Back to Journals » Journal of Pain Research » Volume 16
Interventional Pain Procedures: A Narrative Review Focusing on Safety and Complications. Part 1 Injections for Spinal Pain
Authors Lo Bianco G ![]() , Tinnirello A
, Tinnirello A ![]() , Papa A
, Papa A ![]() , Torrano V
, Torrano V ![]() , Russo G, Stogicza A, Mercadante S, Cortegiani A, Mazzoleni S, Schatman ME
, Russo G, Stogicza A, Mercadante S, Cortegiani A, Mazzoleni S, Schatman ME ![]()
Received 27 December 2022
Accepted for publication 15 May 2023
Published 18 May 2023 Volume 2023:16 Pages 1637—1646
DOI https://doi.org/10.2147/JPR.S402798
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Dawood Sayed
Giuliano Lo Bianco,1,2 Andrea Tinnirello,3 Alfonso Papa,4 Vito Torrano,5 Gianluca Russo,6 Agnes Stogicza,7 Sebastiano Mercadante,8 Andrea Cortegiani,9 Silvia Mazzoleni,3 Michael E Schatman10,11
1Department of Biomedical and Biotechnological Sciences, University of Catania, Catania, Italy; 2Department of Anesthesiology and Pain, Fondazione Istituto G. Giglio, Cefalù, Italy; 3Department of Anesthesiology and Pain Medicine, ASST Franciacorta, Ospedale di Iseo, Iseo, Italy; 4Department of Pain Management– AO “Ospedali dei Colli” – Monaldi Hospital, Naples, Italy; 5Department of Anesthesia, Critical Care and Pain Medicine, Asst Grande Ospedale Metropolitano Niguarda, Milan, Italy; 6Department of Anesthesia, Postoperative Intensive Care and Pain Therapy, Lodi Hospital, Lodi, Italy; 7Department of Anesthesiology Saint Magdolna Hospital, Budapest, Hungary; 8Department of Pain Relief and Supportive Care, Private Hospital La Maddalena, Palermo, Sicilia, Italy; 9Department of Anesthesiology and Intensive Care, Università degli Studi di Palermo, Palermo, Italy; 10Department of Anesthesiology, Perioperative Care, and Pain Medicine, NYU School of Medicine, New York, NY, USA; 11Department of Population Health – Division of Medical Ethics, NYU School of Medicine, New York, NY, USA
Correspondence: Andrea Tinnirello, Department of Anesthesiology and Pain Medicine, ASST Franciacorta, Ospedale di Iseo, Via Giardini Garibaldi 4, Iseo, 25049, Italy, Tel +393392599568, Email [email protected]
Abstract: In recent years, there has been a considerable increase in the number of image-guided interventional procedures performed for the management of acute and chronic pain. Concomitantly, there has also been an increase in the complication rate related to these procedures. The aim of this narrative review is to summarize the primary complications associated with commonly performed image-guided (fluoroscopic- or ultrasound-guided) interventional procedures. We conclude that although complications from interventional pain procedures can be mitigated to a certain degree, they cannot be eliminated altogether. In order to avoid adverse events, patient safety should be given considerable attention and physicians should be constantly aware of the possibility of developing complications.
Keywords: chronic pain, pain management, analgesics, opioid, epidural injection, facet joints
Introduction
Recent years have witnessed a significant increase in image-guided interventional procedures performed to manage acute and chronic pain.1–3 However, an increase in the number of complications related to these procedures has also been observed, varying from minor to severe and debilitating.4–6 The exact incidence of severe adverse events is considered low (under 1%) but it is probably underestimated since they are usually reported as case reports, deaths after epidural injections have been reported as well but the exact mortality rate is unknown (and probably less than 1 every million procedures).7 It is estimated that over 9 million epidural injections are performed each year in the United States.7 Facet joint interventions increased 1.9% annually and 18.8% in total from 2009 to 2018 per 100,000 Fee-for Service (FFS) Medicare patients compared with an annual increase of 17% and an overall increase of 309.9% from 2000 to 2009.8 In order to avoid adverse events, physicians should be mindful of patient safety. Physician expertise, in addition to patient selection and preparation, are of fundamental importance to ensure the safety of interventional procedures. Moreover, regular education, training, and international certification for healthcare providers, as well as collaboration with interdisciplinary teams, can also help to minimize the risk of adverse events.6 Similar to all interventional pain therapy procedures, the number of infiltrative techniques has increased significantly in recent years.4,5 Furthermore, the development of techniques using ultrasound-guidance has allowed their execution (at least to a degree) even in less controlled outpatient settings.9
On the other hand, patients undergoing interventional procedures are often frail, with multiple comorbidities and medications usage. For these reasons, it is essential to emphasize the limits and possible risks linked to these procedures, thereby enabling the clinician to plan a clinical strategy that can manage any complications which may arise. In pain medicine, even apparently simple procedures such as facet joint injections or epidural steroid injections present risks linked to the type of drugs used and the setting in which they are performed. This narrative review describes complications that may result from commonly performed image-guided interventional pain procedures such as epidural steroid injections and facet joint interventions.
Methods
Two authors per topic carried out the bibliographic research for this review on Pubmed, Scopus, Embase and the Cochrane Library for published articles available between 1/1/1980-31/12/2020. A systematic search using the keywords: Epidural injections, facet joint interventions, complications, ultrasound pain interventions. Only papers in English have been evaluated. Only papers with reported adverse events (including single case reports) were included.
