Back to Journals » Infection and Drug Resistance » Volume 19
Prevalence, Clinical Features and Factors Associated with Hypercalcemia Among Patients Diagnosed with Tuberculosis at Lira Regional Referral Hospital, Northern Uganda: A Cross-Sectional Study
Authors Ahmed Jnr AH ![]() , Onyanga N, Adam Deifa AA, Ali HO, Nor FI, Hussein ZA, Mohamed AM, Hashi NA, Hassan MA
, Onyanga N, Adam Deifa AA, Ali HO, Nor FI, Hussein ZA, Mohamed AM, Hashi NA, Hassan MA ![]() , Hirsi AM, Jayte M
, Hirsi AM, Jayte M
Received 21 January 2026
Accepted for publication 30 March 2026
Published 3 April 2026 Volume 2026:19 597775
DOI https://doi.org/10.2147/IDR.S597775
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hazrat Bilal
Abdullahi Hussein Ahmed Jnr,1 Nixson Onyanga,1 Abdalla Ahmed Adam Deifa,1 Hassan Omar Ali,1 Fatima Ibrahim Nor,1 Zakarie Abdullahi Hussein,1 Abdijibar Mohamud Mohamed,2 Najma Ali Hashi,3 Mohamed Abdi Hassan,2 Abshir Mohamud Hirsi,1 Mohamed Jayte1
1Department of Internal Medicine, Faculty of Clinical Medicine and Dentistry, Kampala International University, Ishaka, Bushenyi, Uganda; 2Department of Pediatric and Child Health, faculty of clinical Medicine and Dentistry, Kampala International University, Ishaka, Bushenyi, Uganda; 3Department of Obstetrics and Gynecology, faculty of clinical Medicine and Dentistry, Kampala International University, Ishaka, Bushenyi, Uganda
Correspondence: Abdullahi Hussein Ahmed Jnr, Department of Internal Medicine, faculty of clinical Medicine and Dentistry, Kampala International University, Ishaka, Bushenyi, Uganda, Email [email protected]
Background: Tuberculosis (TB) remains a leading cause of morbidity and mortality globally. Hypercalcemia, a recognized complication of TB, is often asymptomatic but may cause significant clinical consequences. In Uganda, routine screening for hypercalcemia in TB patients is limited, and data on its prevalence and associated factors are scarce. This study aimed to determine the prevalence, clinical features, and factors associated with hypercalcemia among TB patients at Lira Regional Referral Hospital (LRRH).
Methods: A cross-sectional study was conducted among 180 adult TB patients attending the LRRH TB clinic. Socio-demographic, clinical, and laboratory data were collected using structured questionnaires. Total serum calcium was measured using colorimetric method, with hypercalcemia defined as adjusted calcium > 10.5 mg/dL. Logistic regression was used to identify factors independently associated with hypercalcemia, with significance set at p< 0.05.
Results: Of the 180 participants (mean age 41.3± 15.7 years; 54.4% female), 50 had hypercalcemia, giving a prevalence of 27.8% (95% CI: 21.1– 34.4%). The most frequent symptoms associated with hypercalcemia were constipation (74.0%), polyuria (60.0%), and polydipsia (70.0%), all p< 0.05. Independent predictors of hypercalcemia included elderly age (aOR=3.075; 95% CI: 1.035– 7.139; p=0.043), HIV positivity (aOR=2.001; 95% CI: 1.254– 5.631; p=0.011), and elevated creatinine (aOR=3.648; 95% CI: 1.510– 6.517; p=0.006).
Conclusion: The prevalence of hypercalcemia among TB patients in northern Uganda is high. Routine calcium screening should be considered, particularly among elderly patients, those with HIV infection, and those with renal impairment, to enable early detection and management.
Keywords: tuberculosis, hypercalcemia, prevalence, HIV, renal impairment, Uganda, lira regional referral hospital
Introduction
Tuberculosis (TB) has been identified in historical records dating back to ancient civilizations, with skeletal evidence from Egyptian mummies and early medical writings confirming its long-standing presence.1,2 Despite modern advancements in diagnostics and therapy, TB persists as a major global health threat, ranking among the top infectious disease killers with approximately 10 million new cases and over 1 million deaths annually.3
A notable complication of TB is hypercalcemia, defined as abnormally high serum calcium levels, which frequently occurs in granulomatous disorders.4,5 The underlying mechanism involves excessive calcitriol synthesis by activated macrophages within granulomatous lesions.6,7 While sometimes clinically silent, hypercalcemia can lead to severe consequences such as acute kidney injury, cardiac arrhythmias, and neurological disturbances.8,9
The burden of TB is heavily concentrated in low-resource settings, particularly sub-Saharan Africa.10 Regional studies report widely varying hypercalcemia prevalence among TB patients, ranging from 12% to over 60%, with discrepancies attributed to differences in dietary vitamin D, ultraviolet light exposure, and diagnostic methodologies.11–14
Uganda, designated by the WHO as a high-burden country for both TB and HIV, has an estimated TB prevalence of 253 cases per 100,000 population.15 Despite this, hypercalcemia screening remains uncommon in Ugandan TB patients due to resource constraints. No local studies have yet investigated its prevalence or risk factors, though such data could optimize screening practices and clinical outcomes.
