")
Back to Journals » Infection and Drug Resistance » Volume 15
Trends of Tuberculosis Disease from 2013–2018 in Bale Zone, Oromia Region, Ethiopia. Retrospective Review
Authors Hasen Badeso M , Sani Kalil F , Mohammed Ahmed Y , Abdulkadir Godie S , Habtamu Regesu A
Received 16 September 2022
Accepted for publication 17 November 2022
Published 21 November 2022 Volume 2022:15 Pages 6723—6730
DOI https://doi.org/10.2147/IDR.S384402
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Mohammed Hasen Badeso,1 Falaho Sani Kalil,1 Yusuf Mohammed Ahmed,2 Shemsedin Abdulkadir Godie,3 Ashenafi Habtamu Regesu4
1Field Epidemiology Training Program, Jimma University Jimma, Jimma, Oromia Regional State, Ethiopia; 2Health Emergency, World Health Organization, Nekemte, Oromia Regional State, Ethiopia; 3Department of Internal Medicine, Arsi University, Asella, Oromia Regional State, Ethiopia; 4Department of Public Health, Arsi University, Asella, Oromia Regional State, Ethiopia
Correspondence: Mohammed Hasen Badeso, Po.Box 61, Gindhir, Tel +251923728803, Email [email protected]
Purpose: Tuberculosis is a common global public health problem. Ethiopia is among the thirty top Tuberculosis burden countries. Trends of tuberculosis disease in general and at the district level in the Bale Zone have not been assessed and no adequate information existed for informed decision-making. This study was to describe the trends and physical distribution of the tuberculosis disease in the Bale Zone from 2013 to 2018.
Methods: We reviewed the reported data of tuberculosis from 2013 to 2018 in March 2019 and extracted data of tuberculosis from the Bale Zone health information system database. Analysis of the six-year data of tuberculosis was conducted after the data was cleaned and checked for completeness.
Results: We recruited a total of 11, 268 tuberculosis cases. The proportions of sputum smear-positive tuberculosis (SS+), sputum smear-negative tuberculosis (SS−), and extra-pulmonary tuberculosis (EPTB) cases were 40.4%, 29.6% and 30%, respectively. Of all cases, 81.9% are aged greater than 15 years. Prevalence of all types of tuberculosis was 0.005%, 0.127%, 0.133%, 0.136%, 0.131% and 0.093% in 2013, 2014, 2015, 2016, 2017 and 2018, respectively. The death rate from positive pulmonary tuberculosis was 0%. 2.74, 2.10, 2.06, 1.04, and 2.75 in 2013, 2014, 2015, 2016, 2017 and 2018, respectively. The highest average prevalence rate was 198, 152 and 142 per 100,000 populations in Berbere, Rayitu, and Gura-Dhamole Woreda, respectively.
Conclusion: The proportion of sputum smear-positive tuberculosis was high in the Bale Zone. Bale Zone should give more attention to the Tuberculosis program to tackle sputum smear positive. We recommended researchers investigate further research to identify determinants in districts with a high prevalence rate of tuberculosis.
