Back to Journals » Journal of Pain Research » Volume 16
Feasibility and Acceptability of the Pain Profile, a Clinical Questionnaire Aimed at Improving Pain Care
Authors Zarska A ![]() , Slat S
, Slat S ![]() , Kehne A, Macleod C, Rye H, Dehmlow C, Hilliard P
, Kehne A, Macleod C, Rye H, Dehmlow C, Hilliard P ![]() , Jaffe K, Lagisetty P
, Jaffe K, Lagisetty P
Received 31 January 2023
Accepted for publication 17 April 2023
Published 11 May 2023 Volume 2023:16 Pages 1559—1571
DOI https://doi.org/10.2147/JPR.S402354
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Robert Twillman
Aleksandra Zarska,1 Stephanie Slat,1 Adrianne Kehne,1,2 Colin Macleod,1 Heather Rye,3 Cheryl Dehmlow,4 Paul Hilliard,5 Kaitlyn Jaffe,6 Pooja Lagisetty1,2
1Department of Internal Medicine, University of Michigan, Ann Arbor, MI, USA; 2Center for Clinical Management and Research, Ann Arbor Veterans Health Administration, Ann Arbor, MI, USA; 3University of Michigan Medical Group Care Management – Complex Care Management, University of Michigan, Ann Arbor, MI, USA; 4Health Information Technology & Services, Michigan Medicine, University of Michigan, Ann Arbor, MI, USA; 5Department of Anesthesiology, University of Michigan, Ann Arbor, MI, USA; 6Center for Bioethics and Social Sciences in Medicine, University of Michigan, Ann Arbor, MI, USA
Correspondence: Aleksandra Zarska, Department of Internal Medicine, University of Michigan, 2800 Plymouth Road, Building 16, Floor 4, Ann Arbor, MI, 48109, USA, Tel +17186109960, Email [email protected]
Purpose: Despite being one of the most common medical complaints, chronic pain is difficult to manage due to ineffective communication between providers and patients and time restraints during appointments. Patient-centered questionnaires have the potential to optimize communication by assessing a patient’s pain history, prior treatments, and associated comorbidities to develop an effective treatment plan. This study aimed to analyze the feasibility and acceptability of a pre-visit clinical questionnaire aimed at improving communication and pain care.
Patients and Methods: The “Pain Profile” questionnaire was piloted across two specialty pain clinics in a large academic medical center. Patient and provider surveys were conducted with patients who completed the Pain Profile questionnaire and providers who use it in practice. Surveys consisted of multiple-choice and open-ended questions regarding the helpfulness, usability, and implementation of the questionnaire. Descriptive analyses of patient and provider surveys were conducted. Qualitative data were analyzed using matrix framework-based coding.
Results: A total of 171 patients and 32 clinical providers completed the feasibility and acceptability surveys. 77% of patients (N= 131) found the Pain Profile helpful in communicating their pain experiences and 69% of providers (N= 22) found it helpful in guiding clinical decisions. The section that assessed the impact of pain was rated most helpful by patients (4/5) while the open-ended section asking patients to describe their pain history was rated least helpful by patients and providers (3.7/5 and 4.1/5, respectively). Both patients and providers provided suggestions to future iterations of the Pain Profile, including the addition of opioid risk and mental health screening tools.
Conclusion: The Pain Profile questionnaire was feasible and acceptable in a pilot study at a large academic site. Future testing in a large-scale, fully powered trial is needed to assess the effectiveness of the Pain Profile in optimizing communication and pain management.
Keywords: chronic pain, communication, clinical questionnaire, pain management, outpatient care
Introduction
Chronic pain affects an estimated 50.2 million people in the United States.1 However, despite being one of the most common medical complaints, pain is increasingly difficult to manage and treat.2,3 Two prevalent barriers to providing effective pain care include time restraints during medical appointments and poor communication between clinical providers and patients around pain.4–8 In outpatient settings, where the majority of patients with chronic pain regularly seek medical care,9,10 providers are often tasked with collecting comprehensive patient histories during average 15-minute visits.11 However, this can be particularly challenging when treating patients on multiple medications or with numerous comorbidities.12 In addition, pain can be difficult for patients to communicate using objective measures, and therefore, clinicians must rely on subjective, self-reported accounts to measure the impact of pain.13,14 This may result in a lack of understanding between patients and providers, leading to diverging perspectives on goals for treatment.4 Given these challenges, patients with chronic pain often cite feeling misunderstood and frustrated, and unsatisfied with the pain treatment they receive.15,16
Ineffective communication between providers and patients can leave chronic pain patients particularly vulnerable to experiencing uncontrolled pain, diminished quality of life, poor health and functioning, anxiety and depression, and opioid dependence.2,17 As a result, improving communication around pain is essential to improving outcomes for this patient population.4 Clinical tools such as patient-centered decision aids and questionnaires can help address this gap.4,18,19 For patients with chronic pain, clinical questionnaires that assess pain intensity, pain location, and functioning could help physicians garner a comprehensive understanding of a patient’s pain history and develop an effective treatment plan.3 However, thus far there is limited evidence on the use of such questionnaires.3,13 As a result, a clinical questionnaire that (1) is tailored to a patient’s full and comprehensive pain history; (2) integrates patients’ preferences and goals into their treatment plans; and (3) provides patients with the opportunity to freely describe their pain while unhindered by time restraints is warranted to address this critical gap.
