Back to Journals » Risk Management and Healthcare Policy » Volume 18
Remnant Cholesterol Inflammatory Index for Predicting Heart Failure Risk in Patients with Coronary Artery Disease and Type 2 Diabetes: A Retrospective Study Using Multiple Machine Learning Approaches
Received 10 September 2025
Accepted for publication 9 December 2025
Published 26 December 2025 Volume 2025:18 Pages 4027—4036
DOI https://doi.org/10.2147/RMHP.S566696
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Gulsum Kaya
Chaozhong Luo, Juan Du, Changjiang Zhang
Department of Cardiology, Minda Hospital of Hubei Minzu University, Enshi, Hubei, People’s Republic of China
Correspondence: Changjiang Zhang, Email [email protected]
Background: Patients with coronary artery disease (CAD) and type 2 diabetes mellitus (T2DM) are at markedly increased risk of developing heart failure (HF), yet early identification of high-risk individuals remains challenging. The remnant cholesterol inflammatory index (RCII) has been proposed as a predictor of adverse cardiovascular outcomes, but its role in patients with CAD and T2DM has not been fully elucidated.
Methods: We retrospectively analyzed clinical data from patients treated at our center. Demographic characteristics, comorbidities, medication use, and laboratory parameters were collected. Key features were selected using the Boruta algorithm, and five machine learning models—logistic regression (Logistic), decision tree (DT), elastic net regression (ENet), LASSO regression, and naïve Bayes (NB)—were constructed. Discrimination was assessed by receiver operating characteristic (ROC) curves and area under the curve (AUC), calibration by calibration plots and Brier scores, and interpretability by SHAP analysis.
Results: Among 1181 enrolled patients, 73 developed HF. Median RCII levels were significantly higher in the HF group. Boruta feature selection identified 13 key predictors for model development. Logistic regression demonstrated the best performance, achieving AUCs of 0.88 in the training set and 0.85 in the testing set, with overall accuracy of 0.87 and F1-score of 0.79 in the testing cohort. SHAP analysis revealed that elevated RCII, poor nutritional status, and smoking were major contributors to HF occurrence, with RCII showing a positive association with HF risk.
Conclusion: RCII is a valuable predictor of HF in patients with CAD and T2DM. Higher RCII levels are closely linked to an increased risk of HF.
Keywords: remnant cholesterol inflammatory index, coronary artery disease, type 2 diabetes mellitus, heart failure, machine learning
Background
Coronary artery disease (CAD) and type 2 diabetes mellitus (T2DM) are major global public health concerns, often coexisting and synergistically increasing the risk of adverse cardiovascular events and mortality.1–4 Epidemiological evidence indicates that individuals with T2DM have a significantly higher risk of developing CAD compared with the general population.5 Moreover, in patients with established CAD, concomitant diabetes not only accelerates atherosclerotic progression but also markedly raises the incidence of cardiovascular complications.6 In recent years, heart failure (HF) has emerged as one of the most frequent and severe outcomes in patients with coronary artery disease complicated by type 2 diabetes,7,8 characterized by poor prognosis, high readmission rates, and elevated mortality. Early identification of high-risk patients and accurate prediction of HF remain pressing clinical challenges.
Both dyslipidemia and chronic low-grade inflammation are recognized as key drivers of HF development.9–11 In particular, remnant cholesterol (RC) and low-density lipoprotein cholesterol (LDL-C) contribute to atherosclerosis and myocardial injury by promoting lipid accumulation, endothelial dysfunction, and plaque formation, thereby accelerating the progression from CAD to HF. Remnant cholesterol, a major component of non–high-density lipoprotein cholesterol, reflects the level of triglyceride-rich lipoprotein remnants and has been independently associated with atherosclerosis and cardiovascular events.12–14 Beyond traditional lipid measures, systemic inflammation has emerged as a novel marker for cardiovascular events, with high-sensitivity C-reactive protein (hsCRP) and other inflammatory indices providing additional prognostic information for HF onset and progression. High-sensitivity C-reactive protein, a classical biomarker of systemic inflammation, has also been linked to both the onset and progression of HF.15,16 Metabolic abnormalities and inflammatory activation may act synergistically, promoting myocardial injury and adverse remodeling, thereby substantially elevating HF risk.17,18
To capture these dual pathophysiological processes, the remnant cholesterol inflammatory index (RCII) has been proposed. This composite marker integrates lipid metabolism abnormalities and systemic inflammation, offering a more comprehensive assessment of cardiovascular risk. Prior studies have demonstrated strong associations between RCII and major cardiovascular or cerebrovascular events;19–21 however, its prognostic value for HF in patients with CAD and T2DM has not been systematically investigated. Notably, no prior studies have specifically validated RCII as a predictor of HF in CAD patients with T2DM, highlighting a clear knowledge gap that this study aims to address. The present study is the first to explore the predictive role of RCII for HF risk in this population and to evaluate its potential as an early, accessible, and cost-effective biomarker for clinical application.
