Back to Journals » International Journal of Women's Health » Volume 18
Sex Differences in Long COVID Prevalence Over One year After the Acute Phase, and Related Risk Factors. The GINA-COVID Cohort Study
Authors Alvarez-Pedrerol M, Polo-Alonso S, Ramos R ![]() , Martí-Lluch R
, Martí-Lluch R ![]() , Pinsach-Abuin M
, Pinsach-Abuin M ![]() , Dégano IR
, Dégano IR ![]() , Elosua R, Subirana I, Hernáez Á, Selga E, Puigdecanet E, Pruneda-Paz J, Solà-Richarte C, Puigmulé M, Pérez A, Nogués X, Masclans JR
, Elosua R, Subirana I, Hernáez Á, Selga E, Puigdecanet E, Pruneda-Paz J, Solà-Richarte C, Puigmulé M, Pérez A, Nogués X, Masclans JR ![]() , Güerri-Fernández R, Cubero-Gallego H, Tizon-Marcos H, Vaquerizo B, Brugada R, Camps-Vilaró A
, Güerri-Fernández R, Cubero-Gallego H, Tizon-Marcos H, Vaquerizo B, Brugada R, Camps-Vilaró A ![]() , Marrugat J
, Marrugat J
Received 5 May 2025
Accepted for publication 31 January 2026
Published 16 April 2026 Volume 2026:18 538491
DOI https://doi.org/10.2147/IJWH.S538491
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Everett Magann
Mar Alvarez-Pedrerol,1 Sara Polo-Alonso,1 Rafel Ramos,2– 5 Ruth Martí-Lluch,3– 5 Mel·lina Pinsach-Abuin,6 Irene R Dégano,1,7– 9 Roberto Elosua,7,9,10 Isaac Subirana,9,10 Álvaro Hernáez,1,9,11 Elisabet Selga,7,8 Eulàlia Puigdecanet,7,8 Josefina Pruneda-Paz,1 Clàudia Solà-Richarte,1 Marta Puigmulé,6 Alexandra Pérez,6 Xavier Nogués,12– 15 Joan Ramon Masclans,16– 18 Roberto Güerri-Fernández,18– 20 Héctor Cubero-Gallego,21,22 Helena Tizon-Marcos,9,21,22 Beatriz Vaquerizo,9,15,21,22 Ramon Brugada,2,6,9,23 Anna Camps-Vilaró,1,7,9,* Jaume Marrugat1,9,*
1Registre Gironí del Cor (REGICOR) Study Group, Hospital del Mar Research Institute, Barcelona, Spain; 2Medical Science Department, School of Medicine, University of Girona, Girona, Spain; 3Vascular Health Research Group, Institut Universitari per a la Recerca en Atenció Primària Jordi Gol I Gurina, Girona, Spain; 4Research in Vascular Health Group, Girona Biomedical Research Institute, Girona, Spain; 5Network for Research on Chronicity, Primary Care, and Prevention and Health Promotion (RICAPPS), Girona, Spain; 6Cardiovascular Genetics Center, Institut d’Investigació Biomèdica de Girona Dr. Josep Trueta (IdIBGi), Salt, Spain; 7Faculty of Medicine, University of Vic-Central University of Catalonia, Vic, Spain; 8Institute for Research and Innovation in Life Sciences and Health in Central Catalonia (IRIS-CC), Vic, Spain; 9Centro de Investigación Biomédica en Red de Enfermedades Cardiovasculares (CIBERCV), Instituto de Salud Carlos III, Madrid, Spain; 10Cardiovascular Epidemiology and Genetics Group, Hospital del Mar Research Institute, Barcelona, Spain; 11Blanquerna School of Health Sciences, University Ramon Llull, Barcelona, Spain; 12Musculoskeletal Research Unit, Hospital del Mar Research Institute, Barcelona, Spain; 13Department of Internal Medicine, Hospital del Mar, Barcelona, Spain; 14Centro de Investigación Biomédica en Red de Fragilidad y Envejecimiento Saludable, Instituto de Salud Carlos III, Madrid, Spain; 15Department of Medicine, Universitat Autònoma de Barcelona (UAB), Bellaterra, Spain; 16Critical Illness Research Group (GREPAC), Hospital del Mar Research Institute, Barcelona, Spain; 17Department of Critical Care, Hospital del Mar, Barcelona, Spain; 18Medicine and Life Sciences Department, Universitat Pompeu Fabra (UPF), Barcelona, Spain; 19Centro de Investigación Biomédica en Red de Enfermedades Infecciosas, Instituto de Salud Carlos III, Madrid, Spain; 20Department of Infectious Diseases, Hospital del Mar Research Institute, Barcelona, Spain; 21Biomedical Research in Heart Diseases Group, Hospital del Mar Research Institute, Barcelona, Spain; 22Department of Cardiology, Hospital del Mar, Barcelona, Spain; 23Department of Cardiology, Hospital Josep Trueta, University of Girona, Girona, Spain
*These authors contributed equally to this work
Correspondence: Anna Camps-Vilaró, REGICOR Study Group, Hospital del Mar Research Institute, Barcelona, Spain, Email [email protected]
Background: This 1-year cohort study aimed to track long COVID prevalence, identify associated risk factors, and assess its association with hospitalization.
Methods: The GINA-COVID cohort study included 2698 COVID-19 patients from Spain, who reported persistent symptoms spontaneously mentioned in an open questionnaire one year after infection. We recorded symptom onset, duration, and recovery rates at 12 months. Hospitalization data were collected from the Catalan Health System. We performed descriptive statistics and logistic regression models stratified by sex to identify factors associated with long COVID, using multiple imputation for missing values and model selection via stepwise regression based on the Akaike Information Criterion.
Results: Significant sex differences appeared, with females showing a two-fold higher risk of developing long COVID compared to males (OR=1.95; 95% CI, 1.68– 2.29). Females reported higher prevalence and a greater number of persistent symptoms, with fatigue being the most common in both sexes (36% in females, 26% in males at 3 months). The recovery rate at 12 months was lower in females (23% vs. 34%, p< 0.001). Hypertension emerged as the most significant protective factor for long COVID in females (OR=0.64; 95% CI, 0.48– 0.84), whereas COVID-19 severity was the most influential risk factor in males (OR=2.34; 95% CI, 1.79– 3.08). Despite these differences, the trajectory of persistent symptoms over time was similar between the sexes. Importantly, long COVID did not increase hospital admissions.
Conclusion: Findings underscore the importance of sex-specific approaches in managing long COVID and suggest further investigation into hypertension’s protective role in females and disease severity’s impact in males.
Keywords: long COVID, persistent symptom, prevalence, risk factors, sex differences, SARS-CoV-2
Introduction
Persistent health effects after the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection, also known as post-coronavirus disease (COVID-19), long COVID, or as post-acute sequelae of SARS-CoV-2 infection, are a major concern due to its high prevalence and substantial clinical and public health impact.1,2 Almost 800 million cases of COVID-19 have been reported to the World Health Organization (WHO)3 and an alarming proportion of infected patients have experienced symptoms after recovering from COVID-19,4 with incidences above 10% up to 85%.5
This condition refers to a range of ongoing or new symptoms resulting from SARS-CoV-2 infection, which persist usually for at least three months and can last for years.6,7 More than 200 symptoms have been identified and these can affect multiple organ systems, including fatigue as the main symptom, and cognitive, respiratory and cardiovascular dysfunctions, among other health issues.8–11 Long COVID can occur in patients regardless of the severity of their initial infection and can significantly impact patients’ quality of life.7,12
Serious uncertainty remains in defining long COVID,5,7,9 identifying its risk factors, and understanding the underlying pathophysiological mechanisms involved in this condition.1,13 At present, there are no effective treatments or reliable diagnostic biomarkers.1,5,10,13 Moreover, the emergence of new variants continues to sustain high incidence and prevalence rates,14 making research on long COVID a high priority for public health. Importantly, emerging data suggest that biological sex plays a critical role in determining susceptibility to long COVID, with females generally showing higher prevalence and symptom persistence.1,14,15 However, few large-scale studies have systematically explored these sex-specific differences using a longitudinal approach. Understanding these disparities is essential to identify vulnerable populations, develop tailored prevention and management strategies, and inform health policy.
