Back to Journals » Nature and Science of Sleep » Volume 17

Prevalence and Risk Factors of Positional Obstructive Sleep Apnea in Chinese Children: A Retrospective Study
Authors Tang A ![]() , Dai S
, Dai S ![]() , Au CT
, Au CT ![]() , Yu MWL, Li AM
, Yu MWL, Li AM ![]() , Chan KCC
, Chan KCC
Received 26 February 2025
Accepted for publication 1 September 2025
Published 11 November 2025 Volume 2025:17 Pages 2933—2946
DOI https://doi.org/10.2147/NSS.S521723
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Valentina Alfonsi
Agatha Tang,1 Siyu Dai,1 Chun Ting Au,1,2 Michelle Wai Ling Yu,1,3 Albert Martin Li,1,3– 5 Kate Ching-Ching Chan1,3– 5
1Department of Pediatrics, Faculty of Medicine, The Chinese University of Hong Kong, Hong Kong SAR, People’s Republic of China; 2Department of Translational Medicine, Research Institute, The Hospital for Sick Children, Toronto, ON, Canada; 3Department of Pediatrics, Prince of Wales Hospital, Hong Kong SAR, People’s Republic of China; 4Laboratory for Pediatric Respiratory Research, Li Ka Shing Institute of Health Sciences, Faculty of Medicine, The Chinese University of Hong Kong, Hong Kong SAR, People’s Republic of China; 5Hong Kong Hub of Pediatric Excellence, The Chinese University of Hong Kong, Hong Kong SAR, People’s Republic of China
Correspondence: Kate Ching-Ching Chan, Department of Pediatrics, 6/F, Lui Che Woo Clinical Sciences Building, Prince of Wales Hospital, The Chinese University of Hong Kong, Shatin, N.T., Hong Kong SAR, People’s Republic of China, Email [email protected]
Objective: To investigate the prevalence, characteristics, risk factors, and clinical outcomes of positional obstructive sleep apnea (POSA) in Chinese children.
Methods: This was a retrospective analysis of children aged 4– 17 years with OSA from local referrals for sleep-disordered breathing. Children who underwent diagnostic polysomnography (PSG) with at least 30 minutes of total sleep time in both supine and non-supine sleep were included. Standardized sleep questionnaires, Sleepiness Scales, Child Behavior Checklist and 24-hour ambulatory blood pressure monitoring were completed. OSA was defined as obstructive apnea-hypopnea index (OAHI) ≥ 1/h. POSA was defined as OAHI in the supine position ≥ two times the OAHI in the non-supine position.
Results: 314 children (mean age: 10.88± 3.22 years; male: 70%) with OSA were analyzed, of whom 147 (46.8%) had moderate/severe OSA (OAHI≥ 5). Prevalence of POSA was 58% within our cohort and 51% among those with moderate/severe OSA. Children with POSA were older (10.8± 3.3 years vs 9.1± 2.6 years; p< 0.001), had milder disease [OAHI 4.12 (2.14– 8.62) events/h vs 6.16 events/h); p=0.026] and had smaller tonsillar size (55% vs 72%; p=0.011). By logistic regression, POSA was associated with older age (OR 1.20; 95% confidence interval (CI) 1.09– 1.32; p< 0.001) and lower OAHI (B– 0.036; SE 0.011; OR 0.964; 95% CI 0.943– 0.986; p=0.001).
Conclusion: POSA is a prevalent phenotype seen in children, demonstrating strong associations with older age, more mature pubertal development, smaller tonsillar size and milder disease severity. Future studies should also delineate the natural history and longitudinal stability of this subtype over time.
Keywords: obstructive sleep apnea, sleep-disordered breathing, supine position, children, prevalence, risk factor
Introduction
Obstructive sleep apnea (OSA) in children is a prevalent sleep-related breathing disorder associated with a wide spectrum of morbidities, including neurobehavioral, cardiovascular, and metabolic complications.1–5 Recent studies have noted an increasing trend in OSA prevalence among the pediatric population, where the current estimated prevalence is around 5.7%, with higher rates among specific populations, such as obese children.6 Given OSA’s heterogeneity, early identification of risk factors is essential in providing timely targeted treatment based on the underlying cause. Currently, numerous risk factors have been found to be associated with the development of OSA, with obesity, craniofacial anomalies and adenoid and tonsillar hypertrophy as one of the most common predisposing factors.7 With regards to treatment of OSA, adenotonsillectomy remains the first-line treatment for children with adenotonsillar hypertrophy, while continuous positive airway pressure (CPAP) is generally regarded as the treatment of choice for those having persistent disease after surgery and for those not suitable for surgery.8,9 Further research, however, is needed to address the gaps in phenotype-driven management in the pediatric population.
Positional OSA (POSA), commonly defined as an obstructive apnea hypopnea index (OAHI) in the supine position ≥ two times the OAHI in the non-supine position, is one of the distinct clinical phenotypes in which obstructive respiratory events occur predominantly while sleeping in the supine position.10–12 Around 19–58% of children with OSA are identified as having POSA.10 This phenomenon may result from supine-induced morphological changes; specifically, the velopharynx transforms into a more elliptical shape with a reduced anteroposterior diameter but similar cross-sectional area due to the gravitational force favoring the posterior collapse of soft tissue located anterior to the velopharynx, thus resulting in a more collapsible airway.13,14 Importantly, craniofacial morphology and upper airway anatomy exhibit significant ethnic variation. Studies reveal that Chinese patients typically exhibit reduced soft tissue volume, smaller retropalatal airway dimensions, and greater craniofacial bony restriction compared to Europeans.15,16 These anatomical disparities likely contribute to ethnic variations in OSA pathophysiology, clinical characteristics and treatment responsiveness. Elucidating these ethnicity-specific risk profiles, clinical characteristics and disease mechanisms may therefore enable the development of precision therapies optimized for distinct ethnic groups.15 In the pediatric population, positional effects may further interact with age, location of upper airway obstruction, and comorbidities such as obesity or Down syndrome, underscoring the need for tailored, multifactorial management approaches.17–22
As most of the obstructive respiratory events in POSA occur in the supine position, positional therapy has become a potential non-invasive treatment strategy where a lateral sleep position is achieved by a positional device. Before embarking on the evidence of positional therapy in children, understanding the prevalence, risk factors and characteristics commonly seen in those with POSA are essential. However, such data in the pediatric population are limited, particularly polysomnographic characteristics associated with the development of POSA. Existing studies focus predominantly on specific pediatric populations, such as children with obesity23 or Down syndrome,22 whose distinct anatomical and physiological profiles may limit generalizability of findings. Given these limitations and known ethnic variations in airway anatomy, our study aimed to investigate the prevalence, characteristics, and risk factors of POSA in otherwise healthy Chinese children.
