Back to Journals » Cancer Management and Research » Volume 17

Rhabdomyolysis as a Predominant Multisystem Serious Immune-Related Adverse Event Induced by Sintilimab: A Case Report and Literature Review
Received 8 September 2025
Accepted for publication 21 December 2025
Published 31 December 2025 Volume 2025:17 Pages 3383—3392
DOI https://doi.org/10.2147/CMAR.S564116
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Harikrishna Nakshatri
Qingyuan Duan, Xueying Zhang, Minjie Li
Department of Radiotherapy, The Fifth Affiliated Hospital of Zhengzhou University, Zhengzhou, People’s Republic of China
Correspondence: Minjie Li, The Fifth Affiliated Hospital of Zhengzhou University, Zhengzhou, People’s Republic of China, Email [email protected]
Abstract: Cancer treatment has entered the era of immunotherapy after surgery, radiotherapy, chemotherapy, and targeted therapy. The immune-related adverse events (irAEs) associated with immune checkpoint inhibitors (ICIs) have become a significant concern in clinical practice, given the broad application of these agents. This article reports a case of immune polymyositis involving the myocardium and rhabdomyolysis in a patient with lung adenocarcinoma combined with brain metastases treated with sintilimab. In addition, there was simultaneous involvement of other systems with immune-associated hepatitis, thyrotoxicosis, and secondary hypoadrenalism. After high-dose corticosteroid shock therapy administration, the patient’s symptoms and indicators improved significantly.
Keywords: sintilimab, immune-related adverse events, rhabdomyolysis, immune-related myositis, secondary adrenal insufficiency, corticosteroids
Introduction
Immune checkpoints are a class of negative regulatory proteins that inhibit the activity of immune cells. This phenomenon enables certain tumor cells to evade the immune system’s attack. Immune checkpoint inhibitors (ICIs) block down-regulation pathways, stimulating T-cell proliferation, and enhancing the body’s antitumor immunity. While activating antitumor immunity, ICIs may disrupt autoimmune homeostasis, leading to inflammatory toxicities that can affect nearly all systems and organs. These reactions are defined as immune-related adverse events (irAEs), with the skin, gastrointestinal tract and liver being the most frequently affected systems.1 While neuromuscular irAEs occur in <6% of patients, and ICI-associated myocarditis is reported at a frequency of 0.27% to 1.14%.2 The occurrence of multisystem irAEs is much rarer. The present case report concerns a patient with brain metastases from lung adenocarcinoma who developed severe irAEs in multiple systems manifested by rhabdomyolysis after sintilimab, some of which were very insidious in that the patient did not have corresponding clinical symptoms despite the involvement of some systems. To avoid missed diagnosis and facilitate early diagnosis, clinical indicators should be detected promptly, and patients should be monitored for the possibility of multisystem involvement. Our case provides experience and reference for clinical diagnosis and treatment.
Case Presentation
A 55-year-old woman was diagnosed with lung adenocarcinoma in 2022, and genetic testing revealed an epidermal growth factor receptor (EGFR) mutation. She underwent interventional embolization of a lesion in her right lung and received eight cycles of chemotherapy with Pemetrexed. Following that, she received treatment with Gefitinib, a targeted therapy. The patient’s condition demonstrated stability during the period of review. On January 31, 2024, the cranial MRI revealed occupancy in the right frontal lobe and cerebellar hemisphere accompanied by peripheral cerebral parenchymal edema. Given the patient’s medical history, this finding was interpreted as indicative of a metastatic brain tumor. Due to the patient’s condition progression, she discontinued Gefitinib targeted therapy and received systemic chemotherapy three times (details unknown). On March 23, 2024, the cranial MRI revealed that the mass in the right cerebellar hemisphere and the surrounding edematous band had increased in size compared to the previous scan. Chemotherapy was ineffective, and the disease continued to progress. On May 31, 2024, she was hospitalized in the Radiotherapy Department at the Fifth Affiliated Hospital of Zhengzhou University for whole brain radiotherapy, receiving 40 Gy in total,delivered as 20 fractions (Intensity-Modulated Radiotherapy, IMRT) (Figures 1 and 2) On June 13, 2024, she commenced treatment with sintilimab (200 mg) as an anti-immunotherapy, in conjunction with Bevacizumab (600 mg) for anti-vascular therapy. This combined regimen was administered every three weeks for two cycles throughout the radiotherapy course.