Therefore, in this study we aimed to assess the overall feasibility and acceptability of the “Pain Profile”, a succinct, centralized, patient-centered questionnaire embedded within the electronic medical record (EMR) (Supplementary Figure 1). This questionnaire aims to improve communication and pain care by capturing patients’ pain stories, standardized descriptors of patient pain, and comprehensive treatment histories (medication and non-medication-based).
Materials and Methods
The University of Michigan Institutional Review Board approved this study (HUM#00207985) under federal exemption 5, which applies to research centered on improving the quality of an existing project.20
Pain Profile Questionnaire
The Pain Profile questionnaire was developed at a large academic institution in 2019 by a team of multidisciplinary experts as part of a quality improvement initiative aimed at improving pain management. The team consisted of physicians, nurses, physician assistants, and prescribers in ambulatory care, anesthesiology, pain medicine, emergency medicine, and surgery, and incorporated feedback from various stakeholders including patients and their families. The Pain Profile questionnaire was then implemented at two pain clinics and one rheumatology clinic at a large academic site and assigned as a voluntary form to all patients followed by Complex Care Management in 2019 and 2020. The questionnaire is fielded prior to patient visits via either a web-based patient portal or paper and takes on average 5–15 minutes to complete. Providers are able to review patients’ Pain Profile questionnaire responses prior to appointments with the aim of optimizing communication around a patient’s history with pain and prioritizing treatment options.
The patient-facing version of the Pain Profile questionnaire includes five sections: “pain story”, “pain areas”, “past treatments (divided into pharmaceutic and non-pharmaceutic treatments)”, “pain goals”, and “pain impact” (Table 1). The provider-facing version of the Pain Profile questionnaire includes a sixth section: “provider notes”, an open-ended section for providers to write notes specific to the patient’s pain history and treatment plan. The first section, “pain story”, is an open-ended text field in response to the prompt, “Tell us about your pain”. Next, patients complete the “pain areas” section, where they are shown an image of the Michigan Body Map,21 a validated self-report measure to help describe and quantify the areas where chronic pain is experienced. For each pain area chosen on the Michigan Body Map, patients choose from a list of 15 descriptors (eg, throbbing, shooting, stabbing, sharp, cramping, aching, etc) based on the short-form McGill Pain Questionnaire,22 rate the severity of their pain over the last week (0=no pain, 10=worst pain ever)23 while referencing the Faces Pain Scale-Revised,24 and indicate how long they have experienced the pain (less than 6 weeks, 6–12 weeks, more than 3 months). In the next section, “pain impact”, patients are asked how often pain impacts their sleep, mood, and everyday activities (never, almost never, sometimes, often, almost always).25–28 In the medication treatments sections, patients choose from a list of non-pharmaceutical therapies (physical therapy, exercise/yoga/stretching, mindfulness/meditation, counseling/behavioral interventions, chiropractic/massage, acupuncture, music/art therapy, heat/cold, aromatherapy) and pharmaceutical therapies (NSAIDs, antidepressants, anticonvulsants, muscle relaxants, opioids, injections, etc.) and indicate whether they have ever tried, are currently using, or would like to try each therapy.25,26 Lastly, patients complete the “pain goals” section by answering the open-ended question: “what are your goals and expectations for your pain management?”
 |
Table 1 Description of the Components of the Pain Profile Questionnaire |
Following the implementation of the Pain Profile in 2019–2020, receptiveness and utility of the Pain Profile questionnaire was examined by the study team via patient and provider surveys.
Feasibility and Acceptability Surveys
The feasibility and acceptability of the Pain Profile questionnaire was assessed using patient and provider surveys. Patients and providers were asked multiple choice and optional free text questions in two 38–44-question surveys. The major themes that were assessed by the patient and provider surveys were: (1) Helpfulness of the Pain Profile; (2) Usability and implementation of the Pain Profile; and (3) Improvements to future iterations of the Pain Profile.
While question themes were consistent between both patients and providers, survey content was tailored to each group. For example, the helpfulness of the questionnaire was evaluated as a function of how well it helped patients communicate information about their pain in the patient surveys and whether it helped providers make clinical decisions in the provider surveys. Patients were also asked about their perspectives on completion time, while providers were asked about their perceptions on barriers to patient completion, as well as their current utilization of the Pain Profile questionnaire. Patients and providers were also asked about the ease of accessing the Pain Profile questionnaire, their preferred modalities (ie, paper vs virtual), and their preferred frequency of completing (patients) and reviewing (providers) the Pain Profile questionnaire. Questions on ease of access, modality, completion time, and barriers are represented by the overarching concept of usability. Questions on provider utilization are represented by the concept of implementation. When appropriate, patients and providers answered the same questions to increase comparative power.
Patient and Provider Recruitment
The study team used electronic medical records to identify a stratified random sample of 25% (n=325) of patients who had completed the Pain Profile questionnaire between November 2019 and August 2021, stratified by race and insurance type. To be eligible for study participation, patients had to have a phone number or email address listed in the EMR and be above the age of 18 and directly involved in completing the Pain Profile questionnaire (ie, it could not have been completed on their behalf by a caregiver) (Supplementary Figure 2). Eligible patients were contacted by e-mail to complete an optional patient-specific survey with informed consent, which included publication of anonymized responses, via Qualtrics and offered a $25 incentive to complete the survey.
