Back to Journals » Clinical Epidemiology » Volume 16
Patient Safety Climate in Danish Primary Care: Adaption and Validation of the Danish Safety Attitudes Questionnaire (SAQ-DK-PRIM)
Authors Juhl MH, Olesen AE ![]() , Deilkås ET, Bruun NH, Obling KH
, Deilkås ET, Bruun NH, Obling KH ![]() , Rytter N, Larsen MD, Kristensen S
, Rytter N, Larsen MD, Kristensen S
Received 22 March 2024
Accepted for publication 1 August 2024
Published 27 August 2024 Volume 2024:16 Pages 533—547
DOI https://doi.org/10.2147/CLEP.S470111
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Irene Petersen
Marie Haase Juhl,1,2 Anne Estrup Olesen,1,2 Ellen Tveter Deilkås,3 Niels Henrik Bruun,4 Kirsten Høgh Obling,5 Nikoline Rytter,6 Maya Damgaard Larsen,6 Solvejg Kristensen7
1Department of Clinical Pharmacology, Aalborg University Hospital, Aalborg, Denmark; 2Department of Clinical Medicine, Aalborg University, Aalborg, Denmark; 3Health Services Research Unit, Akershus University Hospital, Lørenskog, Norway; 4Research Data and Biostatistics, Aalborg University Hospital, Aalborg, Denmark; 5Care and Rehabilitation, Department of Health and Care Services (Danish: “pleje Og Rehabilitering, Staben Sundhed Og Omsorg”), the Municipality of Aarhus, Aarhus, Denmark; 6Digitalization and Quality, Department of Health and Care Services (Danish: “digitalisering og Kvalitet, Sundhed og Omsorg”), The Municipality of Aarhus, Aarhus, Denmark; 7Aalborg University Hospital, Psychiatry, Aalborg, Denmark
Correspondence: Anne Estrup Olesen, Department of Clinical Pharmacology, Aalborg University Hospital, Gartnerboligen, Ground Floor, Mølleparkvej 8a, Aalborg, 9000, Denmark, Tel +45 97664376, Email [email protected]
Background: A lack of instruments to assess patient safety climate within primary care exists. The objectives of this study were as follows: 1) To adapt the Danish hospital version of the Safety Attitudes Questionnaire (SAQ-DK) for use in primary care; 2) Test the internal consistency and the construct validity of this version; 3) Present benchmark data; and 4) Analyze variance.
Methods: The SAQ-DK was adapted for use in Danish primary care settings (SAQ-DK-PRIM) and distributed to healthcare staff members from nursing homes (N = 11), homecare units (N = 4) and healthcare units (N = 2), within the municipality of Aarhus, Central Denmark Region, Denmark. Face- and content validity were assessed. The construct validity was evaluated by a set of goodness-of-fit indices. The internal reliability was evaluated using the item-rest correlations, the inter-item correlations, and Cronbach’s alpha (α).
Results: The adaptation process resulted in a questionnaire of 10 items. Eight hundred and thirty healthcare staffs participated (78% of the eligible respondents). In total 586 (70.6%) responses were complete and were included in the analysis. Goodness-of-fit indices from the confirmatory factor analysis showed: Chi2=46.90CFI=0.97, RMSEA = 0.063 (90% CI: 0.044– 0.084), Probability RMSEA (p close)=0.12. Internal reliability was high (Cronbach’s α=0.76). Proportions of participants with a positive attitude was 41.1% and did not differ between the healthcare services. Scale mean score was 70.19 (SD: 18.05) and differed between healthcare services. The safety climate scale scores did not vary according to healthcare service type. ICC was 0.68% indicating no clustering of scores by healthcare service type.
Conclusion: Considering the questionnaire’s applicability, short length, strengthened focus on one area of interest and validity, the SAQ-DK-PRIM can serve as a valuable tool for measuring patient safety climate within primary care settings in Denmark.
Keywords: primary care, patient safety culture, patient safety climate, questionnaire, validity, reliability, Denmark
A Letter to the Editor has been published for this article.
A Response to Letter by Dr Zubaidah has been published for this article.
Introduction
Patient Safety Culture a Key to Patient Safety
Primary care encompasses an especially complex network of different healthcare services centred on home care, nursing facilities, social housing, and rehabilitation. Currently, the political arena is increasingly focused on primary care to meet rapidly growing demands on healthcare systems, including in Denmark. Consequently, primary care encounters heightened vulnerability to preventable harm related to healthcare, making it a pivotal focal point in terms of patient safety.1,2 To improve patient safety-related outcomes, better care processes and optimized use of resources are needed. An important first step is to assess patient safety culture, acknowledged as a key to patient safety.3 Previous research clearly holds emphasis on patient safety cultures in hospitals, leaving primary care an urgent key scope.4 The term patient safety climate and patient safety culture are used interchangeable in the literature but “patient safety climate” is generally acknowledged to represent measurable aspects of a patient safety culture.5–9
Assessing Patient Safety Culture
Focusing on patient safety culture as a key to patient safety has become of wide attention as the basis of national patient safety strategies.10 Still, evidence on patient safety culture within primary care remains sparse and inconclusive.3,11 Current recommendations and evidence state the importance of using questionnaires on patient safety climate in guiding the assessment and improvement of patient safety culture6 mainly focused on hospital settings.2,10,12–14 Multiple reliable and valid instruments are available to assess patient safety climate within hospital settings.15 For comparison of these instruments, the reader is referred to the review by Azyabi et al.15 Only few instruments have been found psychometrically sound related to assessing patient safety climate in primary care settings.16,17 This diminishes important opportunities for comparability and learning potential across healthcare sectors, organisations and departments.18 Developing new instruments could further hinder comparability, reflecting the recommended establishment of validity and reliability of existing questionnaires oppositely to developing new ones.16
Safety Attitudes Questionnaire
The Safety Attitudes Questionnaire (SAQ) was originally designed in 2006 as a staff survey that measures 6 safety-related climate domains in 60 items. The SAQ elicits a snapshot of the safety culture through surveys of self-reported health-care worker perceptions.19 SAQ is recommended to guide patient safety improvement initiatives globally2 and a psychometric sound version for use in Danish hospitals exists (SAQ-DK), where DK for Denmark indicates that the original language is Danish.20 The SAQ has shown proof as a valid and reliable instrument across international borders and healthcare sectors globally in measuring healthcare providers self-reported perceptions of patient safety climate.4,13,21 Even though other instruments have been used within primary care internationally,17 studies have found associations between SAQ scores and patient safety-related incidents in hospitals,22 including medication errors and falls.23,24 This supports the current recommendations of SAQ as a proper instrument to assess patient safety climate in OECD countries,10 including Denmark.25 Different SAQ adaptations for use in western European nursing homes and outpatient clinics with acceptable psychometric features have been established.4,17,26–28 SAQ-DK is the only questionnaire validated to capture reflections of patient safety climate within Danish healthcare.20 The six subscales of the generic SAQ were replicated in the SAQ-DK, while a major adaptation was the target-population, including multi-disciplinary organizational employees.20 These adaptations support earlier research suggesting a broadening of the target-population of patient safety climate measures in nursing homes.29 It has been demonstrated that SAQ in different versions is valid for use in primary care, but it is important to adapt and validate the questionnaire to the specific setting and participants under investigation.4 Moreover, it has been demonstrated that differences in SAQ factor scores were related to a variety of descriptive factors that should be considered in future studies.4 As Danish hospital and primary care settings greatly differ both in scope and descriptive factors as eg, healthcare disciplines, the use of SAQ-DK within a Danish primary healthcare frame warrants both adaptation- and psychometrically re-testing.
Thus, to support meaningful and trustworthy guidance of patient safety improvement work in Danish primary care, the objectives of this study were to 1) adapt the SAQ-DK to SAQ-DK-PRIM for use in primary care; 2) Test the internal consistency and the construct validity of SAQ-DK-PRIM; 3) present Danish benchmarking data; and 4) analyse variance between healthcare service type.
Methods
A cross-cultural adaptation and validation process was applied. The new version of the SAQ-DK adapted for primary care (SAQ-DK-PRIM) was distributed across three different healthcare services in primary care.
