Back to Journals » OncoTargets and Therapy » Volume 18
Redefining Therapeutic Boundaries: PD-1 Blockade Facilitates Surgical Cure in EGFR-TKI Refractory EGFR-Mutant NSCLC with Pleural Metastases
Authors Niu YL, Teng XB, Han MF, Ma J ![]()
Received 27 June 2025
Accepted for publication 5 November 2025
Published 11 November 2025 Volume 2025:18 Pages 1259—1264
DOI https://doi.org/10.2147/OTT.S549874
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Sanjay Singh
Yong-Liang Niu,1,* Xiao-Bao Teng,1,* Ming-Feng Han,1,* Jie Ma2
1Department of Respiratory and Critical Care Medicine, No. 2 People’s Hospital of Fuyang City, Fuyang, Anhui, 236000, People’s Republic of China; 2Department of Thoracic Surgery, Anhui Chest Hospital, Hefei, 230022, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jie Ma, Department of Thoracic Surgery, Anhui Chest Hospital, Hefei, 230022, People’s Republic of China, Email [email protected]
Abstract: We present a 57-year-old female diagnosed with stage cT3N1M1a (IVA) EGFR L858R-mutant lung adenocarcinoma (PD-L1 TPS 60%). The patient attained sustained disease control with a partial response lasting 22 months on first-line gefitinib. Following progression with persistent EGFR L858R mutation, second-line platinum-pemetrexed-bevacizumab chemotherapy achieved stable disease (SD) in the primary lesion and shrinkage of pleural nodules. Subsequent neoadjuvant therapy with albumin-bound paclitaxel, carboplatin, bevacizumab, and sintilimab induced marked tumor regression, permitting curative-intent R0 resection. Histopathological analysis confirmed ypT0N0, indicating a pathological complete response (pCR). The patient remained recurrence-free 25 months post-surgery. This case illustrates the potential of immunotherapy-based neoadjuvant regimens to convert unresectable PD-L1–high EGFR-mutant lung adenocarcinoma into operable disease and achieve durable pCR.
Keywords: EGFR-mutant lung adenocarcinoma, pathological complete response, immunotherapy conversion, sintilimab, neoadjuvant therapy
Introduction
The management of locally advanced non–small cell lung cancer (NSCLC) with pleural involvement presents considerable therapeutic challenges. The introduction of immune checkpoint inhibitors (ICIs) combined with chemotherapy has transformed the neoadjuvant treatment landscape for resectable NSCLC, achieving pathological complete response (pCR) rates ranging from 24% to 37% in pivotal trials such as CheckMate 816 and NADIM II.1,2 However, these regimens show limited efficacy in EGFR-mutant tumors, which exhibit inherent primary resistance to PD-1/PD-L1 inhibition, with response rates below 5%.3 Furthermore, the presence of pleural metastases has traditionally been considered a contraindication to surgical resection. Conversion therapy for initially unresectable disease remains particularly challenging, with pCR rates below 5% even in stage IV NSCLC. Here, we report a rare case in which a pCR was attained through a multimodal strategy incorporating an anti–PD-1 antibody after a suboptimal response to EGFR-TKIs and chemotherapy.
Case Presentation
A 57-year-old non-smoking female presented with a 6.6 cm spiculated mass in the right lower lobe, identified on a chest computed tomography (CT) scan performed in October 2020. The mass exhibited malignant characteristics such as lobulation, pleural indentation, and mediastinal lymph node enlargement. Metastatic pleural nodules are indicated by arrows (Figure 1A–B), and the primary lesion in the right lower lobe is shown in Figure 1C–D. A CT-guided biopsy confirmed the diagnosis of moderately differentiated lung adenocarcinoma with an EGFR exon 21 L858R mutation. PD-L1 expression was heterogeneous, with tumor proportion scores (TPS) of 60% (22C3 assay) and 30% (E1L3N assay). Staging identified pleural nodules (cM1a), classifying the disease as stage IVA.
