Back to Journals » Journal of Hepatocellular Carcinoma » Volume 13
Comparable Long-Term Survival After Curative Hepatectomy for Solitary Large (5–10 cm) versus Giant (≥10 cm) Hepatocellular Carcinoma: A Retrospective Study
Authors Jiang K, Li J, Zhang D, Wang W, Chang J
Received 8 March 2026
Accepted for publication 4 June 2026
Published 8 June 2026 Volume 2026:13 607722
DOI https://doi.org/10.2147/JHC.S607722
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Toshihiro Tanaka
Kunyuan Jiang,1,* Jingfei Li,2,* Dongli Zhang,1 Weiping Wang,1 Jun Chang1
1Department of General Surgery, Kunshan Second People’s Hospital, Suzhou, Jiangsu, People’s Republic of China; 2Department of Emergency Surgery, The First Affiliated Hospital of the University of Science and Technology of China, Hefei, Anhui, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jun Chang, Department of General Surgery, Kunshan Second People’s Hospital, No. 999 Qianjin Road, Kunshan, Suzhou, Jiangsu, 215300, People’s Republic of China, Tel +86-18662547598, Email [email protected]
Purpose: This study aims to compare long-term oncological outcomes after curative hepatectomy in patients with solitary large versus giant HCC.
Patients and Methods: This dual-center study included 281 patients with solitary HCC ≥ 5 cm undergoing R0 hepatectomy, stratified into large (5– 10 cm) and giant (≥ 10 cm) cohorts. 1:1 PSM matched potential confounding variables. Primary endpoint was recurrence-free survival (RFS), analyzed through Kaplan-Meier methods with Log rank testing.
Results: At baseline, giant HCC (n=90) patients exhibited significantly higher rates of AFP ≥ 200 ng/mL, major hepatectomy, and intraoperative transfusion compared to large HCC (n=191) cohort. After PSM, 82 patients were allocated to each group, with all baseline characteristics well-balanced. The RFS analysis revealed comparable outcomes between large and giant HCC groups: pre-PSM median RFS, 29.6 vs 26.5 months (HR 0.864, 95% CI 0.615– 1.214, P=0.398); post-PSM median RFS, 21.1 vs 26.5 months (HR 1.128, 95% CI 0.756– 1.681, P=0.555). Median overall survival (OS) was not reached in either group.
Conclusion: Patients with solitary giant HCC amenable to upfront curative hepatectomy achieved similar RFS compared to large HCC after surgery, tumor biological characteristics (AFP levels and MVI status) are the primary determinants of postoperative prognosis in HCC patients.
Keywords: hepatectomy, hepatocellular carcinoma, tumor size, recurrence-free survival, propensity score analysis
Introduction
Hepatocellular carcinoma (HCC) represents one of the most prevalent malignancies worldwide, accounting for over 90% of primary liver cancer cases and ranking as the third leading cause of cancer-related mortality worldwide.1 Current management guidelines uniformly recognize curative hepatectomy as the cornerstone of curative treatment for solitary HCC, regardless of tumor size, as long as the tumor is resectable.2 However, even early-stage patients face 5-year recurrence rates around 70% following R0 resection, contributing to persistently poor long-term prognosis after hepatectomy.3
Tumor size is a critical determinant for both therapeutic decisions and prognostic stratification in solitary HCC. The Barcelona Clinic Liver Cancer (BCLC) staging system uses a 2-cm threshold to differentiate stage 0 (very early) from stage A (early) disease,4 while the China Liver Cancer (CNLC) staging system further stratifies solitary HCC into stage Ia (≤5 cm) and Ib (>5 cm).5 Extensive research demonstrates an inverse correlation between tumor size and postoperative survival, with patients undergoing curative hepatectomy for larger tumors (typically >5 cm) experiencing poorer long-term outcomes than those with smaller HCCs.6,7 On the other hand, microvascular invasion (MVI) has been extensively validated as the most reliable predictor for early postoperative recurrence of HCC.8,9 Tumor size is strongly associated with microvascular invasion and represents an important preoperative indicator for predicting MVI.10 This further indicates that tumor size serves as a significant prognostic factor for HCC following surgical resection.
Owing to its insidious progression, HCC is frequently diagnosed at advanced stages, with many patients presenting with tumors >5 cm at initial detection.11,12 Although modern surgical advances and optimized perioperative care have expanded resection feasibility for giant HCCs (≥10 cm), comprehensive data on long-term oncological outcomes in this subgroup remain limited.13 A meta-analysis evaluating the prognosis after surgical resection for giant HCC (≥10 cm) concluded that despite the procedure’s feasibility and safety, patients face poorer long-term survival than those with sub-10 cm tumors.14 Given the high recurrence rate after resection for giant HCC, some clinicians advocate that surgical resection should not be the first-line treatment and that preoperative neoadjuvant strategies such as TACE or systemic therapy may improve long-term outcomes.15,16 Thus, additional studies examining the long-term outcomes of surgical intervention for giant HCC are warranted.
In this study, large HCC (≥5 cm, at high risk of recurrence) was further subclassified into large HCC and giant HCC groups using a 10-cm cutoff. Long-term postoperative survival was compared between the two groups to determine whether giant tumors further enhance HCC malignancy, impair surgical outcomes, and worsen patient prognosis, thereby providing clinical evidence to guide optimal treatment selection for this patient population.