The SAQ-DK
The SAQ-DK was reported by Kristensen et al as a valid and reliable adaptation of the SAQ to assess patient safety climate in Danish hospitals20 based on the generic version of the SAQ (SAQ) originally developed by Sexton et al in 2006.19 The SAQ comprises six major subscales and 31 items, including teamwork climate (six items), safety climate (seven items), job satisfaction (five items), stress recognition (four items), working conditions (four items) and perceptions of unit/hospital management (five items).19 The SAQ-DK comprises the original 6 subscales and 31 items as well as items regarding demographic information.20 Responses are given on a 5-point-Likert-scale: 1: disagree strongly, 2 = disagree slightly, 3 = neutral, 4 = agree slightly, 5 = agree strongly. Furthermore, SAQ-DK allows responders to select “not applicable” as a possible answer. Items 2 and 11 of SAQ-DK are negatively worded.
Adaptation of the SAQ-DK to SAQ-DK-PRIM for Use in Danish Primary Care
The SAQ-DK was adapted into primary care following modified principles adapted from Beaton et al, which involved a pilot study, and a refinement process via an expert panel.30 To embark on the primary objective, representation of context-specific management was crucial throughout the adaptation process. When doing cross-cultural adaptation, an essential last step, according to Beaton et al, is to assess psychometric properties of the adapted version. Guidelines reported by Beaton et al are accepted to guide cross-cultural adaptational processes, with no golden standards reported.30 These include not only adaptation of questionnaires but also emphasizes the importance of performing new psychometric tests of the adaptations. To confirm a hypothesized, adapted model, Confirmatory factor analysis can be used.
Study Setting and Sample
The Danish healthcare system is mainly part of public administration, financed through general taxes. Healthcare delivery is based on free and equal access to the healthcare system. Overall, The Danish regions and municipalities are responsible for healthcare delivery, including 98 Municipalities.
Aarhus is a principal municipality with 340.275 registered inhabitants, where 42.694 are aged 67 or above. A total of 43 public, non-private nursing homes, 32 homecare units and 12 healthcare units are registered, covering a total of approximately 5900 employees, and 15 defined professions.
Three different types of healthcare services focusing on the elderly were included: 1) Nursing homes: A home for elderly in need of 24-hours health and care,31 2) Homecare units: Healthcare delivered at home, for citizens living in their own home, and 3) Healthcare units: Rehabilitation and nursing services delivered outside the home, for citizens living in their own home.
All healthcare workers with patient contact, and with permanent positions (N = 1064) in nursing homes (N = 11), homecare units (N = 4) or health units (N = 2) were invited. Invitees included social- and healthcare helpers, social- and healthcare assistants, nurses, local managers, and others (eg, dieticians, physio therapists, occupational therapists).
Data Collection
Data were collected between November 2017 and June 2018. The municipal risk manager was appointed data responsible project manager.
The SAQ-DK-PRIM was distributed to 1064 eligible respondents through e-mails. Time-to-respond was 3–6 weeks across healthcare service types. Participation was monitored weekly, and reminders to invitees were sent after 2 weeks, and repeated weekly for a maximum of 3 weeks. Local managers were informed about the participation rate in their healthcare service weekly, enabling their support for participation.
Data Management and Processing
SAQ item scores were described as %-agree (“agree strongly” or “agree slightly”), %-disagree (“disagree strongly” or “disagree slightly”), %-neutral and %-not applicable, item mean scores, and standard deviations (SD). For this purpose, item scores were converted to a 0- to 100-point scale, where disagree strongly = 0, disagree slightly = 25, neutral = 50, agree slightly = 75, and agree strongly = 100 (not applicable = no value). Missing answers were eliminated from the item statistics. For a single negatively worded item (item 5) the score was reversed before analysis, so that its valence matched the positively worded items. Item mean scores were calculated as the total sum of scores, for the individual item, from 0 to 100 from all respondents divided by the number of responses.
Two different outcome scores were used for safety climate scale (item 1–7): Scale mean score and % positive respondents: 1) Scale mean score was calculated as the total sum of scores from 0 to 100 from all respondents divided by the number of responses. The scale mean score was calculated using a denominator that excluded non-respondents and respondents answering, “not applicable”; 2) % positive respondents were calculated as the proportion of respondents with an individual scale mean score of 75 or higher. The percentage of positive respondents was calculated using a denominator that excluded non-respondents and respondents answering, “not applicable”.
Categorical baseline characteristics were reported by counts and percentages using chi-square tests for comparisons. The analyses of construct validity, reliability, benchmarking data, and variance was limited to SAQ-DK-PRIM safety climate scale (item 1 to item 7) and only for the complete cases of the respective items. Construct validity and the internal reliability were evaluated at scale- and item-level. SAQ-DK-PRIM item descriptions are presented in Box 1. Stata 18 was used for the analysis (StataCorp. 2023. Stata Statistical Software: Release 18. College Station, TX: StataCorp LLC).
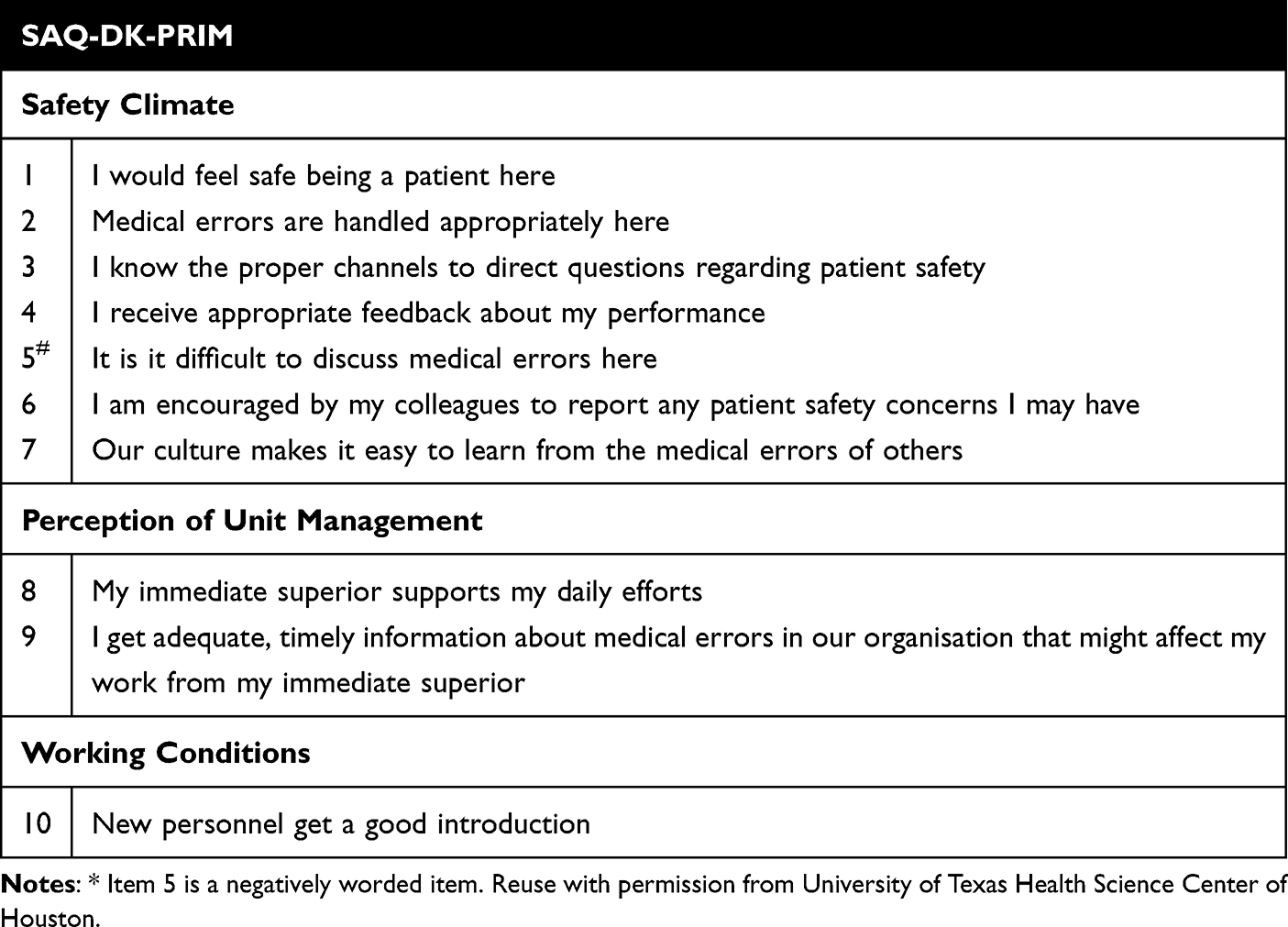 |
Box 1 The SAQ-DK-PRIM Questions. SAQ-DK-PRIM is a Short Version Only Covering the Subscale Safety Climate (7 Items) and Additional Selected Questions from the Subscales Perception of Unit Management and Working Conditions |
Construct Validity
A hypothesized one-factor model, derived from the SAQ-DK and referred to as the safety climate scale (items 1–7), was tested using confirmatory factor analysis, including the entire sample of 586 respondents from three types of healthcare service. Confirmatory factor analysis using structural equation models on five models were performed for construct validity. Formulating the factor analysis model as a structured equation model (SEM), the reported fit of the model was the chi-square statistics (Chi2, degrees of freedom (df)), the comparative fit index (CFI), and the root mean square of approximation (RMSEA). The following threshold values were used for an acceptable model fit: χ2/df <5.00 as suggested by Wheaton et al.32 CFI > 0.90 as suggested by Bentler.33 RMSEA < 0.06 as suggested by Bentler33 and the probability RMSEA (probability RMSEA > 0.05) as suggested by Browne and Cudeck.34 RMSEA 90% CI lower bound <0.05 ≤ good fit, RMSEA 90% CI upper bound >0.10 ≤ poor fit, P-value for the test of close fit (P(RMSEA < 0.05)) is > 5%, CFI > 0.9 and standardized root mean square residual (SRMR) is close to 0.