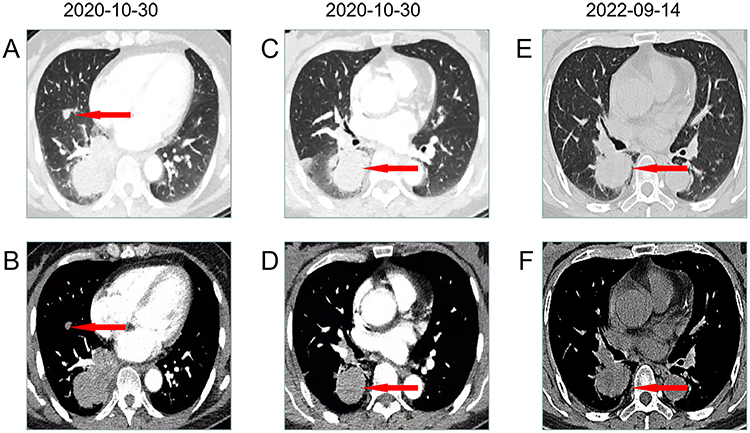 |
Figure 1 Chest CT imaging features of malignant pulmonary mass. (A and B) Axial and coronal views demonstrating metastatic pleural nodules (red arrows). (C and D) Primary lesion in the right lower lobe (red arrows). (E and F) Representative CT images demonstrating progressive disease (PD) of the primary lung mass after 22 months of gefitinib therapy. Red arrows indicate progression of the primary lesion. |
Phase 1: Targeted Therapy
First-line treatment with gefitinib (250 mg/day) was initiated, achieving disease control for 22 months. However, plasma genotyping in July 2022 confirmed persistence of the EGFR L858R mutation (0.1% variant allele frequency, VAF) and emergence of a GNAS R201C mutation (0.2% VAF). Serial CT imaging at 22 months after starting gefitinib revealed disease progression (PD) in the primary lung mass, marked by an increase in lesion size (red arrows, Figure 1E–F), prompting a change in treatment.
Phase 2: Chemoimmunotherapy Conversion
The patient received four cycles of chemotherapy with pemetrexed, carboplatin, and bevacizumab, resulting in stable disease (SD). A PET-CT scan in March 2023 showed metabolic activity in the primary tumor, with a maximum standardized uptake value (SUVmax) of 15.3, and no hypermetabolic lymph nodes. The tumor measured approximately 5.2×3.9 cm (red arrow, Figure 2A–B). The patient then received conversion therapy with nab-paclitaxel (260 mg/m2), carboplatin (AUC 5), bevacizumab (15 mg/kg), and sintilimab (200 mg). Follow-up imaging four weeks later revealed marked shrinkage of the target lung lesion (red arrow, Figure 2C–D), downstaging the disease to a potentially resectable status.
 |
Figure 2 (A and B) PET-CT following 4 cycles of pemetrexed/carboplatin/bevacizumab: Primary tumor (red arrow, 5.2×3.9 cm). (C and D) Post-cycle 1 CT after quadruplet therapy (sintilimab 200 mg, nab-paclitaxel 260 mg/m2, carboplatin AUC 5, bevacizumab 15 mg/kg) demonstrating significant shrinkage of the target lung lesion (red arrow). (E and F) Follow-up chest CT images (>2 years post-operatively, without adjuvant treatment) showing no evidence of recurrence. Abbreviations: SD, stable disease; PD, progressive disease. |
Phase 3: Surgical Intervention & Outcome
In April 2023, the patient underwent muscle-sparing thoracotomy with right lower lobectomy and systematic mediastinal lymph node dissection. Histopathological examination of the resected specimen showed no residual viable tumor cells (ypT0N0), indicating a pathological complete response (pCR). A chest CT scan 25 months post-surgery showed no recurrence (Figure 2E–F), with no adjuvant therapy administered during this period. The initial right pleural metastatic nodule (Figure 3A, red arrow) showed no significant response after 22 months of gefitinib (Figure 3B, red arrow). However, it exhibited pronounced shrinkage after four cycles of chemotherapy combined with anti-angiogenic therapy (Figure 3C, red arrow). After subsequent immunotherapy, the nodule remained stable without further significant change (Figure 3D, red arrow).