Keywords: tuberculosis, trend, Bale
Introduction
Tuberculosis (TB) remains a major global health problem and causes ill-health for about 10 million people each year and the leading cause of a single infectious agent, ranking above Human Immuno-Virus (HIV). In 2016, an estimated 10.4 million people (65% men, 90% adults, and 10% HIV-positive individuals) developed TB. In 2016, 16% of those who contract TB worldwide also passed away from the condition. The World Health Organization (WHO) African Region accounts for 25% of the expected incident case numbers.1
Ethiopia is one of the 30 nations with a high TB burden, accounting for 87% of the projected global TB cases.2 According to the 2017 Global TB report, the incidence of tuberculosis in Ethiopia was 177 per 100,000 population.1 Additionally, the survey conducted in Hadiya stated that the prevalence of smear-positive TB 148 per 1000 population, 237 per 1000 population in men and 56 per 1000 in women.3 The trend analysis conducted at Saint Paul Hospital Millennium medical college showed that among the total reported sputum smear cases 6% sputum smear-positive cases and 3.4% cases reported among women.4 According to a study done in the Amhara and Oromia regions, 128.9 cases out of every 100,000 people were reported.; 126.4 and 131.4 per 100,000 populations in Amhara and Oromia region, respectively, and case notification rate decline annually by 6.5% and male to female ratio 1.2 and cure rate increased by 13.4% and treatment success rate by 4%. From the total reported 34.1%, 33.5%, and 32.4% were sputum smear positive, sputum smear negative and EPTB, respectively.5 As of study conducted in Ethiopia, Awi zone showed that prevalence per 100,000 population of all forms of TB decreases from 213 in 2012 to 189 in 2016.6
After a successful pilot program with the creation of the first combined Tuberculosis and Leprosy Prevention and Control Program handbook, Ethiopia adopted the Directly Observed Therapy (DOTs) technique in 1997. Today, it accepted the new “END TB strategy” in accordance with Ethiopia’s objective to restructure the health system, with the primary goal of eradicating the TB pandemic by 2035.7 The 2030 targets call for a 90% decrease in TB-related mortality and an 80% decrease in TB incidence rates when compared to 2015 levels. The most important benchmarks, set for 2020, are a reduction of 35% in TB mortality, a reduction of 20% in TB incidence rates, and a reduction of 0% in the proportion of TB-affected families facing catastrophe as compared to levels in 2015. The Ethiopian government has used a variety of tactics to reduce the prevalence of TB.2 Despite the efforts made by the government; TB is still a significant public health issue in the Bale Zone. As 80–90% of TB transmission is attributable to SS+ cases, studying trends of all forms of TB and treatment outcome of SS+ tuberculosis cases across different levels can provide clues regarding the magnitude of TB transmission.8 The objective of this study was to describe the trends and geographical patterns of tuberculosis disease from 2013 to 2018 in Bale Zone, Oromia Regions, Ethiopia.
Methods and Materials
Study Area and Period
Bale is located in the Oromia region, Ethiopia, with 18 woredas and two towns administrative. Of those 18 woredas, 9 of them are pastoralists and others are agro-pastoralists. It is located South-east of Addis Ababa at 430km distance from Addis Ababa. The Bale Zone is expected to have 1,911,510 residents overall in 2018 based on housing projections and the 2007 census, and its total area is 67,329.59 km2. The Somale area on the east, the west Arsi on the west, the Guji zone on the south, the west Hararge on the northwest, and the Arsi on the north border the Zone. Geographically, highlands make up 14% of the population while lowlands make up 64%. Three hundred and eighty-seven health posts, 87 health Centers, and 5 hospitals are located in the zone. All of these health-care facilities provide preventative care and follow-up care for TB to the local populations. The research was carried out in March 2019.
Study Design
A review of secondary data on cases of tuberculosis from all Woredas in the Bale Zone from 2013 to 2018.
Population
The source population was all population of Bale Zone from 2013 to 2018. The study subjects are all tuberculosis patient-reported from 2013 to 2018 to Bale Zone health administration, Health information system (HIS).
Operational Definition
Bacteriological Confirmed TB Case
Patient from whom at least one biological specimen has tested positive for mycobacterium TB using smear microscopy, the Xpert MTB/RIF test, culture, or another WHO-approved bacteriologic detection method.
Pulmonary Tuberculosis
Any TB case that has been clinically or bacteriologically diagnosed and involves the tracheobronchial tree or lung parenchyma. A patient should be considered as Pulmonary TB if they have both pulmonary and extrapulmonary TB.
Extrapulmonary Tuberculosis
Any TB case affected organs other than the lungs that has been bacteriologically proven or diagnosed clinically.
New TB cases: refers to individuals who have never received TB treatment or who have taken anti-TB medications for less than one month.
Previously treated: refers to patients who have received one month or more of anti-TB drugs in the past, may have positive or negative bacteriology and may have a disease at any anatomical site.
Relapse: refers to individuals who have previously taken anti-TB medications for at least one month, who may have positive or negative bacteriology, and who may have a disease at any location on the body.
Treatment after failure: patients who have undergone TB treatment in the past but experienced a failure of their most recent course of therapy.
Treatment after loss to follow up: patients who have previously been treated for TB and were declared lost to follow-up at the end of their most recent course of treatment.
Cured: a pulmonary TB patient with bacteriologically confirmed TB at the beginning of treatment who was smear- or culture-negative in the last month of treatment and on at least one previous occasion.
Treatment completed: unable to demonstrate that sputum or culture findings in the final month of treatment and on at least one prior occasion were negative, either because tests were not performed or because results are not accessible, a patient who completed treatment but showed no signs of failure.