Most of the patients with high calcium remain asymptomatic, and hypercalcemia is diagnosed on routine screening or when they develop complications. In a resource-limited setting like Uganda, routine calcium screening of TB patients is not feasible. Undiagnosed hypercalcemia in TB may worsen disease progression, prolong hospitalization, and increase mortality risk.16,17 The current lack of region-specific evidence on its epidemiology and associated variables hinders evidence-based management and policy formulation.
This study will bridge this critical knowledge gap. The study aimed to assess the prevalence, clinical manifestations, and determinants of hypercalcemia among TB patients in northern Uganda. The results will support targeted screening initiatives and enhance patient care strategies.
Methods
Study Design and Setting
This cross-sectional study was conducted at Lira Regional Referral Hospital (LRRH), the primary referral center for the Lango sub-region in northern Uganda. The hospital’s TB clinic operates daily and adheres to Uganda’s national TB management protocols. Data was collected in the months of April, May and June 2025.
Study Population
Eligible participants included adults (≥18 years) with microbiologically or clinically confirmed TB attending the clinic during the study period. Exclusion criteria comprised known malignancy, sarcoidosis, thyrotoxicosis, primary hyperparathyroidism, or current use of medications affecting calcium metabolism. The patients on calcium supplements or vitamin D supplements were also excluded.
Sample Size and Sampling
The sample size was calculated using Kish Leslie’s formula, with an assumed hypercalcemia prevalence (*p*) of 12% based on prior Nigerian data.11 A minimum of 163 participants was required; after adjusting for a 10% non-response rate, the target enrollment was set at 180. Consecutive sampling was employed until the desired sample size was achieved.
Data Collection Procedures
Trained research assistants collected socio-demographic and clinical data through structured interviews. Anthropometric measurements, including body mass index (BMI), were recorded for nutritional assessment. Venous blood samples were drawn for serum calcium, creatinine, and HIV testing. The duration of TB since diagnosis was also recorded and classified as less than one month or at least one month. During data collection, care was taken to ensure that all sections were fully filled. After each data collection session, the questionnaire was proof checked for blank spaces, and if found, they were filled.
Laboratory Methods
Total serum calcium was measured using the colorimetric method. Albumin was measured to determine the adjusted calcium. Hypercalcemia was defined as adjusted calcium level exceeding 10.5 mg/dL.
Statistical Analysis
Data analysis was performed using SPSS version 26. The prevalence of hypercalcemia was reported as a proportion with a 95% confidence interval (CI). Categorical variables were analyzed using chi-square tests, while logistic regression identified predictors of hypercalcemia. Variables with p < 0.2 in bivariable analysis were included in the final multivariable model.
Ethical Considerations
This study complies with the Declaration of Helsinki. Approval was obtained from the Kampala International University (KIU) Research Ethics Committee and LRRH administration. All participants provided written informed consent prior to enrollment.
Results
Characteristics of the Study Participants
In this research, we enrolled 180 participants with TB. Almost two third (59.4%) were middle aged adults. Slightly over half (54.4%) were female. Majority (84.4%) had been with tuberculosis for less than one month. The details are shown in Table 1 below.