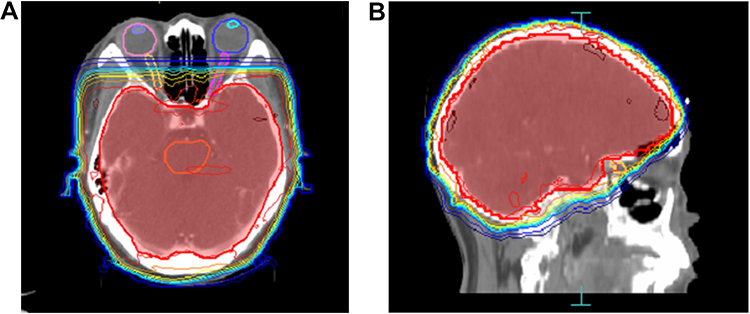 |
Figure 1 Radiotherapy target delineation and organs-at-risk (OARs) protection. (A) Axial view; (B) Sagittal view. The red region denotes the whole-brain planning target volume (PTV). Critical organs at risk—including the lenses, optic nerves, and brainstem—are contoured using distinct color overlays. This delineation strategy ensures adequate dose coverage of the target volume while optimizing the sparing of surrounding normal tissues. |
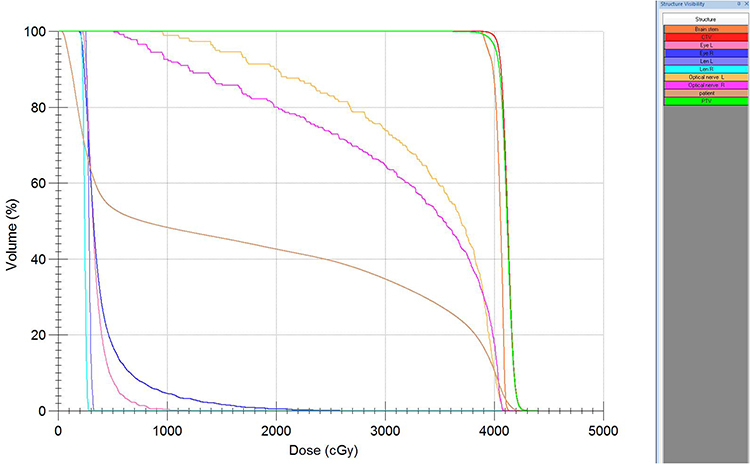 |
Figure 2 Dose-volume histogram (DVH) of the whole-brain radiotherapy plan. The curves delineate the planned dose distributions for the target volumes and OARs. The planning target volume (PTV, green curve) shows that over 95% of its volume received the prescribed dose of 40 Gy, meeting the prescription dose requirements. The dose constraints for all OARs were met. |
On July 8, 2024, the patient gradually experienced symptoms such as poor appetite, difficulty opening the eyes, and impaired tongue mobility, which were initially ignored. After one week, these symptoms progressed, accompanied by dysphagia, choking while drinking, neck weakness, generalized limb weakness and soreness, difficulty lifting both shoulders, and trouble standing up after squatting. The patient did not receive any treatment during this period. On July 20, 2024, she was admitted to our hospital for treatment. Neurological examination revealed normal higher mental functions and slightly unclear articulation, but the patient could respond fluently to questions. Bilateral ptosis was observed, with limited upward gaze of both eyes and restricted tongue protrusion. The patient experienced choking while drinking, dysphagia, and exhibited limb muscle strength at 5- grade, with normal muscle tone. Tendon reflexes in all four limbs were symmetrically diminished, while deep and superficial sensation, as well as coordination showed no significant abnormalities. Signs of meningeal irritation were negative. The patient has hypertension, which is usually well managed. There is no history of hepatitis, immune-related diseases, or other cardiovascular or cerebrovascular diseases.
Laboratory tests performed after admission yielded the following results: Markers of myocardial and skeletal muscle injury were markedly elevated, including creatine kinase (CK) at 11,019 U/L (reference: 40–200), CK-MB isoenzyme at 288.5 U/L (reference: 0–24.0), lactate dehydrogenase (LDH) at 1,540 U/L (reference: 120–250), myoglobin (MYO) at 1,450 ng/L (reference: 25–58), and cardiac troponin T (cTnT) at 0.566 ng/mL (reference: <0.014). Electrolytes, creatinine, and glomerular filtration rate showed no significant abnormalities. Liver function tests also revealed abnormalities, with alanine aminotransferase (ALT) elevated to 367 U/L (reference: 7–40) and aspartate aminotransferase (AST) increased to 430 U/L (reference: 15–40). Endocrine testing revealed abnormalities. Morning adrenocorticotropic hormone (ACTH) was 5.4 pg/mL (reference: 7.2–63.3), cortisol (COR) was 37.0 nmol/L (reference: 172.0–497.0). Thyroid-stimulating hormone (TSH) measured 0.016 mIU/L (reference: 0.50–5.50), free triiodothyronine (FT3) was 7.74 pmol/L (reference: 2.80–6.80), and free thyroxine (FT4) was 33.47 pmol/L (reference: 11.50–22.70) (Table 1). Electrocardiography (ECG) revealed right bundle branch block and ST-T segment abnormalities (Figure 3). Chest CT showed no significant cardiac abnormalities and excluded the possibility of a thymoma. Brain MRI revealed no significant abnormalities in the pituitary gland, and no progression of metastatic brain lesions was observed. Due to the patient’s preference and financial reasons, the myositis-specific autoantibody test was not performed.
