Back to Journals » Patient Preference and Adherence » Volume 17
The Mediating Effect of Resilience on the Relationship Between Symptom Burden and Anxiety/Depression Among Chinese Patients with Primary Liver Cancer After Liver Resection
Authors Zhang X, Zhang H, Zhang Z ![]() , Fan H, Li S
, Fan H, Li S ![]()
Received 20 July 2023
Accepted for publication 4 November 2023
Published 20 November 2023 Volume 2023:17 Pages 3033—3043
DOI https://doi.org/10.2147/PPA.S430790
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Qizhi (Cathy) Yao
Xue Zhang,1 Haoran Zhang,1 Zonghao Zhang,1 Hua Fan,2 Shuwen Li1
1School of Nursing, Anhui Medical University, Hefei, Anhui, People’s Republic of China; 2Department of Hepatobiliary Surgery, Anhui Provincial Hospital, the First Affiliated Hospital of University of Science and Technology of China, Hefei, Anhui, People’s Republic of China
Correspondence: Shuwen Li, School of Nursing, Anhui Medical University, Hefei, Anhui, 230601, People’s Republic of China, Email [email protected]
Purpose: Primary liver cancer (PLC) is a common cancer of the digestive system. Patients with PLC often experience a heavy symptom burden and along with a significant levels of anxiety and depression after liver resection. High levels of symptom burden can lead to increased anxiety and depression, whereas high levels of resilience can alleviate these conditions. Therefore, we aimed to explore the relationships among symptom burden, resilience, and anxiety/depression in Chinese patients with PLC after liver resection and to determine whether resilience mediates the relationship between symptom burden and anxiety/depression.
Patients and Methods: A total of 223 postoperative PLC patients were recruited from two public hospitals in Anhui Province, China. All participants completed the MD Anderson Symptom Inventory (MDASI), Hospital Anxiety and Depression Scale (HADS), and Connor-Davidson Resilience Scale (CD-RISC). The mediating effect of resilience was estimated using the bootstrap method via IBM SPSS AMOS 26.0.
Results: The mean HADS score was 12.37 ± 6.03 points in postoperative PLC patients. Among these patients, 78 (34.98%) had anxiety, and 64 (28.70%) had depression, as indicated by a subscale score ≥ 8. Pearson correlation analysis revealed that anxiety/depression was positively associated with symptom burden (p < 0.05) and negatively associated with resilience (p < 0.05). Furthermore, resilience partially mediated the relationship between symptom burden and anxiety/depression (β = 0.04; 95% confidence interval: 0.01– 0.08).
Conclusion: The levels of anxiety and depression in postoperative PLC patients should be decreased. Resilience partially mediated the relationship between symptom burden and anxiety/depression, but the indirect effect was much weaker than the direct effect of symptom burden on anxiety/depression. Consequently, rather than focusing primarily on resilience interventions, joint symptom-psychological interventions focusing on symptoms should be considered for patients with PLC after hepatectomy to reduce the levels of anxiety/depression.
Keywords: anxiety, depression, liver cancer, resilience, surgery, symptom burden
Introduction
Primary liver cancer (PLC) is a common cancer of the digestive system, encompassing three distinct pathological subtypes: hepatocellular carcinoma (HCC), intrahepatic cholangiocarcinoma (ICC), and mixed hepatocellular carcinoma-cholangiocarcinoma (cHCC-CCA).1 According to the latest data from the World Health Organization (WHO), liver cancer is the sixth most common type of cancer worldwide and the third leading cause of cancer-related death, with 905,700 new cases and 830,200 deaths in 2020. Chinese patients account for more than half of liver cancer patients worldwide.2 In 2020, liver cancer ranked fourth in new cases (410,000) among all malignancies and ranked second in deaths (391,100), well above the global total.2,3 The main curative treatment for liver cancer is liver resection, which entails the direct removal of the diseased tissue and has a significant therapeutic effect on patients who meet surgical conditions. This is the first choice of treatment for liver cancer.4
However, surgical resection involves large blood vessels and vital organs, and most patients experience psychological problems after experiencing surgical trauma.5 Liver resection requires removal of part of the liver tissue, and after the operation, patients are at risk of postoperative complications such as fluid retention in the body cavity, hemorrhage, bile leakage, and hepatic failure, which can lead to psychological problems such as anxiety, fear, and depression.6,7 Patients who undergo liver resection also experience moderate to severe postoperative pain, postoperative anesthesia, various intubation and other stressors, which can easily lead to anxiety and depression.8,9
Anxiety and depression are two of the most common psychological problems in cancer patients. The presence of anxiety and depression can significantly reduce patients’ compliance with treatment,10 leading to more difficulty with symptom management during treatment and prolonged hospitalization,11 thereby seriously affecting their prognosis and reducing overall survival.5,12,13 Studies have shown that approximately 42.00% of PLC patients have varying degrees of anxiety after liver resection, and 48.70% of patients have varying degrees of depression.14 Living with anxiety and depression may seriously affect the quality of life of PLC patients.15
In addition to psychological problems such as anxiety and depression, PLC patients also experience a heavy burden of physical symptoms after undergoing surgery. As liver resection is a significant invasive surgery that involves vital organs and large blood vessels, it can elicit multiple postoperative symptoms in patients. These symptoms can include abdominal incision pain due to pulling,16 metabolic dysfunction or nutrient absorption disorders, which often manifest as feelings of fatigue and lethargy in patients.17,18 The traction of adjacent organs during surgery, as well as the negative effects of anesthetic drugs and prolonged postoperative gastrointestinal dysfunction, may result in gastrointestinal symptoms, including nausea and bloating.19 A systematic review aimed to create an item bank of patient-reported symptoms for patients with hepatobiliary or pancreatic malignancies found that 40 self-reported symptoms were present following hepatectomy.20 A survey on the symptom burden of 160 Chinese patients with PLC who underwent liver resection showed that 100% had fatigue, pain, decreased appetite, dry mouth, and bloating.21 Of the 19 symptoms evaluated on the MD Anderson Symptom Inventory (MDASI) and the Symptom Module specific to Primary Liver Cancer (TSM-PLC) scales, 11 exhibited a prevalence exceeding 50%, with 5 demonstrating a severity score of ≥ 4.21 Thus, PLC patients experience a high number of symptoms, high severity, and a heavy symptom burden.