Methods
Study Population
We retrospectively collected clinical data from patients who underwent first-time coronary angiography (CAG) at Minda Hospital of Hubei Minzu University between January 2021 and June 2025. CAD was defined as ≥70% stenosis in a non–left main coronary artery or ≥50% stenosis in the left main artery. As shown in Figure 1, patients without CAD, without T2DM, lacking high-sensitivity hsCRP measurements, or missing follow-up information were excluded. A total of 1181 patients met the eligibility criteria and were included in the analysis. All data were anonymized. The study was approved by the Ethics Committee of Minda Hospital of Hubei Minzu University. The requirement for informed consent was waived due to the use of de-identified retrospective data and the absence of any interventions. This study was conducted in accordance with the Declaration of Helsinki.
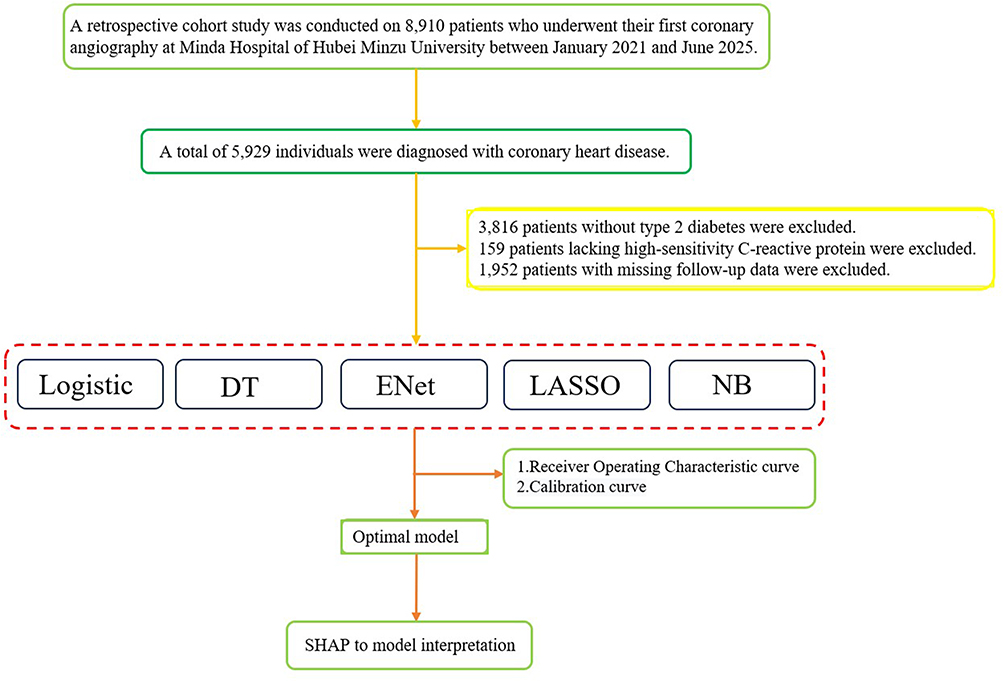 |
Figure 1 Flowchart of the Study Design. |
Data Collection
Clinical variables included demographic characteristics (sex, age), comorbidities (hypertension, hyperlipidemia, stroke, hyperuricemia, atrial fibrillation, smoking history), medication use (β-blockers, angiotensin receptor–neprilysin inhibitors, anticoagulants), and laboratory indices. Laboratory data covered hematologic parameters (white blood cell count [WBC], neutrophils [NEUT], lymphocytes [LYM], monocytes [MONO], hemoglobin [Hb], mean corpuscular volume [MCV], platelets), Lipid profile (total cholesterol[TC], triglycerides [TG], high-density lipoprotein cholesterol [HDL-C], and low-density lipoprotein cholesterol[LDL-C]), biochemical and renal markers (alanine aminotransferase [ALT], direct bilirubin [DBIL], albumin [ALB], creatinine [Cr], uric acid [UA], urea), thyroid function (thyroid-stimulating hormone [TSH]), and coagulation parameters (fibrinogen [FIB], D-dimer). RCII was calculated as remnant cholesterol multiplied by hsCRP, divided by 10.
Feature Selection
To identify the most relevant predictors, the Boruta algorithm was applied to all candidate variables. Boruta, based on the random forest framework, iteratively compares the importance of true features against randomized shadow features, thereby selecting stable and statistically significant predictors. The top-ranked features were retained, and an importance ranking plot was generated to illustrate their relative contributions to model construction.
