Back to Journals » Journal of Pain Research » Volume 19
Practice Patterns of Physicians Who Perform Lumbar Interlaminar Epidural Steroid Injections: A Technical Survey
Authors Hasoon J, Yost C, Leung A, Apai C, Simopoulos TT, Lo Bianco G ![]() , Viswanath O, Gill J, Robinson CL
, Viswanath O, Gill J, Robinson CL ![]()
Received 24 November 2025
Accepted for publication 7 March 2026
Published 11 March 2026 Volume 2026:19 582178
DOI https://doi.org/10.2147/JPR.S582178
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Alaa Abd-Elsayed
Jamal Hasoon,1,* Connor Yost,2,* Amanda Leung,3,* Carol Apai,4 Thomas T Simopoulos,5 Giuliano Lo Bianco,6 Omar Viswanath,7,8,* Jatinder Gill,5,* Christopher L Robinson9,*
1Department of Anesthesiology, Critical Care, and Pain Medicine, the University of Texas Health Science Center at Houston, Houston, TX, USA; 2Department of Internal Medicine, Creighton University, Phoenix, AZ, USA; 3Department of Anesthesiology, Tufts University School of Medicine, Boston, MA, USA; 4Department of Anesthesiology, Rutgers New Jersey Medical School, Newark, NJ, USA; 5Department of Anesthesiology, Critical Care, and Pain Medicine, Harvard Medical School, Beth Israel Deaconess Medical Center, Boston, MA, USA; 6Department of Anesthesiology and Pain, Foundation G. Giglio Cefalù, Palermo, Italy; 7Department of Pain Management, Creighton University School of Medicine, Phoenix, AZ, USA; 8Department of Pain Management, Mountain View Headache and Spine Institute, Phoenix, AZ, USA; 9Department of Anesthesiology and Critical Care, Division of Pain, The Johns Hopkins University School of Medicine, Baltimore, MD, USA
*These authors contributed equally to this work
Correspondence: Jamal Hasoon, Department of Anesthesiology, Critical Care, and Pain Medicine, The University of Texas Health Science Center at Houston, 6410 Fannin St, Houston, TX, 77030, USA, Email [email protected]
Introduction: Interlaminar epidural steroid injections (ESIs) are widely used for chronic spinal pain caused by disc herniation and degenerative stenosis. The interlaminar approach allows for broad medication distribution across multiple nerve roots. However, technical variations, including loss-of-resistance (LOR) technique and injection site selection, may influence efficacy and complication rates. This study examines practice patterns among interventional pain physicians, assessing technique variations and their clinical impact while exploring opportunities for standardization.
Methods: A questionnaire was distributed to interventional pain physicians from a range of specialties and practice settings who perform ESIs. Practice parameters of lumbar ESIs were surveyed including loss-of-resistance (LOR) technique, methods of accessing the epidural space via the interlaminar approach, and contrast spread patterns when using the midline approach.
Results: Among 92 respondents, 53.3% use LOR to saline, while 42.4% use LOR to air. When accessing the epidural space, 80.4% prefer an ipsilateral approach to the side of pain or pathology. Use of a paramedian approach showed wide variation, with 24.2% reporting “always”, 33.0% “most of the time”, 30.8% “sometimes”, and 12.1% “rarely”. For midline approaches, only 4.4% of physicians reported always achieving bilateral contrast spread. The majority noted achieving it “most of the time” (54.4%) or “sometimes” (36.7%). A minority indicated they rarely (2.2%) or never (2.2%) achieve bilateral spread when performing midline ILESIs.
Conclusion: Despite widespread use, significant variability exists in ESI technique. While consensus guidelines offer safety recommendations, standardization remains limited. Identifying common practices can help refine techniques and improve patient outcomes.
Keywords: chronic pain, chronic spinal pain, disc herniation, epidural steroid injection, pain management, spinal stenosis
Introduction
Epidural steroid injections (ESIs) are commonly used interventional treatment options for chronic spinal pain associated with conditions such as disc herniation, degenerative disc disease, and spinal stenosis. These disorders commonly result in radicular pain, neurogenic claudication, and functional impairment that significantly affect quality of life. Epidural administration of local anesthetics, with or without corticosteroids, is intended to reduce pain through modulation of local inflammation, nerve root irritation, and ischemia within the epidural space.1–4 However, the clinical effectiveness of ESIs, particularly in lumbar spinal stenosis, remains a subject of ongoing debate, with randomized controlled trials and meta-analyses demonstrating variable benefit.2,3,5
Several approaches can be used to access the epidural space, including interlaminar, transforaminal, and caudal approach.1,2,6 Interlaminar epidural steroid injections (ILESIs) are one of the most popular techniques to administer corticosteroids and local anesthetics into the epidural space. ILESIs are highly valued because of the ability to spread medication across multiple nerve roots. This may be advantageous in patients with multilevel pathology. For ILESIs, clinicians typically employ a loss-of-resistance (LOR) technique to confirm needle placement.1 However, there are many variations in methodologies such as choice of LOR medium, preference for midline versus paramedian approaches and decision to inject on same side as patient pathology. Clinicians vary significantly in their preferences reflecting variations in training, experience and clinical context.