This research aims to explore the trends in the prevalence of long COVID, the pattern of symptoms, and the impact of risk factors one-year post SARS-CoV-2 infection, with a main focus on sex differences. By examining these patterns and factors, we aim to gain insights into the disease’s causes and improve prevention and personalized treatment strategies.
Methods
Study Design and Participants
We used a cohort design with 1-year follow-up of COVID-19 patients (GINACOVID cohort) who tested positive for SARS-CoV-2 [reverse transcription polymerase chain reaction (RT-PCR), rapid antigen, or IgG test results] between February 2020 and December 2021. Recruitment was conducted across both hospital and primary care settings (Barcelona’s Hospital del Mar, Girona’s Hospital Dr. Josep Trueta, Vic’s Hospital Consortium, and in primary health centers in Girona province), with approximately half of the participants recruited from each. This approach ensured representation of a broad spectrum of disease severity, although the inclusion of hospital-based participants may have increased the proportion of severe COVID-19 cases, while most primary care participants experienced non-severe infections. Participants were excluded if their SARS-CoV-2 positive tests were not confirmed, they were beyond the age range of 35 to 84 years (this group was the most affected by COVID-19 infection during the study period), they lacked clinical records available in the Catalan health care system (which offers universal coverage), they had been vaccinated against COVID-19 before diagnosis, or if they did not take part in the 1-year follow-up. A total of 2698 patients were finally considered for the analysis.
Data Collection
Data on age, sex, height, weight, and blood pressure were collected during hospitalization or at outpatient clinic at inclusion. Clinical data prior to the SARS-CoV-2 infection were collected from electronic medical records, including the history of smoking, hypertension, dyslipidemia, diabetes, coronary artery disease (CAD), stroke, thromboembolism, chronic obstructive pulmonary disease, immune disease, and neoplasia. Additionally, the most recent glycemia, lipid profile, and creatinine values before the COVID-19 diagnosis were collected from these electronic medical records. Ten-year CAD risk was estimated using the REGICOR risk function.16 Patients hospitalized and receiving oxygen therapy, those diagnosed with severe pneumonia, those needing mechanical ventilation, and those with blood oxygen saturation levels of ≤93% or a PaO2/FiO2 ratio of less than 300 mmHg, along with infiltrates in more than 50% of their lung fields, were classified as severe COVID-19 cases.17
Hospital Admissions
Data was linked to the Health Research and Innovation Data Analysis Programme (PADRIS), of the Health Department of the Government of Catalonia (the Catalan Health Surveillance System) to obtain information on hospital admissions. PADRIS provides health data to the scientific community to promote health research, innovation, and evaluation by allowing access to health data generated by Catalonia’s public healthcare system and collected at individual levels. Hospital admission was recorded as a binary variable (yes/no), and the number of admissions within 24 months following the COVID-19 diagnosis was used to evaluate the relationship between hospitalizations and long COVID. In patients with severe COVID-19 that required hospitalization, the admission corresponding to COVID-19 diagnosis was not considered.
Follow-Up and Long COVID Diagnosis
According to WHO definition, participants with presence of at least one persistent symptom related to COVID-19 infection for at least three months post-infection were considered long COVID cases.6 Persistent symptoms were those that had either begun or significantly worsened after the infection, without any other attributable cause.
One year after the COVID-19 acute phase, or after discharge in hospitalized patients, participants were asked about the presence of any symptom (present before COVID-19 diagnosis, during COVID-19 infection or after the infection). For symptoms present after the infection, participants were asked about the duration of them, categorized as less than 3 months, up to 3 months, 6 months, 9 months, or 12 months or longer.
All interviews were conducted by trained nurses and physicians following a standardized protocol. In each participating center, the same interviewer performed all follow-up assessments to ensure consistency in data collection and interpretation. All interviewers were trained by the same senior trainer to harmonize procedures across sites. The questionnaire was administered by these trained professionals, who recorded the reported symptom(s) using a standardized list of the 24 most common long COVID symptoms (>10% of prevalence) described in a meta-analysis by Lopez-Leon et al in 202118 (Figures S2 and S3). The selection of these symptoms was also supported by the WHO and other studies.8,19,20 These symptoms were classified as systemic (fatigue, fever, digestive disorder, hair loss, skin disorder, sweating, nausea, weight loss), respiratory or cardiovascular (cough, dyspnea, palpitations, chest pain, polypnea), muscle-skeletal symptoms (myalgia and arthralgia), and neuropsychiatric (memory loss, headache, other pain, dysgeusia, hyposmia, anosmia, hearing loss, anxiety and depression, and sleep disorder). The trained personnel recorded, in an open questionnaire, only the symptoms spontaneously mentioned by the participants and did not ask about each symptom individually from the questionnaire. The questionnaire also allowed for the inclusion of any additional symptoms not listed among the 24.
We also assessed the duration of long COVID (considering the longest duration of any persistent symptom experienced), the number of symptoms for each patient (for a quantitative long COVID phenotype), and recovery rate at 12 months. The recovery rate was the percentage of patients who had symptoms three months after their initial COVID-19 infection but no longer had symptoms after twelve months, and was calculated by dividing the number of patients who recovered by the total number of long COVID patients at three months. We also considered the existence of each symptom prior to, during, or after the COVID-19 infection. Then, for each symptom, we examined the percentage of individuals who already experienced the symptom during the COVID-19 infection compared to the percentage who developed the symptom after the infection (onset of the symptom).
Statistical Analysis
Prevalence at each point of time assessed during the first year of each persistent symptom related to COVID-19 infection and type of symptom was reported. Recovery rate at 12 months and onset (during or after COVID-19 illness) of each symptom was also described.
Demographic, anthropometric, cardiovascular risk factors and other characteristics were reported as frequencies for categorical variables and as means and standard deviation or median and quartiles for continuous normally and non-normally distributed variables, respectively. Means and medians were compared between males and females, and between individuals with and without long COVID stratified by sex, by Student’s t-test or Mann–Whitney tests, respectively, and frequencies by Chi-square test.
Characteristics were also reported according to long COVID recovery at 12 months and according to the number of symptoms and a p-values for trend was calculated.
The association of all characteristics with the diagnosis of long COVID was examined through a logistic regression model, where the impact of these factors was represented as odds ratios with 95% confidence intervals. For variable selection, both statistical and medical criteria were used. A backward stepwise selection process based on the Akaike Information Criterion (AIC) was used to determine the variables included in the final models. Given the observed interaction between sex and some characteristics, and long COVID diagnosis, a logistic regression model for each sex was fitted. Prior to conducting backward stepwise regression, multiple imputation of missing values was done with the Predictive Mean Matching method to ensure a complete dataset. Selected models were then applied to the original dataset.
Non-linear age patterns were assessed using natural splines with 4 degrees of freedom, and model fit was compared using AIC.
Statistical significance was assumed when p-values were <0.05. All analyses were performed using R Statistical Software (v4.3.2; R Core Team 2023).
Ethical Considerations
This study complied with the Declaration of Helsinki for medical research involving human subjects. All participants were fully informed and gave their informed consent (written or oral with the presence of witnesses) to participate in the study, which was approved by the Ethics Committees of Parc de Salut Mar (#2020/9297/I and #2020/9650/I), Hospital Universitari Dr. Josep Trueta (#2020/058), Foundation University Institute for Primary Health Care Research Jordi Gol i Gurina (IDIAPJGol) (#2021/084-PCV), and Fundació d’Osona per a la Recerca i l’Educació Sanitàries (FORES) (# 2020152/PR283). The study adhered to all international regulations for biomedical research.