Patients and Methods
Study Population and Data Collection
We conducted a dual-center retrospective cohort study analyzing consecutive patients who underwent curative-intent hepatectomy for HCC between January 2019 and December 2022. Inclusion criteria: (1) aged 18–85 years with treatment-naive HCCs (no prior systemic therapy, transarterial chemoembolization, or ablation). (2) ECOG performance status 0–1 and Child-Pugh class A, with preserved cardiopulmonary, lung and renal function on preoperative evaluation. (3) with no radiological evidence of vascular invasion or extrahepatic tumors before surgery. (4) R0 resection achieved (microscopically negative margins, no macroscopic vascular or biliary thrombi). (5) postoperative pathologic confirmation of solitary HCC ≥ 5cm. (6) Complete clinical datasets were available, and patients were actively followed up with full access to their outcome information. Exclusion criteria: (1) had received any antitumor therapy prior to surgery or recurrent tumor after initial resection. (2) not HCC or tumor size < 5 cm. (3) Major postoperative complications (Clavien-Dindo grade ≥III) or 90-day postoperative mortality. (4) Had incomplete medical records or lost to follow-up (Figure 1).
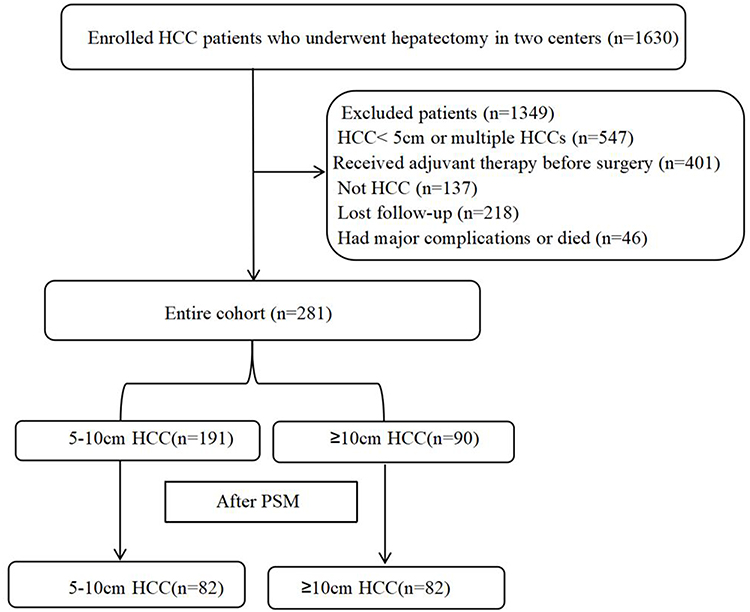 |
Figure 1 Flowchart of this study. |
Patients were stratified into two cohorts based on maximal tumor diameter: large HCC group (LH, 5–10 cm) and giant HCC group (GH, ≥10 cm).
Surgical Procedure and Definition
All patients underwent standardized preoperative assessment to confirm surgical candidacy. Absolute contraindications (including extrahepatic metastasis, unresectable vascular invasion, or inadequate future liver remnant) were systematically excluded. Following detailed patient counseling, written informed consent was obtained for either laparoscopic or open hepatectomy approaches. Curative-intent resection was performed by fellowship-trained hepatobiliary surgeons (minimum 5 years of subspecialty experience). The specific surgical approach (laparoscopic or open), surgical margin, and extent of hepatectomy were determined comprehensively by the surgical team based on preoperative imaging, tumor location and size, severity of liver cirrhosis, and intraoperative findings. All patients received standard perioperative care including liver protection, choleresis, and nutritional support. No major postoperative complications (Clavien–Dindo grade ≥ III) occurred in any included patients. All patients were discharged after postoperative examinations confirmed normal inflammatory markers, liver and renal function, coagulation tests, and unremarkable abdominal CT findings, followed by successful removal of abdominal drainage tubes.
Major liver resection was defined as the removal of ≥4 Couinaud’s segments17 and was considered if the remaining liver function was expected to be sufficient, as evaluated by three-phase-enhanced computed tomography (CT).
Outcome Endpoints and Follow Up
All clinical data were prospectively collected, with follow-up performed through regular outpatient visits and telephone contacts until tumor recurrence or last contact. Follow-up assessments systematically recorded recurrence status, time to recurrence, recurrence patterns, and survival outcomes. The primary endpoint was recurrence-free survival (RFS), defined as the interval from radical surgery to radiologically confirmed HCC recurrence. Secondary endpoints included overall survival (OS) and extrahepatic recurrence rate (ERR). Tumor recurrence was strictly diagnosed when recurrent lesions were verified by at least one of the following imaging modalities: contrast-enhanced ultrasound, contrast-enhanced CT, or contrast-enhanced MRI. All enrolled patients were followed until either an endpoint event occurred or a minimum follow-up duration of 24 months was achieved.
Statistical Analysis
Statistical analyses were performed using SPSS version 26.0 and the R software environment (version 4.1.1; available at https://www.r-project.org/). All baseline characteristics potentially associated with early recurrence, including age, sex, BMI, albumin level, HBsAg status, AFP level, liver cirrhosis, Pringle maneuver application, intraoperative transfusion, tumor differentiation grade, and microvascular invasion (MVI), were systematically compared between the 5–10 cm and ≥10 cm groups. To minimize selection bias, we performed 1:1 propensity score matching (PSM) with a caliper width of 0.02 to balance these variables between the two groups. Categorical variables were analyzed using chi-square tests. Survival outcomes were evaluated using the Kaplan-Meier method with between-group comparisons performed via Log rank tests. All potential prognostic factors for recurrence-free survival (RFS) were incorporated into Cox proportional hazards regression models. Variables demonstrating a P value <0.1 in univariate analysis were subsequently included in multivariate analysis to calculate adjusted hazard ratios (HRs) with corresponding 95% confidence intervals (CIs). A two-sided P value <0.05 was considered statistically significant for all analyses.