Results
Epidural Steroid Injections
Degenerative spine conditions are often treated using epidural steroid injections (ESIs), which are generally effective in the short term in relieving pain caused by disc herniations and spinal stenosis.10,11 The incidence of immediate or delayed complications for cervical and lumbar ESIs was determined to range from 1.6% to 20.0%.12,13 A previous study analyzed 26,061 interventional spine procedures in three different pain services to assess the rate of adverse events.14 Approximately 14,000 of these were epidural injections, including transforaminal and interlaminar approaches performed in the cervicothoracic and lumbar spine. The overall adverse event rate was below 2% (493/26,061).14 The most common adverse event (more common in transforaminal than interlaminar ESI approaches and found in 1.1% (289/26,061) of procedures in this study) was vasovagal reaction.14 Vasovagal reactions, defined as the reflex of increased vagal/decreased sympathetic tone (bradycardia, hypotension, diaphoresis, nausea and visual impairment) occur far more frequently in cervical ESIs than in lumbar ESIs.15 Other major, immediate adverse events include allergic reactions, spinal cord lesions and dural punctures.14 A number of less consequential adverse events are described in various other studies noted in Table 1.12–17
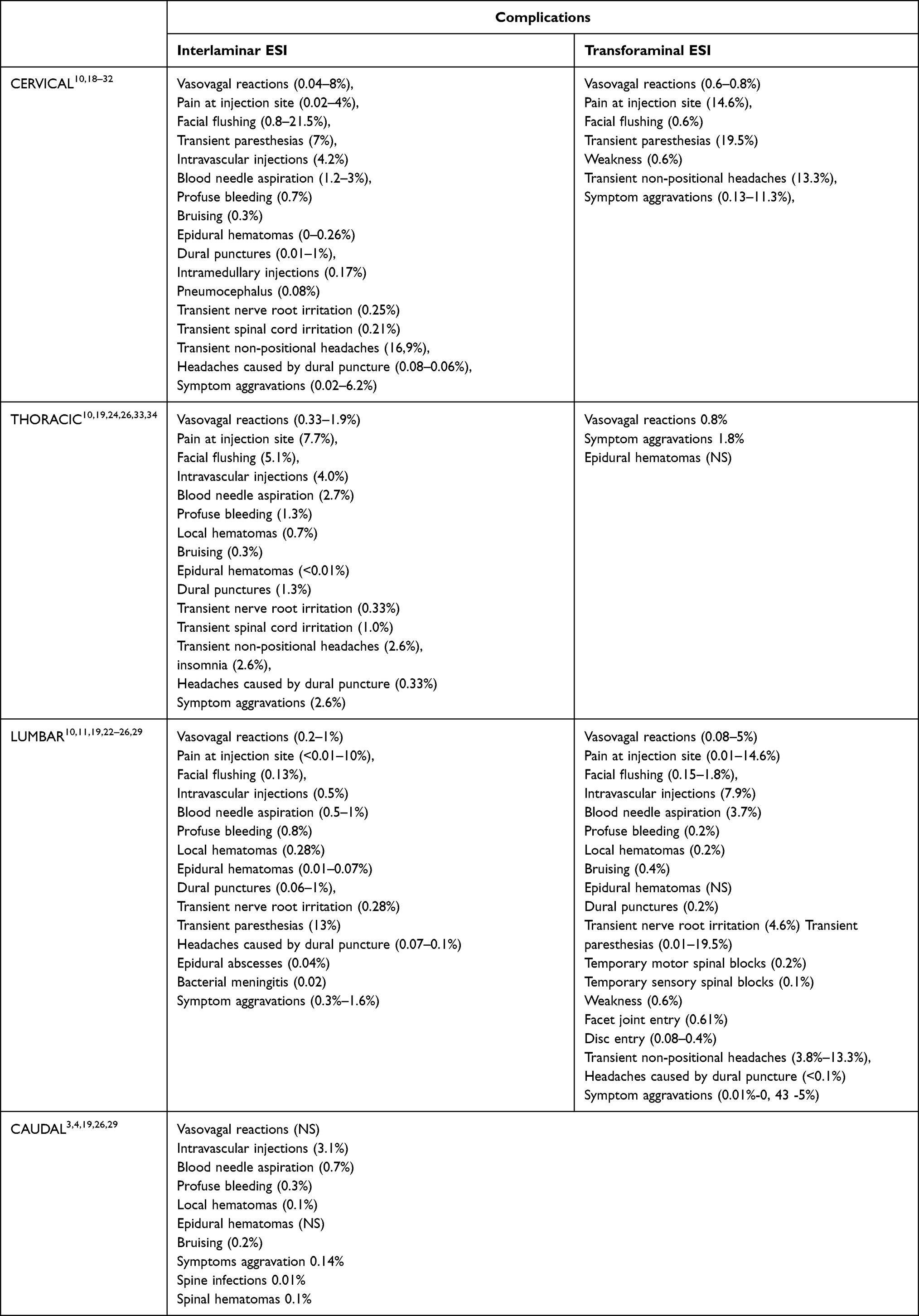 |
Table 1 Complications of ESIs (Values Expressed as Range); NS: Non Stated |
A reasonably frequent complication following epidural injections, with an incidence of 0.06% to 6%, are unintentional dural punctures and cerebrospinal fluid (CSF) leakage.16 Several authors suggest that entering the epidural space above the C7–T1 interspace should be avoided, as it may be easier to penetrate the dura at higher levels.17 Furthermore, the ligamentum flavum is adherent to the dura above C5 in 34% of the population. Since the epidural space becomes narrower above C7, accessing the epidural space at higher levels increases the risk of injuring the spinal cord. Gaps in the ligamentum flavum, demonstrated to be present in up to 74% of patients at C5-C6 level, increase the risk of accidental injection into the spinal cord.35 Dural tears with CSF leakage and subsequent reductions in CSF volume may result in post-dural puncture headaches (PDPHs) within 48 hours of the procedure.16 Needle size and bevel type, among other factors, possibly affect the incidence of PDPH. Other symptoms may include nausea, vomiting, dizziness, neck stiffness, blurred vision, photophobia, diplopia, tinnitus and ear obstruction, and conservative treatments include hydration, bed rest, analgesics and caffeine intake.16,17 In cases in which the aforementioned treatments do not provide adequate symptom relief, a greater occipital nerve block or an epidural blood patch (EBP) is suggested.18,36 Even if its mechanism of action is still debated, EBPs create a clot which seals the leak, thereby increasing intraspinal pressure and ensuring a rapid coagulation response, even if the tear is not located in proximity to the EBP site.16 On rare occasions, adverse events of a more serious nature can occur as a result of dural puncture. Intracranial hypotension following dural punctures and epidural granulomas due to cervical epidural steroid injections have been reported.37 The risk of subdural injection in the cervical region is greater than that in the lumbar spine, as the subdural space is larger in the cervical region. Contrast patterns with fluoroscopic-guided injection must be analyzed carefully to avoid accidental injection into the subdural or subarachnoid space.16 Dural punctures associated with transforaminal lumbar ESI are also documented, despite seemingly technically sound injections.38 Possible complications following dural puncture, and ensuing injections into the subdural and subarachnoid spaces, include persistent paresthesia, temporary respiratory depression, ascending weakness/sensory loss, apnea, unconsciousness, cauda equina and conus medullaris syndromes, arachnoiditis and meningitis. Further highly infrequent yet potentially serious complications of cervical interlaminar ESIs are hematomas of the epidural or subdural space, which potentially result in transient or permanent neurological deficits.39,40
The greatest incidence of spontaneous spinal epidural hematoma following epidural injections occurs as a complication of injections into the cervicothoracic region.17 A number of factors contribute to an increased risk of occurrence, including female gender, advanced age, vertebral anatomy abnormalities, a history of spine surgery, difficult epidural placement, needle size, multiple attempts and use of anticoagulants (or presence of coagulopathy) during the procedure.19 In a large study of 4617 lumbar interlaminar epidural injections and 1182 cervical epidurals, 7 hemorrhagic complications were reported, including epidural hematomas (6 patients) and intramedullary spinal cord hemorrhage (1 patient) at the injection site.41 Other studies have demonstrated that patients undergoing anticoagulant therapy developed epidural hematomas following cervical steroid injections.18,35 Some patients suffered permanent neurologic deficits, despite surgical decompression, while others recovered without any neurological sequelae. In one case, a patient was reported to have developed