Model Development and Evaluation
Five predictive models were established and compared: logistic regression (Logistic), decision tree (DT), elastic net regression (ENet), LASSO regression, and naïve Bayes (NB). The dataset was randomly split into a training set (70%) and a testing set (30%). Models were trained on the training set, with five-fold cross-validation performed to assess generalizability, and validated on the testing set. Discrimination was evaluated using receiver operating characteristic (ROC) curves and area under the curve (AUC). Calibration was assessed by calibration plots and Brier scores. In addition, accuracy, sensitivity, F1-score, positive predictive value (PPV), and negative predictive value (NPV) were calculated in both training and testing cohorts to compare overall performance.
Feature Importance and Interpretability
The best-performing model was further interpreted using SHapley Additive exPlanations (SHAP). Based on Shapley values from cooperative game theory, SHAP quantifies the marginal contribution of each feature across different combinations, thereby assessing its influence on model predictions. Both global and individual interpretability were evaluated, with mean absolute SHAP values used to identify the top five predictors. SHAP summary and dependence plots were generated to visualize feature importance, contribution direction, and consistency.
Statistical Analysis
Continuous variables with normal distribution were expressed as mean ± standard deviation (SD) and compared using independent-samples t tests. Non-normally distributed variables were presented as median (interquartile range, IQR) and compared using the Mann–Whitney U-test. Categorical variables were summarized as counts and percentages (n, %) and compared with χ2 or Fisher’s exact tests. All analyses were two-tailed, and a P value <0.05 was considered statistically significant. Data processing and analysis were conducted using Python 3.9 and R 4.3.2.
Results
Baseline Characteristics
As summarized in Table 1, among the 1181 patients included, 73 developed HF during follow-up. No significant differences were observed between the HF and non-HF groups in sex, age, use of β-blockers, angiotensin receptor–neprilysin inhibitors (ARNI), cerebrovascular disease, or anticoagulant therapy. In contrast, atrial fibrillation, smoking history, hypertension, hyperlipidemia, and hyperuricemia were all significantly more prevalent in the HF group. Patients who developed HF also demonstrated more pronounced inflammatory and hematologic abnormalities, with higher white blood cell and neutrophil counts, lower lymphocyte counts, and reductions in hemoglobin and albumin, suggesting anemia and poorer nutritional status. Renal function parameters, including creatinine and uric acid, differed significantly between groups. Notably, the median RCII was markedly elevated in the HF group compared with the non-HF group (7.14 vs 1.29, P < 0.001), indicating a heightened inflammatory burden. Coagulation indices also differed, with higher fibrinogen and D-dimer levels observed in HF patients.
 |
Table 1 Baseline Characteristics |
Feature Selection by Boruta Algorithm
Figure 2 ranks the predictive importance of candidate variables. The box plot on the left highlights the 13 variables most strongly associated with HF risk in CAD patients with T2DM, while the line plot on the right illustrates the stability of variable importance across 100 classifier iterations. The relatively small fluctuations suggest that the feature selection process was robust. These 13 predictors were retained for model construction.
 |
Figure 2 Boruta Analysis Identifying Key Predictor Variables. |
Model Comparison
We evaluated the performance of five machine learning models in both training and testing cohorts. As shown in Figure 3, all models achieved relatively high discrimination in the training set (AUC range 0.82–0.87). In the testing set, logistic regression yielded the highest AUC, demonstrating the strongest generalizability. Calibration curves (Figure 4) further indicated that logistic regression achieved the best calibration, with Brier scores of 0.0433 in the training set and 0.0368 in the testing set, reflecting close agreement between predicted probabilities and observed outcomes. LASSO and ENet showed moderate calibration, while DT and NB performed less favorably. Table 2 further confirmed the robust overall performance of logistic regression in the testing cohort. Cross-validation results are displayed in Figure 5, showing that, except for DT, all models achieved their best performance in Fold 5. Logistic regression reached ROC_AUC values approaching 0.98, highlighting their stability and generalizability. Taken together, logistic regression demonstrated superior discrimination and calibration across analyses.
