Back to Journals » Hepatic Medicine: Evidence and Research » Volume 14
Prevalence and Factors Associated with Hepatitis B Infection Among Outpatient Adults in South-Western Uganda
Authors Rugaatwa Ndibarema E ![]() , Olum R
, Olum R ![]() , Ayebare D
, Ayebare D ![]() , Kabakyenga J
, Kabakyenga J
Received 10 July 2022
Accepted for publication 29 September 2022
Published 19 October 2022 Volume 2022:14 Pages 163—172
DOI https://doi.org/10.2147/HMER.S381809
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Gerry Lake-Bakaar
Elias Rugaatwa Ndibarema,1– 3 Ronald Olum,4 David Ayebare,1 Jerome Kabakyenga1
1Mbarara University of Science and Technology, Mbarara, Uganda; 2Mother Kevin Postgraduate Medical School / St. Francis Hospital Nsambya, Uganda Martyrs University, Kampala, Uganda; 3Mbarara Regional Referral Hospital, Mbarara, Uganda; 4St Francis Hospital Nsambya, Kampala, Uganda
Correspondence: Elias Rugaatwa Ndibarema, Mother Kevin Postgraduate Medical School / St. Francis Hospital Nsambya, Uganda Martyrs University, Kampala, Uganda, Email [email protected]
Background: About 2 billion people in the world are exposed to hepatitis B virus. Africa contributes 25% of the global Hepatitis B burden and prevalence in Uganda is 4.3%. Routine testing to establish the burden, improve prevention and control through early diagnosis and management are rare in hospital settings. We aimed at establishing the prevalence and factors associated with hepatitis B infection among adults attending outpatient clinic at Mbarara Regional Referral Hospital (MRRH) in Uganda.
Methods: A hospital-based cross-sectional study was conducted among outpatients attending MRRH. Consecutive sampling method was used to recruit participants. Interviewer-administered questionnaires were used to collect data. Blood samples were collected to test HBsAg. Summary statistics were used to describe the socio-demographic characteristics of study participants and the proportion of Serostatus for hepatitis B infection. Bivariate followed by multivariate logistic regression analysis was conducted to assess the factors associated with hepatitis B infections. All independent variables with p-values < 0.2 were entered into a multivariate model to adjust for confounding. A p value < 0.05 was considered statistically significant.
Results: A total of 400 participants were recruited. 64.5% were females (n=258) and aged 18– 29 years (48.5%, n=193). Overall, 22(5.5%) participants were found to be seropositive for hepatitis B infection. Residing in Kiruhura district (AOR = 11.9, 95% CI: 2.40– 59.25, p< 0.003) was significantly associated with hepatitis B infection while being female (AOR = 0.3, 95% CI: 0.11– 0.88, p< 0.018) was protective.
Conclusion: Prevalence of hepatitis B infection among adult patients attending outpatient clinic at MRRH was 5.5% with male gender and residing in Kiruhura district as factors associated with high prevalence of hepatitis B infection. Ministry of Health should scale up hepatitis B routine testing and treatment at MRRH and its catchment area, with special control programs such as screening, vaccination, and sensitization involving men.
