinese Society of Clinical Oncology (CSCO). Esophageal Cancer Diagnosis and Treatment Guidelines 2026. Beijing: People’s Medical Publishing House; 2026:1–112.
28. Tang C, Wu F, Wang R, et al. Comparison between nedaplatin and cisplatin plus docetaxel combined with intensity-modulated radiotherapy for locoregionally advanced nasopharyngeal carcinoma: a multicenter randomized Phase II clinical trial. Am J Cancer Res. 2016;6:2064–2075.
29. Zhou ML, Ding XM, Lv PK. Analysis of adverse drug reactions of platinum drugs in a hospital from 2022 to 2023. Life Sci Instrum. 2025;23:177–179. doi:10.11967/2025230261
30. Wang XY, Liu JH, Ma X, Zhang YH, Liu H. Analysis of adverse reactions of nedaplatin in Beijing from 2017 to 2022. Modern Pharm Clinic. 2023;38:213–218.
31. Wu YQ, Zhu T, Tong T, Li M, Shen AZ. Analysis of related factors of adverse reactions/events of albumin-bound paclitaxel. Chin J Pharmacovigilance. 2022;19:1123–1127. doi:10.19803/j.1672-8629.20210148
32. Shi YY, Hang YF, Huang YY. Analysis of clinical rationality of albumin-bound paclitaxel for injection. Eval Analysis Drug-Use Hospitals China. 2024;24:999–1002. doi:10.14009/j.issn.1672-2124.2024.08.023
33. Wang Y, Liu X. Safety signals of albumin-bound paclitaxel: data mining of the Food and Drug Administration adverse event reporting system. Indian J Pharmacol. 2023;55:167–173. doi:10.4103/ijp.ijp_640_22
34. Yamamoto Y, Kawano I, Iwase H. Nab-paclitaxel for the treatment of breast cancer: efficacy, safety, and approval. Onco Targets Ther. 2011;4:123–136. doi:10.2147/OTT.S13836
35. Zhao XC, Xu R, Wang YG, Cheng PQ, Guo C, Zhang JP. Study on pharmaceutical care pathway for albumin-bound paclitaxel for injection based on real-world data. Eval Analysis Drug-Use Hospitals China. 2024;24:
36. Shannon VR, Anderson R, Blidner A, et al. Multinational Association of Supportive Care in Cancer (MASCC) 2020 clinical practice recommendations for the management of immune-related adverse events: pulmonary toxicity. Support Care Cancer. 2020;28:6145–6157. doi:10.1007/s00520-020-05708-2
37. Puzanov I, Diab A, Abdallah K, et al. Managing toxicities associated with immune checkpoint inhibitors: consensus recommendations from the Society for Immunotherapy of Cancer (SITC) Toxicity Management Working Group. J Immunother Cancer. 2017;5:95. doi:10.1186/s40425-017-0300-z
38. Naranjo CA, Shear NH, Lanctôt KL. Advances in the diagnosis of adverse drug reactions. J Clin Pharmacol. 1992;32:897–904. doi:10.1002/j.1552-4604.1992.tb04632.x
39. Wu YY, Shao H. Research progress of sintilimab in the treatment of cancer (Review). Oncol Lett. 2025;29:240. doi:10.3892/ol.2025.14986
40. Ni CX, Zhao Y, Qian H, et al. Long survival in a pancreatic carcinoma patient with multi-organ toxicities after sintilimab treatment: a case report. Front Pharmacol. 2023;14:1121122. doi:10.3389/fphar.2023.1121122
41. Imada S, Sato S, Hirose N, Hayami R, Tsuneizumi M, Matsunuma R. Sequential multiple-organ immune-related adverse events during and after pembrolizumab therapy in triple-negative breast cancer: a case report. Case Rep Oncol. 2026;19:248–255. doi:10.1159/000550528
42. Matull J, Livingstone E, Wetter A, et al. Durable complete response in a melanoma patient with unknown primary, associated with sequential and severe multi-organ toxicity after a single dose of CTLA-4 plus PD-1 blockade: a case report. Front Oncol. 2020;10:592609. doi:10.3389/fonc.2020.592609
43. Brazel D, Lee S, Mahadevan A, Warnecke B, Parajuli R. Multiorgan failure from nivolumab and ipilimumab: a case report and literature review. Cureus. 2023;15e41781. doi:10.7759/cureus.41781
44. Nakako S, Nakashima Y, Okamura H, et al. Delayed immune-related neutropenia with hepatitis by pembrolizumab. Immunotherapy. 2022;14:101–105. doi:10.2217/imt-2021-0131
45. Chennuri RN, Madine M, Prathipati R, et al. Immune checkpoint inhibitor-associated myocarditis with multisystem immune toxicity in renal cell carcinoma. JACC Case Rep. 2026;31:107003. doi:10.1016/j.jaccas.2026.107003
46. Jonsdottir E, Robertsson IA, Hilmarsson A, Benediktsson R, Haraldsdottir S. Multisystem immune-related adverse events during combined ipilimumab-nivolumab with subsequent disease progression: a case report. Immunotherapy. 2025;17:1189–1195. doi:10.1080/1750743X.2025.2604430