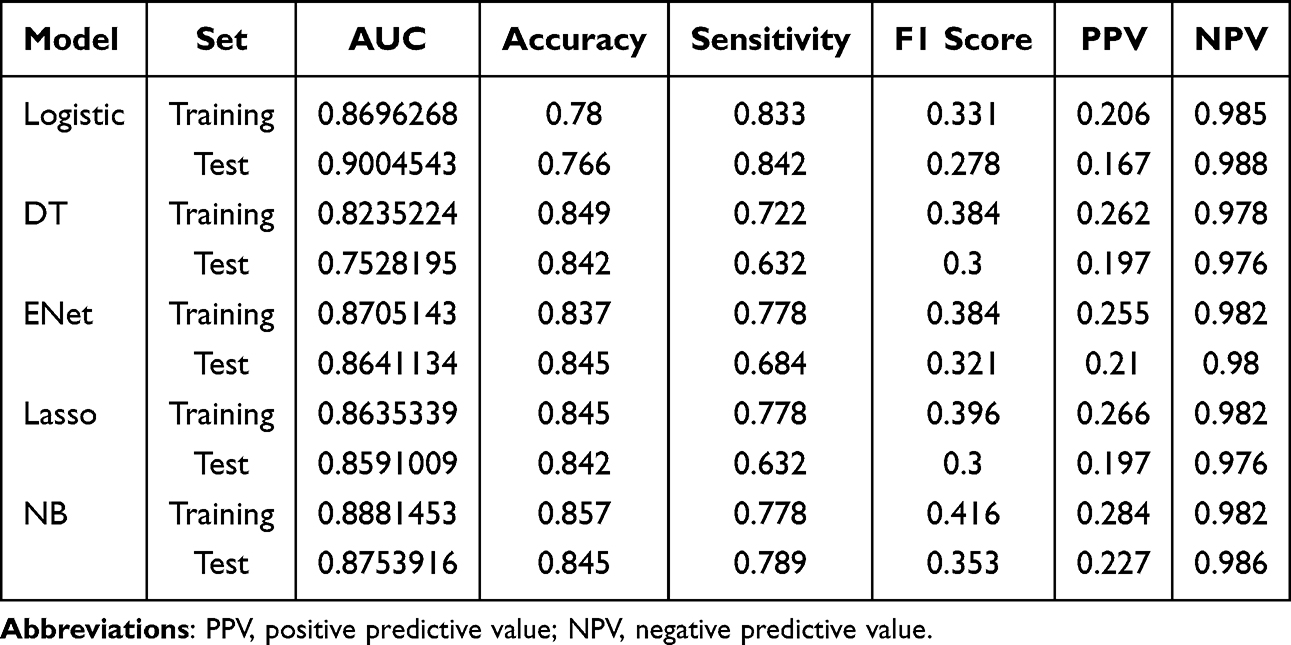 |
Table 2 The Comprehensive Evaluation of the Performance of Predictive Models |
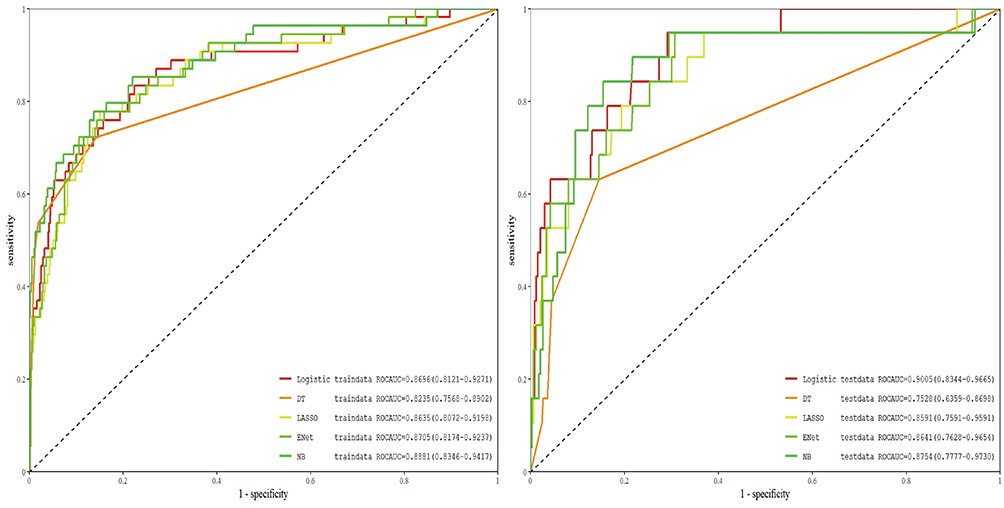 |
Figure 3 Receiver Operating Characteristic (ROC) Curves for Test and Validation Sets. |
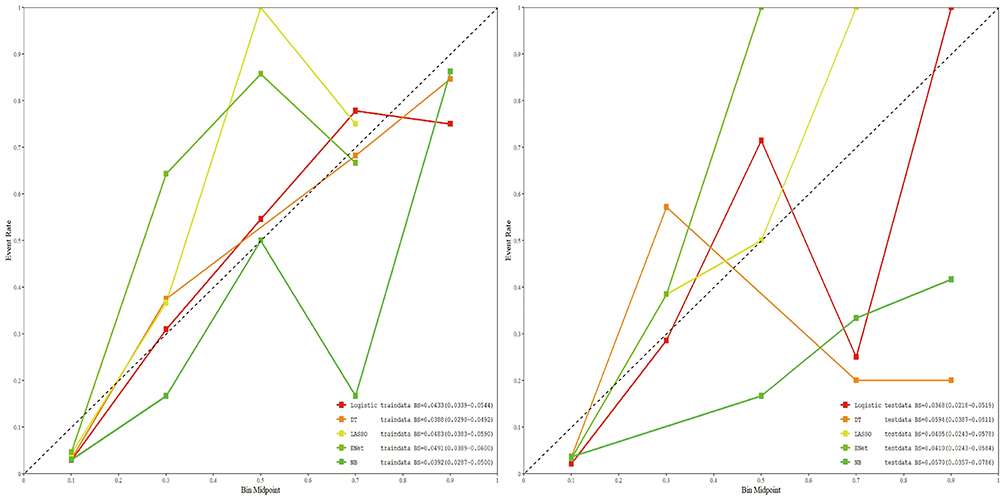 |
Figure 4 Calibration Curves for Test and Validation Sets. |
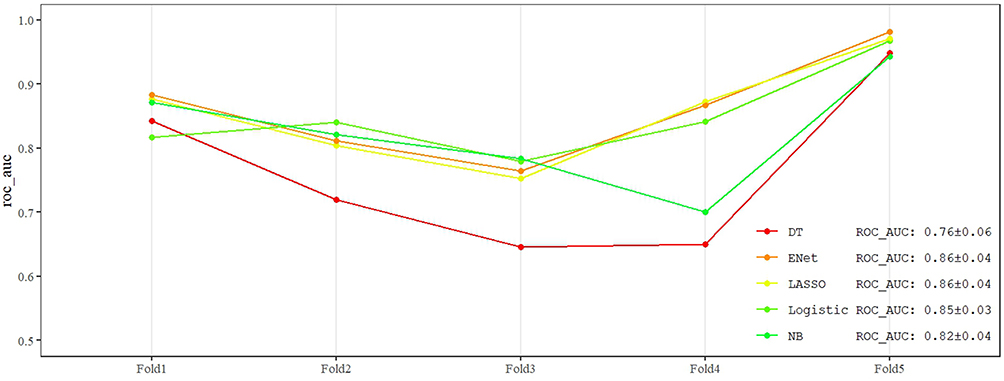 |
Figure 5 Comparison of ROC AUC for Five Machine Learning Models Across 5-Fold Cross-Validation. |
Interpretability of the Logistic Regression Model Using SHAP
As illustrated in Figure 6, SHAP analysis was applied to interpret the logistic regression model. The SHAP summary plot (Figure 6A) indicated that poor nutritional status (both low hemoglobin and low serum albumin), elevated RCII, and smoking were among the most influential factors driving HF occurrence. The mean absolute SHAP values (Figure 6B) ranked the relative importance of predictors, with RCII consistently the second-highest contributor. Dependence analysis (Figure 6C) showed a positive relationship between RCII and SHAP values, demonstrating that higher RCII levels were consistently associated with an increased predicted risk of HF.
 |
Figure 6 SHAP Analysis of Feature Importance. (A) Feature Attributes; (B) SHAP-Based Feature Importance Ranking; (C) SHAP Dependence Plot. |
Discussion
In the present study, RCII levels were markedly elevated in CAD patients with T2DM who developed HF compared with those who did not (7.14 vs 1.29). The presence of atrial fibrillation also increased the likelihood of HF onset. Using the Boruta algorithm, we identified 13 variables most strongly associated with HF risk in this population. Among the predictive models evaluated, logistic regression achieved the best overall performance in both training and testing cohorts, with superior accuracy and calibration, suggesting strong predictive capability for HF development. Model interpretability analysis with SHAP further revealed that poor nutritional status, elevated RCII, and smoking were major contributors to HF risk. The SHAP dependence plots highlighted a consistent positive relationship between RCII and model output, reinforcing its importance as a predictor.