In liver cancer patients, several studies have confirmed the relationships of symptoms with anxiety and depression, reporting that a heavy symptom burden leads to high levels of anxiety and depression.22,23 However, the mechanisms by which symptoms affect anxiety and depression are unclear. Resilience is a dynamic process that maintains normal psychological and physiological functions24 and dynamically and appropriately self-regulates after experiencing severe stress or trauma to avoid or reduce psychological problems. The American Psychological Association defines resilience as a “process” ability that enables individuals to adapt well to adversity, trauma, tragedy, threat, and even severe stressors.25 Previous studies have shown that a high level of resilience can help patients face the disease optimistically, actively cooperate with treatment and rehabilitation, and alleviate anxiety and depression levels.26 Resilience may reduce anxiety and depression by fostering some unique characteristics (self-examination, responsibility, tolerance, the ability to adapt to different environmental requirements, and a sound perspective on reality).27,28 Previous studies have confirmed the mediating role of resilience in the relationships of some psychological symptoms with anxiety and depression, including stress, loneliness, and burnout.29–32 However, physical symptoms such as pain and bloating are the primary symptoms experienced by patients with PLC after liver resection, alongside psychological symptoms. Further research is needed to investigate the relationships of symptom burdens with anxiety and depression in PLC patients.
Therefore, we conducted this survey to identify and explore the relationships among symptom burden, resilience, and anxiety/depression in postoperative PLC patients. There were two main hypotheses. First, we hypothesized that a lighter symptom burden and higher resilience in postoperative PLC patients are associated with lower anxiety/depression. Second, we hypothesized that the relationship between symptom burden and anxiety/depression is mediated by resilience.
Materials and Methods
Methods
Study Design
This cross-sectional study was conducted from September 2021 to July 2022 in two general hospitals in Anhui Province, China. This study was approved by the Ethics Committee of Anhui Medical University (No. 84220046). All participants provided informed consent. The research was conducted in accordance with the ethical guidelines outlined in the Declaration of Helsinki.
Participants
A total of 223 patients with PLC who underwent surgery were selected by convenience sampling methods. The inclusion criteria for hospitalized patients were as follows: (1) age ≥ 18 years, diagnosed with PLC encompassing HCC, ICC and cHCC-CCA by pathological examination; (2) underwent liver resection for the first time; and (3) provided informed consent to participate in the study. The exclusion criteria were as follows: (1) diagnosed with other serious physical diseases; (2) participating in other clinical trials or related treatments that may impact this study; (3) unconsciousness or communication impairment and (4) family protection of the patient’s condition.
Procedures
This survey was conducted after PLC patients were hospitalized for surgery. Before the investigation, the researchers contacted the hospital and obtained consent. Then, the researchers distributed questionnaires to PLC patients with stable vital signs, and clear consciousness within 3 days after the operation. Three trained researchers who were trained were responsible for administering the questionnaire survey. The training content included the research purpose and significance, content description of questionnaires and scales, and data collection methods and precautions. Before the formal investigation, each researcher explained the purpose and significance of the study to the patients using standardized instructions. After obtaining informed consent, the researchers distributed questionnaires face-to-face, and the patients completed the questionnaires according to their current conditions. The researchers collected the questionnaires on the spot and checked their completion to ensure the quality of the questionnaires. A total of 223 questionnaires were distributed, all of which were returned, thus yielding a survey recovery rate of 100%. Clinical data were reviewed and supplemented based on the information documented in the hospital information system (HIS).
Materials
The Demographic Information Questionnaire
The self-designed demographic and disease-related questionnaire collected sociodemographic information such as age, sex, education level, and residence, as well as disease characteristics including time since diagnosis, history of hepatitis, and history of cirrhosis.