Treatment failure: a TB patient receiving therapy who has a positive sputum culture or smear at month five or later.
Died: a patient who passes away while receiving treatment for TB.
Lost to follow up: a patient whose treatment has been ongoing for at least four weeks but has been discontinued for eight or more straight weeks.
Data Source and Collection Procedure
Data taken out from the Bale Zone HMIS unit database. The health facilities were reported to the district. Then, all tuberculosis cases data was reported to the zone by the districts every month. At the Bale Zonal Health Department, information was computerized and kept in the HMIS Unit. Six years’ tuberculosis data (2013–2018) extracted by person (Age, sex), place (Woreda, Hospital), and time (Years; 2013–2018).
Data Analysis and Management
After all data validated for completeness and consistency, analyzed by person, place and time using Epi info 7 and Microsoft office excel 2016. Tuberculosis case detection rate calculated according to the annual global tuberculosis report as divided the number of new and relapsed cases of tuberculosis that were reported by the total number of cases that were anticipated to occur. Figure, table, and graph, the frequency and percentage as well as the prevalence rate were determined and then summarized.
Ethical Consideration
The study was granted an exemption by ethical committee from Jimma ethical review board by the reference number IHRPGO/768/2018. Additionally, permission to use data for the study has obtained from Bale Zone health Office by the reference number BFG/30004/18. Confidentiality of the data was assured and used only for study.
Results
A total of 11,727 all TB cases were reported from 2013 to 2018 to the Bale Zonal Health Department. Of these cases, 41.7%, 29.0%, and 29.3% were sputum smear-positive, sputum smear-negative and EPTB, respectively (Figure 1).
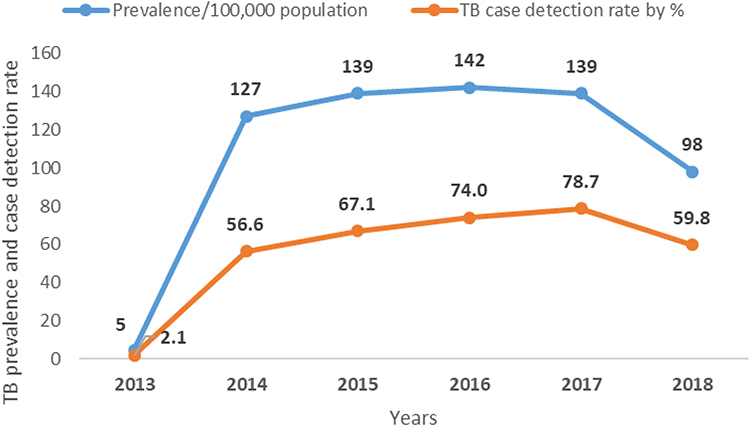 |
Figure 1 TB prevalence and cases detection rate in Bale Zone, 2013–2018. |
Among the total reported 6407 (54.6%) were males. Regarding the age group distribution, 9632 (82.1%), 1592 (13.6%) and 503 (4.3%) were greater than 15 years, 5–14 years and 0–4 years’ age groups, respectively.
The prevalence rate significantly increased from 5.3 per 100,000 population in 2013 to 98.1 per 100,000 population in 2018 with a downward trend in the odd ratios (χ2=33.4; p value = 0.0000). The prevalence rate increased by the average yearly 92.8 per 100,000 population. However, the prevalence rate decreased insignificantly from 126.7 in 2014 to 98.1 in 2018 with a downward trend in the odd ratios (χ2=2.7; p value = 0.103), declined by 0.028%. The tuberculosis case detection rate increased from 2.1% in 2013 to 59.8 in 2018. The average annual tuberculosis cases detection rate at the Bale Zone was 56.4% (Figure 2).