To identify potential provider participants, a list of clinical providers was created using all providers listed in patient EMR data as well as a list provided by a clinical administrator. This list included physicians, nurse practitioners, physician assistants, social workers, and pain psychologists who had used the Pain Profile questionnaire at the institution. Eligible providers were sent an email with a link to complete an optional provider-specific survey via Qualtrics asking about their experience using the Pain Profile and offered a $25 incentive to complete the survey. Informed consent, which included publication of anonymized responses, was obtained prior to completing the survey.
Data Analysis
Quantitative data analysis was largely descriptive and was performed on patient information and results of the original Pain Profile questionnaire, the patient survey, and the provider survey. Survey results are reported as frequency-percent for multinomial and dichotomous variables, and as mean-standard deviation for continuous variables. Where appropriate, patient and provider responses to comparable question themes were examined in tandem to examine the effect of role difference on the perception of the Pain Profile questionnaire. A sensitivity analysis of bivariate comparisons of outcome variables and demographic variables, accounting for multiple comparisons using a Bonferroni29 p-value correction, was conducted to ensure that outcome variables did not differ significantly across demographic categories (ie, sex, age, race, or health insurance category).
Qualitative data were analyzed using a matrix framework-based thematic coding method30 in order to identify the prevalence and relative importance of subtopics provided by optional open-text responses. First, text information was deidentified to remove any personal identifiers and preserve respondent anonymity. Next, themes were identified and responses to each optional, open-text survey question were coded into categories by two study team members independently. Following independent analysis, the study team members convened to discuss differences in category placement, category creation, and fit. Any inconsistencies were discussed and agreed upon to ensure consensus among the two study team members. Theme frequencies were constructed to identify the most prevalent themes generated (eg, Pain Profile not used enough by physicians, Pain Profile should be used on an as-needed basis). Theme importance was derived from the relative frequency of the theme in each open-ended question. Final consensus was reached in study team meetings by selecting illustrative and cogent quotes from the most representative themes throughout the free text question responses.
Results
There were 1298 patients who completed the Pain Profile questionnaire prior to a clinical appointment. Of these patients, 1235 met eligibility criteria to complete the evaluation survey. Of this group, 325 (25%) patients were randomly selected to complete the survey assessing feasibility and acceptability of using the Pain Profile Questionnaire. Of the 325 patients sampled, 105 were unable to be reached by email or phone call. Of those who were successfully contacted by email or phone call, 171 completed the feasibility and acceptability survey. Patients’ mean age was 51.5 years, and 114 (67%) patient respondents were female (Table 2). When correcting for multiple comparisons, no significant difference was found in the outcome variables as it related to demographic categories including sex, age, race, or health insurance category.
 |
Table 2 Demographic Characteristics of Survey Patient Participants |
Of 44 potential provider subjects, 32 (73%) completed the provider survey. Twenty-three of the 32 (72%) providers were physicians, five (16%) were nurse practitioners or physician assistants, and two (6%) were pain psychologists. Of the 32 physicians, 19 (59%) specialized in anesthesiology, two (6%) specialized in general medicine, one specialized in rheumatology (3%), one specialized in neurology, and nine (28%) marked “other” as their specialty.
Pain Profile Helpfulness
Patients
Overall, patients found the Pain Profile helpful in communicating their pain stories (2.6/4, SD=1.1) (Table 3). Of the five sections of the Pain Profile, patients rated “pain impact” (4/5, SD=1.1) and “past treatments: medications” (3.9/5, SD=1.0) sections most favorably. Of the five sections of the Pain Profile questionnaire, the “pain story” was rated least favorably by patients (3.7/5, SD=1.0). When asked which section of the Pain Profile contains unnecessary questions, 131 of 171 patients (76.6%) said none, 16 (9.4%) selected the “pain story”, 14 (8.2%) selected “pain goals”, 10 (5.6%) selected “past treatments (non-medications)”, six (3.5%) selected “pain areas”, six (3.5%) selected “past treatments (medications)”, and four (2.3%) selected “pain impact”. One patient pointed to the burden of completing the “pain story” section stating, “[It] takes too long to type it all out. [It] would have been easier to just tell someone”.
 |
Table 3 Patient and Provider Views on the Helpfulness of the Pain Profile |
Providers
Overall, providers reported that the Pain Profile was helpful in making clinical decisions (2.5/4, SD=0.8). Of the six sections of the Pain Profile, providers rated the “past treatments (non-medications)” (4.7/5, SD=0.5) and “past treatments (medications)” (4.6/5, SD=0.8) sections most favorably, and the “pain story” (4.1/5, SD=0.8) and “pain areas” (4.1/5, SD=1.0) sections least favorably on a scale of 1–5. In the open-ended survey responses, one provider noted that the Pain Profile questionnaire “helps to focus the appointment on those [pain complaints] that are most pertinent”. On the other hand, one provider expressed concerns about the Pain Profile replacing the patient-provider relationship:
I worry that . . . providers will use this as a substitute for actually listening to patients in person. What I hear most often from patients is that providers aren’t paying attention to them from behind their computer screens. [The Pain Story] should not replace hearing a person tell their pain story in person.
Of 32 providers, 18 (56.3%) reported that the Pain Profile was helpful in reviewing treatment history, 15 (46.9%) reported it was helpful in understanding patients’ pain regions, 13 (40.6%) reported it was helpful in guiding pharmacologic treatment, 11 (34.4%) reported it was helpful in guiding non-pharmacologic treatment, and five (15.6%) reported it was helpful in developing a better patient-provider relationship. However, providers also expressed concerns on the accuracy of the medications section in their open-ended responses. One provider stated, “The medical literacy . . . is high . . . patients may not . . . correctly identify medications they have taken”.