Mechanistically, hs-CRP can activate endothelial cells, facilitate inflammatory cell infiltration into myocardial tissue, and promote myocardial fibrosis through NF-κB and TGF-β signaling.22,23 Additionally, hs-CRP induces oxidative stress and cardiomyocyte apoptosis, impairing contractile function.24 RC, a triglyceride-rich lipoprotein particle, can penetrate the vascular endothelium and deposit in the arterial wall, triggering localized inflammation and atherosclerosis. Beyond endothelial injury and ischemia,25 RC activates inflammatory mediators further contributing to myocardial remodeling and fibrosis.26 The combined effect of RC and hs-CRP may be particularly detrimental, with stronger predictive value for cardiovascular events than either marker alone.27,28 Elevated RC together with low-grade inflammation may act synergistically to substantially increase the risk of adverse outcomes.29
Malnutrition is common among HF patients and strongly linked to poor prognosis.30,31 Elevated hs-CRP levels have been consistently associated with HF onset and progression, even in patients with well-controlled LDL-C,32 highlighting inflammation as an independent driver of cardiovascular risk. Notably, most prior studies linking hsCRP to HF focus on HFpEF, emphasizing the broader relevance of inflammatory biomarkers across HF phenotypes. Smoking remains a major modifiable risk factor, with long-term smokers exhibiting nearly double the risk of HF compared with non-smokers;33 this excess risk may persist even years after cessation. Other inflammatory indices, such as the CRP/albumin ratio and systemic immune-inflammation index, have also been associated with HF risk, although RCII may provide a more integrated measure of lipid-driven inflammation. Additionally, dyslipidemia plays a critical role not only in coronary disease but also in carotid plaque instability and related cerebrovascular events,34 suggesting that RCII could have broader vascular implications beyond the coronary circulation. These findings align with our results, reinforcing the reliability of our conclusions. Notably, the prediction model developed in this study achieved AUCs ranging from 0.75 to 0.90 across both training and testing sets, outperforming previously reported models. The improved discrimination suggests that integrating RCII into risk calculators or follow-up protocols could help identify high-risk CAD/T2DM patients earlier and guide individualized preventive strategies. It is important to note that RCII should currently be considered a correlative biomarker rather than a confirmed causal factor, reflecting the combined effect of lipid abnormalities and inflammation on HF risk.
Nevertheless, several limitations warrant consideration. First, this was a single-center retrospective study with a relatively limited sample size, restricting the generalizability of our findings. Second, certain potential predictors, such as cardiac imaging parameters and natriuretic peptides (eg, BNP), were not included, which may limit the comprehensiveness of the model. Future research should validate our findings in larger, multicenter cohorts with longer follow-up and integrate additional HF-specific biomarkers to further refine model accuracy and enhance clinical utility.
Looking forward, translating this predictive model into clinical practice will require prospective multicenter validation and integration with electronic health records. Developing a user-friendly decision support interface and establishing clear clinical pathways for high-risk patients are essential steps. Such efforts could move this work beyond retrospective analysis toward practical risk stratification and evidence-based interventions, ultimately enhancing patient care and informing policy or risk management decisions.
Conclusions
Elevated RCII is closely associated with increased HF risk in CAD patients with T2DM. Logistic regression models incorporating RCII demonstrated strong predictive performance, with poor nutritional status, RCII, and smoking identified as key contributors. RCII may serve as a practical biomarker for early risk stratification, supporting targeted prevention and follow-up in high-risk patients.
Acknowledgments
ChatGPT provided assistance in sentence editing. The authors reviewed and edited the content as needed and take full responsibility for the scientific content of this manuscript.
Funding