Results
Patients and Baseline Characteristics
Between January 2019 and December 2022, 281 consecutive HCC patients meeting the study criteria were enrolled, consisting of 234 males (83.3%) and 47 females (16.7%), with a median age of 57 years (range: 22–83 years). The cohort included 191 patients with 5–10 cm HCC and 90 patients with ≥10 cm HCC. Propensity score matching yielded 82 well-balanced pairs from each group for comparative analysis. Prior to matching, the ≥10 cm group demonstrated significantly higher rates of AFP ≥200 ng/mL, major hepatectomy, and intraoperative transfusion compared to the 5–10 cm group (all P<0.05). Following PSM, all baseline characteristics showed comparable distributions between groups (all P>0.05), confirming effective matching.(Table 1).
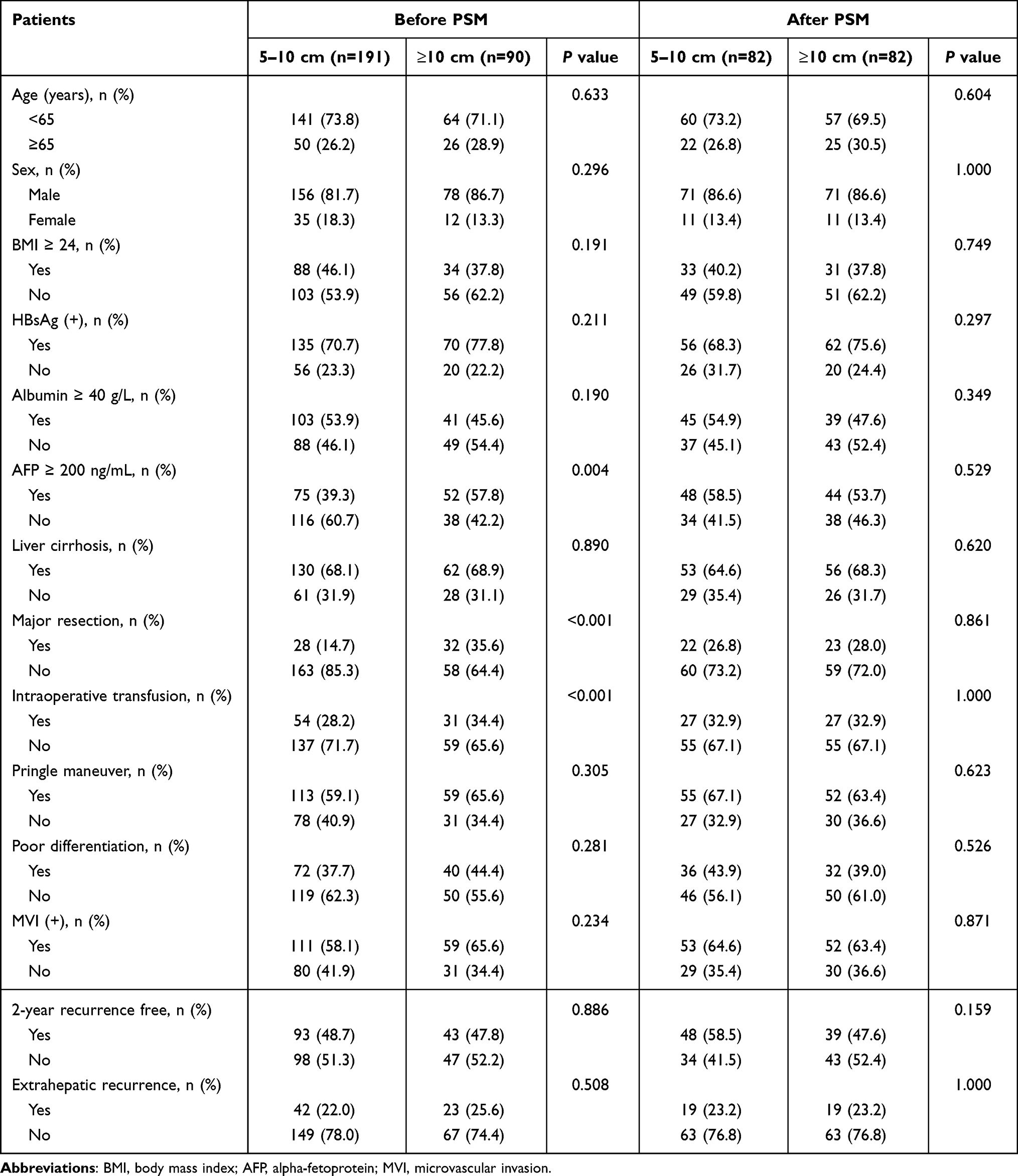 |
Table 1 Baseline Demographic and Disease Characteristics Before and After PSM |
Survival Outcomes Before and After PSM
The median follow-up time was 35.3 months. Before PSM, the extrahepatic recurrence rates (ERR) were 22.0% (42/191) in the 5–10 cm HCC group versus 25.6% (23/90) in the ≥10 cm HCC group (P=0.508). The median RFS was 29.6 months (95% CI: 15.6–44.0) for LH group compared to 26.5 months (95% CI: 12.0–41.0) for GH group (HR=0.864; 95% CI: 0.615–1.214; P=0.398) (Figure 2a). Following PSM, both groups demonstrated identical ERR rates of 23.2% (19/82). The median RFS post-matching was 21.1 months (95% CI: 15.6–26.5) for LH group and 26.5 months (95% CI: 13.0–39.9) for GH group (HR=1.128; 95% CI: 0.756–1.681; P=0.555) (Figure 3a). Median overall survival was not reached in either group before (P=0.765) or after (P=0.228) matching (Figures 2b and 3b).