MD Anderson Symptom Inventory (MDASI)
The symptom burden of individuals was assessed with the Chinese version of the MDASI, which was originally developed by Cleeland et al33 and translated by Wang et al34 (Cronbach’s α values of 0.86 and 0.84, respectively). The inventory contains 19 items divided into 2 sections. The MDASI-Part I evaluates the severity of 13 common cancer symptoms, such as pain, nausea, and fatigue, in the past 24 hours. Each item is scored on a scale from 0 (no symptoms) to 10 (the most severe imaginable). The MDASI-Part II evaluates the distressing effects of the 13 abovementioned symptoms on six aspects of daily life, including general activities, emotions, work, relationships with others, walking, and joy of life. Each item is scored on a scale from 0 (no trouble) to 10 (completely bothered). Cronbach’s α coefficient for this scale was 0.81 in this study.
Hospital Anxiety and Depression Scale (HADS)
The levels of anxiety and depression were measured using the HADS, which was originally developed by Zigmond et al35 (Cronbach’s α = 0.88). The scale contains 14 items divided into 2 subscales, namely anxiety (n = 7) and depression (n = 7). Each item is scored on a 4-point scale from 0 to 3, with higher scores indicating higher anxiety and depression. A subscale score ≥8 indicates anxiety or depression. Cronbach’s α coefficient for this scale was 0.86 in this study.
Connor-Davidson Resilience Scale (CD-RISC)
Resilience was measured using the CD-RISC, which was originally developed by Conner et al36 and then translated and revised by Yu et al37 (Cronbach’s α = 0.90). The scale contains 25 items divided into 3 subdimensions, including tenacity (n = 13), strength (n = 8) and optimism (n=4). Each item is rated on a 4-point scale ranging from 1 (completely inconsistent) to 4 (completely consistent), with higher scores indicating better resilience. Cronbach’s α coefficient for this scale was 0.89 in this study.
Statistical Analysis
Data were processed with Excel, and data analysis was completed with SPSS 26.0. Quantitative variables that exhibited a normal distribution are presented as the mean ± standard deviation; otherwise variables are presented as the median and interquartile range (IQR). Qualitative data are described with the frequency and percentage. Means were compared between two groups using a t test if the data were independent, normally distributed, and exhibited homogeneity of variance; means were compared between more than two groups using one-way analysis of variance (ANOVA) if the data were independent, normally distributed, and exhibited homogeneity of variance. If the data did not meet these assumptions, a rank sum test was performed. In addition, Pearson correlation analysis was performed to explore the relationships among symptom burden, resilience and anxiety/depression. The bootstrap method implemented in IBM SPSS AMOS 26.0 was used to estimate the mediating effect of resilience. All tests were two tailed, and results were considered significant at p values of 0.05.
Results
Demographic and Clinical Characteristics
As shown in Table 1, the mean age of the participants was 57.70 (SD = 12.60) years, with a range of 28–85 years, and the median duration of disease diagnosis was 0.80 (IQR= 0.70) months. Most of the patients were male (77.13%) and had junior high school education or below (76.23%).
