Back to Journals » Journal of Inflammation Research » Volume 18
Prognostic Role of Inflammatory Hematologic Indices in Predicting Acute Coronary Syndrome in Elderly Patients with Chronic Coronary Syndrome
Authors Bao Q, Liu T, Song H, Bao W, Fan W
Received 13 March 2025
Accepted for publication 9 July 2025
Published 22 July 2025 Volume 2025:18 Pages 9637—9653
DOI https://doi.org/10.2147/JIR.S528161
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Quan Zhang
Qianxiao Bao,1 Tao Liu,2 Hui Song,3 Weiguo Bao,4 Weiguo Fan5
1Queen Mary College, Nanchang University, Nanchang, Jiangxi, 330031, People’s Republic of China; 2Medical Experimental Diagnostic Center; Administrative Office, Central Hospital Affiliated to Shandong First Medical University, Jinan, Shandong, 250013, People’s Republic of China; 3Department of Cardiology, Central Hospital Affiliated to Shandong First Medical University, Jinan, Shandong, 250013, People’s Republic of China; 4Department of Cardiovascular Surgery, The Second Hospital of Shandong University, Jinan, Shandong, 250013, People’s Republic of China; 5Department of Cardiology, The Second Affiliated Hospital of Nanchang University, Nanchang, Jiangxi, 330000, People’s Republic of China
Correspondence: Weiguo Fan, Department of Cardiology, The Second Affiliated Hospital of Nanchang University, No. 1, Mingde Road, Nanchang, Jiangxi, 330000, People’s Republic of China, Email [email protected] Weiguo Bao, Department of Cardiovascular Surgery, The Second Hospital of Shandong University, No. 247 Beiyuan Street, Jinan, Shandong, 250013, People’s Republic of China, Email [email protected]
Background: Coronary artery disease (CAD) remains a leading cause of morbidity and mortality, with inflammation playing a central role in the transition from Chronic Coronary Syndrome (CCS) to acute coronary syndrome (ACS). This study investigates the predictive value of multiple inflammatory indices in assessing the risk of ACS.
Methods: This retrospective case-control study included 1, 116 patients aged 60 and older diagnosed with CCS or ACS between June 2018 and June 2023. Patients were grouped into CCS and ACS categories, with inflammatory indices derived from hematological parameters. Key indices included the neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), systemic inflammatory response index (SIRI; calculated as monocyte count × neutrophil count / lymphocyte count), systemic immune-inflammation index (SII; platelet count × neutrophil count / lymphocyte count), and C-reactive protein-albumin-lymphocyte (CALLY) index (albumin × lymphocyte count / [C-reactive protein × 10]). Multivariate logistic regression and receiver operator characteristic (ROC) curve analyses assessed the indices’ predictive capacity for ACS.
Results: The ACS group demonstrated significantly elevated levels of inflammatory markers such as White Blood Cell Count (WBC), neutrophils, and monocytes. Among inflammatory indices, PLR, SIRI, and the SII were significant predictors of ACS. PLR had the highest area under the curve (AUC=0.841), with strong sensitivity (0.828) and specificity (0.747). SIRI followed with notable predictive efficacy (AUC=0.802). Increased BMI, diabetes, and adverse lipid profiles also correlated with heightened ACS risk.
Conclusion: PLR, SIRI, and SII emerge as valuable prognostic markers for ACS, reflecting the underlying inflammatory processes central to CAD progression. Their integration into clinical assessments could improve risk stratification and guide interventions. Future research should aim to elucidate mechanisms linking systemic inflammation to coronary events and explore therapeutic strategies targeting these pathways.
Keywords: coronary artery disease, inflammatory biomarkers, acute coronary syndrome, neutrophil-to-lymphocyte ratio, platelet-to-lymphocyte ratio, systemic inflammatory response index
Introduction
Coronary artery disease (CAD) remains a leading cause of morbidity and mortality worldwide, underscoring the need for better understanding and management of this prevalent condition.1 The pathophysiology of CAD was complex, involving a multifaceted interplay between endothelial dysfunction, lipid metabolism disorders, and chronic inflammation, which collectively contribute to the formation and progression of atherosclerotic plaques within the coronary arteries.2 A particularly acute and life-threatening manifestation of CAD was the acute coronary syndrome (ACS), which includes a spectrum of clinical presentations such as myocardial infarction and unstable angina, resulting from the sudden disruption of coronary blood flow.3
Inflammation plays a central role in the pathogenesis of atherosclerosis and its progression to ACS. The inflammatory milieu leads to a cascade of events that encompass endothelial activation, leukocyte recruitment, and the secretion of pro-inflammatory cytokines. These processes cumulatively engender plaque instability and rupture, precipitating thrombotic events that characterize ACS.4–6 In recent years, a focus has emerged within cardiovascular research to identify reliable biomarkers that can not only elucidate underlying pathogenetic mechanisms but also serve as predictive indicators of adverse outcomes, allowing for early intervention and improved risk stratification.7–9
Among various potential biomarkers, inflammatory indices derived from routine hematological parameters have gained attention due to their simplicity, cost-effectiveness, and growing evidence of prognostic value in cardiovascular diseases. Indices such as the neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), systemic immune-inflammation index (SII; platelet count × neutrophil count / lymphocyte count), and systemic inflammatory response index (SIRI; calculated as monocyte count × neutrophil count / lymphocyte count), provide insights into the balance between pro-inflammatory and anti-inflammatory processes. These indices integrate multiple aspects of immune response and platelet activation, both of which have been implicated in the pathophysiology of ACS.10–12
Despite their potential, the clinical utility of these indices in predicting the transition from Chronic Coronary Syndrome (CCS) to Acute Coronary Syndrome (ACS) remains under-explored. Prior studies have demonstrated associations between elevated inflammatory indices and worsened cardiovascular outcomes;13–15 however, comprehensive evaluations of these markers specifically for predicting ACS development in CCS patients—particularly in the elderly—are limited. Furthermore, the comparative prognostic value of multiple indices (eg, PLR, SIRI, SII) and their integration with clinical risk factors in this context are yet to be fully delineated. This study aims to bridge this gap by systematically assessing the predictive capacity of key inflammatory indices derived from routine hematological parameters for ACS occurrence in elderly patients with CCS.
Methods
Study Design
This retrospective case-control study included 1, 116 patients diagnosed with CCS and ACS who were admitted to our hospital between June 2018 and June 2023. The patients’ demographic information was systematically collected. Due to the retrospective nature of this study, obtaining informed consent from participants was not possible. As a result, an exemption was granted by the Hospital Ethics Committee. This exemption and the study itself were approved by the Ethics Committee of the Second Affiliated Hospital of Nanchang University. The study was conducted in accordance with the principles of the Declaration of Helsinki. All patient data were anonymized and maintained confidentially throughout the research process in compliance with institutional guidelines.
Inclusion, Exclusion, and Grouping Criteria
Inclusion criteria for the study were as follows: (1) participants aged 60 years or older; (2) a confirmed diagnosis of CCS or ACS verified through clinical and imaging examinations, adhering to established diagnostic criteria;16,17 and (3) the availability of comprehensive clinical and follow-up data.
Exclusion criteria included: (1) a history of coronary artery interventions; (2) current or recent use of hormone medications; (3) use of anti-infective drugs within the previous seven days; (4) presence of severe valvular heart disease, refractory heart failure, cardiomyopathy, or other significant cardiac conditions; (5) existence of severe infections, hematologic disorders, immunological connective tissue diseases, or complications arising from malignant tumors; and (6) severe hepatic or renal insufficiency.
Grouping criteria were established based on the type of disease among the enrolled patients: the CCS group comprised 973 patients, while the ACS group included 143 patients. Furthermore, the CCS group was subdivided based on whether patients progressed to ACS within one year of follow-up. This resulted in two subgroups: the Non-ACS Occurrence Group, consisting of 909 patients, and the ACS Occurrence Group, consisting of 64 patients. The follow-up period for this study concluded in June 2024.
Detection of Blood Markers and Calculation of the Inflammatory Indices
Collection and Preparation of Blood Samples
Baseline blood samples were obtained from patients at the time of admission. A 5 mL sample of venous blood was collected from fasting patients prior to 8 a.m., following an overnight fast of at least 8 hours. Hematological parameters were assessed using whole blood samples. For biochemical markers, serum separation was necessary. This process was carried out by centrifuging clotted blood samples at 3, 000 rpm for 10 minutes within 30 minutes of collection.
Measurement of Hematological Parameters
Hematological parameters such as White Blood Cell Count (WBC), Neutrophils (Neu), Monocytes (Mon), Lymphocytes (Lym), Platelet Count (Plt), Hemoglobin (Hb), and Glycated Hemoglobin (HbA1c) were measured using a SYSMEX-XN9000 automated hematology analyzer (Japan), following the manufacturer’s instructions.
Measurement of Biochemical Markers
Biochemical analyses were performed on the serum samples to measure levels of Total Cholesterol (TC), Triglycerides (TG), High-Density Lipoprotein (HDL), Low-Density Lipoprotein (LDL), Fasting Plasma Glucose (FPG), Alanine Transaminase (ALT), Aspartate Transaminase (AST), Gamma-Glutamyl Transferase (GGT), Alpha-Fetoprotein (AFP), C-Reactive Protein (CRP), Albumin (Alb), Urea Nitrogen (BUN), Creatinine (Cre), and Uric Acid (UA). These measurements were obtained using enzymatic colorimetric methods or specific assays with a HITACHI-008AS biochemical analyzer (Japan).
Calculation of Inflammatory Indices
Inflammatory indices were computed using the hematological and biochemical data collected as follows: Neutrophil-Lymphocyte Ratio (NLR) was calculated as Neu/Lym; Platelet-Lymphocyte Ratio (PLR) as Plt/Lym; Lymphocyte-Monocyte Ratio (LMR) as Lym/Mon; Systemic Immune-Inflammation Index (SII) as (Plt × Neu)/Lym; Platelet-to- Alb Ratio (PAR) as Plt/Alb; SIRI as Mon × Neu/Lym; CRP-to-Lymphocyte Ratio (CLR) as CRP/Lym; and C-reactive protein-albumin-lymphocyte (CALLY) as (Alb × Lym)/ (CRP × 10).18–20
All baseline blood marker data were sourced from the hospital’s case collection system at the time of patient admission. These data were subsequently used for statistical analysis to determine differences between groups.