Methods
Study Design and Participants
This study was a retrospective analysis of a hospital-based cohort with data drawn from the sleep research database of the Department of Pediatrics, Prince of Wales Hospital (PWH), a tertiary pediatric respiratory and sleep referral center, from October 2009 to October 2022. Referrals for sleep-disordered breathing were mainly from public and private primary care services and pediatric units of regional hospitals throughout Hong Kong. In this study, Chinese children and adolescents aged 4–17 years with suspected sleep-disordered breathing who had a diagnosis of OSA (see definition of OSA in Polysomnography and Definitions) confirmed by an overnight sleep study (polysomnography, PSG) were included. The sample size was determined by the available records rather than a priori calculation. Data from 1746 children were screened, however, only 501 children remained after exclusion, as illustrated in Figure 1. Among the remaining children, 314 had OSA (OAHI ≥1), of whom 147 (46.8%) of them had moderate/severe OSA (OAHI ≥5). Participants were further classified as having either POSA or non-POSA as seen in Figure 1. Meanwhile, patients with genetic, syndromal or metabolic disease, congenital or acquired neuromuscular disease, craniofacial abnormalities, structural or congenital heart disease, severe chronic respiratory disease that may affect the oxygen saturation or ventilation during sleep, previous adenotonsillectomy and current treatment with positive airway pressure, positional device or orthodontic device were excluded. To ensure the reliability of the diagnosis of POSA, children with less than 30 minutes of total sleep time spent in supine or non-supine position during the sleep study were also excluded; this enabled sufficient time for observation of OSA at different sleep stages, thereby reducing the risk of over- or under-estimation of positional OAHI.10,11,23,24 Written informed consent was obtained from parents or legal guardians of eligible children for their participation and data utilization in this research. For data analysis, children and adolescents aged 4 to 17 years old with a diagnostic polysomnography (PSG) performed at our center were included; participants with acute illness within 4 weeks from the PSG test date would have their PSG rescheduled. To delineate whether the respiratory events were position-dependent, at least 30 minutes of total sleep time in the supine and non-supine position were included.10,11,25 This study was conducted in accordance with the principles of the Helsinki Declaration and was approved by The Joint Chinese University of Hong Kong – New Territories East Cluster Clinical Research Ethics Committee – approval: CRE-2013.011 and 2017.710. Although an a priori sample size calculation was not performed due to the retrospective nature of the study, the inclusion of a relatively large number of cases strengthens the reliability and statistical validity of the findings.
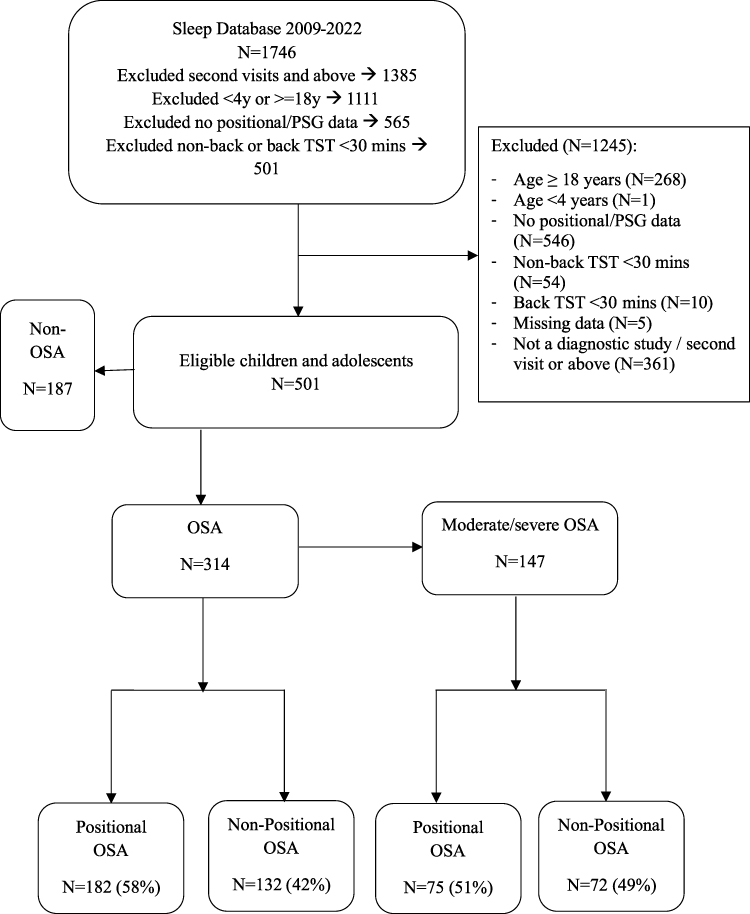 |
Figure 1 Study flow chart. |
Data Collection and Anthropometric Measurements
Data obtained from parents and participants incorporated information from various validated sleep questionnaires, such as the Hong Kong Children Sleep Questionnaire (HK-CSQ), as well as included past personal and family medical history.26 Participants also completed a 1-week sleep diary prior to their hospital admission for PSG, the modified Epworth sleepiness scale for children,27 the Pediatric Daytime Sleepiness Scale (PDSS),28 the OSA-1829,30 and the Child Behavior Checklist (CBCL).31 Permission was obtained to use the PDSS, ESS and CBCL for this study. We have requested for permission from the developer of OSA-18 and have cited their original publication for transparency and accountability. Since the HK-CSQ was developed by our team, no external permission was needed for its use. Modified ESS and PDSS were used to evaluate the sleepiness of participants, with higher scores suggesting greater propensity to fall asleep. Meanwhile, OSA severity and its impact on one’s quality of life (QOL) were reflected in the OSA-18, where higher scores indicated more severe OSA symptoms and poorer QOL. Lastly, behavioral problems were assessed using the CBCL.
Anthropometric measurements were performed on the day of PSG. Body Mass Index (BMI) was calculated as weight/height2 (kg/m2) and converted to z-scores appropriate for age and sex according to local reference.32 Standing height without shoes was measured with a Harpenden stadiometer (Holtain) to the nearest 0.1 cm, and body weight with the lightest clothing was obtained with an electronic weighing scale to the nearest 0.1 kg (BF-522; Tanita). Overweight and obesity were defined as a BMI z-score (BMIz) of ≥1.036 and ≥1.645, corresponding to the 85th and 95th percentile respectively. Waist circumference was assessed midway between the lowest rib and the superior border of the iliac crest whereas the hip circumference was at the maximal protrusion of the buttocks. The circumference was given as the mean of two measurements to the nearest 0.1cm.33 Pubertal stage was recorded with a validated self-assessment questionnaire to categorize Tanner stages with Tanner stage 1 signifying prepubertal.34
Polysomnography and Definitions
A single overnight PSG was performed in a dedicated sleep laboratory with SiestaTM 802 PSG monitor (Compumedics Telemed, Abbotsford, Victoria, Australia) recording the following parameters: electroencephalogram (F4/A1, C4/A1, O2/A1), bilateral electrooculogram, electromyogram of mentalis activity, and bilateral anterior tibialis. Electrocardiogram and heart rate were continuously recorded from two anterior chest leads. Arterial oxyhemoglobin saturation (SaO2) was measured by an oximeter with a finger probe. Respiratory movements of the chest and abdomen were measured by inductance plethysmography. Respiratory airflow was detected via an oronasal thermal sensor, while airflow pressure was measured via a nasal catheter placed in the anterior nares and was connected to a pressure transducer. Snoring was measured using a microphone placed near the throat. Body position was monitored via a body position sensor. An adequate overnight PSG was defined as a recorded total sleep time of ≥6 hours. All computerized sleep data were manually edited and scored by experienced PSG technologists and clinicians according to standardized criteria. Respiratory events including obstructive apneas, mixed apneas, central apneas, and hypopneas were manually scored based on the American Academy of Sleep Medicine (AASM) Manual for the Scoring of Sleep and Associated Events,35–37 where only those lasting ≥2 breaths irrespective of its duration were scored. Obstructive apnea was defined as ≥90% drop in airflow for ≥ 2 breath cycles and when the event was associated with continued or increased inspiratory effort, while hypopnea was ≥30% reduction in airflow associated with arousal or a ≥3% decrease in oxygen saturation for at least 2 breath cycles.35–37 Arousal was defined as a sudden shift in EEG frequency during sleep, lasting 3 to 15 seconds, which may include the presence of alpha waves or frequencies greater than 16 Hz but simultaneously are not spindles. In REM sleep, however, only those with concomitant increases in submental EMG amplitude were considered as a state of arousal.