Keywords: hepatitis B, Uganda, prevalence, associated factors
Introduction
Globally, about two billion people are exposed to hepatitis B virus,1 of which 296 million are chronic carriers of hepatitis B surface antigen.2 WHO Western Pacific Region has the highest, followed by the African Region, where 116 and 81 million people, are chronically infected, respectively.2 In 2019 alone, there were approximately 820,000 deaths associated with hepatitis B, mainly secondary to liver cirrhosis and hepatocellular carcinoma.2
Hepatitis B infection is caused by the hepatitis b virus (HBV), a double stranded enveloped DNA virus with icosahedral nucleocapsid.2 The virus can be spread through vertical transmission (mother-to-child), or horizontally by exposure to blood and body fluids of infected individuals (saliva, vaginal fluids, seminal fluids, etc), through needle stick injury, body fluid splashes, and sexual intercourse especially among individuals with multiple sexual partners.2 HBV can also be spread through blood transfusion although the incidence has greatly reduced due to the routine screening of blood products before transfusion.3 HBV infection is self-limiting in up to 90% of patients who acquire HBV in adulthood. It becomes chronic in less than 5% of the cases, with only 1% experiencing a fulminant acute hepatitis which can be fatal. Hepatitis B infection predisposes infected persons and health workers to serious morbidity risks such as liver cirrhosis and primary liver cancer.4
Uganda is one of the countries with the highest prevalence of HBV globally. In the 2005 Uganda National Serosurvey, prevalence of hepatitis B was reported at 10%.5 In 2018, the prevalence was reported at 4.3% (5.6% among men and 3.1% among women).6 The survey indicated that hepatitis B prevalence was highest in Northern region with 4.6% in mid North, 4.4% in Northeast and 3.8% in West Nile. Hepatitis B infection was lower in the rest of the country with a range of 0.8% in Southwest region to 2.7% in East Central region.7 Ochola and others had earlier found that up to 17.6% of the people in Gulu (Northern Uganda) had HBV infection, with a lifetime exposure of 72.4%. Individual anecdotal reports from health workers suggest that Hepatitis B is on the rise in western Uganda. A household cross-sectional study in Kiruhura district, south-western Uganda recently reported a prevalence of 4.1%.8
There have been various Hepatitis B prevention strategies by The Ministry of Health and Non-Governmental Organizations such as vaccination of children since 2002 under Uganda National Expanded Programme on Immunization (UNEPI). HBV vaccination protects individuals against morbidity, mortality, and complications of HBV infection.2 Despite the above, there is still limited information on the prevalence of HBV in the hospital settings in western Uganda. There is no routine screening of hepatitis B in most hospitals in Uganda and suspected cases with the clinical signs and symptoms are usually referred to private laboratories for hepatitis B surface antigen (HBSAg). A higher prevalence is presumed in a health facility compared to the household reports.
The aim of this study was to assess the prevalence and factors associated with HBV infection among patients seeking care at a regional referral hospital in south western Uganda.
Methodology
Study Design and Duration
This was a cross-sectional study using quantitative techniques. The study was carried out between June 2019 and July 2019.
Study Site
The study was carried out at the outpatient department, Mbarara Regional Referral Hospital (MRRH), a public hospital located in Southwestern Uganda. The hospital serves over 10 districts with a population of more than 2.5 million people. It also receives patients from neighbouring countries of Rwanda, Tanzania, and The Democratic Republic of Congo. It doubles as a teaching hospital for Mbarara University of Science and Technology (MUST). According to the ministry of health (2018), every day 1200–1500 patients seek health services at MRRH, out of which over 200 visit the OPD. The study targeted patients seeking health services at the OPD which is an entry point into the hospital.
Selection Criteria
Adults aged 18–59 years seeking general medical services at the OPD of Mbarara Regional Referral Hospital who consented to participate were included in the study. Those aged 18–59 years who were very sick and too weak to undergo an interview were excluded and referred to the emergency ward. The latter admits very sick medical and surgical patients for resuscitation and further management.
Sample Size and Sampling
Sample size calculation for single population.9
E = 1/√N
where,
N= the sample size (respondents to be interviewed)
E = the precision of the study (5%)
E = 5% = 0.05
0.05 = 1/√N
n = 400
A total of 400 respondents were interviewed.
Participants were consecutively recruited into the study, with the first patient aged 18 to 59 years in the OPD register consented as the starting point. The next consenting patient was enrolled. The procedure was repeated until the sample size was obtained.
Data Collection
Data was collected using a structured and pretested questionnaire by two trained research assistants (RAs) supervised by the principal investigator (PI). The PI trained the RA in data collection procedure and study tools. Data were collected daily in the outpatient clinic of MRRH from 20th June to 10th July 2019. Both English and local languages (Runyakitara) were used. The dependent variable was HBV infection status which was recorded either seronegative or seropositive. The HBV infection was determined by doing a hepatitis B surface antigen (HBsAg) which confirms the presence of infection in the body.1 The independent variables were the socio-demographic characteristics, lifestyle factors and medical factors.