an intracranial subdural hemorrhage following an epidural injection.39 The patient then developed meningitis and died from cardiopulmonary arrest.39 The possibility of hematoma cannot be excluded even in the absence of risk factors. Previous cervical manipulation and local vessel friability following repeated steroid injections may affect these complications. Permanent neurological lesions of the lumbar spine caused by epidural hematoma after interlaminar ESI have also been reported. In a study examining potential complications in 52,935 procedures provided at a single institution, epidural hematomas linked to interlaminar lumbar and caudal epidural steroid injections developed in 2 cases.19 Epidural hematomas following lumbar steroid injection were also reported in patients with undiagnosed bleeding disorders or those on anticoagulation medications.19,40–42 Significantly greater risk is associated with cervical injections than with lumbar injections. Urgent surgical consultation is fundamental when hyposthenia in the upper limbs is detected during or following steroid injections, particularly in the cervical spine.42 A rare complication that has been reported following cervical interlaminar ESIs are cervical epidural abscesses.43,44 This should be taken into consideration in cases in which increased pain, spasm, motor, sensory, bowel, and bladder dysfunction in the patient are accompanied by fever. Epidural abscesses and bacterial meningitis can occur as a complication of lumbar interlaminar injections.42–45 The American Society of Regional Anesthesia and Pain Medicine published guidelines for administering neuraxial blocks in patients taking anticoagulation medications.46 However, it is important to note that the risk of hemorrhagic complications may still be present, even when closely following the guidelines. Furthermore, the suspension of anticoagulant therapies due to invasive procedures can lead to thromboembolic complications. A complication rate of 0.4% (including a fatal stroke and a fatal myocardial infarction) in those who discontinued anticoagulants/antiaggregants according to ASRA guidelines has been reported.20 Paresthesia following cervical interlaminar ESIs may be transient, prolonged, or permanent, and injury to the nerve root may ensue from needle insertion. A case of permanent paresthesia following sudden movement in an unsettled patient was also reported.21 Thus, for some patients, sedation may be considered necessary to avoid complications from excessive patient movement. Inadvertent intramedullary puncture may result during cervical ESIs and, on more rare occasions, lumbar ESIs.22 A report on 2 cases of intrinsic spinal cord damage following fluoroscopically guided cervical interlaminar ESIs in sedated patients has been published, and another study reported a case of quadriplegia in a patient who was sedated, due to an intramedullary injection following a cervical interlaminar ESI.23 Therefore, excessive sedation is discouraged to ensure that patients are able to indicate experiences of inadvertent spinal cord irritation. Particulate steroid use during cervical transforaminal injections should also be given careful consideration as it represents the primary cause of neurological injury associated with the procedure.22 Thirteen deaths and 31 brain and spinal cord infarctions with persistent neurological injuries resulting from cervical transforaminal ESIs have been reported, with most of the patients having been treated with particulate steroids.24 Neurological injuries subsequent to transforaminal ESIs in the lumbar spine were also reported in 18 cases.45 The transforaminal approach is associated with greater risk of neurological injury compared to the interlaminar approach.25,45 However, 2 cases following cervical interlaminar epidural injections and one case subsequent to a thoracic interlaminar epidural injection have been reported.22 It is worth noting that these 3 cases are not necessarily indicative of a causal relationship consequent to steroid injections.22 A frequent complication of ESIs is intravascular injection.45 Although real-time fluoroscopy with the injection of a contrast agent is most commonly employed as a precaution against intravascular penetration, digital subtraction angiography may prove to be a more useful alternative to real-time fluoroscopy.26
Facet Joint Procedures
Facet joint procedures are common in the management of chronic spinal pain.33
They are perceived as safe and effective approaches to treating patients suffering from chronic facet joint pain in the cervical, thoracic, and lumbosacral spine.47 Facet joints are furnished from above and below with a rich supply of nerves by the medial branches of the dorsal rami. The joints can be blocked by the medial branches of the dorsal rami or by intraarticular injections.5,48 The general rate of adverse events linked to facet joint injections was found to be 0.84% (101/11,980) per case and 1.63% (99/6066) per patient.4 Potential complications reported include intra-arterial or intravenous injections, dural punctures, spinal anesthesia, spinal cord trauma, neural trauma, hematoma formation, pneumothorax, facet capsule ruptures, infections, chemical meningitis, radiation exposure, and steroid side effects.4,48 There are also known side effects of denervation from radiofrequency, which include increased