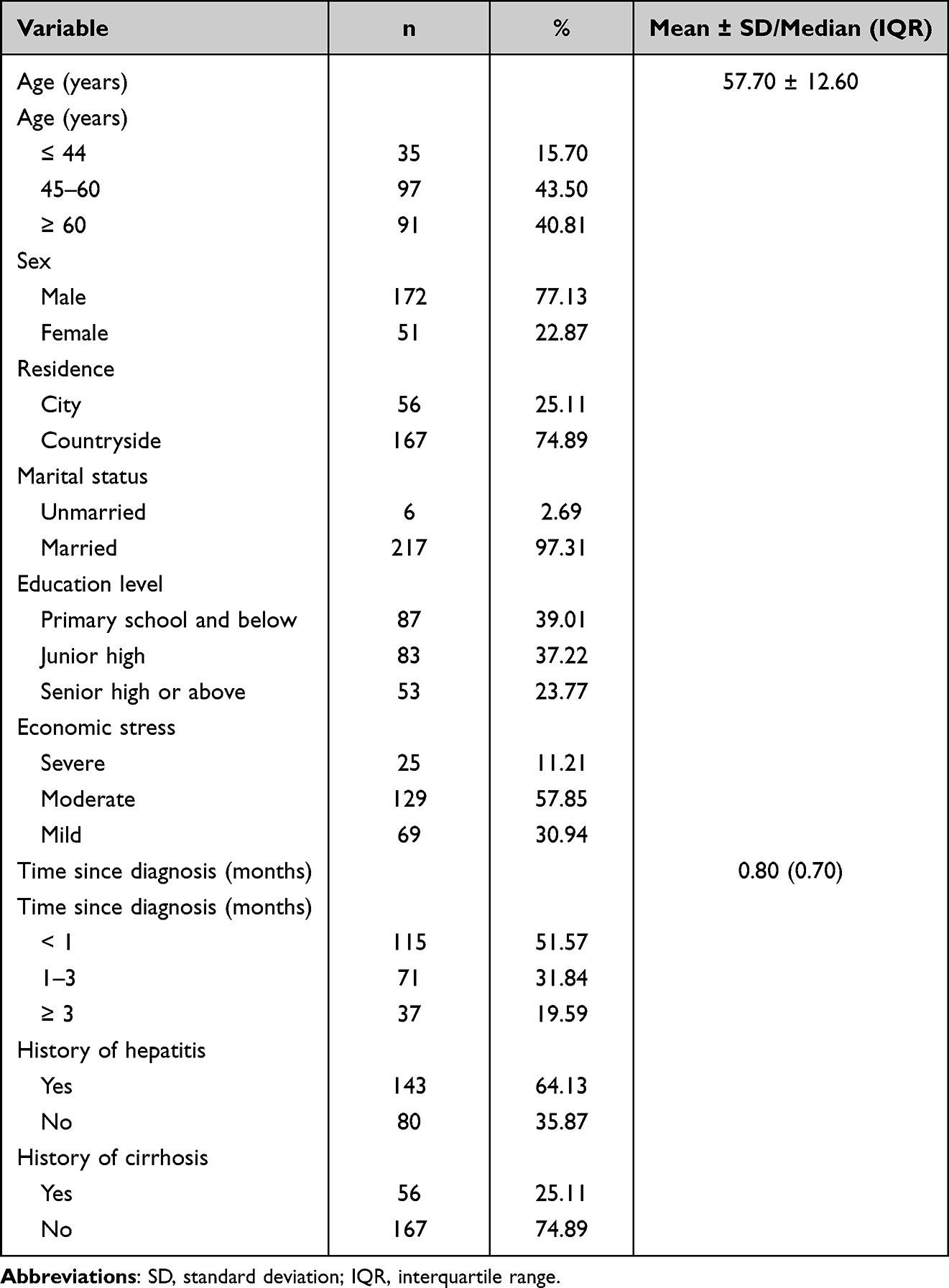 |
Table 1 Demographic and Clinical Characteristics of Participants (N = 223) |
Differences in Anxiety/Depression by Demographic and Clinical Features
Significant differences were found in anxiety/depression according to marital status and economic stress (Table 2).
 |
Table 2 Differences in Anxiety/Depression by Demographic and Clinical Features (N = 223) |
Descriptive Statistics and Correlations of Variables
As shown in Appendix 1, the mean HADS score was 12.37 ± 6.03 points, the mean anxiety score was 6.21 ± 3.11 points, and the mean depression score was 6.16 ± 3.23 points in postoperative PLC patients. Among these patients, 34.98% had anxiety, and 28.70% had depression (HADS subscale scores ≥ 8 points). The mean CD-RISC score was 73.40 ± 11.13 points, the mean tenacity score was 36.96 ± 6.86 points, the mean strength score was 25.44 ± 3.90 points, and the mean optimism score was 11.00 ± 1.82 points. The mean MDASI score was 68.55 ± 15.79 points, the mean MDASI-Part I score was 37.68 ± 11.59 points, and the mean MDASI-Part II score was 30.87 ± 6.21 points. The six symptoms with the highest average severity were fatigue (6.11 ± 1.86), dry mouth (6.03 ± 1.69), pain (5.97 ± 1.53), lack of appetite (3.56 ± 1.62), drowsiness (3.49 ± 2.28), and disturbed sleep (3.44 ± 1.86). The six symptoms with the highest incidence were pain (100%), fatigue (100%), dry mouth (99.55%), lack of appetite (99.10%), drowsiness (88.34%), and distress (87.89%). The postoperative symptom burden of PLC patients is mainly involves distress with physical function, which is a systemic manifestation.
Pearson correlation analysis showed that anxiety/depression was significantly and negatively correlated with resilience in postoperative PLC patients (r = -0.41, p < 0.05). In addition, anxiety/depression was significantly and positively associated with symptom burden (r = 0.57, p < 0.05). As shown in Table 3.
 |
Table 3 Descriptive Statistics and Correlations of Variables (N = 223) |
Model Test
We used SEM in SPSS Amos to test the relationships among anxiety/depression, resilience, and symptom burden. The goodness-of-fit indices (χ2/df = 2.72, SRMR = 0.04, RMSEA = 0.09, GFI = 0.98, NFI = 0.97, TLI = 0.96, and CFI = 0.98) indicated that the model fit was satisfactory. Based on the model fitting results, the bias-corrected percentile method was used to test for mediating effects. Symptom burden significantly and negatively predicted resilience (β = −2.42, p < 0.01), symptom burden significantly and positively predicted anxiety/depression (β = 0.25, p < 0.01), and resilience significantly and negatively predicted anxiety/depression (β = -0.02, p < 0.01). The results also showed that the indirect effect of symptom burden on anxiety/depression through resilience was 0.04 (p < 0.05), with a 95% confidence interval (5000 samples) of [0.01–0.08]. Since this confidence interval did not include zero, we concluded that resilience had a significant mediating effect on the relationship of symptom burden with anxiety/depression; the indirect effect, as a proportion of the total effect, was 13.79% (Figure 1).
