Back to Journals » Journal of Blood Medicine » Volume 13
Anaemia, Morphological Classification and Its Associated Risk Factors Among Lactating Mothers at Mbarara City Council Health Centre IV, Southwestern Uganda
Authors Clinton O ![]() , Micheal K, Namyalo Angella K, Mary M, Mike M, Muwanguzi E, Okongo B
, Micheal K, Namyalo Angella K, Mary M, Mike M, Muwanguzi E, Okongo B ![]() , Wagubi R
, Wagubi R ![]()
Received 31 March 2022
Accepted for publication 23 August 2022
Published 2 September 2022 Volume 2022:13 Pages 473—481
DOI https://doi.org/10.2147/JBM.S367453
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Martin H Bluth
Olong Clinton,1 Kanyesigye Micheal,1 Kimuli Namyalo Angella,1 Muhawenimana Mary,1 Mugume Mike,1 Enoch Muwanguzi,1 Benson Okongo,1 Robert Wagubi2
1Department of Medical Laboratory Science, Mbarara University of Science and Technology, Mbarara City, Uganda; 2Department of Clinical Laboratories, Mbarara Regional Referral Hospital, Mbarara City, Uganda
Correspondence: Benson Okongo, Department of Medical Laboratory Science, Faculty of Medicine, Mbarara University of Science and Technology, P.O. BOX 1410, Mbarara City, Uganda, Tel +256 778557867/759 101508, Fax +256 485 20782, Email [email protected]
Purpose: The objectives of this study were to determine the prevalence of anaemia, morphological classification and its associated risk factors among the lactating mothers accessing postnatal care at Mbarara City Health Centre IV, Southwestern Uganda.
Patients and Methods: A cross-sectional study was conducted at Mbarara City Health Centre IV among 264 participants. A structured questionnaire was used to capture characteristics of study participants. 4 mL of venous blood was collected from each participant for complete blood count (CBC) and peripheral blood smear (PBS). CBC was done using hematology analyzer (BC-2800 Mindray Hematology Analyzer) while PBS were taken for participants with hemoglobin (Hb) < 12.0g/dl and stained using Giemsa–Maygrunwald stain. Bivariate analysis and multivariate logistic regression were used to determine the associations between factors and anaemia. A p-value of < 0.05 was considered significant.
Results: The overall prevalence of anaemia was 65 (24.6%), with mean hemoglobin (Hb) concentration of 12.5g/dL. Out of the anaemic participants (24.6%), morphological classifications of anaemia were as follows: normocytic normochromic 27 (41.5%), microcytic hypochromic 20 (30.8%), normocytic hypochromic 16 (24.1%) and macrocytic normochromic 2 (3.1%). According to the severity of anaemia, majority had mild anaemia 52 (80%), moderate anaemia was 11 (16.9%), and severe anaemia was 2 (3.1%). The following risk factors were significantly associated with anaemia: duration of lactation (between 5 to 8 months, p-value 0.017, 95% CI (0.12– 0.82) and alcohol consumption (p-value 0.032, 95% CI (1.12– 12.16). The rest of the variables had no association with anaemia.
Conclusion: The prevalence of anaemia among lactating mothers is high and it is a moderate public health problem as defined by WHO. Nutrition promotion, and health education, may be the ideal way to reduce the prevalence of anaemia in this region.
Keywords: anaemia, prevalence, risk factors, lactating mothers
Introduction
Anaemia is a condition in which blood hemoglobin concentration is below normal for age and sex with inadequate oxygen carrying capacity of red blood cells for normal physiological processes.1 World Health Organization (WHO) defines anaemia in non-pregnant women as blood hemoglobin concentration <120 g/L and severe anaemia as blood hemoglobin concentration <70g/L.2
Anaemia is a global public health burden affecting about 1.74 billion people,3 with 29.6% of non-pregnant women anaemic worldwide.4 Anaemia has impacts on health as well as social and economic development of both rich and poor countries. Regional prevalence of anaemia among non-pregnant women ranges from 16% in high income countries to 48% in central and western Africa.5
Several studies have reported prevalence of anaemia among lactating mothers as: 32.7% in China,6 60.3% in Myanmar in 20147 and 73.8% in 2016,8 62.9% in India9 and 8–24% in Denmark.10
Lactating mothers are vulnerable to anaemia because of iron depletion during lactation and blood loss during delivery.8,11 Breast milk iron concentration has been known to be maintained at the expense of the mother’s iron stores and mothers who had anaemia during pregnancy have higher chances to develop anaemia during lactation.1 East African region has reported 22%12 and 25%13 prevalence of anaemia among postnatal mothers in Tanzania and Kenya, respectively, and the Horn of Africa is equally affected by anaemia in lactating mothers. Studies have estimated prevalence of anaemia among lactating mothers in Ethiopia to have increased from 21.8%14 and 22.1%11 to 28.3%.15
Several factors have been found to predict anaemia in lactating mothers in low income countries and these include: iron deficiency, vitamin A, C, B12 and folate deficiency, parasitic infection, multi-gravidity, antepartum anaemia, low income level, young lactating age and infectious diseases.1,6,7
In Uganda the prevalence of anaemia among breastfeeding mothers is 34%.16 The regional variation of anaemia among non-pregnant women ranges from 16.9% in Kigezi to 47.1% in Acholi.17 There is scarcity of data on the prevalence of anaemia among lactating mothers in Mbarara district and in Uganda in general. The aim of this study was therefore to determine the prevalence of anaemia and its associated risk factors among lactating mothers at Mbarara City Health Centre IV (MC HC IV), Southwestern Uganda.