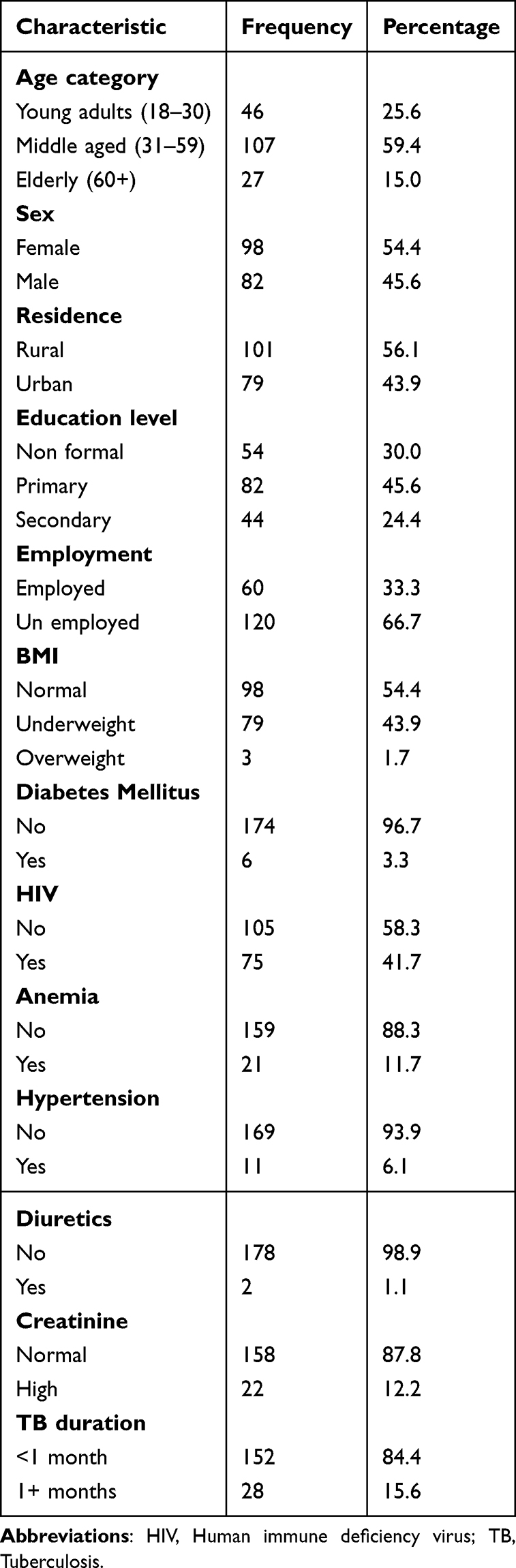 |
Table 1 Characteristics of Study Participants |
Prevalence of Hypercalcemia Among Patients Diagnosed with Tuberculosis at LRRH
Of the 180 participants enrolled, 50 were found to have hypercalcemia, representing a prevalence of 27.8%, with a 95% confidence interval of 21.1–34.4% (Figure 1).
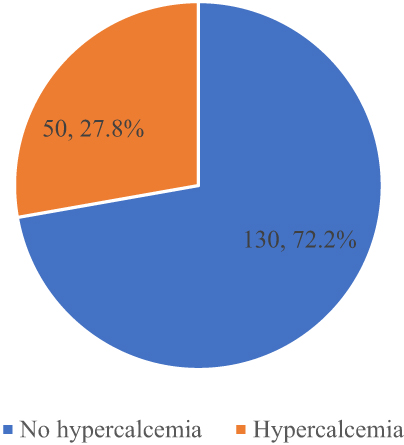 |
Figure 1 Prevalence of hypercalcemia among patients diagnosed with tuberculosis at LRRH. |
Clinical Features Associated with Hypercalcemia Among Patients Diagnosed with TB at LRRH
The three clinical features that were importantly linked to hypercalcemia of the individuals diagnosed with tuberculosis at LRRH were constipation, polyuria and polydipsia. These clinical features were significantly higher among the participants with hypercalcemia compared to those who did not have hypercalcemia with 70.0% versus 49.2% for polydipsia, 60.0% versus 35.4% for polyuria and 74.0% versus 46.9% for constipation (P<0.05 for all the three) as shown in Table 2 below.