 |
Figure 1 Model of the mediating effect of resilience on the association of symptom burden with anxiety/depression. **p value < 0.01, *p value < 0.05. Values on paths are path coefficients (non-standardized βs). |
Discussion
Current Status of Symptom Burden, and Anxiety/Depression in Postoperative PLC Patients
The mean MDASI score was 68.55 ± 15.79 points, and the mean MDASI-Part II score was 30.87 ± 6.21 points. Up to 9 out of the 13 symptoms in the MDASI scale were present in over 50% of the patients, with 47% of patients scoring ≥ 7 on at least one symptom. This suggests considerable disruption in the patient’s daily life. Wang et al enrolled 150 patients who underwent hepatectomy in order to validate a patient-reported outcome tool for perioperative care. The study found that over 50% of patients experienced 9 of the 13 symptoms included in the MDASI scale before discharge, and a significant 46.7% of patients experienced at least one severe symptom (score ≥ 7) that significantly affected their daily life.38 These findings align with our research. In addition, we found that the six symptoms with the highest incidence and severity among PLC patients were mainly involved in distress with physical function, such as fatigue, dry mouth, pain, lack of appetite, drowsiness and disturbed sleep. All of these symptoms cause distress and dysfunction in the body and affect the patient’s daily life. Patients with PLC experienced a significant symptom burden after hepatectomy that severely impacted their daily life. Symptomatic interventions for PLC patients after hepatectomy are urgently needed. The investigation into cancer symptom intervention in China commenced belatedly,39 with a predominant emphasis on singular symptom following hepatectomy.40,41 In recent years, a few researchers have started to acknowledge the significance of core symptoms and carried out studies.42,43 Of these, most scholars define core symptoms as those with the highest incidence or severity.44,45 It is suggested that medical staff pay close attention to the occurrence and severity of symptoms in postoperative PLC patients, conduct systematic and continues assessment of various symptoms, especially the core symptoms, provide timely and appropriate interventions when symptoms cause distress.
The mean HADS score was 12.37 ± 6.03 points, the mean anxiety score was 6.21 ± 3.11 points, and the mean depression score was 6.16 ± 3.23 points in postoperative PLC patients. Among these patients, 34.98% had anxiety, and 28.70% had depression (subscale scores ≥ 8 points), consistent with the results of Yu46,47 et al but higher than the domestic norm.48 In addition, significant differences were found in anxiety/depression according to marital status and economic stress. The study indicated that patients who are unmarried have noticeably higher levels of anxiety/depression in comparison to those who are married. Additionally, patients who experience severe economic stress exhibit significantly higher levels of anxiety/depression than those who experience mild economic stress. The reasons for this discrepancy may be that the patients in this study were mainly middle-aged and elderly men (84.30%), who are the backbone of the family and the main income earners. However, due to the poor prognosis of the disease, the disease itself and the adverse effects of treatment, patients often experience anxiety, depression and other psychological problems. In addition, patients often worry that the cancer cannot be cured and will have a negative impact on their family, aggravating their anxiety and depression levels. Patients who are married, they may receive more family support than unmarried patients, potentially leading to an improvement in their anxiety/depression. For such patients, the medical staff should describe the recovery experience of patients after undergoing similar surgeries and encourage patients to feel confident in the likelihood of overcoming the disease. In addition, medical staff should guide patients’ families to provide good social support.
Associations Among Symptom Burden, Resilience and Anxiety/Depression in Postoperative PLC Patients
Our findings support the hypothesis that a lighter symptom burden and higher resilience may reduce anxiety/depression in patients. This study demonstrates that symptom burden not only has a direct effect on anxiety/depression, but also has an indirect effect on anxiety/depression through resilience. Correlation analyses further revealed that resilience partially mediates the relationship between symptom burden and anxiety/depression in postoperative PLC patients. A heavy symptom burden leads to serious distress in the patient’s physical function, which affects daily life, resulting in worry, depression, and unpleasant sensations. If these feelings are not addressed, they can lead to psychological problems such as anxiety/depression. Studies have found that a lighter symptom burden can promote resilience in patients, help them to regulate themselves, stimulate positive emotions, and reduce anxiety and depression.49 However, a heavy symptom burden leads to severe distress, a weaker ability to quickly adapt to and change stressful external and internal situations, a lower level of self-regulation, and an inability to maintain mental health. Therefore, the heavier the symptom burden is, the lower the resilience of the patient, and the less likely they are to maintain good mental health, leading to anxiety/depression. Improving the patient’s resilience can alleviate anxiety/depression. Studies have shown that resilience, which is an important psychological intervention target, can be improved by focusing on the solution model and positive psychological intervention.50 Therefore, it is suggested that different interventions should be used to improve the resilience of patients, thereby reducing their level of anxiety/depression.
Surprisingly, the mediating effect of resilience on the relationship of symptom burden with anxiety/depression in postoperative PLC patients explained only 13.79% of the variance, and the direct effect of symptom burden on anxiety/depression was as high as 86.21%. We speculate that this finding may be because the included subjects being postoperative PLC patients, and their psychological state is closely related to the disease itself. The significant burden of symptoms experienced by postoperative PLC patients results in significant disruptions to their daily lives, uncertainty, and changes to their physical bodies,51 all of which contribute to the development of anxiety/depression. While resilience can assist individuals in effectively coping with adversity and stress, its potential to mediate the impact of such substantial life changes and discomfort may be limited. Studies have found that the application of a combined intervention model of psychological intervention combined with nutrition and exercise interventions is significant for tumor patients.52,53 Therefore, joint symptom-psychological interventions focusing on symptoms should be considered for patients with PLC after hepatectomy to reduce the level of anxiety/depression in patients. In the clinical setting, it is recommended that medical staff pay close attention to the presence and severity of anxiety/depression in patients with PLC after hepatectomy, in addition to symptom burden. Additionally, medical staff should explain to the patients the reason why these symptoms occur in order to alleviate the worries and fears caused by the symptoms. Furthermore, patients should be encouraged to express their inner emotions and actively seek help from medical staff when they are anxious or worried about the disease or treatment. When interventions are necessary to alleviate anxiety and depression, joint symptom-psychological interventions focusing on symptoms should be considered.
