Back to Journals » Cancer Management and Research » Volume 18

Post-IMvigor011 Era: CtDNA-Guided Postoperative Adjuvant Treatment Stratification in Muscle-Invasive Bladder Cancer
Authors Sui J, Chen Y, Jiang Y, He Q, Guo X
Received 17 March 2026
Accepted for publication 26 June 2026
Published 10 July 2026 Volume 2026:18 609903
DOI https://doi.org/10.2147/CMAR.S609903
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Giuseppe Colloca
Jie Sui,1,* Yunfan Chen,2,* Yu Jiang,2 Qiyu He,3 Xiping Guo4
1Department of Geratology, The First Hospital of China Medical University, Shenyang, Liaoning, People’s Republic of China; 2Department of Urology, The First Hospital of China Medical University, Shenyang, Liaoning, People’s Republic of China; 3Emergency Department, The First Hospital of China Medical University, Shenyang, Liaoning, People’s Republic of China; 4Department of Pancreatic-Biliary Surgery, The First Hospital of China Medical University, Shenyang, Liaoning, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiping Guo, Department of Pancreatic-Biliary Surgery, The First Hospital of China Medical University, No. 155 Nanjing North Street, Heping District, Shenyang, Liaoning, 110001, People’s Republic of China, Email [email protected]
Abstract: Muscle-invasive bladder cancer (MIBC) remains characterized by substantial postoperative heterogeneity after radical cystectomy, and conventional pathology and imaging incompletely identify patients with biologically active residual disease. Circulating tumor DNA (ctDNA) has emerged as the most clinically advanced liquid-biopsy marker of molecular residual disease (MRD) in this setting because it can detect recurrence before radiographic progression and, more importantly, can now inform postoperative treatment selection. The Phase III IMvigor011 trial provided the first prospective randomized evidence that ctDNA-guided adjuvant atezolizumab improves disease-free and overall survival in patients who become ctDNA-positive after cystectomy, thereby establishing molecular relapse as an actionable postoperative state rather than a merely prognostic observation. By contrast, the favorable outcomes observed in persistently ctDNA-negative patients support surveillance-based de-escalation but do not yet constitute randomized proof that adjuvant therapy can be safely omitted. In this review, we examine how the field evolved from early prognostic studies to biomarker-directed intervention, synthesize the distinct clinical logics of escalation and de-escalation, and analyze the remaining barriers to implementation, including assay selection, sampling kinetics, false-negative risk, clonal hematopoiesis of indeterminate potential (CHIP) interference, pre-analytical control, and economic feasibility. We also discuss how emerging data from TOMBOLA, MODERN, and complementary plasma/urine multi-analyte approaches may determine whether ctDNA-guided management matures from selective escalation into a broader risk-adapted postoperative strategy. The central challenge in the post-IMvigor011 era is therefore no longer whether ctDNA is clinically relevant, but how to integrate it rigorously, reproducibly, and contextually into contemporary perioperative MIBC care.
Keywords: circulating tumor DNA, minimal residual disease, muscle-invasive bladder cancer, adjuvant immunotherapy, atezolizumab, treatment escalation, treatment de-escalation, molecular residual disease, IMvigor011, liquid biopsy
Introduction
For localized muscle-invasive bladder cancer (MIBC), radical cystectomy with bilateral pelvic lymph node dissection remains the cornerstone local treatment, and cisplatin-based neoadjuvant chemotherapy is the standard perioperative approach for patients who are eligible for cisplatin.1 Despite curative-intent surgery, postoperative recurrence remains a major clinical burden. In a large radical cystectomy series, 5-year recurrence-free survival was approximately 68% overall and was markedly lower among patients with extravesical extension or nodal involvement, indicating that a substantial proportion of patients relapse despite definitive local treatment.2 This recurrence burden highlights the likelihood that some patients harbor biologically active residual disease that is not captured by routine postoperative imaging or conventional pathological risk assessment. Long-term outcomes are therefore strongly conditioned by pathological stage and nodal status; patients with organ-confined node-negative disease fare substantially better than those with extravesical extension or nodal involvement, underscoring the persistent heterogeneity that remains hidden within conventional clinicopathological risk groups.1,2
The adjuvant treatment landscape for MIBC has changed substantially since CheckMate 274 demonstrated a disease-free survival benefit for nivolumab in patients at high risk of recurrence after radical surgery.3 However, postoperative treatment allocation is still driven mainly by pathological and clinical risk features rather than direct evidence of molecular residual disease. In practice, adjuvant cisplatin-based chemotherapy is generally relevant only for patients who remain cisplatin-eligible and who did not already receive prior neoadjuvant cisplatin, whereas adjuvant immunotherapy is applied largely according to clinicopathological high-risk criteria.1,3 This framework can plausibly lead to undertreatment of some patients with occult molecular residual disease and overtreatment of others. The phase III IMvigor010 trial of adjuvant atezolizumab versus observation in unselected high-risk patients failed to demonstrate a disease-free survival benefit in the intention-to-treat population, whereas AMBASSADOR showed a significant disease-free survival benefit with adjuvant pembrolizumab, with overall survival still immature. Together, these data sharpen the question of whether pathology-only selection is the optimal framework for postoperative treatment allocation in this disease.4,5
Current postoperative surveillance in MIBC remains fundamentally reactive: imaging identifies recurrence only after macroscopic disease has emerged. In this setting, molecular residual disease (MRD) refers to biologically active residual tumor burden that persists after curative-intent treatment but remains below the detection threshold of conventional imaging or clinical assessment. Blood-based MRD assays therefore seek to identify residual disease earlier in its natural history. Circulating tumor DNA (ctDNA) is particularly attractive because the rapid turnover of plasma cell-free DNA allows near-real-time molecular assessment of tumor burden, treatment response, and relapse risk.6 Early MIBC data also extended this rationale to urine-based monitoring: Patel et al reported that tumor-derived DNA signals in plasma and urine were associated with clinical outcomes, supporting liquid-biopsy approaches as early tools for treatment-response and relapse-risk assessment in MIBC7 Subsequent urothelial carcinoma studies showed that postoperative ctDNA positivity is strongly associated with recurrence and that ctDNA detection can precede radiographic relapse by several weeks to months.8,9 This prognostic framework was later advanced by IMvigor011, a phase III ctDNA-guided adjuvant trial in which patients who became ctDNA-positive after cystectomy were randomized to atezolizumab or placebo. By demonstrating improved outcomes with ctDNA-triggered adjuvant atezolizumab, IMvigor011 repositioned molecular relapse from a surveillance finding to a therapeutically actionable postoperative state.10
The central question in the post-IMvigor011 era is no longer whether ctDNA is prognostic, but how ctDNA should be integrated with pathology, perioperative treatment context, and longitudinal surveillance to support clinically defensible postoperative decision-making in MIBC. This review therefore traces the evidentiary transition of ctDNA from an early-detection biomarker to a treatment-selection tool, reconstructs the dual clinical logic of escalation and de-escalation, and critically examines the technical, interpretive, and implementation barriers that must be resolved before ctDNA-guided postoperative management can be considered mature clinical practice. The key clinical trials and prospective studies shaping ctDNA-guided postoperative management in MIBC are summarized in Table 1. The major escalation and de-escalation scenarios, together with practical implementation challenges for ctDNA-guided postoperative care, are summarized in Table 2. The overall ctDNA-guided postoperative decision framework proposed in this review is illustrated in Figure 1.