When asked which sections of the Pain Profile contain unnecessary questions, 17 providers (53.1%) responded none, six (18.8%) selected “provider notes”, four (12.5%) selected “pain goals”, three (9.4%) selected “pain story”, two (6.3%) selected “pain areas”, one (3.1%) selected “pain impact”, one (3.1%) selected “past treatments (medications)”, and zero providers selected “past treatments (non-medications)”.
Pain Profile Usability and Implementation
Patients
Patients rated the ease of accessing and completing the Pain Profile high (4/5, SD=1.0) (Table 4). Of 171 patients, 133 (77.8%) reported that the Pain Profile took an appropriate amount of time to complete, 28 (16.4%) reported that the Pain Profile was too long, and seven (4.1%) reported that it was too short. Of the 171 patients surveyed, 68 (39.8%) patients stated they completed the Pain Profile in the patient portal, 41 (24%) stated they used a paper form, and 62 (36.2%) respondents were not sure or missing. When asked if they would prefer to complete the Pain Profile through a different modality, 87 patients (50.9%) stated no and nine (5.3%) stated yes. Additionally, the majority of patients expressed interest in completing the Pain Profile regularly: 111 of 171 patients (64.9%) responded that they would like to complete the survey prior to every visit or every 6–12 months.
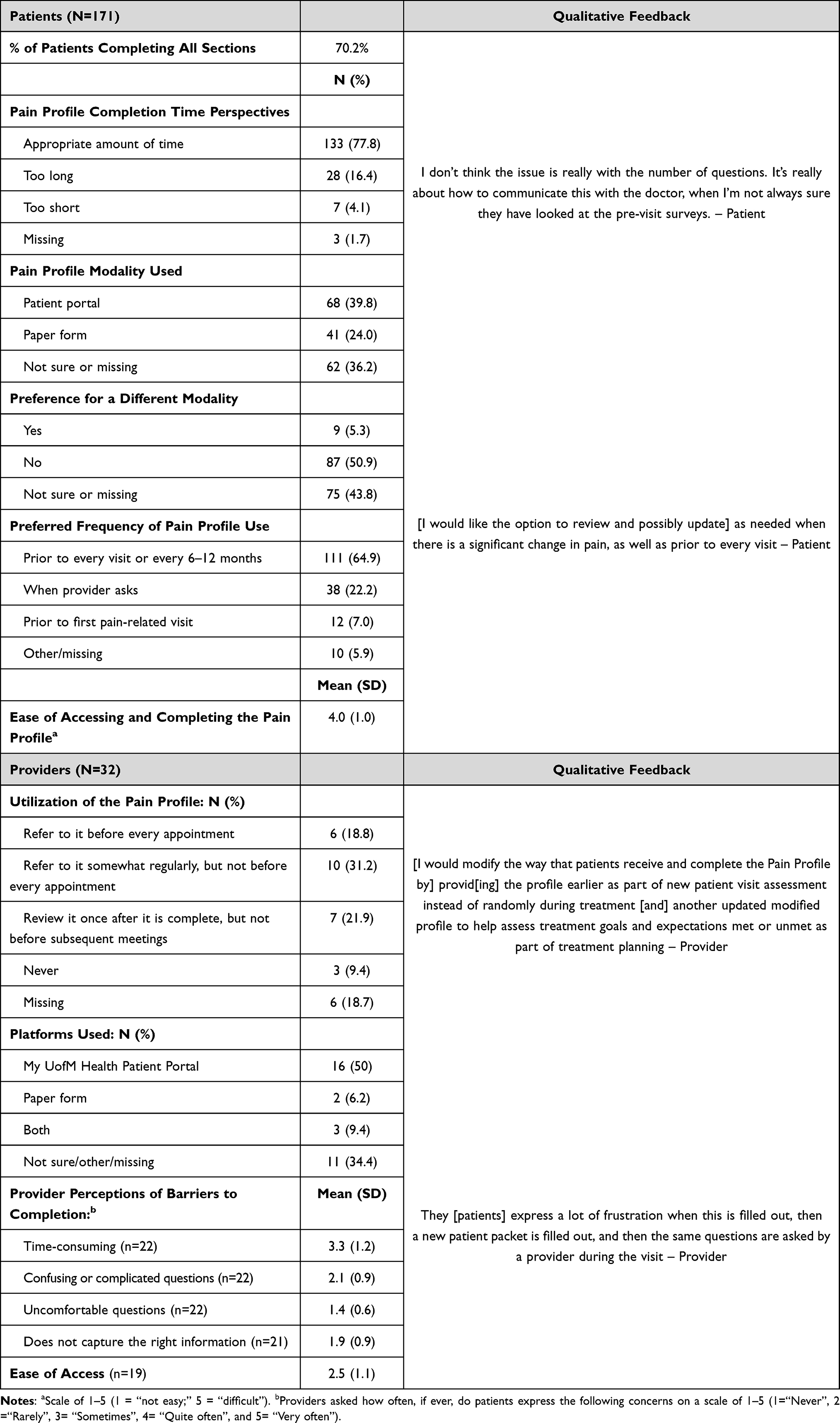 |
Table 4 Patient and Provider Views on Usability and Implementation of the Pain Profile |
Providers
Of the 32 providers surveyed, 10 (31.2%) stated that they refer to the Pain Profile somewhat regularly, but not before every appointment; seven (21.9%) stated that they review it once after it is complete, but not before subsequent meetings; six (18.8%) stated that they refer to the Pain Profile before every appointment, and three (18.9%) responded that they have never referred to the Pain Profile. When asked to rate how easy it is to access the Pain Profile on a scale of 1–5 (5 representing “difficult”), providers (n=19) responded with a mean rating of 2.5 (SD=1.1). In response to the open-ended free text survey question asking providers what other changes would make the Pain Profile helpful for them, as clinicians, one provider brought up concerns about the location and burden of accessing the information gathered by the Pain Profile in the EMR, stating: “It doesn’t feel as helpful to me to have the information. buried in the chart”. Several providers also expressed that they have never used the Pain Profile and/or are not sure where to find it. Patients echoed this sentiment, with one patient sharing: “In my experience, it seems like the doctors don’t review the information, or don’t take it seriously”. When asked if there are any other concerns that patients express about the Pain Profile, one provider also cited the patient burden of redundant paperwork:
[Patients] express a lot of frustration when this is filled out, then a new patient packet is filled out, and then the same questions are asked by a provider during the visit.