Study Limitations
This study was a cross-sectional survey. Using a structural equation model can only test the correlation between variables but cannot prove the causal relationship between variables. The mediating role of resilience should be verified longitudinally. Additionally, the study employed convenience sampling to recruit participants, a method that is easy to apply but carries limitations such as high sampling bias, low representativeness, and an inability to accurately extrapolate to the wider population. In this study, we included only a few disease-related characteristics such as hepatitis and cirrhosis, and did not consider other factors of patient’s basic health status such as comorbidities and complications, which may not be comprehensive enough for the analysis of anxiety/depression.
Clinical Implications
Compared with the mediating effect of resilience, the various symptoms of the disease and treatment have a greater impact on the anxiety/depression in patients with PLC after hepatectomy. Consequently, joint symptom-psychological interventions focusing on symptoms should be considered for patients with PLC after hepatectomy, rather than focusing primarily on resilience interventions. Nevertheless, patients after hepatectomy typically encounter multiple interrelated symptoms. Medical staff often have limited time and energy to address all of the symptoms experienced by patients. Therefore, it is important to prioritize the symptoms that are most significant and require immediate attention. It is crucial to closely observe the occurrence and severity of core symptoms. Provide timely and appropriate interventions from the perspective of core symptoms when symptoms cause distress to minimize the patient’s symptom burden and ultimately alleviate the patient’s level of anxiety/depression, and to promote physical and psychological recovery.
Conclusion
The levels of anxiety/depression and symptom burden in patients with PLC after hepatectomy should be improved. Lower anxiety/depression is associated with a lighter symptom burden and higher resilience in patients. Resilience was found to partially mediates the relationship of symptom burden with anxiety/depression, but the mediation effect was much lower than the direct effect of symptom burden on anxiety/depression. It has been demonstrated that joint symptom-psychological interventions focusing on symptoms should be considered for patients with PLC after hepatectomy, rather than focusing primarily on resilience interventions. This combined intervention can alleviate patients’ heavy symptom burden and anxiety/depression level, thereby promoting their physical and psychological recovery. Considering the numerous symptoms experienced by patients after hepatectomy, and the limited availability of time and energy for medical staff, exploring symptom intervention from the core symptoms perspective is warranted.
Ethics Approval and Informed Consent
This study was approved by the Ethics Committee of Anhui Medical University (No. 84220046).
Consent for Publication
Written informed consent for publication of their details was obtained from the patient.
Acknowledgments
Thanks to all the investigators who contributed to the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The work was partially supported by the Nursing School of Anhui Medical University Qingmiao’s Program (No. hlqm12023047).
Disclosure
The authors report no conflicts of interest in this work.
References
1. General Office of National Health Commission. Standard for diagnosis and treatment of primary liver cancer (2022 edition). J Clin Hepatol. 2022;38(2):288.
2. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249.
3. Petrick JL, Florio AA, Znaor A, et al. International trends in hepatocellular carcinoma incidence, 1978-2012. Int J Cancer. 2020;147(2):317–330.
4. Orcutt ST, Anaya DA. Liver resection and surgical strategies for management of primary liver cancer. Cancer Control. 2018;25(1):1073274817744621.
5. Graf J, Stengel A. Psychological burden and psycho-oncological interventions for patients with hepatobiliary cancers-a systematic review. Front Psychol. 2021;12:662777.
6. Ghoneim MM, O’Hara MW. Depression and postoperative complications: an overview. BMC Surg. 2016;16:5.
7. Yu BJ. The Study on the Effect of Sham Feeding on Anxiety in Patients with Primary Hepatocellular Carcinoma After Hepatectomy by Laparotomy [Master’s Thesis]. Fujian Medical University; 2018.
8. Xu L, Xu Y, Li G, Yang B. Study on anxiety and depression in elderly patients with malignant liver tumor undergoing hepatectomy. Eur J Med Res. 2023;28(1):87.
9. Cancer Prevention and Treatment Expert Committee. Cross-Straits Medicine Exchange Association. Chinese expert consensus on the peri-operative management of hepatectomy for liver cancer (2021 Edition). Chine j Oncol. 2021;43(4):57.
10. Stoudemire A, Thompson TL. Medication noncompliance: systematic approaches to evaluation and intervention. Gen Hosp Psychiatry. 1983;5(4):233–239.
11. Hopwood P, Stephens RJ. Depression in patients with lung cancer: prevalence and risk factors derived from quality-of-life data. J Clin Oncol. 2000;18(4):893–903.
12. Lee KT, Lin JJ, Shi HY. Anxiety and depression are associated with long-term outcomes of hepatocellular carcinoma: a nationwide study of a cohort from Taiwan. World J Biol Psychiatry. 2018;19(6):431–439.