pain due to neuritis or neurogenic inflammation, painful cutaneous dysesthesias, cutaneous hyperesthesia, pneumothorax, ataxia, anesthesia dolorosa and deafferentation pain.48 Another possible complication is accidental spinal nerve damage caused during medial branch radiofrequency with a consequential motor deficit.48 In a study of 7500 facet joint procedures, Manchikanti et al reported multiple side effects and complications which included overall intravascular penetration in 11.4% of cases, with the highest incidence in the cervical region and local bleeding in 76.3% of cases, with the highest rate in the thoracic region, and oozing in 19.6%.49 Local hematomas were reported in only 1.2% of patients, and profuse bleeding, bruising, soreness, nerve root irritation and all other adverse effects, such as vasovagal reactions, were observed in 1% or fewer instances.49 The complications most frequently observed within 2 days of the procedure were injection site discomfort, (6.0%) pain exacerbation, (4.3%) sleeplessness, (2.2%) and transient headaches (1.6%).49 Specific details are presented in Table 2. Infection is a complication which is highly infrequent although potentially serious. Infectious complications which have been reported include meningitis, discitis, spondylitis and systemic aspergillosis following spondylitis, epidural abscess and paraspinal abscesses, which can lead to endocarditis.16,48,50
 |
Table 2 Complications of Procedures Related to Facet Joints (Values Expressed as Ranges) |
Complications in Ultrasound (US) Guided Procedures
Ultrasound guidance has become progressively more commonly used by interventionists when administering various injections.51,52 Due to its ability to allow for visualization of soft tissue, vessels and nerves, this guidance method is becoming preferred over fluoroscopy for several interventions involving areas in which nerves and vessels are abundant. It has been suggested that the most frequent complications occurring as a result of regional anesthesia, such as blood vessel punctures or inadvertent intraneural or intravascular injections, may be reduced although not completely eliminated with the use of expert ultrasound guidance.51,53 The ability to visualize bony structures for accurate and safe facet injections and interlaminar epidural steroid injections is fundamental. Although facet joint injections can be performed using ultrasound guidance, interventions on obese patients, in whom visualization of the deep anatomical structures is poor, can represent a challenge. In the case of transforaminal ESIs, there is still limited evidence to suggest that this guidance technology is as effective as or leads to fewer complications compared to fluoroscopy.53 A report suggests that the main limitations posed by ultrasound technology are related to the experience of the operator.54 A study of nearly 60 ultrasound-guided blocks performed by trainees indicated that the most frequent errors regarded not recognizing local anesthetic maldistribution or needle tip prior to injection and misjudgment in the needle insertion site and angle that led to poor visualization of the needle tip. However, ultrasound technology depends not only on the operator but also on anatomic location and the patient.55
Obesity, degenerative changes and a history of surgical intervention may negatively affect the ultrasound image quality. A case of pneumothorax following interscalene block was reported, notwithstanding the dynamic visualization of cervical structures under ultrasound.56 The authors of this case report argued that the complication was linked to the patient’s characteristics, ie, the accidental pleural puncture likely to have been facilitated by the patient’s uncommonly high pleural dome due to hyperinflated lungs secondary to smoking.56 Other complications, such as a neurologic complications following US-guided supraclavicular brachial plexus blocks (BPBs) and a pulmonary complication provoked by phrenic nerve block following interscalene block were also reported.57,58 Furthermore, the quality of the images may not be adequate in certain areas. These images are often of poor quality in the axial or spine structures, where bones create an acoustic shadow artifact. Certain neuraxial procedures for chronic pain, for example, often cannot be guided by ultrasound, as the technology is unable to detect epidural intravascular injection and the spread of the injected solution.59 Authors with extensive clinical experience have reported cases of inadvertent intravascular injections of local anesthetics and intravascular injections in ultrasound-guided axillary plexus blocks.59,60 This is a demonstration of the limits posed by the technology rather than a demonstration of an inexpert operators, thus complicating reliable detection of an intravascular injection during ultrasound-guided nerve blocks. Tracking the path of the needle, the disposition of the local anesthetics and visualization of the anatomy may also be affected by a series of additional technical factors.54
Discussion
The evaluation of existing evidence suggest that the incidence of adverse events after interventional pain procedures is low but not negligible, however, the exact rate of complication is unknown since they are often unreported and, for serious events, they are reported as case reports or claims made to insurances.