Future Improvements to the Pain Profile
Patients
When asked what additional questions they would like to see included in the Pain Profile, several patients expressed an interest in having more autonomy over their treatment plan (Table 5). One patient suggested including an option to rank the treatments patients would most like to try for their pain management. Patients also pointed to the inherent subjectiveness of pain, indicating that they would like to be asked about their functioning, rather than rating their pain on an objective scale:
[I would like to see additional questions on] a point of reference for pain. Chronic pain patients have a very high tolerance for pain and what. “hurts bad” to a chronic pain sufferer may be excruciating to others.
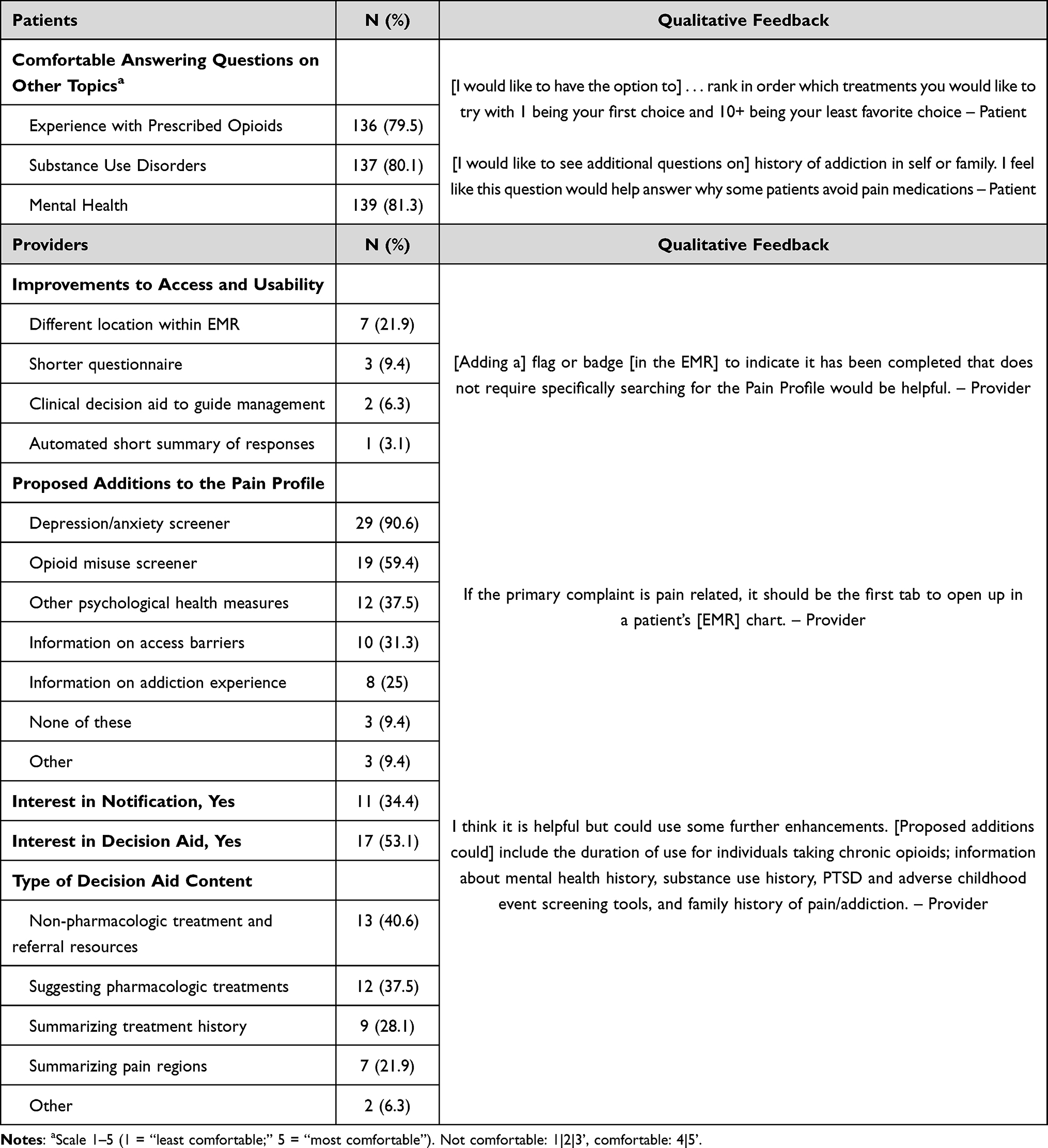 |
Table 5 Patient and Provider Suggestions on Future Improvements to the Pain Profile |
Many patients also indicated that they would feel comfortable answering additional questions on addiction, substance use, and mental health: 80% of patients expressed they would feel comfortable answering questions about their experiences with prescribed opioids and substance use disorders. While 81% of patients also indicated they would be comfortable answering questions on mental health in the quantitative survey data, a few patients expressed concerns about privacy and abuse of the sensitive information provided in the Pain Profile.