Statistical Analysis
Data analysis was conducted using SPSS version 29.0 statistical software (SPSS Inc., Chicago, IL, USA). Categorical data were presented as [n (%)]. For sample sizes of 40 or more with a theoretical frequency (T) of 5 or greater, the chi-square test, denoted as χ², was employed. If the sample size was 40 or more but the theoretical frequency ranged from 1 to less than 5, an adjusted chi-square test using a correction formula was applied. For samples with a size of less than 40 or a theoretical frequency of less than 1, Fisher’s exact probability method was used. Continuous variables were assessed for normal distribution using the Shapiro–Wilk test. For continuous data following a normal distribution, results were expressed as mean±standard deviation (Eqn±s), and comparisons were made using a t-test. Non-normally distributed data were presented as median (interquartile range) and compared using the Mann–Whitney U-test. Spearman’s rank correlation coefficient was used to evaluate correlations between variables. Multivariate logistic regression analyses was conducted to calculate the odds ratio (OR) and 95% confidence interval (CI) for each parameter. A p-value of less than 0.05 was considered statistically significant.
Results
Demographic and Clinical Characteristics of Patients in the CCS and ACS Groups
The ACS group was noted to be significantly older with a mean age of 70.19±9.18 years compared to 68.43±8.67 years in the CCS group (P=0.025) (Table 1). Body mass index (BMI) was also higher among ACS patients, averaging 26.12±3.69 kg/m² versus 25.47±3.54 kg/m² in the CCS group (P=0.043). Diabetes was more prevalent among ACS patients, with 41.26% affected compared to 30.22% in the CCS group (P=0.008). Furthermore, a greater proportion of ACS patients had involvement of two or more CAD vessels at 32.17%, relative to 19.43% in the CCS group, which was statistically significant (P < 0.001). The degree of coronary stenosis showed a higher occurrence of total occlusion among ACS patients (7.69%) compared to those with CCS (3.29%), contributing to significant findings (P=0.02). No statistically significant differences were found between the groups regarding gender distribution, employment, marital status, residence, smoking history, drinking history, hypertension, congestive heart failure, or medication use (P > 0.05). These findings suggest that age, BMI, diabetes prevalence, number of CAD vessels involved, and degree of coronary stenosis were strongly associated with the transition from CCS to ACS.
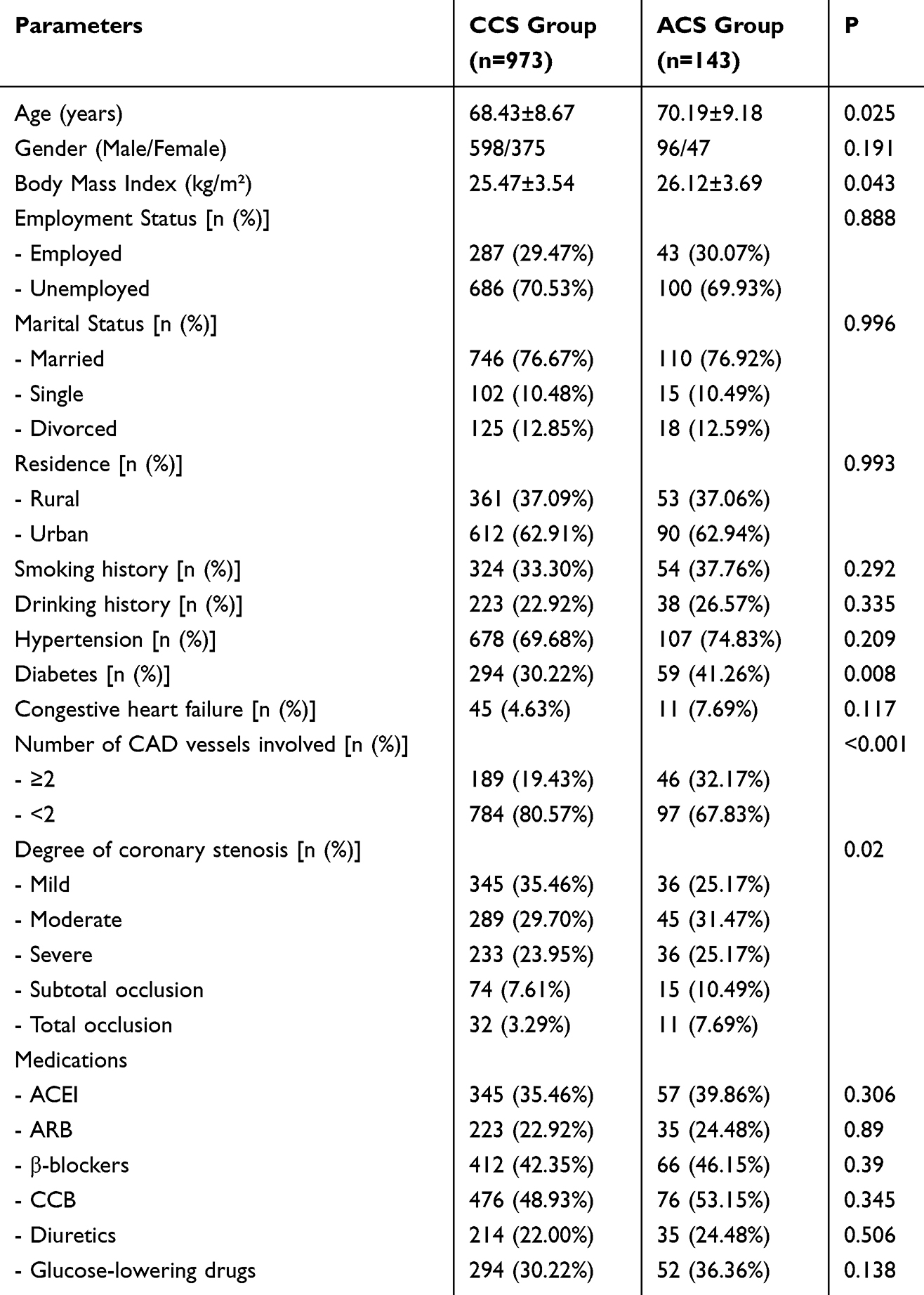 |
Table 1 Comparison of Baseline Demographic and Clinical Characteristics Between CCS and ACS Groups |
Baseline Blood Markers in CCS and ACS Groups
The ACS group demonstrated higher levels of WBC count (7.54±2.13 × 10^9/L vs 6.78±1.89 × 10^9/L, P < 0.001), Neu (4.92±1.78 × 10^9/L vs 4.21±1.56 × 10^9/L, P < 0.001), and Mon (0.64±0.21 × 10^9/L vs 0.56±0.18 × 10^9/L, P < 0.001) compared to the CCS group, indicating a heightened inflammatory response (Table 2). Additionally, Plt was significantly elevated in the ACS group (258.12±74.36 × 10^9/L vs 234.56±67.89 × 10^9/L, P < 0.001). Metabolic parameters such as HbA1c were notably higher in the ACS cohort (6.69±1.04% vs 6.43±0.97%, P=0.003), alongside FPG (6.87±1.54 mmol/L vs 6.38±1.23 mmol/L, P < 0.001), and TG (1.89±0.98 mmol/L vs 1.77±0.87 mmol/L, P < 0.001). Conversely, HDL levels were lower in ACS patients (1.14±0.37 mmol/L vs 1.23±0.34 mmol/L, P=0.002). No significant differences were found between groups for hemoglobin, Lym, CRP, Alb, TC, LDL, BUN, Cre, and UA concentrations (all P > 0.05). These findings underscore the role of inflammatory and metabolic dysregulation as potential predictors of ACS progression.