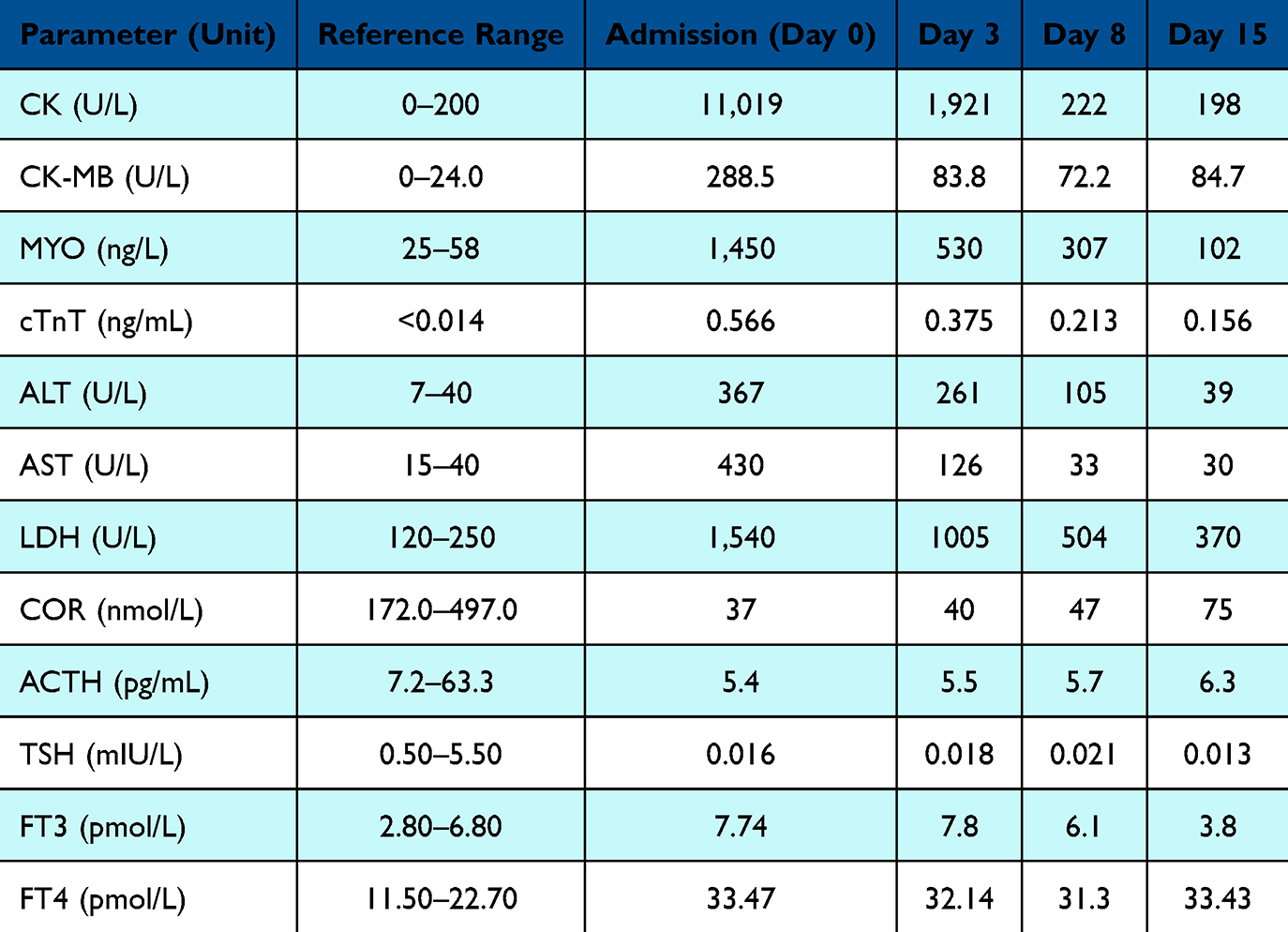 |
Table 1 Dynamic Changes in Key Laboratory Parameters During Hospitalization. Serial Measurements of Biomarkers for Cardiac, Skeletal Muscle, Hepatic, and Endocrine Function are Shown at Specified Time Points After Admission (Admission Day, Hospital Day 3, 8, and 15). Data are Presented with Reference Ranges |
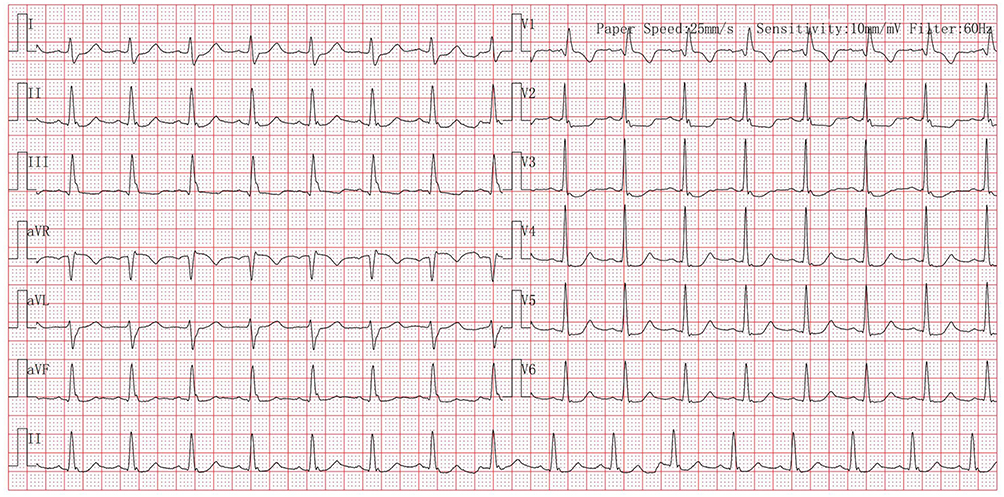 |
Figure 3 The standard 12-lead ECG obtained at hospital admission. The ECG findings of right bundle branch block and ST-T segment changes, combined with elevated cTnT and CK-MB, are consistent with immune-mediated myocarditis. |
The patient, diagnosed with lung adenocarcinoma with brain metastases, had undergone two cycles of sintilimab treatment. Recently, the patient developed symptoms including ptosis, dysphagia, and limb weakness. After admission, recurrence or progression of brain tumors and stroke were excluded as potential causes. Based on laboratory findings and multidisciplinary consultations involving neurology, cardiology, endocrinology, and rheumatology departments, the diagnosis was established as sintilimab -induced multisystem irAEs, including polymyositis (Grade 3 and Grade 4) involving myocardium (Grade 1), rhabdomyolysis, hepatitis (Grade 3), thyrotoxicosis, and secondary adrenal insufficiency (Grade 2). Given the occurrence of these severe (Grades 3–4) multisystem irAEs, immunotherapy was permanently discontinued.