Standard Operating Procedure for HBV Testing
For the detection of HBsAg, 4 mL of venous blood was collected into a labelled plain vacutainer by a trained laboratory technician from the participant upon consent. The sample was transported in a cold box to Mbarara Diagnostic Laboratory Centre located on plot 56 high street Mbarara town for HBsAg testing. The blood sample was centrifuged to obtain serum. About 80μL of serum was then pipetted and transferred onto the sample pad of an SD BIO-LINE HBsAg WB one step, rapid, Immunochromatographic test strip for hepatitis B surface antigen test (expiry date: October 2020) and started the timer immediately. Results were read at 15 minutes. The seropositive was indicated by the appearance of two red or pink lines (the test and control lines). Negative results were indicated by only one red or pink line appearing in the Control Zone (C). The HBsAg rapid Immunochromatographic test has a sensitivity and specificity of about 91% and 98%, respectively.10 Test results for hepatitis B were collected from the lab and a hard copy filed with the in-charge nurse at OPD. Participants were called by telephone to receive their results. Those found positive for hepatitis B surface antigen were called to receive their results and linked to a physician in the OPD specialised medical clinic for individualised follow-up including further blood work-up on the viral load, HbeAg and HbcAg before the decision to treat was made. Those found negative were counselled on preventive measures such as hepatitis B vaccination.
Data Management and Analysis
Data was entered into Epi Info version 3.0 for cleaning and then exported into Stata 14.0 software (StataCorp LLC, College Station, Texas, USA) for statistical analysis. Frequencies and percentages were calculated and reported for all the categorical characteristics. Continuous variables were assessed for normal distribution using Shapiro–Wilk test and thereafter reported as mean and standard deviation for normally distributed data, and median (interquartile range) for nonparametric data.
The overall prevalence was calculated as the proportion of participants that were seropositive for hepatitis B infection (HBsAg positive) in relation to the sample size (denominator). Chi square tests for associations were computed to detect differences in all the categorical variables with probability values (p values) calculated at p<0.05 level of statistical significance, and corresponding odds ratios and 95% confidence intervals. Logistic regression was done to determine factors that were associated with Hepatitis B infection. Covariates associated with p values ≤0.2 in the binary logistic regression analysis were entered into multivariate logistic regression model through forward stepwise elimination method to obtain the final predictive model of covariates that were independently associated with HBV at p<0.05 level of statistical significance.
Ethical Consideration
This study was conducted in line with the principles described in the Declaration of Helsinki. The study protocol was approved by Mbarara University of Science and Technology Research Ethics Committee (Study IRB Number 26/14−19). Written informed consent was obtained from each study participant to confirm willingness to participate after explaining the objective of the study. Confidentiality was ensured by using codes instead of participants’ names. Recruitment to participate in the study was free, and voluntary and participants were assured of freedom to withdraw from the study at any point.
Results
Characteristics of the Participants
Table 1 summarizes the demographic characteristics of the participants. A total of 400 participants were recruited into the study (response rate=100%). The majority of the participants were females (n=258, 64.5%), married (n=209, 52.38%), and aged 18–29 years (n=193, 48.25%). Up to 95.5% (n=381) were Ugandans and more than half had regular income (63%, n=250), resided in urban areas (52.8%, n= 21) and protestants by religion (55%, n=220).