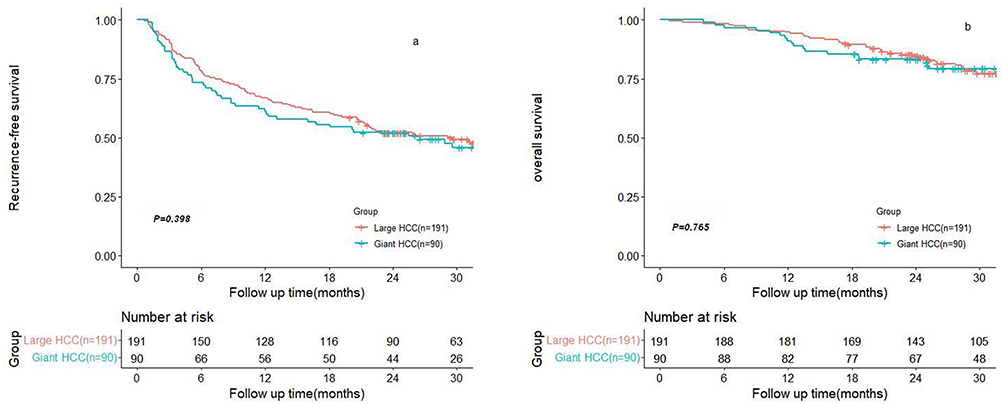 |
Figure 2 Kaplan-Meier analysis of RFS (a) and OS (b) before PSM. |
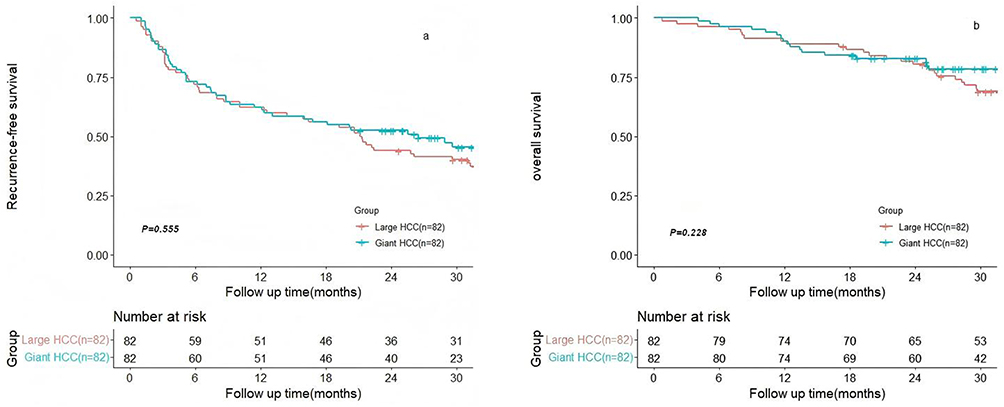 |
Figure 3 Kaplan-Meier analysis of RFS (a) and OS (b) after PSM. |
Univariate Cox regression analysis of the entire cohort revealed that age <65 years, albumin <40 g/L, AFP ≥200 ng/mL, major resection, poor differentiation, and MVI positivity were all significantly associated with increased recurrence risk (all P<0.1). Multivariate analysis identified three independent prognostic factors for HCC recurrence: MVI negativity (HR 0.347, 95% CI 0.235–0.512, P<0.001), AFP <200 ng/mL (HR 0.581, 95% CI 0.415–0.812, P=0.001), and age <65 years (HR 1.605, 95% CI 1.085–2.374, P=0.018). In the PSM cohort, Cox regression analysis confirmed the persistent predictive value of these three factors: MVI negativity (HR 0.354, 95% CI 0.220–0.568, P<0.001), AFP <200 ng/mL (HR 0.512, 95% CI 0.334–0.786, P=0.002), and age <65 years (HR 2.120, 95% CI 1.303–3.450, P=0.002) for RFS (Table 2).