Obstructive apnea hypopnea index (OAHI) was defined as the total number of obstructive and mixed apneas and hypopneas per hour of sleep. OSA was defined as an OAHI ≥ 1.38 Moderate/severe OSA was defined as an OAHI ≥ 5.26,39,40 Oxygen desaturation index (ODI) was defined as the total number of dips in arterial oxygen saturation ≥3% per hour of sleep. The arousal index (ArI) was the total number of arousals per hour of sleep. Respiratory arousal index (RAI) was the total number of arousals per hour of sleep that were associated with apnea, hypopnea, or flow limitation. POSA was defined by an OAHI in the supine position ≥ two times the OAHI in the non-supine position.10,11
Twenty-Four-Hour Ambulatory Blood Pressure Monitoring
Ambulatory blood pressure (ABP) was measured on the same day as the overnight PSG, using an oscillometric monitor (model 90217; SpaceLabs Medical, Redmond, Washington) that has been validated for use in children.41 Systolic blood pressure (SBP), diastolic blood pressure (DBP), and mean arterial blood pressure (MAP) were recorded hourly from 2130 to 0700 hours and every half-hour out of this period. The cuff was placed on the non-dominant arm, with the appropriate cuff size selected based on the subject’s arm length. Mean SBP, DBP, and MAP were calculated for the awake and asleep periods; the exact cutoff time of these periods were defined through correlating the blood pressure measurements to the PSG tracing. Only those with at least 7 successful readings for both active wakefulness and sleep were deemed adequate and subsequently incorporated in the analysis.3 SBP and DBP were converted into BP z-scores using the Hong Kong reference values (relative to age, sex, and height).42 Nocturnal dipping of SBP and DBP were derived by calculating the difference between mean awake BP and mean sleep BP and expressed as a percentage of mean awake BP. Subjects with a nocturnal BP dip of < 10% were defined as “non-dippers”.43
Statistical Analysis
Statistical analyses were performed using SPSS statistical software package V.25.0 for Windows. Parametric data were expressed as mean ± standard deviation (SD), non-parametric data as median (interquartile range [IQR]), and categorical data as number (percentage). Shapiro–Wilk test was used to check for normality. T-test, Mann–Whitney U, and chi-squared tests were used for normally distributed, skewed, and categorical data, respectively, to assess differences in demographic characteristics, sleep symptoms, polysomnographic parameters and BP between those with POSA and non-positional OSA. Logistic regression was performed to examine the independent factors associated with POSA. Covariates and potential confounders included age, BMI z-score, sex, tonsil size, and obesity status. Multiple linear regression models were used to assess the associations of OSA subtypes (POSA vs non-positional OSA) with BP outcomes. Covariates and potential confounders defined as factors potentially related to childhood OSA and BP outcomes included sex, BMI z-score, age, and height. A p-value of <0.05 was considered statistically significant.
Results
Prevalence and Clinical Characteristics