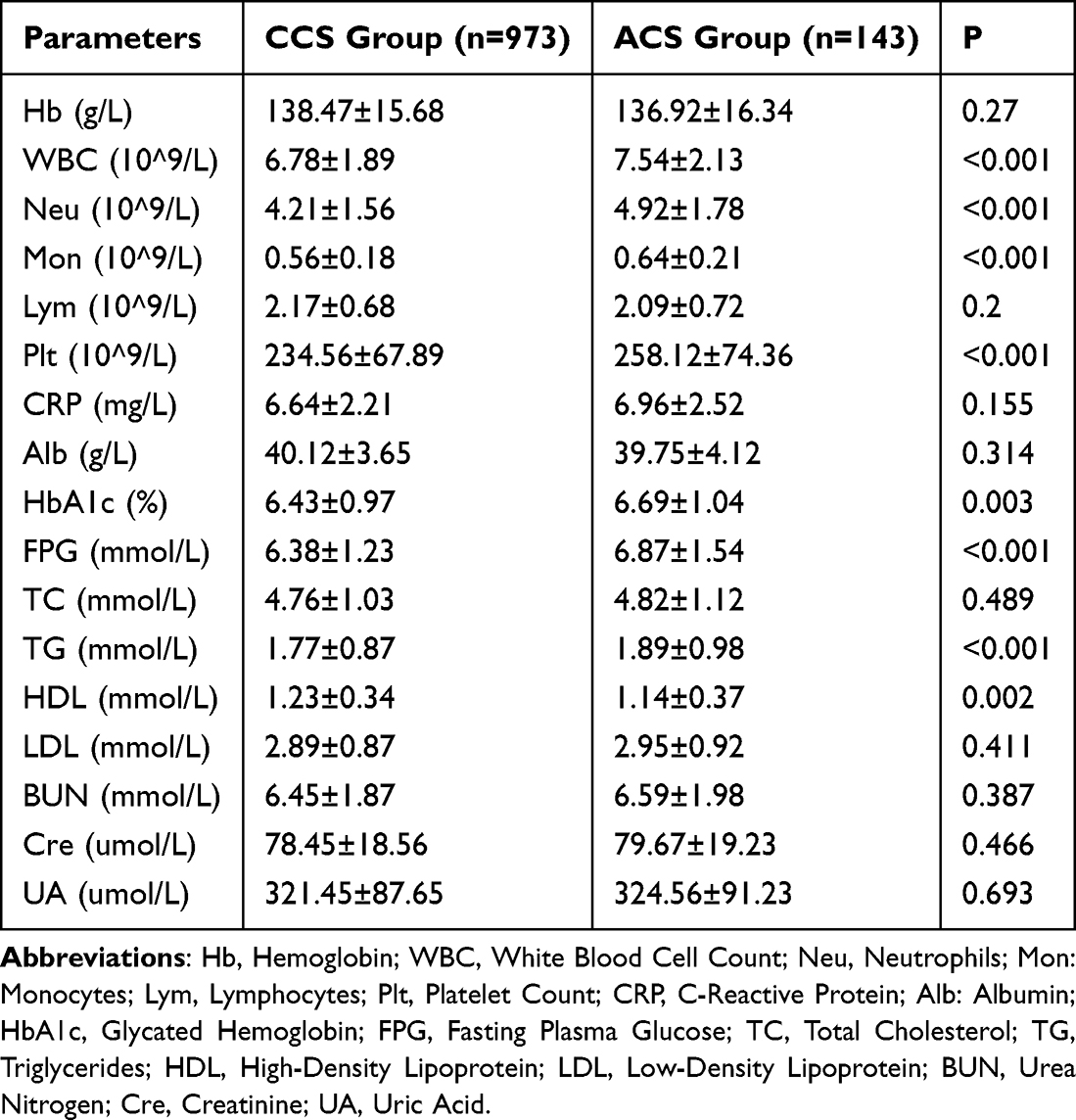 |
Table 2 Comparison of Baseline Hematological and Biochemical Parameters Between CCS and ACS Groups |
Baseline Inflammatory Indices in CCS and ACS Groups
The NLR was notably higher in the ACS group, with values of 3.11±1.02 compared to 2.56±0.89 in the CCS group (P < 0.001), indicative of enhanced systemic inflammation in ACS (Figure 1). Similarly, the PLR and SIRI were significantly greater in patients with ACS, with PLR at 126.56±38.21 and SIRI at 0.78±0.31, compared to 119.34±34.78 (P=0.022) and 0.71±0.23 (P=0.012) in the CCS group, respectively. The LMR and the CLR also presented significant differences, being lower in the ACS cohort (LMR: 3.88±1.15; CLR: 3.63±1.54) compared to the CCS group (LMR: 4.21±1.29, P=0.004; CLR: 3.07±1.02, P < 0.001). The SII was substantially elevated in ACS patients (977.43±287.32 vs 815.32±215.67, P < 0.001), emphasizing its potential as a predictive marker for acute coronary events. Additionally, the PAR was lower in the ACS group (6.04±1.76) compared to CCS (6.52±1.94, P=0.005), and the CALLY index was significantly reduced in ACS patients (2.31±0.84 vs 2.53±0.97, P=0.004). These findings suggest that alterations in these inflammatory indices were closely associated with the advancement to ACS, underscoring their potential utility as prognostic markers in coronary atherosclerosis.
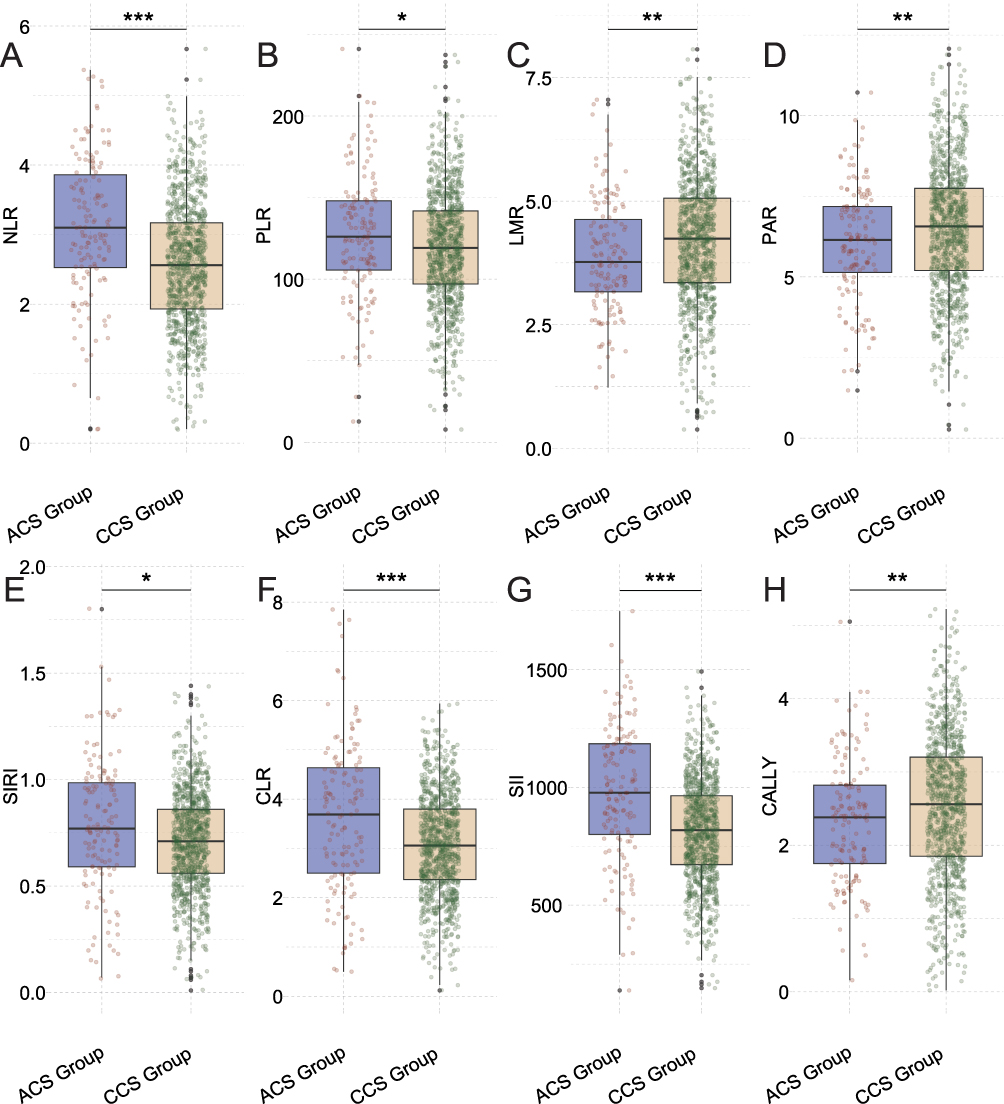 |
Figure 1 Comparison of Baseline Inflammatory Indices Between CCS and ACS Groups. (A) NLR; (B) PLR; (C) LMR; (D) PAR; (E) SIRI; (F) CLR; (G) SII; (H) CALLY. Abbreviations: NLR, Neutrophil-to-Lymphocyte Ratio; PLR, Platelet-to-Lymphocyte Ratio; LMR, Lymphocyte-to-Monocyte Ratio; PAR, Platelet-to-Albumin Ratio; SIRI, Systemic Inflammatory Response Index (monocyte count × neutrophil count / lymphocyte count); CLR: C-Reactive Protein-to-Lymphocyte Ratio; SII: Systemic Immune-Inflammation Index (Plt × neutrophil count / lymphocyte count); CALLY: Albumin × Lymphocyte / (C-Reactive Protein × 10). Ns: No significant difference. Note: *P < 0.05; **P < 0.01; ***P < 0.001. |
Correlation Analysis
The analysis of Spearman’s rank correlation coefficients revealed several significant associations between patient characteristics, laboratory parameters, and disease progression in coronary atherosclerosis (Table 3). Age and BMI showed weak but significant positive correlations with disease progression, with coefficients of 0.066 (P=0.027) and 0.063 (P=0.036), respectively. Diabetes exhibited a stronger positive correlation (rho=0.079, P=0.008). Among clinical characteristics, the number of CAD vessels involved (≥2) had a notable positive correlation (rho=0.104, P < 0.001), as did the degree of coronary stenosis (rho=0.085, P=0.005). Laboratory parameters displayed significant positive correlations with disease progression, particularly WBC, Neu, Mon, Plt, FPG, TG, and HbA1c, with rho values of 0.120, 0.136, 0.141, 0.103 (all P < 0.001), 0.107 (P < 0.001), 0.106 (P < 0.001), and 0.086 (P=0.004), respectively. Conversely, HDL was negatively correlated with disease progression (rho=−0.088, P=0.003). These findings highlight the significant influence of inflammatory markers and metabolic parameters on the advancement of coronary atherosclerosis, underscoring their potential predictive value for ACS.