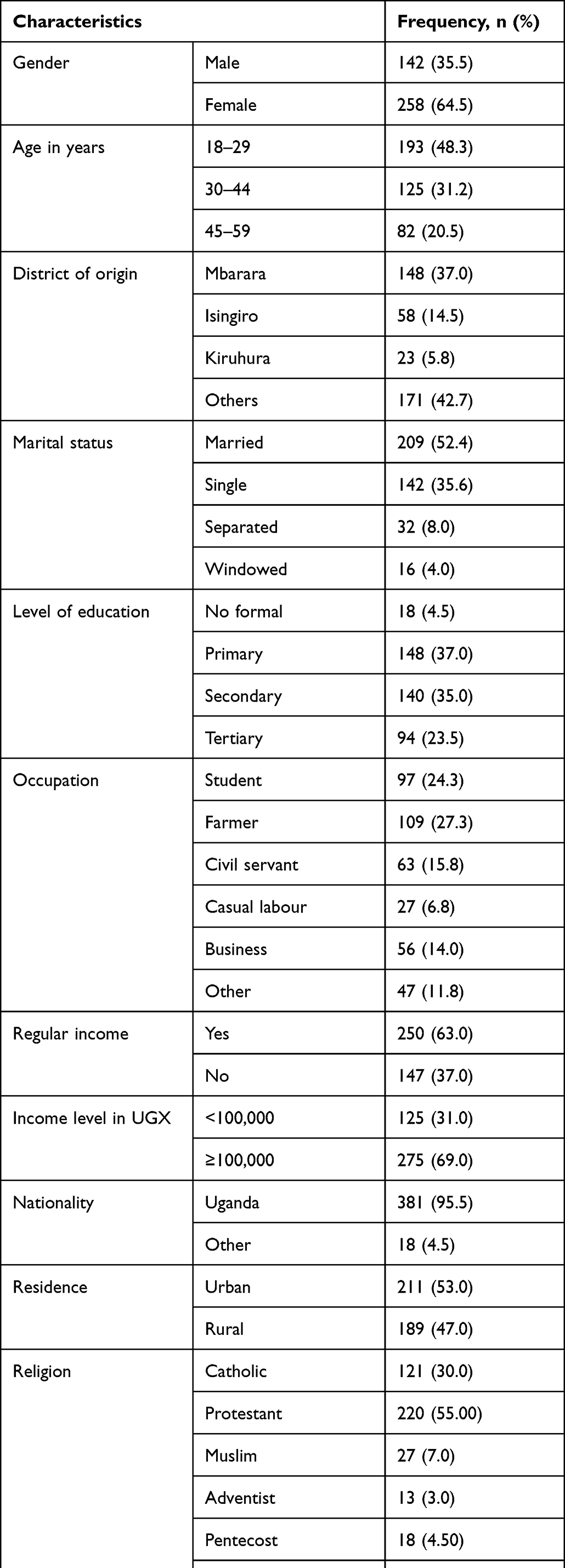 |
Table 1 Socio demographic Characteristics of Adult Outpatients Attending Mbarara Regional Referral Hospital |
Prevalence of Hepatitis B Infection
The prevalence of hepatitis B infection was 5.5% (22/400, Figure 1). In the bivariate analysis, gender (p=0.017) and district of origin (p=0.002) were significantly associated with HBV infection among the study participants (Table 2). Findings show that gender, district of origin were associated with hepatitis B infection among outpatients attending MRRH. Females were less likely to be seropositive compared to males (unadjusted odds ratio (UOR) = 0.4, 95% CI: 0.14–0.95, p = 0.017). Outpatients from Kiruhura district were 13.4 times more likely to be seropositive compared to those from Mbarara District (UOR = 13.4, 95% CI: 2.96–60.95, p = 0.002).