Despite widespread use, there is scarcity in the literature exploring the technical aspects of ILESIs. Variations in application, including the selection of injection techniques and procedural nuances can affect critical outcomes such as spread of medication, efficacy and risk of complications. For example, LOR with air has been linked to complications such as pneumocephalus, while saline-based LOR may make it challenging to differentiate saline leakage from cerebrospinal fluid.1,7,8 Similarly, choosing between midline and paramedian techniques may involve important clinical trade-offs between targeting specific pathology and achieving broader medication distribution.6,9,10
The aim of this study was to identify differences in practice patterns among interventional pain physicians who perform ILESIs. Using data collected from a broad sample of practitioners across academic and private practice settings, we aimed to delineate prevailing preferences. By focusing on critical aspects such as the choice of LOR medium, the preferred injection site relative to pathology, the use of paramedian approaches, and contrast spread with a midline approach, this study sheds light on the diversity of interlaminar ESI techniques that are employed in practice.
Methods
Study Design
An anonymous cross-sectional questionnaire survey evaluated practice parameters of interventional pain physicians who perform ESIs. The study was approved by the Institutional Review Board at The University of Texas Health Science Center in Houston, Texas, USA (IRB Number: HSC-MS-23-0490). The study was conducted in compliance with the Declaration of Helsinki (1964) and its subsequent amendments. All participants were informed prior to data collection about the study objectives and the intent to publish findings. Participation was entirely voluntary, and responses were collected anonymously.
Questionnaire Administration
A survey link was distributed via Email to academic physicians in ACGME-approved fellowship training programs and shared through Email and social media to interventional pain physicians across academic, hospital based, and private practice settings. Responses were collected from March 1, 2024, through May 31, 2024. The link was restricted from multiple attempts on the same device to mitigate duplicate results.