Materials and Methods
Study Design and Site
This was a cross-sectional study carried out at Mbarara City Health Centre IV (MC-HC IV) from October to December 2021, located in Mbarara City in Southwestern Uganda. MCHC-IV is a public health facility that serves the population of Mbarara city, including referrals from other low level health centres within the city. It offers services like: immunization, family planning, ante/postnatal care, prevention of mother-to-child transmission (PMTCT), HIV/AIDS clinic, general outpatient (OPD), minor surgeries for male circumcision and laboratory services.
Sample Size Calculation
The sample size for this study was estimated using the formula for a single population proportion, with the following assumptions: anaemia prevalence of 22% in lactating mothers,12 at 95% confidence level, and 5% marginal error. Using the formula for sample size calculation for the proportion.
n= Z2P(1-P)/d2
Where: n=the desired sample size
Z=critical values of normal distribution at 95%, which corresponds to 1.96
P=the proportion of the target population estimated to have anaemia
d=estimated margin of error 5%
n=264
Sample size was then adjusted for 10% non-response rate and the minimum sample size calculated was 290 lactating mothers. There was however low turn up to postnatal clinic so this was not attained but considering the fact that ratio of each variables under study to sample size was between 5 to 10, this sample size was adequate for multivariate level of analysis.
Sampling Procedure
Two hundred and sixty four (n=264) lactating mothers were randomly selected and subjected to structured questionnaires to obtain information on sociodemographic characteristics, dietary intake, mid upper arm circumference (MUAC), iron supplementation, number of antenatal and postnatal visits, use of treated mosquito nets, tea consumption, alcohol intake, deworming status, source of drinking water, and history of post-partum hemorrhage.
Laboratory Procedure
About 4mL of venous blood was collected aseptically into an EDTA vacutainer. Complete blood count was performed using (BC 2800 Mindray Hematology Analyzer), peripheral thin blood smears were made, fixed with absolute methanol and stained using 10% Giemsa–Maygrunwald stain for the morphological classification of anaemia.
Ethical Consideration
This study was approved by the Faculty Research Committee (FRC) of Mbarara University of Science and Technology and Mbarara City health officer (approval number MUST/MLS/023). Written Informed consent was obtained from the study participants and the study protocol conformed to the ethical guidelines of the 1975 Declaration of Helsinki (1964). Privacy and confidentiality was followed all through the study process and those with anaemia were referred to physicians for management.
Results
Demographic Characteristics of the Study Participants
The mean age was 26 years, 95% CI (25.4–26.7). The participants’ ages ranged from 18 years to 45 years. Majority of the lactating mothers were aged between 20 to 29 years, 192 (72.7%), and those within the first 4 months of lactation were 169 (64%), mothers who had attained secondary education 126 (47.7%), married 252 (95.4%), and employed 155 (58.7%). Those with 1–2 parities, 195 (73.9%), and those with ≥4 antenatal visits during pregnancy were 214 (81.1%), as shown in Table 1.