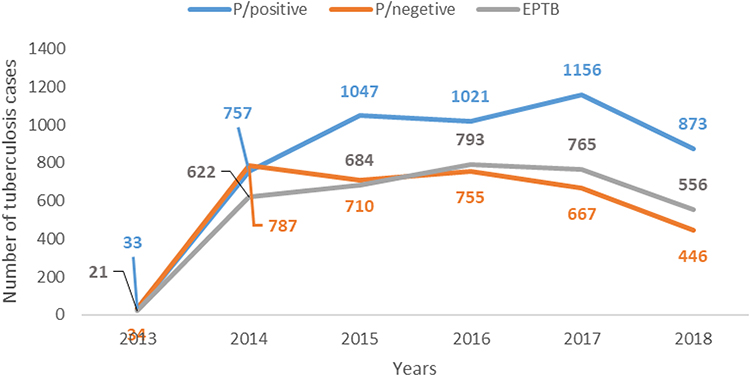 |
Figure 2 Number of TB cases in Bale Zone from 2013–2018. |
The results indicated, 86.4% of all newly diagnosed cases of tuberculosis with positive sputum smears were successfully treated, whereas 81.9%, 4.5%, 2.1%, 0.6%, 0.7%, 0.3%, and 0.14% were, respectively, cured, treated to completion, lost to follow-up, treated unsuccessfully, not evaluated, and advanced to MDR treatment (Table 1).
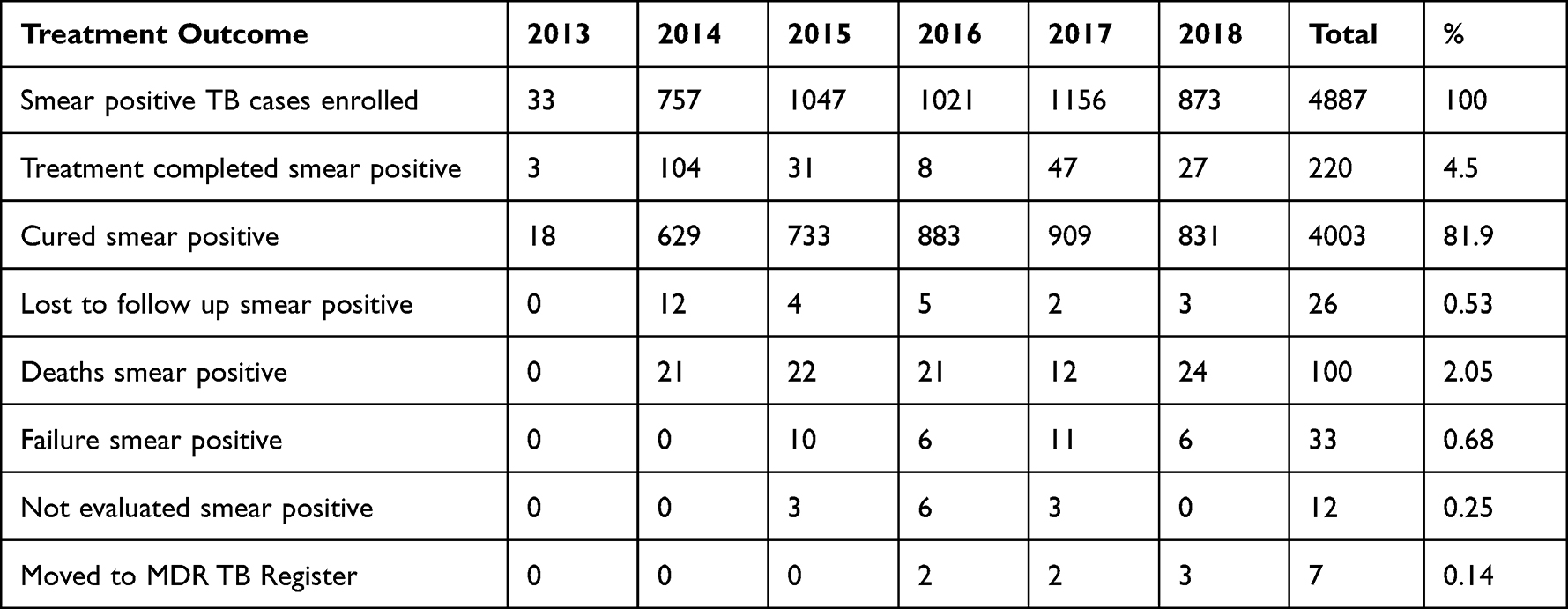 |
Table 1 Trends of Treatment Outcome of Sputum Smear Positive Tuberculosis 2013–2018, Bale Zone, Oromia Region, Ethiopia |
The cure rate ranged from 98.5% to 76.6% at Rayitu and Meda walebu Woredas. The death rate was high at Goba referral hospital and followed by Gura dhamole and Lega Hidha Woredas which were recorded as 74.1, 44.9,41.2 per 1000 sputum smear-positive population, respectively (Figure 3).