ESIs and Facet Joint interventions are widely applied procedures for treating chronic back pain. Even if the incidence of adverse events is not precisely defined, ranging from 0.04% to 13%, these procedures are generally safe, most complications are transient and modest, with an incidence of severe accidents of less than 1%. Very severe events after ESIs (permanent nerve or spinal cord damage with persistent neurological deficits) are reported only as case reports, even if their incidence is probably underestimated (since many adverse events are not reported) we can conclude that their incidence is extremely low, presumably less than 0.1%. The key to reduce complications to the lowest rate is to apply all safety features available and perform a technically flawless intervention. Regarding bleeding, ESIs at all levels and cervical facet interventions are considered intermediate risk procedures while lumbar and thoracic facet joint interventions are amongst procedures deemed to be of low risk, and according to ASRA guidelines, discontinuation of antithrombotics is recommended only for intermediate risk procedures.46 Irrespective, the risks and benefits need to be considered in each case individually. Minimal sedation is recommended to ensure patient cooperation and immediately detect intra-procedural neurological deficits. Several guidelines emphasize the necessity of using fluoroscopic guidance for all ESIs regardless of their approach (interlaminar or transforaminal), while for caudal injections, ultrasound guidance is considered sufficient.61–63 Contrast medium injections should be considered mandatory to exclude intravascular injections and real time fluoroscopy or digital subtraction angiography is recommended for transforaminal injections, particularly at cervical levels. It is worth mentioning that some authors advocate for a complete avoidance of transforaminal injection at the cervical level, given the possibility of devastating neurological complications.64,65 The physical properties of injected medications play a major role in the development of complications. Particulate steroid epidural injections contain particles of the steroid medication, while non-particulate steroid epidural injections are free of particles. Particulate steroids may provide longer-lasting pain relief, but they also are associated with severe neurological injuries, particularly at cervical levels, and, therefore, non-particulate steroids are recommended for all cervical procedures and for transforaminal ESIs at lumbar levels. Moreover, epidural steroids are associated with the potential of fungal contamination, with the possibility of creating a fungal meningitis.26 700 cases of fungal meningitis after ESIs with contaminated steroids have been reported by the FDA.26 Even if non- particulate steroids are considered safe, it should be emphasized that these compounds can form large crystals when injected with local anesthetics, ropivacaine or levobupivacaine and betamethasone sodium phosphate. Accordingly, their use may require extra caution during an epidural steroid injection, and lidocaine, bupivacaine and dexamethasone are considered safer options.66 Recommendations from guidelines are summarized in Table 3. The use of ultrasound is more and more common and could help reducing the procedure-associated complications, particularly when treating highly vascularized tissues such as the cervical region.67 However, technical, and anatomical issues (penetration into deep tissues, obesity, bony shadows), limits this technology. In summary, the use of ultrasound guidance may lead to a reduction in complications induced by interventional pain procedures yet are not likely to eliminate them entirely.
 |
Table 3 Summary of Guideline Recommendations |
Conclusion
Pain is a multidimensional problem that that is best explained and ideally treated using a multimodal paradigm, of which interventional approaches are an important aspect. This narrative review has sought to provide a comprehensive evaluation of evidence regarding safety and complications of interventional pain procedures for managing spinal pain. We conclude that interventional spine procedures are generally safely performed when utilizing evidence-based practice guidelines. However, it is essential to emphasize the limits and possible risks linked to these procedures, thereby enabling the clinician to plan a clinical strategy that can manage any complications that may arise. Irrespective of claims that interventional procedures are perfectly safe, we posit that no treatment of pain is perfectly safe. However, we conclude that the low rate of adverse events and iatrogenic complications that have been reported in the literature suggest that interventional procedures should be considered important tools in pain physicians’ armamentaria.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
Dr Giuliano Lo Bianco reports personal fees from Stryker Italia, outside the submitted work. Dr Andres Tinnirello reports personal fees from Avanos Medical Belgium, outside the submitted work. Dr Michael E Schatman is a reseach consultant for Modoscript and part of the Scientific Steering Committee for Collegium, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Papa A, Di Dato MT, Lo Bianco G, et al. Intraarticular STP radiofrequency for painful osteoarthritis in the knee: a retrospective single center analysis. J Pain Res. 2021;14:2441–2447. PMID: 34413678; PMCID: PMC8370597. doi:10.2147/JPR.S317569
2. Leoni MLG, Schatman ME, Demartini L, Lo Bianco G, Terranova G. Genicular Nerve Pulsed Dose Radiofrequency (PDRF) compared to intra-articular and genicular nerve PDRF in knee osteoarthritis pain: a propensity score-matched analysis. J Pain Res. 2020;13:1315–1321. PMID: 32581573; PMCID: PMC7280065. doi:10.2147/JPR.S240138
3. Vigneri S, Sindaco G, La Grua M, et al. Electrocatheter-mediated high-voltage pulsed radiofrequency of the dorsal root ganglion in the treatment of chronic lumbosacral neuropathic pain: a randomized controlled study. Clin J Pain. 2020;36(1):25–33. PMID: 31577546; PMCID: PMC690335. doi:10.1097/AJP.0000000000000766
4. Hynes JP, Fhlatharta MN, Ryan JW, MacMahon PJ, Eustace SJ, Kavanagh EC. Complications in image-guided musculoskeletal injections. Skeletal Radiol. 2021;50(2):343–349. doi:10.1007/s00256-020-03565-y
5. Manchikanti L, Hirsch JA, Pampati V, Boswell MV. Utilization of facet joint and sacroiliac joint interventions in medicare population from 2000 to 2014: explosive growth continues! Curr Pain Headache Rep. 2016;20(10):58. doi:10.1007/s11916-016-0588-2
6. Lo Bianco G, Tinnirello A, Papa A, et al. PART 2 interventional procedures for back pain. J Pain Res. 2023;16:761–772. PMID: 36925622; PMCID: PMC10010974. doi:10.2147/JPR.S396215
7. Cohen SP, Greuber E, Vought K, Lissin D. Safety of epidural steroid injections for lumbosacral radicular pain: unmet medical need. Clin J Pain. 2021;37(9):707–717. doi:10.1097/AJP.0000000000000963
8. Manchikanti L, Sanapati MR, Pampati V, et al. Update of utilization patterns of facet joint interventions in managing spinal pain from 2000 to 2018 in the US fee-for-service medicare population. Pain Physician. 2020;23(2):E133–E149.