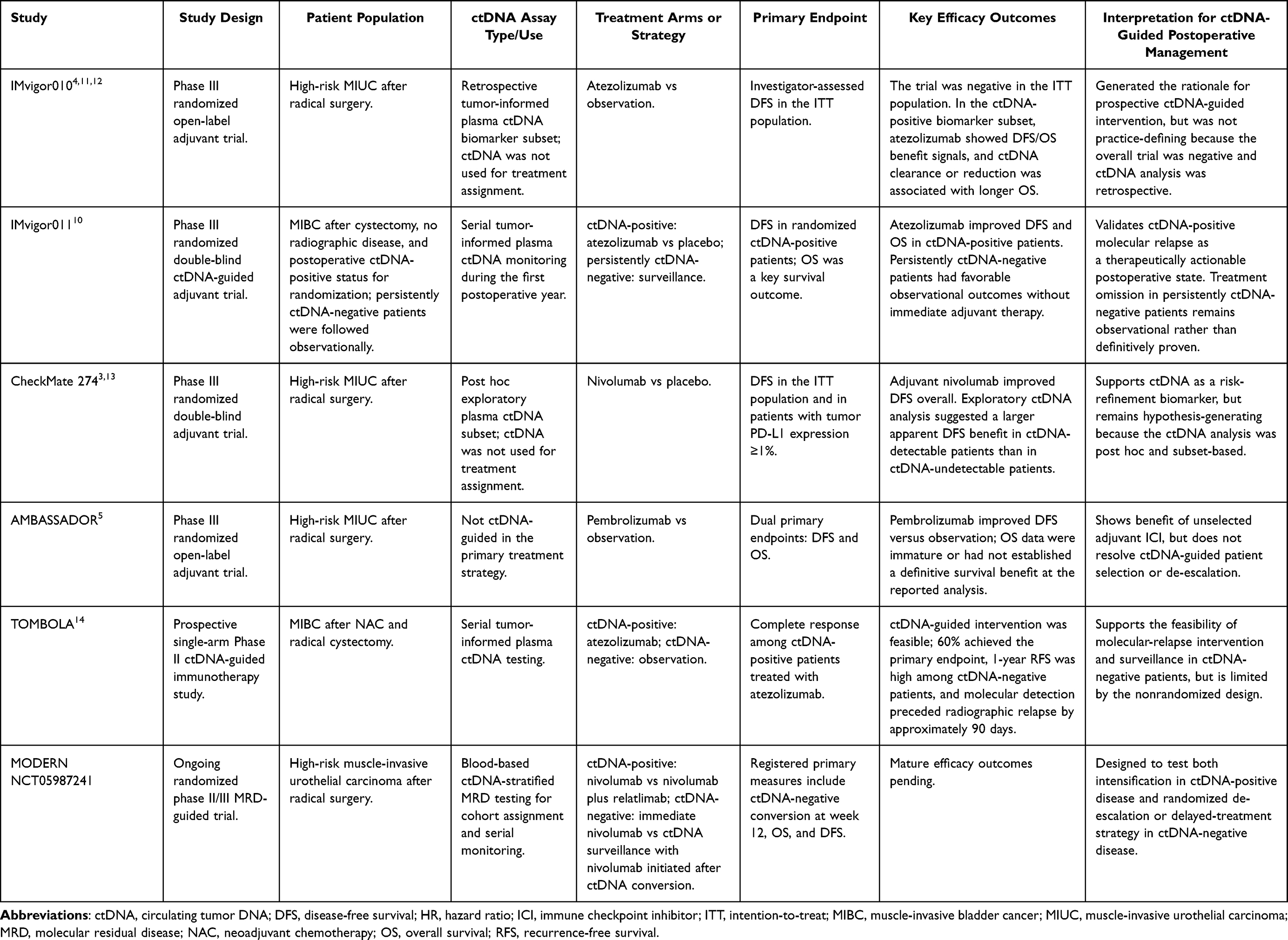 |
Table 1 Major Studies Shaping ctDNA-Guided Postoperative Management in Muscle-Invasive Bladder Cancer |
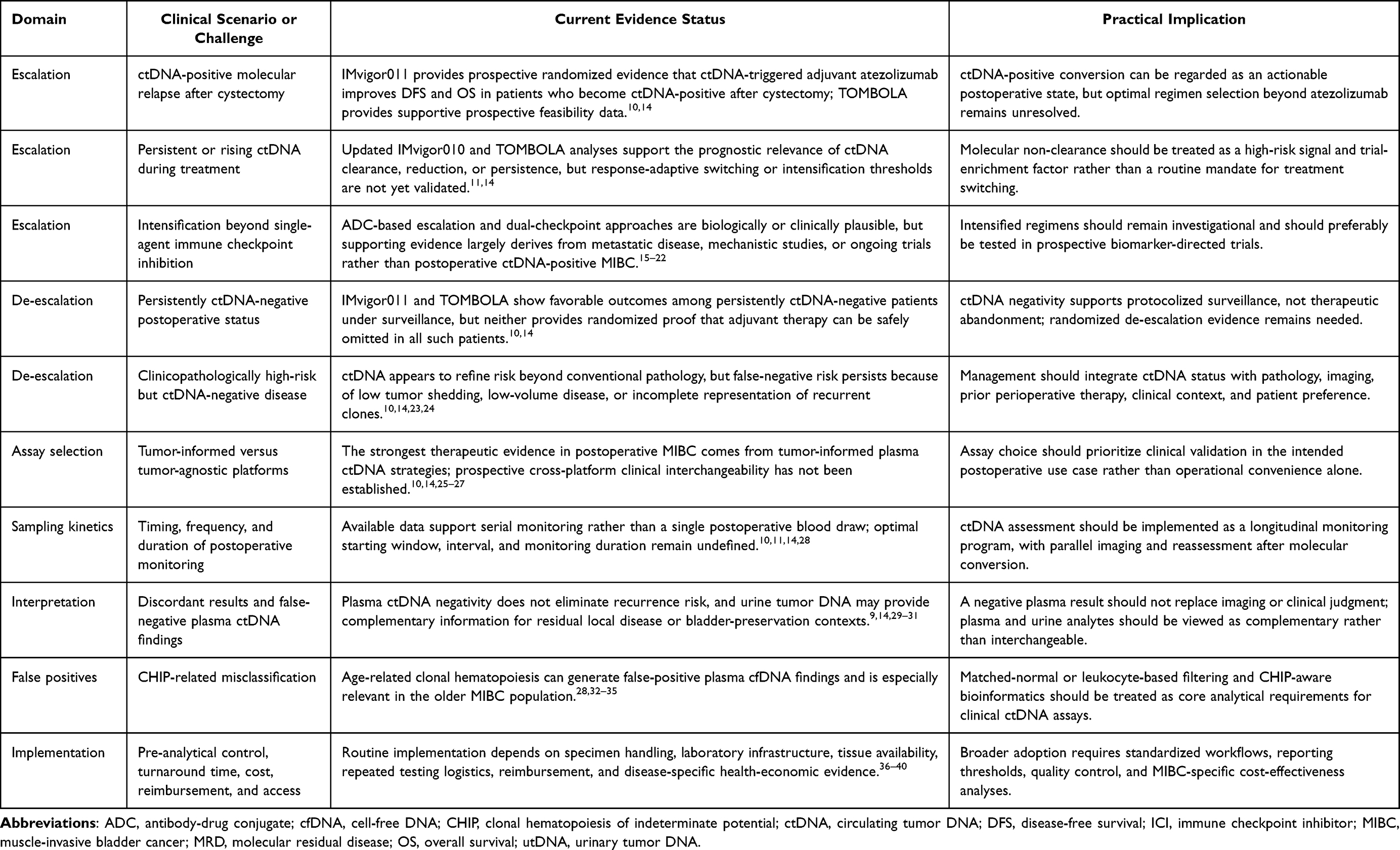 |
Table 2 Escalation, De-Escalation, and Implementation Considerations for ctDNA-Guided Postoperative Management in Muscle-Invasive Bladder Cancer |
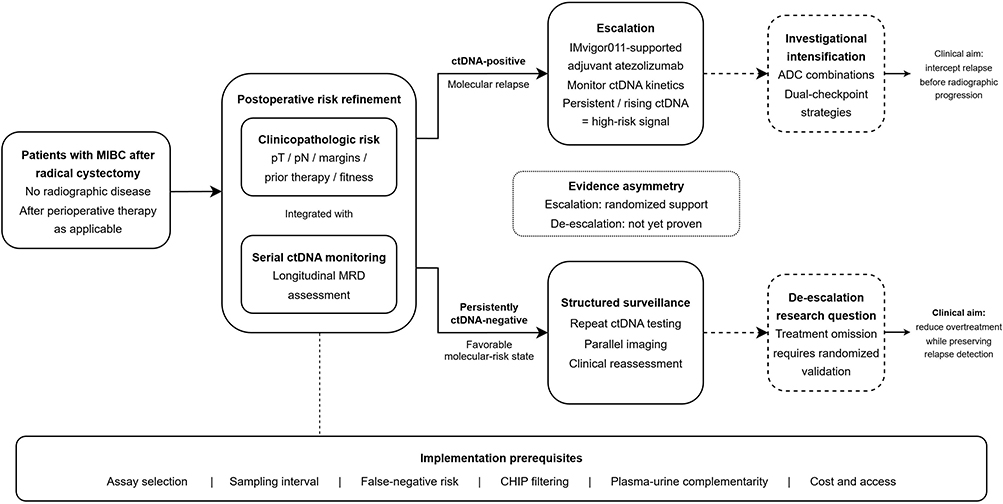 |
Figure 1 Post-IMvigor011 ctDNA-guided postoperative decision framework in muscle-invasive bladder cancer. Solid arrows indicate currently supported clinical logic, whereas dashed arrows indicate investigational or not-yet-practice-defining extensions. Abbreviations: ctDNA, circulating tumor DNA; MRD, molecular residual disease; MIBC, muscle-invasive bladder cancer; CHIP, clonal hematopoiesis of indeterminate potential; ADC, antibody–drug conjugate. |
Evolution of Evidence: From Prognostic Biomarker to Treatment-Selection Biomarker
Early Explorations: Establishing ctDNA as a Prognostic Tool in Bladder Cancer
Among the earliest prospective studies in bladder cancer, Birkenkamp-Demtröder et al showed that personalized tumor-informed ctDNA analysis could detect metastatic relapse before radiographic confirmation in patients monitored after radical cystectomy, thereby providing an early proof-of-concept for postoperative molecular relapse surveillance.41 Christensen et al subsequently extended this signal in 68 patients with localized advanced bladder cancer using ultra-deep sequencing of plasma cell-free DNA; postoperative ctDNA surveillance identified all patients who later developed metastatic relapse, with 100% sensitivity, 98% specificity, and a median lead time of 96 days over radiographic imaging.8 These observations established the early clinical validity and prognostic potential of tumor-informed ctDNA monitoring in the postoperative setting.8,41
A small exploratory study further suggested that persistent ctDNA detection during neoadjuvant chemotherapy may anticipate subsequent recurrence in MIBC, although these data should be interpreted as treatment-monitoring feasibility evidence rather than definitive validation of postoperative MRD performance.7 More recently, whole-genome tumor-informed approaches have expanded the breadth of patient-specific variant tracking and further strengthened the technical basis for highly sensitive postoperative ctDNA detection in urothelial carcinoma.42 Biologically, integrated analyses suggest that baseline ctDNA-positive tumors are enriched for the Basal/Squamous subtype and for epithelial-to-mesenchymal transition and cell cycle–associated gene sets, supporting the concept that ctDNA detectability partly reflects aggressive tumor biology.43
The IMvigor010 Inflection Point: Retrospective Rescue of a Negative Trial
In the phase III IMvigor010 trial, 809 patients with high-risk muscle-invasive urothelial carcinoma after radical surgery were randomized to adjuvant atezolizumab or observation. In the intention-to-treat population, adjuvant atezolizumab did not improve disease-free survival, and updated analyses likewise did not show an overall survival benefit in the unselected intention-to-treat population.4,11 However, an exploratory ctDNA biomarker analysis published in Nature in 2021 provided a clinically important reinterpretation of the negative trial. In a biomarker-evaluable subset of 581 of the 809 intention-to-treat patients, ctDNA testing at the start of therapy identified 214 patients (37%) as ctDNA-positive, a group with markedly worse outcomes in the observation arm.12
The prognostic value of ctDNA was striking: in the observation arm, ctDNA positivity versus negativity was associated with shorter OS (HR 6.3; 95% CI 4.3–9.3).12 In the ctDNA-positive subgroup, atezolizumab was associated with longer OS than observation (HR 0.59; 95% CI 0.42–0.83), supporting the predictive relevance of ctDNA in this exploratory analysis.11 Week-6 ctDNA clearance was more frequent with atezolizumab than with observation (18% versus 4%), and greater ctDNA reduction was associated with longer OS.12 The updated 2024 European Urology analysis further showed a graded association between the magnitude of ctDNA reduction and overall survival: 100% clearance was associated with a median OS of 60.0 months, 50–99% reduction with 34.3 months, and less than 50% reduction with 19.9 months. In the same analysis, combining C1D1 and C3D1 ctDNA status yielded higher sensitivity for relapse detection than C1D1 alone (68% versus 57%), supporting serial assessment rather than reliance on a single time point.11
These retrospective findings provided the rationale for prospectively testing ctDNA-guided adjuvant atezolizumab in IMvigor011.10
IMvigor011: The First Prospective Randomized Validation
The phase III IMvigor011 trial (NCT04660344) provides the first prospective randomized validation of ctDNA-guided adjuvant therapy in MIBC. In this global double-blind study, patients with muscle-invasive bladder cancer and no radiographic evidence of disease after cystectomy underwent serial postoperative ctDNA monitoring for up to 1 year. Patients who became ctDNA-positive during surveillance were randomly assigned in a 2:1 ratio to receive intravenous atezolizumab or placebo every 4 weeks for up to 1 year, whereas those who remained persistently ctDNA-negative did not receive blinded study treatment. The primary end point was investigator-assessed disease-free survival, and overall survival was assessed hierarchically as a key secondary end point.10
Among 761 enrolled patients, 250 ctDNA-positive patients underwent randomization (167 to atezolizumab and 83 to placebo). Median disease-free survival was 9.9 months with atezolizumab versus 4.8 months with placebo (HR 0.64, 95% CI 0.47–0.87; P=0.005), and median overall survival was 32.8 months versus 21.1 months (HR 0.59, 95% CI 0.39–0.90; P=0.01). The 12-month disease-free survival rates were 44.7% with atezolizumab and 30.0% with placebo, and the corresponding 12-month overall survival rates were 85.1% and 70.0%, respectively. Among 357 patients with persistent ctDNA negativity, disease-free survival was 95% at the end of the 1-year monitoring period and 88% at 2 years; reported 12- and 24-month overall survival rates in this observational ctDNA-negative cohort were 100% and 97.1%, respectively, supporting a favorable prognosis under surveillance, although these observational data are insufficient to definitively establish that adjuvant therapy can be safely withheld in all ctDNA-negative patients.10
IMvigor011 should be read as a biomarker-enabled treatment trial rather than simply another positive adjuvant immunotherapy study. Its central contribution is to prospectively validate molecular relapse as an actionable postoperative state and to confirm, in randomized fashion, the biomarker-enrichment signal that had previously been inferred retrospectively from IMvigor010.10–12 Just as importantly, the trial also defines the present evidentiary boundary of the field: randomized evidence now supports ctDNA-triggered treatment escalation, whereas treatment omission in persistently ctDNA-negative patients remains an observational inference rather than a randomized conclusion.10 This asymmetry is not semantic; it should shape both current clinical interpretation and the design priorities of the next generation of trials.
Supportive but Exploratory Evidence: CheckMate 274 Five-Year ctDNA Analysis