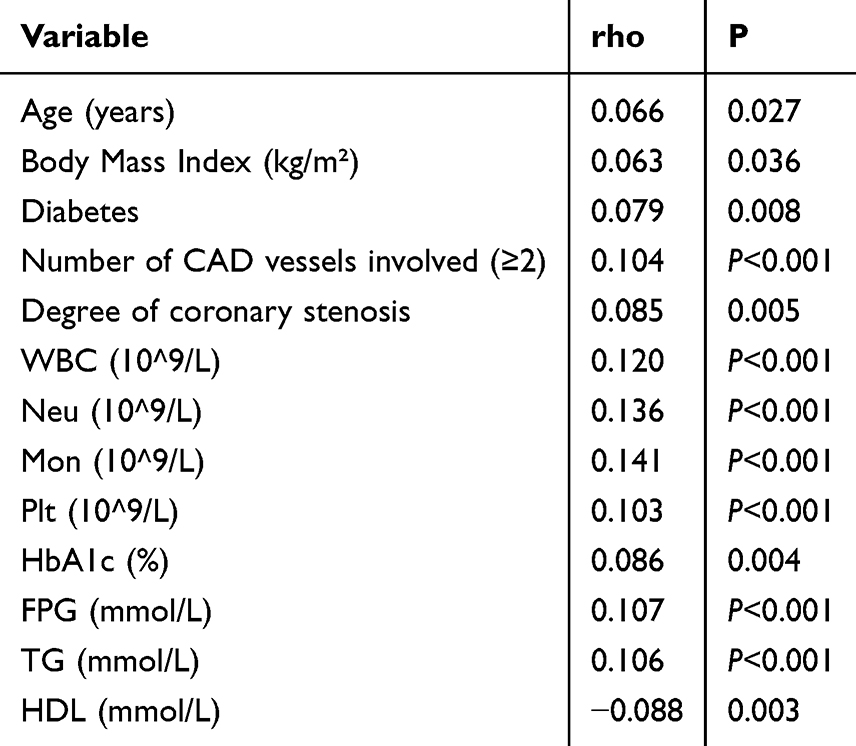 |
Table 3 Spearman’s Rank Correlation Coefficients Between Patient Characteristics, Laboratory Parameters, and Disease Progression |
Demographic and Clinical Characteristics of Patients in the Non-ACS Occurrence and ACS Occurrence Groups Within the CCS Cohort
Patients in the ACS occurrence group were significantly older, with a mean age of 71.23±6.24 years compared to 68.37±7.59 years in the non-ACS group (P=0.003) (Table 4). They also had a higher mean BMI of 26.28±2.84 kg/m² compared to 25.41±2.92 kg/m² in the non-ACS group (P=0.02). A significantly greater proportion of ACS patients had diabetes (43.75% vs 29.26%, P=0.015) and congestive heart failure (10.94% vs 4.18%, P=0.029) than those in the non-ACS group. Additionally, the ACS group had a larger number of patients with ≥2 CAD vessels involved (35.94% vs 19.36%, P=0.001) and a higher incidence of subtotal and total coronary occlusion (subtotal: 17.19% vs 6.93%, total: 9.38% vs 2.86%, P < 0.001 for stenosis severity). However, no significant differences were observed in gender distribution, employment, marital status, residence, smoking and drinking history, hypertension prevalence, or in the use of common cardiovascular medications such as ACE inhibitors, ARBs, β-blockers, calcium channel blockers, diuretics, and glucose-lowering drugs (P > 0.05). These findings underscore the importance of age, BMI, diabetes, heart failure, the extent of CAD, and the degree of stenosis as key factors associated with the progression from CCS to ACS.
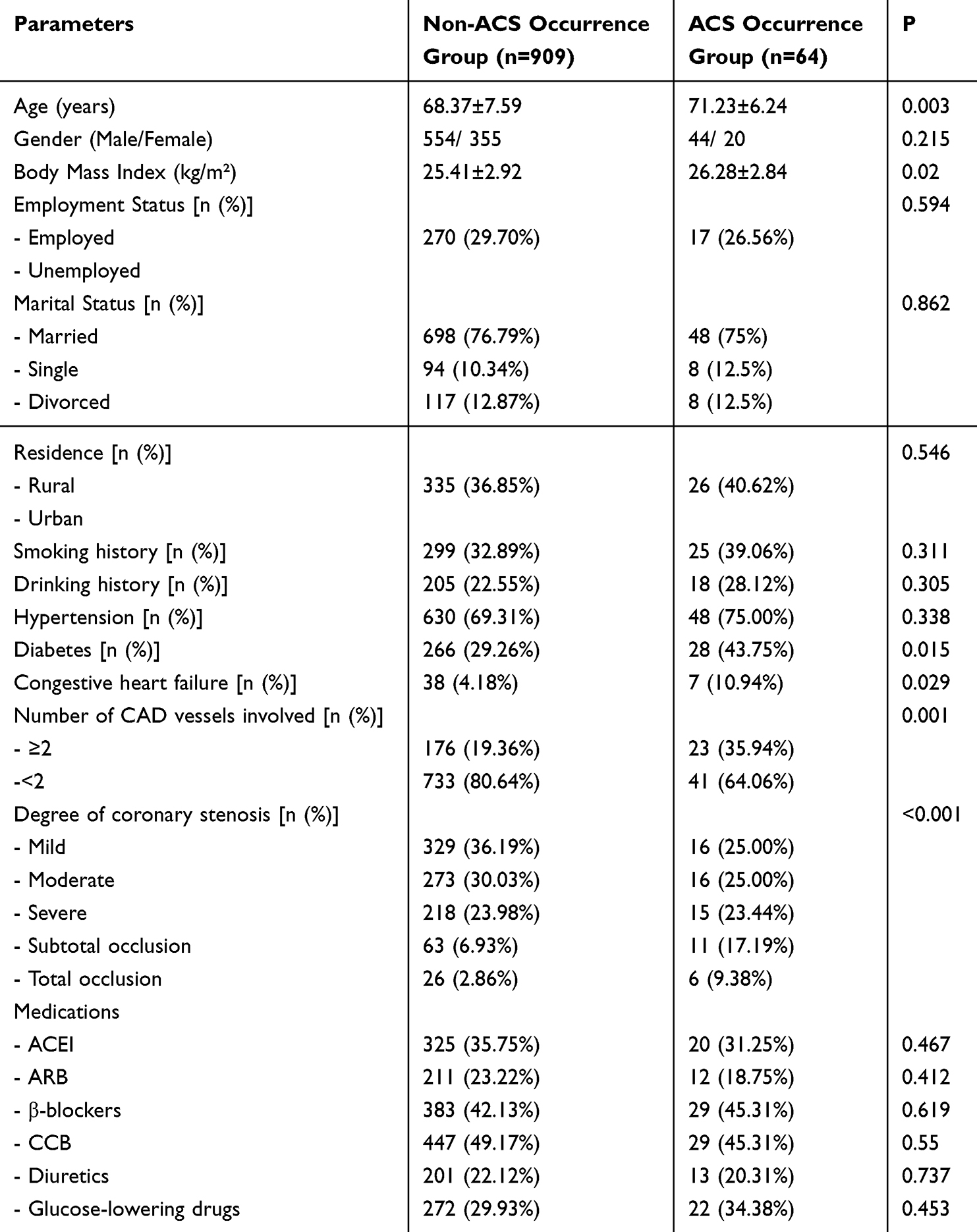 |
Table 4 Comparison of Baseline Demographic and Clinical Characteristics Between Non-ACS Occurrence and ACS Occurrence Groups Within the CCS Cohort |
Baseline Blood Markers in Non-ACS Occurrence and ACS Occurrence Groups Within the CCS Cohort
The ACS occurrence group showed elevated WBC counts (7.12±1.71 × 10^9/L vs 6.59±1.67 × 10^9/L, P=0.015) and increased levels of Neu (4.63±1.14 × 10^9/L vs 4.12±1.24 × 10^9/L, P=0.001) and Mon (0.59±0.13 × 10^9/L vs 0.54±0.14 × 10^9/L, P=0.006), indicating a heightened inflammatory state (Table 5). Additionally, Plt were higher in the ACS group (241.73±54.30 × 10^9/L vs 224.61±57.85 × 10^9/L, P=0.022). Despite similar CRP levels between the groups (P=0.129), Alb levels were significantly lower in the ACS occurrence group (38.57±3.19 g/L vs 40.74±3.14 g/L, P < 0.001). HbA1c and FPG were both significantly elevated in the ACS group (HbA1c: 6.57±0.73% vs 6.24±0.76%, P < 0.001; FPG: 6.58±1.03 mmol/L vs 6.19±1.12 mmol/L, P=0.007), reflecting poorer glycemic control associated with ACS progression. TG were also higher (1.86±0.57 mmol/L vs 1.71±0.66 mmol/L, P=0.021), while HDL levels were lower (1.19±0.26 mmol/L vs 1.26±0.27 mmol/L, P=0.034) in the ACS occurrence group, reflecting adverse lipid profiles. No significant differences were observed in hemoglobin, Lym, total and LDL cholesterol, BUN, Cre, or UA levels (P > 0.05). These findings suggest that specific inflammatory and metabolic parameters may serve as predictive markers for the advancement to ACS within the CCS cohort.