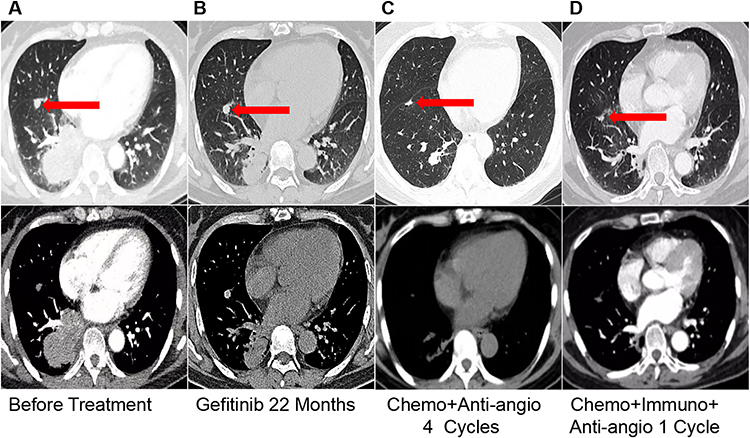 |
Figure 3 Evolution of pleural metastatic nodules: initial nodule (A) as indicated by the red arrow. After 22 months of gefitinib therapy (B), (red arrow); after four cycles of chemotherapy+anti-angiogenic therapy (C), (red arrow);After one cycle of immunotherapy+chemotherapy+anti-angiogenic therapy (D), (red arrow). |
Discussion
Emerging evidence from recent case reports indicates that patients with traditionally unresectable stage IIIB NSCLC, who harbor both high PD-L1 expression and specific driver mutations, may derive considerable benefit from combined targeted therapy and immunotherapy. Such regimens have enabled tumor downstaging, successful R0 resection, and pCR. In one report by Zhang et al, a patient with an ERBB2 mutation achieved surgical conversion and pCR following treatment with T-DXd plus a PD-1 inhibitor.4 Similarly, Cheng et al documented pCR in a case with a BRAF V600E mutation using neoadjuvant dabrafenib and trametinib combined with a PD-1 inhibitor.5 In contrast, the present case involves stage IV NSCLC, initially characterized by an EGFR mutation and high PD-L1 expression, which, after multiple lines of therapy, underwent successful conversion therapy, R0 resection, and attained pCR. This outcome is particularly remarkable in advanced driver-mutant lung cancer and offers valuable clinical insights for managing similarly challenging cases.
Although high PD-L1 expression (≥50%) in EGFR-mutant NSCLC is typically associated with poor prognosis and primary resistance to TKIs,6 the patient described in this report, who had high PD-L1 expression and an EGFR mutation, initially exhibited a favorable response to EGFR-TKIs. However, as discussed in a previous review,7 the tumor immune microenvironment (TIME) in EGFR-mutant lung cancer following targeted therapy is often characterized by an immunosuppressive state. This includes the enrichment of regulatory T cells (Tregs), functional exhaustion of cytotoxic T cells, and polarization of tumor-associated macrophages (TAMs) toward a pro-tumor M2 phenotype. These factors contribute to an “immune-excluded” or “immune-desert” type of “cold” tumor microenvironment, where the immune system fails to effectively recognize and eliminate resistant tumor clones that eventually emerge, leading to disease progression. The poor response of the pleural nodules further suggests that metastatic niches may reside within a more profoundly immunosuppressive ecological milieu. After developing resistance to targeted therapy, the patient received four cycles of pemetrexed-carboplatin-bevacizumab, which resulted in shrinkage of the pleural nodules but no significant reduction of the primary lesion. However, due to severe gastrointestinal adverse effects attributed to pemetrexed intolerance, the regimen was adjusted. We transitioned to a sintilimab-based quadruple regimen, replacing pemetrexed with nab-paclitaxel. This decision was based on several considerations: the family’s strong preference to continue therapy, evidence supporting the efficacy and safety of nab-paclitaxel/carboplatin/bevacizumab,8,9 and findings from trials such as IMpower13010 and ORIENT-31,11 Crucially, nab-paclitaxel is a more rational partner for immunotherapy. Unlike pemetrexed or solvent-based paclitaxel, it does not require routine steroid premedication, thereby avoiding potential immunosuppression. Moreover, nab-paclitaxel has demonstrated superior immunomodulatory effects and, due to its unique formulation, achieves higher intratumoral drug concentrations.12,13
The remarkable success of this subsequent combination regimen hinges on its synergistic remodeling of the previously immunosuppressive TIME, as outlined in a prior review:7 1. The “Priming” Effect of Chemotherapy: Platinum-based agents and nab-paclitaxel induce immunogenic cell death, releasing tumor antigens and damage-associated molecular patterns (DAMPs). This process effectively “sounds the alarm” for the immune system. Concurrently, chemotherapy selectively depletes immunosuppressive Tregs, thereby “creating space” for effector T cells to function optimally. 2.The “Pathway” Effect of Anti-angiogenesis: Bevacizumab, by inhibiting VEGF, promotes the “normalization” of disordered tumor vasculature. This enhances intratumoral blood perfusion, alleviates hypoxia, reduces immunosuppression, and facilitates the infiltration and activation of cytotoxic T cells within the tumor core.3. The “Releasing” Effect of Immune Checkpoint Inhibitors: Building upon the successful “preparation of the battlefield” and “opening of pathways” achieved in prior steps, sintilimab (a PD-1 inhibitor) releases the “brakes” (PD-1/PD-L1 signaling) on infiltrating T cells. This reinvigoration restores their potent tumor-killing function, ultimately leading to a pathologically confirmed complete response.