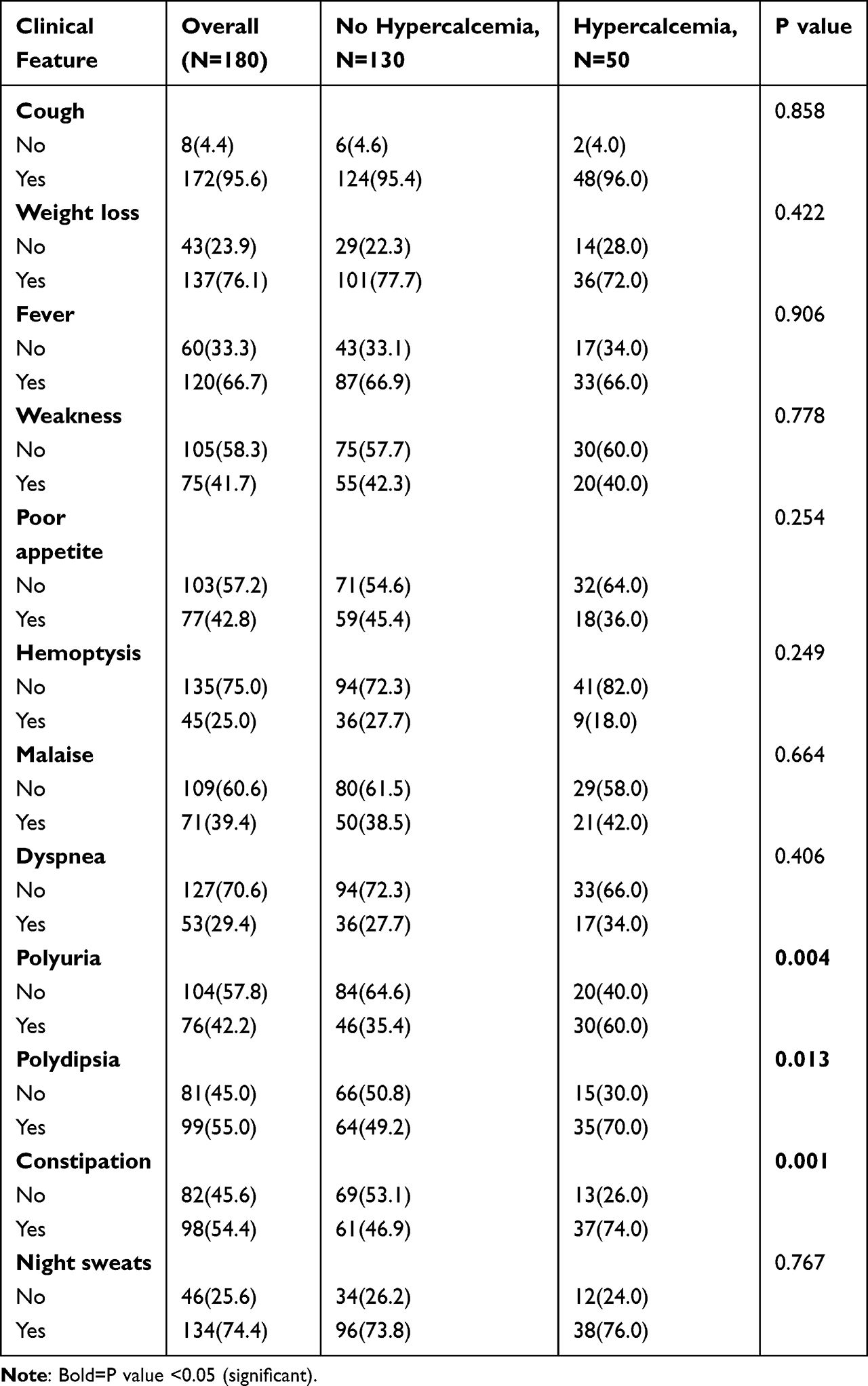 |
Table 2 Clinical Features Associated with Hypercalcemia Among Patients Diagnosed with Tuberculosis at LRRH |
Factors Associated with Hypercalcemia Among Patients Diagnosed with TB at LRRH
The variables considered for multivariate analysis (P<0.2) were: age category, HIV status, creatinine level and duration of tuberculosis as detailed in Table 3 below.