This work was supported by the Natural Science Foundation of Hubei Province (No. JCZRYB202501509).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Frąk W, Wojtasińska A, Lisińska W, Młynarska E, Franczyk B, Rysz J. Pathophysiology of cardiovascular diseases: new insights into molecular mechanisms of atherosclerosis, arterial hypertension, and coronary artery disease. Biomedicines. 2022;10(8):1938. doi:10.3390/biomedicines10081938
2. Barrea L, Verde L, Colao A, Mandarino LJ, Muscogiuri G. Medical nutrition therapy for the management of type 2 diabetes mellitus. Nat Rev Endocrinol. 2025;21(12):769–782. doi:10.1038/s41574-025-01161-5
3. Yankah RK, Anku EK, Eligar V. Sodium-glucose cotransporter-2 inhibitors and cardiovascular protection among patients with type 2 diabetes mellitus: a systematic review. J Diabetes Res. 2024;2024:9985836. doi:10.1155/2024/9985836
4. Król M, Kupnicka P, Żychowska J, et al. Molecular insights into the potential cardiometabolic effects of GLP-1 receptor analogs and DPP-4 inhibitors. Int J Mol Sci. 2025;26(14):6777. doi:10.3390/ijms26146777
5. Docimo A, Verde L, Barrea L, et al. Type 2 diabetes: also a “Clock Matter”? Nutrients. 2023;15(6):1427. doi:10.3390/nu15061427
6. Karakasis P, Patoulias D, Kassimis G, et al. Therapeutic potential of sodium-glucose Co-transporter-2 inhibitors and glucagon-like Peptide-1 receptor agonists for patients with acute coronary syndrome: a review of clinical evidence. Curr Pharm Des. 2024;30(27):2109–2119. doi:10.2174/0113816128304097240529053538
7. Gonzalez-Manzanares R, Anguita-Gámez M, Muñiz J, et al. Prevalence and incidence of heart failure in type 2 diabetes patients: results from a nationwide prospective cohort-the DIABET-IC study. Cardiovasc Diabetol. 2024;23(1):253. doi:10.1186/s12933-024-02358-0
8. Thomas MC. Type 2 diabetes and heart failure: challenges and solutions. Curr Cardiol Rev. 2016;12(3):249–255. doi:10.2174/1573403x12666160606120254
9. Şahin A, Çöllüoğlu T, Çelik A, et al. Exploring regional disparities in heart failure epidemiology and outcomes: a comprehensive study across geographical regions in Türkiye. Balkan Med J. 2024;41(1):47–53. doi:10.4274/balkanmedj.galenos.2023.2023-10-5
10. Ozkan B, Ndumele CE. Exploring the mechanistic link between obesity and heart failure. Curr Diab Rep. 2023;23(12):347–360. doi:10.1007/s11892-023-01526-y
11. Kostin S, Krizanic F, Kelesidis T, Pagonas N. The role of NETosis in heart failure. Heart Fail Rev. 2024;29(5):1097–1106. doi:10.1007/s10741-024-10421-x
12. Burnett JR, Hooper AJ, Hegele RA. Remnant cholesterol and atherosclerotic cardiovascular disease risk. J Am Coll Cardiol. 2020;76(23):2736–2739. doi:10.1016/j.jacc.2020.10.029
13. Sandesara PB, Virani SS, Fazio S, Shapiro MD. The forgotten lipids: triglycerides, remnant cholesterol, and atherosclerotic cardiovascular disease risk. Endocr Rev. 2019;40(2):537–557. doi:10.1210/er.2018-00184
14. Cummings BB, Joing MP, Bouchard PR, et al. Safety and efficacy of a novel ANGPTL4 inhibitory antibody for lipid lowering: results from Phase 1 and phase 1b/2a clinical studies. Lancet. 2025;405(10493):1923–1934. doi:10.1016/s0140-6736(25)00825-6
15. Moissl AP, Delgado GE, Scharnagl H, et al. Comparing inflammatory biomarkers in cardiovascular disease: insights from the LURIC Study. Int J Mol Sci. 2025;26(15):7335. doi:10.3390/ijms26157335
16. Pan Y, Fan F, Jiang J, Zhang Y. Clinical outcomes of anti-inflammatory therapies inhibiting the NLRP3/IL-1β/IL-6/CRP pathway in coronary artery disease patients: a systemic review and meta-analysis of 37,056 individuals from 32 randomized trials. Inflamm Res. 2025;74(1):99. doi:10.1007/s00011-025-02058-9
17. Castillo RL, Farías J, Sandoval C, et al. Role of NLRP3 inflammasome in heart failure patients undergoing cardiac surgery as a potential determinant of postoperative atrial fibrillation and remodeling: is SGLT2 cotransporter inhibition an alternative for cardioprotection? Antioxidants. 2024;13(11):1388. doi:10.3390/antiox13111388
18. Yang R, Pang J, Zhong X, et al. Molecular mechanisms of aberrant fatty acids metabolism in driving cardiovascular diseases: key regulatory targets and dietary interventions. Food Funct. 2025;16(15):5961–5993. doi:10.1039/d5fo01237f
19. Yu Y, Zhang Y, Zhu C, Duan T, Rao Z. Remnant cholesterol inflammatory index, calculated from residual cholesterol to C-reactive protein ratio, and stroke outcomes: a retrospective study using the National institutes of health stroke scale and modified Rankin scale. Lipids Health Dis. 2025;24(1):228. doi:10.1186/s12944-025-02650-2
20. Wang Y, Bi L, Li Q, Wang Q, Lv T, Zhang P. Remnant cholesterol inflammatory index and its association with all-cause and cause-specific mortality in middle-aged and elderly populations: evidence from US and Chinese national population surveys. Lipids Health Dis. 2025;24(1):155. doi:10.1186/s12944-025-02580-z