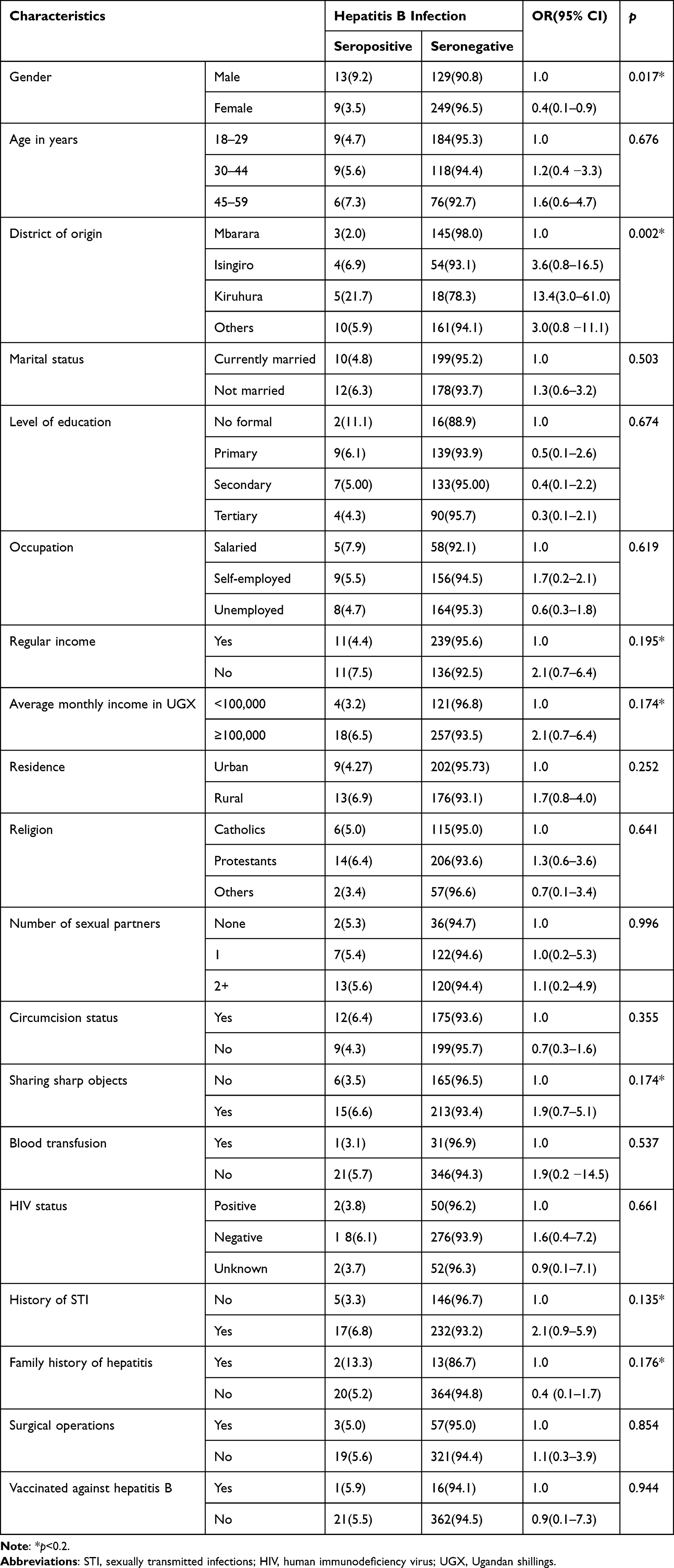 |
Table 2 Bivariate Analysis of Factors Associated with Hepatitis B Infection (N = 400) |
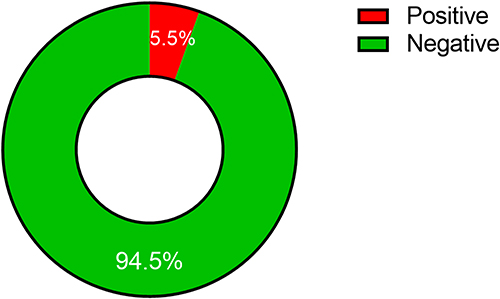 |
Figure 1 Prevalence of hepatitis B infection among adult outpatients attending Mbarara Regional Referral Hospital. |
Factors Associated with Hepatitis B Infection
In the multivariate model (Table 3), gender and district of origin were then factors associated with hepatitis B infection among outpatients attending MRRH. Females were less likely to be seropositive compared to males (AOR = 0.3, 95% CI: 0.11–0.88, p<0.05). Also, outpatients from Kiruhura district were 11.9 times more likely to be seropositive compared to those from Mbarara District (AOR = 11.9, 95% CI: 2.40–59.25, p<0.05).