9. Di Pietro S, Mascia B, Lo Bianco G, Perlini S, Iotti GA. Anterior cutaneous nerve block for analgesia in anterior chest trauma: is the parasternal approach necessary? Clin Exp Emerg Med. 2020; (1):67–70. PMID: 32252136; PMCID: PMC7141978. doi:10.15441/ceem.18.089
10. Kozlov N, Benzon HT, Malik K. Epidural steroid injections: update on efficacy, safety, and newer medications for injection. Minerva Anestesiol. 2015;81(8):901–909.
11. Verheijen EJA, Bonke CA, Amorij EMJ, Vleggeert-Lankamp CLA. Epidural steroid compared to placebo injection in sciatica: a systematic review and meta-analysis. Eur Spine J. 2021;30(11):3255–3264. doi:10.1007/s00586-021-06854-9
12. Manchikanti L, Singh V, Cash KA, Pampati V, Falco FJE. A randomized, double-blind, active-control trial of the effectiveness of lumbar interlaminar epidural injections in disc herniation. Pain Physician. 2014;17(1):E61–E74.
13. Manchikanti L, Cash KA, McManus CD, Damron KS, Pampati V, Falco FJE. A randomized, double-blind controlled trial of lumbar interlaminar epidural injections in central spinal stenosis: 2-year follow-up. Pain Physician. 2015;18(1):79–92.
14. Carr CM, Plastaras CT, Pingree MJ, et al. Immediate adverse events in interventional pain procedures: a multi-institutional study. Pain Med. 2016;17(12):2155–2161. doi:10.1093/pm/pnw051
15. El-Yahchouchi CA, Plastaras CT, Maus TP, et al. Adverse event rates associated with transforaminal and interlaminar epidural steroid injections: a multi-institutional study: adverse events epidural steroid injections. Pain Med. 2015. doi:10.1111/pme.12896
16. Plastaras C, McCormick ZL, Garvan C, et al. Adverse events associated with fluoroscopically guided lumbosacral transforaminal epidural steroid injections. Spine J. 2015;15(10):2157–2165. doi:10.1016/j.spinee.2015.05.034
17. Abbasi A, Malhotra G, Malanga G, Elovic EP, Kahn S. Complications of interlaminar cervical epidural steroid injections: a review of the literature. Spine. 2007;32(19):2144–2151. doi:10.1097/BRS.0b013e318145a360
18. Desai MJ, Dave AP, Martin MB. Delayed radicular pain following two large volume epidural blood patches for post-lumbar puncture headache: a case report. Pain Physician. 2010;13(3):257–262.
19. Lee JW, Lee E, Lee GY, Kang Y, Ahn JM, Kang HS. Epidural steroid injection-related events requiring hospitalisation or emergency room visits among 52,935 procedures performed at a single centre. Eur Radiol. 2018;28(1):418–427. doi:10.1007/s00330-017-4977-7
20. Endres S, Shufelt A, Bogduk N. The risks of continuing or discontinuing anticoagulants for patients undergoing common interventional pain procedures. Pain Med. 2017;18(3):403–409. doi:10.1093/pm/pnw108
21. Landers MH. Spinal cord injury during attempted cervical interlaminar epidural injection of steroids. Pain Med. 2018;19(4):652–657. doi:10.1093/pm/pnx081
22. Epstein N. Neurological complications of lumbar and cervical dural punctures with a focus on epidural injections. Surg Neurol Int. 2017;8(1):60. doi:10.4103/sni.sni_38_17
23. Hodges SD, Castleberg RL, Miller T, Ward R, Thornburg C. Cervical epidural steroid injection with intrinsic spinal cord damage: two case reports. Spine. 1998;23(19):2137–2140. doi:10.1097/00007632-199810010-00020
24. Epstein N. Major risks and complications of cervical epidural steroid injections: an updated review. Surg Neurol Int. 2018;9(1):86. doi:10.4103/sni.sni_85_18
25. Jasper JF. Is digital subtraction fluoroscopy a useful tool for the interventional pain physician? Pain Physician. 2002;5(1):36–39.
26. Manchikanti L, Benyamin RM. Key safety considerations when administering epidural steroid injections. Pain Manag. 2015;5(4):261–272. doi:10.2217/pmt.15.17
27. Derby R, Lee SH, Kim BJ, Chen Y, Seo KS. Complications following cervical epidural steroid injections by expert interventionalists in 2003. Pain Physician. 2004;7(4):445–449.
28. Goel A, Pollan JJ. Contrast flow characteristics in the cervical epidural space: an analysis of cervical epidurograms. Spine. 2006;31(14):1576–1579. doi:10.1097/01.brs.0000222020.45794.ac
29. Trentman TL, Rosenfeld DM, Seamans DP, Hentz JG, Stanek JP. Vasovagal reactions and other complications of cervical vs. lumbar translaminar epidural steroid injections. Pain Pract. 2009;9(1):59–64. doi:10.1111/j.1533-2500.2008.00242.x
30. McGrath JM, Schaefer MP, Malkamaki DM. Incidence and characteristics of complications from epidural steroid injections. Pain Med. 2011;12(5):726–731. doi:10.1111/j.1526-4637.2011.01077.x
31. Manchikanti L, Malla Y, Wargo BW, Cash KA, Pampati V, Fellows B. A prospective evaluation of complications of 10,000 fluoroscopically directed epidural injections. Pain Physician. 2012;15(2):131–140.