Questionnaire Description
The questionnaire was developed based on the perceived clinical importance within the interventional pain community with a broad range of topics covered (Table 1). The validity and clarity of the questionnaire was pilot tested by a group of three academic interventional pain physicians prior to distribution. Due to the broad scope of the survey, key clinical aspects were categorized for separate publication. This paper focuses on the practice styles and technical approaches of physicians performing ILESIs.
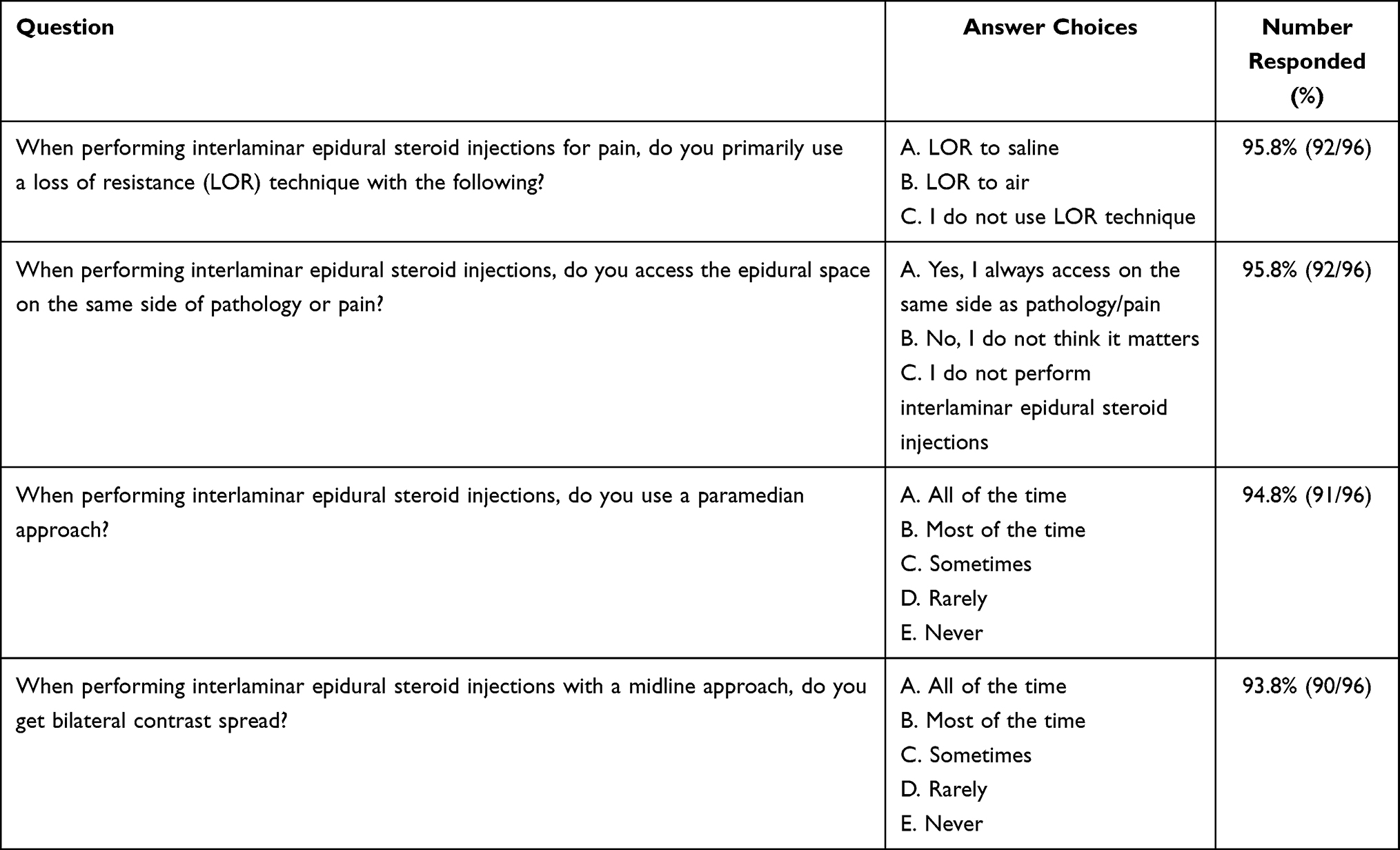 |
Table 1 Questionnaire: Question and Answer Choices and Number Responded. Total Number to Complete Was 96 |
Results
Study Cohort
The survey results are summarized below, with responses collected from March 1, 2024, to May 31, 2024. The survey included four key questions examining the techniques and practice patterns of ILESIs. Ninety-six physicians participated in the survey. Four participants declined to answer the questions on both LOR technique and ipsilateral side pathology access, five participants declined to answer the question on the use of the paramedian approach, and six participants declined to answer the question on getting bilateral contrast spread when using the midline approach (Table 1). Since the questionnaire was distributed across multiple platforms and completed on a voluntary basis, the results are based on the participants who completed the survey questions. A response rate is unavailable due to the lack of data on the participants who started but did not submit the survey.
Demographics
Physician specialty and practice setting were obtained in the questionnaire. For physician specialty, 75.0% (72/96) of physicians were anesthesiologists, 18.8% (18/96) were physiatrists, 4.2% (4/96) were neurologists, 1.0% (1/96) were radiologists, and 1.0% (1/96) were emergency medicine physicians (Table 2). For practice setting, 52.6% (50/95) were academic-based employees, 20.0% (19/95) were private practice employees, 19.0% (18/95) were hospital-based employees, and 8.4% (8/95) were private practice owners or partners (Table 2). One physician elected to skip the practice setting question. No additional demographic data was gathered.