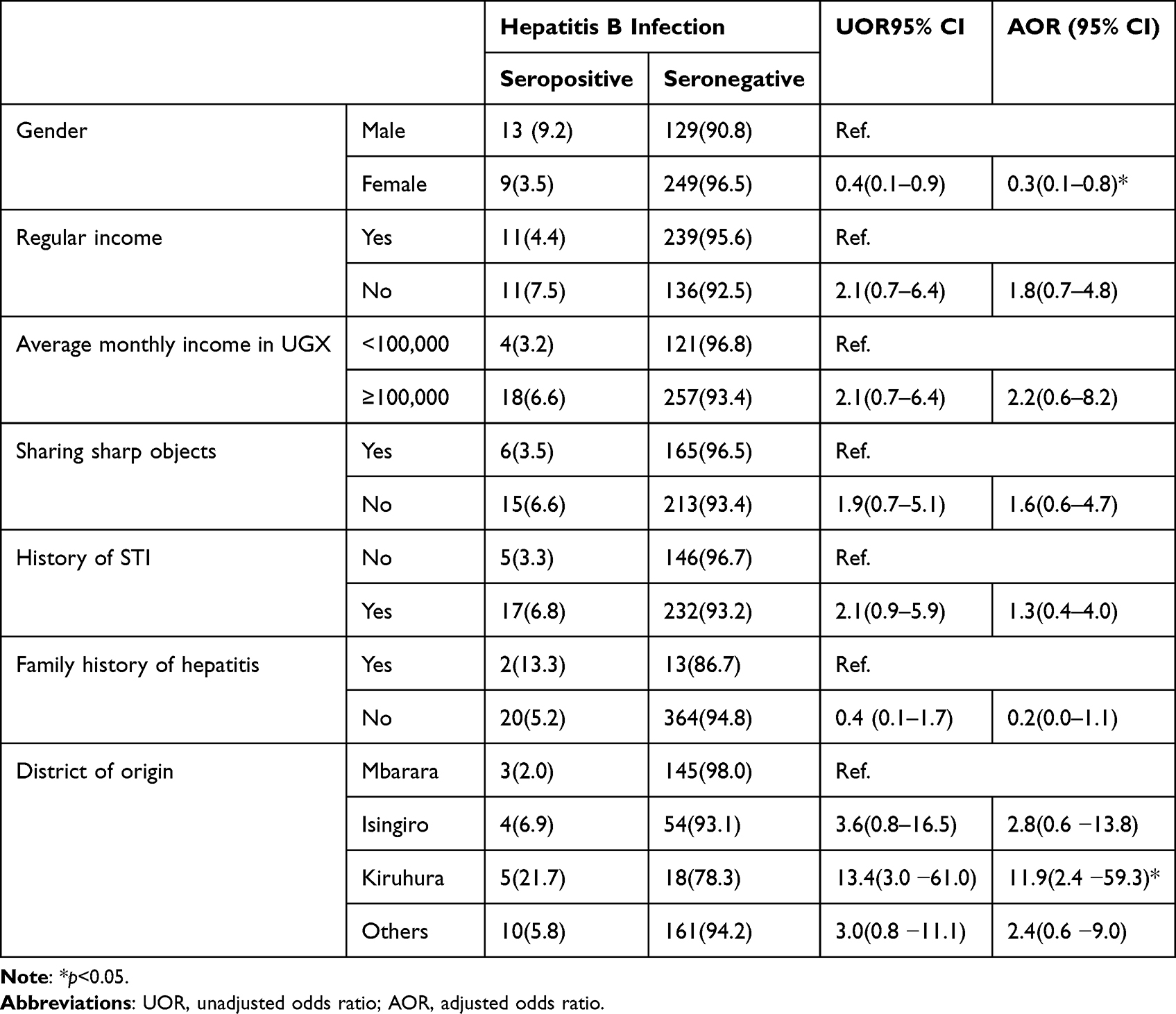 |
Table 3 Multivariate Analysis of Factors Associated with Hepatitis B Infection Among Outpatients Attending Mbarara Regional Referral Hospital |
Discussion
In this study, we investigated the prevalence of hepatitis B infection among outpatients attending Mbarara Regional Referral Hospital in southwestern Uganda. Of the study participants, 5.5% were seropositive. This prevalence is higher than 3.8% (for western region) reported by Bwogi et al while conducting a nationwide population-based cross-sectional survey involving adults of ages 15–59 years and children less than 5 years old.5 It is also higher than the national prevalence of 4.3% reported in the results of Uganda Population-based HIV Impact Assessment Survey of 2016. It is lower than 7% reported among fishing communities around Lake Victoria.11 Within southwestern Uganda, Apecu et al recently indicated still a low prevalence of HBV at 4.1% in a household cross-sectional study in Kiruhura district.8 In our study, a higher prevalence implies an increasing incidence of hepatitis B infection among the populations, but also this being a hospital-based study, the disease burden is expected to be higher compared to community/household surveys.