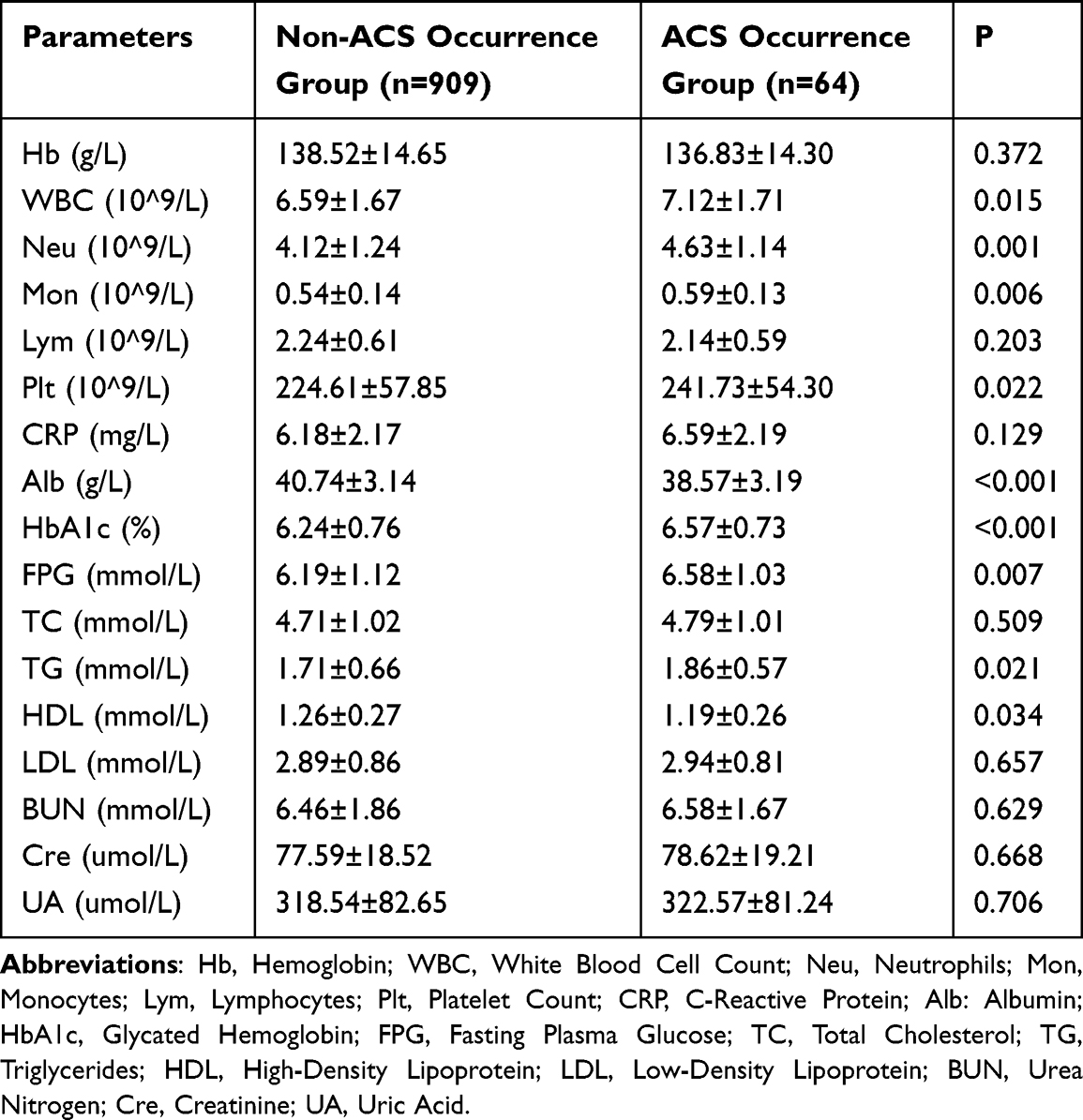 |
Table 5 Comparison of Baseline Hematological and Biochemical Parameters Between Non-ACS Occurrence and ACS Occurrence Groups Within the CCS Cohort |
Baseline Inflammatory Indices in Non-ACS Occurrence and ACS Occurrence Groups Within the CCS Cohort
The NLR was significantly higher in the ACS occurrence group (2.71±0.71) compared to the non-ACS group (2.42±0.78, P=0.004), signifying increased systemic inflammation among those progressing to ACS (Figure 2). The PLR showed a marked elevation in the ACS group (136.40±17.15) relative to the non-ACS group (112.50±16.75, P < 0.001), further indicating a heightened inflammatory profile. In contrast, the LMR was lower in the ACS group (4.02±1.14) compared to the non-ACS group (4.36±1.18, P=0.024), reflecting a shift towards a pro-inflammatory state. The SIRI also demonstrated substantial differences, being elevated in the ACS group (1.07±0.20 vs 0.81±0.21, P < 0.001). Similarly, the SII was significantly higher in patients who developed ACS (887.31±132.33) compared to those who did not (764.43±143.62, P < 0.001). The CLR and PAR did not show statistically significant differences between the groups (P=0.172 and P=0.114, respectively). However, the Alb × lymphocyte / (CRP × 10) index (CALLY) was lower in the ACS group (2.42±0.63) compared to the non-ACS group (2.68±0.66, P=0.003). These findings suggest that specific inflammatory indices, particularly NLR, PLR, SIRI, SII, and CALLY, effectively distinguish patients with CCS at higher risk of transitioning to ACS, underscoring their potential utility as predictive markers.
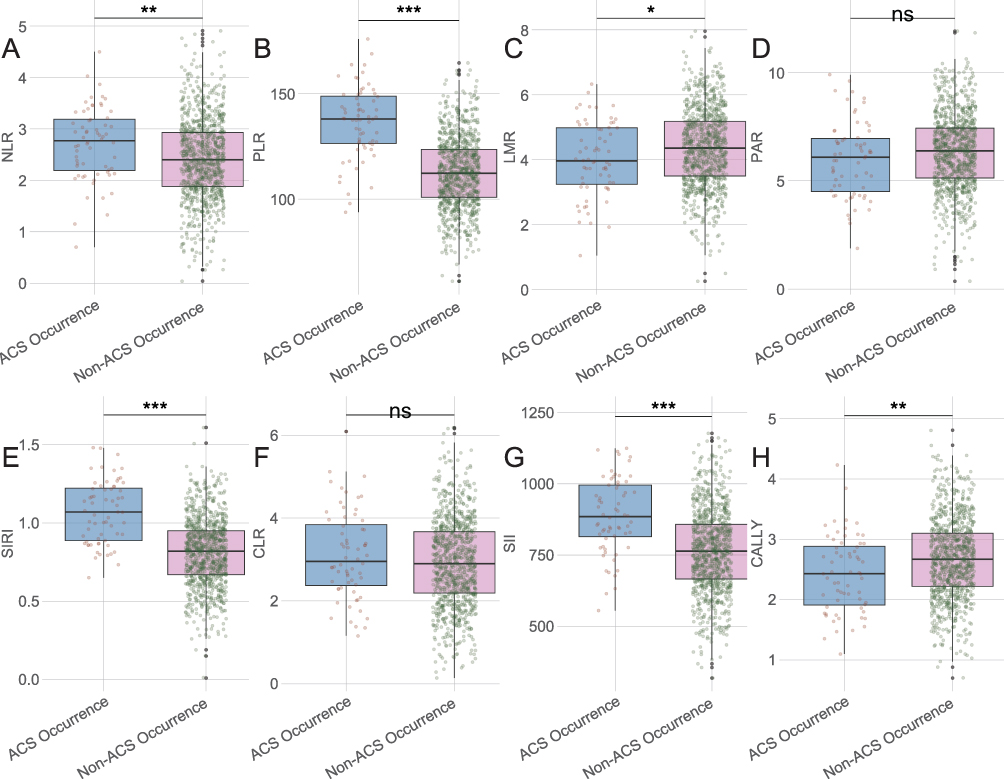 |
Figure 2 Comparison of Baseline Inflammatory Indices Between Non-ACS Occurrence and ACS Occurrence Groups Within the CCS Cohort. (A) NLR; (B) PLR; (C) LMR; (D) PAR; (E) SIRI; (F) CLR; (G) SII; (H) CALLY. Abbreviations: NLR, Neutrophil-to-Lymphocyte Ratio; PLR, Platelet-to-Lymphocyte Ratio; LMR, Lymphocyte-to-Monocyte Ratio; PAR, Platelet-to-Albumin Ratio; SIRI, Systemic Inflammatory Response Index (monocyte count × neutrophil count / lymphocyte count); CLR: C-Reactive Protein-to-Lymphocyte Ratio; SII: Systemic Immune-Inflammation Index (Plt × neutrophil count / lymphocyte count); CALLY: Albumin × Lymphocyte / (C-Reactive Protein × 10). Ns: No significant difference. Note: *P < 0.05; **P < 0.01; ***P < 0.001. |
Correlation Analysis of Patient Characteristics and Laboratory Parameters with ACS Occurrence
The Spearman’s rank correlation analysis revealed several significant relationships between patient characteristics, laboratory parameters, and the occurrence of ACS within the cohort (Table 6). Age demonstrated a positive correlation with ACS occurrence (rho=0.092, P=0.004), suggesting that older patients were more likely to experience ACS. Additionally, BMI and the presence of diabetes and congestive heart failure showed significant positive correlations with ACS occurrence, with rho values of 0.075 (P=0.020), 0.078 (P=0.015), and 0.080 (P=0.013), respectively. The number of CAD vessels involved (≥2) and the degree of coronary stenosis were also positively associated with ACS occurrence (rho=0.102, P=0.001 and rho=0.099, P=0.002, respectively).
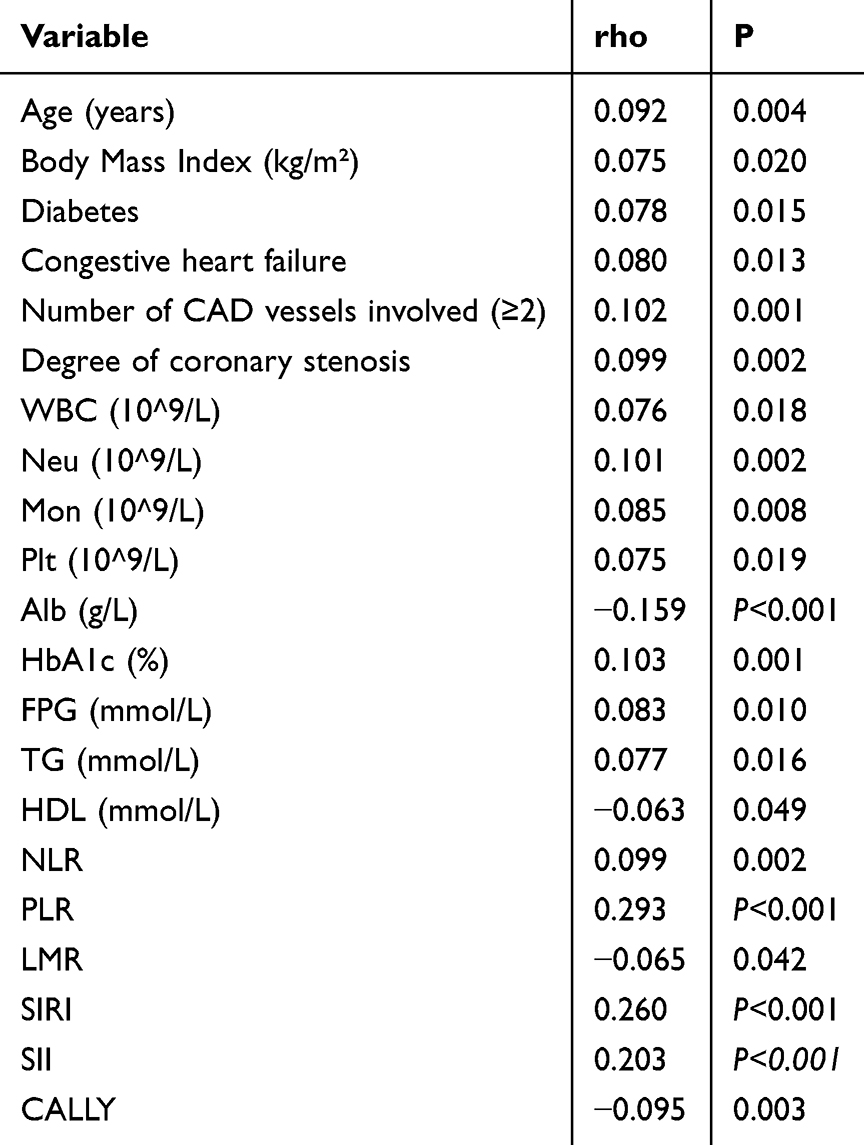 |
Table 6 Spearman’s Rank Correlation Coefficients Between Patient Characteristics, Laboratory Parameters, and ACS Occurrence |
In terms of laboratory parameters, inflammatory markers such as white blood cell (WBC) count, Neu, Mon, and Plt were all positively correlated with ACS occurrence, emphasizing the role of inflammation in ACS pathogenesis, with rho values ranging from 0.075 to 0.101 (all P ≤ 0.019). Conversely, Alb levels exhibited a negative correlation (rho=−0.159, P < 0.001), indicating that lower Alb levels were linked to higher ACS occurrence. HbA1c, FPG, and TG were positively correlated with ACS occurrence (rho ranging from 0.077 to 0.103, all P ≤ 0.016), while HDL showed a weak negative correlation (rho=−0.063, P=0.049).