Results
Participants’ Characteristics
The analysis included a total of 2698 participants (of whom 54% were females), who met the study criteria and completed the 1-year follow-up questionnaire. Among them, more than half of the participants (1531 participants, of whom 62% were females) reported persistent symptoms and were classified as long COVID cases (Figure 1).
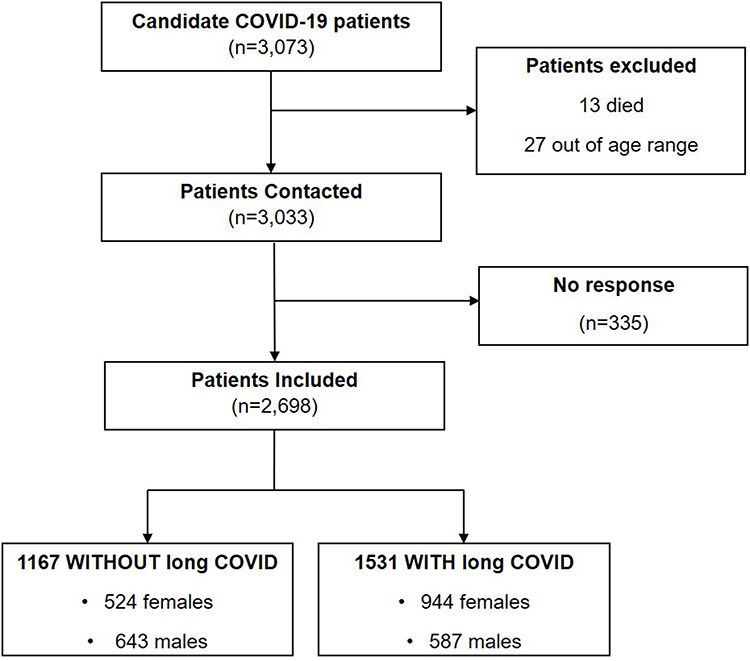 |
Figure 1 Flow diagram of patients included in the analysis. |
Baseline characteristics of the study population are summarized in Table 1 (columns 2–3). Females and males differed in almost all characteristics assessed.
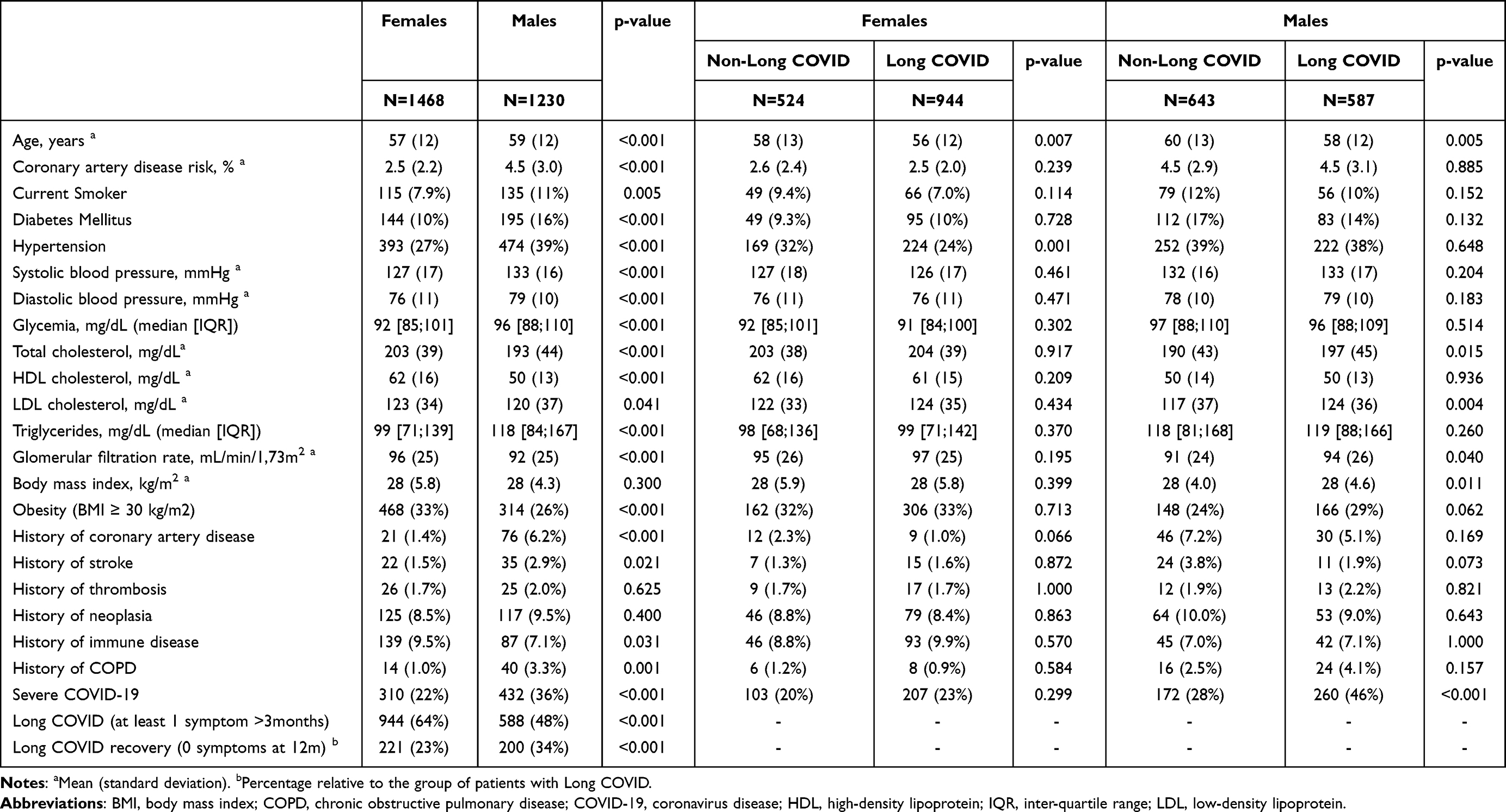 |
Table 1 Demographic Profile, Anthropometry, Cardiovascular Risk and Medical History in COVID-19 Positive Patients, Stratified by Sex and by Presence of Long COVID |
Long COVID Prevalences and Recovery Rates
A 57% (N=1532) of the study population reported persistent symptoms at 3 months and 41% (N=1107) at 1 year (recovery rate of 27.5%). Among females, 22% (N=310) had suffered a severe COVID-19 infection, and 64% (N=944) of them developed long COVID [36% (N=432) and 48% (N=588) among males, respectively]. At 12 months, a greater percentage of males had recovered compared to females, with recovery rates of 34% (N=200) for males versus 23% for females (N=221). (Tables 1, columns 2–3, and S1). Overall, females had a 2-fold higher risk of developing long COVID compared to males (OR=1.95; 95% CI, 1.68–2.29). Moreover, among those with long COVID, females had less probability to recover at 12 months (OR=0.59; 95% CI, 0.47–0.74).
Sex-Specific Determinants of Long COVID and of Long COVID Recovery
Subsequent analyses were conducted separately for each sex, and also after confirming the interaction of sex with some of the characteristics (hypertension and COVID-19 severity) in the association with long COVID in multivariate logistic regression models (p-value=0.019 and 0.002, respectively). In the sex-specific bivariate analysis (Table 1, columns 4–7), only a small number of characteristics continued showing a significant association with long COVID when compared to the analysis not differentiated by sex (Table S2). Females with long COVID were younger and less likely to have hypertension, while males were also younger and more likely to have had a severe COVID-19 illness in comparison with those without long COVID. Non-linear age patterns were examined, but no statistically significant results were identified. Males with long COVID also had higher levels of total and LDL cholesterol, and higher glomerular filtration rate.