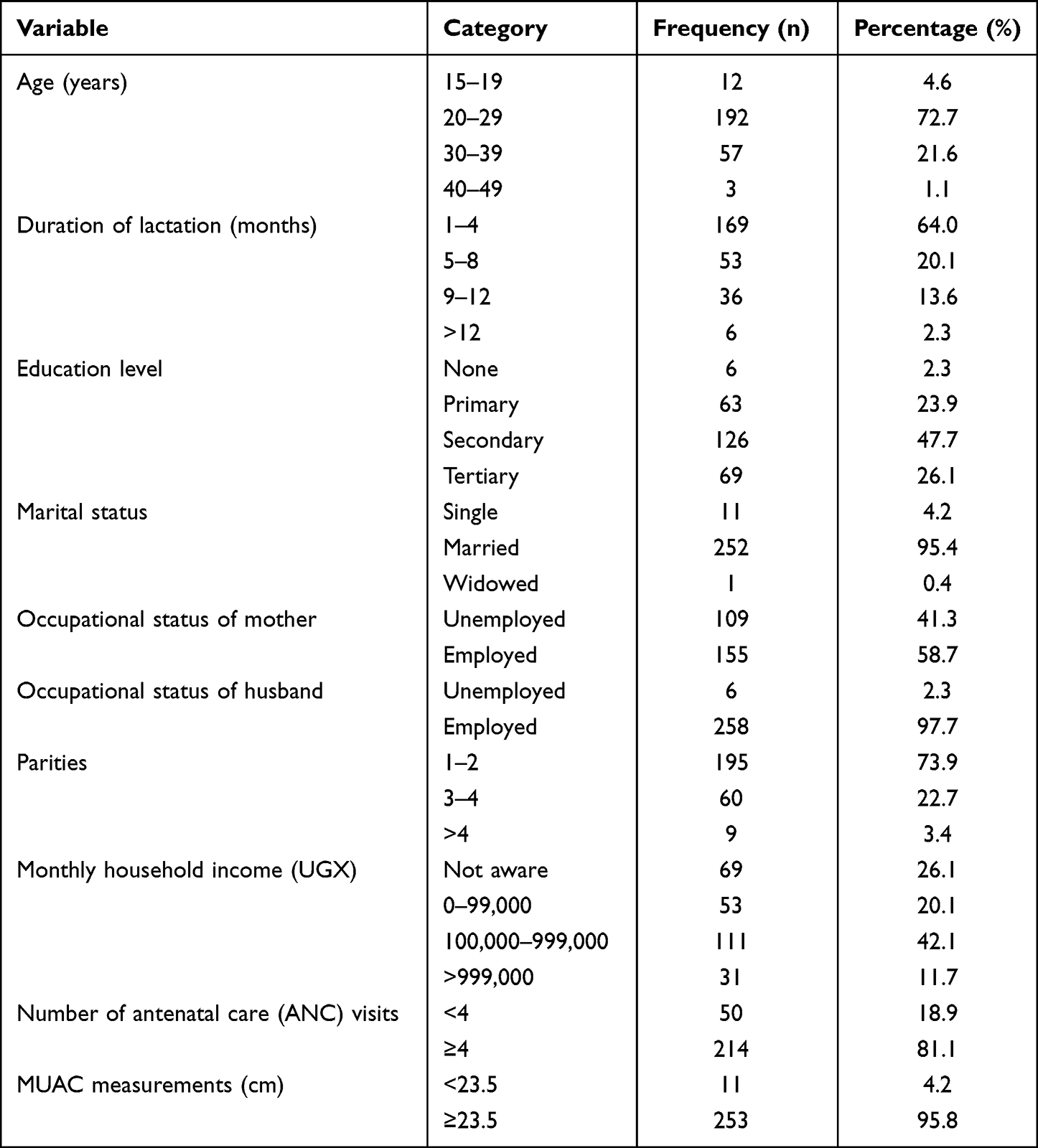 |
Table 1 Demographic Characteristics of Study Participants |
Prevalence of Anaemia
The overall prevalence of anaemia among lactating mothers was 65 (24.6%), as shown in Figure 1. According to WHO’s definition of severity of anaemia, anaemia is classified as mild anaemia when the Hb is (10.0–11.9g/dL), moderate (7.0–9.9g/dL) and severe (<7.0g/dL). In this study, 2 (0.7%) had severe anaemia, 11 (4.2%) had moderate anaemia and 52 (19.7%) had mild anaemia.
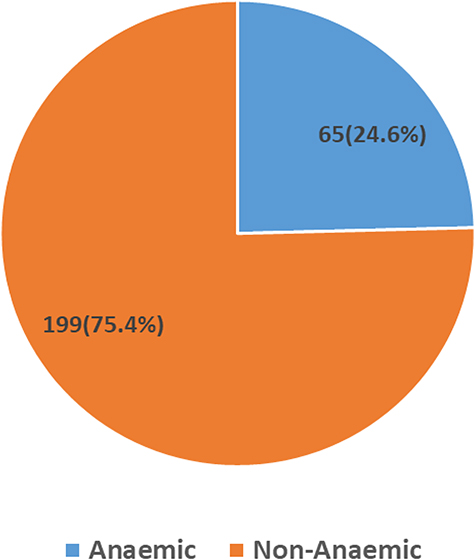 |
Figure 1 Pie chart showing prevalence of anaemia among lactating mothers at Mbarara City Health Centre IV. |
Morphological Classification of Anaemia
Based on the peripheral blood reports, majority 27 (41.5%), of the participants had normocytic normochromic anaemia, 20 (30.8%) had microcytic hypochromic, 16 (24.1%) had normocytic hypochromic and 2 (3.1%) had macrocytic normochromic anaemia, as shown in Figure 2.