The phase III CheckMate 274 trial randomized 709 patients with high-risk muscle-invasive urothelial carcinoma (MIUC) after radical surgery to adjuvant nivolumab 240 mg every two weeks versus placebo for up to one year.3 In the peer-reviewed 5-year analysis published in Annals of Oncology, adjuvant nivolumab continued to show a durable disease-free survival (DFS) benefit: median DFS was 21.9 months versus 11.0 months in all randomized patients (HR 0.74; 95% CI 0.61–0.90), and 55.5 months versus 8.4 months in patients with tumor PD-L1 expression ≥1% (HR 0.58; 95% CI 0.42–0.79). Median OS in all randomized patients was 75.0 months versus 50.1 months (HR 0.83; 95% CI 0.67–1.02), but the prespecified boundary for statistical significance had not been crossed at the time of this analysis.13
The post hoc exploratory ctDNA analysis was based on only 133 of 709 randomized patients and should therefore be interpreted as supportive, hypothesis-generating evidence rather than practice-defining validation, a positioning that is also consistent with recent bladder cancer–focused reviews of ctDNA implementation.9 Baseline ctDNA after radical surgery was detected in 54 (40.6%) of 133 assessable patients. Median DFS was 52.1 months versus 5.0 months in patients with undetectable versus detectable ctDNA at baseline (HR 0.30; 95% CI 0.18–0.48). Among patients with detectable ctDNA, median DFS was 7.4 months with nivolumab versus 2.8 months with placebo (HR 0.35; 95% CI 0.18–0.66), whereas among those with undetectable ctDNA, no clear DFS advantage was observed (HR 0.99; 95% CI 0.51–1.93).13 Taken together, these exploratory data are directionally concordant with IMvigor011 and with the broader TOMBOLA experience, supporting the hypothesis that ctDNA-defined MRD may enrich for postoperative benefit from adjuvant ICI. However, because the CheckMate 274 ctDNA dataset was small, post hoc, and agent-specific, these findings should be interpreted as supportive rather than independently confirmatory, and cross-agent predictive validity remains unproven.10,13,14
The AMBASSADOR Trial and the Unresolved Question of Unselected Adjuvant ICI Benefit
The phase III AMBASSADOR trial evaluated adjuvant pembrolizumab versus observation in patients with high-risk muscle-invasive urothelial carcinoma after radical surgery and showed a significant disease-free survival benefit in the intention-to-treat population, whereas overall survival remained immature at the time of reporting.5 Unlike IMvigor011, which prospectively randomized patients after ctDNA positivity during surveillance, AMBASSADOR was not designed as a ctDNA-guided biomarker-integrated trial. The ctDNA findings from CheckMate 274 were likewise exploratory rather than used for prospective patient selection. Accordingly, AMBASSADOR is best interpreted within a broader but methodologically heterogeneous evidence base for adjuvant immune checkpoint inhibition in clinicopathologically selected high-risk disease.5,10,13 Because AMBASSADOR did not report prospective ctDNA stratification or ctDNA biomarker results in its primary publication, it does not resolve whether ctDNA can refine patient selection for pembrolizumab-based adjuvant therapy. In light of IMvigor011 and the broader maturation of MRD-oriented studies in urothelial cancer, prospective ctDNA incorporation is a rational next step for future perioperative trial design, but the available evidence does not yet support describing ctDNA assessment as a mandated standard.9,10,25
The Perioperative Context: NIAGARA and Its Implications for ctDNA-Guided Adjuvant Strategies
The perioperative treatment landscape for MIBC was materially reshaped by NIAGARA, in which perioperative durvalumab added to gemcitabine-cisplatin improved both event-free survival and overall survival versus neoadjuvant gemcitabine-cisplatin alone in cisplatin-eligible patients with operable disease. As perioperative ICI-containing regimens now have phase III survival-level support, the postoperative question becomes less whether adjuvant therapy should be given broadly and more which residual-risk subsets, if any, still warrant additional treatment after prior systemic intensification.44 Neoadjuvant ICI programs such as NABUCCO and PURE-01 established that deep pathologic responses can be achieved before cystectomy. However, long-term PURE-01 follow-up showed that survival remained strongly stratified by pathologic response, indicating that patients without a complete or major pathologic response continue to carry clinically meaningful recurrence risk.45,46 In this context, postoperative ctDNA is best framed as a candidate residual-risk stratification tool rather than a universally validated arbiter across all perioperative regimens. Direct prospective support exists after neoadjuvant chemotherapy plus cystectomy in TOMBOLA, where serial tumor-informed ctDNA testing guided early atezolizumab in ctDNA-positive patients, whereas ctDNA-negative patients received immunotherapy only upon radiographic detection of metastases; whether the same principle can be generalized to ICI-containing perioperative regimens remains unproven.14
Postoperative ctDNA can therefore no longer be interpreted within the older binary framework of cystectomy followed by optional adjuvant therapy. In contemporary practice, postoperative MRD assessment increasingly occurs after heterogeneous perioperative regimens, including chemotherapy-alone, chemoimmunotherapy, and ADC-containing approaches, each of which may alter both residual disease biology and the clinical meaning of postoperative ctDNA positivity or negativity.44,47 The central translational question is therefore shifting from whether ctDNA can identify residual risk after cystectomy per se to whether it can reliably re-stratify risk after prior systemic intensification and thereby guide selective postoperative escalation rather than indiscriminate continuation of therapy. In this setting, postoperative ctDNA should currently be regarded as a biologically plausible and clinically promising stratification tool, but not yet as a universally validated decision-maker across all intensified perioperative pathways.44,47
ctDNA-Guided Adjuvant Treatment Reconstruction: Escalation and De-Escalation Strategies
Treatment Escalation: Targeting ctDNA-Positive (MRD+) Patients
The phase III IMvigor011 trial established that ctDNA-positive patients derived significant clinical benefit from adjuvant atezolizumab, with hazard ratios of 0.64 for disease-free survival and 0.59 for overall survival versus placebo, corresponding to relative reductions of 36% in recurrence or death and 41% in the risk of death.10 Compared with the negative intention-to-treat result of IMvigor010 in an unselected postoperative population (DFS HR 0.89), the positive IMvigor011 signal among ctDNA-positive patients supports ctDNA-based enrichment of therapeutic benefit; however, this inference remains cross-trial and should not be interpreted as a formally quantified efficiency gain within a single randomized framework.4,10