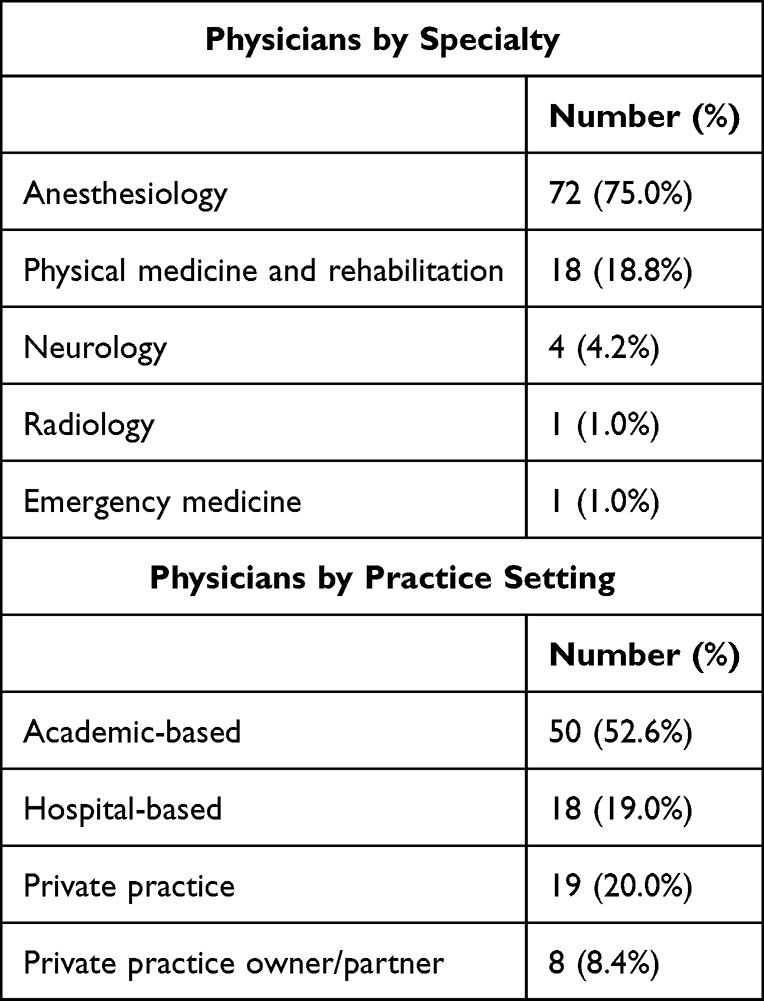 |
Table 2 Demographics |
Outcomes
Physician use of the LOR technique to saline, air, or neither when performing lumbar ESI was examined. 53.3% (49/92) of physicians report using a LOR to saline technique, 42.4% (39/92) use a LOR to air technique, and 4.3% (4/92) do not use a LOR technique (Figure 1). Ninety-two physicians answered this question with four physicians skipping this question.
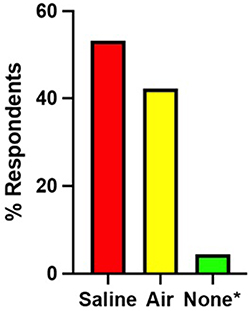 |
Figure 1 Loss of resistance technique for lumbar interlaminar epidural steroid injections. Loss of resistance (LOR) techniques to saline was the most selected option (53.3%, 49/92), followed by air (42.4%, 39/92), and none/no LOR (4.4%, 4/92). Ninety-two physicians answered this question with four physicians not answering. Questions located in Table 1. *Group does not use LOR technique. |
Access to the epidural space on the same side of the pain or pathology when performing ILESIs was examined. 80.4% (74/92) of physicians always access the epidural space from the same side of the pain or pathology, while 19.6% (18/92) do not think access from the same side of pain or pathology matters (Figure 2). The results showed that the majority of physicians access the epidural space from the same side as the pain or pathology. Again, ninety-two physicians answered this question with four physicians skipping this question.
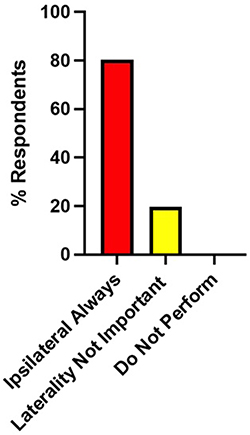 |
Figure 2 Laterality when accessing the epidural space for lumbar interlaminar epidural steroid injections based on the laterality of the pathology or pain. The most selected option was ipsilateral (80.4%, 74/92), followed by laterality was not important (19.6%, 18/92), and do not perform (0%, 0/92). Ninety-two physicians answered this question with four physicians skipping it. Questions located in Table 1. |
Physician use of a paramedian approach when performing lumbar ILESIs was examined. 24.2% (22/91) of physicians use a paramedian approach all the time, 33.0% (30/91) use a paramedian approach most of the time, 30.8% (28/91) sometimes use a paramedian approach, and 12.1% (11/91) rarely use a paramedian approach (Figure 3). There were no physicians who never use a paramedian approach. The results indicate variability in the use of the paramedian approach, with the majority favoring its routine implementation. Ninety-one physicians answered this question with five physicians skipping it.