This remarkable outcome is supported by several factors:1. Synergy of Anti-angiogenesis and Immunotherapy: Bevacizumab simultaneously inhibits angiogenesis and enhances the durability of the immune response,14 promoting sustained effector T-cell activity. This mitigates immune evasion and extends therapeutic efficacy. The Phase III ATTLAS trial, where the same ABCP regimen significantly improved progression-free survival (PFS) in EGFR/ALK-positive NSCLC with a profound benefit in high PD-L1 expressors (HR 0.24),15 underscores this potential. 2.Favorable Biomarker Profile: The patient’s high PD-L1 expression (TPS >50%) is a recognized predictor of immune checkpoint inhibitor (ICI) efficacy, as demonstrated in the CheckMate 77T trial where perioperative nivolumab significantly improved event-free survival (EFS) in PD-L1-positive patients (HR 0.52).16 3.Aggressive Surgical Intervention and pCR: Postoperative pathology confirmed pCR, which is associated with excellent long-term outcomes. In the CheckMate 816 trial, pCR was linked to improved EFS.1 No adjuvant therapy was administered post-surgery, and the patient has remained recurrence-free throughout an extended follow-up period of 25 months.
In conclusion, for patients with stage IV lung adenocarcinoma harboring EGFR mutations and high PD-L1 expression accompanied by pleural metastases, a multimodal approach that incorporates sequential targeted therapy, immune checkpoint inhibition in conjunction with chemotherapy, and anti-angiogenic treatment can result in a pCR. Subsequent surgical intervention may facilitate long-term disease-free survival, providing a successful and instructive model for patients with similar profiles. This treatment trajectory, which deviates from the current therapeutic paradigm, warrants in-depth consideration and further investigation.
Ethical Approval
The ethics Statement was not applicable for case reports according to the No.2 People’s Hospital of Fuyang City; however, informed consent was obtained from the patient. This study was conducted in accordance with the principles of the Declaration of Helsinki.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Forde PM, Spicer J, Lu S, et al. Neoadjuvant nivolumab plus chemotherapy in resectable lung cancer. New Engl J Med. 2022;386(21):1973–1985. doi:10.1056/NEJMoa2202170
2. Provencio M, Nadal E, González-Larriba JL, et al. Perioperative nivolumab and chemotherapy in stage III non-small-cell lung cancer. New Engl J Med. 2023;389(6):504–513.
3. Gainor JF, Shaw AT, Sequist LV, et al. EGFR mutations and ALK rearrangements are associated with low response rates to PD-1 pathway blockade in non-small cell lung cancer: a retrospective analysis. Clin Cancer Res. 2016;22(18):4585–4593. doi:10.1158/1078-0432.CCR-15-3101
4. Zhang R, Cheng S, Sun K, Zhang L, Yan X, Yang F. Case report: a R0 resection successfully induced by T-DXd plus PD-1 inhibitor regimen in a primary unresectable stage IIIB NSCLC with ERBB2-mutation. NPJ Precision Oncology. 2025;9(1):169. doi:10.1038/s41698-025-00982-x
5. Cheng S, Zhang R, Yang F, et al. Induction therapy with dabrafenib, trametinib, and PD-1 inhibitor and surgical conversion in unresectable stage III non-small cell lung cancers with BRAF V600E mutation: 2 cases. Lung Cancer. 2025;205:108592. doi:10.1016/j.lungcan.2025.108592
6. Liu J, Itchins M, Nagrial A, et al. Relationship between PD-L1 expression and outcome in EGFR-mutant lung cancer patients treated with EGFR tyrosine kinase inhibitors. Lung Cancer. 2021;155:28–33. doi:10.1016/j.lungcan.2021.03.004
7. Wan Y, Li G, Cui G, Duan S, Chang S. Reprogramming of thyroid cancer metabolism: from mechanism to therapeutic strategy. Mol Cancer. 2025;24(1):74.