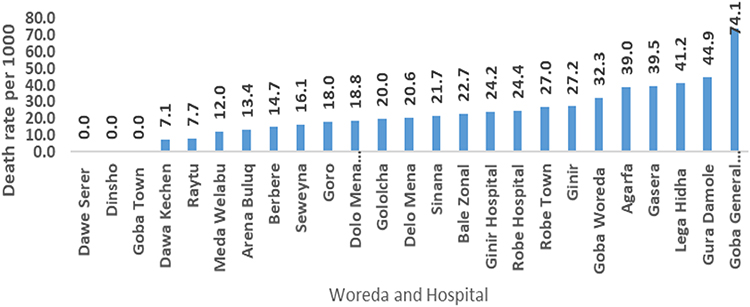 |
Figure 3 TB death rate per 1000 population among Bale Zone population from 2013–2018. |
The prevalence rate of tuberculosis at Bale Zone Woredas ranged from 25 to 198 per 100,000 population. The highest prevalence rate was reported from Berbere, Rayitu, and Gura Dhamole Woreda which were reported as 198, 152 and 142 per 100,000 population, respectively (Figure 4).
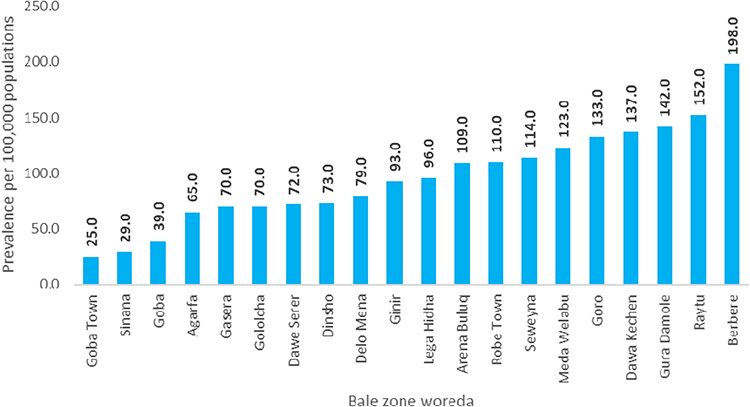 |
Figure 4 Prevalence of Tuberculosis among Bale Zone Populations from 2013–2018. |
Discussion
The public health issue of tuberculosis persists, particularly in developing nations like Ethiopia.1–3 Therefore, this review was identified the TB detection rate, prevalence of TB and TB death rate in study area.
The most of the reported cases were smear-positive tuberculosis which was recorded as 41.7% and almost no significant difference between smear-negative (29.0%) and extrapulmonary (29.3%) tuberculosis were observed. This result is consistent with the research conducted in Sidama Zone, Southern Ethiopia which was observed as the smear positive tuberculosis was the predominant followed by smear negative which were recorded as 61% and 22%, respectively,9 and study conducted in Jimma, Ethiopia which showed that 48.8%, 29.4% and 22.1% were smear-positive pulmonary, smear-negative pulmonary and extrapulmonary tuberculosis, respectively.10 The possible explanation for this results can be due to the fact that pulmonary type of tuberculosis is the overcome types of tuberculosis as supported by the body of science.11 Additionally, comparable to the report of 2017 WHO tuberculosis report which indicated that the smear-positive tuberculosis was the leading (57%).1 However, our result is paradoxical with the study done in different areas of Ethiopia which indicated that smear-positive tuberculosis is the least dominant from all types of tuberculosis.5,6,11,12 This contradictory might be due to increased access to TB diagnostic tests or more implementers on the ground increasing TB screening coverage.