Internal Reliability
The internal consistency reliability of the adapted questionnaire was described by Cronbach’s alpha, a measure of internal consistency. Collections of items hypothesized as a factor were regarded as closely related if Alpha exceeded 0.70.35 The item-rest correlation, ie, the correlation between the score on the item and the total scale score of the other items in the scale, and the Cronbach’s alpha for the test scale, which consists of all but the one item are also reported. Inter-Item correlations were examined to investigate item discrimination as was done by Kristensen et al.20 Item discrimination was regarded acceptable if the correlation coefficients exceeded 0.30 as per Hair et al.36
Item Description
For each item, the number of respondents, the proportions of respondents agreeing, disagreeing, and being neutral are reported as well as the mean of the item score, and the standard deviation of the score.
Benchmarking Data
Benchmarking data were presented for the entire sample and for the nursing home, homecare units and healthcare units, respectively, as percent of respondents with a positive attitude (% positive) and scale mean scores and SD. Results of the three types of healthcare services were compared.
Variance
Analysis of variance (ANOVAs) was performed to test for significant between-service variability in scale mean scores within the subsamples of the three healthcare services, respectively. Organizational-level variance in safety climate was calculated by the intraclass correlation coefficient (ICC): the ratio of the variance at healthcare service type to the total variance in the data. Multiplied by 100 the ICC can be read as the percentage of the total variance in the data set that belongs to the organizational level. An ICC of 10 (%) or more, is commonly seen as a strong clustering of scores by organizational units.37,38 The Akaike Information Criterion (AIC), where smaller values mean better model fit, was applied to compare the models.39,40
Ethics
The project was approved by the Management in the Municipality of Aarhus (represented by co-author Kirsten Høgh Obling). According to Danish legislation, no formal permission from the national or regional Committee on Health Research Ethics was required for this type of study for two reasons: 1) it only included questionnaires and interviews (not related to health issues), and it did not include collection of biological material;41 2) According to the Danish Health Care Act the project, classified as a quality study, with the purpose of developing and improving the quality of patient care, does not require any additional ethic assessment according to Danish legislation.42. The study was conducted in compliance with the General Data Protection Regulation and registered at the Municipality of Aarhus (EMN-2017-056312). The participants were informed that participation was voluntary and anonymous that all answers would be treated with confidentiality.
Results
Adaptation
Item-reduction was required from the top management including the head of quality and safety of The Municipality of Aarhus, to meet actual resources (including language barriers and time limitations in the clinical setting) as well as relevance for primary care. Also, previous experiences from survey studies within the Municipality showed that 10 items were considered maximum regarding participants capacity and motivation. Thus, a maximum of 10 items focusing on the core activities within patient safety and clinical risk management in primary care was aimed for. Surveying the culture was a quality initiative to support the implementation of the mandatory reporting adverse events in primary care, and it was desired to have a tool to support patient safety work in primary care going forward. With this focus, an expert panel including leaders, researchers and quality consultants selected the 10 items. Some items were omitted due to their perceived complexity or relevance in relation to others, and the core patient safety/risk management work. Understanding of the 10 selected questions and the questionnaire help text was tested on municipal employees with direct citizen contact through semi-structured interviews. After the interviews, it became clear that it was necessary to develop more detailed help texts to ensure comprehensibility. The final version of the SAQ-DK-PRIM for use in Danish primary care comprised 10 items, covering the subscale safety climate (items 1 to 7) from the original SAQ-DK added additional two items from the SAQ-DK subscale perception of unit management (items 8–9) and one item related to the subscale working condition (Item 10) (Box 1). Minor changes in question wordings were made to tailor the questionnaire to a specific primary care setting. Content validity was established through consensus-building in an expert-group (N = 5) to produce a pre-final adaptation of the SAQ-DK-PRIM for pilot testing. Members of the expert group were purposively recruited to ensure relevant linguistic skills, knowledge of terminology as well as experience with both clinical and patient safety work in Denmark, including the original developer of the SAQ-DK.20 A pilot test was conducted through qualitative interviews with a variety of healthcare workers with contact to patients. As a result of the pilot test, help texts were developed by the expert group and added to all items (N = 10), to guide the respondent to respond to the items focusing on the work processes, and the conditions related to the safety of their clients. With the purpose to get feedback and suggestions on the wording of SAQ-DK-PRIM (including help text), face validity was assessed in a target population group pilot test (N = 13) of the pre-final adapted questionnaire. The pilot test included qualitative, individual interviews with representants from the three different healthcare services.
Psychometric Testing
Sample
Of 1064, a total of 830 questionnaires were returned (78%), however 199 only provided descriptive information, 43 returned incomplete safety climate scores and 2 answered “not applicable” for one of the questions in the safety climate scale. In total 244 (29.4%) questionnaires were incomplete. Thus, 586 complete questionnaires with 436, 101 and 49 from nursing home, homecare, and healthcare unit subsamples, respectively, were included in the analyses.
Respondent Characteristics
Respondent characteristics are provided in Table 1. Respondents were predominantly female (89.1%). The prevailing work pattern exhibited a leaning towards part-time employment, with 30 to 36 hours of engagement (55.7%). This trend was consistent across nursing homes, homecare, and healthcare units.