Multivariable logistic regression models are shown in Figure 2. Among females (Figure 2a), baseline hypertension (OR=0.64; 95% CI, 0.48–0.84) was the only factor significantly associated to long COVID. In males (Figure 2b) COVID-19 severity (OR=2.34; 95% CI, 1.79–3.08) and baseline BMI (per 10 kg/m2 increase) (OR=1.36; 95% CI, 1.01–1.84) were risk factors for developing long COVID, while age (OR(+10yr)=0.89; 95% CI, 0.79–0.99) was also significant as a protective factor.
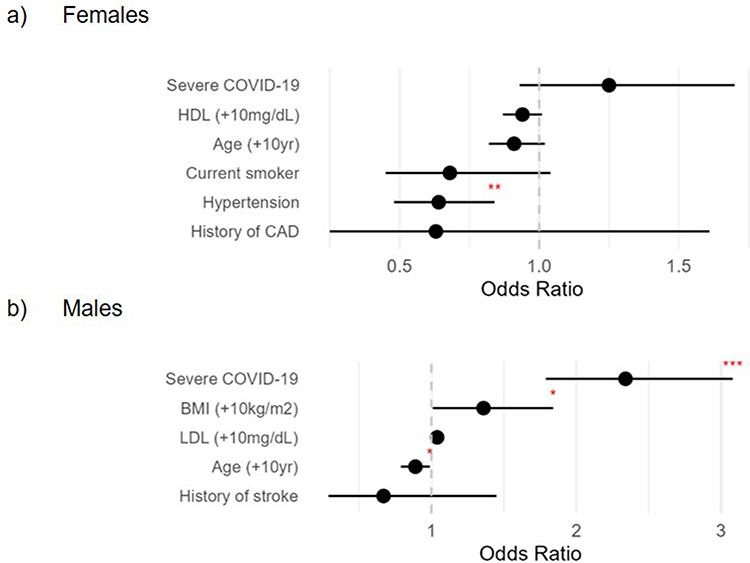 |
Figure 2 Forest plots of Odds Ratio for Long COVID, from multivariate logistic regression models, stratified by sex, females (a) and males (b). *p-value<0.05, **p-value<0.01, ***p-value<0.001. |
For both males and females with long COVID, those who recovered from the persistent symptoms, exhibited lower rates of severe COVID-19 (Table 2). No other factors were associated with recovery, except for history of thrombosis in females, which was only present in long COVID females who did not recover.
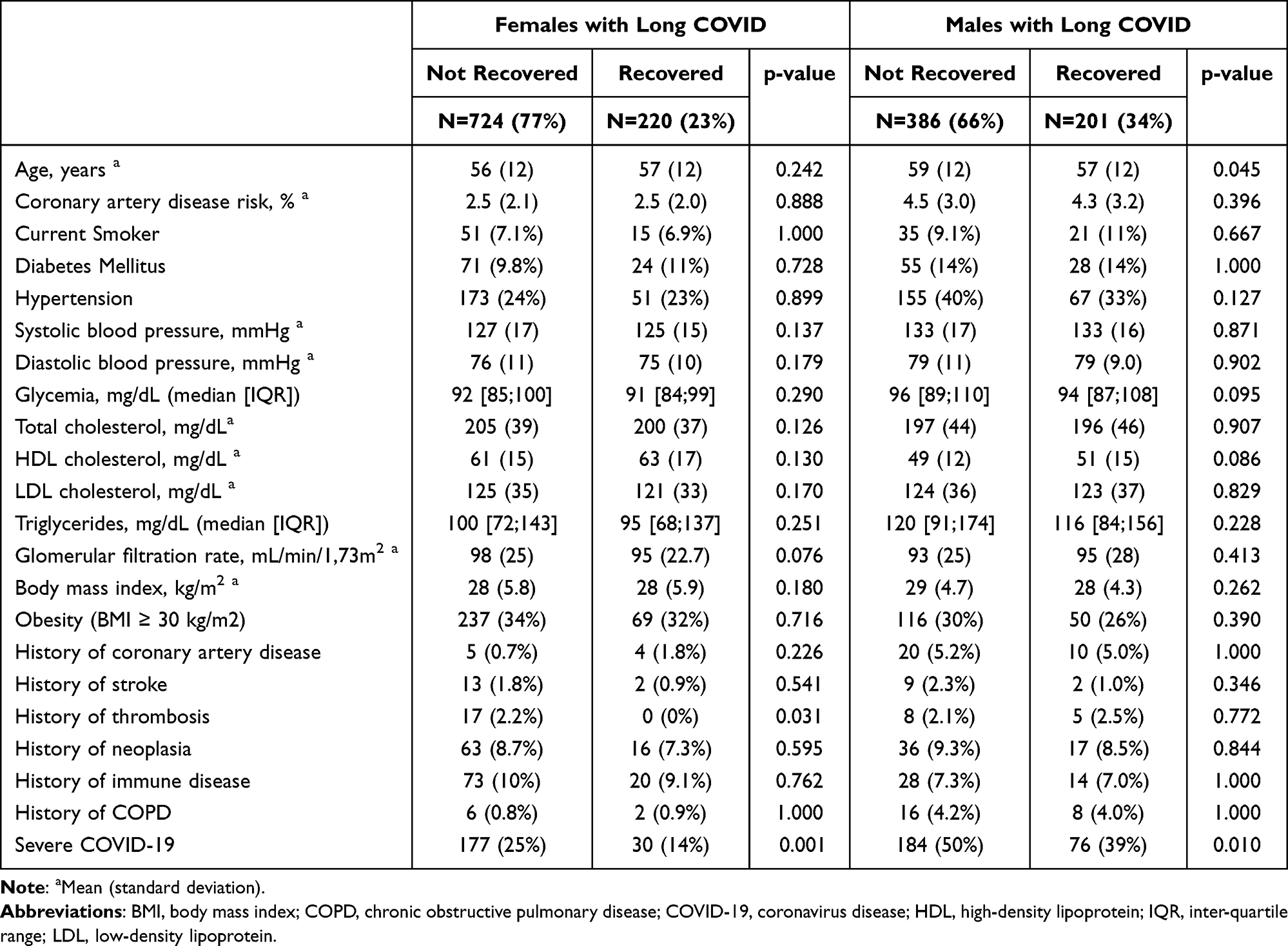 |
Table 2 Demographic Profile, Anthropometry and Cardiovascular Risk Prevalence in Patients with Long COVID According to Recovery from the Long COVID at 12 months, Stratified by Sex |
Females reported a greater number of persistent symptoms than males (Figure S1 and Table S3). Among females, when comparing the characteristics according to the number of persistent symptoms they experienced at three months, hypertension and age confirmed a significant trend, being females younger and with lower rates of hypertension as more symptoms reported. Additionally, a greater number of symptoms were also associated with COVID-19 severity and higher glomerular filtration rate. For males, the same characteristics that were identified as related in Table 1 also exhibited a significant pattern of association with an increasing number of persistent symptoms. Prevalence of history of COPD and obesity also increased with the number of symptoms reported (Table S3).
Hospital Admissions
There were no differences in hospital admissions (yes/no and number of admissions) within 24 months of COVID-19 diagnosis, between individuals with and without long COVID, regardless of sex. Among females with long COVID, 46% had at least one hospital admission compared to 44% of those without (similarly in males, 45% and 48%, respectively). Multivariate logistic regression models adjusted for COVID-19 severity, also showed no association between admissions (yes/no) and long COVID (OR=1.09 (95% CI, 0.88–1.37)) in females and OR=0.85 (95% CI, 0.67–1.09) in males.