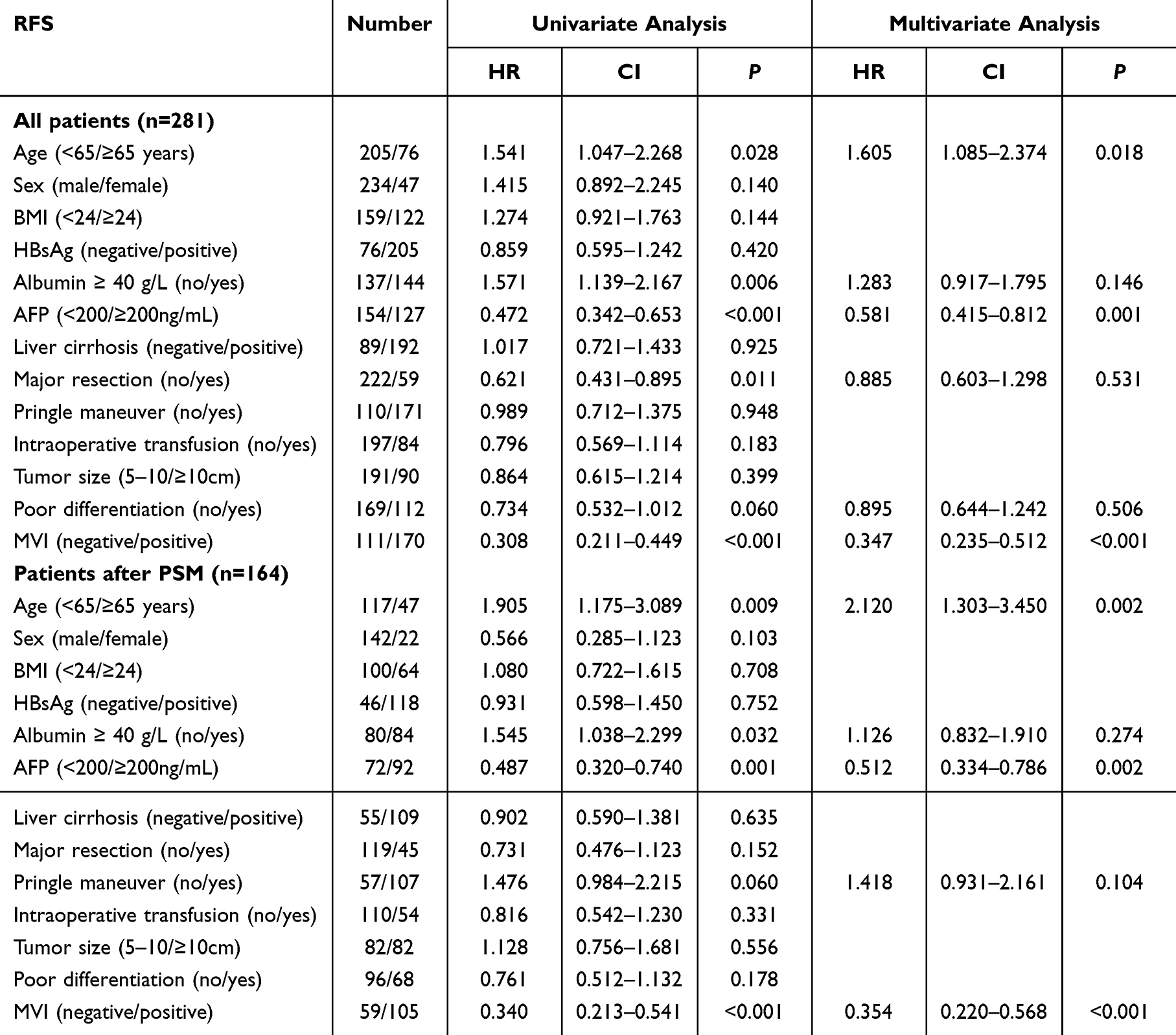 |
Table 2 Univariate and Multivariate Analysis for RFS in Patients with HCC ≥ 5 cm |
Discussion
Surgical resection remains the recommended treatment for solitary hepatocellular carcinoma (HCC), regardless of tumor size; however, prognosis varies significantly with tumor dimensions. Most current studies consider tumor size >5 cm as a risk factor for HCC recurrence.18,19 This study revealed comparable 2-year recurrence rates between patients with tumors 5–10 cm and those with tumors ≥10 cm (48.7% vs 47.8%), also demonstrating the aggressive biological behavior and high early recurrence propensity of HCCs ≥5 cm following curative hepatectomy.
The observed discrepancy between technical resectability and biological curability highlights the critical need for refined prognostic stratification beyond the 5 cm threshold. Zhang et al20 demonstrated that tumor size remains a significant prognostic determinant even after stratifying small HCCs (<5 cm). Similarly, tumor size variations likely correlate with distinct outcomes within the large HCC category (>5 cm). Notably, for solitary HCCs ≥10 cm, existing literature primarily focuses on surgical safety and short-term complications; comprehensive data on long-term oncological outcomes remain limited and warrant systematic investigation. To address this gap and further explore the impact of tumor size within large HCCs, this study stratified patients with HCC ≥5 cm into subgroups (5–10 cm vs ≥10 cm) for detailed analysis of postoperative outcomes.
The biological aggressiveness of HCC typically correlates with tumor size, where larger lesions often demonstrate more advanced malignant behavior and necessitate wider resection margins to achieve R0 status. This established association between tumor dimensions and surgical complexity was evident in our pre-matched cohort: patients with HCC ≥10 cm demonstrated significantly higher rates of AFP ≥200 ng/mL, major hepatectomy, and intraoperative transfusion requirements compared to those with tumors measuring 5–10 cm. These clinically significant baseline differences were effectively balanced through PSM, resulting in well-matched cohorts with no significant differences in baseline characteristics (all P>0.05).
Both Kaplan-Meier survival analysis and multivariable Cox regression demonstrated no statistically significant difference in RFS between LH group and GH group. Furthermore, comparative analysis of recurrence patterns revealed no significant differences between the two cohorts. Collectively, these findings demonstrate that tumor size does not serve as an independent prognostic factor for HCC ≥5 cm following curative hepatectomy. Our findings are consistent with existing literature, including Ariizumi et al21 who reported favorable surgical outcomes for solitary HCC ≥10 cm without macrovascular invasion. Similarly, Levi Sandri et al22 found tumor size did not significantly affect long-term survival, though it was associated with prolonged postoperative hospitalization.