The escalation question should now be framed at three levels: whether ctDNA-positive disease warrants postoperative systemic treatment at all, whether single-agent PD-1/PD-L1 blockade is sufficient for all ctDNA-positive patients, and whether molecular non-clearance or molecular progression should trigger intensification beyond standard ICI. IMvigor011 addresses the first question directly; the latter two remain unresolved. In that sense, ctDNA-guided escalation has crossed the threshold from biologic hypothesis to practice-relevant principle, whereas regimen selection within the ctDNA-positive state remains investigational.10
Several escalation routes are biologically plausible but should be kept analytically distinct. ADC-based intensification is attractive because enfortumab vedotin plus pembrolizumab has redefined first-line therapy in untreated locally advanced or metastatic urothelial carcinoma; however, this evidence derives from unresected advanced disease and does not establish postoperative utility in molecularly relapsed disease after cystectomy.15 Likewise, sacituzumab govitecan has shown activity in advanced disease, but current evidence does not support treating it as an established postoperative escalation backbone.16,17 Dual-checkpoint approaches such as nivolumab plus relatlimab are supported by a coherent immunobiologic rationale, including nonredundant PD-1/LAG-3 cooperation in T-cell exhaustion and emerging urothelial data linking the LAG-3/FGL1 axis to immune-evasive tumor states, but direct postoperative MIBC evidence remains absent.18–20 A mature interpretation is therefore that ctDNA currently selects for a higher-risk interventional state, whereas the optimal intensified regimen within that state remains an open clinical-development question.
Longitudinal ctDNA kinetics may prove more informative than a single postoperative MRD snapshot. In updated IMvigor010 analyses, greater on-treatment ctDNA reduction—including complete clearance—was associated with progressively longer overall survival, and combining C1D1 with C3D1 improved relapse sensitivity compared with C1D1 alone.11 TOMBOLA similarly suggested that ctDNA status and levels, together with on-treatment ctDNA dynamics, were associated with recurrence risk and response to immunotherapy.14 Taken together, these data support dynamic molecular response as a promising clinical framework, but not yet a validated decision rule: rapid ctDNA clearance may identify treatment-sensitive disease, whereas persistent or rising ctDNA should currently be interpreted as a high-risk signal requiring prospective validation before being used to mandate treatment intensification or treatment switching. In the post-IMvigor011 era, the clinically relevant question may therefore extend beyond baseline ctDNA positivity to the trajectory of molecular residual disease under therapeutic pressure.11,14
Treatment De-Escalation: Sparing ctDNA-Negative (MRD−) Patients
The clinically meaningful question in de-escalation is not whether ctDNA-negative patients do better—they clearly do—but whether persistent ctDNA negativity can justify withholding immediate postoperative therapy without compromising cure opportunity. IMvigor011 and TOMBOLA both support the prognostic value of a persistently negative molecular state, but neither provides randomized proof that ctDNA-negative patients derive no incremental benefit from adjuvant treatment.10,14 That distinction matters because the evidentiary threshold for avoiding treatment is higher than the threshold for identifying a favorable-risk subgroup under surveillance. Cross-trial comparisons with unselected adjuvant immunotherapy studies should therefore remain hypothesis-generating rather than practice-defining. The randomized DYNAMIC trial in stage II colon cancer offers a conceptual precedent for ctDNA-guided treatment reduction in another solid tumor, but it should be interpreted strictly as proof of principle rather than as direct support in MIBC.48
Accordingly, de-escalation in postoperative MIBC should be defined as protocolized surveillance, not therapeutic nihilism. Persistent ctDNA negativity should be interpreted as a lower-risk molecular state that supports close observation with serial ctDNA reassessment and parallel imaging, not as evidence of complete disease eradication. Residual relapse risk may reflect low ctDNA shedding, limited analytical sensitivity in very low-volume disease, or incomplete representation of recurrent clones in patient-specific panels.25,49 Clinically, this means that ctDNA-negative patients still require structured follow-up, and any subsequent molecular conversion, radiographic change, or new clinical concern should trigger renewed risk stratification and reconsideration of systemic therapy.10,14 Shared decision-making remains essential because the current evidence base supports surveillance as a rational strategy, but not yet as a universally proven omission strategy.
ctDNA-Based Stratification versus Traditional Pathological Risk Assessment
Across IMvigor011, TOMBOLA, and independent cystectomy cohorts, ctDNA status appears to add prognostic—and potentially treatment-selective—information beyond conventional pathological risk assessment.10,14,23 In a prospective tumor-informed cystectomy cohort, detectable pre-cystectomy ctDNA was independently associated with nodal involvement, locally advanced pathology, and recurrence, supporting ctDNA as a complement to rather than a restatement of conventional staging.23 In TOMBOLA, ctDNA-positive disease was not restricted to clinicopathologically high-risk subsets, and ctDNA-positive, low-risk patients emerged as a clinically relevant group for early immunotherapy. Conversely, TOMBOLA also suggested that some ctDNA-negative patients with conventionally high-risk features can experience favorable outcomes under surveillance.14
The added value of ctDNA is best understood in integrative rather than substitutional terms. Pathological stage, nodal status, and prior treatment define baseline postoperative risk, whereas ctDNA functions as a post-treatment molecular readout that revises that risk according to whether residual disease is actually detectable.10,14,23,24 The clinically most informative patients are therefore often the discordant ones: clinicopathologically high-risk but ctDNA-negative patients, who may be candidates for intensified surveillance rather than automatic treatment, and patients outside the highest conventional risk strata who are nonetheless ctDNA-positive and therefore molecularly high-risk. In this framework, pathology provides the structural risk scaffold, while ctDNA identifies which patients appear to harbor biologically active residual disease within that scaffold. The emerging association of ctDNA positivity with more aggressive tumor biology, including basal/squamous enrichment in translational analyses, further supports the view that ctDNA is not merely restaging anatomy but capturing biologically relevant residual-risk states.23,24,43,50,51
Technological and Translational Challenges for Clinical Implementation
Assay Platform Selection: Tumor-Informed versus Tumor-Naïve Approaches
Assay selection in postoperative MIBC should be treated first as a question of clinical validity, and only second as a question of operational convenience. The strongest current therapeutic data—IMvigor011 and TOMBOLA—were both generated with tumor-informed strategies, meaning that the best-validated use case in this disease is still personalized plasma MRD tracking anchored to tumor sequencing.10,14 That validation status matters because an assay that is analytically attractive is not necessarily clinically interchangeable.