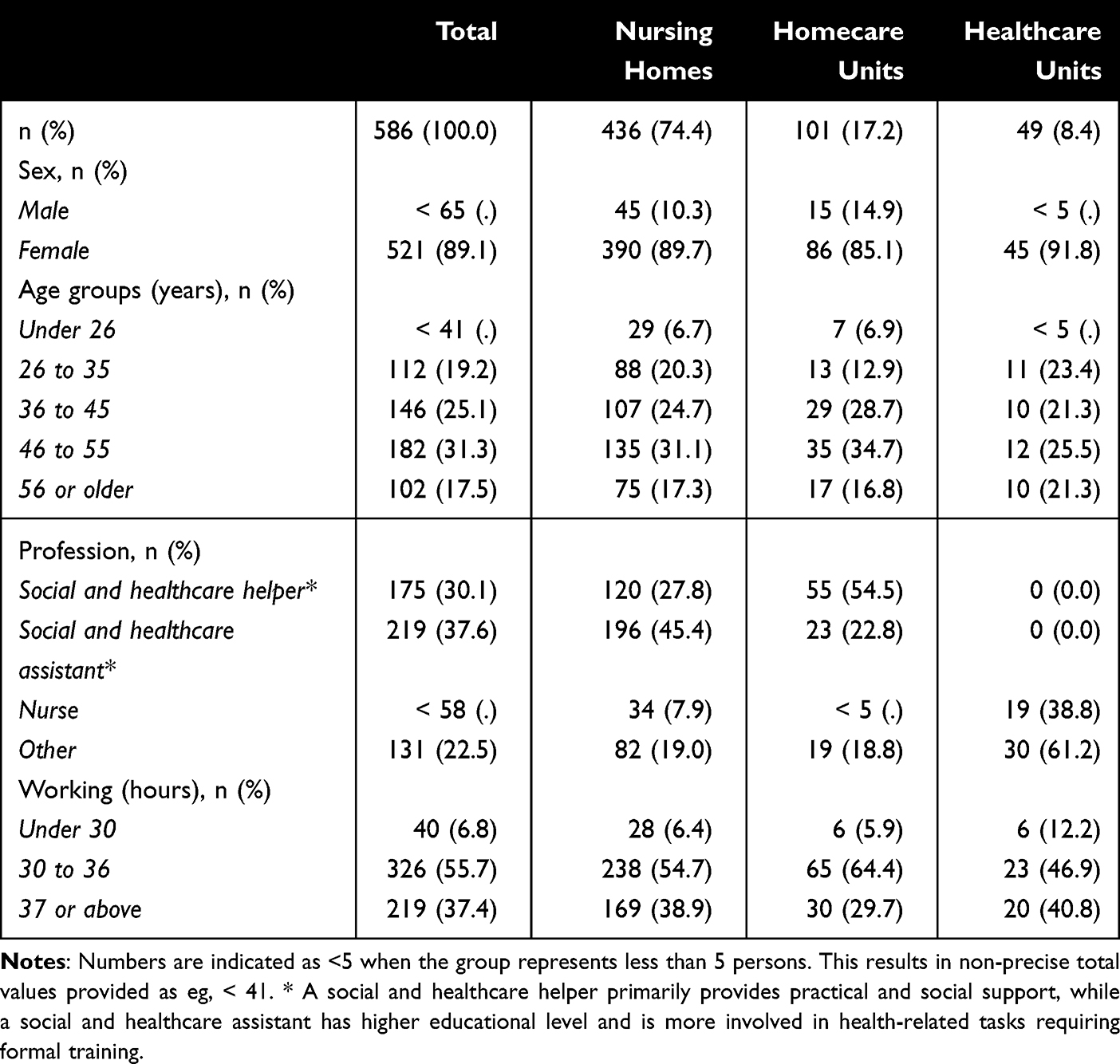 |
Table 1 Respondent Characteristics |
Most responses emanated from non-academic healthcare workers, including social and healthcare assistants (N=219; 37.6%) and social and health helpers (N = 175; 30.1%). In healthcare units, the proportion of nurses was higher (N = 19; 38.8%) compared to nursing homes (N = 34; 7.9%) and homecare units (<5). Also “other professions”, including general practitioners were more present in the subsample of healthcare units (N = 30; 61.2%) compared to both nursing homes (N = 82; 19%) and homecare units (N = 19; 18.8%).
Construct Validity
Construct validity of SAQ-DK-PRIM was investigated by testing the one-factor structure. Results of the confirmatory factor resulted in an acceptable fit of the hypothesized factor (safety climate) to data. Results of the CFA revealed the goodness-of-fit indices shown in Table 2.
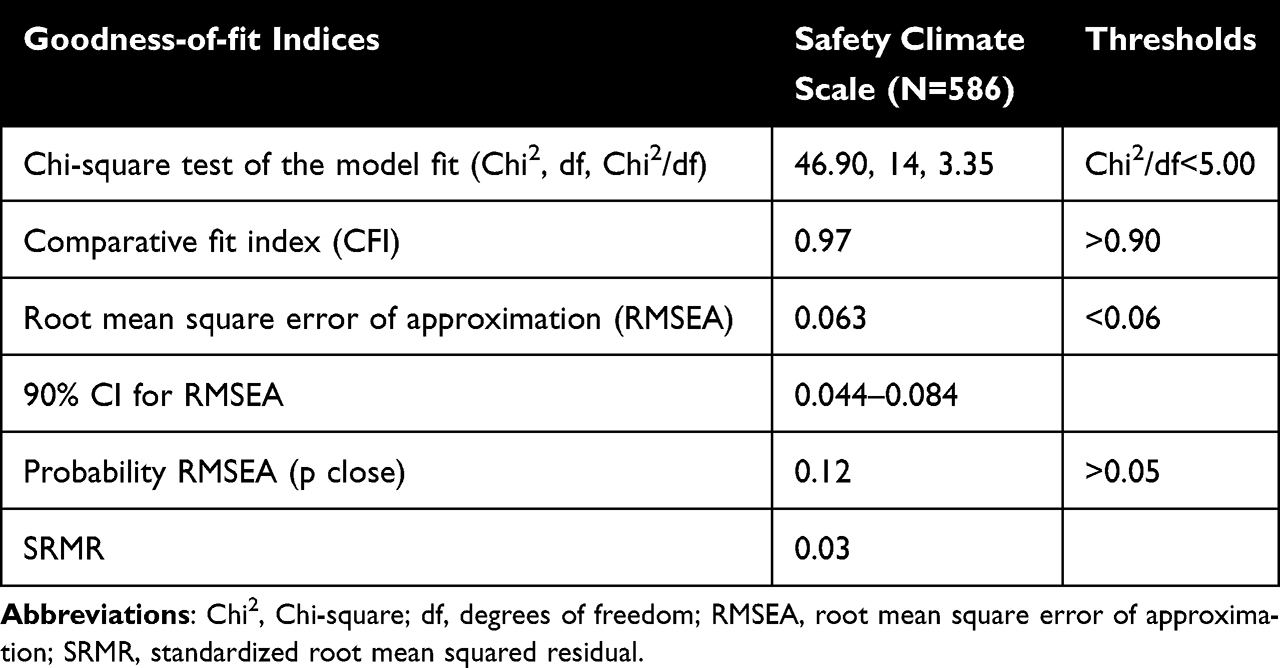 |
Table 2 Goodness-of-Fit Results of the Confirmatory Factor Analysis for SAQ-DK-PRIM “Safety Climate” Scale |
All model-of-fit indices fulfilled the threshold criteria for a good model fit set prior to the analysis. The chi-square test of the model fit revealed a Chi2/df ratio of 3.35, which as desired is below the maximum limit of 5.00. The CFI exceeded the threshold value of 0.90, as also desired. The RMSEA was not below the threshold value of 0.06, but close. Finally, the probability of RMSEA (p close) was above the threshold of 0.05, as wanted.
Internal Reliability
In the last two columns of Table 3, the item-rest correlation, ie, the correlation between the score on the item and the total scale score of the other items in the scale, and the Cronbach’s alpha for the test scale, which consists of all but one item are reported. Item 5 “It is it difficult to discuss medical errors here” had a low item-rest correlation (0.03), indicating a weak relationship with the other items in the hypothesized factor. All other items correlated modestly to well with the sum of other items. By excluding item 5, the Cronbach’s alpha for the test scale would increase to 0.82. Results indicated a good level of internal consistency/scale reliability with Cronbach’s alpha being 0.76 of the safety climate scale (Item 1–7). Inter-item correlations ranged from −0.07 to 0.57 (Table 3). Only item 5 had an inter-item correlation below the anticipated threshold value of 0.30. Thus, no relationship between item 5 and the other items in the scale was present.
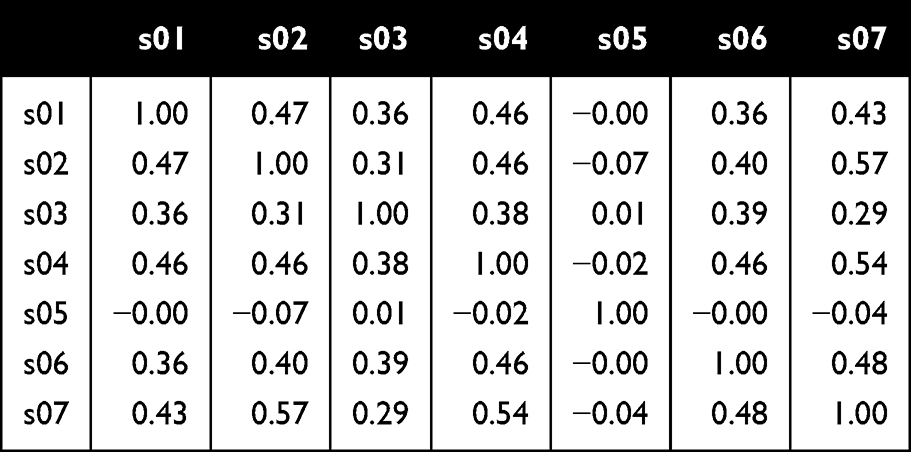 |
Table 3 Inter-Item Correlations of SAQ-DK-PRIM Safety Climate Scores (N=586) |
Item Descriptions
Table 4 shows item mean scores of SAQ-DK-PRIM safety climate scale with standard deviations for each of the 7 items including one negatively worded item (item 5 “It is it difficult to discuss medical errors here”). In addition, item mean scores for the three additional items are provided. All items were observed holding full range of scores between 1 and 5.