32. El Abd O, Amadera J, Pimentel DC, Gomba L. Immediate and acute adverse effects following transforaminal epidural steroid injections with dexamethasone. Pain Physician. 2015;18(3):277–286.
33. Lo Bianco G, Misseri G, Stogicza AR, et al. Radiofrequency Ablation for Chronic Lumbar Zygapophyseal Joint Pain Using a V-Shaped Active Tip Needle: an Observational Retrospective Study. J Pain Res. 2023;16:1243–1255. PMID: 37069943; PMCID: PMC10105587. doi:10.2147/JPR.S406714
34. Botwin KP, Baskin M, Rao S. Adverse effects of fluoroscopically guided interlaminar thoracic epidural steroid injections. Am J Phys Med Rehabil. 2006;85(1):14–23. doi:10.1097/01.phm.0000184475.44853.82
35. Hogan QH. Epidural anatomy examined by cryomicrotome section. Influence of age, vertebral level, and disease. Reg Anesth. 1996;21(5):395–406.
36. Nair AS, Kodisharapu PK, Anne P, Saifuddin MS, Asiel C, Rayani BK. Efficacy of bilateral greater occipital nerve block in postdural puncture headache: a narrative review. Korean J Pain. 2018;31(2):80–86. doi:10.3344/kjp.2018.31.2.80
37. Dietrich CL, Smith CE. Epidural granuloma and intracranial hypotension resulting from cervical epidural steroid injection. Anesthesiology. 2004;100(2):445–447. doi:10.1097/00000542-200402000-00039
38. Goodman BS, Bayazitoglu M, Mallempati S, Noble BR, Geffen JF. Dural puncture and subdural injection: a complication of lumbar transforaminal epidural injections. Pain Physician. 2007;10(5):697–705.
39. Reitman CA, Watters W. Subdural hematoma after cervical epidural steroid injection. Spine. 2002;27(6):E174–E176. doi:10.1097/00007632-200203150-00022
40. Yoo HS, Park SW, Han JH, et al. Paraplegia caused by an epidural hematoma in a patient with unrecognized chronic idiopathic thrombocytopenic purpura following an epidural steroid injection. Spine. 2009;34(10):E376–E379. doi:10.1097/BRS.0b013e31819d0d45
41. Erbay RH, Senoglu N, Atalay H. Spinal or epidural haematoma. In: Whizar-Lugo VM editor. Topics in Spinal Anaesthesia. InTech;2014. doi:10.5772/58702
42. Smith GA, Pace J, Strohl M, Kaul A, Hayek S, Miller JP. Rare neurosurgical complications of epidural injections: an 8-yr single-institution experience. Operat Surg. 2017;13(2):271–279. doi:10.1093/ons/opw014
43. Huang RC, Shapiro GS, Lim M, Sandhu HS, Lutz GE, Herzog RJ. Cervical epidural abscess after epidural steroid injection. Spine. 2004;29(1):E7–E9. doi:10.1097/01.BRS.0000106764.40001.84
44. Waldman SD. Cervical epidural abscess after cervical epidural nerve block with steroids. Anesth Analg. 1991;72(5):717–718. doi:10.1213/00000539-199105000-00033
45. Epstein N. The risks of epidural and transforaminal steroid injections in the Spine: commentary and a comprehensive review of the literature. Surg Neurol Int. 2013;4(3):74. doi:10.4103/2152-7806.109446
46. Narouze S, Benzon HT, Provenzano D, et al. Interventional spine and pain procedures in patients on antiplatelet and anticoagulant medications (Second Edition): guidelines From the American Society of Regional Anesthesia and Pain Medicine, the European Society of Regional Anaesthesia and Pain Therapy, the American Academy of Pain Medicine, the International Neuromodulation Society, the North American Neuromodulation Society, and the World Institute of Pain. Reg Anesth Pain Med. 2017;1. doi:10.1097/AAP.0000000000000700
47. Boswell MV, Colson JD, Spillane WF. Therapeutic facet joint interventions in chronic spinal pain: a systematic review of effectiveness and complications. Pain Physician. 2005;8(1):101–114.
48. Kim BR, Lee JW, Lee E, Kang Y, Ahn JM, Kang HS. Intra-articular facet joint steroid injection–related adverse events encountered during 11,980 procedures. Eur Radiol. 2020;30(3):1507–1516. doi:10.1007/s00330-019-06483-3
49. Manchikanti L, Malla Y, Wargo BW, Cash KA, Pampati V, Fellows B. Complications of fluoroscopically directed facet joint nerve blocks: a prospective evaluation of 7500 episodes with 43,000 nerve blocks. Pain Physician. 2012;15(2):E143–E150.
50. Plastaras C, McCormick Z, Macron D, et al. Adverse events associated with fluoroscopically guided zygapophyseal joint injections. Pain Physician. 2014;17(4):297–304.