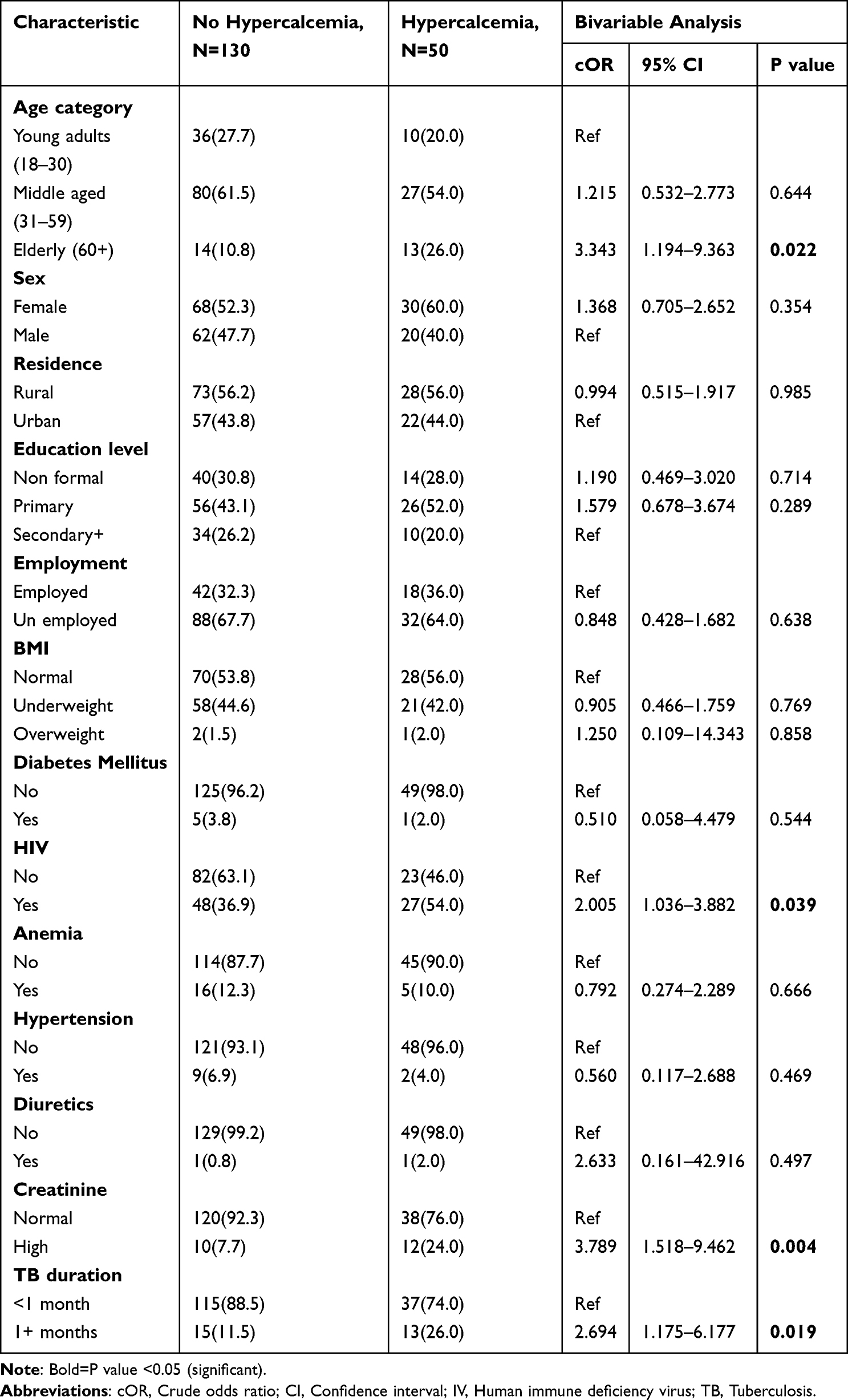 |
Table 3 Bivariable Analysis of Factors Associated with Hypercalcemia Among Patients Diagnosed with Tuberculosis at LRRH |
In the multivariable analysis, the independent determinants linked to hypercalcemia of the individuals diagnosed having TB at LRRH were: being elderly (aOR=3.075, CI=1.035–7.139, P=0.043), being HIV positive (aOR=2.001, CI=1.254–5.631, P=0.011) and having high creatinine (aOR=3.648, CI=1.510–6.517, P=0.006). The odds for hypercalcemia were increased by over 3 times for those who were elderly, by over 2 times for those that were HIV positive and by over 3.5 times for those who had high creatinine. The details are shown in Table 4 below.