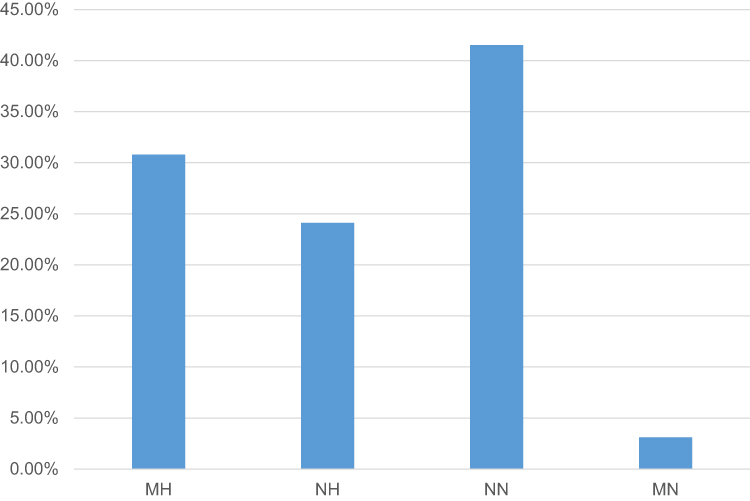 |
Figure 2 Morphological classification of anaemia among lactating mothers at Mbarara City Health Centre IV. Abbreviations: MH, Microcytic hypochromic anaemia; NH, Normocytic hypochromic anaemia; NN, Normocytic normochromic anaemia; MN, Macrocytic normochromic anaemia. |
Risks Factors Associated with Anaemia
Several factors considered to be associated with anaemia during lactation were studied. These included age, duration of lactation, education level, marital status, occupation of mother, occupation of spouse, number of parities, household income, use of mosquito bed net, history of postpartum haemorrhage, use of iron supplements, alcohol consumption, tea consumption, deworming status, source of drinking water, malnutrition (MUAC <23.5 cm), number of antenatal (ANC) visits and consumption of iron-rich food (meat, fish, green vegetables, fruits and eggs).
On bivariate logistic regression, the following variables were found to be associated with anaemia: age group (40–49 years) (OR: 68.25, p-value 0.037), duration of lactation of 5 to 8 months (OR: 0.31, p-value 0.014), alcohol consumption (OR: 5.0, p-value 0.016) and having been dewormed in the last 3 months (OR: 0.41 and p-value 0.045); see Table 2.
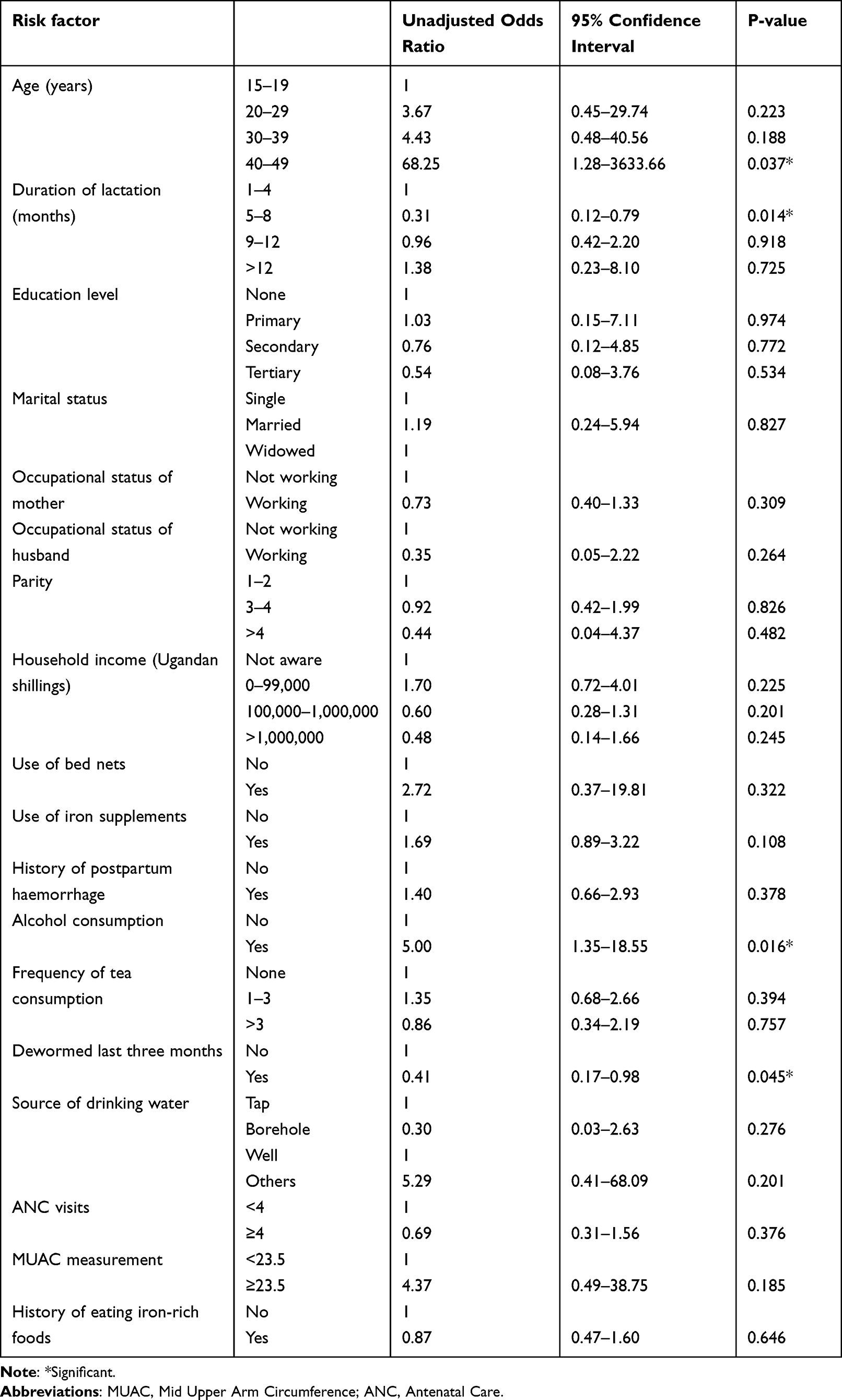 |
Table 2 Bivariate Analysis of Risk Factors Predisposing Lactating Mothers to Anaemia |
The factors that were significantly associated with anaemia in the bivariate logistic regression analysis were then subjected to multivariate logistic regression. Duration of lactation of 5 to 8 months (OR: 0.32, p-value 0.017) and alcohol consumption (OR: 3.69, p-value 0.032) remained significantly associated with anaemia during lactation (Table 3).