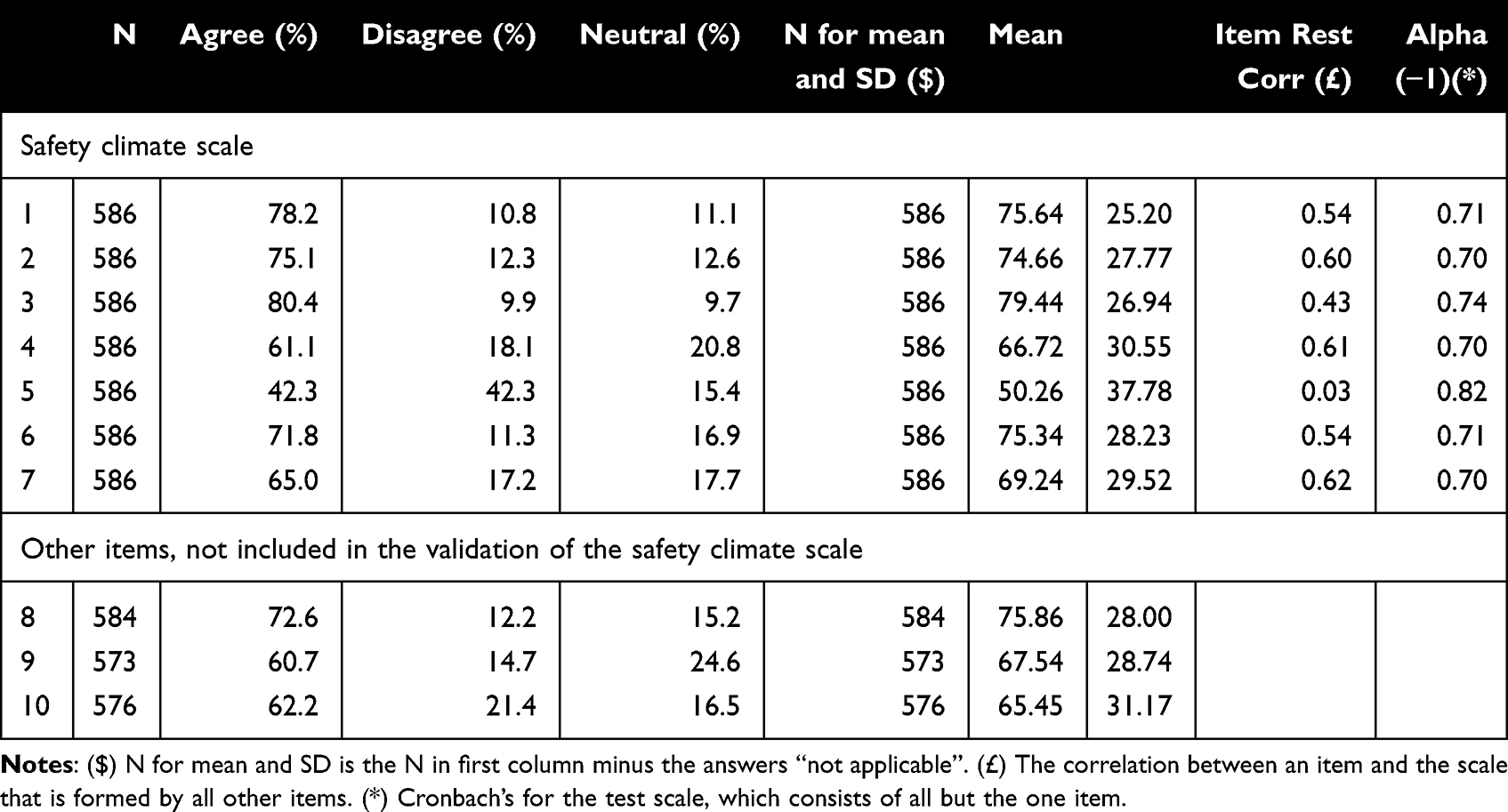 |
Table 4 SAQ-DK-PRIM Scores. Item Descriptions as Proportion of Agreeing, Disagreeing, Answering Neutral or “Not Applicable” and Mean and Standard Deviation for the Score (0–100) |
Missing values at the item level ranged from 0 to 13 (0–2.2%), with increasing tendency from increasing item number of item.
For positive worded items (1 to 4 and 6 to 10), item mean scores were all above 60, reflecting agreement. The highest mean score was found in item 3 “I know the proper channels to direct questions regarding patient safety” [79 (26.94)] and item 1 “I would feel safe being a patient here” [76 (25.20)]. A positive skew of responses was found with indications of variation. Item 3 showed highest %-agree (80.4%), with lowest %-agree revealed from item 9 (60.7%). The strongest disagreement was found in item 10 “New personnel get a good introduction” (21.4%).
Regarding the negatively worded item 5 “It is it difficult to discuss medical errors here” %-agree was 42.3% and %-disagree 42.3% (after item reversal).
Benchmarking Data
Table 5 provides benchmarking data. Proportions of participants with a positive attitude towards safety climate was 41.1% (N = 586) and did not differ between the three types of healthcare services. Scale mean score was 70.19; SD = 18.05 and was different between the three types of healthcare services.
 |
Table 5 Benchmarking Data for the Entire Sample and for the Three Types of Healthcare Services |
Variance
Four respondents did not provide their age and were therefore not included in the analysis of variance. Distribution of respondents across units are provided in Table 6.
 |
Table 6 Distribution of Respondents Across Types of Health Care Services |
The safety climate scale scores did not vary according to type of healthcare service. ICC was 0.68% indicating low clustering of scores by type of healthcare service (Table 7).
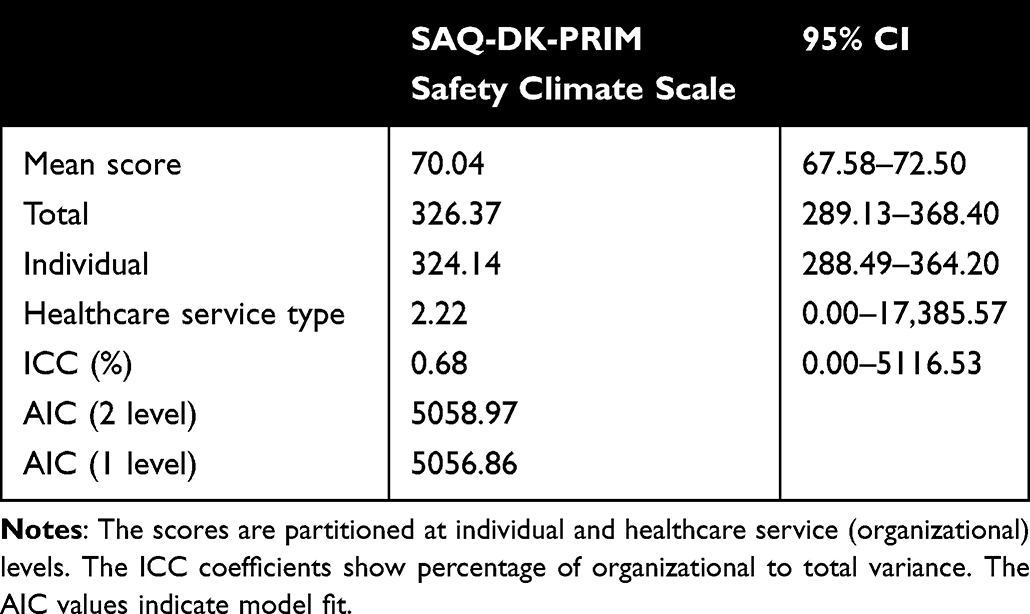 |
Table 7 Total Variance of SAQ-DK-PRIM Safety Climate Scores (N=586) |
Discussion
The successful cross-cultural adaptation of the SAQ-DK for primary care context culminated in the SAQ-DK-PRIM, demonstrating acceptable psychometric properties. Validation of the SAQ-DK-PRIM attests to its validity and reliability in assessing the patient safety climate within nursing homes, homecare units and healthcare units, representing differing healthcare services within Danish primary care, all concerning healthcare delivery of people older of age. Being the focal point of this assessment is the single-factor structure of the SAQ-DK-PRIM, resonating with the primary objective of this study to tailor the questionnaire to primary care’s unique settings and challenges.