In this hospital-based cross-sectional study, gender and district of origin were factors associated with hepatitis B infection among outpatients attending MRRH. Males reported a higher likelihood of hepatitis B infection compared to their females. This finding is consistent with findings in a study conducted on HBsAg seroclearance among 52 patients in which males showed a higher proportion of HBV infection.12 Apecu et al also showed that males were at a higher risk of hepatitis B infection compared to females.8 This could be attributed to risky sexual behavioural practices of polygamy and multiple sexual partners in men.
This study showed that outpatients from Kiruhura district reported a significantly higher likelihood of HBV infection than those from Mbarara district. This indicates contextual differences in residence. Similarly, Reekie et al13 showed that the HBV prevalence differed between Aboriginal women residing in remote areas compared to those in major cities. Bwogi et al also showed that region of residence was significantly associated with Hepatitis B.5 Kiruhura district, southwestern Uganda is home to Bahima ethnic group who contribute about 12.1% of the district population.8 A household survey had shown that belonging to the Bahima ethnic group was significantly associated with Hepatitis B and HIV infections.8 This was partly attributed to anecdotal evidence of risky sexual behaviour of “sharing” wives that could promote the spread of the virus. This study also showed significant gender difference in the burden of hepatitis B virus. This is comparable to other studies in China14 and Sierra Leone.15
This study was the first to assess for the prevalence and associated factors of hepatitis B infection among outpatients aged 15–59 years at the largest referral and teaching hospital in southwestern Uganda. The Ministry of Health should scale up routine testing and treatment of hepatitis B at Mbarara hospital and its catchment areas. There is a need to engage men in hepatitis B routine testing and other control programs such as vaccination and sensitization to minimise the chances of transmission. The results can also be used as reference for future surveys in other regional referral hospitals.
Limitations of the Study
Self-reported information was obtained from the respondents. Therefore, there might have been a possibility of social desirability bias on the scales used to assess the study variables. Information obtained was also subject to recall bias as participants might not recall all required information accurately.
Conclusions
The prevalence of hepatitis B infection among outpatients attending Mbarara Regional Referral Hospital was generally high at 5.5%. This study has demonstrated that gender and district of residence are reliable factors associated with hepatitis B infection among outpatients attending Mbarara Regional Referral Hospital.
Data Sharing Statement
The data from this study are available on request from the corresponding author.
Acknowledgments
The authors acknowledge the great contribution and support rendered by the research assistants, especially in data collection and cleaning and participants for volunteering the information.
Funding
The study was funded by the authors and did not receive extra funding from any organisations or parties.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. World Health Organisation. Guideline for the Prevention, Care and Treatment of Persons with Chronic Hepatitis B Infection. World Health Organisation; 2015:124.
2. World Health Organization. Hepatitis B. Fact sheets; 2022. Available from: https://www.who.int/news-room/fact-sheets/detail/hepatitis-b.
3. Candotti D, Allain JP. Transfusion-transmitted hepatitis B virus infection. J Hepatol. 2009;51(4):798–809. doi:10.1016/j.jhep.2009.05.020
4. Alqahtani SA, Colombo M. Viral hepatitis as a risk factor for the development of hepatocellular carcinoma. Hepatoma Res. 2020;2020. doi:10.20517/2394-5079.2020.49
5. Bwogi J, Braka F, Makumbi I, et al. Hepatitis B infection is highly endemic in Uganda: findings from a national serosurvey. Afr Health Sci. 2009;9(2):98–108.
6. Opendi S. World hepatitis day 2018: press statement on the progress of implementation of Hepatitis B vaccination program in Uganda. Govt.Uganda; 2018.