Persistent Symptoms Prevalences and Patterns
The prevalence of the 24 identified persistent symptoms slightly declined over time (Figure 3 and Table S1), but many symptoms remained significant even after one year. Females showed a higher prevalence of all symptoms at all time intervals, though the time pattern was similar for both sexes, with fatigue being the most prevalent symptom. In females, the prevalence of fatigue was 36% at 3 months and 24% at 12 months (34% of recovery rate), and among the 36% of females who experienced persistent fatigue, 90% began experiencing it during their COVID-19 infection. A similar pattern was found with dyspnea, (the third most prevalent symptom in females and second in males), which was also mainly experienced during the infection and with a recovery rate of 30% in females. In contrast, memory loss, the second most common symptom in females (and third in males), had a recovery rate of just 18% at 12 months, and mainly appeared after the infection (Table S1). Hair loss, which was significantly more common in females than in males (15% versus 2.5% at 3 months), showed the highest recovery rate in both females and male (66% and 72%, respectively).
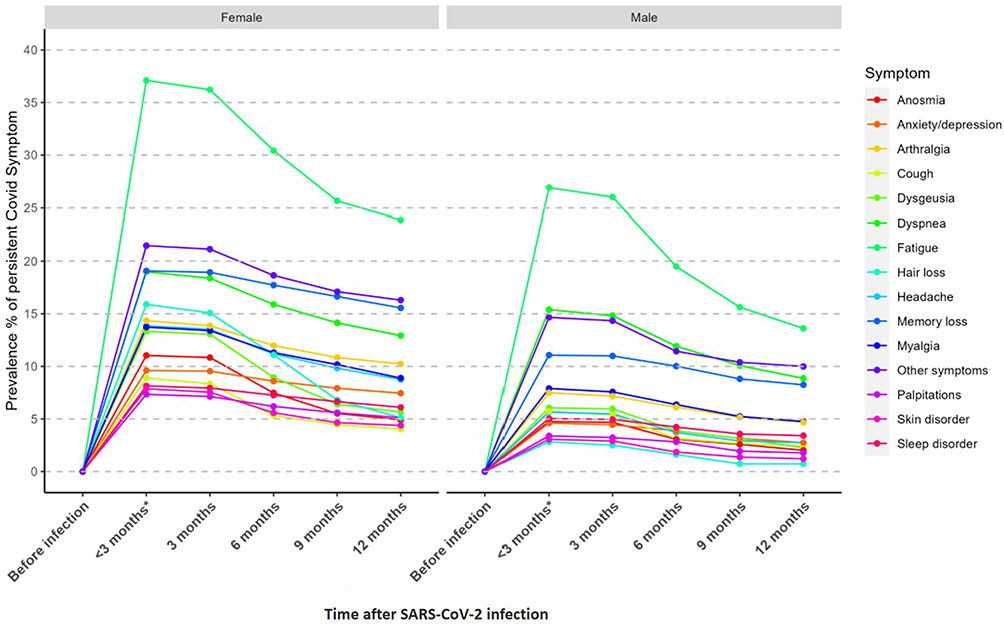 |
Figure 3 Persistent COVID-19 symptoms prevalence according to duration of symptoms in COVID-19 patients stratified by sex. Panels ordered by frequency. *Symptoms with a duration less than 3 months are not considered persistent symptoms. |
When categorized by symptom type (Figure 4 and Table S1), systemic symptoms, predominantly driven by fatigue, were the most prevalent. The prevalence of all symptom types decreased over time, with systemic symptoms showing the greatest decline. Neuro-psychiatric symptoms, however, experienced a slightly smaller reduction in female. Also, 60,2% (N=260) of males with severe COVID-19 develop long COVID, and 66,8% (N=207) of females, respectively.
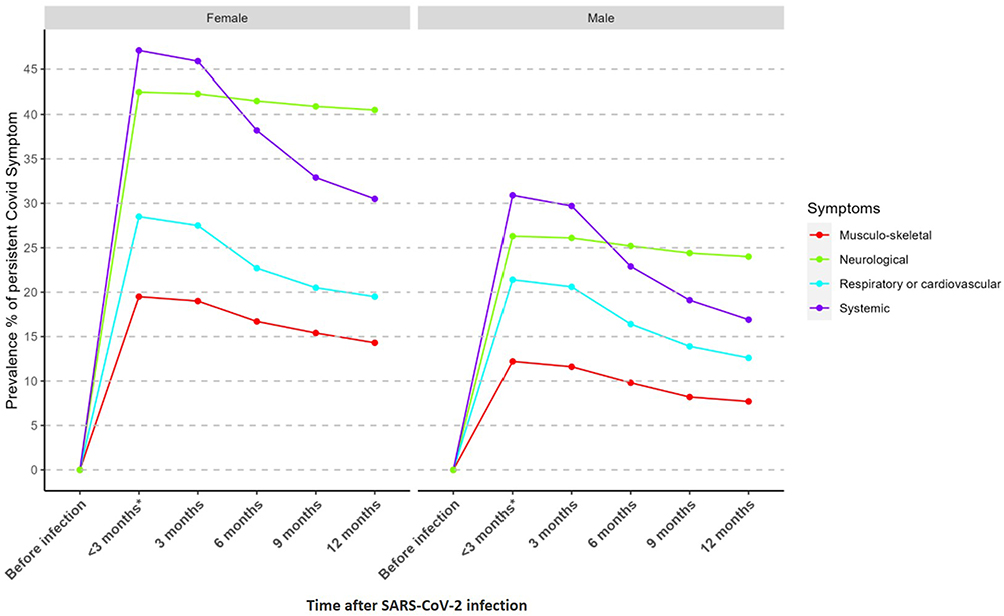 |
Figure 4 Persistent COVID-19 symptoms prevalence (grouped by type of symptoms and according to duration) in COVID-19 stratified by sex. *Symptoms with a duration less than 3 months are not considered persistent symptoms. |
Discussion
In this one-year cohort study, 57% of COVID-19 patients reported persistent symptoms at three months, and 41% continued to experience symptoms after one year. Females had twice the risk of developing long COVID compared to males (p-value <0.001) and were less likely to recover at 12 months (p-value <0.001). Risk factors associated to long COVID also differed between sexes highlighting the importance of sex-specific strategies for identifying and managing long COVID.