Sample Representativeness and Characteristics
Danish municipalities employ mostly females aged between 35 and 55 years, including social- and healthcare assistants and helpers representing by far the largest sub-group of professionals.43 Results are therefore representative of the actual primary care settings under investigation, including a sample of middle-aged, female social and healthcare assistants-and helpers, primarily employed part-time. Response rate was high compared to other studies on different versions of SAQ in international primary care settings,4 possibly reflecting an overall acceptance, adaptation ability and perceived usefulness/value of the very short 10-item SAQ-DK-PRIM. In this study, the integrative aspect of the design ensured local management support, directly addressing structural issues concerning time and resource limitations within the primary care context. In fact, the overall response rate was high if noticing the multiple barriers and possible questionnaire-fatigue within the included primary care setting. The managerial support and quality initiative could have increased attention towards overall patient safety, with higher response rates as a result.
Primary Care Settings
International studies referring to relatively comparable healthcare systems to the Danish have reported samples similar to the sample included in this study. In the Netherlands, 62% of the respondents in a study investigating patient safety climate though use of SAQ in long-term-care setting were licensed practical nurses.26 This corresponds with the findings of this study, where approximately one-third of the respondents were social and healthcare assistants and helpers, respectively. Nevertheless, important variations in the types of healthcare services included in the analysis are to be noticed. In the Dutch study, spanning nine long-term healthcare facilities across the country, only one-fifth of respondents provided nursing care, with most employed in residential care (77%).26 Oppositely, in a Norwegian study, nursing homes were the primary focus of analysis, including five nursing homes. Almost half of the respondents were nursing assistants.44 Nevertheless, the Norwegian nursing homes were in a single town with relatively few inhabitants reported,44 compared to this study based on a principal municipality in Denmark. Thus, demographical results related to respondents in this study correspondent to western European studies in terms of respondent characteristics, but great variation in number and characteristics of included healthcare services limits further comparison. Focus on a single, principal municipality of Denmark, is a strength of this study in terms of safety climates, as all types of healthcare services are subject to the same multiple moderating organizational factors at municipal level that may influence the patient safety culture, compared to inclusion of healthcare services potentially representing multiple different organizational factors. Nevertheless, this narrow focus could also limit generalizability and applicability to the overall Danish primary care settings and international settings that may differ from the investigated setting. For example, contextual factors may affect safety attitudes within an organization. These factors encompass a range of influences differing across settings and countries such as, eg, organizational culture, leadership, environmental conditions, individual characteristics, and external regulations. Therefore, more studies targeted other primary care contexts with focus on comparability in number and location are clearly needed to support generation of clear evidence within the field of patient safety culture and related climate in nursing homes in general.
Results from countries other than Europe seem to report more varying samples,4 leaving the results of this study to reflect important primary care workforce differences across different healthcare systems. In the present study, the inclusion of different healthcare services did indicate differences in respondent characteristics and benchmark data. Social- and healthcare assistants were found significantly more represented in nursing homes and homecare units compared with their non-representation within healthcare units. Healthcare units, on the other hand, were represented by a subsample including more registered nurses. Thus, healthcare units mirror studies from nursing homes in the US, where nurses seem to be more present than in the Danish nursing home context.
In this study, nursing homes and homecare units were predominantly represented by professions being of non-academical healthcare professionals, whereas this trend was not seen in healthcare units, where a higher proportion of nurses was seen. Despite overall positive perceptions of safety climate, scale mean scores differed significantly, with lower mean scores reported from healthcare units compared to nursing homes and homecare units. In contrast, no difference was seen when comparing % positive. The difference in scale mean scores may be attributed to the unique organizational structure and leadership styles. Additionally, the variation in educational levels reflected in profession, where nurses have the highest educational level, might play a role, with lower educational levels possibly leading to a greater felt need for support within risk-prone environments. However, the differences in scale mean scores may also be explained by other issues, not accounted for in this study and the inclusion of only two healthcare units in in the present study that may limit statistical power in the comparison. Thus, in future studies it could be beneficial to focus on settings with varying levels of academic and non-academic staff as well as specific professions. Academical education could increase knowledge and thereby awareness of safety hazards, leading to their identification, being an important step in prevention of harm in healthcare.45 Moreover, these nuances hint at the need for a granular understanding of how context and staff qualifications influence patient safety culture perceptions and supports doing a new cross-cultural-adaptation even when only seemingly small differences in healthcare settings are observed.
Important differences at other levels of the healthcare system have been reported. A Dutch study found significant more positive perceptions of safety climate in nursing and residential homes compared to inpatient settings (eg, Hospitals).26 These findings support our results, revealing relatively positive scores compared to those found in Danish hospitals by Kristensen et al.20 Findings therefore state the importance of acknowledging differences within sectoral organizational settings, supporting recommendations of cross-cultural adaptation when the target setting of a survey changes.30
Questionnaire Adaptation
Positive correlations have been revealed for 5 of the 6 SAQ-factors of the original SAQ, including safety climate internationally.26 Despite holding a narrow focus, the single-factor-focus of the SAQ-DK-PRIM holds promise in terms of safety climate. An important feature of SAQ-DK is the non-specific addressing of healthcare workers perceptions of multiple aspects of patient safety climate. This, however, could also represent a disadvantage, if staff are not familiar with the practical contents of the concepts of patient safety and medical error, which are frequently used in the SAQ-DK and SAQ-DK-PRIM questionnaire. Nevertheless, as this study was anchored to ongoing patient safety-related initiatives, managerial support was already in place, and eligible respondents were informed of these concepts before being invited to participate in the survey. Item 5 “It is it difficult to discuss medical errors here”, presented with a lower item mean in the present study. This may be explained by a potential lack of understanding of its meaning. However, in the present study, this limitation was minimized by the information given to support the knowledge concerning “unintended events” and “medical errors”, indicating useful results. Yet, comparison of item 5 in the SAQ-DK-PRIM with other SAQ adaptations should be performed with caution, taking the above points into consideration. In summary, the integrative approach was a strength of this study. Also, embedding of the research occurred at the level of experts, including an experienced researcher in patient safety climate and its assessment as part of the validation team.
Psychometric Tests
Goodness-of-fit-indices revealed acceptable levels for the total-hypothesized model. Even though the P-value was found under threshold when analyzing the “safety climate” related items solely (item 1–7), the co-tested indices were found at acceptable levels. A certain concern is that the item-lead to a decrease in statistical power. On the other hand, results of the revealed acceptable levels overall indicate a strong instrument, with added items potentially creating more acceptable levels.
Cronbach’s alpha of 0.76 for the total hypothesized model (SAQ-DK-PRIM) confirmed the robustness of the SAQ safety climate scale. This supports earlier SAQ studies within primary care settings4 and leaves the SAQ-DK-PRIM as a useful instrument adding value to existing knowledge.
Benchmarking Data
A noteworthy stride lies in the potential for benchmarking across diverse healthcare sectors. The adaptation of the SAQ for both primary care and hospital settings permits cross-national comparisons, particularly within the European and Scandinavian framework. This, in turn, paves the way for collaborative learning and sharing of best practices, fostering improvements in patient safety culture.