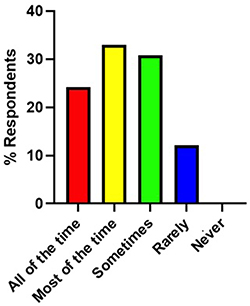 |
Figure 3 Utilization of paramedian approach for lumbar interlaminar epidural steroid injections. The distribution of practice by physicians that use a paramedian approach for lumbar interlaminar epidural steroid injections with most of the time being the most selected option (33.0%, 30/91), followed by sometimes (30.8%, 28/91), all of the time (24.2%, 22/91), rarely (12.1%, 11/91), and never (0%, 0/91). Ninety-one physicians answered this question with five physicians skipping it. Questions located in Table 1. |
The frequency of obtaining bilateral contrast spread during midline ILESI was evaluated. 4.4% (4/90) reported obtaining bilateral contrast spread with a midline approach all the time, 54.4% (49/90) obtain bilateral contrast spread most of the time, 36.7% (33/90) sometimes obtain bilateral contrast spread, 2.2% (2/90) rarely obtain bilateral contrast spread, and 2.2% (2/90) never get bilateral contrast spread when performing midline ILESIs (Figure 4). The results suggest variability in obtaining bilateral contrast spread during midline ILESIs, with many physicians routinely achieving it. Of note, ninety physicians answered this question with six physicians skipping it.
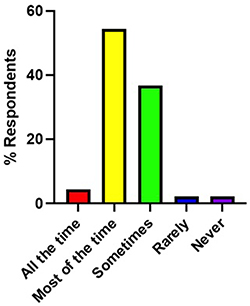 |
Figure 4 Utilization of bilateral contrast spread with a midline approach for lumbar interlaminar epidural steroid injections. The distribution of practice by physicians that get a bilateral contrast spread with a midline approach for lumbar interlaminar epidural steroid injections with most of the time being the most selected option (54.4%, 49/90), followed by sometimes (36.7%, 33/90), all of the time (4.4%, 4/90), rarely (2.2%, 2/90), and never (2.2%, 2/90). Ninety physicians answered this question with six physicians skipping it. Questions located in Table 1. |
Discussion
This study aimed to characterize contemporary practice patterns among interventional pain physicians performing lumbar ILESIs, with a focus on technical variability in loss-of-resistance technique, epidural access laterality, use of the paramedian approach, and achievement of bilateral contrast spread. Survey responses from 96 physicians demonstrated substantial heterogeneity across multiple procedural domains. These findings highlight the persistent lack of procedural standardization in ILESIs and underscore the need to better understand how technical choices may influence injectate distribution, clinical outcomes, and procedural safety.
Despite the popularity of ILESI’s, standardization has remained elusive over the years. In 2014, the Food and Drug Administration (FDA) warned “injection of corticosteroids into the epidural space of the spine may result in rare but serious adverse events, including loss of vision, stroke, paralysis, and death”. 11 In response, a consortium composed of the US FDA Safe Use Initiative, an interdisciplinary expert working group, and representatives from more than a dozen medical societies released a series of recommendations in 2015 aimed at improving the safety of ESIs.12 These “consensus opinions” endeavored to alleviate concerns surrounding catastrophic ESI complications that had arisen following the FDA’s 2014 safety warning.12 The authors unanimously agreed that epidural injections of steroids were rarely associated with serious complications due to injuries of the central nervous system.12 The group also proposed several safety-enhancing procedural guidelines, such as the use of contrast to verify accurate needle placement prior to injection.12 Nonetheless, the 2015 recommendations are broad and discretionary, leaving much to the practitioner’s discretion and individual clinical judgment. Indeed, a decade later we are a long way from standardizing ESI procedures. A 2022 survey of ESI practitioners revealed marked variability in technical approaches, both relative to the 2015 safety guidelines and among clinicians themselves.13 In the absence of a unified procedural framework and given the variability in physician training, differences in technique and approach continue to contribute to inconsistent patient outcomes.
Although our study focuses on whether practitioners use air or saline in the LOR technique, a 2018 survey of 249 physicians investigated which method they employed to identify the epidural space during ILESIs, specifically looking at LOR, hanging drop, fluid column, or fluoroscopy-only techniques.14 Within the LOR category, the 2018 study did not differentiate between the use of air or saline. However, the overall prevalence of LOR usage was comparable to our findings, with 95.7% of practitioners in our study using either saline or air for LOR, and 93.4% of practitioners utilizing LOR techniques for ILESIs in the 2018 study. The relative preference for saline over air may reflect concerns about potential complications associated with injecting air near the spinal cord, such as pneumocephalus, or may simply reflect a clinical preference.7,8
The overwhelming majority (80.4%) of our study’s respondents access the epidural space on the ipsilateral side of the targeted pathology when performing ILESIs. Accessing the epidural space ipsilaterally increases the likelihood that the injectate will reach the intended target site directly, minimizing the risk of unintended spread.2,9 Our findings also indicate that 57.2% of respondents “always” or “most of the time” use a paramedian approach, while an additional 30.8% “sometimes” employ this technique. Collectively, 87.9% of our respondents use a paramedian approach at least some of the time.