Providers
Although providers found the Pain Profile helpful in making clinical decisions, many expressed that strategies should be implemented to improve use of and access to the questionnaire. Seven of 32 providers (21.9%) indicated that they would like to see the Pain Profile in a different location within the EMR, while 11 (34.4%) said they would like a notification to be added once a patient completes the Pain Profile (Table 5). When asked how they would change the location of the questionnaire, some providers pointed to the burden of searching for the Pain Profile in the EMR:
Physicians will not look at it unless they know it exists; I think most of our physicians do not. Some kind of flag or badge . . . would be helpful.
While only three of 32 providers (9.4%) expressed interest in a shorter questionnaire and one (3.1%) expressed interest in a shorter summary of responses in the quantitative survey findings, multiple providers supported including a “succinct summary” of the Pain Profile in the EMR. Interest in mental health and substance use screeners was also high among providers: 29 of 32 providers (90.6%) supported adding a depression/anxiety screener, 19 (59.4%) supported adding an opioid misuse screener, 12 (37.5%) supported other psychological health measures, and eight (25%) supported adding information on addiction experience. Lastly, provider views on a decision aid were mixed among providers, with 17 of 32 (53%) indicating they would like to see a decision aid included in the Pain Profile. The most popular types of decision aid content were non-pharmacologic treatment and referral resources (40.6% of providers), pharmacologic treatments (37.5%), and summary of treatment history (28.1%).
Discussion
Poor communication around chronic pain between providers and patients coupled with time restraints during short appointment times can lead to uncontrolled pain, poor outcomes, and dissatisfaction with pain treatment.2,14,17 In this study, we evaluated a novel pre-visit patient-facing questionnaire aimed at optimizing pain-related communication. Both patients and providers surveyed found the Pain Profile questionnaire to be feasible and acceptable, indicating that the Pain Profile is a promising questionnaire for addressing these issues in the management of chronic pain in outpatient settings.
To our knowledge, this study was the first to explore the use of a comprehensive, patient-centered questionnaire embedded in the electronic medical record for the management of chronic pain in the outpatient setting.3,13 One recent pilot study of a virtual shared decision-making tool called the PainAPP tool, which aimed to improve patient-provider communication around pain by incorporating patients’ treatment goals as well as a pain assessment with an opioid risk screening component, found the tool to be feasible.4 However, the study was limited by a small sample size, and unlike the Pain Profile questionnaire, the PainAPP tool was not embedded in the electronic medical record, but rather used as an independent online application. Because the Pain Profile questionnaire is completed as an EMR-based questionnaire outside of clinician notes, it provides a portable account of patients’ pain stories, which are complex, multi-faceted, and often difficult to comprehensively discuss in time-constrained office visits. Therefore, by reviewing the Pain Profile in advance, providers can better prioritize treatments and incorporate patients’ goals and motivations into practice. Furthermore, the Pain Profile questionnaire may also help reduce emotional and psychological burden for patients and promote healing by providing them with a platform to explain their pain narrative.31 Lastly, the Pain Profile may help mitigate care fragmentation by reducing the need for patients to re-explain their pain history to various providers across the care spectrum, as well as reduce history-taking burden on clinicians given that patients can complete and frequently update the questionnaire before appointments.32
While providers and patients found the questionnaire helpful, both groups also offered suggestions for modifications to future iterations of the Pain Profile questionnaire. Both patients and providers indicated that the open-ended “pain story” was the least clinically helpful section, with providers echoing fears that this section might serve as a replacement to the act of actively listening to a patient’s story in-person. Patient storytelling has been recognized as a critical way for patients to explain their pain in their own words and for providers to assess pain and plan treatments.33 However, this finding may warrant a modification in how the pain story is collected and recorded in the questionnaire, perhaps with the pain story instead serving as a verbal dictation taken from patients during an initial office visit. Other suggested modifications include the addition of screening tools about opioid risk and depression and anxiety, which were endorsed by both provider and patient respondents. Notably, our finding that several providers do not use the Pain Profile questionnaire, or know where to find it in the EMR, also suggests that improvements to usability and implementation are necessary.
Our pilot study has several limitations. First, we sampled only a subset of patients who completed the Pain Profile questionnaire and did not assess barriers to use in those who did not complete the questionnaire initially. However, we successfully contacted over 200 diverse patient respondents to gather input on the Pain Profile questionnaire and conducted a sensitivity analysis which showed that there was no significant difference between the demographics (sex, race, and health insurance type) of completers and non-completers of the questionnaire outside of age. Additionally, our survey assessed patient perspectives on the Pain Profile questionnaire on average 12 months after patient completion of the questionnaire in clinics. Consequently, this may have limited patient recall and assessment of specific portions of the questionnaire and may have counteracted a recency bias effect which can yield results skewed towards favorability. To address this limitation and aid with patient and provider recall, surveys included screen-capture images of each section of the Pain Profile questionnaire that respondents were asked to assess. Furthermore, qualitative data were derived from optional, open-text questions, but not all patients provided comments. Thus, there may have been some response bias. Despite this limitation, qualitative themes were consistent with quantitative survey results, indicating that the Pain Profile was feasible and acceptable in the pilot study. Also, we did not assess native language as a variable, which may have affected response data if patients whose first language was not English did not feel comfortable answering the optional, open-text response questions. Lastly, our pilot studies were conducted at two pain clinics and one rheumatology clinic at a large academic medical center and may not be generalizable to other outpatient settings or specialty pain clinics independent of a large health system.