Among the inflammatory indices, the NLR, PLR, SIRI, SII, and CALLY displayed significant correlations with ACS occurrence. PLR and SIRI showed particularly strong positive correlations (rho=0.293 and rho=0.260, respectively, both P < 0.001), while CALLY was negatively correlated (rho=−0.095, P=0.003). These findings underscore the predictive value of these parameters for ACS occurrence, highlighting their potential role in risk stratification and management of patients with coronary atherosclerosis.
Multivariate Logistic Regression Analysis for Predictors of ACS Occurrence
The multivariate logistic regression analysis of inflammatory indices as predictors of ACS occurrence revealed several independent risk factors (Table 7). The PLR emerged as a strong predictor, with a coefficient of 0.089 and an OR of 1.094 (95% CI: 1.069–1.119, P < 0.001), indicating that higher PLR was associated with increased odds of ACS occurrence. Similarly, the SIRI demonstrated a substantial predictive value, with a coefficient of 6.552 and an exceedingly high OR of 700.440 (95% CI: 115.882–4233.766, P < 0.001), highlighting its potential as a powerful marker for ACS risk.
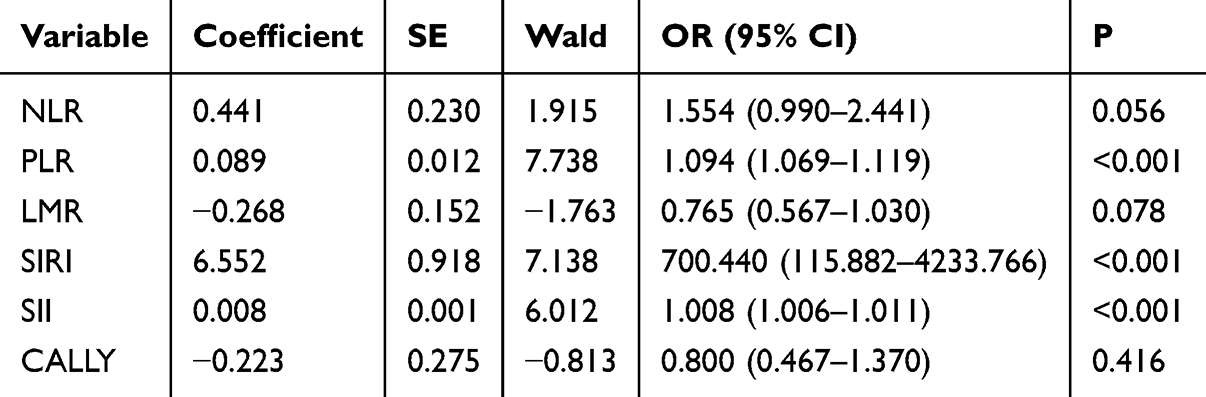 |
Table 7 Multivariate Logistic Regression Analysis of Inflammatory Indices as Predictors of ACS Occurrence |
The SII also contributed significantly, with a coefficient of 0.008 and an OR of 1.008 (95% CI: 1.006–1.011, P < 0.001), further supporting its role in predicting ACS occurrence. The NLR showed a positive association with ACS, albeit not reaching conventional statistical significance (coefficient=0.441, OR=1.554, 95% CI: 0.990–2.441, P=0.056). In contrast, the LMR and the CALLY index did not show significant predictive effects for ACS (LMR coefficient=−0.268, OR=0.765, 95% CI: 0.567–1.030, P=0.078; CALLY coefficient=−0.223, OR=0.800, 95% CI: 0.467–1.370, P=0.416), with LMR approaching borderline significance. These findings suggest that PLR, SIRI, and SII were key inflammatory indices with prognostic utility in identifying patients at elevated risk for ACS, which can inform targeted therapeutic strategies in coronary atherosclerosis management.
ROC Curve Analysis for Predictive Value of Inflammatory Indices
The ROC curve analysis for the diagnostic performance of inflammatory indices in predicting ACS occurrence highlighted varying levels of sensitivity, specificity, and overall diagnostic efficacy (Table 8). The PLR emerged as the most robust indicator, with an area under the curve (AUC) of 0.841, indicating excellent discriminative power. It demonstrated high sensitivity (0.828) and specificity (0.747), resulting in a Youden index of 0.575, suggesting its strong potential in clinical settings for predicting ACS.
 |
Table 8 ROC Curve Analysis of Inflammatory Indices for Predicting ACS Occurrence |
The SIRI also showed strong diagnostic performance, with an AUC of 0.802 and a high sensitivity of 0.875; however, its specificity was moderate at 0.578, yielding a Youden index of 0.453, indicating effective risk prediction with some limitations in specificity. The SII followed, achieving an AUC of 0.737 with a balanced sensitivity of 0.75 and specificity of 0.651, producing a Youden index of 0.401.
In contrast, the NLR and CRP -to- Alb index (CALLY) exhibited lower diagnostic performance, with AUCs of 0.616 and 0.611, respectively. NLR showed moderate sensitivity and specificity (0.594 and 0.608, respectively), while CALLY reported lower sensitivity (0.391) but higher specificity (0.801), yielding Youden indices of 0.202 and 0.192, respectively.
The LMR had the weakest performance, with an AUC of 0.576, sensitivity of 0.547, and specificity of 0.601, resulting in a Youden index of 0.148, indicating limited utility as a standalone predictive measure for ACS. These results underscore the importance of PLR, SIRI, and SII as valuable tools in the risk stratification of patients with coronary atherosclerosis for developing ACS, advocating for their consideration in clinical diagnostic protocols. Decision curve analysis (DCA) and confusion matrix analysis were shown in Figures 3 and 4.
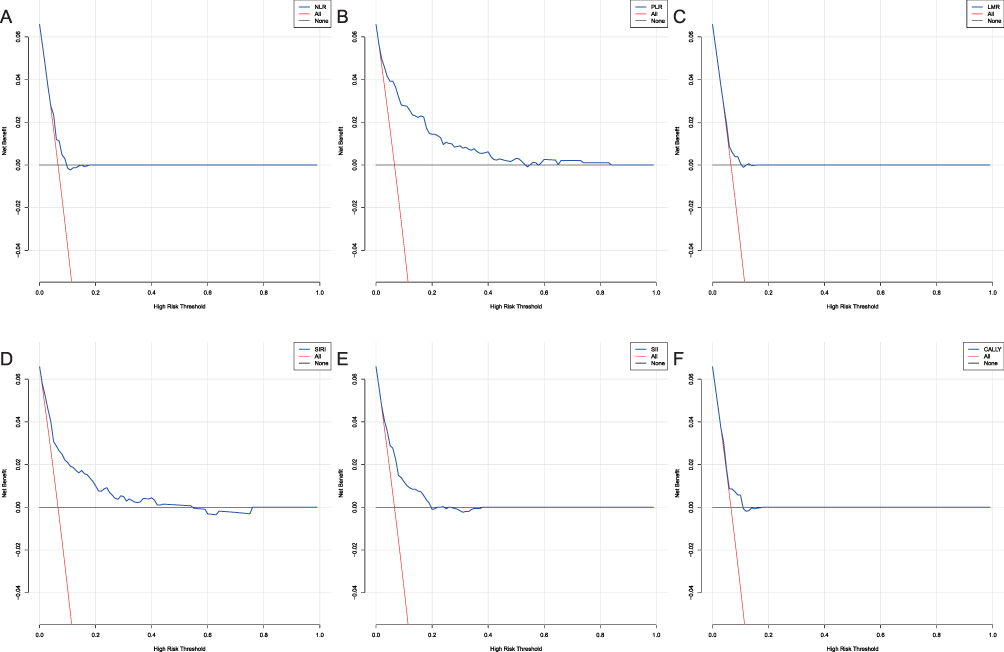 |
Figure 3 Decision Curve Analysis (DCA) for Predicting ACS Occurrence Using Various Inflammatory Indices. (A) NLR; (B) PLR; (C) LMR, (D) SIRI; (E) SII; (F) CALLY. |
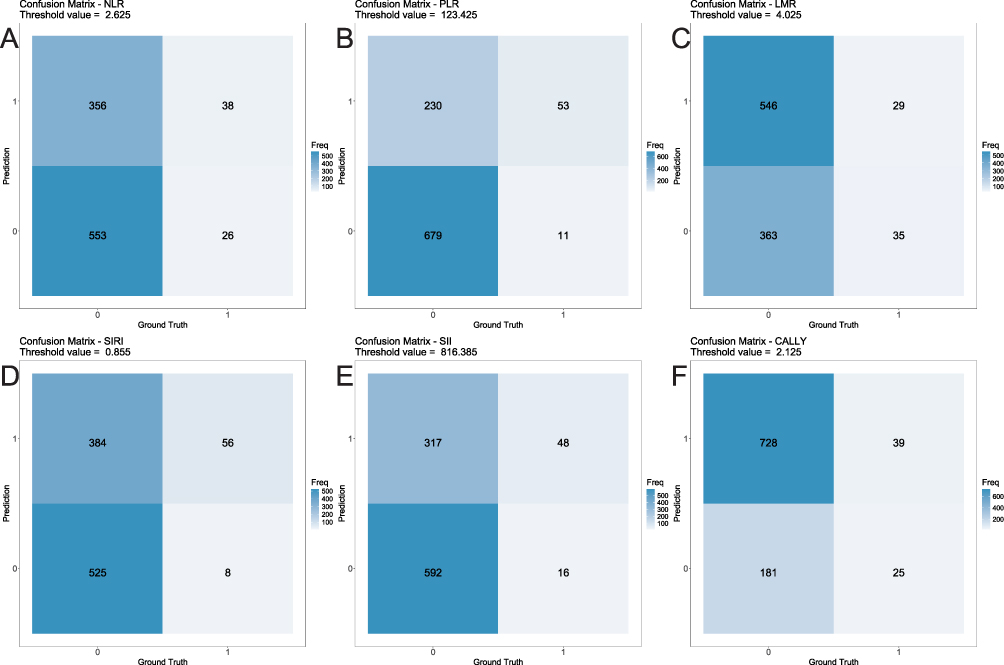 |
Figure 4 Confusion Matrix Analysis for Predicting ACS Occurrence Using Various Inflammatory Indices. (A) NLR; (B) PLR; (C) LMR, (D) SIRI; (E) SII; (F) CALLY. |
Discussion
In this retrospective study, we evaluated the predictive capacity of multiple inflammatory indices for the transition from CCS to ACS. The underlying mechanism driving the link between elevated inflammatory indices and ACS may involve the systemic and localized inflammatory processes that contribute to plaque instability, rupture, and subsequent thrombotic events leading to ACS.21 Chronic inflammation was known to promote endothelial dysfunction, facilitate lipid accumulation within arterial walls, and lead to the formation of vulnerable atherosclerotic plaques.22 The inflammatory milieu also enhances the recruitment and activation of immune cells within the plaque, creating an environment conducive to plaque rupture. The subsequent exposure of thrombogenic material in the blood can precipitate acute events such as myocardial infarction, characterizing the transition from CCS to ACS.23,24
PLR, identified as the most robust predictor in our study, reflects the inflammatory and thrombotic responses associated with ACS. Elevated Plt can enhance thrombus formation and contribute to vascular complications, while a decrease in lymphocyte count, often observed in stress responses, was indicative of immune dysregulation. The combined evaluation of platelet and lymphocyte counts in PLR provides an integrative assessment of these processes.25,26 Our findings were consistent with previous studies that have identified PLR as a significant predictor of adverse cardiovascular outcomes, emphasizing its potential utility as a simple, cost-effective marker for ACS risk stratification.12,27
The SIRI emerged as another potent predictor of ACS progression, displaying high odds ratios in multivariate analyses. SIRI combines monocyte, neutrophil, and lymphocyte counts, capturing different facets of the inflammatory response. Mon play a critical role in atherogenesis; they infiltrate the arterial intima, differentiate into macrophages, and contribute to foam cell formation.11,12 Neu, on the other hand, were key players in acute inflammatory responses and have been implicated in plaque destabilization through the release of proteolytic enzymes and reactive oxygen species.28,29 The predictive value of SIRI in our study underscores the importance of these cellular players in precipitating acute coronary events, suggesting that SIRI could be a valuable marker for early identification of high-risk patients.