Tumor-informed assays offer their clearest advantage in low-burden postoperative disease, where sensitivity, background suppression, and clonal hematopoiesis of indeterminate potential (CHIP) control are decisive.25,26 Their liabilities are equally clear: they require adequate tissue, bespoke assay construction, and longer initial turnaround35,36. Tumor-agnostic platforms may alleviate some of these logistical constraints, but they should presently be described as promising rather than equivalent in postoperative MIBC, because prospective evidence showing cross-platform clinical interchangeability is not available.10,14,27
The forward direction is therefore unlikely to be a simple replacement of one platform by another. A more mature formulation is that different assay architectures may solve different biological problems: mutation-based tumor-informed assays currently provide the most robust systemic MRD framework, whereas methylation-, fragmentomic-, and other multi-analyte approaches may prove particularly valuable in low-shedding or diagnostically discordant settings.6,32,33 At present, however, these next-generation approaches remain developmental rather than practice-defining in MIBC.9
Sampling Kinetics: Optimal Timing and Frequency of ctDNA Assessment
Sampling kinetics should be framed as part of the clinical strategy rather than as a technical afterthought. Immediately after cystectomy, surgical trauma can transiently increase total cfDNA and potentially obscure ctDNA detection, which helps explain why the pivotal interventional studies did not rely on ultra-early postoperative testing.28 Available data instead support a serial surveillance model: IMvigor011 used repeated monitoring over the first postoperative year, IMvigor010 showed that combining early time points improves relapse sensitivity compared with a single baseline sample,11 and TOMBOLA demonstrated that a substantial proportion of ctDNA-positive conversions occur during continued follow-up rather than at one fixed postoperative draw.14 The practical implication is that postoperative MRD assessment should not be conceptualized as a one-time test, but as a longitudinal monitoring program. What remains unresolved is the optimal starting window, testing interval, monitoring duration, and whether surveillance intensity can eventually be adapted according to prior kinetics or treatment context.
The “Gray Zone”: Managing Discordant Results and False Negatives
The clinical scenario of radiographic negativity with ctDNA positivity—molecular relapse—is precisely the clinical state that IMvigor011 was designed to address, and the trial’s positive results support early intervention in this setting. However, ctDNA negativity does not eliminate subsequent recurrence risk. In IMvigor011, patients with persistent ctDNA negativity had disease-free survival of 95% at the end of the 1-year monitoring period and 88% at 2 years, and TOMBOLA reported a 1-year recurrence-free survival of 97% in ctDNA-negative patients.10,14 These data indicate that ctDNA negativity identifies a favorable-risk state rather than guaranteed disease eradication.
Several factors may reduce the detectability of plasma ctDNA and thereby contribute to false-negative results. In particular, low plasma tumor fraction and disease distribution may limit assay sensitivity, and ctDNA performance should therefore be interpreted in conjunction with clinical context rather than in isolation.9,26 In addition, urothelial carcinoma shows marked intra-patient molecular heterogeneity and treatment-associated clonal evolution; recurrent disease may therefore be incompletely represented by variants selected from the original tumor specimen for a personalized assay. Consistent with this, Faltas et al showed substantial intrapatient mutational heterogeneity in chemotherapy-treated urothelial carcinoma, with most mutations not shared across matched samples.29
An additional interpretive boundary is that plasma ctDNA should not be assumed to perform uniformly across all disease contexts. Recent MIBC biomarker data support further investigation of utDNA and plasma ctDNA as biomarkers of residual local and nonlocal disease, respectively.9,30 Accordingly, when the dominant concern is intravesical residual disease or local bladder recurrence, a negative plasma ctDNA result should not be interpreted as proof of complete disease eradication; plasma ctDNA and utDNA are better viewed as complementary rather than interchangeable analytes.
From a current clinical standpoint, the residual recurrence observed in ctDNA-negative patients argues for continued parallel imaging surveillance rather than ctDNA-only follow-up.10,14 From an assay-development standpoint, next-generation MRD platforms integrating mutation-based tracking with orthogonal cfDNA features, including methylation and fragmentomic signals, represent rational approaches to reduce false-negative risk, but prospective MIBC-specific validation remains limited.25,52
CHIP
CHIP is a recognized biological source of false-positive findings in plasma cfDNA/ctDNA analyses. Age-related somatic mutations arising in hematopoietic clones—classically involving DNMT3A, TET2, and ASXL1—may be misclassified as tumor-derived variants if paired leukocyte-derived or other matched-normal DNA is not adequately assessed.32,33 This issue is particularly relevant in bladder cancer, an age-associated malignancy with a median age at diagnosis of approximately 73 years.28 Because clinically relevant CHIP increases with age, the practical risk of CHIP-related misclassification is expected to be higher in postoperative MIBC cohorts than in younger solid-tumor populations, making rigorous matched-normal or leukocyte-based filtering especially important in this disease context.28,32,33
Tumor-informed assays can reduce CHIP-related misclassification because patient-specific variant selection is anchored to tumor sequencing and often incorporates matched-normal or leukocyte-derived DNA filtering; however, this risk is reduced rather than categorically eliminated.34 By contrast, tumor-agnostic plasma assays are more vulnerable to CHIP-related misclassification unless they incorporate paired leukocyte sequencing and/or robust CHIP-aware bioinformatic filtering. Accordingly, rigorous CHIP subtraction should be treated as a core analytical requirement for clinical ctDNA assays, especially when plasma results are used to support treatment decisions.34,35
Health-Economic Considerations and Accessibility
The clinical adoption of ctDNA-guided adjuvant therapy depends not only on clinical validity but also on assay-related logistics, reimbursement, and broader health-economic feasibility.36 Personalized tumor-informed MRD assays require tumor sequencing, bespoke assay design, and repeated longitudinal testing, making implementation complexity and economic value central translational considerations.37 In resource-limited settings, the infrastructure and workflow requirements of tumor-informed ctDNA assays may constrain uptake.37 TOMBOLA nevertheless suggests that a tumor-informed ddPCR strategy can be implemented in hospital laboratory settings, supporting the feasibility of more decentralized assay models, although formal comparative cost data remain lacking.14
Formal disease-specific health-economic data for ctDNA-guided postoperative adjuvant strategies in MIBC remain limited. By contrast, economic studies in colorectal cancer suggest potential budgetary benefit or conditional cost-effectiveness for ctDNA-guided approaches, although these findings are model-dependent rather than uniformly favorable.53,54 Generating disease-specific economic evidence should therefore be a priority as ctDNA-integrated postoperative strategies move closer to clinical implementation in MIBC.