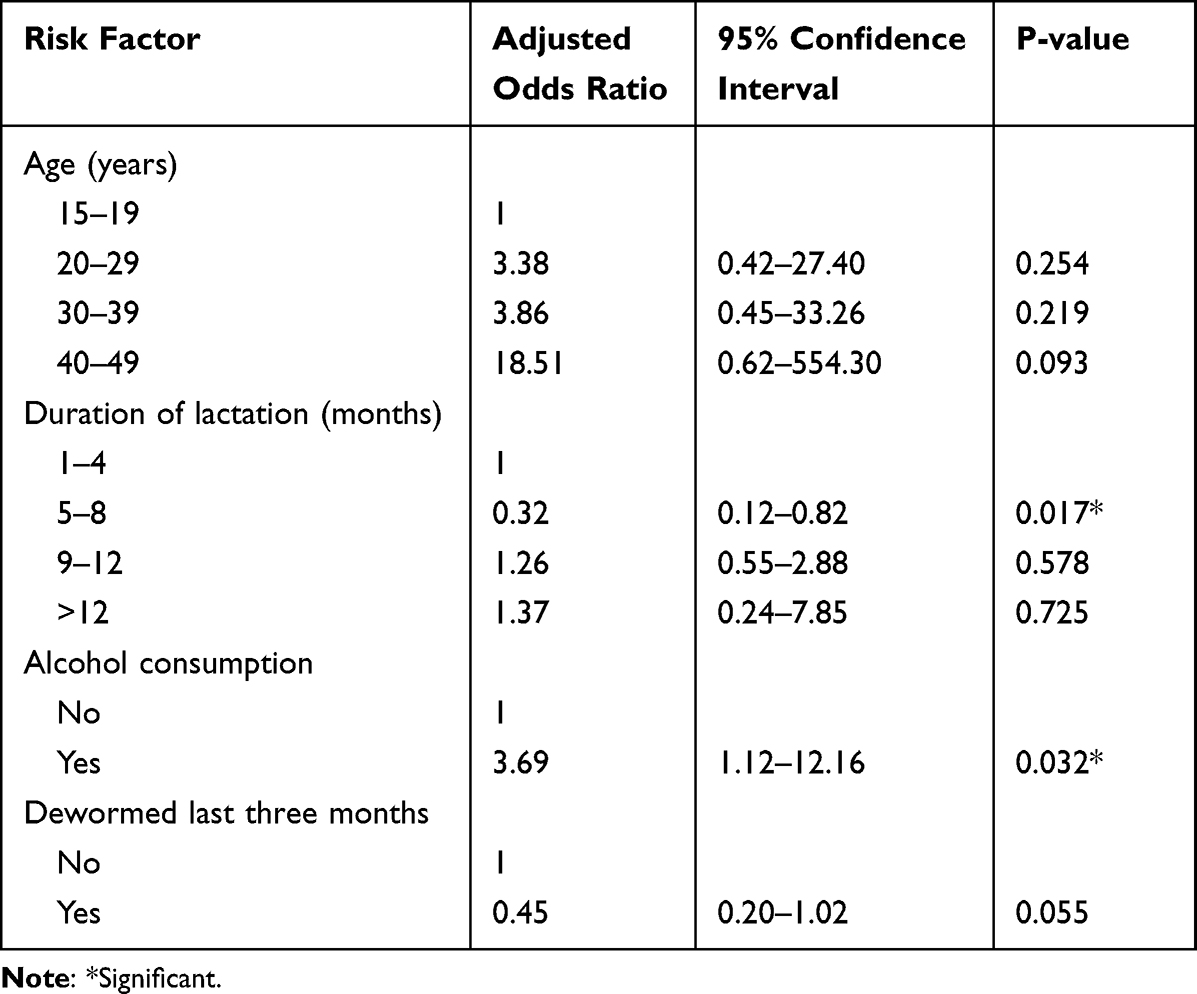 |
Table 3 Multivariate Analysis of Risk Factors Predisposing Lactating Mothers to Anaemia |
Discussion
Prevalence of Anaemia
Anaemia in lactating mothers remains a public health burden affecting both the mother and the newborn.18 We determined the prevalence and risk factors of anaemia among lactating mothers at Mbarara City Health Centre IV (MCHC-IV). The overall prevalence of anaemia among lactating mothers was 24.6%. This prevalence is lower than the national prevalence of anaemia among lactating mothers in Uganda, which is 34%.16 The difference in prevalence in these two studies could be attributed to study design since the study across Uganda was a demographic health survey and this study was only in one region. The sample size in this study was also smaller than the health survey conducted among a very large number of study participants and differences in the techniques used in anaemia diagnosis.
This finding is comparable with studies from Kenya 25%,13 Tanzania with 22%12 and several studies in Ethiopia 22.1%,11 28.3%15 and 28.9%.19 Our study was also similar to studies in Argentina and Nepal, with 25.8%20 and 20%,21 respectively.
The prevalence of anaemia in this study is however lower than the prevalence reported in East Africa 36.5%,18 Myanmar 73.8%,8 India 62.9%,9 Binjai in Indonesia 52%,22 Ethiopia,43%23 and Somalia 48.7%.11 The lower prevalence of anaemia could be attributed to geographical location, feeding habits, differences in sample size and socioeconomic status of these lactating mothers in these studies compared to ours.