The patient received intravenous methylprednisolone pulse therapy at a dosage of 500 mg per day. To prevent stress ulcers and gastrointestinal bleeding, omeprazole was administered. For rhabdomyolysis, aggressive intravenous fluid therapy was simultaneously started, consisting of approximately 6 liters of isotonic saline per day, aiming to maintain a urine output of 200–300 mL per hour during the first 24 hours. Calcium gluconate was administered to counteract hyperkalemia, and 100 mL of 5% sodium bicarbonate was used to alkalinize the urine. Urine output and electrolytes were closely monitored. After two days, the patient showed improvement in ptosis and neck muscle weakness and was able to gradually resume slow oral intake. Laboratory evaluations demonstrated a marked and rapid decline in CK and CK-MB levels, which supported the initiation of a stepwise tapering of methylprednisolone (250 mg/d × 2 d → 125 mg/d × 2 d → 80 mg/d × 2 d → 40 mg/d until discharge). Thereafter, CK and CK-MB continued to decline steadily throughout hospitalization and had normalized by the time of discharge. In addition, liver enzyme levels—including ALT, AST, and LDH—also demonstrated a progressive decline, which was highly consistent with the patient’s gradual clinical improvement (Figures 4–6). Fluid therapy was also reduced to 2 liters per day once symptoms improved and CK decreased below 2000 U/L, with subsequent adjustments and tapering based on the patient’s condition and laboratory results. During treatment, blood pressure fluctuations were observed and managed with oral sustained-release metoprolol and continuous sodium nitroprusside infusion to stabilize blood pressure. Laboratory parameters normalized approximately 15 days following admission. The patient was discharged on hospital day 17 following marked clinical improvement. The patient was advised to keep taking oral prednisone acetate (50 mg/day) with a tapering regimen for maintenance therapy and to attend regular follow-up appointments. A telephone follow-up two months after discharge revealed that the patient indicated that all symptoms had fully resolved and had recently self-discontinued prednisone acetate, having taken it for approximately two months in total. However, hospital follow-up examinations had not been attended. The overall clinical course is summarized in Figure 7 (Timeline).
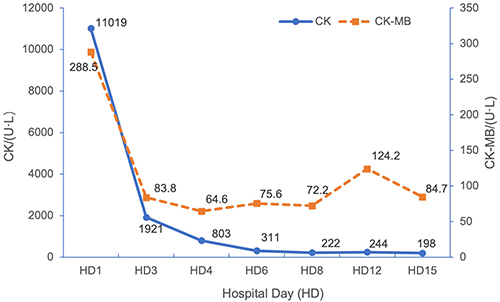 |
Figure 4 Dynamic changes of CK and CK-MB after admission. Following initiation of methylprednisolone pulse therapy, CK and CK-MB levels exhibited a rapid and marked decline. At admission, CK was 11,019 U/L (over 50-fold above the upper limit of normal) and CK-MB was 288.5 U/L (11-fold above the upper limit of normal). By Hospital Day 15 (HD15), both markers had decreased to near-normal levels (CK 83.8 U/L, CK-MB 7.2 U/L), reflecting resolution of rhabdomyolysis and concomitant myocardial injury. |
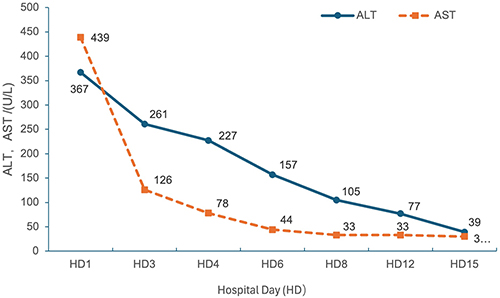 |
Figure 5 Dynamic changes of liver function indices (ALT, AST) after admission. At admission, AST (430 U/L) and ALT (367 U/L) were both markedly elevated, exceeding 10 times the upper limit of normal, indicating moderate liver injury. Following treatment, both enzymes showed a continuous and gradual decline: on Hospital Day 3 (HD3), AST decreased to 261 U/L and ALT to 227 U/L; by HD15, both returned to within normal limits (33 U/L). |
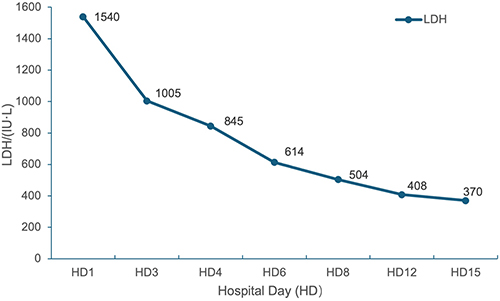 |
Figure 6 Dynamic changes of LDH after admission. At admission, LDH was markedly elevated at 1540 U/L, approximately six times the upper limit of normal, indirectly reflecting concomitant muscle and liver injury. Following treatment, LDH demonstrated a gradual decline, initially slower than CK and AST, but eventually normalized with tissue recovery, indicating overall clinical improvement. |
 |
Figure 7 Timeline of the patient’s clinical course. The timeline summarizes key clinical events, including tumor-directed therapies, initiation of sintilimab, onset and progression of irAEs, hospitalization, initiation of corticosteroid pulse therapy, stepwise tapering of steroids, and eventual clinical recovery. |
Discussion
Since the initial FDA approval of ipilimumab for metastatic melanoma in 2011, various checkpoint blockade therapies have been authorized for multiple tumor types. Sintilimab is a Programmed Death-1 (PD-1) inhibitor. Initially approved in China in Dec 2018, indicated for Hodgkin’s lymphoma, sintilimab has since demonstrated substantial clinical efficacy across multiple malignancies. Its approved indications now encompass classical Hodgkin’s lymphoma, non-small cell lung cancer (NSCLC), adenocarcinoma of the stomach and gastroesophageal junction, among others. In this case, sintilimab combined with bevacizumab was used to treat metastatic NSCLC, aligning with its approved clinical indications.