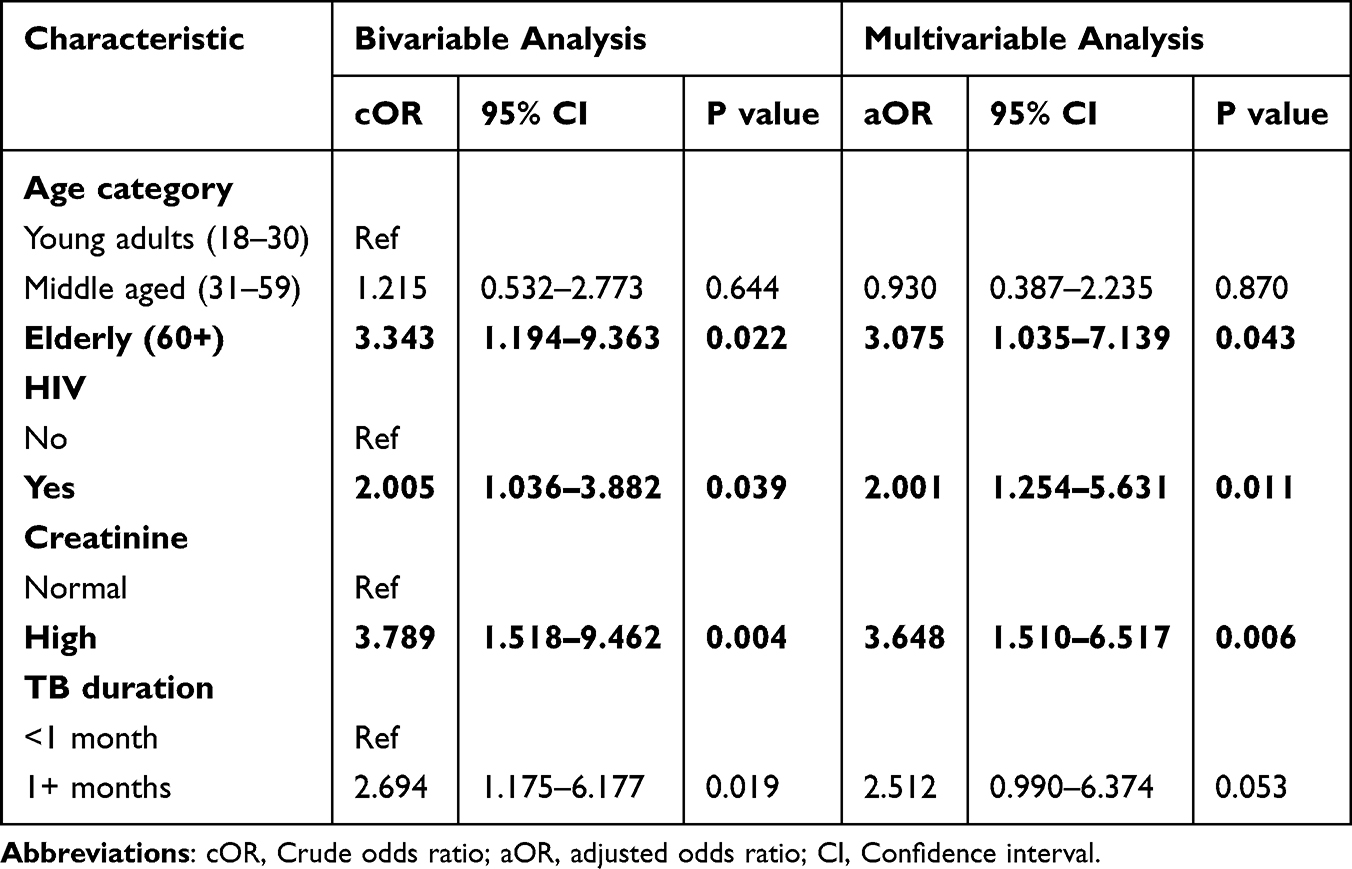 |
Table 4 Multivariable Analysis of Factors Associated with Hypercalcemia Among Patients Diagnosed with Tuberculosis at LRRH |
Discussion
This study investigated the prevalence, clinical features, and risk factors of hypercalcemia among tuberculosis patients at Lira Regional Referral Hospital in northern Uganda. Among 180 enrolled participants, we found a hypercalcemia prevalence of 27.8% (50 cases), with significant variations observed when compared to other regions. Our findings align with studies from Greece (25%)14 and Nigeria (27.5%),11 while showing higher rates than reported in India (20.15%)13 and lower rates than found in Ethiopia (52.3%)15 and Pakistan (71.3%).16 These geographical differences likely reflect variations in HIV co-infection rates, study methodologies, and population characteristics.