People over the age of 15 made up the majority of cases (82.1%), followed by those between the ages of 5 and 15 (13.6%) and children under the age of 5 (4.3%). This result is consistent with a research done in the Amhara region of Ethiopia’s Awi zone, which found that the majority of cases (87.3%) included adults over the age of 15, followed by those between the ages of 5 and 15 (10.2%), and those under the age of 5 (2.5%).6 And the study conducted in ten zones of Ethiopia also shows the same results.5 Additionally, a different study conducted in different areas of Ethiopia has supported our finding.10,13,14 This may be due to the diagnosis of tuberculosis difficult in young children and tuberculosis is most common in adults as supported by the body of science.15
Males are more likely than females to contract tuberculosis in most nations, including wealthy ones.1,10,14,16 Our findings, however, did not identify a statistically significant difference between the proportion of males and females with tuberculosis, which was similar with research done elsewhere in Ethiopia.5,6,9,13 This slight variation might be brought on by variations in social positions, risky behaviors, and activities. Males may travel more frequently, interact with more people socially, and spend more time in environments that may encourage transmission.17
The Bale Zone’s TB trends grew from the year 2013 to 2017, peaked in 2017, and then started to decline in 2018. The average annual prevalence rate was increased by 0.016% yearly, this increment was contributed more by the upswing of case notification from 2013 to 2014, may as a result of TB program strengthened in the zone by different project.18 Compared to the study conducted in the Sidama zone of southern Ethiopia, the prevalence rate of our findings was lower, but the general trend line was comparable with that of this study.9 However, from 2014 to 2018 the prevalence rate was decreased insignificantly by 0.026% annually. This result was in line with a study done in 10 Zones of Ethiopia that showed the prevalence rate in Oromia was declining annually by 2.8%5 and study conducted in Awi zone which indicated that the prevalence rate of TB was declined.6
The trends of tuberculosis cases detection rate were substantially increased from 2.1% in 2013 to 59.8% in 2018. This finding might be due to community tuberculosis strengthening and expansion by the engagement of the health extension workers in tuberculosis screening and referral of the presumptive tuberculosis.18
Our finding indicated that 86.4% were successfully treated among reported sputum smear-positive TB cases and 81.9% cured. This result is similar with a study done in 10 Zones of Ethiopia, which revealed that Oromia had an 86% cure rate and a 93.4% success rate for therapy.5 Additionally, our finding is also in line with a systemic review study conducted in Ethiopia indicated that treatment success rate in Oromia was 88.5%.19 Furthermore, this finding is higher than that of the Ethiopian study done in Wolaita Sodo town.20 The decentralization of tuberculosis treatment services to the lowest levels of health-care facilities close to the population may be the cause of this high treatment success rate. Sputum smear-positive cases had an average mortality rate of 2.2%. This result was in line with the research done in the Sidama zone.9 Moreover, decreased in comparison to the 2017 WHO TB report.1 This lower death rate might be due to the attribute of the execution effort of the tuberculosis prevention and control program. Our finding showed that treatment failure was 0.72%. This result was higher as compared to the study conducted in Sidama Zone9 and Dilla.14 However, this is in line with the study done in the Wolaita Sodo.20
Our finding indicated that prevalence was high in Berbere Woreda followed by Rayitu and Gura Dhamole. This finding is higher as compared with the study conducted in 10 zones of Ethiopia.5 This high prevalence of tuberculosis in the area might be due to the function of health posts in communities monitoring for tuberculosis and raising public awareness of the disease.
According to the End TB strategy milestone, about 20% decrease in the overall number of TB cases by 2020 as compared to the baseline year of 2015.2 Our finding indicated that the absolute number of all TB cases was decreased by 24.1% in 2018 compared with the baseline 2015, so this finding is consistent with the End TB strategy program.
Limitations of the Study
The research results were produced by the assessment of HMIS data utilizing retrospective data analysis. There were various inconsistent and partial data retrieval problems. The research’s results, however, have a substantial scientific significance and offer a rich field for further prospective studies.
Conclusions
Proportion of sputum smear positive tuberculosis was high in Bale Zone and age group greater than 15 years was more affected by tuberculosis. The prevalence of tuberculosis was started to decline from the year 2016 and also this study depicted that treatment success was high in study area during 2013–2018. Finally, we recommend that Bale Zonal Health Department should give more attention on TB program prevention and control to tackle sputum smear positive to realize the END TB strategy declared by global community and accepted by Ethiopia.
Acknowledgments
We would like to thank Jimma University for their letter of support and for their training program in Ethiopian field epidemiology and laboratories. We also like to express our gratitude to the Bale Zone Health Office’s Health Information System Department for approving our request to use their data for analysis.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation critically reviewing the article and gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declared that they have no competing interests.
References
1. World Health Organization. WHO Global Tuberculosis Report 2017. World Health Organization; 2017.
2. World Health Organization. The End TB Strategy, Global Strategy and Targets for Tuberculosis Prevention, Care and Control After 2015. Sixty Seventh World Health Assembly; 2014.