A total of 1746 Chinese children from sleep research data were screened. 1245 were excluded due to the reasons listed in Figure 1. Among the remaining 501 children, 314 children had OSA, of whom 147 (46.8%) of them had moderate/severe OSA. Participants were further classified as having either POSA or non-positional OSA as seen in Figure 1. The prevalence of POSA was 58% among all with OSA, and 51% among those with moderate/severe OSA. Their demographic, anthropometric, and PSG data are summarized in Tables 1 and 2 for all children with OSA, while the description of the characteristics of children with moderate/severe OSA is provided in Supplementary Tables 1 and 2.
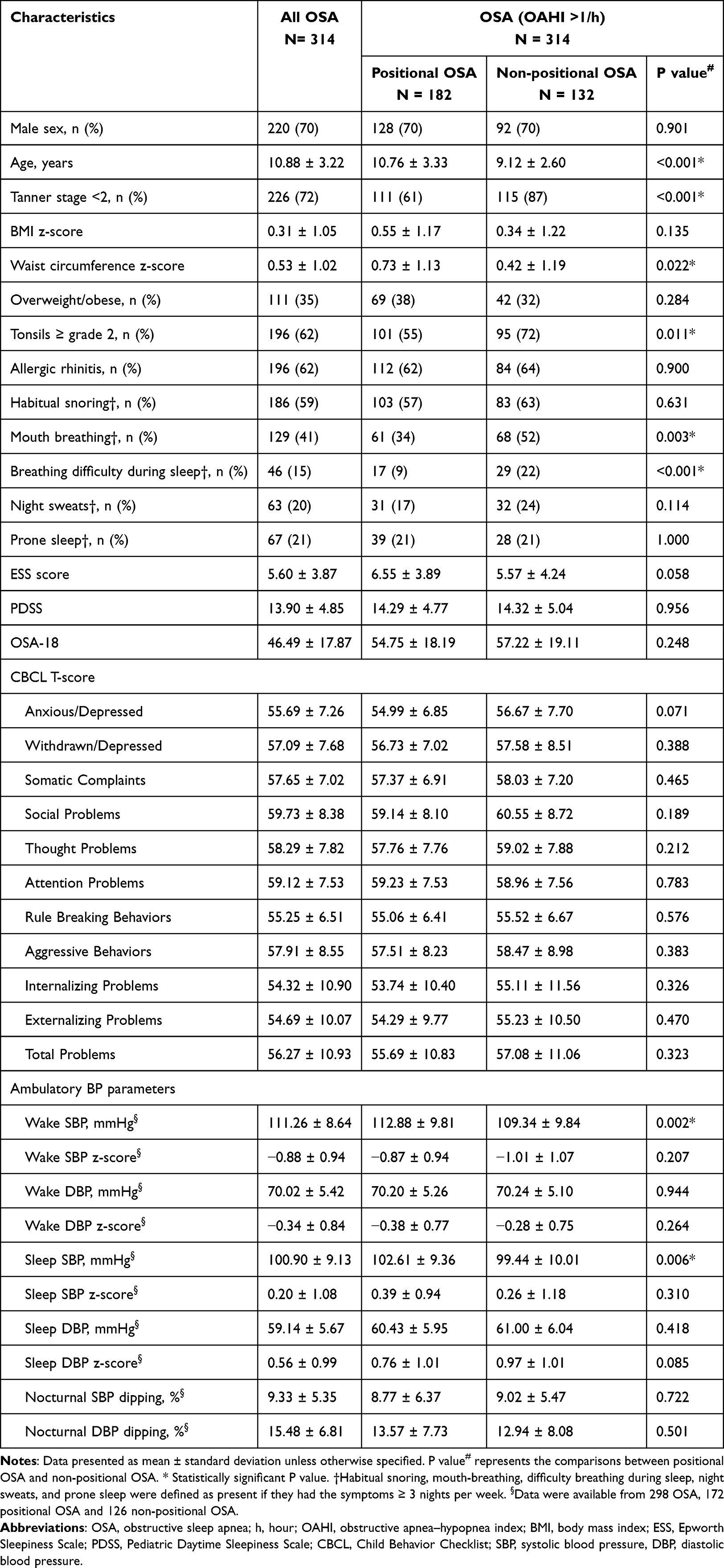 |
Table 1 Comparison of the Characteristics Between Children with Positional OSA and Those with Non-Positional OSA (N=314) |
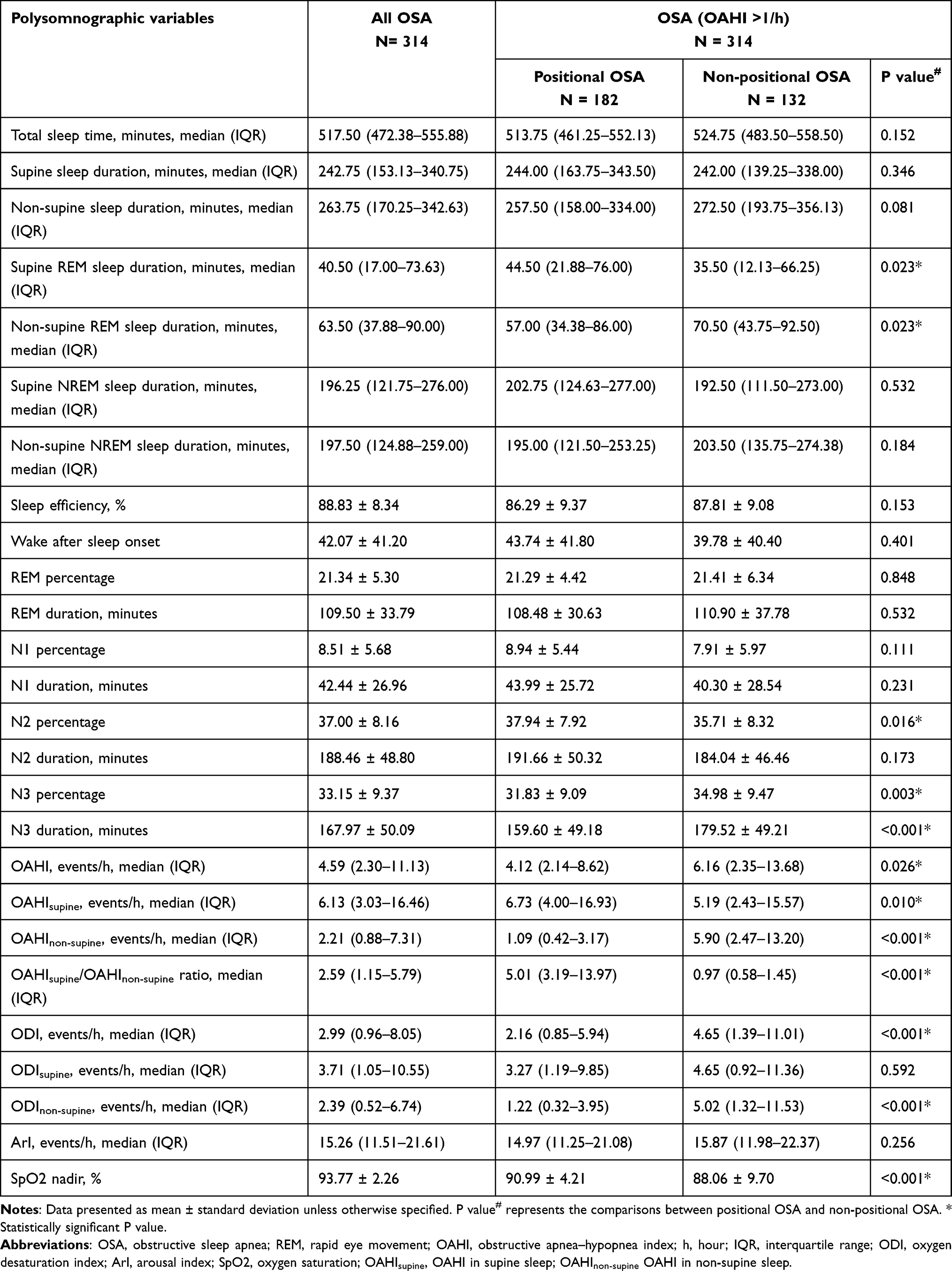 |
Table 2 Comparisons of Polysomnographic Variables Between Children with Positional OSA and Those with Non-Positional OSA (N=314) |
When compared to children with non-positional OSA, children with POSA were older (10.76 ± 3.33 vs 9.12 ± 2.60 years; p < 0.001) and had greater waist circumference z-score (0.73 ± 1.13 vs 0.42 ± 1.19; p=0.022). Fewer children with POSA were prepubertal (ie, Tanner stage < 2) (61% vs 87%; p < 0.001), had tonsil size ≥ grade 2 (55% vs 72%; p=0.011), mouth breathing during sleep (34% vs 52%; p=0.003), and breathing difficulty during sleep (9% vs 22%; p < 0.001). BMI z-scores (0.55 ± 1.17 vs 0.34 ± 1.22; p=0.135) and obesity status (38% vs 32%; p=0.284) revealed no statistically significant difference between both groups.
For the PSG parameters, the two groups had comparable total sleep time and spent similar time in supine and non-supine sleep positions. However, children with POSA had longer REM sleep duration on supine position while children with non-positional OSA had longer REM sleep duration on non-supine position. Children with POSA had shorter N3 percentage and duration than their counterparts. There was a lower median OAHI [4.12 (IQR 2.14–8.62) vs 6.16 (2.35–13.68) events/h; p=0.026), lower ODI [2.16 (0.85–5.94) vs 4.65 (1.39–11.01) events/h; p < 0.001), and a higher mean SpO2 nadir (90.99 ± 4.21% vs 88.06 ± 9.70%; p < 0.001) in POSA group than the non-positional OSA group.
Clinical Outcomes of Children with Positional OSA
There were no statistically significant differences in the clinical outcomes of children with POSA and non-positional OSA, as reflected by the ESS, PDSS, OSA-18 and CBCL scores. The CBCL score encompassed multiple domains, ranging from somatic complaints to psychological manifestations.
Predictors for Positional OSA in Children
Through logistic regression, two variables were identified as significant predictors associated with POSA in children as seen in Table 3. Older age (Odds ratio 1.20; 95% confidence interval (CI) 1.09–1.32; p<0.001) was positively associated with POSA, whereas OAHI (Odds ratio 0.964; 95% CI 0.943–0.986; p=0.001) was inversely associated with POSA. In contrast, BMI z-scores (Odds ratio 1.142; 95% CI 0.928–1.405; p=0.210) were not significantly associated with POSA. Similarly, waist circumference z-scores, after adjustment for age and sex, showed no significant association with POSA (Odds ratio 1.11; 95% CI 0.89–1.37; p=0.36). Findings remained consistent when the analysis was confined to children with moderate/severe OSA (Supplementary Table 3). Given that this study involved Chinese children, validation in multiethnic cohorts is needed to establish universal predictors.