The clinical presentation of hypercalcemia in our TB patients was characterized by three predominant symptoms: constipation (74% prevalence among hypercalcemic patients versus 46.9% in normocalcemic patients), polyuria (60% versus 35.4%), and polydipsia (70% versus 49.2%). The constipation results from calcium-induced slowing of intestinal motility, while polyuria occurs due to calcium-mediated interference with renal concentrating ability through aquaporin-2 channel downregulation and direct effects on the loop of Henle. Polydipsia develops secondary to the water loss from polyuria, creating a compensatory thirst response. These findings are mechanistically explained by calcium’s effects on gastrointestinal motility and renal function, as previously described in the literature.17
Multivariable logistic regression analysis identified three independent risk factors for hypercalcemia in our TB population. Elderly patients (≥60 years) showed 3.1-fold increased odds (aOR 3.1) of developing hypercalcemia compared to younger patients, consistent with known age-related declines in calcium homeostasis mechanisms.18 HIV co-infection was associated with 2.4-fold greater odds (aOR 2.4), potentially through immune reconstitution inflammatory syndrome (IRIS)-mediated overproduction of calcitriol by granuloma macrophages.19 Patients with elevated creatinine levels demonstrated 3.5-fold increased risk (aOR 3.5), reflecting the critical role of renal function in calcium excretion and homeostasis.20 However, it is important to note that the association with elevated creatinine could be bidirectional as hypercalcemia causes renal impairment, and renal impairment reduces calcium excretion. However, the cross-sectional design used in this study could cannot determine directionality.
These findings carry important clinical implications for TB management in similar high-burden settings. The relatively high prevalence of hypercalcemia, particularly among elderly, HIV-positive, and renally impaired patients, suggests that targeted calcium monitoring should be considered in these high-risk groups. The characteristic symptom triad of constipation, polyuria, and polydipsia can serve as valuable clinical indicators for hypercalcemia in resource-limited settings where laboratory testing may not be routinely available.
Several limitations should be acknowledged when interpreting these results. The single-center design may affect generalizability to other settings. The cross-sectional nature prevents assessment of causality or hypercalcemia’s impact on long-term TB outcomes. Additionally, we did not measure parathyroid hormone or vitamin D levels, which could have provided further mechanistic insights into the observed hypercalcemia cases. Consecutive sampling was used and this non-probability sampling may have introduced selection bias.
Hypercalcemia, identified in about 28% of patients, necessitates targeted monitoring in elderly, HIV-positive, and renal-impaired tuberculosis cases. Clinical management should include screening for a triad of constipation, polyuria, and polydipsia to guide diagnosis, especially in resource-limited settings guidelines may enhance immune recovery and overall patient outcomes.
Conclusion
The prevalence of hypercalcemia among TB patients at Lira Regional Referral Hospital was high, affecting over one-quarter of the study population. Constipation, polyuria, and polydipsia were the clinical features most strongly associated with hypercalcemia. Elderly age, HIV positivity, and elevated creatinine emerged as independent predictors.
Recommendations
Routine screening for hypercalcemia should be considered for all TB patients to facilitate early diagnosis; more especially the elderly, HIV-positive, and those with renal impairment. Serial renal function tests should be incorporated into routine TB care to enable early detection and management of renal diseases, thereby preventing hypercalcemia. Additionally, further research is needed to determine optimal strategies for managing elderly TB patients with the aim of reducing hypercalcemia risk.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Ethical Approval and Consent to Participate
The study received ethical approval from the Research Ethics Committee of Kampala International University (Ref No: KIU-2024-721). Written informed consent was obtained from all participants prior to their inclusion in the study.
Consent for Publication
Written informed consent was obtained from the participants for the publication of this study and any accompanying data.
Acknowledgments
The authors extend their sincere gratitude to all participants who took part in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare that they have no competing interests.
References
1. Barberis I, Bragazzi NL, Galluzzo L, Martini M. The history of tuberculosis: from the first historical records to the isolation of Koch’s bacillus. J Prev Med Hyg. 2017;58(1):E9–9.
2. Daniel TM, Iversen PA. Hippocrates and tuberculosis. Int J Tuberc Lung Dis. 2015;19(4):373–374. doi:10.5588/ijtld.14.0736
3. Prabhu M, Singh AK. Tuberculosis: a comprehensive clinical reference. Indian J Med Res. 2019;149(3):403–405.
4. Huang CT, Wu MF. Hypercalcemia in patients with tuberculosis. J Microbiol Immunol Infect. 2017;50(2):159–160.
5. Kavanaugh A, Adams C, Reichlin M, Duong C, Mandel D. Hypercalcemia in granulomatous diseases: pathophysiology and management. Clin Rheumatol. 2015;34(4):659–664.
6. Abebe M, Zegeye Bonsa Z. Prevalence of hypercalcemia among TB patients and associated factors. Ethiop Med J. 2017;55(3):233–240.
7. Dosumu EA, Momoh MA. Serum calcium levels in newly diagnosed pulmonary tuberculosis patients in Nigeria. Niger J Med. 2006;15(3):261–264.