13. Tan DJH, Quek SXZ, Yong JN, et al. Global prevalence of depression and anxiety in patients with hepatocellular carcinoma: systematic review and meta-analysis. Clin Mol Hepatol. 2022;28(4):864–875.
14. Zhou XQ, Zhong FX, Wu L. Investigation and analysis of anxiety and depression in 150 patients after liver cancer resection. J Mathematical Med. 2021;34(12):1771–1774.
15. Lee HH, Chiu CC, Lin JJ, et al. Impact of preoperative anxiety and depression on quality of life before and after resection of hepatocellular carcinoma. J Affect Disord. 2018;246.
16. Watanabe G, Ishizawa T, Yamamoto S, et al. Impact of Abdominal Incision Type on Postoperative Pain and Quality of Life Following Hepatectomy. World J Surg. 2021;45(6):1887–1896.
17. Kasvis P, Vigano A, Bui T, Carli F, Kilgour RD. Cancer symptom burden negatively affects health-related quality of life in patients undergoing prehabilitation prior to liver resection: results from a 12-week randomized controlled trial. Appl Physiol Nutr Metab. 2023.
18. Chen DY, Bian XJ, Liu JC, et al. Standardized nutrition medication therapy procedure during perioperative period of hepatic resection surgery. Pharm Clin Res. 2021;29(03):193–198.
19. Li Y, Feng Y, Yan Q. Clinical research progress of postoperative gastrointestinal dysfunction. J Clin Anesthesiol. 2022;38(03):299–303.
20. Zhang J, Zhan Y, Chen J, et al. Development of a Patient-Reported Symptom Item Bank for Patients with Hepatobiliary or Pancreatic Malignancies: a Systematic Review. Patient Prefer Adherence. 2023;17:199–207.
21. Ma HQ, Xiao XM, Guo YB, Li Q. Study on perioperative symptom cluster and related factors in patients with primary carcinoma of liver. J Nursing Sci. 2018;33(04):19–23.
22. Huang TW, Lin CC. The mediating effects of depression on sleep disturbance and fatigue: symptom clusters in patients with hepatocellular carcinoma. Cancer Nurs. 2009;32(5):398–403.
23. Shun SC, Lai YH, Jing TT, et al. Fatigue patterns and correlates in male liver cancer patients receiving transcatheter hepatic arterial chemoembolization. Support Care Cancer. 2005;13(5):311–317.
24. Rutter M. Annual research review: resilience--clinical implications. J Child Psychol Psychiatry. 2013;54(4):474–487.
25. Southwick SM, Charney DS. The science of resilience: implications for the prevention and treatment of depression. Science. 2012;338(6103):79–82.
26. Gonzalez-Flores CJ, Garcia-Garcia G, Lerma A, et al. Resilience: a protective factor from depression and anxiety in Mexican dialysis patients. Int J Environ Res Public Health. 2021;18(22):57.
27. Richardson GE. The metatheory of resilience and resiliency. J Clin Psychol. 2002;58(3):307–321.
28. Vanderpol M. Resilience: a missing link in our understanding of survival. Harv Rev Psychiatry. 2002;10(5):302–306.
29. Song H, Zhang M, Wang Y, Yang L, Wang Y, Li Y. The impact of resilience on anxiety and depression among grass-roots civil servants in China. BMC Public Health. 2021;21(1):710.
30. Devi HM, Purborini N, Chang HJ. Mediating effect of resilience on association among stress, depression, and anxiety in Indonesian nursing students. J Prof Nurs. 2021;37(4):706–713.
31. Wang H, Hou Y, Zhang L, Yang M, Deng R, Yao J. Chinese elderly migrants’ loneliness, anxiety and depressive symptoms: the mediation effect of perceived stress and resilience. Front Public Health. 2022;10:998532.
32. Yu S, Zhang C, Xu W. Self-compassion and depression in Chinese undergraduates with left-behind experience: mediation by emotion regulation and resilience. J Clin Psychol. 2023;79(1):168–185.
33. Cleeland CS, Mendoza TR, Wang XS, et al. Assessing symptom distress in cancer patients: the M.D. Anderson Symptom Inventory. Cancer. 2000;89(7):1634–1646.
34. Wang XS, Wang Y, Guo H, Mendoza TR, Hao XS, Cleeland CS. Chinese version of the M. D. Anderson Symptom Inventory: validation and application of symptom measurement in cancer patients. Cancer. 2004;101(8):1890–1901.
35. Zigmond AS, Snaith RP. The Hospital Anxiety and Depression Scale. Acta Psychiatr Scand. 1983;67(6):361–370.
36. Connor KM, Davidson JR. Development of a new resilience scale: the Connor-Davidson Resilience Scale (CD-RISC). Depress Anxiety. 2003;18(2):76–82.
37. Yu XN, Zhang JX. Factor analysis and psychometric evaluation of the Connor-Davidson Resilience Scale (CD-RISC) with Chinese people. Soc Behav Pers. 2007;35:19–30.
38. Wang XS, Shi Q, Williams LA, et al. Development of a patient-reported outcome tool for assessing symptom burden during perioperative care in liver surgery: the MDASI-PeriOp-Hep. Eur J Oncol Nurs. 2021;52:101959.