Previously, four studies have presented descriptive data for SAQ in comparable primary care settings: eg, homecare setting, nursing and residential homes.4 The present study demonstrated a safety climate scale mean score of 70.19. Comparatively, it falls within the range of scores reported in other studies.26,44,46,47 Lousada et al and Buljac-Samardzic et al reported slightly lower mean safety climate scores in studies from Brazil and The Netherlands respectively,26,46 while Bondevik et al reported a score close to the present study in a Norwegian study.44 The Swiss study by Züniga et al had a different design where subscales were merged.47 Thus, it is challenging to draw direct comparisons to the present study. None of the four previous studies reported % positive scores, although it is recommended by the developers of SAQ.48 In summary, the present study’s safety climate score aligns with or slightly surpasses the mean scores reported in the other studies, seemingly showcasing a generally positive safety climate in the respective primary care settings. However, the low percentage of positive respondents highlights a potential lack of consensus among staff, which is important since climate levels with higher consensus among unit members better predict patient safety.49 Variation in staff consensus may be explored further in future studies in primary care. It is therefore essential to interpret the findings regarding variation in this study cautiously.
Variance
Contrary to studies based on US nursing homes, our results support findings from more comparable healthcare systems, including the Norwegian- and Dutch nursing- and residential- homes. Focus on variance could therefore be beneficial, not directing improvement efforts towards what’s “most negatively perceived”, instead investigating underlying factors contributing to the variance. Analysis of variance revealed that the safety climate scale scores did not vary according to type of healthcare service, whereas variance to a high degree could be attributed to individual variation. Thus, the lower scale mean score reported by healthcare units may be explained by individual variance. Total variance of the safety climate scale was comparable to that found in a previous Norwegian study investigating general practitioner practices and out-of-hour clinics.39 Three studies have investigated organizational variance of SAQ in primary care where organizational variance of 8% to 16.4% were found.4 But in those studies, variance was analyzed at the work unit level and not according to the types of healthcare services, as in our study. Low variance between the three types of healthcare services found in our study may be explained by the fact that they were comparable in organizational structure and leadership style. This complies with theory and other studies indicating that priorities at higher organizational levels are modified by local leaders in a way that increases variation in safety climate the closer to the frontline it is analyzed.50,51
Strengths and Limitations
The study’s strengths include robust data collection and alignment with quality processes. However, the reduction in items and focus on response rates come with trade-offs. However, the study’s strategic decision to reduce the number of questionnaire items aligns with resource constraints and concerns over respondent fatigue. This pragmatic approach is in harmony with patient safety perspectives, emphasizing domain-specific focus over extensive assessment. While item reduction may impact statistical power, it aligns with the evolving complexity of patient safety culture research and the need for targeted insights. The cross-cultural adaptation process with relevant stakeholders for face- and content validity together with psychometric validation strengthens this study. Another strength is the sample size and representativeness, which supports statistical power. Yet, the same representativeness minimizes the potential for direct comparison both across national healthcare sectors and international healthcare system-borders, why more studies are needed. Data collection occurred in 2017–2018, preceding the COVID-19 pandemic. The potential influence of the pandemic and the related health care processes on patient safety culture in primary care settings cannot be excluded. Nevertheless, these data provide valuable pre-pandemic benchmark information. To assess the possible impact of the pandemic, further studies are necessary and may be compared to these pre-pandemic findings.
Conclusions
Considering the questionnaire’s applicability, short length, strengthened focus on one area of interest and validity, the SAQ-DK-PRIM serves as a valuable tool for measuring patient safety climate. Use of the SAQ-DK-PRIM may therefore support ongoing work to assess patient safety climate within primary care settings. Overall mean benchmarking scores were high. We did not have data to analyze variance at work unit level in the Danish primary care settings, which may have demonstrated potential opportunities to intervene on patient safety climate at ward and work unit level. As SAQ adaptations are now available for use in both Danish hospitals and primary care, it is possible to generate comparable benchmarking data, implying possible learning across healthcare sectors too.
Acknowledgments
We would like to express our sincere gratitude to the municipality of Aarhus for their invaluable contribution to the crucial work on patient safety. Additionally, we extend our thanks to all the leaders and participants involved in the distribution and completion of questionnaires. Their dedication and effort have been pivotal in gathering essential data, shaping our study.
Funding
Salary for the first author MHJ was covered by VELUX FONDEN (00034143) whom we greatly acknowledge for funding a study leading to this validation study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Patient safety. World Health Organization.
2. WHO. Global Patient Safety Action Plan 2021–2030; 2021. Available from: https://www.who.int/teams/integrated-health-services/patient-safety/policy/global-patient-safety-action-plan.
3. Dennis S, Short SD, Abdulhadi NN, Abdulhadi NN. Patient safety and safety culture in primary health care: a systematic review. BMC Fam Pract. 2018;19(1):104. doi:10.1186/s12875-018-0793-7
4. Olesen AE, Juhl MH, Deilkås ET, Kristensen S. Review: application of the Safety Attitudes Questionnaire (SAQ) in primary care - A systematic synthesis on validity, descriptive and comparative results, and variance across organisational units. BMC Prim Care. 2024;25(1):1–26. doi:10.1186/s12875-024-02273-z
5. Halligan M, Zecevic A. Safety culture in healthcare: a review of concepts, dimensions, measures and progress. BMJ Qual Saf. 2011;20(4):338–343. doi:10.1136/bmjqs.2010.040964
6. Palmieri PA, Peterson LT, Pesta BJ, Flit MA, Saettone DM. Safety culture as a contemporary healthcare construct: theoretical review, research assessment, and translation to human resource management. In: Fottler MD, Khatri N, Savage GT editors. Strategic Human Resource Management in Health Care. Vol 9. Advances in Health Care Management. Emerald Group Publishing Limited; 2010:97–133. doi:10.1108/S1474-8231(2010)0000009009
7. Churruca K, Ellis LA, Pomare C, et al. Dimensions of safety culture: a systematic review of quantitative, qualitative and mixed methods for assessing safety culture in hospitals. BMJ Open. 2021;11(7):e043982–e043982. doi:10.1136/bmjopen-2020-043982
8. Guldenmund FW. The nature of safety culture: a review of theory and research. In: Safety Science. Vol. 34. Elsevier Sci Ltd; 2000:215–257. doi:10.1016/S0925-7535(00)00014-X
9. Reiman T, Pietikäinen E, Oedewald P. Multilayered approach to patient safety culture. Qual Saf Health Care. 2010;19:e20. doi:10.1136/qshc.2008.029793
10. De Bienassis K. Culture as a cure: assessments of patient safety culture in OECD countries. OECD Heal Work Pap. 2020;119. doi:10.1787/6ee1aeae-en
11. Mazzuco de Souza M, Dal Ongaro J, Carpes Lane T, Andolhe R, Bernat Kolankiewicz AC, Bosi de Souza Magnago TS. Patient safety culture in the Primary Health Care. Rev Bras Enferm. 2019;72(1):27–34. doi:10.1590/0034-7167-2017-0647
12. de Wet C, Spence W, Mash R, Johnson P, Bowie P. The development and psychometric evaluation of a safety climate measure for primary care. Qual Saf Heal Care. 2010;19(6):578LP–584. doi:10.1136/qshc.2008.031062
13. Bartoníčková D, Kalánková D, Žiaková K. How to Measure Patient Safety Culture? A Literature Review of Instruments. Acta Medica Martiniana. 2021;21(2):69–79. doi:10.2478/acm-2021-0010
14. Singla AK, Kitch BT, Weissman JS, Campbell EG. Assessing patient safety culture: a review and synthesis of the measurement tools. J Patient Saf. 2006;2(3):105–115. doi:10.1097/01.jps.0000235388.39149.5a
15. Azyabi A, Karwowski W, Davahli MR. Assessing patient safety culture in hospital settings. Int J Environ Res Public Health. 2021;18(5):1–36. doi:10.3390/ijerph18052466
16. Curran C, Lydon S, Kelly M, Murphy A, Walsh C, O’Connor P. A systematic review of primary care safety climate survey instruments: their origins, psychometric properties, quality, and usage. J Patient Saf. 2018;14(2):e9–e18. doi:10.1097/PTS.0000000000000393
17. Desmedt M, Bergs J, Vertriest S, et al. Systematic psychometric review of self-reported instruments to assess patient safety culture in primary care. J Adv Nurs. 2018;74(3):539–549. doi:10.1111/jan.13464
18. Godycki-Cwirko M, Esmail A, Dovey S, et al. Patient safety initiatives in Central and Eastern Europe: a mixed methods approach by the LINNEAUS collaboration on patient safety in primary care. Eur J Gen Pract. 2015;21(sup1):62–68. doi:10.3109/13814788.2015.1043727
19. Sexton JB, Helmreich RL, Neilands TB, et al. The Safety Attitudes Questionnaire: psychometric properties, benchmarking data, and emerging research. BMC Health Serv Res. 2006;6(1):44. doi:10.1186/1472-6963-6-44
20. Kristensen S, Sabroe S, Bartels P, Mainz J, Christensen KB. Adaption and validation of the safety attitudes questionnaire for the Danish hospital setting. Clin Epidemiol. 2015;7:149–160. doi:10.2147/CLEP.S75560
21. Madden C, Lydon S, O’Dowd E, Murphy AW, O’Connor P. A Systematic Review of Patient-Report Safety Climate Measures in Health Care. J Patient Saf. 2020;16(1):1–10. doi:10.1097/pts.0000000000000705
22. Singer S, Lin S, Falwell A, Gaba D, Baker L. Relationship of safety climate and safety performance in hospitals. Health Serv Res. 2009;44(2P1):399–421. doi:10.1111/j.1475-6773.2008.00918.x
23. Abstoss KM, Shaw BE, Owens TA, Juno JL, Commiskey EL, Niedner MF. Increasing medication error reporting rates while reducing harm through simultaneous cultural and system-level interventions in an intensive care unit. BMJ Qual & Saf. 2011;20(11):914LP–922. doi:10.1136/bmjqs.2010.047233
24. Thomas KS, Hyer K, Castle NG, Branch LG, Andel R, Weech-Maldonado R. Patient Safety Culture and the Association with Safe Resident Care in Nursing Homes. Gerontologist. 2012;52(6):802–811. doi:10.1093/geront/gns007