Our study finding was however higher than the prevalence reported in Japan, 10.5%.24 This higher prevalence in our study could be due to differences in socio-economic status of lactating women in Japan and Uganda. It can also be due to larger sample size, geographical location, retrospective cohort study design and larger time period employed in the Japanese study.
Morphological Classification of Anaemia
According to our study, most of the anaemic study participants had normocytic normochromic blood picture (41.5%), followed by microcytic hypochromic blood picture (30.8%), normocytic hypochromic blood picture (24.1%) and macrocytic normochromic blood picture (3.1%). This finding disagreed with a study that reported microcytic hypochromic anaemia as the most prevalent morphological type of anaemia among lactating mothers in Ethiopia.23 Normocytic normochromic anaemia was the commonest type of anaemia in our study because lactating mothers lose blood during delivery and also are at risk of being malnourished during lactation. This blood picture could also be attributed to early stage of iron deficiency, in which majority of the red blood cells are normocytic normochromic. However, normocytic normochromic anaemia is also found in other conditions like chronic infection, inflammatory diseases, malignant diseases, renal failure, hypothyroidism, hypopituitarism, marrow failure, acute blood loss and rheumatoid arthritis.25 These conditions can also happen in the lactating phase, which could have contributed to normocytic normochromic anaemia to being the major morphological type of anaemia in this study. Generally, there is a scarcity of literatures on morphological classification of anaemia in lactating mothers; most studies that studied anaemia in lactating mothers used Hb, serum iron levels and ferritin in determining anaemia.