The incidence of long COVID in the present analysis was high, but similar to that reported in other studies.4,10,15,21 O’Mahoney et al reported persistent symptoms in approximately 40% of previously infected individuals.4 Likewise, Li et al described sex-specific immune and inflammatory responses that may underlie this disparity.10 Other European cohorts, such as Moreno-Pérez et al identified disease severity as a strong predictor;21 and Bai et al, also found a predominance of long COVID symptoms in females.15 Together, these studies support our findings and reinforce the need for sex-stratified analyses to better understand biological and clinical mechanisms associated with long COVID. However, our results may be biased by the inclusion of many severe COVID-19 patients due to the recruitment at hospitals.22 Additionally, vaccinated patients were not included in the study, and it is known that vaccination before infection significantly decreases the risk of long COVID.23
Sex was identified as the key factor influencing the progression to long COVID, with females being more susceptible to developing long COVID, and less likely to recover from it. Studies have consistently shown that females are more likely to experience long COVID,15,22,24–28 on the contrary, risk of severity and mortality of COVID-19 is higher in males.29–31 Although the contribution of sex as a biological variable in long COVID pathology is still unclear, research indicates that these differences may be linked to immune system functioning. Females generally have stronger and faster immune responses than males,32 which is effective for resolving the infection; however, if the response is prolonged this can lead to chronic or inflammatory conditions33 potentially contributing to long COVID, as observed in other infections with chronic sequelae (ie. those caused by Epstein-Barr or cytomegalovirus),31 or to the development of autoimmunity.34 Presence of autoantibodies has been related to long COVID, although its clinical relevance is unclear.35–37 Hormone interaction with immune system38 may play a role in this sex disparity. Testosterone has an immunosuppressive effect that can weaken the immune response to initial viral infections and contribute to more severe outcomes in acute COVID-19 but protects against autoimmunity.39 In contrast, estrogen usually enhances immune activity, which decreases the viral load and the presence of severe symptoms in early stages but can result in prolonged immune activation.40 Silva et al25 observed that higher testosterone levels were negatively associated with long COVID in either sex, supporting the hypothesis of an immunoendocrine dysregulation in sex-specific differences in the pathology of long COVID. However, other mechanisms different to sex hormones regulation may play a role in the long COVID sex bias, such as X-linked genetic mechanisms32,34 or lifestyle and differences in health conditions. It is important to consider that there might also be differences related to gender in the impact of these symptoms on the patient’s quality of life, and therefore in the perception and reporting of these symptoms.41
This study not only identifies being female as a significant risk factor for long COVID, but also emphasizes the importance of stratifying studies by sex to better comprehend the physiopathology of the disease and to identify the sex-specific risk factors and therapeutic targets, optimizing the management of the condition and providing targeted prevention and care to the most vulnerable and affected.24 Despite sex differences in the prevalence and patterns of long COVID have been reported in many studies, few studies have reported sex-stratified data.24,42 This issue can result in biased results, and limited sex-specific strategies for clinical management that may impact the outcomes.31
In this research, analyses were stratified by sex, and females showed a higher prevalence of all symptoms, especially systemic and neuropsychiatric symptoms. Females also reported higher number of symptoms than males and lower recovery rates. Risk factors associated to long COVID also differed by sex. The most notable findings were the identification of hypertension as a protective factor of developing long COVID in females, and the severity of acute COVID-19 infection as a risk factor, exclusively in males. However, severity was associated with lower recovery rate at 12 months and number of persistent symptoms at 3 months in both males and females. Hypertension has been consistently reported as a risk factor for poor prognosis in COVID-19,17 and it was associated with long COVID in few studies,27,28 thus, not consistent with our results. However, Ozawa et al43 also found that females with hypertension were less likely to develop long COVID than those without (OR: 0.51 (0.27–0.98)). These authors explored the use of drugs for hypertension and found that Calcium channel blocker administration was associated with reduced persistent symptoms such as alopecia, memory loss and sleeping disorders, which are prevalent symptoms in females from our study, and less prevalent in males. Regarding age, there are also conflicting results. Advanced age is known to be a significant risk factor for poor outcomes in COVID-19 infection,44 however, the effect of age on long COVID remains a subject of debate.5 Results from our study suggests that age is a protective factor of long COVID (yes/no and number of symptoms) in both males and females, similar to results found by Ziauddenn et al45 and Subramanian et al.46 However, other studies have identified age as a risk factor47,48 or no association.49 Discrepancies may be due to differences in participant selection criteria (age, hospitalization, vaccination) or to differences in control by other confounding factors observed in older people. These may also reflect differences in the waves of the pandemic, with high mortality in older people in the first waves.5 Furthermore, survival bias could also contribute to this apparent protective association, as older adults with greater frailty or comorbidities may have been less likely to participate or survive to the follow-up period, leading to an underrepresentation of the oldest individuals among long COVID cases. Thus, the role of age on long COVID requires further investigation.
Even though the notable differences in prevalences and risk factors between sexes, the ranking of symptom prevalence was similar in both sexes, being fatigue the most frequent symptom as consistently reported in other studies,5,8 followed by memory loss and dyspnea.8,45 Except for hair loss, described mainly in females, being the third most prevalent symptom. Trajectories over time (onset, duration and recovery of each symptom) were also similar in both sexes, especially when grouping symptoms according to their type, although these differed within symptoms type. Neuropsychiatric symptoms tend to persist longer (except for dysgeusia), notably in females, and some of these symptoms, such as memory loss or anxiety and depression, started with a delay compared to other symptoms. This pattern was very similar across both sexes, though it was more prevalent in females. Similar patterns have also been observed in other studies.8,10 A large study involving 236,379 COVID-19 patients found that one third of them experienced ongoing neurological or psychiatric symptoms six months after diagnosis, similar to the prevalences observed in the present study when males and females are considered together.50 In contrast, fatigue and dyspnea started just after the acute infection and had higher recovery rate. Additionally, a recent longitudinal study51 reported that female sex was a predictor of improvement in pulmonary function after COVID-19, suggesting that respiratory recovery does not necessarily parallel the persistence of self-reported symptoms. This apparent discrepancy may be explained by the higher frequency of non-respiratory symptoms such as fatigue, cognitive impairment, and sleep disturbances in females, which contribute substantially to the perception of ongoing illness. Many of these symptoms have plausible biological mechanisms that have been widely described.5,8 In particular, chronic fatigue, the most common symptom, has been linked to inflammatory and immune dysregulation involving cytokines such as IL-6 and IL-1β, shared genetic pathways, and microRNA profiles, all supporting the role of inflammation in long COVID.10 Additionally, dysregulation of endothelin-1 observed in patients with persistent fatigue suggests underlying endothelial dysfunction contributing to symptom persistence.10
The study also indicated that long COVID had no effect on hospitalization rates during the two years following the infection. However, despite no need of hospitalization because of persistent symptoms, other studies have described that many long COVID patients experience a significant decline in quality of life12 and functional impairment.5 This likely increases the healthcare demand through an increase of drugs prescription, or more frequent visits to Primary Care physicians, Specialists or emergency departments, depending on the affected systems of each patient.52 The healthcare system is generally insufficient given the complexity of long COVID and its high prevalence.5 Unfortunately, data on healthcare visits was not available for the analysis. From a public health perspective, these findings underscore the need for sex-sensitive approaches in long COVID surveillance, prevention, and care. Tailoring follow-up programs to recognize the higher symptom burden in females could improve diagnosis, management, and rehabilitation outcomes.
This study has several limitations that need to be acknowledged. Firstly, the symptom questionnaire was administered at the end of the first year after COVID-19 infection, which may have introduced recall bias and affected the reliability of symptom prevalence estimates. Participants were asked to recall and report any symptoms experienced since their acute infection, including their duration, but were not provided with a structured checklist to confirm each symptom individually. This approach likely led to underreporting rather than overreporting of symptoms. To minimize variability, all interviews were conducted by trained nurses and physicians following a standardized protocol. In each participating center, the same interviewer performed all follow-up assessments to ensure consistency, and all interviewers were trained by the same senior trainer to harmonize procedures across sites. Additionally, the most prevalent symptom reported was fatigue, but the intensity of fatigue and the impact on patients’ quality of life was not assessed, and fatigue is known to cause a significant impact on patient’s daily activities and functional impairment,12,53 specially in females.41 In addition, number of symptoms experience together, also higher in females, can have an impact in quality of life.41 Moreover, there is currently no clear and consistent definition of long COVID,5,9 mainly due to the high heterogeneity of this outcome, and no agreed and validated instruments specifically designed to measure it.5 In addition, definitions do not include severity and still diverge on duration.5 This makes it difficult to compare with other studies and perform unbiased systematic reviews.5,22 Lastly, socioeconomic variables such as education, income, occupation, household size, or care of family members were not assessed, and these could also be predictors of long COVID54 and probably differ between sexes.41,42 These limitations highlight the need for more rigorous and comprehensive studies to better understand and address the long-term effects of COVID-19.