3. Datiko DG, Guracha EA, Michae E, et al. Sub-national prevalence survey of tuberculosis in rural communities of Ethiopia. BMC Public Health. 2019;19(1):295. doi:10.1186/s12889-019-6620-9
4. Bikila D, Yohannes W, Abdeta A, et al. Seasonality and trend analysis of pulmonary tuberculosis at St. Paul Hospital Millennium Medical college, Addis Ababa. Austin J Respir Med. 2017;4(2):1054.
5. Dememew ZG ZG, Habte D, Melese M, et al. Trends in tuberculosis case notification and treatment outcomes after interventions in 10 zones of Ethiopia. Int J Tuberc Lung Dis. 2016;20(9):1192–1198. doi:10.5588/ijtld.16.0005
6. Alemu T, Gutema H. Trend in magnitude of tuberculosis in Awi Zone, Northwest Ethiopia: a five-year tuberculosis surveillance data analysis. BMC Res Notes. 2019;12:209. doi:10.1186/s13104-019-4234-z
7. Ministry of Health of Ethiopia. Guidelines for Clinical and Programmatic Management of TB, TB/HIV and Leprosy in Ethiopia. Federal democratic republic of Ethiopia ministry of health; 2016.
8. Federal democratic republic of Ethiopia ministry of health. Guidelines for Clinical and Programmatic Management of TB, TB/HIV and Leprosy in Ethiopia Six Edition. Ethiopia federal ministry of health; 2016.
9. Dangisso MH, Daniel Gemechu DDG, Lindtjørn B. Trends of tuberculosis case notification and treatment outcomes in the sidama zone, southern Ethiopia: ten-year retrospective trend analysis in urban-rural settings. PLoS One. 2014;9(12):e114225. doi:10.1371/journal.pone.0114225
10. Abebe T, Angamo MT. Treatment outcomes and associated factors among tuberculosis patients in Southwest Ethiopia. Gülhane Tip Derg. 2015;57:397–407.
11. Lee JY. Diagnosis and treatment of extrapulmonary tuberculosis. Tuberc Respir Dis. 2015;78(2):47–55. doi:10.4046/trd.2015.78.2.47
12. Fisseha HZ. Trends and treatment outcome of tuberculosis patients in Assella Hospital from July 2011-June 2017, Oromia, Ethiopia, seven year retrospective study. J Tuberc Therap. 2018;3:112.
13. Getahun B, Ameni G, Medhin G, Biadgilign S. Treatment outcome of tuberculosis patients under directly observed treatment in Addis Ababa, Ethiopia. Brazilian J Infect Dis. 2013;17(5):521–528. doi:10.1016/j.bjid.2012.12.010
14. Gebrezgabiher G, Romha G, Ejeta E, Asebe G, Zemene E, Ameni G. Treatment outcome of tuberculosis patients under directly observed treatment short course and factors affecting outcome in southern Ethiopia: a five-year retrospective study. PLoS One. 2016;11(2):e0150560. doi:10.1371/journal.pone.0150560
15. Richard E, Robert MK, Jenson MJ. Nelson Textbook of Pediatrics.
16. Centers for Disease Control and Prevention. Reported tuberculosis in United States 2017. National Center for HIV/AIDS, viral hepatitis, STD, and TB prevention Division of Tuberculosis Elimination; 2018.
17. Nhamoyebonde S, Leslie A. Biological differences between the sexes and susceptibility to tuberculosis. J Infect Dis. 2014;209(Suppl 3):s100–s106. doi:10.1093/infdis/jiu147
18. Help Ethiopia Address Low TB Performance (HEAL TB) Project. The rapid expansion of comprehensive, high-quality tuberculosis services in Ethiopia final report 2011–2016. Management Sciences for Health; 2016.
19. Eshetie S, Gizachew M, Alebel A, Van Soolingen D. Tuberculosis treatment outcomes in Ethiopia from 2003 to 2016, and impact of HIV co-infection and prior drug exposure: a systematic review and meta-analysis. PLoS One. 2018;13(3):e0194675. doi:10.1371/journal.pone.0194675
20. Yakob B, Alemseged F, Paulos W, Badacho AS. Trends in treatment success rate and associated factors among tuberculosis patients in Ethiopia: a retrospective cohort study. Heal Sci J. 2018;12(5):598. doi:10.21767/1791-809X.1000598
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.