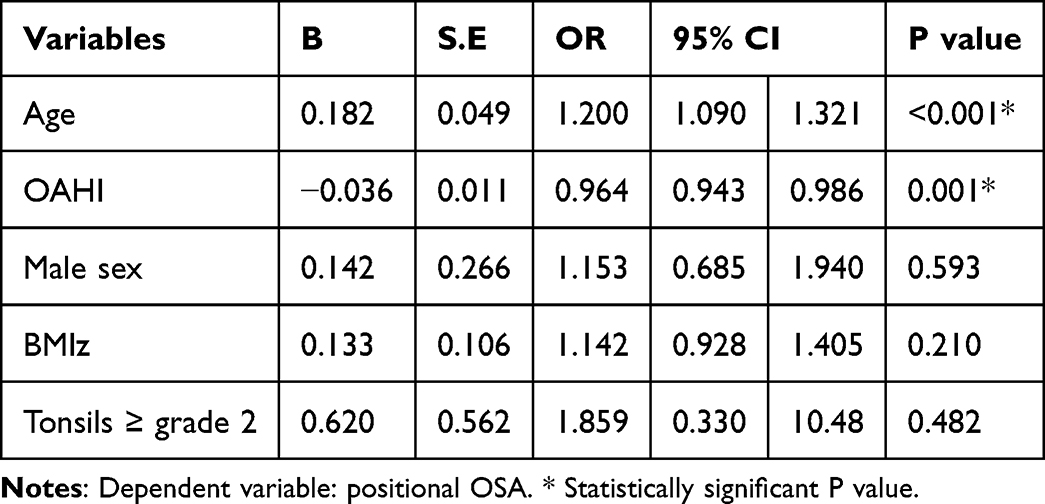 |
Table 3 Predictors for Positional OSA in Children by Logistic Regression (N=314) |
Association Between Positional OSA and Blood Pressure
Higher wake SBP (112.88 ± 9.81 vs 109.34 ± 9.84 mmHg; p=0.002) and sleep SBP (102.61 ± 9.36 vs 99.44 ± 10.01 mmHg; p=0.006) were observed in those with POSA compared to the non-positional OSA group (Table 1). However, there were no statistically significant differences in the BP z-scores between the two groups. By linear regression, POSA was not significantly associated with wake or sleep SBP after adjusting for sex, BMIz, height and OAHI (Tables 4 and 5). Nevertheless, future studies involving larger cohorts may explore whether statistically significant differences in BP can be found between both groups after adjusting for confounders and measuring BP over 28 nights.44
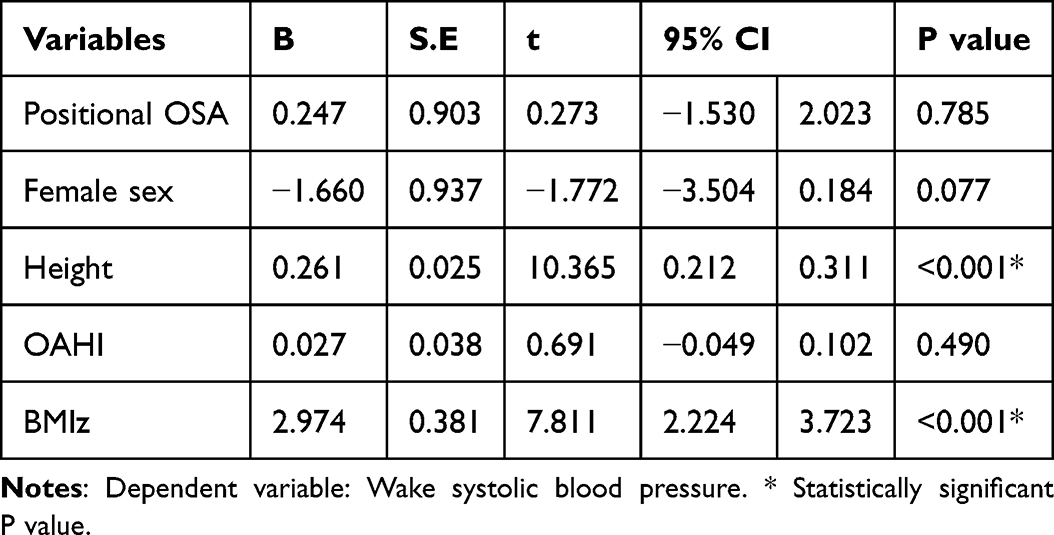 |
Table 4 Associations Between Positional OSA and Wake Systolic Blood Pressure in Children by Linear Regression (N=298) |
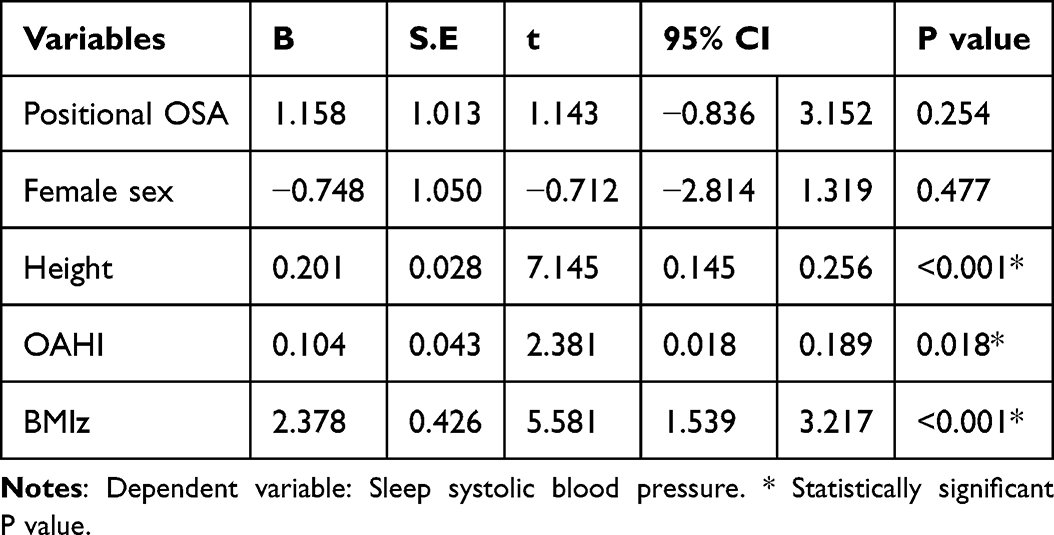 |
Table 5 Associations Between Positional OSA and Sleep Systolic Blood Pressure in Children by Linear Regression (N=298) |
Discussion
Our study explored the prevalence, characteristics and predictive factors of POSA in children. The prevalence of POSA was 58% among all children with OSA, and 51% among those with moderate/severe OSA. When compared to children with non-positional OSA, children with POSA were older, had a more advanced pubertal development and had less severe OSA as measured by OAHI. The relationship between POSA and advanced pubertal development has rarely been reported; this highlights the need for future studies to validate the generalizability of this association across ethnicities and investigate whether underlying hormonal mechanisms drive the development of POSA. Fewer children with POSA had large tonsils, mouth breathing and breathing difficulty during sleep. In regression analysis, older age and lower OAHI were significantly associated with POSA in children. There were no statistically significant differences in other outcomes, such as ambulatory blood pressure, daytime sleepiness, OSA-18 and CBCL scores, between the two groups.
The high prevalence of POSA in our study population aligned broadly with previous publications, though prevalence rates still varied across studies, potentially attributable to differences in diagnostic criteria and population characteristics.11,23,25 POSA is commonly identified when the frequency of respiratory events is at least twice as high in the supine position compared to the non-supine position and with children’s sleep time in both supine and non-supine positions longer than 30 minutes. Previous studies in children adopted similar diagnostic criteria but with variations in the study population or required sleep duration in different body positions. For instance, Selvadurai et al focused on obese children with OSA with an overall OAHI ≥5 events/hour and at least 20 minutes spent in both supine and non-supine positions. They reported a higher prevalence (58%) of POSA compared to other studies.23 Meanwhile, Wu et al reported a lower prevalence of POSA of 38.2%, a finding that may be explained by the younger study population of Chinese children aged 2–12 years with a diagnosis of OSA and OAHI >1 event/hour.25 On the other hand, Verhelst et al studied a heterogeneous group of children with younger age, moderate/severe OSA (OAHI >5 events/hour), with or without comorbidities, and reported a lower prevalence at 19%.11 Despite these variations, the high prevalence of POSA in our study population underscores the need for early identification of OSA phenotypes in children to guide targeted interventions. While positional therapy is first-line for adults with POSA, anatomical and pathophysiological differences in children necessitate pediatric-specific validation. Notably, POSA was associated with milder disease severity, suggesting distinct mechanistic pathways among OSA phenotypes that warrant further research into phenotype-specific management approaches.