Ongoing Trials and Future Perspectives
In the post-IMvigor011 era, the major unresolved questions have bifurcated into two closely related tracks: whether ctDNA-positive patients require more effective postoperative escalation than single-agent checkpoint blockade, and whether ctDNA-negative patients can safely undergo treatment de-escalation under surveillance. Within this framework, TOMBOLA provides prospective support for ctDNA-triggered postoperative intervention, whereas MODERN is positioned to test escalation and de-escalation more explicitly in parallel.21
TOMBOLA: Full Results and Their Translational Implications
The TOMBOLA trial, a Danish multicenter, open-label, single-arm phase II study, provides a mature prospective dataset on ctDNA-guided postoperative immunotherapy in MIBC outside the randomized IMvigor program. TOMBOLA enrolled low- and high-risk patients with MIBC treated with NAC followed by RC and used serial tumor-informed ctDNA testing to guide postoperative management. Patients with detectable ctDNA initiated atezolizumab for up to 1 year irrespective of imaging, whereas ctDNA-negative patients were observed and received immunotherapy only after radiographic metastatic recurrence.14 This design is clinically notable because it operationalized molecular relapse as an interventional state rather than a purely prognostic observation.9,14
In the full peer-reviewed analysis published in Annals of Oncology in 2026, 60% of the 84 ctDNA-positive patients who completed atezolizumab and had paired ctDNA and imaging assessment achieved the primary endpoint of molecular and radiographic complete response. One-year recurrence-free survival was 97% in ctDNA-negative patients and 76% in ctDNA-positive patients, and the median lead time from ctDNA detection to imaging-confirmed recurrence was 90 days.14 This molecular lead-time signal is directionally consistent with earlier urothelial ctDNA studies and reinforces the biological rationale for intervention at molecular rather than radiographic relapse.8,9
Several translational insights emerge from TOMBOLA. First, prespecified biomarker analyses showed that ctDNA status and levels, together with immune-related gene-expression signatures, were associated with recurrence risk and response to immunotherapy, supporting ctDNA as a dynamic biomarker rather than a purely binary postoperative classifier.14 Second, this interpretation is concordant with independent tumor-informed cystectomy cohorts in which ctDNA detectability before and after radical cystectomy was associated with adverse pathology and shorter disease-free survival, indicating that molecular residual-risk assessment can add information beyond conventional clinicopathological staging.23,24 Third, the use of a patient-specific tumor-informed ddPCR workflow indicates that clinically informative ctDNA-guided management may be achievable beyond a single centralized commercial platform, although cross-platform clinical equivalence remains unproven.9,14
A key limitation of TOMBOLA is its single-arm design, which precludes causal quantification of the incremental benefit of ctDNA-triggered atezolizumab versus observation in ctDNA-positive patients.14 Nevertheless, its directional consistency with the randomized IMvigor011 trial, together with broader bladder-cancer syntheses that frame ctDNA as a treatment-guiding and surveillance biomarker, supports the ctDNA-guided postoperative paradigm while still falling short of within-trial randomized confirmation for de-escalation or platform interchangeability.9,10,14
The MODERN Trial: A Dual-Track Randomized Evaluation of Escalation and De-Escalation
The MODERN trial (Alliance A032103; ClinicalTrials.gov identifier: NCT05987241) is an ongoing phase II/III randomized ctDNA-guided study in high-risk muscle-invasive urothelial carcinoma after radical surgery. According to the registered trial record, patients are assigned to cohorts according to postoperative ctDNA status: ctDNA-positive patients are randomized to adjuvant nivolumab alone versus nivolumab plus relatlimab, whereas ctDNA-negative patients are randomized to immediate adjuvant nivolumab versus ctDNA surveillance with nivolumab initiated only after ctDNA conversion.21,22
A key unresolved question after IMvigor011 is whether the favorable observational outcomes seen in persistently ctDNA-negative patients are sufficient to support treatment de-escalation in a randomized setting.10 By prospectively comparing immediate adjuvant nivolumab with ctDNA surveillance in the ctDNA-negative cohort, MODERN is designed to test this question directly.21,22
If nivolumab plus relatlimab improves molecular and clinical outcomes in ctDNA-positive disease, MODERN would provide prospective support for biomarker-directed postoperative intensification beyond single-agent checkpoint blockade. Whether this strategy would redefine standard care will depend on the magnitude, durability, safety, and generalizability of benefit.
Emerging Complementary Biomarkers: UtDNA, Methylation, and Multi-Analyte Integration
Although plasma ctDNA has led MRD research in MIBC, urinary tumor DNA (utDNA) appears to provide complementary rather than redundant information, particularly for residual disease confined to the bladder. In bladder-preservation cohorts and peri-cystectomy localized bladder cancer cohorts, utDNA has shown stronger performance for detecting residual local disease and has been associated with lack of pathologic complete response and worse oncologic outcomes.30,31 Accordingly, utDNA seems most informative when local bladder failure is the dominant concern, whereas plasma ctDNA remains more closely aligned with systemic residual-risk assessment.
Methylation- and fragmentomics-based cell-free DNA (cfDNA) assays represent attractive next-generation MRD strategies because they interrogate tumor-associated signals beyond sequence variants alone. This rationale is particularly relevant in low-burden disease, in which tumor fraction can approach the analytical limits of mutation-only assays.6,55,56 However, in MIBC, direct prospective evidence that these approaches reduce false-negative postoperative MRD classification beyond current mutation-based platforms remains limited.
The most defensible forward-looking model is biomarker complementarity rather than simple biomarker substitution. A future MIBC platform may integrate plasma ctDNA for systemic residual-risk assessment with utDNA for local urothelial disease, potentially augmented by orthogonal cfDNA features such as methylation and fragmentomics.9,55 However, the incremental value, optimal sequencing, and clinical thresholds of such multi-analyte frameworks remain to be prospectively defined before they can be regarded as established postoperative tools.
Toward Standardization: Regulatory Pathways and Clinical Practice Integration
The most defensible implication of IMvigor011 is not that a specific assay–drug pairing is already ready for routine companion-diagnostic deployment, but that prospective therapeutic validation of a tumor-informed ctDNA MRD strategy in postoperative MIBC is now demonstrably feasible. This provides a credible clinical foundation for future assay–drug co-development and regulatory translation, without overstating the immediacy of any specific approval pathway.10
However, broader clinical adoption remains constrained by assay heterogeneity. Tumor-informed and tumor-agnostic platforms differ in analytical architecture, sensitivity, specificity, and practical feasibility, and standardized interpretation, reporting, and validation frameworks for ctDNA MRD testing remain incomplete across laboratories and disease settings. ASCO and CAP have provided a general framework for ctDNA assay evaluation,38 but postoperative MIBC still lacks disease-specific, assay-harmonized implementation standards.9,39
Routine implementation of ctDNA testing will also depend on rigorous control of pre-analytical variables, appropriate laboratory infrastructure, and assay-specific interpretive expertise. Pre-analytical handling is not a minor operational detail: blood-collection conditions, time to processing, and specimen storage can materially influence cfDNA quantity, fragmentation profiles, and downstream analytical reliability.38,40
Limitations of This Review
Several limitations of this review should be acknowledged. First, this article is a narrative review rather than a systematic review or meta-analysis; therefore, it does not apply a prespecified search strategy, formal risk-of-bias assessment, or quantitative evidence synthesis. The aim was instead to provide a critical and clinically oriented interpretation of a rapidly evolving field. Second, several key datasets discussed in this review were published or updated in 2025–2026, and some aspects of their long-term follow-up, regulatory implications, assay-specific implementation, and cross-platform generalizability may continue to evolve after publication. Third, formal health-economic evidence for ctDNA-guided postoperative management in MIBC remains limited, and the economic analyses discussed in Health-Economic Considerations and Accessibility derive from colorectal cancer models. Direct extrapolation to MIBC should therefore be cautious because patient demographics, disease biology, treatment pathways, recurrence patterns, assay use cases, and downstream therapeutic costs differ between colorectal cancer and MIBC. Accordingly, the conclusions presented here should be interpreted as a calibrated synthesis of the currently available evidence rather than as final practice standards for all postoperative MIBC settings.
Conclusion
The post-IMvigor011 era should not be interpreted as the arrival of a universally deployable ctDNA standard, but as the point at which ctDNA became clinically actionable in one clearly defined postoperative state: molecular relapse after cystectomy. Randomized evidence now supports ctDNA-triggered treatment escalation, whereas ctDNA-guided omission of therapy, cross-platform assay interchangeability, and generalization across increasingly heterogeneous perioperative regimens remain incompletely validated.
Future research should therefore focus on several clinically decisive priorities. First, randomized data are needed to determine whether persistently ctDNA-negative patients can safely avoid immediate adjuvant therapy while remaining under structured surveillance. Pending such data, a pragmatic interim approach for persistently ctDNA-negative patients is not treatment abandonment, but protocolized surveillance: serial ctDNA reassessment should be maintained at relatively short intervals during the first postoperative year, where feasible reflecting trial-based monitoring intensity, while guideline-based cross-sectional imaging continues in parallel, for example every 6 months during the first 3 years after cystectomy and annually thereafter. Any subsequent ctDNA conversion, radiographic abnormality, or new clinical concern should prompt repeat staging and reconsideration of systemic therapy. Second, prospective studies should define optimal sampling intervals, monitoring duration, and response-adaptive thresholds based on serial ctDNA kinetics. Third, assay platforms require disease-specific validation, including standardization of CHIP filtering, pre-analytical handling, reporting thresholds, and the complementary use of plasma and urine analytes. Finally, health-economic analyses specific to MIBC are needed before ctDNA-guided postoperative strategies can be broadly implemented.