7. Ochola E, Ocama P, Orach CG, et al. High burden of hepatitis B infection in Northern Uganda: results of a population-based survey. BMC Public Health. 2013;13(1):727. doi:10.1186/1471-2458-13-727
8. Apecu R, Bagenda F, Byarugaba F, Bum I. Human immunodeficiency virus and hepatitis B virus co-infection: a cross-sectional household survey in Kiruhura District, Southwestern, Uganda. Int J Trop Dis Heal. 2018;30(2):1–12. doi:10.9734/IJTDH/2018/40254
9. Hulley BS, Cummings RS. Designing Clinical Research.
10. Saboor Soomro R, Shah IA, Saboor A, Bhutto AUB, Memon S. Sensitivity and specificity of hepatitis B virus screening via rapid immunoassay chromatographic test. Cureus. 2021. doi:10.7759/cureus.12909
11. Kitandwe PK, Muyanja E, Nakaweesa T, et al. Hepatitis B prevalence and incidence in the fishing communities of Lake Victoria, Uganda: a retrospective cohort study. BMC Public Health. 2021;21(1):394. doi:10.1186/s12889-021-10428-1
12. Moucari R, Korevaar A, Lada O, et al. High rates of HBsAg seroconversion in HBeAg-positive chronic hepatitis B patients responding to interferon: a long-term follow-up study. J Hepatol. 2009;50(6):1084–1092. doi:10.1016/j.jhep.2009.01.016
13. Reekie J, Kaldor JM, Mak DB, et al. Long-term impact of childhood hepatitis B vaccination programs on prevalence among Aboriginal and non-Aboriginal women giving birth in Western Australia. Vaccine. 2018;36(23):3296–3300. doi:10.1016/j.vaccine.2018.04.057
14. Wang H, Men P, Xiao Y, et al. Hepatitis B infection in the general population of China: a systematic review and meta-analysis. BMC Infect Dis. 2019;19(1):811. doi:10.1186/s12879-019-4428-y
15. Lakoh S, García-Tardón N, Adekanmbi O, van der Valk M, Smith SJ, Grobusch MP. Prevalence of viral hepatitis B and C in Sierra Leone—current knowledge and knowledge gaps: a narrative review. Trans R Soc Trop Med Hyg. 2021;115(10):1106–1113. doi:10.1093/trstmh/trab054
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Drug Resistance Patterns and Trends in Patients with Suspected Drug-Resistant Tuberculosis in Dalian, China: A Retrospective Study
Pan Y, Yu Y, Lu J, Yi Y, Dou X, Zhou L
Infection and Drug Resistance 2022, 15:4137-4147
Published Date: 30 July 2022
Prevalence and Factors Associated with Alcohol Consumption Among Secondary School Students in Nekemte, Ethiopia: A Cross-Sectional Study
Shibiru T, Arulandhu A, Belete A, Etana J, Amanu W
Substance Abuse and Rehabilitation 2023, 14:35-47
Published Date: 12 May 2023
Prevalence and Associated Factors of Chronic Obstructive Pulmonary Disease Among Adults in Neno District, Malawi: A Cross-Sectional Analytical Study
Zaniku HR, Connolly E, Aron MB, Matanje BL, Ndambo MK, Talama GC, Munyaneza F, Ruderman T, Rylance J, Dullie LW, Lalitha R, Banda NPK, Muula AS
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:389-401
Published Date: 5 February 2024
Prevalence and Determinants of Self‑Medication Among Adult Outpatients in a Rural Health Facility in Northern Uganda: A Cross‑Sectional Study
Watuwa PP, Opito R, Okello S, Asapo RM, Baguma I, Okello J, Onap O, Ayikobua ET, Odung T, Lubogo P
Patient Preference and Adherence 2026, 20:575475
Published Date: 29 January 2026
Prevalence and Factors Associated with Type 2 Diabetes Self-Management Among Patients Attending Mbale Regional Referral Hospital: A Cross-Sectional Study in Eastern Uganda
Makonje R, Omolo RO, Mudenda S, Mugenyi N
Diabetes, Metabolic Syndrome and Obesity 2026, 19:598398
Published Date: 23 May 2026