Consistent with some previous studies, our results revealed that older age and less severe OSA were associated with POSA in all children with OSA and also among those with moderate/severe disease.11,25 POSA may represent a distinct clinical phenotype within paediatric OSA, often characterized by milder disease severity and unique physiological or anatomical traits.11 Older children may be more likely to exhibit POSA due to developmental changes in upper airway anatomy and sleep architecture. As children age, the impact of adenotonsillar hypertrophy on upper airway obstruction may diminish, and other factors such as body position and body fat distribution become more prominent contributors to airway collapsibility.45,46 The time that children spend in supine and non-supine positions during sleep may also modulate the interactions between severity of respiratory events and the positional nature of their OSA.45 In line with these observations, children with POSA demonstrated more mature pubertal development, had smaller tonsil size and had fewer OSA symptoms such as breathing difficulty and mouth breathing during sleep. However, no significant differences in blood pressure and behavioral outcomes were detected between the disease subtypes.
Our findings revealed that children with POSA had higher BMI z-scores and significantly higher waist circumference z-scores compared to those with non-positional OSA, highlighting a pattern of increased central adiposity. Our results align with some previous evidence of a bidirectional relationship between obesity and POSA.11,23,45 The higher waist circumference in children with POSA suggest that the central adiposity may play a critical role in positional airway obstruction. These findings underscore the importance of identifying obesity-related risk factors to optimize management of POSA in children.45
Our data revealed the potential role of OSA severity, as delineated by the OAHI, ODI and oxygen saturation nadir, in reflecting the development of POSA. With no statistically significant difference in median supine and non-supine sleep duration, a negative correlation between OAHI and POSA was observed, where children with non-positional OSA demonstrated higher OAHI and ODI, and lower oxygen saturation nadir. These findings are supported by existing literature, which suggests that POSA often presents as a milder disease overall when compared to non-positional OSA.23,25 The exact mechanism behind the interaction between disease severity and POSA has yet to be explored. It is also unclear why in some individuals, the upper airway obstruction and respiratory events predominantly occur in the supine position, while in others, the development of respiratory events is not determined by body position.21,25 In the adult population, higher collapsibility and smaller minimum cross-sectional area of the upper airway have been demonstrated in patients with non-positional OSA compared to their positional counterparts, thereby potentially contributing to an overall more severe disease regardless of the sleep position.13,47,48 Furthermore, a recent study reported that patients with POSA demonstrated a lower loop gain, lower arousal thresholds, lower airway collapsibility and higher muscle compensation compared to those with non-positional OSA, and they were found to be crucial factors in predicting POSA severity.47 Although the observed differences in endotypic traits between individuals with POSA and counterparts may shed some light regarding the disease mechanism, the interpretation needs to be cautious. Firstly, the findings require further studies to confirm, and their exact role in the disease mechanism of POSA has yet to be investigated. Secondly, the observations were all driven by data from adult studies and may not be directly extrapolated to the pediatric population.
The blood pressure analysis revealed no statistically significant differences between POSA and non-positional OSA groups after adjusting for sex, BMIz, height and OAHI. Our regression analysis indicated that among children with OSA, height and BMI z-score were significantly associated with blood pressure, but not the positional subtype. This finding suggests that the positional subtype of OSA does not independently influence blood pressure outcomes. In our study population, the major determinants of blood pressure in children with OSA appear to be related to growth parameters rather than the specific type of OSA. Future studies are needed to further investigate whether respiratory events predominantly occurring in the supine position have any substantial effect on the cardiovascular system compared to the overall severity of OSA.
Our study demonstrated distinct REM sleep distribution patterns in pediatric OSA: children with POSA exhibited longer supine REM sleep, whereas children with non-positional OSA had a longer non-supine REM sleep duration. Given the known changes in airway collapsibility at different sleep stages, with respiratory events occurring more commonly during REM sleep, prolonged supine REM sleep may elevate respiratory event frequency in that sleep position, potentially biasing POSA classification.24 Our data underscored the importance of considering the interplay between sleep stage (REM and non-REM) and sleep position (supine and non-supine), exploring their influence on subtype classification of POSA. Notably, Kevat et al demonstrated that non-supine positioning effectively reduced obstructive events in REM-predominant OSA, suggesting positional therapy remained beneficial in REM-related OSA.49 Moving forward, longitudinal studies should explore how REM sleep distribution patterns evolve with age, particularly during pubertal airway remodeling, to optimize phenotype-specific management and identify critical windows for intervention.
This study, however, has several important limitations. First, as a hospital-based cohort instead of a population-based cohort, our results may overrepresent severe OSA cases and lack generalizability to community populations. However, our analysis revealed similar characteristics associated with POSA in both children with OSA and children with moderate/severe OSA. Second, the high exclusion rate (71% of screened cohort), raises concerns about selection bias, limiting the external validity of the observed associations. Furthermore, as this was a retrospective study, the lack of longitudinal data makes it challenging to determine if the observed associations drive POSA development or are simply epiphenomena. There is a potential dynamic nature of POSA as shown by a recent study, indicating that POSA status may not be stable over time, especially in the context of growth, weight changes, or evolving airway anatomy. Therefore, ongoing assessment is important viewing the potential transition between POSA and non-POSA subtypes.50 Third, the current POSA definition also has intrinsic constraints. Previous studies have shown inherent variability in supine-related polysomnographic phenotypes across different sexes, as well as potential fluctuations based on exact head and neck sleeping positions.24 Specifically, night to night repeatability of supine-related polysomnographic phenotype exists predominantly in males and those with low non-supine AHI, where a minimum observed time in a supine position of 30 minutes was applied.24 Thus, the night-to-night variability along with the lack of a strict definition of the sleeping position of POSA may restrict the use of the current POSA definition in clinical practice or research purposes.51 Fourth, as the definition of OSA severity in our study did not follow the AASM and distinguish between moderate and severe OSA, this may obscure potential differences in predictive factors between these subgroups. Lastly, as discussed before, there may be a potential sampling error due to changes in sleep stage throughout one’s sleep. If the duration of supine and non-supine sleep recorded was less than 60 minutes, for example, this may only coincide with a specific sleep stage. At different sleep stages, there are varying effects on airway collapsibility; slow wave sleep, for example, is often associated with an improvement in airway collapsibility, while OSA typically worsens during REM sleep.52,53 These differences can subsequently affect the supine and non-supine OAHI.53 Thus, this warrants further investigation into the optimal sampling time by exploring the relationship of airway collapsibility at different sleep stages to optimize the diagnosis and achieve a more confident and repeatable classification of the POSA subtypes.
Conclusion
To conclude, POSA was significantly associated with older age, milder disease, advanced pubertal development and smaller tonsillar size in Chinese children. Anatomical differences in upper airway between different ethnicities may limit the generalizability of the findings. Thus, future studies may explore the validity of these associations in multiethnic cohorts. Given the cross-sectional nature of this study, longitudinal studies are also warranted to evaluate the natural history and stability of this OSA phenotype over time. Early identification of this OSA phenotype may play a role in driving therapeutic direction, as adult studies have shown positional therapy as a safe alternative to CPAP for those with POSA.54 Nevertheless, pathophysiological and anatomical differences between pediatric and adult OSA highlight the need for further studies to evaluate the efficacy of various OSA treatment modalities for different OSA phenotypes.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author, Kate C. Chan, upon reasonable request.
Acknowledgments
The authors thank all the participants and their parents for their contribution to this study.
Author Contributions
All authors made a significant contribution to the work reported, with the respective roles charted below:
A Tang, S Dai, CT Au, MW Yu, AM Li - Conceptualization, Data curation, Formal analysis, Methodology, Validation, Visualization, Writing – original draft, review and editing.
KC Chan - Conceptualization, Data curation, Formal analysis, Methodology, Validation, Visualization, Writing – original draft, review and editing, Supervision.