51. Narouze SN, Provenzano DA. Sonographically guided cervical facet nerve and joint injections: why sonography? J Ultrasound Med. 2013;32(11):1885–1896. doi:10.7863/ultra.32.11.1885
52. Lo Bianco G, Papa A, Gazzerro G, et al. Dorsal root ganglion stimulation for chronic postoperative pain following thoracic surgery: a pilot study. Neuromodulation. 2021;24(4):774–778. PMID: 32909359. doi:10.1111/ner.13265
53. Hadzic A, Sala-Blanch X, Xu D. Ultrasound guidance may reduce but not eliminate complications of peripheral nerve blocks. Anesthesiology. 2008;108(4):557–558. doi:10.1097/ALN.0b013e318168efa1
54. Wang D. Image guidance technologies for interventional pain procedures: ultrasound, fluoroscopy, and CT. Curr Pain Headache Rep. 2018;22(1):6. doi:10.1007/s11916-018-0660-1
55. Cappelleri G, Fanelli A, Ghisi D, et al. The role of regional anesthesia during the SARS-CoV2 pandemic: appraisal of clinical, pharmacological and organizational aspects. Front Pharmacol. 2021;12:574091. PMID: 34149401; PMCID: PMC8213435. doi:10.3389/fphar.2021.574091
56. Mandim BLS, Alves RR, Almeida R, Pontes JPJ, Arantes LJ, Morais FP. Pneumothorax post brachial plexus block guided by ultrasound: a case report. Braz J Anesthesiol. 2012;62(5):741–747. doi:10.1016/S0034-7094(12)70173-3
57. Kang BJ, Song J, Ji SM, Kim JP. Myoclonus of ipsilateral upper extremity after ultrasound-guided supraclavicular brachial plexus block with mepivacaine. Korean J Anesthesiol. 2017;70(5):577. doi:10.4097/kjae.2017.70.5.577
58. Beh ZY, Tham HM, Lim YC, Lim NL. Diagnosis of pulmonary embolism due to the use of interscalene block. Korean J Anesthesiol. 2017;70(5):580. doi:10.4097/kjae.2017.70.5.580
59. Loubert C, Williams SR, Hélie F, Arcand G. Complication during ultrasound-guided regional block: accidental intravascular injection of local anesthetic. Anesthesiology. 2008;108(4):759–760. doi:10.1097/ALN.0b013e3181684bfd
60. Zetlaoui PJ, Labbe JP, Benhamou D. Ultrasound guidance for axillary plexus block does not prevent intravascular injection. Anesthesiology. 2008;108(4):761. doi:10.1097/ALN.0b013e3181684c0f
61. Manchikanti L, Knezevic NN, Navani A, et al. Epidural interventions in the management of chronic spinal pain: American Society Of Interventional Pain Physicians (ASIPP) comprehensive evidence-based guidelines. Pain Physician. 2021;24(S1):S27–S208.
62. Van Boxem K, Rijsdijk M, Hans G, et al. Safe use of epidural corticosteroid injections: recommendations of the WIP Benelux Work Group. Pain Pract. 2019;19(1):61–92. doi:10.1111/papr.12709
63. Hurley RW, Adams MCB, Barad M, et al. Consensus practice guidelines on interventions for cervical spine (facet) joint pain from a multispecialty international working group. Pain Med. 2021;22(11):2443–2524. doi:10.1093/pm/pnab281
64. Rathmell JP, Aprill C, Bogduk N. Cervical transforaminal injection of steroids. Anesthesiology. 2004;100(6):1595–1600. doi:10.1097/00000542-200406000-00035
65. Bush K, Mandegaran R, Robinson E, Zavareh A. The safety and efficiency of performing cervical transforaminal epidural steroid injections under fluoroscopic control on an ambulatory/outpatient basis. Eur Spine J. 2020;29(5):994–1000. doi:10.1007/s00586-019-06147-2
66. Choi EJ, Kim DH, Han WK, et al. Non-particulate steroids (Betamethasone Sodium Phosphate, Dexamethasone Sodium Phosphate, and Dexamethasone Palmitate) Combined with Local Anesthetics (Ropivacaine, Levobupivacaine, Bupivacaine, and Lidocaine): a potentially unsafe mixture. JPR. 2021;14:1495–1504. doi:10.2147/JPR.S311573
67. Sehgal N, Dunbar EE, Shah RV, Colson J. Systematic review of diagnostic utility of facet (zygapophysial) joint injections in chronic spinal pain: an update. Pain Physician. 2007;10(1):213–228.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Opioid Utilization and Management in the Setting of Stewardship During Inpatient Rehab Care
Murphy L, Leblanc K, Badr S, Ching E, Mao L, Steenhof N, Hamandi B, Rubin B, Seto A, Furlan AD
Drug, Healthcare and Patient Safety 2022, 14:161-170
Published Date: 11 September 2022
Surveying Canadian Pain Physicians’ Attitudes and Beliefs Regarding Medical Cannabis for Chronic Noncancer Pain: A Qualitative Study
Ng JY, Quach H, Phillips MR, Busse JW
Journal of Pain Research 2022, 15:3899-3910
Published Date: 14 December 2022
Radiofrequency Ablation for Chronic Lumbar Zygapophyseal Joint Pain Using a V-Shaped Active Tip Needle: An Observational Retrospective Study
Lo Bianco G, Misseri G, Stogicza AR, Cesare G, Li S, Day M, Kennedy DJ, Schatman ME
Journal of Pain Research 2023, 16:1243-1255
Published Date: 11 April 2023
A Randomized, Double-Blind, Placebo-Controlled Trial to Evaluate the Therapeutic Effect of Magnesium-L-Threonate Supplementation for Persistent Pain After Breast Cancer Surgery
Ni Y, Deng F, Yu S, Zhang J, Zhang X, Huang D, Zhou H
Breast Cancer: Targets and Therapy 2023, 15:495-504
Published Date: 25 July 2023
Methylnaltrexone Treatment for Opioid-Induced Constipation in Patients with and without Cancer: Effect of Initial Dose
Chamberlain BH, Rhiner M, Slatkin NE, Stambler N, Israel RJ
Journal of Pain Research 2023, 16:2595-2607
Published Date: 27 July 2023