47. Yamamoto A, Yano Y, Ueda Y, et al. Clinical features of immune-mediated hepatotoxicity induced by immune checkpoint inhibitors in patients with cancers. J Cancer Res Clin Oncol. 2021;147:1747–1756. doi:10.1007/s00432-020-03448-8
48. Zhou YM, Xiao LL, Li SM. Literature analysis of immune-related adverse reactions induced by sintilimab. Pharm J Chin People’s Liberation Army. 2023;36:140–145. doi:10.3969/j.issn.1008-9926.2023.02.012
49. Tang YJ, Shi JP, Zhang Y, Bai J, Yuan HL. Real-world study on immune-related liver injury caused by immune checkpoint inhibitors. Central South Pharm. 2024;22:772–777. doi:10.7539/j.issn.1672-2981.2024.03.033
50. Lasagna A, Sacchi P. The ABC of immune-mediated hepatitis during immunotherapy in patients with cancer: from pathogenesis to multidisciplinary management. Cancers. 2024;16:795. doi:10.3390/cancers16040795
51. Groha S, Alaiwi SA, Xu W, et al. Germline variants associated with toxicity to immune checkpoint blockade. Nat Med. 2022;28:2584–2591. doi:10.1038/s41591-022-02094-6
52. Chinese Society of Clinical Oncology (CSCO). Management of Immune Checkpoint Inhibitor-Related Toxicity Guidelines 2023. Beijing: People’s Medical Publishing House; 2023:1–192.
53. Liu S, Liu S, Chang Y, Nie M, Feng Y, Zhang L. A multidimensional investigation of myelosuppression associated with sintilimab: integrating pharmacovigilance signal mining with real-world clinical evidence. Front Pharmacol. 2026;17:1784033. doi:10.3389/fphar.2026.1784033
54. Xu J, Jiang H, Pan Y, et al; ORIENT-16 Investigators. Sintilimab Plus chemotherapy for unresectable gastric or gastroesophageal junction cancer: the ORIENT-16 randomized clinical trial. JAMA. 2023;330:2064–2074. doi:10.1001/jama.2023.19918
55. Mei D, Ni MX, Gu HJ, Guo XH, Gu PP. Pharmaceutical practice and analysis of immune-related adverse reactions induced by sintilimab. Pract Pharm Clin Remedies. 2021;24:1129–1132. doi:10.14053/j.cnki.ppcr.202112017
56. Votavova H, Belickova M. Hypoplastic myelodysplastic syndrome and acquired aplastic anemia: immune‑mediated bone marrow failure syndromes (Review). Int J Oncol. 2022;60:7. doi:10.3892/ijo.2021.5297
57. Dai Y, Yang W, Sun Z, Wu L, Shao K, Wu D. Current knowledge of immune checkpoint inhibitor-induced thrombocytopenia: epidemiology, mechanisms, and management. Cancer Med. 2026;15:e71948. doi:10.1002/cam4.71948
58. Michot JM, Lazarovici J, Tieu A, et al. Haematological immune-related adverse events with immune checkpoint inhibitors, how to manage? Eur J Cancer. 2019;122:72–90. doi:10.1016/j.ejca.2019.07.014
59. Hu YP, Zhang AW. Occurrence and literature analysis of immune-related adverse reactions caused by sintilimab in the treatment of lung cancer. J Dis Monitor Control. 2024;18:425–430. doi:10.19891/j.issn1673-9388.(2024)06-0425-06
60. Li Y, Zhang Y, Jia X, et al. Effect of immune-related adverse events and pneumonitis on prognosis in advanced non-small cell lung cancer: a comprehensive systematic review and meta-analysis. Clin Lung Cancer. 2021;22:e889–e900. doi:10.1016/j.cllc.2021.05.004
61. Cui P, Liu Z, Wang G, et al. Risk factors for pneumonitis in patients treated with anti-programmed death-1 therapy: a case-control study. Cancer Med. 2018;7:4115–4120. doi:10.1002/cam4.1579
62. Karayama M. Immune checkpoint inhibitor-related pneumonitis: from guidelines to the front lines. Respir Investig. 2025;63:1002–1011. doi:10.1016/j.resinv.2025.07.023
63. Chinese Thoracic Society. Chinese Anti-Cancer Association Committee on Respiratory Oncology, Beijing Cancer Prevention and Treatment Research Association. Expert consensus on diagnosis and management of immune checkpoint inhibitor-related pneumonitis (2025). Chin J Tuberc Respir Dis. 2025;48:329–343. doi:10.3760/cma.j.cn112147-20241121-00694
64. Chen Y, Xu L, Zou S, Chen J, Xu X. Risk factors and mechanisms of immune checkpoint inhibitor-related pneumonitis. Hum Vaccin Immunother. 2025;21:2564554. doi:10.1080/21645515.2025.2564554
65. Li S, Geng Z, Hong S, et al. Advances in the mechanisms, imaging characteristics and management strategies for immune checkpoint inhibitor-related pneumonitis. Front Immunol. 2025;16:1656063. doi:10.3389/fimmu.2025.1656063
66. Chinese Society of Clinical Oncology (CSCO). Anti-Cancer Drug-Induced Liver Injury Guidelines 2024. Beijing: People’s Medical Publishing House; 2024:1–113.