The main take-home message is that ctDNA should currently be viewed as a powerful postoperative risk-refinement tool rather than a stand-alone replacement for clinicopathologic assessment, imaging, or clinical judgment. In ctDNA-positive molecular relapse, treatment escalation is now supported by prospective randomized evidence. In persistently ctDNA-negative patients, surveillance-based de-escalation is clinically plausible but remains a research question until randomized evidence confirms that treatment omission is safe.
Declaration of Generative AI Use
Authors declare no AI use during the preparation of this work.
Abbreviations
MIBC, muscle-invasive bladder cancer; ctDNA, Circulating tumor DNA; MRD, molecular residual disease; MIUC, muscle-invasive urothelial carcinoma; DFS, disease-free survival; CHIP, clonal hematopoiesis of indeterminate potential; utDNA, urinary tumor DNA; cfDNA, cell-free DNA.
Ethics Statement
This study did not directly involve the testing of human and animal samples; ethical approval is not applicable.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare no competing interests in this work.
References
1. St-Laurent MP, Nikkola J, Tomiyama E, Black PC. Advances in the management of localized bladder cancers. Nat Rev Clin Oncol. 2026;23:158–16. doi:10.1038/s41571-025-01104-z
2. Stein JP, Lieskovsky G, Cote R, et al. Radical cystectomy in the treatment of invasive bladder cancer: long-term results in 1,054 patients. J Clin Oncol. 2001;19:666–675. doi:10.1200/jco.2001.19.3.666
3. Bajorin DF, Witjes JA, Gschwend JE, et al. Adjuvant nivolumab versus placebo in muscle-invasive urothelial carcinoma. N Engl J Med. 2021;384:2102–2114. doi:10.1056/NEJMoa2034442
4. Bellmunt J, Hussain M, Gschwend JE, et al. Adjuvant atezolizumab versus observation in muscle-invasive urothelial carcinoma (IMvigor010): a multicentre, open-label, randomised, Phase 3 trial. Lancet Oncol. 2021;22:525–537. doi:10.1016/s1470-2045(21)00004-8
5. Apolo AB, Ballman KV, Sonpavde G, et al. Adjuvant Pembrolizumab versus Observation in Muscle-Invasive Urothelial Carcinoma. N Engl J Med. 2025;392:45–55. doi:10.1056/NEJMoa2401726
6. Pantel K, Alix-Panabières C. Minimal residual disease as a target for liquid biopsy in patients with solid tumours. Nat Rev Clin Oncol. 2025;22:65–77. doi:10.1038/s41571-024-00967-y
7. Patel KM, van der Vos KE, Smith CG, et al. Association of plasma and urinary mutant DNA with clinical outcomes in muscle invasive bladder cancer. Sci Rep. 2017;7:5554. doi:10.1038/s41598-017-05623-3
8. Christensen E, Birkenkamp-Demtröder K, Sethi H, et al. Early detection of metastatic relapse and monitoring of therapeutic efficacy by ultra-deep sequencing of plasma Cell-Free DNA in patients with urothelial bladder carcinoma. J Clin Oncol. 2019;37:1547–1557. doi:10.1200/jco.18.02052
9. Lindskrog SV, Strandgaard T, Nordentoft I, et al. Circulating tumour DNA and circulating tumour cells in bladder cancer - from discovery to clinical implementation. Nat Rev Urol. 2025;22:590–608. doi:10.1038/s41585-025-01023-9
10. Powles T, Kann AG, Castellano D, et al. ctDNA-Guided adjuvant atezolizumab in muscle-invasive bladder cancer. N Engl J Med. 2025;393:2395–2408. doi:10.1056/NEJMoa2511885
11. Powles T, Assaf ZJ, Degaonkar V, et al. Updated overall survival by circulating tumor DNA status from the phase 3 IMvigor010 trial: adjuvant atezolizumab versus observation in muscle-invasive urothelial carcinoma. Eur Urol. 2024;85:114–122. doi:10.1016/j.eururo.2023.06.007
12. Powles T, Assaf ZJ, Davarpanah N, et al. ctDNA guiding adjuvant immunotherapy in urothelial carcinoma. Nature. 2021;595:432–437. doi:10.1038/s41586-021-03642-9
13. Galsky MD, Gschwend JE, Milowsky MI, et al. Adjuvant nivolumab versus placebo for high-risk muscle-invasive urothelial carcinoma: 5-year efficacy and ctDNA results from CheckMate 274. Ann Oncol. 2026;37:69–78. doi:10.1016/j.annonc.2025.09.139
14. Dyrskjøt L, Birkenkamp-Demtröder K, Nordentoft I, et al. ctDNA-guided immunotherapy following radical cystectomy for muscle-invasive bladder cancer: results from the TOMBOLA trial. Ann Oncol. 2026. doi:10.1016/j.annonc.2025.12.018
15. Powles T, Valderrama BP, Gupta S, et al. Enfortumab vedotin and pembrolizumab in untreated advanced urothelial cancer. N Engl J Med. 2024;390:875–888. doi:10.1056/NEJMoa2312117
16. Tagawa ST, Balar AV, Petrylak DP, et al. TROPHY-U-01: a phase II open-label study of sacituzumab govitecan in patients with metastatic urothelial carcinoma progressing after platinum-based chemotherapy and checkpoint inhibitors. J Clin Oncol. 2021;39:2474–2485. doi:10.1200/jco.20.03489
17. Powles T, Tagawa S, Vulsteke C, et al. Sacituzumab govitecan in advanced urothelial carcinoma: tROPiCS-04, a phase III randomized trial. Ann Oncol. 2025;36:561–571. doi:10.1016/j.annonc.2025.01.011
18. Tawbi HA, Schadendorf D, Lipson EJ, et al. Relatlimab and nivolumab versus nivolumab in untreated advanced melanoma. N Engl J Med. 2022;386:24–34. doi:10.1056/NEJMoa2109970
19. Yoshida T, Nakamoto T, Atsumi N, et al. Impact of LAG-3/FGL1 pathway on immune evasive contexture and clinical outcomes in advanced urothelial carcinoma. J Immunother Cancer. 2024;12: doi:10.1136/jitc–2024–009358.
20. Andrews LP, Butler SC, Cui J, et al. LAG-3 and PD-1 synergize on CD8(+) T cells to drive T cell exhaustion and hinder autocrine IFN-γ-dependent anti-tumor immunity. Cell. 2024;187:4355–4372.e4322. doi:10.1016/j.cell.2024.07.016
21. Meeks JJ. The changing landscape of urothelial carcinoma: on the edge of a paradigm shift. J Clin Invest. 2026;136. doi:10.1172/jci202079
22. ClinicalTrials.gov 2024. Testing the role of DNA released from tumor cells into the blood in guiding the use of immunotherapy after surgical removal of the bladder, kidney, ureter, and urethra for urothelial cancer treatment, MODERN study. Available from: https://clinicaltrials.gov/study/NCT05987241.