The SII, another composite index calculated from platelet, neutrophil, and lymphocyte counts, demonstrated significant predictive capability. The SII reflects the balance between various inflammatory and immunological responses, encapsulating the complex interplay between thrombosis and inflammation.30 This index has gained attention in recent years for its prognostic utility in cardiovascular diseases, supporting the notion that systemic inflammation and thrombus formation were intimately linked processes in atherosclerosis.31,32 Our findings lend further support to the use of SII as a reliable indicator of ACS risk, advocating for its integration into clinical protocols for comprehensive patient assessment.
While the NLR also indicated some degree of predictive value for ACS, its utility was slightly less pronounced compared to PLR, SIRI, and SII. Nevertheless, NLR still provides valuable insights into the inflammatory burden present in CAD, particularly given the ease with which it can be determined from standard blood tests.33
Our study did not find significant predictive power for the LMR or the CALLY in forecasting ACS occurrence. This may be attributed to the complex nature of inflammatory processes involved in atherosclerosis that might not be fully captured by these indices alone. For instance, while LMR considers immune cell ratios, it might not adequately reflect the full inflammatory spectrum associated with ACS.34 Similarly, CALLY, which incorporates Alb and CRP, might not be as sensitive in detecting nuanced changes pertinent to coronary instability.35
Interestingly, metabolic parameters such as increased BMI, diabetes prevalence, and lipid profile anomalies were also significantly associated with ACS progression. These metabolic factors interplay with inflammatory processes to exacerbate endothelial dysfunction and accelerate plaque progression and instability.36,37 Insulin resistance and hyperglycemia, common features of diabetes, promote oxidative stress and inflammatory cytokine production, further advancing atherosclerotic disease.38 The association of these metabolic parameters with ACS highlights the need for comprehensive management strategies addressing both inflammation and metabolic disease to mitigate ACS risk.
Moreover, our study identified age as a significant demographic factor associated with ACS progression. This aligns with the ESC CCS guidelines, which highlight the importance of risk stratification in CCS populations. In our cohort, 6.58% (64/973) of CCS patients progressed to ACS within one year. While this exceeds the annualized rate of approximately 4% for major adverse cardiovascular events reported in lower-risk CCS cohorts,39 it is consistent with studies focusing on elderly patients with multiple comorbidities, underscoring the high-risk profile of our population and the need for enhanced predictive tools. Aging was naturally accompanied by increased systemic inflammation and was considered a risk factor for both atherosclerosis and its complications. The positive correlation of age with ACS reflects the cumulative effect of prolonged exposure to cardiovascular risk factors, endothelial damage, and chronic inflammation.40,41
The strengths of our study include a large sample size and the use of routinely collected hematological and biochemical markers, enhancing the translational potential of our findings. However, several limitations should be acknowledged. Firstly, as a retrospective analysis, our study may be subject to inherent biases, and prospective studies are warranted to validate these findings. Additionally, while inflammatory indices were promising, optimal thresholds for risk stratification remain to be established and should be tailored at the population level. Secondly, although we noted significant associations with diabetes and other metabolic parameters, results were not stratified by key demographics (eg, diabetic vs non-diabetic, male vs female). Future analyses could provide more nuanced insights into how these factors influence ACS risk. Thirdly, given the complexity of comparisons between CCS and ACS, as well as those who progressed from CCS to ACS, this manuscript could benefit from being divided into two separate studies. One focusing on chronic coronary syndrome versus ACS, and another comparing those who progressed from CCS to ACS. This would enhance clarity and readability, making the results clearer to the reader. Lastly, the length and complexity of the results section make it challenging to follow. Dividing the manuscript into two parts would significantly improve the presentation of data, making it less tiring to read and more informative.
Conclusion
In conclusion, the strong association of PLR, SIRI, and SII with ACS occurrence provides compelling evidence of their potential role as prognostic markers in coronary atherosclerosis. These indices offer significant advantages by reflecting underlying inflammatory pathology, which was critical in ACS development. Incorporating these markers in clinical practice could enhance risk assessment and guide therapeutic interventions, ultimately improving outcomes for patients with CAD. Future studies should focus on elucidating precise pathways linking systemic inflammation to coronary plaque rupture and explore interventions targeting these inflammatory pathways as potential therapeutic strategies.
Data Sharing Statement
The datasets used during the present study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
This exemption and the study itself were approved by the Ethics Committee of the Second Affiliated Hospital of Nanchang University. The study was conducted in accordance with the principles of the Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors have no conflicts of interest to declare in this work.