Early postoperative recurrence (occurring within 2 years) remains the most critical determinant of long-term prognosis for HCC patients undergoing curative hepatectomy.23 The prevailing understanding attributes this early recurrence primarily to occult micrometastases, undetectable by preoperative imaging or intraoperative evaluation. These residual microscopic tumor deposits are strongly associated with the intrinsic biological aggressiveness of the primary tumor. While numerous investigations have sought to establish reliable predictors of recurrence, significant interstudy variability persists - a phenomenon likely reflecting differences in patient populations and surgical selection criteria across institutions.24–26
In this study, multivariate Cox regression analysis identified MVI positivity and AFP ≥200 ng/mL as independent negative prognostic factors for recurrence-free survival (all P<0.05). These findings align with established literature, where both MVI and elevated AFP levels have been consistently validated as robust predictors of postoperative recurrence.25–27 It is noteworthy that our study identified younger age as a high-risk factor for recurrence after HCC resection, a finding less commonly reported in the literature.28–30 Conventionally, younger patients are often considered to have better hepatic functional reserve, which is typically associated with a more favorable prognosis. We postulate that this observed association may stem from the fact that younger patients possess more abundant hepatic blood supply and greater regenerative capacity. This enhanced microenvironment could potentially promote the growth and metastasis of residual microscopic tumor deposits. Furthermore, the inclusion of only large HCCs (≥5 cm) in our cohort may further increase this risk. This hypothesis—that postoperative recurrence is jointly determined by both tumor biological aggressiveness and postoperative hepatic functional reserve—may also explain the conflicting results regarding adjuvant TACE across different clinical studies. Specifically, the varying efficacy of TACE in eradicating occult micrometastases versus its detrimental impact on hepatic function among distinct patient subpopulations.31–34 Future efforts to refine patient selection for adjuvant therapy and develop regimens with optimized efficacy-toxicity profiles hold promise for reducing postoperative recurrence.
This study has several limitations that should be acknowledged. First, as a retrospective study, although PSM was rigorously applied to control for intergroup variables, certain potentially outcome-influencing factors—such as surgical margin —were not incorporated. This omission may exert an impact on the results.35,36 Second, longer follow-up is warranted to fully evaluate long-term survival outcomes, particularly for OS. Moreover, the sample size in this study is relatively small, particularly the matched sample size. Future studies incorporating standardized follow-up protocols, detailed tumor molecular profiling, and comprehensive liver function assessments would provide more definitive evidence regarding the prognostic significance of tumor size in HCC.
Conclusion
Our study reveals that postoperative RFS are comparable between solitary large HCCs (5–10 cm) and giant HCCs (≥10 cm) who are eligible for upfront curative resection, indicating that tumor size alone is not an independent prognostic factor for solitary HCC ≥5 cm after curative resection. Tumor biological characteristics (AFP levels and MVI status) are the primary determinants of postoperative prognosis in HCC patients. These findings suggest that surgical decision-making for solitary large HCC should integrate comprehensive tumor biological characteristics rather than overemphasizing tumor size. However, these conclusions are limited to selected patients eligible for curative resection and should be validated in future prospective studies with larger sample sizes and longer follow-up for overall survival.
Abbreviations
HCC, hepatocellular carcinoma; BCLC, The Barcelona Clinic Liver Cancer; CNLC, the China Liver Cancer; ECOG, Eastern Cooperative Oncology Group; CT, computed tomography; RFS, recurrence-free survival; OS, overall survival; ERR, extrahepatic recurrence rate; AFP, alpha-Fetoprotein; MVI, microvascular invasion; PSM, propensity score matching; TACE, transarterial chemoembolization.
Data Sharing Statement
Dataset available from the corresponding author at [email protected].
Ethics Approval Statement and Informed Consent
This study was reviewed and approved by the Ethics Committee of the First Affiliated Hospital of the University of Science and Technology of China (ID:2025-RE-371) and Kunshan Second People’s Hospital (ID: ksehllsp 2025-008).