8. Amare B, Moges B, Fantahun B, et al. Serum calcium and vitamin D levels in tuberculosis patients with and without HIV co-infection in Ethiopia. BMC Infect Dis. 2012;12:307. doi:10.1186/1471-2334-12-307
9. Oussos C, Rapti A, Tsirigotis P, Sotiropoulou C, Papadaki E, Roussos C. Hypercalcemia in patients with pulmonary tuberculosis. Respiration. 2001;68(4):343–348. doi:10.1159/000050524
10. John R, Mathew M, Paul TV, Rajaratnam S. Factors associated with hypercalcemia in tuberculosis patients: a case-control study. Indian J Tuberc. 2020;67(2):195–200.
11. Dosumu EA, Momoh JA. Hypercalcaemia in patients with tuberculosis in Ibadan, Nigeria. Afr J Med Med Sci. 2006;35(3):365–369.
12. Abbasi A, Corpeleijn E, Gansevoort RT, et al. Hypercalcemia in active pulmonary tuberculosis. J Clin Tuberc Other Mycobact Dis. 2017;8:1–5. doi:10.1016/j.jctube.2017.04.001
13. John J, Mathew M, Paul TV, Rajaratnam S. Hypercalcemia in tuberculosis: a retrospective case-control study from India. J Bone Miner Metab. 2020;38(5):692–697.
14. Oussos D, Rapti A, Tsirigotis P, Sotiropoulou C, Papadaki E, Roussos C. Hypercalcaemia in Greek patients with tuberculosis before the initiation of anti-tuberculosis treatment. Respir Med. 2001;95(3):187–190. doi:10.1053/rmed.2000.1019
15. Amare H, Gelaw A, Anagaw B, Gelaw B. Smear positive pulmonary tuberculosis and associated factors among homeless individuals in Dessie and Debre Birhan towns, Northeast Ethiopia. Ann Clin Microbiol Antimicrob. 2012;11:24.
16. Banu S, Hossain A, Uddin MK, et al. Hypercalcemia in tuberculosis: analysis of 1142 patients from a tertiary care center in Bangladesh. J Clin Tuberc Other Mycobact Dis. 2021;22:100205.
17. McIlroy G, McKee MD, Khan SR. Hypercalcemia and tuberculosis. QJM. 1999;92(5):287–291. doi:10.1093/qjmed/92.5.287
18. Raymakers JA. Calcium homeostasis in the elderly. Neth J Med. 1990;36(5–6):208–212.
19. Nongnuch A, Assanatham M, Wacharanawat S, Anutrakulchai S, Phrommintikul A. Hypercalcemia in HIV-infected patients: a 5-year retrospective study. HIV Med. 2020;21(9):591–597.
20. Iampornpipopchai P, Supasyndh O, Satirapoj B. Hypercalcemia and acute kidney injury in tuberculosis. Nephrology. 2014;19(7):431–436.
21. Pamart A, Bouvard B, Legrand E. Hypercalcemia in the elderly. Geriatr Psychol Neuropsychiatr Vieil. 2021;19(1):7–14.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Prevalence and Factors Associated with Hepatitis B Infection Among Outpatient Adults in South-Western Uganda
Rugaatwa Ndibarema E, Olum R, Ayebare D, Kabakyenga J
Hepatic Medicine: Evidence and Research 2022, 14:163-172
Published Date: 19 October 2022
Trends of Tuberculosis Disease from 2013–2018 in Bale Zone, Oromia Region, Ethiopia. Retrospective Review
Hasen Badeso M, Sani Kalil F, Mohammed Ahmed Y, Abdulkadir Godie S, Habtamu Regesu A
Infection and Drug Resistance 2022, 15:6723-6730
Published Date: 21 November 2022
Prevalence of HIV in Kazakhstan 2010–2020 and Its Forecasting for the Next 10 Years
Mussina K, Kadyrov S, Kashkynbayev A, Yerdessov S, Zhakhina G, Sakko Y, Zollanvari A, Gaipov A
HIV/AIDS - Research and Palliative Care 2023, 15:387-397
Published Date: 4 July 2023
Predictors of Tuberculosis and Non-Communicable Disease Comorbidities Among Newly Enrolled Tuberculosis Patients, Southern Ethiopia
Nunemo MH, Gidebo KD, Woticha EW, Lemu YK
Integrated Blood Pressure Control 2023, 16:95-109
Published Date: 22 November 2023
COPD in People with HIV: Epidemiology, Pathogenesis, Management, and Prevention Strategies
Byanova KL, Abelman R, North CM, Christenson SA, Huang L
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:2795-2817
Published Date: 29 November 2023