References
1. Doenst T, Thiele H, Haasenritter J, Wahlers T, Massberg S, Haverich A. The treatment of coronary artery disease. Dtsch Arztebl Int. 2022;119:716–723. doi:10.3238/arztebl.m2022.0277
2. Duggan JP, Peters AS, Trachiotis GD, Antevil JL. Epidemiology of coronary artery disease. Surg Clin North Am. 2022;102:499–516. doi:10.1016/j.suc.2022.01.007
3. Atwood J. Management of acute coronary syndrome. Emerg Med Clin North Am. 2022;40:693–706. doi:10.1016/j.emc.2022.06.008
4. Bulnes JF, González L, Velásquez L, Orellana MP, Venturelli PM, Martínez G. Role of inflammation and evidence for the use of colchicine in patients with acute coronary syndrome. Front Cardiovasc Med. 2024;11:1356023. doi:10.3389/fcvm.2024.1356023
5. Napoli G, Pergola V, Basile P, et al. Epicardial and pericoronary adipose tissue, coronary inflammation, and acute coronary syndromes. J Clin Med. 2023;12:7212. doi:10.3390/jcm12237212
6. Tuzimek A, Dziedzic EA, Beck J, Kochman W. Correlations between acute coronary syndrome and novel inflammatory markers (systemic immune-inflammation index, systemic inflammation response index, and aggregate index of systemic inflammation) in patients with and without diabetes or prediabetes. J Inflamm Res. 2024;17:2623–2632. doi:10.2147/JIR.S454117
7. Adali MK, Buber I, Kilic O, Turkoz A, Yilmaz S. Ticagrelor improves systemic immune-inflammation index in acute coronary syndrome patients. Acta Cardiol. 2022;77:632–638. doi:10.1080/00015385.2021.1973770
8. Gao Y, Li Y, Chen X, et al. The systemic inflammation index predicts poor clinical prognosis in patients with initially diagnosed acute coronary syndrome undergoing primary coronary angiography. J Inflamm Res. 2023;16:5205–5219. doi:10.2147/JIR.S435398
9. Wang X, Wei C, Fan W, et al. Advanced lung cancer inflammation index for predicting prognostic risk for patients with acute coronary syndrome undergoing percutaneous coronary intervention. J Inflamm Res. 2023;16:3631–3641. doi:10.2147/JIR.S421021
10. Dziedzic EA, Gąsior JS, Tuzimek A, Dąbrowski M, Jankowski P. The association between serum vitamin d concentration and new inflammatory biomarkers-systemic inflammatory index (SII) and systemic inflammatory response (SIRI)-In patients with ischemic heart disease. Nutrients. 2022;14:4212. doi:10.3390/nu14194212
11. Han K, Shi D, Yang L, et al. Prognostic value of systemic inflammatory response index in patients with acute coronary syndrome undergoing percutaneous coronary intervention. Ann Med. 2022;54:1667–1677. doi:10.1080/07853890.2022.2083671
12. Rajakumar HK, Coimbatore Sathyabal V, Vasanthan M, Dasarathan R. The predictive role of Systemic Inflammation Response Index (SIRI), Neutrophil-Lymphocyte Ratio (NLR), and Platelet-Lymphocyte Ratio (PLR) in the prognosis of acute coronary syndrome in a tertiary care hospital. Heliyon. 2024;10:e39029. doi:10.1016/j.heliyon.2024.e39029
13. Gu L, Xia Z, Qing B, et al. Systemic Inflammatory Response Index (SIRI) is associated with all-cause mortality and cardiovascular mortality in population with chronic kidney disease: evidence from NHANES (2001-2018). Front Immunol. 2024;15:1338025. doi:10.3389/fimmu.2024.1338025
14. Nascimento MAL, Ferreira LGR, Alves TVG, Rios DRA. Inflammatory hematological indices, cardiovascular disease and mortality: a narrative review. Arq Bras Cardiol. 2024;121:e20230752. doi:10.36660/abc.20230752
15. Xia Y, Xia C, Wu L, Li Z, Li H, Zhang J. Systemic Immune Inflammation Index (SII), System Inflammation Response Index (SIRI) and Risk of All-Cause Mortality and Cardiovascular Mortality: a 20-Year Follow-Up Cohort Study of 42,875 US Adults. J Clin Med. 2023;12:1128. doi:10.3390/jcm12031128
16. Ford TJ, Corcoran D, Berry C. Stable coronary syndromes: pathophysiology, diagnostic advances and therapeutic need. Heart. 2018;104:284–292. doi:10.1136/heartjnl-2017-311446
17. Bhatt DL, Lopes RD, Harrington RA. Diagnosis and treatment of acute coronary syndromes: a review. JAMA. 2022;327:662–675. doi:10.1001/jama.2022.0358
18. Dziedzic EA, Gąsior JS, Tuzimek A, et al. Investigation of the Associations of Novel Inflammatory Biomarkers-Systemic Inflammatory Index (SII) and systemic inflammatory response index (SIRI)-with the severity of coronary artery disease and acute coronary syndrome occurrence. Int J Mol Sci. 2022;23:9553. doi:10.3390/ijms23179553
19. Chen K, Liu Y, Xu B, et al. Relationship between the lymphocyte to C‑reactive protein ratio and coronary artery disease severity. Exp Ther Med. 2024;27:60. doi:10.3892/etm.2023.12348
20. Tudurachi BS, Anghel L, Tudurachi A, Sascău RA, Stătescu C. Assessment of inflammatory hematological ratios (NLR, PLR, MLR, LMR and Monocyte/HDL-Cholesterol Ratio) in acute myocardial infarction and particularities in young patients. Int J Mol Sci. 2023;24:14378. doi:10.3390/ijms241814378
21. Cimmino G, Di Serafino L, Cirillo P. Pathophysiology and mechanisms of Acute Coronary Syndromes: atherothrombosis, immune-inflammation, and beyond. Expert Rev Cardiovasc Ther. 2022;20:351–362. doi:10.1080/14779072.2022.2074836
22. Malekmohammad K, Bezsonov EE, Rafieian-Kopaei M. Role of lipid accumulation and inflammation in atherosclerosis: focus on molecular and cellular mechanisms. Front Cardiovasc Med. 2021;8:707529. doi:10.3389/fcvm.2021.707529
23. Nardin M, Verdoia M, Laera N, Cao D, De Luca G. New insights into pathophysiology and new risk factors for ACS. J Clin Med. 2023;12:2883. doi:10.3390/jcm12082883
24. Laera N, Malerba P, Vacanti G, Nardin S, Pagnesi M, Nardin M. Impact of immunity on coronary artery disease: an updated pathogenic interplay and potential therapeutic strategies. Life. 2023;13. doi:10.3390/life13112128
25. Karadeniz F, Karadeniz Y, Altuntaş E. Systemic immune-inflammation index, and neutrophil-to-lymphocyte and platelet-to-lymphocyte ratios can predict clinical outcomes in patients with acute coronary syndrome. Cardiovasc J Afr. 2023;34:1–7. doi:10.5830/CVJA-2023-011
26. Kazem N, Hofer F, Koller L, et al. The age-specific prognostic impact of the platelet-to-lymphocyte ratio on long-term outcome after acute coronary syndrome. Eur Heart J Open. 2022;2:oeab031. doi:10.1093/ehjopen/oeab031
27. Li Q, Ma X, Shao Q, et al. Prognostic impact of multiple lymphocyte-based inflammatory indices in acute coronary syndrome patients. Front Cardiovasc Med. 2022;9:811790. doi:10.3389/fcvm.2022.811790
28. Wang H, Huang Z, Wang J, et al. Predictive value of system immune-inflammation index for the severity of coronary stenosis in patients with coronary heart disease and diabetes mellitus. Sci Rep. 2024;14:31370. doi:10.1038/s41598-024-82826-5
29. Wang H, Jiang M, Li X, et al. Anti-inflammatory therapies for coronary heart disease: a systematic review and meta-analysis. Front Cardiovasc Med. 2021;8:726341. doi:10.3389/fcvm.2021.726341
30. Bani Hani DA, Alshraideh JA, Saleh A, Alduraidi H, Alwahadneh AA, Al-Zaiti SS. Lymphocyte-based inflammatory markers: novel predictors of significant coronary artery disease(✰,✰✰). Heart Lung. 2024;70:23–29. doi:10.1016/j.hrtlng.2024.11.006
31. Candemir M, Kiziltunç E, Nurkoç S, Şahinarslan A. Relationship between systemic immune-inflammation index (SII) and the severity of stable coronary artery disease. Angiology. 2021;72:575–581. doi:10.1177/0003319720987743
32. Zhao Z, Lian H, Liu Y, Sun L, Zhang Y. Application of systemic inflammation indices and lipid metabolism-related factors in coronary artery disease. Coron Artery Dis. 2023;34:306–313. doi:10.1097/MCA.0000000000001239
33. Luo J, Zhou Y, Song Y, et al. Association between the neutrophil-to-lymphocyte ratio and in-hospital mortality in patients with chronic kidney disease and coronary artery disease in the intensive care unit. Eur J Med Res. 2024;29:260. doi:10.1186/s40001-024-01850-3
34. Abramavičiūtė A L, Mongirdienė A, Laukaitienė J. Relationship between inflammatory readings and the degree of coronary atherosclerosis (Pilot Study). J Clin Med. 2024;14. doi:10.3390/jcm14010122
35. Pan Y, Wu TT, Deng CJ, et al. Association between the C-Reactive Protein-Albumin-Lymphocyte (CALLY) Index and Adverse Clinical Outcomes in CAD Patients after PCI: findings of a real-world study. Rev Cardiovasc Med. 2024;25:111. doi:10.31083/j.rcm2504111
36. Talmor-Barkan Y, Bar N, Shaul AA, et al. Metabolomic and microbiome profiling reveals personalized risk factors for coronary artery disease. Nat Med. 2022;28:295–302. doi:10.1038/s41591-022-01686-6
37. Siagian SN, Christianto C, Angellia P, Holiyono HI. The risk factors of acute coronary syndrome in young women: a systematic review and meta-analysis. Curr Cardiol Rev. 2023;19:e161122210969. doi:10.2174/1573403X19666221116113208
38. Chen Q, Xiong S, Ye T, et al. Insulin resistance, coronary artery lesion complexity and adverse cardiovascular outcomes in patients with acute coronary syndrome. Cardiovasc Diabetol. 2024;23:172. doi:10.1186/s12933-024-02276-1
39. Vrints C, Andreotti F, Koskinas KC, et al. 2024 ESC Guidelines for the management of chronic coronary syndromes. Eur Heart J. 2024;45:3415–3537. doi:10.1093/eurheartj/ehae177
40. Carvalho PR, Bernardo MC, Carvalho CR, et al. Age shock index as an early predictor of cardiovascular death in acute coronary syndrome patients. Coron Artery Dis. 2024;35:322–327. doi:10.1097/MCA.0000000000001342
41. Georgiopoulos G, Kraler S, Mueller-Hennessen M, et al. MODIFICATION of the GRACE Risk Score for Risk Prediction in Patients With Acute Coronary Syndromes. JAMA Cardiol. 2023;8:946–956.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Neutrophil-to-Lymphocyte Ratio Can Distinguish Patients with Liver Cirrhosis from Healthy People but Cannot Distinguish Patients with Cirrhotic Hepatocellular Carcinoma from Patients with Liver Cirrhosis
Zhu X, Zhou H
Journal of Hepatocellular Carcinoma 2022, 9:1127-1136
Published Date: 29 October 2022
The Platelet-to-Lymphocyte Ratio Predicts Diabetic Retinopathy in Type 2 Diabetes Mellitus
Zeng J, Chen M, Feng Q, Wan H, Wang J, Yang F, Cao H
Diabetes, Metabolic Syndrome and Obesity 2022, 15:3617-3626
Published Date: 22 November 2022
Association of Neutrophil-to-Lymphocyte Ratio and Platelet-to-Lymphocyte Ratio with Diabetic Kidney Disease in Chinese Patients with Type 2 Diabetes: A Cross-Sectional Study
Li L, Shen Q, Rao S
Therapeutics and Clinical Risk Management 2022, 18:1157-1166
Published Date: 28 December 2022
Low-Grade Inflammation in Gestational Diabetes Mellitus and Its Correlation with Maternal Insulin Resistance and Fetal Growth Indices
Xuan Nguyen K, Bui Minh T, Dinh HT, Viet Tran T, Dinh Le T, Phi Thi Nguyen N, Tran TTH, Hien Vu T, Ho Thi Nguyen L, Trung Nguyen K, Huy Thong N, Do K, Nguyen TK, Nguyen Dao H, Tien Nguyen S
International Journal of General Medicine 2023, 16:1429-1436
Published Date: 20 April 2023
Preoperative Inflammation-Associated Blood Cell Markers in Patients with Non-Metastatic Clear Cell Renal Cell Carcinoma: A Retrospective Study
Cheng Y, Kou W, Zhu Y
International Journal of General Medicine 2023, 16:3067-3080
Published Date: 19 July 2023