To our knowledge, the Pain Profile is the first clinical questionnaire embedded in the electronic medical record that encompasses comprehensive and open-ended information on the area, impact, history, and treatment of a patient’s pain in the outpatient setting. Chronic pain is a multi-faceted and complex condition that, if left untreated, can cause debilitating outcomes for patients ranging from uncontrolled pain to anxiety, depression, and opioid dependence.2,17 Our results indicate that the Pain Profile questionnaire is a promising way to help address these issues by improving patient-provider communication around pain and providing patients with the opportunity to voice their pain histories and incorporate their preferences and goals into their treatment plans. While improvements to the questionnaire surrounding usability, access, and content are warranted, our pilot study findings indicate that the Pain Profile is a feasible and acceptable clinical questionnaire in the outpatient management of chronic pain. Future testing in a large-scale, fully powered trial is needed to assess the effectiveness of the Pain Profile in optimizing communication and improving chronic pain management on a wider scale.
Disclosure
This work was funded by the National Institute on Drug Abuse of the National Institutes of Health [grant number K23 DA047475 (PAL)]. Dr Pooja Lagisetty reports grants from National Institutes of Health, during the conduct of the study. The authors have no financial relationships or conflicts of interest to disclose.
References
1. Yong RJ, Mullins PM, Bhattacharyya N. Prevalence of chronic pain among adults in the United States. Pain. 2022;163(2):e328–e332. doi:10.1097/j.pain.0000000000002291
2. Dydyk AM, Conermann T. Chronic pain. In: StatPearls. StatPearls Publishing; 2022. Available from: http://www.ncbi.nlm.nih.gov/books/NBK553030/.
3. Dansie EJ, Turk DC. Assessment of patients with chronic pain. Br J Anaesth. 2013;111(1):19–25. doi:10.1093/bja/aet124
4. Col N, Hull S, Springmann V, et al. Improving patient-provider communication about chronic pain: development and feasibility testing of a shared decision-making tool. BMC Med Inform Decis Mak. 2020;20(1):267. doi:10.1186/s12911-020-01279-8
5. Kenny DT. Constructions of chronic pain in doctor-patient relationships: bridging the communication chasm. Patient Educ Couns. 2004;52(3):297–305. doi:10.1016/S0738-3991(03)00105-8
6. Esquibel AY, Borkan J. Doctors and patients in pain: conflict and collaboration in opioid prescription in primary care. Pain. 2014;155(12):2575–2582. doi:10.1016/j.pain.2014.09.018
7. Henry SG, Matthias MS. Patient-clinician communication about pain: a conceptual model and narrative review. Pain Med. 2018;19(11):2154–2165. doi:10.1093/pm/pny003
8. Militello LG, Hurley RW, Cook RL, et al. Primary care clinicians’ beliefs and strategies for managing chronic pain in an era of a national opioid epidemic. J Gen Intern Med. 2020;35(12):3542–3548. doi:10.1007/s11606-020-06178-2
9. Bifulco L, Anderson DR, Blankson ML, et al. Evaluation of a chronic pain screening program implemented in primary care. JAMA Network Open. 2021;4(7):e2118495. doi:10.1001/jamanetworkopen.2021.18495
10. Harle CA, Bauer SE, Hoang HQ, Cook RL, Hurley RW, Fillingim RB. Decision support for chronic pain care: how do primary care physicians decide when to prescribe opioids? A qualitative study. BMC Fam Pract. 2015;16(1):48. doi:10.1186/s12875-015-0264-3
11. Blumenthal D, Causino N, Chang YC, et al. The duration of ambulatory visits to physicians. J Fam Pract. 1999;48(4):264–271.
12. Reid MC, Eccleston C, Pillemer K. Management of chronic pain in older adults. BMJ. 2015;350(feb13 2):h532. doi:10.1136/bmj.h532
13. Younger J, McCue R, Mackey S. Pain outcomes: a brief review of instruments and techniques. Curr Pain Headache Rep. 2009;13(1):39–43. doi:10.1007/s11916-009-0009-x
14. Wideman TH, Edwards RR, Walton DM, Martel MO, Hudon A, Seminowicz DA. The multimodal assessment model of pain. Clin J Pain. 2019;35(3):212–221. doi:10.1097/AJP.0000000000000670
15. Allvin R, Fjordkvist E, Blomberg K. Struggling to be seen and understood as a person – chronic back pain patients’ experiences of encounters in health care: an interview study. Nurs Open. 2019;6(3):1047–1054. doi:10.1002/nop2.290
16. Upshur CC, Bacigalupe G, Luckmann R. “They don’t want anything to do with you”: patient views of primary care management of chronic pain. Pain Med. 2010;11(12):1791–1798. doi:10.1111/j.1526-4637.2010.00960.x
17. Fine PG. Long-term consequences of chronic pain: mounting evidence for pain as a neurological disease and parallels with other chronic disease states. Pain Med. 2011;12(7):996–1004. doi:10.1111/j.1526-4637.2011.01187.x
18. Wieringa TH, Kunneman M, Rodriguez-Gutierrez R, et al. A systematic review of decision aids that facilitate elements of shared decision-making in chronic illnesses: a review protocol. Syst Rev. 2017;6(1):155. doi:10.1186/s13643-017-0557-9
19. Bowen E, Nayfe R, Milburn N, et al. Do decision aids benefit patients with chronic musculoskeletal pain? A systematic review. Pain Med. 2020;21(5):951–969. doi:10.1093/pm/pnz280
20. United States code of federal regulations, title 45, subtitle A, subchapter A §46.104. Available from: https://www.ecfr.gov/current/title-45/subtitle-A/subchapter-A/part-46/subpart-A/section-46.104.