All authors took part in drafting, revising or critically reviewing the article, gave final approval of the version to be published, have agreed on the journal to which the article has been submitted, and agree to be accountable for all aspects of the work. The corresponding author, Kate C. Chan, had full access to all the data in the study and had final responsibility for the decision to submit for publication.
Funding
No funding was received for this research.
Disclosure
The authors declare no conflicts of interest. Preliminary findings from this study were presented at the World Sleep Congress 2023 (October 20–25, Rio de Janeiro, Brazil; https://doi.org/10.1016/j.sleep.2023.11.761) and the 4th Asian Society of Sleep Medicine Congress 2023 (December 10–13, Bangkok, Thailand; symposium presentation).
References
1. Chan KC, Shi L, So HK, et al. Neurocognitive dysfunction and grey matter density deficit in children with obstructive sleep apnea. Sleep Med. 2014;15(9):1055–1061. doi:10.1016/j.sleep.2014.04.011
2. Chan JYS, Li AM, Au CT, et al. Cardiac remodelling and dysfunction in children with obstructive sleep apnea: a community based study. Thorax. 2009;64(3):233–239. doi:10.1136/thx.2007.094904
3. Li AM, Au CT, Sung RYT, et al. Ambulatory blood pressure in children with obstructive sleep apnea: a community based study. Thorax. 2008;63(9):803–809. doi:10.1136/thx.2007.091132
4. Chan KCC, Au CT, Chook P, et al. Endothelial function in children with OSA and the effects of adenotonsillectomy. Chest. 2015;147(1):132–139. doi:10.1378/chest.14-1307
5. Chan KCC, Au CT, Hui LL, Wing YK, Li AM. Childhood OSA is an independent determinant of blood pressure in adulthood: longitudinal follow-up study. Thorax. 2020;75(5):422–431. doi:10.1136/thoraxjnl-2019-213692
6. Yang Q, Huang X, Lin Y, et al. Exploring the multifaceted landscape of pediatric obstructive sleep apnea: insights into prevalence, severity, and coexisting conditions. Nat Sci Sleep. 2024;16:359–368. doi:10.2147/NSS.S452221
7. Xu Z, Wu Y, Tai J, et al. Risk factors of obstructive sleep apnea syndrome in children. J Otolaryngol. 2020;49(1). doi:10.1186/s40463-020-0404-1
8. Marcus CL, Moore RH, Rosen CL, et al. A randomized trial of adenotonsillectomy for childhood sleep apnea. N Engl J Med. 2013;368(25):2366–2376. doi:10.1056/NEJMoa1215881
9. Marcus CL, Brooks LJ, Draper KA, et al. Diagnosis and management of childhood obstructive sleep apnea syndrome. Pediatrics. 2012;130(3):576–584. doi:10.1542/peds.2012-1671
10. Xiao L, Baker A, Voutsas G, et al. Positional device therapy for the treatment of positional obstructive sleep apnea in children: a pilot study. Sleep Med. 2021;85:313–316. doi:10.1016/j.sleep.2021.07.036
11. Verhelst E, Clinck I, Deboutte I, Vanderveken O, Verhulst S, Boudewyns A. Positional obstructive sleep apnea in children: prevalence and risk factors. Sleep Breath. 2019;23(4):1323–1330. doi:10.1007/s11325-019-01853-z
12. Joosten SA, O’Driscoll DM, Berger PJ, Hamilton GS. Supine position related obstructive sleep apnea in adults: pathogenesis and treatment. Sleep Med Rev. 2014;18(1):7–17. doi:10.1016/j.smrv.2013.01.005
13. Pevernagie DA, Stanson AW, Sheedy PF, Daniels BK, Shepard JW. Effects of body position on the upper airway of patients with obstructive sleep apnea. Am J Respir Crit Care Med. 1995;152(1):179–185. doi:10.1164/ajrccm.152.1.7599821
14. Joosten SA, Edwards BA, Wellman A, et al. The effect of body position on physiological factors that contribute to obstructive sleep apnea. Sleep. 2015;38(9):1469–1478. doi:10.5665/sleep.4992
15. Xu L, Keenan BT, Wiemken AS, et al. Differences in three-dimensional upper airway anatomy between Asian and European patients with obstructive sleep apnea. Sleep. 2019;43(5).
16. Lee RWW, Vasudavan S, Hui DS, et al. Differences in craniofacial structures and obesity in caucasian and Chinese patients with obstructive sleep apnea. SLEEP. 2010;33(8):1075–1080. doi:10.1093/sleep/33.8.1075
17. Marques M, Genta PR, Sands SA, et al. Effect of sleeping position on upper airway patency in obstructive sleep apnea is determined by the pharyngeal structure causing collapse. Sleep. 2017;40(3):zsx005. doi:10.1093/sleep/zsx005
18. Cuhadaroglu C, Keles N, Erdamar B, et al. Body position and obstructive sleep apnea syndrome. Pediatr Pulmonol. 2003;36(4):335–338. doi:10.1002/ppul.10366
19. Zhang XW, Li Y, Zhou F, Guo CK, Huang ZT. Association of body position with sleep architecture and respiratory disturbances in children with obstructive sleep apnea. Acta Otolaryngol. 2007;127(12):1321–1326. doi:10.1080/00016480701242451
20. Lackey TG, Tholen K, Pickett K, Friedman N. Residual OSA in Down syndrome: does body position matter? J Clin Sleep Med. 2023;19(1):171–177. doi:10.5664/jcsm.10288
21. Tholen K, Meier M, Kloor J, Friedman N. Persistent OSA in obese children: does body position matter? J Clin Sleep Med. 2021;17(2):227–232. doi:10.5664/jcsm.8902
22. Nisbet LC, Phillips NN, Hoban TF, O’Brien LM. Effect of body position and sleep state on obstructive sleep apnea severity in children with Down syndrome. J Clin Sleep Med. 2014;10(1):81–88. doi:10.5664/jcsm.3368
23. Selvadurai S, Voutsas G, Massicotte C, et al. Positional obstructive sleep apnea in an obese pediatric population. J Clin Sleep Med. 2020;16(8):1295–1301. doi:10.5664/jcsm.8496
24. Landry SA, Beatty C, Thomson LDJ, et al. A review of supine position related obstructive sleep apnea: classification, epidemiology, pathogenesis and treatment. Sleep Med Rev. 2023;72:101847. doi:10.1016/j.smrv.2023.101847
25. Wu Y, Zheng L, Cui G, Xu Z, Ni X. Subtypes of obstructive sleep apnea in children and related factors. J Clin Sleep Med. 2022;18(10):2397–2404. doi:10.5664/jcsm.10124
26. Li AM, Cheung A, Chan D, et al. Validation of a questionnaire instrument for prediction of obstructive sleep apnea in Hong Kong Chinese children. Pediatr Pulmonol. 2006;41(12):1153–1160. doi:10.1002/ppul.20505
27. Chan EYT, Ng DK, Chong C, et al. Modified Epworth sleepiness scale in Chinese children with obstructive sleep apnea: a retrospective study. Sleep Breath. 2009;13(1):59–63. doi:10.1007/s11325-008-0205-7
28. Yang CM, Huang YS, Song YC. Clinical utility of the Chinese version of the pediatric daytime sleepiness scale in children with obstructive sleep apnea syndrome and narcolepsy. Psychiatry Clin Neurosci. 2010;64(2):134–140. doi:10.1111/j.1440-1819.2009.02054.x
29. Huang YS, Hwang FM, Lin CH, Lee LA, Huang PY, Chiu ST. Clinical manifestations of pediatric obstructive sleep apnea syndrome: clinical utility of the Chinese-version Obstructive Sleep Apnea Questionaire-18. Psychiatry Clin Neurosci. 2015;69(12):752–762. doi:10.1111/pcn.12331
30. Franco RA, Rosenfeld RM, Rao M. Quality of life for children with obstructive sleep apnea. Otolaryngology. 2000;123(1):9–16. doi:10.1067/mhn.2000.105254
31. Leung PWL, Kwong SL, Tang CP, et al. Test-retest reliability and criterion validity of the Chinese version of CBCL, TRF, and YSR. J Child Psychol Psychiatr. 2006;47(9):970–973. doi:10.1111/j.1469-7610.2005.01570.x
32. Leung SS, Cole TJ, Tse LY, Lau JT. Body mass index reference curves for Chinese children. Ann Hum Biol. 1998;25(2):169–174. doi:10.1080/03014469800005542
33. Sung RYT, So HK, Choi KC, et al. Waist circumference and waist-to-height ratio of Hong Kong Chinese children. BMC Public Health. 2008;8:324. doi:10.1186/1471-2458-8-324
34. Chan NPT, Sung RYT, Kong AP, Goggins WB, So HK, Nelson EAS. Reliability of pubertal self-assessment in Hong Kong Chinese children. J Paediatr Child Health. 2008;44(6):353–358. doi:10.1111/j.1440-1754.2008.01311.x
35. Iber C, Ancoli-Israel S, Chesson AL, et al. The AASM Manual for the Scoring of Sleep and Associated Events: Rules, Terminology and Technical Specifications.