Some studies have shown that paramedian or parasagittal ILESIs may result in greater pain relief and improved functionality compared to midline ILESIs particularly when treating unilateral radicular complaints.15–18 However, other investigations comparing paramedian, midline, and transforaminal approaches for lumbar ESIs have reported comparable reductions in pain intensity (VAS scores), depression, and disability across all three techniques.19 This may help explain why 42.9% of physicians in our survey reported using the paramedian approach only “sometimes” or “rarely”, as many clinicians may perceive that its use is not essential for achieving effective clinical outcomes.
Similar to the variability observed in the use of the paramedian approach, respondents also demonstrated inconsistent success in achieving bilateral contrast spread when performing midline ILESIs. A slight majority (58.8%) report obtaining bilateral contrast spread “always” or “most of the time” when performing midline ILESIs. The final needle position appears to play a key role in determining the pattern of injectate distribution. A study of more than 400 patients undergoing lumbar ESI found that injections in which the needle tip deviated from the midline were significantly more likely to result in a unilateral block.20 It is possible that physicians intended to approach the epidural space via a midline approach, but the needle tip may inadvertently deviate to one side without the practitioner noticing. This may occur when physicians use multiplanar imaging, including lateral or contralateral oblique views, to assess needle depth and advance the needle in these views. To confirm proper trajectory and ensure the needle has not deviated from midline, an anteroposterior view should be obtained to confirm proper positioning.
A separate study further examined the relationship between injection approach and final needle tip position.21 Approximately 90% of ESIs in that study were performed using a paramedian approach, and 36% achieved bilateral contrast spread. Notably, among those cases with bilateral spread, the final needle tip was positioned at the midline in 80% of instances.21 These results suggest that final needle tip location matters more than initial injection approach. Nonetheless, anatomical variability between patients likely remains a contributing factor, potentially explaining why only 4.4% of our respondents reported “always” achieving bilateral contrast spread.
We previously published findings on practice patterns and physician perspectives on ESIs, examining the importance of precise injectate placement, perceived effectiveness for axial versus limb pain, and preference for fixed versus variable injectate volumes based on contrast spread.22 We hope the current study provides additional insight into practice variability, specifically among ILESIs.
In summary, our findings highlight the persistent heterogeneity in ILESI techniques among practitioners, despite nearly a decade of guidance aimed at improving procedural safety and consistency. Variations in approach, injectate selection, and technical execution, such as the use of air versus saline for LOR, choice of paramedian versus midline entry, and differences in achieving bilateral contrast spread underscore the ongoing need for standardized best practice recommendations. While flexibility in technique allows clinicians to tailor procedures to individual anatomy and pathology, the lack of procedural uniformity may contribute to inconsistent outcomes and complicate cross-study comparisons.
Limitations
This study has several limitations that should be acknowledged. First, because the survey was distributed across multiple platforms, an exact response rate could not be determined. Additionally, some participants did not complete all survey items or skipped individual questions; these omissions were reported and analyzed accordingly. Another limitation is the potential for sampling bias, as a notable proportion of respondents were affiliated with academic hospital settings, which may not fully reflect the broader community of interventional pain physicians in private or nonacademic practice. Furthermore, the self-reported nature of the survey introduces a risk of recall and reporting bias, as participants may have unintentionally misrepresented their procedural habits or provided responses that align with perceived professional norms. Nonetheless, the anonymous design of the survey likely mitigated some of these effects by reducing social desirability bias.
Despite these limitations, this study provides valuable preliminary data on practice patterns among interventional pain physicians performing ILESIs. These findings can serve as a foundation for future research to assess whether practice patterns evolve over time and to support efforts toward standardizing techniques for improved patient outcomes.
Conclusion
This study highlights the considerable variability in ILESI techniques among interventional pain physicians, reflecting the absence of a universally accepted standard. Differences in the use of air versus saline for loss-of-resistance, selection of midline versus paramedian approaches, and consistency in achieving bilateral contrast spread underscore the need for greater procedural alignment. While such flexibility allows physicians to tailor interventions to patient-specific anatomy and pathology, it also contributes to heterogeneity in outcomes and limits comparability across studies. Understanding these variations in physician preferences and procedural techniques can help identify opportunities for standardization, ultimately improving safety, efficacy, and patient outcomes in the performance of ILESIs for pain management.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethical Approval
This study was approved by the Institutional Review Board at the University of Texas Health Science Center at Houston (HSC-MS-23-0490). The study was performed in accordance with the Helsinki Declaration of 1964 and its later amendments. Participants were informed in advance of data collection and the intent to publish results. Participation was anonymous and voluntary.