39. Xiao YP, Li Q. Research advances in cancer symptom management. Military Nursing. 2016;33(17):34–37.
40. Xu Y, Ye M, Hong Y, et al. Efficacy of Perioperative Continuous Intravenous Lidocaine Infusion for 72 Hours on Postoperative Pain and Recovery in Patients Undergoing Hepatectomy: study Protocol for a Prospective Randomized Controlled Trial. J Pain Res. 2021;14:3665–3674.
41. Ge X, Pan Y, Jin D, Wang Y, Ge S. Effect of perioperative use of parecoxib on chronic post-surgical pain in elderly patients after hepatectomy: a prospective randomized controlled study. BMC Pharmacol Toxicol. 2021;22(1):35.
42. Zhang HL, Dong YM, Cai X, Xu CY, Wang ZH. Core symptom active attention to the use of combined focus resolution mode in patients after laparoscopic hepatectomy. Chine J Rural Med Pharm. 2021;28(02):58–59.
43. Papachristou N, Barnaghi P, Cooper B, et al. Network Analysis of the Multidimensional Symptom Experience of Oncology. Sci Rep. 2019;9(1):2258.
44. Liao J, Wang Y, Dai W, et al. Profiling symptom burden and its influencing factors at discharge for patients undergoing lung cancer surgery: a cross-sectional analysis. J Cardiothorac Surg. 2022;17(1):229.
45. Browall M, Brandberg Y, Nasic S, et al. A prospective exploration of symptom burden clusters in women with breast cancer during chemotherapy treatment. Support Care Cancer. 2017;25(5):1423–1429.
46. Yu SM, Zhu Y, Wang LF, et al. Effects of anxiety and depressive states on immune function in patients with primary liver cancer. Chine Hepatol. 2018;23(06):496–498.
47. Liu SY, He FY, Chen MX, Wu T, Zhang M, Qin HY. Mediating effect analysis of self-efficacy in the relationship between fear of progression, and anxiety and depression among liver cancer patients. J Nursing Adm. 2021;21(02):91–94.
48. Fan Q, Ji JL, Xiao ZP, et al. Use of Hospital Anxiety and Depression Scale in Chinese outpatient in department of internal medicine. Chine Mental Health J. 2010;24(05):325–328.
49. Shanahan ML, Fischer IC, Rand KL. Hope, optimism, and affect as predictors and consequences of expectancies: the potential moderating roles of perceived control and success. J Res Pers. 2020;84:103903.
50. Sun T, Liu L, Zhang BY, Zhao WY, Pang R, Lv YM. Effect of sleep quality on quality of life in patients with thyroid cancer after surgery: the chain mediating effect of neuroticism and resilience. China J Health Psychol. 2023;1–13.
51. Drott J, Björnsson B, Sandström P, Berterö C. Experiences of Symptoms and Impact on Daily Life and Health in Hepatocellular Carcinoma Patients: a Meta-synthesis of Qualitative Research. Cancer Nurs. 2022;45(6):430–437.
52. Cui X, Shan T, Qiao L. Effect of Self-Transcendence Theory Combined with Comprehensive Nursing Intervention under Tumor Nutrition Education on Symptom Improvement, Nutritional Status, and Positive Psychology of Elderly Patients with Gastric Cancer. Contrast Media Mol Imaging. 2022;2022:6084732.
53. Holtdirk F, Mehnert A, Weiss M, et al. Results of the Optimune trial: a randomized controlled trial evaluating a novel Internet intervention for breast cancer survivors. PLoS One. 2021;16(5):57.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Resilience Moderates the Association of Sleep Disturbance and Sleep Reactivity with Depressive Symptoms in Adult Volunteers
Terao I, Masuya J, Morishita C, Higashiyama M, Shimura A, Tamada Y, Inoue T, Fujimura Y
Neuropsychiatric Disease and Treatment 2022, 18:1249-1257
Published Date: 20 June 2022
A Narrative Review of Research on Adjustment to Spinal Cord Injury and Mental Health: Gaps, Future Directions, and Practice Recommendations
Sandalic D, Arora M, Pozzato I, Simpson G, Middleton J, Craig A
Psychology Research and Behavior Management 2022, 15:1997-2010
Published Date: 5 August 2022
Resilience and Depressive Symptoms Mediated Pathways from Social Support to Suicidal Ideation Among Undergraduates During the COVID-19 Campus Lockdown in China
Zhang X, Liu X, Mi Y, Wang W, Xu H
Psychology Research and Behavior Management 2022, 15:2291-2301
Published Date: 23 August 2022
How Interpersonal Sensitivity Affects Depression Under the COVID-19 Lockdown Among College Students in South China: A Moderated Mediation Model
Zhang Y, Sun Q
Psychology Research and Behavior Management 2023, 16:1271-1282
Published Date: 18 April 2023
Longitudinal Problematic Social Media Use in Students and Its Association with Negative Mental Health Outcomes
Shannon H, Bush K, Shvetz C, Paquin V, Morency J, Hellemans KGC, Guimond S
Psychology Research and Behavior Management 2024, 17:1551-1560
Published Date: 8 April 2024