21. Brummett CM, Bakshi RR, Goesling J, et al. Preliminary validation of the Michigan body map. Pain. 2016;157(6):1205–1212. doi:10.1097/j.pain.0000000000000506
22. Melzack R. The short-form McGill pain questionnaire. Pain. 1987;30(2):191–197. doi:10.1016/0304-3959(87)91074-8
23. Breivik H, Borchgrevink PC, Allen SM, et al. Assessment of pain. Br J Anaesth. 2008;101(1):17–24. doi:10.1093/bja/aen103
24. Hicks CL, von Baeyer CL, Spafford PA, van Korlaar I, Goodenough B. The faces pain scale-revised: toward a common metric in pediatric pain measurement. Pain. 2001;93(2):173–183. doi:10.1016/S0304-3959(01)00314-1
25. Melzack R. The McGill pain questionnaire: major properties and scoring methods. Pain. 1975;1(3):277–299. doi:10.1016/0304-3959(75)90044-5
26. Tan G, Jensen MP, Thornby JI, Shanti BF. Validation of the brief pain inventory for chronic nonmalignant pain. J Pain. 2004;5(2):133–137. doi:10.1016/j.jpain.2003.12.005
27. Bernstein IH, Jaremko ME, Hinkley BS. On the utility of the west haven-yale multidimensional pain inventory. Spine. 1995;20(8):956–963. doi:10.1097/00007632-199504150-00014
28. Ayearst LE, Harsanyi Z, Michalko KJ. The Pain and Sleep Questionnaire three-item index (PSQ-3): a reliable and valid measure of the impact of pain on sleep in chronic nonmalignant pain of various etiologies. Pain Res Manag. 2012;17(4):281–290. doi:10.1155/2012/635967
29. Haynes W. Bonferroni correction. In: Dubitzky W, Wolkenhauer O, Cho KH, Yokota H, editors. Encyclopedia of Systems Biology. Springer; 2013:154. doi:10.1007/978-1-4419-9863-7_1213
30. Gale NK, Heath G, Cameron E, Rashid S, Redwood S. Using the framework method for the analysis of qualitative data in multi-disciplinary health research. BMC Med Res Methodol. 2013;13(1):117. doi:10.1186/1471-2288-13-117
31. “Power of storytelling”: a content analysis of chronic pain narratives on YouTube. Available from: https://www.tandfonline.com/doi/epub/10.1080/24740527.2021.1929117?needAccess=true&role=button.
32. Varsi C, Ledel Solem IK, Eide H, et al. Health care providers’ experiences of pain management and attitudes towards digitally supported self-management interventions for chronic pain: a qualitative study. BMC Health Serv Res. 2021;21(1):275. doi:10.1186/s12913-021-06278-7
33. Fink R. Pain assessment: the cornerstone to optimal pain management. Proc (Bayl Univ Med Cent). 2000;13(3):236–239. doi:10.1080/08998280.2000.11927681
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Surveying Canadian Pain Physicians’ Attitudes and Beliefs Regarding Medical Cannabis for Chronic Noncancer Pain: A Qualitative Study
Ng JY, Quach H, Phillips MR, Busse JW
Journal of Pain Research 2022, 15:3899-3910
Published Date: 14 December 2022
Radiofrequency Ablation for Chronic Lumbar Zygapophyseal Joint Pain Using a V-Shaped Active Tip Needle: An Observational Retrospective Study
Lo Bianco G, Misseri G, Stogicza AR, Cesare G, Li S, Day M, Kennedy DJ, Schatman ME
Journal of Pain Research 2023, 16:1243-1255
Published Date: 11 April 2023
Interventional Pain Procedures: A Narrative Review Focusing on Safety and Complications. Part 1 Injections for Spinal Pain
Lo Bianco G, Tinnirello A, Papa A, Torrano V, Russo G, Stogicza A, Mercadante S, Cortegiani A, Mazzoleni S, Schatman ME
Journal of Pain Research 2023, 16:1637-1646
Published Date: 18 May 2023
A Randomized, Double-Blind, Placebo-Controlled Trial to Evaluate the Therapeutic Effect of Magnesium-L-Threonate Supplementation for Persistent Pain After Breast Cancer Surgery
Ni Y, Deng F, Yu S, Zhang J, Zhang X, Huang D, Zhou H
Breast Cancer: Targets and Therapy 2023, 15:495-504
Published Date: 25 July 2023
Exploring Pain Clinical Specialists’ Perspectives on Opioid Optimization for Chronic Non-Malignant Pain in England
Alenezi A, Paudyal V, Yahyouche A
Journal of Pain Research 2025, 18:4037-4051
Published Date: 13 August 2025