Associated Risk Factors with Anaemia
Alcohol affects the production of red bloods cells from bone marrow and promotes the production of abnormally shaped red blood cells that are destroyed earlier than their 120-day life cycle and this causes anaemia since destruction of abnormally shaped red blood cells reduces haemoglobin levels and reduces the oxygen carrying capacity of red blood cells that the body requires for normal physiology.26 Alcohol consumption was found to be significantly associated with high odds of developing anaemia during lactation. This disagreed with a study done in agro-ecological zones of Ethiopia that studied drinking of Tella (local alcohol) and anaemia during lactation in rural Ethiopia and found no association.14
Lower duration of lactation that is 5 to 8 months were found to be significantly associated with lower odds of developing anaemia during lactation. This disagrees with a study that was done by Liyew et al in Ethiopia that showed that neither low nor high duration of breastfeeding was associated with anaemia during lactation.15 This could be due to health habit that since mothers lose blood during delivery, they are put on iron supplementation to restore their haemoglobin levels when they give birth at MCC-HC IV, so this lowers their odds of developing anaemia.
Conclusion
The reported prevalence of anaemia among lactating mothers in this study is a moderate public health problem. Duration of lactation (5 to 8 months) and alcohol consumption were risk factors found to be associated with anaemia. Routine anaemia screening of all postnatal mothers and iron supplementation immediately after delivery is recommended. Lactating mothers are also advised to reduce alcohol consumption during lactation period. Further studies are recommended to explore the underlying causes of anaemia during lactation.
Limitations of the Study
This study did not collect data on factors such as malaria, tuberculosis and HIV infection that can also predispose lactating mothers to anaemia.
Acknowledgments
The authors acknowledge the staff of Mbarara City Health Centre IV for the assistance rendered to us during our data collection. We also acknowledge the study participants for participating in this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Alemayehu M. Factors associated with anemia among lactating mothers in subsistence farming households from selected districts of Jimma zone, south western Ethiopia: a community based cross-sectional study. J Nutr Food Sci. 2017;7(3). doi:10.4172/2155-9600.1000595
2. World Health Organization. WHO Methods and Data Sources for Global Burden of Disease Estimates 2000–2011. Geneva: Department of Health Statistics and Information Systems; 2013.
3. Gardner W, Kassebaum N. Global, regional, and national prevalence of anemia and its causes in 204 countries and territories, 1990–2019. Curr Develop Nutr. 2020;4(Supplement_2):830. doi:10.1093/cdn/nzaa053_035
4. World Health Organization. WHO Global Anaemia estimates, 2021 Edition. Global anaemia estimates in women of reproductive age, by pregnancy status, and in children aged 6–59 months; 2021. Available from: https://www.who.int/data/gho/data/themes/topics/anaemia_in_women_and_children.
5. Stevens GA, Finucane MM, De-regil LM, et al. Global, regional, and national trends in haemoglobin concentration and prevalence of total and severe anaemia in children and pregnant and non-pregnant women for 1995–2011: a systematic analysis of population-representative data. Lancet Global Health. 2013;1(1):e16–e25. doi:10.1016/S2214-109X(13)70001-9
6. Zhao A, Zhang J, Wu W, Wang P, Zhang Y. Postpartum anemia is a neglected public health issue in China: a cross-sectional study. Asia Pac J Clin Nutr. 2019;28(4):793. doi:10.6133/apjcn.201912_28(4).0016
7. Gao H, Zhang Y, Wang P, et al. Prevalence of anemia and its risk factors among lactating mothers in Myanmar. Am J Trop Med Hyg. 2014;90(5):963–967. doi:10.4269/ajtmh.13-0660
8. Zhang Y. Anemia among lactating mothers in Kokang, Myanmar; 2016.
9. Siddiqui MZ, Goli S, Reja T, et al. Prevalence of anemia and its determinants among pregnant, lactating, and nonpregnant nonlactating women in India. Sage Open. 2017;7(3):2158244017725555. doi:10.1177/2158244017725555
10. Milman N. Postpartum anemia I: definition, prevalence, causes, and consequences. Ann Hematol. 2011;90(11):1247–1253. doi:10.1007/s00277-011-1279-z
11. Lakew Y, Biadgilign S, Haile D. Anaemia prevalence and associated factors among lactating mothers in Ethiopia: evidence from the 2005 and 2011 demographic and health surveys. BMJ open. 2015;5(4):e006001. doi:10.1136/bmjopen-2014-006001
12. Tairo SR. Prevalence and risk factors associated with postpartum anaemia among postnatal women in Dodoma city: the University of Dodoma; 2020.