Acknowledgments
Jamal Hasoon, Connor Yost, and Amanda Leung are co-first authors for this study. Omar Viswanath, Jatinder Gill, and Christopher L Robinson are co-senior authors for this study. The authors would like to thank the participants of the study and the Institutional Review Board who reviewed the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The present investigation did not receive external funding, and no financial conflicts of interest influenced its design, conduct, or reporting.
Disclosure
Omar Viswanath and Christopher L Robinson are Editorial Board members of Journal of Pain Research. Jamal Hasoon reports personal fees from Nevro, Biotronik, and SPR Therapeutics, outside the submitted work. The other authors declare no relevant conflicts of interest for this work.
References
1. Lee E, Lee JW, Kang HS. Interlaminar versus transforaminal epidural steroid injections: a review of efficacy and safety. Skeletal Radiol. 2023;52(10):1825–9. PMID: 35859019. doi:10.1007/s00256-022-04124-3
2. Wilkinson IM, Cohen SP. Epidural steroid injections. Curr Pain Headache Rep. 2012;16(1):50–59. PMID: 22090263. doi:10.1007/s11916-011-0236-9
3. Peene L, Cohen SP, Kallewaard JW, et al. 1. Lumbosacral radicular pain. Pain Pract. 2024;24(3):525–552. PMID: 37985718. doi:10.1111/papr.13317
4. Friedly JL, Comstock BA, Turner JA, et al. Long-term effects of repeated injections of local anesthetic with or without corticosteroid for lumbar spinal stenosis: a randomized trial. Arch Phys Med Rehabil. 2017;98(8):1499–1507.e2. PMID: 28396242. doi:10.1016/j.apmr.2017.02.029
5. Huygen F, Kallewaard JW, van Tulder M, et al. “evidence-based interventional pain medicine according to clinical diagnoses”: update 2018. Pain Pract. 2019;19(6):664–675. PMID: 30957944; PMCID: PMC6850128. doi:10.1111/papr.12786
6. Brown A, Parmar J, Ganji-Angirekula S, et al. Practice patterns of physicians who perform caudal epidural steroid injections. Orthop Rev. 2024;16:123283. PMID: 39286465; PMCID: PMC11405026. doi:10.52965/001c.123283
7. Simopoulos T, Peeters-Asdourian C. Pneumocephalus after cervical epidural steroid injection. Anesth Analg. 2001;92(6):1576–1577. PMID: 11375849. doi:10.1097/00000539-200106000-00045
8. Sorber J, Levy D, Schwartz A. Pneumocephalus and seizures following epidural steroid injection. Am J Emerg Med. 2017;35(12):
9. Li T, Gonzalez C, Provost J, Hasoon J, Nguyen A. Understanding the landscape of lumbar epidural steroid injections: a review of interlaminar, transforaminal, and caudal approaches. Orthop Rev. 2025;17:138210. PMID: 40416592; PMCID: PMC12103295. doi:10.52965/001c.138210
10. Tran DQ, González AP, Bernucci F, Finlayson RJ. Confirmation of loss-of-resistance for epidural analgesia. Reg Anesth Pain Med. 2015;40(2):166–173. PMID: 25642911. doi:10.1097/AAP.0000000000000217
11. U.S. Food and Drug Administration. FDA drug safety communication: fda requires label changes to warn of rare but serious neurologic problems after epidural corticosteroid injections for pain [Internet]. Silver Spring (MD): U.S. Food and Drug Administration; 2014 [cited 2025 Oct 19]. Available from: https://www.fda.gov/drugs/drug-safety-and-availability/fda-drug-safety-communication-fda-requires-label-changes-warn-rare-serious-neurologic-problems-after.
12. Rathmell JP, Benzon HT, Dreyfuss P, et al. Safeguards to prevent neurologic complications after epidural steroid injections: consensus opinions from a multidisciplinary working group and national organizations. Anesthesiology. 2015;122(5):974–984. PMID: 25668411. doi:10.1097/ALN.0000000000000614
13. Bingham N, Dhall R, Montuori M, Padjen K, Gharibo C, Doan L. Variations in epidural steroid injection practice patterns by pain medicine physicians in the United States. Pain Physician. 2022;25(6):E857–E862. PMID: 36122269.