Conclusions
Long COVID impacts females and males differently, with a higher 3-month and 1-year prevalence in females. In terms of key predictors, hypertension seems to be protective in females, whereas COVID-19 severity is a significant risk factor in males. Importantly, while long COVID is prevalent, it does not lead to severe health outcomes in terms of hospital admissions, though it may increase the use of other healthcare services. These findings highlight the importance of collecting and analyzing sex-stratified data to better understand risk profiles and improve patient care. Future longitudinal and interventional studies are warranted to clarify causal mechanisms, identify modifiable predictors, and develop targeted, gender-sensitive strategies for the prevention, detection, and management of long COVID.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Acknowledgments
We also thank all the GINA COVID participants and collaborators who participated in this study. A full roster of contributors can be found at: https://regicor.cat/cargencors_inv/.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was supported by CIBER - Consorcio Centro de Investigación Biomédica en Red- (CIBERCV CB16/11/00229 and CB16/11/00246), Instituto de Salud Carlos III, Ministerio de Ciencia e Innovación and Unión Europea – European Regional Development Fund, by a grant from the Government of Catalonia through the Agency for Management of University and Research Grants (2021SGR144), by the Crue-CSIC-Santander FONDO SUPERA COVID-19, and by Fundació La Marató de TV3 (202119-30).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Davis HE, McCorkell L, Vogel JM, Topol EJ. Long COVID: major findings, mechanisms and recommendations. Nat Rev Microbiol. 2023;21(3):133–14. doi:10.1038/S41579-022-00846-2
2. Cogliandro V, Bonfanti P. Long COVID: lights and shadows on the clinical characterization of this emerging pathology. New Microbiol. 2024;47(1):15–27.
3. World Health Organization. WHO Coronavirus (COVID-19) Dashboard. Available from: https://covid19.who.int/.
4. O’Mahoney LL, Routen A, Gillies C, et al. The prevalence and long-term health effects of Long Covid among hospitalised and non-hospitalised populations: a systematic review and meta-analysis. EClinicalMedicine. 2022;55. doi:10.1016/J.ECLINM.2022.101762
5. Greenhalgh T, Sivan M, Perlowski A, Nikolich JŽ. Long COVID: a clinical update. Lancet. 2024;404(10453):707–724. doi:10.1016/S0140-6736(24)01136-X
6. Soriano JB, Murthy S, Marshall JC, Relan P, Diaz JV. A clinical case definition of post-COVID-19 condition by a Delphi consensus. Lancet Infect Dis. 2022;22(4):e102–e107. doi:10.1016/S1473-3099(21)00703-9
7. Ely EW, Brown LM, Fineberg HV. National Academies of Sciences, Engineering, and Medicine Committee on Examining the Working Definition for Long Covid. Long Covid Defined. N Engl J Med. 2024;391(18):1746–1753. doi:10.1056/NEJMsb2408466
8. Davis HE, Assaf GS, McCorkell L, et al. Characterizing long COVID in an international cohort: 7 months of symptoms and their impact. EClinicalMedicine. 2021;38:101019. doi:10.1016/J.ECLINM.2021.101019
9. Thaweethai T, Jolley SE, Karlson EW, et al. Development of a Definition of Postacute Sequelae of SARS-CoV-2 Infection. JAMA. 2023;329(22):1934–1946. doi:10.1001/JAMA.2023.8823
10. Li J, Zhou Y, Ma J, et al. The long-term health outcomes, pathophysiological mechanisms and multidisciplinary management of long COVID. Signal Transduct Target Ther. 2023;8(1). doi:10.1038/S41392-023-01640-Z
11. Fairbank R. Long COVID still has no cure - so these patients are turning to research. Nature. 2024;628(8006):26–28. doi:10.1038/D41586-024-00901-3
12. Carlile O, Briggs A, Henderson AD, et al. Impact of long COVID on health-related quality-of-life: an OpenSAFELY population cohort study using patient-reported outcome measures (OpenPROMPT). Lancet Region Health. 2024;40:100908. doi:10.1016/j.lanepe.2024.100908
13. Long COVID basics. CDC. Avaiable from: https://www.cdc.gov/coronavirus/2019-ncov/long-term-effects/index.html.
14. Mandel H, Yoo Y, Allen A, et al. Long COVID incidence in adults and children between 2020 and 2023: a real-world data study from the RECOVER Initiative. Res Sq. 2024. doi:10.21203/RS.3.RS-4124710/V1
15. Bai F, Tomasoni D, Falcinella C, et al. Female gender is associated with long COVID syndrome: a prospective cohort study. Clin Microbiol Infect. 2022;28(4):611.e9–611.e16. doi:10.1016/J.CMI.2021.11.002
16. Marrugat J, Solanas P, D’Agostino R, et al. [Coronary risk estimation in Spain using a calibrated Framingham function]. Rev Esp Cardiol. 2003;56(3):253–261. doi:10.1016/S0300-8932(03)76861-4
17. Figliozzi S, Masci PG, Ahmadi N, et al. Predictors of adverse prognosis in COVID-19: a systematic review and meta-analysis. Eur J Clin Invest. 2020;50(10). doi:10.1111/ECI.13362
18. Lopez-Leon S, Wegman-Ostrosky T, Perelman C, et al. More than 50 long-term effects of COVID-19: a systematic review and meta-analysis. Sci Rep. 2021;11(1):16144. doi:10.1038/S41598-021-95565-8
19. Manifestacions persistents de la COVID-19. Guia de pràctica clínica CAMFIC. Available from: http://gestor.camfic.cat/uploads/ITEM_13380_EBLOG_4143.pdf.
20. Huang C, Huang L, Wang Y, et al. 6-month consequences of COVID-19 in patients discharged from hospital: a cohort study. Lancet. 2021;397(10270):220–232. doi:10.1016/S0140-6736(20)32656-8
21. Moreno-Pérez O, Merino E, Leon-Ramirez JM, et al. Post-acute COVID-19 syndrome. Incidence and risk factors: a Mediterranean cohort study. J Infect. 2021;82(3):378–383. doi:10.1016/J.JINF.2021.01.004
22. Hua MJ, Butera G, Akinyemi O, Porterfield D, Santos PAAP. Biases and limitations in observational studies of Long COVID prevalence and risk factors: a rapid systematic umbrella review. PLoS One. 2024;19(5):e0302408. doi:10.1371/JOURNAL.PONE.0302408
23. Watanabe A, Iwagami M, Yasuhara J, Takagi H, Kuno T. Protective effect of COVID-19 vaccination against long COVID syndrome: a systematic review and meta-analysis. Vaccine. 2023;41(11):1783–1790. doi:10.1016/J.VACCINE.2023.02.008
24. Sylvester SV, Rusu R, Chan B, Bellows M, O’Keefe C, Nicholson S. Sex differences in sequelae from COVID-19 infection and in long COVID syndrome: a review. Curr Med Res Opin. 2022;38(8):1391–1399. doi:10.1080/03007995.2022.2081454
25. Silva J, Takahashi T, Wood J, et al. Sex differences in symptomatology and immune profiles of Long COVID. medRxiv. 2024. doi:10.1101/2024.02.29.24303568
26. Mateu L, Tebe C, Loste C, et al. Determinants of the onset and prognosis of the post-COVID-19 condition: a 2-year prospective observational cohort study. Lancet Region Health. 2023;33:100724. doi:10.1016/J.LANEPE.2023.100724
27. Elias TP, Gebreamlak TW, Gebremeskel TT, et al. Determinants of post-acute COVID-19 syndrome among hospitalized severe COVID-19 patients: a 2-year follow-up study. PLoS One. 2024;19(5):e0298409. doi:10.1371/JOURNAL.PONE.0298409