Informed Consent Statement
Patients were not required to give informed consent to the study because the analysis used anonymous clinical data that were obtained after each patient agreed to treatment by written consent.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hwang SY, Danpanichkul P, Agopian V, et al. Hepatocellular carcinoma: updates on epidemiology, surveillance, diagnosis and treatment. Clin Mol Hepatol. 2025;31(Suppl):S228–10. doi:10.3350/cmh.2024.0824
2. Brown ZJ, Tsilimigras DI, Ruff SM, et al. Management of hepatocellular carcinoma: a review. JAMA Surg. 2023;158(4):410–420. doi:10.1001/jamasurg.2022.7989
3. Gentile D, Donadon M, Lleo A, et al. Surgical treatment of hepatocholangiocarcinoma: a systematic review. Liver Cancer. 2020;9(1):15–27. doi:10.1159/000503719
4. Reig M, Forner A, Rimola J, et al. BCLC strategy for prognosis prediction and treatment recommendation: the 2022 update. J Hepatol. 2022;76(3):681–693. doi:10.1016/j.jhep.2021.11.018
5. Xie DY, Zhu K, Ren ZG, Zhou J, Fan J, Gao Q. A review of 2022 Chinese clinical guidelines on the management of hepatocellular carcinoma: updates and insights. Hepatobiliary Surg Nutr. 2023;12(2):216–228. doi:10.21037/hbsn-22-469
6. Xie QS, Chen ZX, Zhao YJ, Gu H, Geng XP, Liu FB. Systematic review of outcomes and meta-analysis of risk factors for prognosis after liver resection for hepatocellular carcinoma without cirrhosis. Asian J Surg. 2021;44(1):36–45. doi:10.1016/j.asjsur.2020.08.019
7. Liang BY, Gu J, Xiong M, et al. Tumor size may influence the prognosis of solitary hepatocellular carcinoma patients with cirrhosis and without macrovascular invasion after hepatectomy. Sci Rep. 2021;11(1):16343. doi:10.1038/s41598-021-95835-5
8. Wang W, Guo Y, Zhong J, et al. The clinical significance of microvascular invasion in the surgical planning and postoperative sequential treatment in hepatocellular carcinoma. Sci Rep. 2021;11(1):2415. doi:10.1038/s41598-021-82058-x
9. Lee S, Kang TW, Song KD, et al. Effect of microvascular invasion risk on early recurrence of hepatocellular carcinoma after surgery and radiofrequency ablation. Ann Surg. 2021;273(3):564–571. doi:10.1097/sla.0000000000003268
10. Wang Q, Zhou Y, Yang H, Zhang J, Zeng X, Tan Y. MRI-based clinical-radiomics nomogram model for predicting microvascular invasion in hepatocellular carcinoma. Med Phys. 2024;51(7):4673–4686. doi:10.1002/mp.17087
11. Singal AG, Kanwal F, Llovet JM. Global trends in hepatocellular carcinoma epidemiology: implications for screening, prevention and therapy. Nat Rev Clin Oncol. 2023;20(12):864–884. doi:10.1038/s41571-023-00825-3
12. Department of Medical Administration, National Health and Health Commission of the People’s Republic of China. [Guidelines for diagnosis and treatment of primary liver cancer in China (2019 edition)]. Zhonghua Gan Zang Bing Za Zhi. 2020;28(2):112–128. Chinese. doi:10.3760/cma.j.issn.1007-3418.2020.02.004
13. Liu D, Song T. Changes in and challenges regarding the surgical treatment of hepatocellular carcinoma in China. Biosci Trends. 2021;15(3):142–147. doi:10.5582/bst.2021.01083
14. Lee AJ, Wu AG, Yew KC, Shelat VG. Does size matter for resection of giant versus non-giant hepatocellular carcinoma? A meta-analysis. World J Gastrointest Surg. 2023;15(2):273–286. doi:10.4240/wjgs.v15.i2.273
15. Personeni N, Rimassa L. Exploring novel avenues for neoadjuvant treatment of hepatocellular carcinoma. Lancet Gastroenterol Hepatol. 2022;7(3):198–199. doi:10.1016/s2468-1253(21)00462-3
16. Wei X, Jiang Y, Zhang X, et al. Neoadjuvant three-dimensional conformal radiotherapy for resectable hepatocellular carcinoma with portal vein tumor thrombus: a randomized, open-label, multicenter controlled study. J Clin Oncol. 2019;37(24):2141–2151. doi:10.1200/jco.18.02184
17. Germain T, Favelier S, Cercueil JP, Denys A, Krausé D, Guiu B. Liver segmentation: practical tips. Diagn Interv Imaging. 2014;95(11):1003–1016. doi:10.1016/j.diii.2013.11.004
18. Hwang S, Lee YJ, Kim KH, et al. The impact of tumor size on long-term survival outcomes after resection of solitary hepatocellular carcinoma: single-institution experience with 2558 patients. J Gastrointest Surg. 2015;19(7):1281–1290. doi:10.1007/s11605-015-2849-5
19. Bi X, Zhao H, Zhao H, et al. Consensus of chinese experts on neoadjuvant and conversion therapies for hepatocellular carcinoma: 2023 update. Liver Cancer. 2025;14(2):223–238. doi:10.1159/000541249
20. Zhang W, Wang X, Jiang R, et al. Effect of tumor size on cancer-specific survival in small hepatocellular carcinoma. Mayo Clin Proc. 2015;90(9):1187–1195. doi:10.1016/j.mayocp.2015.06.018
21. Ariizumi S, Kotera Y, Takahashi Y, Katagiri S, Yamamoto M. Impact of hepatectomy for huge solitary hepatocellular carcinoma. J Surg Oncol. 2013;107(4):408–413. doi:10.1002/jso.23226
22. Levi Sandri GB, Spoletini G, Vennarecci G, Francone E, Abu Hilal M, Ettorre GM. Laparoscopic liver resection for large HCC: short- and long-term outcomes in relation to tumor size. Surg Endosc. 2018;32(12):4772–4779. doi:10.1007/s00464-018-6225-x