13. Fujita M, Wander K. A test of the optimal iron hypothesis among breastfeeding Ariaal mothers in northern Kenya. Am J Phys Anthropol. 2017;164(3):586–597. doi:10.1002/ajpa.23299
14. Roba KT, O’Connor TP, Belachew T, O’Brien NM. Seasonal variation in nutritional status and anemia among lactating mothers in two agro-ecological zones of rural Ethiopia: a longitudinal study. Nutrition. 2015;31(10):1213–1218. doi:10.1016/j.nut.2015.03.007
15. Liyew AM, Teshale AB. Individual and community level factors associated with anemia among lactating mothers in Ethiopia using data from Ethiopian demographic and health survey, 2016; a multilevel analysis. BMC Public Health. 2020;20:1–11. doi:10.1186/s12889-020-08934-9
16. UDHS. Uganda demographic health survey 2016, Uganda bureau of statistics Kampala, Uganda, The DHS Program ICF Rockville, Maryland, USA; 2016.
17. UDHS. Uganda demographic and health survey 2016 key indicators report Uganda bureau of statistics Kampala, Uganda The DHS program ICF International Rockville, Maryland, USA, March 2017; 2016.
18. Tusa BS, Weldesenbet AB, Bahiru N, Enyew DB. Magnitudes of Anemia and its determinant factors among lactating mother in East Africa countries; using generalized mixed effect model. Front Nutr. 2021;8:401. doi:10.3389/fnut.2021.667466
19. Seifu B, Yilma D. Prevalence and associated factors of anemia among lactating women in Ethiopia from 2010 to 2020: a systematic review and meta-analysis. BioMed Res J. 2020;5(2):327–342.
20. Varea A, Malpeli A, Disalvo L, et al. Evaluation of the impact of a food program on the micronutrient nutritional status of Argentinean lactating mothers. Biol Trace Elem Res. 2012;150(1):103–108. doi:10.1007/s12011-012-9512-8
21. Chandyo RK, Henjum S, Ulak M, et al. The prevalence of anemia and iron deficiency is more common in breastfed infants than their mothers in Bhaktapur, Nepal. Eur J Clin Nutr. 2016;70(4):456–462. doi:10.1038/ejcn.2015.199
22. Sudaryati E, Nasution E, Yustina I, editors. Stunting and anemia in infants among breastfeeding mothers in Binjai City.
23. Feleke BE, Feleke TE. Pregnant mothers are more anemic than lactating mothers, a comparative cross-sectional study, Bahir Dar, Ethiopia. BMC Hematol. 2018;18(1):1–7. doi:10.1186/s12878-018-0096-1
24. Amano I, Murakami A. Prevalence of infant and maternal anemia during the lactation period in Japan. Pediatr Int. 2019;61(5):495–503. doi:10.1111/ped.13833
25. Weatherall DJ. Oxford Textbook of Medicine. Normochromic, Normocytic Anaemia. Oxford University Press; 2011.
26. Gonzalez-Casas R, Jones EA, Moreno-Otero R. Spectrum of anemia associated with chronic liver disease. WJG. 2009;15(37):4653. doi:10.3748/wjg.15.4653
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Psychological Impact of Quarantine During the COVID-19 Pandemic on Quarantined Non-Healthcare Workers, Quarantined Healthcare Workers, and Medical Staff at the Quarantine Facility in Saudi Arabia
Alfaifi A, Darraj A, El-Setouhy M
Psychology Research and Behavior Management 2022, 15:1259-1270
Published Date: 17 May 2022
Anemia and Associated Factors Among Under Five Year Old Children Who Attended Bule Hora General Hospital in West Guji zone, Southern Ethiopia
Aliyo A, Jibril A
Journal of Blood Medicine 2022, 13:395-406
Published Date: 5 July 2022
Dry Season Eimeria Infection in Dairy Cattle and Sheep in and Around Adama and Bishoftu Towns, Oromia, Ethiopia
Ayana D, Temesgen K, Kumsa B, Alkadir G
Veterinary Medicine: Research and Reports 2022, 13:235-245
Published Date: 9 September 2022
Chronic Obstructive Pulmonary Disease Prevalence and Associated Risk Factors in Adults Aged 40 Years and Older in Southeast China: A Cross-Sectional Study During 2019–2020
Chen J, Yin Y, Zhang Y, Lin X, Chen T, Yang Z, Wang D, Zhong W
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2317-2328
Published Date: 17 September 2022
Prevalence, Management, and Risk Factors of Asthma Among School-Age Children in Yogyakarta, Indonesia
Triasih R, Setyowireni D, Nurani N, Setyati A
Journal of Asthma and Allergy 2023, 16:23-32
Published Date: 5 January 2023