Given the pervasive utilization of ICIs in clinical practice, more irAEs have come to our attention. Understanding the mechanisms behind their occurrence is crucial for enhancing the safety of immunotherapy. The mechanisms by which irAEs occur are complex, involving multiple immune cells, cytokines, and imbalances in regulating immune tolerance. T cells are central to this process, though the exact mechanism remains unclear. The main mechanisms include:3 1) Reduced peripheral immune tolerance by T cells and the proliferation of self-reactive CD4+ and CD8+ T cell clones, resulting in autoimmune activation. 2) Normal tissues and tumor tissues share common antigens, where specific T cell clones recognize these antigens and induce ICI-related toxicity through specific autoimmune responses. 3) Treg cells maintain immune homeostasis by eliminating self-reactive T cells. ICIs directly result in Treg cell depletion, thereby disrupting the immune balance.
The incidence of adverse events varies among different inhibitors. Retrospective analysis revealed that PD-1 inhibitors are better tolerated than Cytotoxic T-Lymphocyte-Associated Protein 4 (CTLA-4) inhibitors and are more frequently associated with thyroiditis and respiratory adverse events.4 Neuromuscular system-related irAEs are rare across all types of ICIs, with the incidence of ICI-associated myositis being less than 1%. Despite its low occurrence, ICI-associated myositis often coexists with conditions like myasthenia gravis (MG) and myocarditis overlap syndrome, which can lead to rapid and severe progression with high mortality rates. Patients diagnosed with both myositis and myocarditis face mortality rates exceeding 50%, and more than one-third of survivors experience persistent neuromuscular sequelae.5 Anti-PD-1 therapy confers a 2.4-fold greater myositis risk than anti-CTLA-4 treatment, primarily affecting men over the age of 65 (70%). Safety data for sintilimab indicate that ICI-associated myositis occurred only in patients receiving sintilimab combination therapy, with an infrequent occurrence rate (<1/100 to >1/1000). Currently, reports of sintilimab -associated myositis are limited, and most cases involve overlap syndromes with poor prognosis. Early recognition and intervention for ICI-associated myositis are critically important.
ICI-associated myositis tends to have an early onset, usually occurring within the initial 4 weeks of checkpoint inhibitor therapy, commonly following the first or second administration cycle.6 Our patient also presented with systemic symptoms such as difficulty opening the eyes, choking while drinking, and limb weakness within one week after the second treatment. Additionally, blood biochemical analysis indicated substantially increased levels of cardiac biomarkers, creatine kinase, and transaminases, with creatine kinase exceeding 50-fold the normal upper limit. Although the patient did not present with cardiac symptoms like chest pain, chest pressure or dyspnea, the ECG showed conduction blocks and “ST-T” changes, which were not observed before immunotherapy. Combined with elevated troponin and CK-MB levels, these findings indicate a certain degree of myocardial injury. The diagnosis was confirmed as “immune-related polymyositis involving the myocardium” and “rhabdomyolysis.” In contrast to the clinical symptoms of primary inflammatory myopathies, ICI-associated myositis primarily involves significant ocular muscle and bulbar regions. However, ICI-related myositis appears to overlap with the clinical symptoms of myasthenia gravis (MG). Some ICI-associated myositis patients, even without anti-acetylcholine receptor antibodies, exhibit MG-like symptoms. Similar to myositis, ICI-associated MG is less common with anti-CTLA-4 treatment than it is with anti-PD-1/PD-L1 treatment.5 Therefore, the link between ICI-associated myositis and MG may not be coincidental and requires further investigation. Clinically, vigilance is warranted for the overlapping diagnoses of these two conditions, with muscle biopsy being the gold standard for differentiation. Unfortunately, the patient declined this examination due to its invasive nature. The patient did not exhibit typical MG features such as fluctuation or symptoms that are mild in the morning and worsen by evening, and both the fatiguability test and ice pack test were negative. Given the clinical presentation and examination outcomes, a diagnosis of myasthenia gravis is not being considered at this time. Previous pathological findings of ICI-associated myositis showed macrophage and CD8+ T cell infiltration, along with muscle fiber necrosis.6 This further supports the notion that irAEs are linked to T-cell overactivation.