23. Wang MD, Li C, Liang L, et al. Early and late recurrence of Hepatitis B virus-associated hepatocellular carcinoma. Oncologist. 2020;25(10):e1541–e51. doi:10.1634/theoncologist.2019-0944
24. He Y, Luo L, Shan R, et al. Development and validation of a nomogram for predicting postoperative early relapse and survival in hepatocellular carcinoma. J Natl Compr Canc Netw. 2023;22(1d):e237069. doi:10.6004/jnccn.2023.7069
25. Fuster-Anglada C, Mauro E, Ferrer-Fàbrega J, et al. Histological predictors of aggressive recurrence of hepatocellular carcinoma after liver resection. J Hepatol. 2024;81(6):995–1004. doi:10.1016/j.jhep.2024.06.018
26. Norman JS, Li PJ, Kotwani P, Shui AM, Yao F, Mehta N. AFP-L3 and DCP strongly predict early hepatocellular carcinoma recurrence after liver transplantation. J Hepatol. 2023;79(6):1469–1477. doi:10.1016/j.jhep.2023.08.020
27. Lv K, Cao X, Du P, Fu JY, Geng DY, Zhang J. Radiomics for the detection of microvascular invasion in hepatocellular carcinoma. World J Gastroenterol. 2022;28(20):2176–2183. doi:10.3748/wjg.v28.i20.2176
28. Nevola R, Ruocco R, Criscuolo L, et al. Predictors of early and late hepatocellular carcinoma recurrence. World J Gastroenterol. 2023;29(8):1243–1260. doi:10.3748/wjg.v29.i8.1243
29. Lu YX, Zhao JP, Yuan GD, et al. Prevalence, patterns, risk factors and outcomes of peritoneal metastases after laparoscopic hepatectomy for hepatocellular carcinoma: a multicenter study from China. Hepatobiliary Surg Nutr. 2024;13(1):3–15. doi:10.21037/hbsn-22-506
30. He Y, Qian J, Zhu G, et al. Development and validation of nomograms to evaluate the survival outcome of HCC patients undergoing selective postoperative adjuvant TACE. Radiol Med. 2024;129(4):653–664. doi:10.1007/s11547-024-01792-0
31. Su JY, Huang DJ, Liu SP, et al. Adjuvant transarterial chemoembolization after truly curative resection does not improve survival of patients with hepatocellular carcinoma at high risk of recurrence: a target trial emulation study. Hepatol Res. 2025;55(9):1263–1273. doi:10.1111/hepr.14219
32. Ma T, Bai X, Zhang Q, et al. Adjuvant transarterial chemoembolization for hepatocellular carcinoma following curative resection: a randomized, open-label, Phase 3 trial. Hepatology. 2025. doi:10.1097/hep.0000000000001233
33. Wang Z, Ren Z, Chen Y, et al. Adjuvant transarterial chemoembolization for HBV-related hepatocellular carcinoma after resection: a randomized controlled study. Clin Cancer Res. 2018;24(9):2074–2081. doi:10.1158/1078-0432.Ccr-17-2899
34. Li SH, Mei J, Cheng Y, et al. Postoperative adjuvant hepatic arterial infusion chemotherapy with FOLFOX in hepatocellular carcinoma with microvascular invasion: a multicenter, Phase III, randomized study. J Clin Oncol. 2023;41(10):1898–1908. doi:10.1200/jco.22.01142
35. Zhang XP, Xu S, Lin ZY, et al. Significance of anatomical resection and resection margin status in patients with HBV-related hepatocellular carcinoma and microvascular invasion: a multicenter propensity score-matched study. Int J Surg. 2023;109(4):679–688. doi:10.1097/js9.0000000000000204
36. Yang S, Ni H, Zhang A, Zhang J, Zang H, Ming Z. Significance of anatomical resection and wide surgical margin for HCC patients with MVI undergoing laparoscopic hepatectomy: a multicenter study. Eur J Surg Oncol. 2025;51(1):109353. doi:10.1016/j.ejso.2024.109353
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Histological Severity of Cirrhosis Influences Surgical Outcomes of Hepatocellular Carcinoma After Curative Hepatectomy
Liang BY, Gu J, Xiong M, Zhang EL, Zhang ZY, Lau WY, Wang SF, Guan Y, Chen XP, Huang ZY
Journal of Hepatocellular Carcinoma 2022, 9:633-647
Published Date: 23 July 2022
Predictive Value of Preoperative Serum AFP, CEA, and CA19-9 Levels in Patients with Single Small Hepatocellular Carcinoma: Retrospective Study
Gan L, Ren S, Lang M, Li G, Fang F, Chen L, Liu Y, Han R, Zhu K, Song T
Journal of Hepatocellular Carcinoma 2022, 9:799-810
Published Date: 13 August 2022
Nomogram Based on Inflammatory Biomarkers to Predict the Recurrence of Hepatocellular Carcinoma—A Multicentre Experience
Zheng Z, Guan R, Zou Y, Jian Z, Lin Y, Guo R, Jin H
Journal of Inflammation Research 2022, 15:5089-5102
Published Date: 5 September 2022
Prognostic Value of Red Blood Cell Distribution Width (RDW) in the Recurrence of Hepatocellular Carcinoma Following Curative Resection
Golriz M, Ramouz A, Ali-Hasan-Al-Saegh S, Shafiei S, Aminizadeh E, Hammad A, Mieth M, Rupp C, Springfeld C, Hoffmann K, Büchler M, Mehrabi A
Journal of Hepatocellular Carcinoma 2022, 9:1137-1147
Published Date: 31 October 2022
Postoperative Adjuvant Transcatheterarterial Chemoembolization Should Be Considered Selectively for Patients with Cytokeratin-19 Positive Hepatocellular Carcinoma
Mai RY, Tao Z, Huang HY, Zeng C, Mo KX, Zeng DD, Liang R, Lin Y, Wang XB, Bai T, Li LQ, Ye JZ, Wu GB
Journal of Hepatocellular Carcinoma 2025, 12:2407-2419
Published Date: 27 October 2025