36. Berry RB, Brooks R, Gamaldo CE, et al. The AASM manual for the scoring of sleep and associated events: rules, terminology and technical specifications. Version 2.0. Darien, Illinois: American Academy of Sleep Medicine; 2012.
37. Berry RB, Brooks R, Gamaldo CE, et al. The AASM manual for the scoring of sleep and associated events: rules, terminology and technical specifications. Version 2.4. Darien, IL: American Academy of Sleep Medicine; 2017.
38. Sateia MJ. International classification of sleep disorders-third edition: highlights and modifications. Chest. 2014;146(5):1387–1394. doi:10.1378/chest.14-0970
39. Gouthro K, Slowik JM. Pediatric Obstructive Sleep Apnea. StatPearls; 2023.
40. Solano-Pérez E, Coso C, Castillo-García M, et al. Diagnosis and treatment of sleep apnea in children: a future perspective is needed. Biomedicines. 2023;11(6):1708. doi:10.3390/biomedicines11061708
41. O’Brien E, Asmar R, Beilin L, et al. European Society of hypertension recommendations for conventional, ambulatory and home blood pressure measurement. J Hypertens. 2003;21(5):821–848. doi:10.1097/00004872-200305000-00001
42. Yip GWK, Li AM, So HK, et al. Oscillometric 24-h ambulatory blood pressure reference values in Hong Kong Chinese children and adolescents. J Hypertens. 2014;32(3):606–619. doi:10.1097/HJH.0000000000000062
43. Flynn JT, Daniels SR, Hayman LL, et al. Update: ambulatory blood pressure monitoring in children and adolescents. Hypertension. 2014;63(5):1116–1135. doi:10.1161/HYP.0000000000000007
44. Schwarz EI. Night-to-night variability in obstructive sleep apnea: when might a multi-night measurement be helpful? Expert Rev Respir Med. 2025;19(2):73–76. doi:10.1080/17476348.2025.2457370
45. Wang Q, Huang G, Wang R, et al. Evaluating positional obstructive sleep apnea in children: prevalence, characteristics, and risk factors. Nat Sci Sleep. 2024;16:1569–1581. doi:10.2147/NSS.S481742
46. Huang X, Gong X, Gao X. Age-related hypertrophy of adenoid and tonsil with its relationship with craniofacial morphology. BMC Pediatric. 2023;23(1):163. doi:10.1186/s12887-023-03979-2
47. Wang X, Zhou T, Huang W, et al. Differences in physiologic endotypes between nonpositional and positional OSA: results from the Shanghai sleep health study cohort. Chest. 2024;166(1):212–225. doi:10.1016/j.chest.2024.01.021
48. Kastoer C, Benoist LB, Dieltjens M, et al. Comparison of upper airway collapse patterns and its clinical significance: drug-induced sleep endoscopy in patients without obstructive sleep apnea, positional and non-positional obstructive sleep apnea. Sleep Breath. 2018;22(4):939–948. doi:10.1007/s11325-018-1702-y
49. Kevat A, Alwadhi D, Chew AX, et al. Positional obstructive sleep apnea in children prescribed continuous positive airway pressure therapy for obstructive sleep‐disordered breathing. J Sleep Res. 2025;34. doi:10.1111/jsr.14443
50. Dai S, Yang M, Au CT, et al. Supine position-related obstructive sleep apnea in children: insights from the childhood adenotonsillectomy trial. Sleep Breath. 2025;29(4):230. doi:10.1007/s11325-025-03393-1
51. Joosten SA, O’Donoghue FJ, Rochford PD, et al. Night-to-night repeatability of supine-related obstructive sleep apnea. Ann Am Thoracic Soc. 2014;11(5):761–769. doi:10.1513/AnnalsATS.201309-306OC
52. Huang J, Karamessinis LR, Pepe ME, et al. Upper airway collapsibility during REM sleep in children with the obstructive sleep apnea syndrome. Sleep. 2009;32(9):1173–1181. doi:10.1093/sleep/32.9.1173
53. Carberry JC, Jordan AS, White DP, Wellman A, Eckert DJ. Upper airway collapsibility (Pcrit) and pharyngeal dilator muscle activity are sleep stage dependent. Sleep. 2016;39(3):511–521. doi:10.5665/sleep.5516
54. Gao Y, Zhu S, Li W, Lai Y. Comparative efficacy of sleep positional therapy, oral appliance therapy, and CPAP in obstructive sleep apnea: a meta-analysis of mean changes in key outcomes. Front Med. 2025.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Prevalence, Clinical Profile and Risk Factors of Nosocomial Infection in Ayder Pediatric Intensive Care Unit, Tigray, Ethiopia
Mohamed AA, Haftu H, Hadgu A, Seyoum D, Gebrekidan G, Ebrahim MM, Yusuf AA, Mustefa M
International Journal of General Medicine 2022, 15:7145-7153
Published Date: 9 September 2022
Prevalence and Factors Influencing Sarcopenia Among Community-Dwelling Older Adults Using the Asian Working Group for Sarcopenia Definition
He X, Song Y, Ma L, Ainsworth BE, Liu Y, Chen N
Clinical Interventions in Aging 2022, 17:1707-1727
Published Date: 29 November 2022
Prevalence, General and Periodontal Risk Factors of Gastroesophageal Reflux Disease in China
Liu Z, Gao X, Liang L, Zhou X, Han X, Yang T, Huang K, Lin Y, Deng S, Wang Z, Wang C
Journal of Inflammation Research 2023, 16:235-244
Published Date: 17 January 2023
Prevalence and Associated Factors of Thyroid Nodules Among 52,003 Chinese ‘Healthy’ Individuals in Beijing: A Retrospective Cross-Sectional Study
Xu J, Lau P, Ma Y, Zhao N, Yu X, Zhu H, Li Y
Risk Management and Healthcare Policy 2024, 17:181-189
Published Date: 17 January 2024
Prevalence and Risk Factors of Childhood Asthma in Jazan Region, Saudi Arabia
Gohal G, Yassin A, Darraj H, Darraj A, Maghrabi R, Abutalib YB, Talebi S, Mutaen AA, Hamdi S
Journal of Asthma and Allergy 2024, 17:33-43
Published Date: 20 January 2024