67. Thompson JA, Schneider BJ, Brahmer J, et al. NCCN Guidelines® Insights: management of immunotherapy-related toxicities, Version 2.2024. J Natl Compr Canc Netw. 2024;22:582–592. doi:10.6004/jnccn.2024.0057
68. Riveiro-Barciela M, Barreira-Díaz A, Salcedo MT, et al. An algorithm based on immunotherapy discontinuation and liver biopsy spares corticosteroids in two thirds of cases of severe checkpoint inhibitor-induced liver injury. Aliment Pharmacol Ther. 2024;59:865–876. doi:10.1111/apt.17898
69. Remash D, Prince DS, McKenzie C, Strasser SI, Kao S, Liu K. Immune checkpoint inhibitor-related hepatotoxicity: a review. World J Gastroenterol. 2021;27:5376–5391. doi:10.3748/wjg.v27.i32.5376
70. Yamamoto T, Ito T, Suzuki T, et al. Steroid initiation dose and duration of steroid reduction for immune checkpoint inhibitor-induced liver injury. Hepatol Res. 2025;55:977–985. doi:10.1111/hepr.14200
71. Zhang N, Li Z, Liu Y, et al. Management and treatment of severe immune-related hepatotoxicity based on clinical and pathological characteristics. Hepatol Int. 2024;18:1770–1780. doi:10.1007/s12072-024-10688-0
72. Li M, Wong D, Vogel AS, et al. Effect of corticosteroid dosing on outcomes in high-grade immune checkpoint inhibitor hepatitis. Hepatology. 2022;75:531–540. doi:10.1002/hep.32215
73. Awada A, Tarhini A, Hammoud A, et al. Hematologic toxicity of immune checkpoint inhibitors: real-world burden and risk profiles from a five-year cohort from the Middle East. BMC Cancer. 2026. doi:10.1186/s12885-026-16117-9
74. Schneider BJ, Naidoo J, Santomasso BD, et al. Management of immune-related adverse events in patients treated with immune checkpoint inhibitor therapy: ASCO guideline update. J Clin Oncol. 2021;39:4073–4126. doi:10.1200/JCO.21.01440
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Case of Hepatocellular Carcinoma Successfully Resumed Atezolizumab and Bevacizumab After Associated Grade 3 Diarrhea and Grade 2 Colitis: Case Report and Literature Review
Fuji T, Arai J, Otoyama Y, Nio Y, Sugiura I, Nakajima Y, Kajiwara A, Ichikawa Y, Uozumi S, Shimozuma Y, Uchikoshi M, Sakaki M, Nozawa H, Momo K, Sasaki T, Yoshida H
OncoTargets and Therapy 2022, 15:1281-1288
Published Date: 25 October 2022
Onychopathy Following Durvalumab Treatment for Extensive-Stage Small-Cell Lung Cancer: A Case Report
Zhang C, Wang K, Zhang H, Liu J, Zheng C, Tao J, Lin L, Zhai L
Clinical, Cosmetic and Investigational Dermatology 2023, 16:2429-2432
Published Date: 5 September 2023
Immune Checkpoint Inhibitor-Associated Systemic Sclerosis in the Treatment of a Small Cell Lung Cancer Patient with Durvalumab: A Case Report
Li DH, Xiong XZ
Clinical, Cosmetic and Investigational Dermatology 2024, 17:663-669
Published Date: 18 March 2024
Case Report and Literature Review on Skin Toxicity Induced by PD-1 Inhibitor in a Penile Cancer with Massive Ulceration of Chemoradiotherapy-Resistant and Successful Treatment by Immunotherapy
Zhu Y, Cai D, Jiang J, Tu J, Tian Z, Zhang X, Luo S, Wang Y
Clinical, Cosmetic and Investigational Dermatology 2025, 18:699-707
Published Date: 22 March 2025
Rhabdomyolysis as a Predominant Multisystem Serious Immune-Related Adverse Event Induced by Sintilimab: A Case Report and Literature Review
Duan Q, Zhang X, Li M
Cancer Management and Research 2025, 17:3383-3392
Published Date: 31 December 2025