“Rhabdomyolysis” represents the most prominent feature in our patient. PD-1 inhibitor-induced rhabdomyolysis is uncommon, with only one previously documented case associated with sintilimab. That case involved a 66-year-old patient suffering from lung adenocarcinoma who experienced immune-related myositis overlapping with myocarditis and myasthenia gravis after two cycles of sintilimab.7 This patient also had a previous history of thymoma. Similarly, a colorectal cancer patient developed a syndrome of overlapping rhabdomyolysis, myasthenia gravis, and myocarditis following treatment with tislelizumab, with elevated anti-acetylcholine receptor antibody (anti-AChR-Ab) levels detected.8 There has also been a report of a case where a patient developed acute rhabdomyolysis accompanied by severe polymyositis after receiving combination therapy with nivolumab and ipilimumab. Notably, this patient had elevated anti-SM antibody levels before treatment.9 Furthermore, there is a patient with subclinical elevation of anti-AChR-Ab who developed immune checkpoint inhibitor-associated myositis and myasthenic crisis following nivolumab treatment.10 These observations suggest that the development of ICI-associated myopathy may be associated with autoimmune diseases or elevated titers of specific antibodies. Such patients have a higher likelihood of overlap syndromes and tend to exhibit more severe conditions. Sumimoto et al’s retrospective analysis11 further corroborates this view, showing that autoimmune diseases constitute an independent risk factor for irAEs in patients undergoing ICI therapy. Interestingly, in contrast to the severe cases mentioned above, their findings indicate that irAEs are generally less severe, even among patients with pre-existing immune system diseases. Nevertheless, CIS should be used cautiously in this population, accompanied by close monitoring for potential adverse reactions. Antibody testing prior to ICI therapy is necessary. Relevant serum immunological markers in reported cases primarily include myositis-specific antibodies (MSAs), myositis-associated antibodies (MAAs), anti-skeletal muscle antibodies (AsM-Ab), and acetylcholine receptor antibodies (AchR-Ab). Furthermore, rhabdomyolysis after ICI therapy could be attributed to other factors, requiring clinicians to consider differential diagnoses carefully. Min et al12 described a melanoma patient who experienced hypothyroidism and rhabdomyolysis following ipilimumab treatment. After receiving only levothyroxine replacement therapy, the patient’s thyroid function and creatine kinase levels normalized, indicating that rhabdomyolysis was likely associated with hypothyroidism rather than the ICIs itself.
Of particular interest in this case is the occurrence of endocrine-related adverse events, particularly adrenal insufficiency (AI) and thyrotoxicosis. For NSCLC patients, the occurrence of AI during anti-PD-1 therapy is 1.4%with males being more frequently affected than females.13–15 ICI-induced AI typically presents with nonspecific symptoms, including fatigue, weight loss, nausea, and decreased appetite, with fatigue being the most frequent manifestation. Due to the vague nature of these symptoms, clinicians often face challenges in achieving prompt and accurate diagnosis of AI. Early identification primarily depends on measuring 8:00 AM serum cortisol, ACTH, and electrolyte levels. In our case, a significant reduction in cortisol and ACTH levels led to the diagnosis of secondary AI caused by ICI-related pituitary injury. Although cranial MRI showed no abnormalities in the pituitary gland, this aligns with previous findings: hypophysitis induced by anti-PD-1 therapy often presents without detectable changes on MRI,14,15 and any observed MRI abnormalities typically disappear completely after stopping the treatment.16 Clinically, cortisol and ACTH are not routine assessment measures, emphasizing the need for biomarkers to facilitate early diagnosis. A study suggests that eosinophilia might be linked to secondary AI, and some case reports indicate elevated eosinophil counts prior to the onset of symptoms.14,15 In our patient, eosinophil levels were normal, and the predictive potential of eosinophils warrants further investigation. Moreover, a study17 has indicated that eosinophilia may function as a predictive biomarker for antitumor efficacy and overall survival. Based on this, we hypothesize that development of AI may be associated with enhanced therapeutic efficacy. Analyses18,19 have indicated that cancer patients (notably those with melanoma and lung cancer) demonstrate improved therapeutic outcomes, particularly regarding PFS and OS, after experiencing irAEs, especially those affecting the endocrine, skin, and gastrointestinal systems. Nevertheless, the mechanisms driving this correlation are not yet fully understood, and different types of irAEs may have varying effects on prognosis and survival.
Thyroid irAEs represents one of the most frequent endocrine toxicities observed during ICI therapy. The overall incidence of thyroid irAEs is approximately 10.8%, with PD-1 inhibitors demonstrating a stronger association than their occurrence than CTLA-4 inhibitors.20 Additionally, female patients are more commonly affected than males.21 Thyroid irAEs encompass hyperthyroidism, thyrotoxicosis, hypothyroidism, and thyroid storm. Thyrotoxicosis generally manifests early, within 3 to 6 weeks following treatment,20 although there have been reports of thyrotoxicosis appearing as late as one year after therapy. Thyrotoxicosis is often asymptomatic, and most progress dynamically to hypothyroidism within a short period (median 42 days).21 Of these, approximately 40% of patients develop permanent hypothyroidism, requiring lifelong levothyroxine replacement therapy.22 We recommend regular thyroid function monitoring for patients receiving ICI therapy to detect changes promptly and implement tailored management—such as β-blockers for symptomatic thyrotoxicosis or levothyroxine replacement for hypothyroidism.