14. Doan L, Patel H, Aronova Y, Gharibo C. Variations in interlaminar epidural steroid injection practice patterns by interventional pain management physicians in the United States. Pain Physician. 2018;21(5):E493–E499. [PMID: 30282397]. doi:10.36076/ppj.2018.5.E493
15. Knezevic NN, Paredes S, Cantillo S, Hamid A, Candido KD. Parasagittal approach of epidural steroid injection as a treatment for chronic low back pain: a systematic review and meta-analysis. Front Pain Res. 2021;2:676730. PMID: 35295439; PMCID: PMC8915709. doi:10.3389/fpain.2021.676730
16. Ghai B, Vadaje KS, Wig J, Dhillon MS. Lateral parasagittal versus midline interlaminar lumbar epidural steroid injection for management of low back pain with lumbosacral radicular pain: a double-blind, randomized study. Anesth Analg. 2013;117(1):219–227. PMID: 23632053. doi:10.1213/ANE.0b013e3182910a15
17. Hasoon J, Viswanath O, Kaye AD, Pasqualucci A, Varrassi G. Patient outcomes following parasagittal interlaminar epidural steroid injections for bilateral lumbar radicular symptoms: correlation of contrast spread with symptom relief. Cureus. 2025;17(2):e78817. PMID: 40078239; PMCID: PMC11901417. doi:10.7759/cureus.78817
18. Hasoon J, Robinson CL, Viswanath O, Urits I, Kaye AD. Evaluating bilateral symptom relief following parasagittal interlaminar epidural steroid injections. Orthop Rev. 2025;17:143088. PMID: 40823275; PMCID: PMC12356689. doi:10.52965/001c.143088
19. Kaur S, Gupta R, Singh S, Kumar R, Singh K. Impact of different approaches of epidural steroid injection on outcome of patients treated for low backache. Anesth Essays Res. 2017;11(3):697–701. PMID: 28928574; PMCID: PMC5594793. doi:10.4103/0259-1162.204205
20. Whitlock EL, Bridwell KH, Gilula LA. Influence of needle tip position on injectate spread in 406 interlaminar lumbar epidural steroid injections. Radiology. 2007;243(3):804–811. PMID: 17463137. doi:10.1148/radiol.2433060983
21. Mojarrad M, Wieschhoff GG, Mandell JC. Contrast flow in CT-guided lumbar interlaminar epidural steroid injections: does needle position effect the laterality of contrast flow? Skeletal Radiol. 2024;53(7):1313–1318. PMID: 38238455. doi:10.1007/s00256-024-04588-5
22. Abdullah S, Ku JB, Sutton O, et al. Practice patterns and perspectives on epidural steroid injections by interventional pain physicians. Pain Ther. 2025;14(6):1735–1743. Epub ahead of print. PMID: 40971109. doi:10.1007/s40122-025-00772-0
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Surveying Canadian Pain Physicians’ Attitudes and Beliefs Regarding Medical Cannabis for Chronic Noncancer Pain: A Qualitative Study
Ng JY, Quach H, Phillips MR, Busse JW
Journal of Pain Research 2022, 15:3899-3910
Published Date: 14 December 2022
Radiofrequency Ablation for Chronic Lumbar Zygapophyseal Joint Pain Using a V-Shaped Active Tip Needle: An Observational Retrospective Study
Lo Bianco G, Misseri G, Stogicza AR, Cesare G, Li S, Day M, Kennedy DJ, Schatman ME
Journal of Pain Research 2023, 16:1243-1255
Published Date: 11 April 2023
Feasibility and Acceptability of the Pain Profile, a Clinical Questionnaire Aimed at Improving Pain Care
Zarska A, Slat S, Kehne A, Macleod C, Rye H, Dehmlow C, Hilliard P, Jaffe K, Lagisetty P
Journal of Pain Research 2023, 16:1559-1571
Published Date: 11 May 2023
Interventional Pain Procedures: A Narrative Review Focusing on Safety and Complications. Part 1 Injections for Spinal Pain
Lo Bianco G, Tinnirello A, Papa A, Torrano V, Russo G, Stogicza A, Mercadante S, Cortegiani A, Mazzoleni S, Schatman ME
Journal of Pain Research 2023, 16:1637-1646
Published Date: 18 May 2023
A Randomized, Double-Blind, Placebo-Controlled Trial to Evaluate the Therapeutic Effect of Magnesium-L-Threonate Supplementation for Persistent Pain After Breast Cancer Surgery
Ni Y, Deng F, Yu S, Zhang J, Zhang X, Huang D, Zhou H
Breast Cancer: Targets and Therapy 2023, 15:495-504
Published Date: 25 July 2023