28. Tleyjeh IM, Saddik B, AlSwaidan N, et al. Prevalence and predictors of Post-Acute COVID-19 Syndrome (PACS) after hospital discharge: a cohort study with 4 months median follow-up. PLoS One. 2021;16(12):e0260568. doi:10.1371/JOURNAL.PONE.0260568
29. Alwani M, Yassin A, Al-Zoubi RM, et al. Sex-based differences in severity and mortality in COVID-19. Rev Med Virol. 2021;31(6). doi:10.1002/RMV.2223
30. G P, M T, J N, R T, R A, S N. Sex differences in the mortality rate for coronavirus disease 2019 compared to other causes of death. medRxiv. 2021. doi:10.1101/2021.02.23.21252314
31. Bechmann N, Barthel A, Schedl A, et al. Sexual dimorphism in COVID-19: potential clinical and public health implications. Lancet Diabetes Endocrinol. 2022;10(3):221–230. doi:10.1016/S2213-8587(21)00346-6
32. Libert C, Dejager L, Pinheiro I. The X chromosome in immune functions: when a chromosome makes the difference. Nat Rev Immunol. 2010;10(8):594–604. doi:10.1038/NRI2815
33. Torcia MG, Nencioni L, Clemente AM, et al. Sex differences in the response to viral infections: TLR8 and TLR9 ligand stimulation induce higher IL10 production in males. PLoS One. 2012;7(6):e39853. doi:10.1371/JOURNAL.PONE.0039853
34. Miquel CH, Faz-Lopez B, Guéry JC. Influence of X chromosome in sex-biased autoimmune diseases. J Autoimmun. 2023;137:102992. doi:10.1016/J.JAUT.2023.102992
35. Wong C. What causes long COVID? Case builds for rogue antibodies. Nature. 2024;630(8018):798–799. doi:10.1038/D41586-024-02010-7
36. L’huillier AG, Pagano S, Baggio S, et al. Autoantibodies against apolipoprotein A-1 after COVID-19 predict symptoms persistence. Eur J Clin Invest. 2022;52(10):13818. doi:10.1111/eci.13818
37. Notarte KI, Hudson T, Culasino Carandang D, et al. Autoantibodies in COVID-19 survivors with post-COVID symptoms: a systematic review. Front Immunol. 2024;15. doi:10.3389/fimmu.2024.1428645
38. Klein SL, Flanagan KL. Sex differences in immune responses. Nat Rev Immunol. 2016;16(10):626–638. doi:10.1038/NRI.2016.90
39. Wilhelmson AS, Lantero Rodriguez M, Stubelius A, et al. Testosterone is an endogenous regulator of BAFF and splenic B cell number. Nat Commun. 2018;9(1). doi:10.1038/S41467-018-04408-0
40. Roved J, Westerdahl H, Hasselquist D. Sex differences in immune responses: hormonal effects, antagonistic selection, and evolutionary consequences. Horm Behav. 2017;88:95–105. doi:10.1016/J.YHBEH.2016.11.017
41. Marcilla-Toribio I, Moratalla-Cebrián ML, Notario-Pacheco B, Escudero-Lopez MA, Morales-Cuenca N, Martinez-Andres M. Gender differences in symptomatology, socio-demographic information and quality of life in Spanish population with long COVID condition: a cross-sectional study. Front Public Health. 2024;12. doi:10.3389/FPUBH.2024.1355973
42. Gebhard CE, Sütsch C, Bengs S, et al. Sex- and Gender-specific Risk Factors of Post-COVID-19 Syndrome: a Population-based Cohort Study in Switzerland. medRxiv. 2021:21259757. doi:10.1101/2021.06.30.21259757
43. Ozawa T, Kimura R, Terai H, et al. Calcium channel blockers may reduce the development of long COVID in females. Hypertens Res. 2024;47(4):934–943. doi:10.1038/S41440-023-01501-W
44. Bonanad C, García-Blas S, Tarazona-Santabalbina F, et al. The effect of age on mortality in patients with COVID-19: a meta-analysis with 611,583 subjects. J Am Med Dir Assoc. 2020;21(7):915–918. doi:10.1016/J.JAMDA.2020.05.045
45. Ziauddeen N, Gurdasani D, O’Hara ME, et al. Characteristics and impact of Long Covid: findings from an online survey. PLoS One. 2022;17(3):e0264331. doi:10.1371/JOURNAL.PONE.0264331
46. Subramanian A, Nirantharakumar K, Hughes S, et al. Symptoms and risk factors for long COVID in non-hospitalized adults. Nat Med. 2022;28(8):1706–1714. doi:10.1038/S41591-022-01909-W
47. Sudre CH, Murray B, Varsavsky T, et al. Attributes and predictors of long COVID. Nat Med. 2021;27(4):626–631. doi:10.1038/S41591-021-01292-Y
48. Badenes Bonet D, Caguana Vélez OA, Duran Jordà X, et al. Treatment of COVID-19 during the acute phase in hospitalized patients decreases post-acute sequelae of COVID-19. J Clin Med. 2023;12(12):4158. doi:10.3390/JCM12124158
49. Notarte KI, de Oliveira MHS, Peligro PJ, et al. Age, sex and previous comorbidities as risk factors not associated with SARS-CoV-2 infection for long COVID-19: a systematic review and meta-analysis. J Clin Med. 2022;11(24):7314. doi:10.3390/JCM11247314
50. Taquet M, Geddes JR, Husain M, Luciano S, Harrison PJ. 6-month neurological and psychiatric outcomes in 236 379 survivors of COVID-19: a retrospective cohort study using electronic health records. Lancet Psychiatry. 2021;8(5):416–427. doi:10.1016/S2215-0366(21)00084-5
51. Freund O, Breslavsky A, Givoli-Vilensky R, et al. Assessment of a close respiratory follow-up schedule at 3 and 6 months after acute COVID-19 and its related investigations. Respir Med. 2023;217:107367. doi:10.1016/j.rmed.2023.107367
52. Valdivieso-Martínez B, Sauri I, Philibert J, et al. Clinical medicine impact of long-COVID on health care burden: a case control study. J Clin Med. 2023;12(18):5768. doi:10.3390/jcm12185768
53. Walker S, Goodfellow H, Pookarnjanamorakot P, et al. Impact of fatigue as the primary determinant of functional limitations among patients with post-COVID-19 syndrome: a cross-sectional observational study. BMJ Open. 2023;13(6):e069217. doi:10.1136/BMJOPEN-2022-069217
54. Shabnam S, Razieh C, Dambha-Miller H, et al. Socioeconomic inequalities of Long COVID: a retrospective population-based cohort study in the United Kingdom. J R Soc Med. 2023;116(8):263. doi:10.1177/01410768231168377
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Psychological Impact of Quarantine During the COVID-19 Pandemic on Quarantined Non-Healthcare Workers, Quarantined Healthcare Workers, and Medical Staff at the Quarantine Facility in Saudi Arabia
Alfaifi A, Darraj A, El-Setouhy M
Psychology Research and Behavior Management 2022, 15:1259-1270
Published Date: 17 May 2022
Sex-Specific Risk Factors Associated with Helicobacter pylori Infection Among Individuals Undergoing Health Examinations in China
Wu Y, Zeng H, Zhang M, Li C, Tang Y, Li X, Yuan S, Wei Q, Wang J, Ning X, Zhang X
International Journal of General Medicine 2022, 15:5861-5868
Published Date: 29 June 2022
Anaemia, Morphological Classification and Its Associated Risk Factors Among Lactating Mothers at Mbarara City Council Health Centre IV, Southwestern Uganda
Clinton O, Micheal K, Namyalo Angella K, Mary M, Mike M, Muwanguzi E, Okongo B, Wagubi R
Journal of Blood Medicine 2022, 13:473-481
Published Date: 2 September 2022
Chronic Obstructive Pulmonary Disease Prevalence and Associated Risk Factors in Adults Aged 40 Years and Older in Southeast China: A Cross-Sectional Study During 2019–2020
Chen J, Yin Y, Zhang Y, Lin X, Chen T, Yang Z, Wang D, Zhong W
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2317-2328
Published Date: 17 September 2022
Prevalence, Management, and Risk Factors of Asthma Among School-Age Children in Yogyakarta, Indonesia
Triasih R, Setyowireni D, Nurani N, Setyati A
Journal of Asthma and Allergy 2023, 16:23-32
Published Date: 5 January 2023