Currently, corticosteroids remain the first-line treatment for irAEs. Consensus on irAEs management includes discontinuing ICIs, providing supportive care, and administering high-dose corticosteroids.23 As per ASCO clinical guidelines, treatment strategies are determined by the severity of the irAEs. Higher grades of irAEs require increased doses of corticosteroids. For grade 3 adverse events, high-dose corticosteroid therapy is indicated—typically prednisone or methylprednisolone at 1–2 mg/kg/day, followed by a slow tapering over 4–6 weeks. For those with persistent symptoms, further immunosuppressive therapy, such as infliximab, is needed. Recurrent grade 3 and 4 adverse events warrant permanent discontinuation of ICIs.24 For the treatment of ICI-associated myositis, grade 1–2 cases can be managed with corticosteroid therapy (0.5–1 mg/kg). For grade 3–4 cases, high-dose methylprednisolone (500–1000 mg/day) pulse therapy is advised, in addition to discontinuing ICIs. For critically ill patients, plasma exchange and/or life support therapy may be required. After two days of pulse therapy with 500 mg/day, the patient’s fatigue symptoms improved, accompanied by a reduction in creatine kinase levels and other relevant biomarkers. No additional immunosuppressive therapy was administered. If symptoms remain unresolved after pulse therapy, particularly in myocarditis patients, studies show that 25%-50% of ICI-related myocarditis patients do not improve or may even worsen following high-dose methylprednisolone pulse therapy.25 In these instances, intravenous immunoglobulin (IVIG) or other immunosuppressive treatments, including IL-6 antagonists, TNF-α inhibitors, and biologics (such as rituximab) should be considered. If symptoms and markers have not returned to normal after 4 weeks, other immunosuppressive agents—including methotrexate, azathioprine, and mycophenolate mofetil—ought to be considered.24 However, the widespread clinical use of corticosteroids has raised several concerns: corticosteroid side effects, the potential for corticosteroids to promote tumor progression and resistance to corticosteroids in certain irAEs.26,27 These limitations have also driven researchers to seek alternative drugs in pursuit of more optimal treatments. Currently, the main drugs under investigation include biologics (infliximab, tocilizumab, abatacept), antibody-based drugs (rituximab, secukinumab), targeted small molecule drugs (baricitinib, tofacitinib), intravenous immunoglobulin (IVIG), anti-thymocyte globulin (ATG), and mycophenolate mofetil (MMF).23 Overall, the landscape of irAEs pharmacotherapy is becoming increasingly diversified and precise. By incorporating new biologics, targeted therapies, and personalized treatment strategies, it is anticipated that future irAEs therapies will effectively manage immune-related adverse events while preserving antitumor effectiveness.
This case has several limitations. First, the patient declined both antibody testing and muscle biopsy, making it impossible to speculate whether the occurrence of irAEs in this patient is associated with antibody elevation. The absence of pathological results also precluded further investigation into the cellular and molecular mechanisms underlying the irAEs. Second, the reporting timeline is relatively close to the onset of the patient’s symptoms, and no long-term follow-up data are available. Consequently, the influence of irAEs on the patient’s primary tumor and brain metastases remains unclear. We intend to maintain ongoing follow-up for this patient in the future.
Conclusion
In conclusion, this case report describes a 55-year-old female lung cancer patient who developed severe multisystem irAEs, dominated by rhabdomyolysis, following sintilimab treatment. Following high-dose corticosteroid pulse therapy, the patient exhibited significant clinical improvement as early as the third day. Although the side effects of corticosteroids cannot be overlooked, the outcome in this case supports their role as an effective and practical core therapeutic option in critical situations. Nevertheless, regular multisystem monitoring and early differential diagnosis are essential for timely identification and management.
Data Sharing Statement
Materials supporting this study’s findings are in the article or its supplements. Should you need additional details, please get in touch with the corresponding author.
Ethics Approval
All the methods were carried out in accordance with the Declaration of Helsinki. In compliance with our institutional policies, the publication of this case report does not require specific ethical approval from an institutional review board.
Consent for Publication
The patient are informed and have given their consent to publish this paper.
Acknowledgments
The views expressed in this article are the authors’ alone and do not reflect the views of their affiliations, the publisher, editors, or reviewers. Mention of any products or claims does not imply endorsement by the publisher.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors confirm that the entire research process, from investigation to article publication, was conducted without external financial support.
Disclosure
The authors report no potential conflicts of interest in this work.
References
1. Postow MA, Sidlow R, Hellmann MD, Longo DL. Immune-Related Adverse Events Associated with Immune Checkpoint Blockade. New England J Med. 2018;378(2):158–168. doi:10.1056/NEJMra1703481
2. Casagrande S, Sopetto GB, Bertalot G, et al. Immune-Related Adverse Events Due to Cancer Immunotherapy: immune Mechanisms and Clinical Manifestations. Cancers. 2024;16(7):1440. doi:10.3390/cancers16071440
3. Arnaud-Coffin P, Maillet D, Gan HK, et al. A systematic review of adverse events in randomized trials assessing immune checkpoint inhibitors. Int J Cancer. 2019;145(3):639–648. doi:10.1002/ijc.32132
4. Nguyễn T, Maria ATJ, Ladhari C, et al. Rheumatic disorders associated with immune checkpoint inhibitors: what about myositis? An analysis of the WHO’s adverse drug reactions database. Ann Rheum Dis. 2022;81(2):e32. doi:10.1136/annrheumdis-2020-217018
5. O’Hare M, Guidon AC. Peripheral nervous system immune-related adverse events due to checkpoint inhibition. Nat Rev Neurol. 2024;20(9):509–525. doi:10.1038/s41582-024-01001-6.