21. Chen J, Wu Q, Liu H, et al. Predictive value of remnant cholesterol inflammatory index for stroke risk: evidence from the China health and Retirement Longitudinal study. J Adv Res. 2024;76:543–552. doi:10.1016/j.jare.2024.12.015
22. Amara M, Stoler O, Birati EY. The role of inflammation in the pathophysiology of heart failure. Cells. 2025;14(14):1117. doi:10.3390/cells14141117
23. Sun W, Wu Y, Gao M, et al. C-reactive protein promotes inflammation through TLR4/NF-κB/TGF-β pathway in HL-1 cells. Biosci Rep. 2019;39(8):BSR20190888. doi:10.1042/bsr20190888
24. Rees K, Hartley L, Day C, Flowers N, Clarke A, Stranges S. Selenium supplementation for the primary prevention of cardiovascular disease. Cochrane Database Syst Rev. 2013;2013(1):CD009671. doi:10.1002/14651858.cd009671.pub2
25. Duran EK, Aday AW, Cook NR, Buring JE, Ridker PM, Pradhan AD. Triglyceride-rich lipoprotein cholesterol, small dense LDL cholesterol, and incident cardiovascular disease. J Am Coll Cardiol. 2020;75(17):2122–2135. doi:10.1016/j.jacc.2020.02.059
26. Pintó X, Fanlo M, Esteve V, Millán J. Colesterol remanente, riesgo vascular y prevención de la arteriosclerosis [Remnant cholesterol, vascular risk, and prevention of atherosclerosis]. Clin Investig Arterioscler. 2023;35(4):206–217. doi:10.1016/j.arteri.2023.02.001
27. Hou L, Su K, He T, Zhao J, Li Y. Prediction model for in-stent restenosis post-PCI based on boruta algorithm and deep learning: the role of blood cholesterol and lymphocyte ratio. J Multidiscip Healthc. 2024;17:4731–4739. doi:10.2147/jmdh.S487511
28. Elías-López D, Doi T, Nordestgaard BG, Kobylecki CJ. Remnant cholesterol and low-grade inflammation jointly in atherosclerotic cardiovascular disease: implications for clinical trials. Curr Opin Clin Nutr Metab Care. 2024;27(2):125–135. doi:10.1097/mco.0000000000000999
29. Li J, Yan K, Zhu P, et al. Association between multiple inflammatory biomarkers and remnant cholesterol levels in patients with percutaneous coronary intervention: a large-scale real-world study. Nutr Metab Cardiovasc Dis. 2024;34(2):377–386. doi:10.1016/j.numecd.2023.09.006
30. Huang T, An Z, Huang Z, Gao W, Hao B, Xu J. Serum albumin and cardiovascular disease: a Mendelian randomization study. BMC Cardiovasc Disord. 2024;24(1):196. doi:10.1186/s12872-024-03873-4
31. Su G, Xiao R, Ji D, et al. Diagnostic work-up of anemia and associated health outcomes in people with heart failure. BMC Med. 2025;23(1):471. doi:10.1186/s12916-025-04303-8
32. Peikert A, Kaier K, Merz J, et al. Residual inflammatory risk in coronary heart disease: incidence of elevated high-sensitive CRP in a real-world cohort. Clin Res Cardiol. 2020;109(3):315–323. doi:10.1007/s00392-019-01511-0
33. Chelikam N, Vyas V, Dondapati L, et al. Epidemiology, burden, and association of substance abuse amongst patients with cardiovascular disorders: national cross-sectional survey study. Cureus. 2022;14(7):e27016. doi:10.7759/cureus.27016
34. Servadei F, Scimeca M, Palumbo V, et al. Aging and sex modify the risk of carotid plaque thrombosis related to dyslipidemic profile. Stroke. 2025;56(10):2879–2887. doi:10.1161/strokeaha.125.051754
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Predictive Value of Noninvasive Peripheral Atherosclerosis Measurement for Coronary Artery Disease in Patients with Long T2DM Duration
Chen W, Wang L, Hu B, Zheng Y, Zhang S, Zhou Z, Mai Y
Diabetes, Metabolic Syndrome and Obesity 2023, 16:1075-1083
Published Date: 18 April 2023
Development of Machine Learning Models for Predicting Osteoporosis in Patients with Type 2 Diabetes Mellitus—A Preliminary Study
Wu X, Zhai F, Chang A, Wei J, Guo Y, Zhang J
Diabetes, Metabolic Syndrome and Obesity 2023, 16:1987-2003
Published Date: 30 June 2023
Identification of Shared Immune Cells and Immune-Related Co-Disease Genes in Chronic Heart Failure and Systemic Lupus Erythematosus Based on Transcriptome Sequencing

Luo Z, Lu G, Yang Q, Ding J, Wang T, Hu P
Journal of Inflammation Research 2023, 16:2689-2705
Published Date: 30 June 2023
Resistance Training in Cardiovascular Diseases: A Review on Its Effectiveness in Controlling Risk Factors
Nazir A, Heryaman H, Juli C, Ugusman A, Martha JW, Moeliono MA, Atik N
Integrated Blood Pressure Control 2024, 17:21-37
Published Date: 18 March 2024
Development and External Validation of a Machine Learning-Based Model for Predicting Heart Failure Risk in Type 2 Diabetes
Liu Y, Wang P, Wang M, Chen Y, Kasyanju SM, Yang Y, Yang T, Peng L, Sun M
Diabetes, Metabolic Syndrome and Obesity 2025, 18:4177-4191
Published Date: 13 November 2025