23. Ben-David R, Tillu N, Cumarasamy S, et al. Longitudinal tumor-informed circulating tumor DNA status predicts disease upstaging and poor prognosis for patients undergoing radical cystectomy. Eur Urol Oncol. 2024;7:1105–1112. doi:10.1016/j.euo.2024.03.002
24. Sfakianos JP, Basu A, Laliotis G, et al. Association of tumor-informed circulating tumor DNA detectability before and after radical cystectomy with disease-free survival in patients with bladder cancer. Eur Urol Oncol. 2025;8:306–314. doi:10.1016/j.euo.2024.07.001
25. Patel KR, Rais-Bahrami S, Basu A. High sensitivity ctDNA assays in genitourinary malignancies: current evidence and future directions. Oncologist. 2024;29:731–737. doi:10.1093/oncolo/oyae198
26. Cheng ML, Pectasides E, Hanna GJ, Parsons HA, Choudhury AD, Oxnard GR. Circulating tumor DNA in advanced solid tumors: clinical relevance and future directions. CA Cancer J Clin. 2021;71:176–190. doi:10.3322/caac.21650
27. Necchi A, Guerrero-Ramos F, Crispen PL, et al. Gemcitabine intravesical system plus cetrelimab or cetrelimab alone as neoadjuvant therapy in muscle-invasive bladder cancer: sunRISe-4 primary analysis and biomarker results. J Clin Oncol. 2026;44:586–597. doi:10.1200/jco-25-02382
28. Cumberbatch MGK, Jubber I, Black PC, et al. Epidemiology of bladder cancer: a systematic review and contemporary update of risk factors in 2018. Eur Urol. 2018;74:784–795. doi:10.1016/j.eururo.2018.09.001
29. Faltas BM, Prandi D, Tagawa ST, et al. Clonal evolution of chemotherapy-resistant urothelial carcinoma. Nat Genet. 2016;48:1490–1499. doi:10.1038/ng.3692
30. Galsky MD, Izadmehr S, Yu M, et al. Monitoring of plasma and urine tumor-derived DNA to inform bladder-sparing approaches for patients with muscle-invasive bladder cancer. Proc Natl Acad Sci U S A. 2026;123:e2533449123. doi:10.1073/pnas.2533449123
31. Chauhan PS, Chen K, Babbra RK, et al. Urine tumor DNA detection of minimal residual disease in muscle-invasive bladder cancer treated with curative-intent radical cystectomy: a cohort study. PLoS Med. 2021;18:e1003732. doi:10.1371/journal.pmed.1003732
32. Hu Y, Ulrich BC, Supplee J, et al. False-Positive plasma genotyping due to clonal hematopoiesis. Clin Cancer Res. 2018;24:4437–4443. doi:10.1158/1078-0432.Ccr-18-0143
33. Jaiswal S, Fontanillas P, Flannick J, et al. Age-related clonal hematopoiesis associated with adverse outcomes. N Engl J Med. 2014;371:2488–2498. doi:10.1056/NEJMoa1408617
34. Leal A, van Grieken NCT, Palsgrove DN, et al. White blood cell and cell-free DNA analyses for detection of residual disease in gastric cancer. Nat Commun. 2020;11:525. doi:10.1038/s41467-020-14310-3
35. Magee D, Domenyuk V, Abraham J, et al. Characterization of plasma Cell-Free DNA variants as of tumor or clonal hematopoiesis origin in 16,812 advanced cancer patients. Clin Cancer Res. 2025;31:2710–2718. doi:10.1158/1078-0432.Ccr-24-3335
36. Douglas MP, Ragavan MV, Chen C, et al. Private payer and medicare coverage policies for use of circulating tumor DNA tests in cancer diagnostics and treatment. J Natl Compr Canc Netw. 2023;21:609–616.e604. doi:10.6004/jnccn.2023.7011
37. Chen K, Shields MD, Chauhan PS, et al. Commercial ctDNA assays for minimal residual disease detection of solid tumors. Mol Diagn Ther. 2021;25:757–774. doi:10.1007/s40291-021-00559-x
38. Merker JD, Oxnard GR, Compton C, et al. Circulating tumor DNA analysis in patients with cancer: American Society of Clinical Oncology and College of American Pathologists joint review. J Clin Oncol. 2018;36:1631–1641. doi:10.1200/jco.2017.76.8671
39. Abdo T, Alhalabi A, Yaghi S, et al. Minimal residual disease in solid tumors: clinical applications and future directions. Cancer. 2026;132:e70286. doi:10.1002/cncr.70286
40. van der Pol Y, Moldovan N, Verkuijlen S, et al. The effect of preanalytical and physiological variables on cell-free DNA fragmentation. Clin Chem. 2022;68:803–813. doi:10.1093/clinchem/hvac029
41. Birkenkamp-Demtröder K, Christensen E, Nordentoft I, et al. Monitoring treatment response and metastatic relapse in advanced bladder cancer by liquid biopsy analysis. Eur Urol. 2018;73:535–540. doi:10.1016/j.eururo.2017.09.011
42. Nordentoft I, Lindskrog SV, Birkenkamp-Demtröder K, et al. Whole-genome mutational analysis for tumor-informed detection of circulating tumor DNA in patients with urothelial carcinoma. Eur Urol. 2024;86:301–311. doi:10.1016/j.eururo.2024.05.014
43. Lindskrog SV, Birkenkamp-Demtröder K, Nordentoft I, et al. Circulating tumor DNA analysis in advanced urothelial carcinoma: insights from biological analysis and extended clinical follow-up. Clin Cancer Res. 2023;29:4797–4807. doi:10.1158/1078-0432.Ccr-23-1860
44. Powles T, Catto JWF, Galsky MD, et al. Perioperative durvalumab with neoadjuvant chemotherapy in operable bladder cancer. N Engl J Med. 2024;391:1773–1786. doi:10.1056/NEJMoa2408154
45. Van Dorp J, Pipinikas C, Suelmann BBM, et al. High- or low-dose preoperative ipilimumab plus nivolumab in stage III urothelial cancer: the phase 1B NABUCCO trial. Nat Med. 2023;29:588–592. doi:10.1038/s41591-022-02199-y
46. Tateo V, Basile G, Giannatempo P, et al. Updated 5-year survival results from PURE-01, a phase 2 study of neoadjuvant pembrolizumab followed by radical cystectomy in patients with muscle-invasive bladder cancer. Eur Urol. 2026. doi:10.1016/j.eururo.2026.01.015
47. Vulsteke C, Adra N, Danchaivijitr P, et al. Perioperative enfortumab vedotin and pembrolizumab in bladder cancer. N Engl J Med. 2026. doi:10.1056/NEJMoa2511674
48. Tie J, Cohen JD, Lahouel K, et al. Circulating tumor DNA analysis guiding adjuvant therapy in stage ii colon cancer. N Engl J Med. 2022;386:2261–2272. doi:10.1056/NEJMoa2200075
49. Camblor DG, Martínez-Castedo B, Martín-Arana J, et al. Clinical performance of tumor-informed versus tumor-agnostic ctDNA assays for colorectal cancer recurrence: a systematic review and diagnostic accuracy meta-analysis. Cancer Treat Rev. 2026;142:103066. doi:10.1016/j.ctrv.2025.103066
50. Robertson AG, Kim J, Al-Ahmadie H, et al. Comprehensive molecular characterization of muscle-invasive bladder cancer. Cell. 2017;171:540–556.e525. doi:10.1016/j.cell.2017.09.007
51. Kamoun A, de Reyniès A, Allory Y, et al. A consensus molecular classification of muscle-invasive bladder cancer. Eur Urol. 2020;77:420–433. doi:10.1016/j.eururo.2019.09.006
52. Bruhm DC, Vulpescu NA, Foda ZH, Phallen J, Scharpf RB, Velculescu VE. Genomic and fragmentomic landscapes of cell-free DNA for early cancer detection. Nat Rev Cancer. 2025;25:341–358. doi:10.1038/s41568-025-00795-x
53. Li Y, Heer AK, Sloane HS, et al. Budget impact analysis of circulating tumor DNA testing for colon cancer in commercial health and medicare advantage plans. JAMA Health Forum. 2024;5:e241270. doi:10.1001/jamahealthforum.2024.1270
54. Kramer A, Greuter MJE, Schraa SJ, et al. Early evaluation of the effectiveness and cost-effectiveness of ctDNA-guided selection for adjuvant chemotherapy in stage II colon cancer. Ther Adv Med Oncol. 2024;16:17588359241266164. doi:10.1177/17588359241266164
55. Tsui WHA, Jiang P, Lo YMD. Cell-free DNA fragmentomics in cancer. Cancer Cell. 2025;43:1792–1814. doi:10.1016/j.ccell.2025.09.006
56. Stetson D, Labrousse P, Russell H, et al. Next-Generation molecular residual disease assays: do we have the tools to evaluate them properly? J Clin Oncol. 2024;42:2736–2740. doi:10.1200/jco.23.02301
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Overcoming Obstacles in Liquid Biopsy Developments for Prostate Cancer
Jang A, Rauterkus GP, Vaishampayan UN, Barata PC
OncoTargets and Therapy 2022, 15:897-912
Published Date: 26 August 2022
Clinical Utility and Application of Liquid Biopsy Genotyping in Lung Cancer: A Comprehensive Review
Nigro MC, Marchese PV, Deiana C, Casadio C, Galvani L, Di Federico A, De Giglio A
Lung Cancer: Targets and Therapy 2023, 14:11-25
Published Date: 3 February 2023
Cost-Effectiveness of Abemaciclib in Early Breast Cancer Patients: One Size Fits All or Tailoring to Patients’ Needs?
Jongbloed EM, Blommestein HM, van Schoubroeck HM, Martens JW, Wilting SM, Uyl-de Groot CA, Jager A
Breast Cancer: Targets and Therapy 2023, 15:147-161
Published Date: 16 February 2023
Evaluating the Prognostic Value of a Pan-Cancer Circulating Tumor DNA Next-Generation Sequencing Panel in Advanced Cancer Patients
Lee J, Cho JH, Lee S, Kim HS, Han SJ, Jung Y, Byun JH, Kim M
OncoTargets and Therapy 2025, 18:1179-1188
Published Date: 25 October 2025
Circulating Tumor DNA in Cholangiocarcinoma: A Precision Oncology Roadmap

Wei H, Wang J, Wu Q, Qin M
Cancer Management and Research 2026, 18:574678
Published Date: 6 February 2026