6. Xing Q, Zhang ZW, Lin QH, et al. Myositis-myasthenia gravis overlap syndrome complicated with myasthenia crisis and myocarditis associated with anti-programmed cell death-1 (Sintilimab) therapy for lung adenocarcinoma. Ann Transl Med. 2020;8(5):250. doi:10.21037/atm.2020.01.79
7. Wang S, Peng D, Zhu H, et al. Acetylcholine receptor binding antibody-associated myasthenia gravis, myocarditis, and rhabdomyolysis induced by tislelizumab in a patient with colon cancer: a case report and literature review. Front Oncol. 2022;12:1053370. doi:10.3389/fonc.2022.1053370
8. Bilen MA, Subudhi SK, Gao J, Tannir NM, Tu SM, Sharma P. Acute rhabdomyolysis with severe polymyositis following ipilimumab-nivolumab treatment in a cancer patient with elevated anti-striated muscle antibody. J Immunother Cancer. 2016;4(36). doi:10.1186/s40425-016-0139-8
9. Kimura T, Fukushima S, Miyashita A, et al. Myasthenic crisis and polymyositis induced by one dose of nivolumab. Cancer Sci. 2016;107(7):1055–1058. doi:10.1111/cas.12961
10. Sumimoto H, Noda S, Koide H, et al. Pre-existing autoimmune disease as a risk factor for immune-related adverse events in cancer patients receiving immune checkpoint inhibitors. PLoS One. 2024;19(7):e0306995. doi:10.1371/journal.pone.0306995
11. Min L, Hodi FS. Anti-PD1 following ipilimumab for mucosal melanoma: durable tumor response associated with severe hypothyroidism and rhabdomyolysis. Cancer Immunol Res. 2014;2(1):15–18. doi:10.1158/2326-6066.CIR-13-0146
12. Ida H, Goto Y, Sato J, et al. Clinical characteristics of adrenal insufficiency as an immune-related adverse event in non-small-cell lung cancer. Med Oncol. 2020;37(4):30. doi:10.1007/s12032-020-01357-x
13. Suzuki K, Terakawa T, Furukawa J, et al. Nivolumab-induced Adrenal Insufficiency in Patients with Renal Cell Carcinoma. Journal of Immunotherapy. 2020;43(1):38–42. doi:10.1097/CJI.0000000000000299
14. Ariyasu R, Horiike A, Yoshizawa T, et al. Adrenal Insufficiency Related to Anti-Programmed Death-1 Therapy. Anticancer Res. 2017;37(8):4229–4232. doi:10.21873/anticanres.11814
15. Carpenter KJ, Murtagh RD, Lilienfeld H, Weber J, Murtagh FR. Ipilimumab-induced hypophysitis: MR imaging findings. AJNR Am J Neuroradiol. 2009;30(9):1751–1753. doi:10.3174/ajnr.A1623
16. Weide B, Martens A, Hassel JC, et al. Baseline biomarkers for outcome of melanoma patients treated with pembrolizumab. Clin Cancer Res. 2016;22(22):5487–5496. doi:10.1158/1078-0432.CCR-16-0127
17. Shankar B, Zhang J, Naqash AR, et al. Multisystem immune-related adverse events associated with immune checkpoint inhibitors for treatment of non-small cell lung cancer. JAMA Oncol. 2020;6(12):1952–1956. doi:10.1001/jamaoncol.2020.5012
18. Zhou X, Yao Z, Yang H, Liang N, Zhang X, Zhang F. Are immune-related adverse events associated with the efficacy of immune checkpoint inhibitors in patients with cancer? A systematic review and meta-analysis. BMC Med. 2020;18(1):87. doi:10.1186/s12916-020-01549-2
19. Muir CA, Menzies AM, Clifton-Bligh R, Tsang VHM. Thyroid toxicity following immune checkpoint inhibitor treatment in advanced cancer. Thyroid. 2020;30(10):1458–1469. doi:10.1089/thy.2020.0032
20. Lee H, Hodi FS, Giobbie-Hurder A, et al. Characterization of thyroid disorders in patients receiving immune checkpoint inhibition therapy. Cancer Immunol Res. 2017;5(12):1133–1140. doi:10.1158/2326-6066.CIR-17-0208
21. Muir CA, Tsang VHM, Menzies AM, Clifton-Bligh RJ. Immune related adverse events of the thyroid - A narrative review. Front Endocrinol. 2022;13:886930. doi:10.3389/fendo.2022.886930
22. Chen YH, Kovács T, Ferdinandy P, Varga ZV. Treatment options for immune-related adverse events associated with immune checkpoint inhibitors. Br J Pharmacol. 2024. doi:10.1111/bph.16405
23. Schneider BJ, Naidoo J, Santomasso BD, et al. Management of immune-related adverse events in patients treated with immune checkpoint inhibitor therapy: ASCO guideline update. J Clin Oncol. 2021;39(36):4073–4126. doi:10.1200/JCO.21.01440
24. Mahmood SS, Fradley MG, Cohen JV, et al. Myocarditis in patients treated with immune checkpoint inhibitors. J Am Coll Cardiol. 2018;71(16):1755–1764. doi:10.1016/j.jacc.2018.02.037
25. Arbour KC, Mezquita L, Long N, et al. Impact of baseline steroids on efficacy of programmed cell death-1 and programmed death-ligand 1 blockade in patients with non-small-cell lung cancer. J Clin Oncol. 2018;36(28):2872–2878. doi:10.1200/JCO.2018.79.0006
26. Khadka S, Druffner SR, Duncan BC, Busada JT. Glucocorticoid regulation of cancer development and progression. Front Endocrinol. 2023;14:1161768. doi:10.3389/fendo.2023.1161768
27. In conclusion, this case report describes a 55-year-old female lung cancer patient who developed severe multisystem irAEs, dominated by rhabdomyolysis, following sintilimab treatment. Her rapid and significant clinical improvement, observed as early as the third day of high-dose corticosteroid pulse therapy, underscores the potential efficacy of corticosteroids in managing such life-threatening irAEs, even in complex presentations. This outcome reinforces that corticosteroids remain a critical, accessible, and cost-effective option in the therapeutic arsenal against severe irAEs. However, their use should be balanced against potential adverse effects. Importantly, this single case experience highlights the necessity for vigilant, multisystem monitoring and early differential diagnosis to ensure timely intervention. Future studies are needed to validate these findings and optimize management strategies across broader patient populations.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Sintilimab-Induced Sequential Multi-System Severe Immune-Related Adverse Events in an Elderly Patient with Esophageal Squamous Cell Carcinoma: A Case Report and Literature Review
Xia X, Yu T, Sun H, Li J, Liu F, Zhu X
OncoTargets and Therapy 2026, 19:606668
Published Date: 9 July 2026