8. Reynolds C, Barrera D, Jotte R, et al. Phase II trial of nanoparticle albumin-bound paclitaxel, carboplatin, and bevacizumab in first-line patients with advanced nonsquamous non-small cell lung cancer. J Thorac Oncol. 2009;4(12):1537–1543.
9. Heist RS, Duda DG, Sahani DV, et al. Improved tumor vascularization after anti-VEGF therapy with carboplatin and nab-paclitaxel associates with survival in lung cancer. Proc Natl Acad Sci USA. 2015;112(5):1547–1552.
10. West H, McCleod M, Hussein M, et al. Atezolizumab in combination with carboplatin plus nab-paclitaxel chemotherapy compared with chemotherapy alone as first-line treatment for metastatic non-squamous non-small-cell lung cancer (IMpower130): a multicentre, randomised, open-label, phase 3 trial. Lancet Oncol. 2019;20(7):924–937. doi:10.1016/S1470-2045(19)30167-6
11. Lu S, Wu L, Jian H, et al. Sintilimab plus chemotherapy for patients with EGFR-mutated non-squamous non-small-cell lung cancer with disease progression after EGFR tyrosine-kinase inhibitor therapy (ORIENT-31): second interim analysis from a double-blind, randomised, placebo-controlled, phase 3 trial. Lancet Respir Med. 2023;11(7):624–636.
12. Socinski MA, Jotte RM, Cappuzzo F, et al. Association of immune-related adverse events with efficacy of atezolizumab in patients with non-small cell lung cancer: pooled analyses of the phase 3 IMpower130, IMpower132, and IMpower150 randomized clinical trials. JAMA Oncol. 2023;9(4):527–535. doi:10.1001/jamaoncol.2022.7711
13. Desai N, Trieu V, Yao Z, et al. Increased antitumor activity, intratumor paclitaxel concentrations, and endothelial cell transport of cremophor-free, albumin-bound paclitaxel, ABI-007, compared with cremophor-based paclitaxel. Clin Cancer Res. 2006;12(4):1317–1324. doi:10.1158/1078-0432.CCR-05-1634
14. Socinski MA, Jotte RM, Cappuzzo F, et al. Atezolizumab for first-line treatment of metastatic nonsquamous NSCLC. New Engl J Med. 2018;378(24):2288–2301. doi:10.1056/NEJMoa1716948
15. Park S, Kim TM, Han JY, et al. Phase III, randomized study of atezolizumab plus bevacizumab and chemotherapy in patients with EGFR- or ALK-mutated non-small-cell lung cancer (ATTLAS, KCSG-LU19-04). J Clin Oncol. 2024;42(11):1241–1251. doi:10.1200/JCO.23.01891
16. Cascone T, Awad MM, Spicer JD, et al. Perioperative nivolumab in resectable lung cancer. New Engl J Med. 2024;390(19):1756–1769. doi:10.1056/NEJMoa2311926
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Case of Complete Remission in Proficient Mismatch Repair (pMMR) Advanced Colon Cancer Treated with Sintilimab and XELOX
Zhu J, Li G, Zhang Z, Wang Y
ImmunoTargets and Therapy 2023, 12:17-23
Published Date: 19 February 2023
Efficacy and Safety of Neoadjuvant Stereotactic Body Radiotherapy (SBRT) Combined with Chemoimmunotherapy in Locally Advanced Breast Cancer: A Single-Center, Retrospective Pilot Study
Zhai M, Bi J, Ke Z, Hu M, Pi G, Li Y, He H, Li Y, Zheng H, Wu X, Verma V, Shao J, Han G
Breast Cancer: Targets and Therapy 2026, 18:577469
Published Date: 7 March 2026
Inflammatory and Nutritional Biomarkers Predict Response to Neoadjuvant Dual Anti-HER2 Therapy in HER2-Positive Breast Cancer: A Retrospective Cohort Study
Şahinli H, Uyar GC, Yeşilbaş E
Cancer Management and Research 2026, 18:598948
Published Date: 16 April 2026
A Structured Classification of Pyrotinib-Containing Neoadjuvant Regimens for HER2-Positive Breast Cancer: Efficacy, Safety, and Regimen Selection
Liu J, Peng X, Yang Y, Huang X, Du Y, Liu K
Breast Cancer: Targets and Therapy 2026, 18:600575
Published Date: 20 May 2026