25. Styrelsen for Patientsikkerhed. En rapport om Patientsikkerhed; 2016.
26. Buljac-Samardzic M, van Wijngaarden JDH, Dekker-van Doorn CM. Safety culture in long-term care: a cross-sectional analysis of the Safety Attitudes Questionnaire in nursing and residential homes in the Netherlands. BMJ Qual Saf. 2016;25(6):424–431. doi:10.1136/bmjqs-2014-003397
27. Smits M, Keizer E, Giesen P, Deilkås ECT, Hofoss D, Bondevik GT. Patient safety culture in out-of-hours primary care services in the Netherlands: a cross-sectional survey. Scand J Prim Health Care. 2018;36(1):28–35. doi:10.1080/02813432.2018.1426150
28. Smits M, Keizer E, Giesen P, Deilkås ECT, Hofoss D, Bondevik GT. The psychometric properties of the ‘safety attitudes questionnaire’ in out-of-hours primary care services in the Netherlands. PLoS One. 2017;12(2):e0172390. doi:10.1371/journal.pone.0172390
29. Singer S, Kitch BT, Rao SR, et al. An exploration of safety climate in nursing homes. J Patient Saf. 2012;8(3):104–124. doi:10.1097/PTS.0b013e31824badce
30. Beaton DE, Bombardier C, Guillemin F, Ferraz MB. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine. 2000;25(24):3186–3191. doi:10.1097/00007632-200012150-00014
31. Sanford AM, Orrell M, Tolson D, et al. An international definition for “nursing home”. J Am Med Dir Assoc. 2015;16(3):181–184. doi:10.1016/j.jamda.2014.12.013
32. Wheathon B, Muthén B, Alwin DF, Summers GF. Assessing reliability and stability in panel models. Sociological Methodol. 1977;8:84–136. doi:10.2307/270754
33. Bentler PM. Comparative fit indexes in structural models. Psychol Bull. 1990;107(2):238–246. doi:10.1037//0033-2909.107.2.238
34. Browne MW, Cudeck R. Alternative ways of assessing model fit. In: Bollen KA, Long JS, editors. Testing Structural Equation Models. Sage; 1993:136–162.
35. Pett MA, LAckey NR, Sullivan JJ. Making Sense of Factor Analysis. SAGE Publications, Inc.; 2003.
36. Hair JF, Black WC, Babin BJ, Andersen RE. Multivariate Data Analysis.
37. Kahn JH. Multilevel modeling: overview and applications to research in counseling psychology. J Couns Psychol. 2011;58(2):257–271. doi:10.1037/a0022680
38. Gulliford MC, Ukoumunne OC, Chinn S. Components of variance and intraclass correlations for the design of community-based surveys and intervention studies: data from the Health Survey for England 1994. Am J Epidemiol. 1999;149(9):876–883. doi:10.1093/oxfordjournals.aje.a009904
39. Deilkås ECT, Hofoss D, Hansen EH, Bondevik GT. Variation in staff perceptions of patient safety climate across work sites in Norwegian general practitioner practices and out-of-hour clinics. PLoS One. 2019;14(4):e0214914. doi:10.1371/journal.pone.0214914
40. Akaike H. A new look at the statistical model identification. IEEE Trans Automat Contr. 1974;19(6):716–723. doi:10.1109/TAC.1974.1100705
41. Komitéloven. Danske Love (Danish Laws). Available from: https://danskelove.dk/komitéloven/14.
42. Danish Research Ethics Committees. Overblik over anmeldelsespligten. Available from: https://videnskabsetik.dk/ansoegning-til-etisk-komite/overblik-over-anmeldelsespligten.
43. The Municipal Labor Market in Numbers 2021; 2022.
44. Bondevik GT, Hofoss D, Husebø BS, Tveter Deilkås EC, Deilkås ECT. Patient safety culture in Norwegian nursing homes. BMC Health Serv Res. 2017;17(1):1–10. doi:10.1186/s12913-017-2387-9
45. Auzoult L, Ngueutsa R. Attitude to safety rules and reflexivity as determinants of safety climate. J Safety Res. 2019;71:95–102. doi:10.1016/j.jsr.2019.09.016
46. Lousada LM, da Silva Dutra FC, da Silva BV, et al. Patient safety culture in primary and home care services. BMC Fam Pract. 2020;21(1):188. doi:10.1186/s12875-020-01263-1
47. Zúñiga F, Ausserhofer D, Hamers JPH, Engberg S, Simon M, Schwendimann R. The relationship of staffing and work environment with implicit rationing of nursing care in Swiss nursing homes - A cross-sectional study. Int J Nurs Stud. 2014;52(9):1463–1474. doi:10.1016/j.ijnurstu.2015.05.005
48. Pronovost P, Sexton B. Assessing safety culture: guidelines and recommendations. Qual Saf Heal Care. 2005;14(4):231–233. doi:10.1136/qshc.2005.015180
49. Zohar D, Livne Y, Tenne-Gazit O, Admi H, Donchin Y. Healthcare climate: a framework for measuring and improving patient safety. Crit Care Med. 2007;35(5):1312–1317. doi:10.1097/01.CCM.0000262404.10203.C9
50. Deilkås ECT, Hofoss D, Husebo BS, Bondevik GT. Opportunities for improvement in nursing homes: variance of six patient safety climate factor scores across nursing homes and wards—Assessed by the Safety Attitudes Questionnaire. PLoS One. 2019;14(6):e0218244. doi:10.1371/journal.pone.0218244
51. Zohar D, Luria G. A multilevel model of safety climate: cross-level relationships between organization and group-level climates. J Appl Psychol. 2005;90(4):616–628. doi:10.1037/0021-9010.90.4.616
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Validation of the Connor-Davidson Resilience Scale-10 in South Africa: Item Response Theory and Classical Test Theory
Pretorius TB, Padmanabhanunni A
Psychology Research and Behavior Management 2022, 15:1235-1245
Published Date: 16 May 2022
Validity and Reliability of the Thai Version of the 19-Item Compliance-Questionnaire-Rheumatology
Panichaporn S, Chanapai W, Srisomnuek A, Thaweeratthakul P, Katchamart W
Patient Preference and Adherence 2022, 16:2149-2158
Published Date: 17 August 2022
Psychometric Properties of the Montreal Cognitive Assessment (MoCA) to Detect Major Neurocognitive Disorder Among Older People in Ethiopia: A Validation Study
Daniel B, Agenagnew L, Workicho A, Abera M
Neuropsychiatric Disease and Treatment 2022, 18:1789-1798
Published Date: 22 August 2022
Development and Initial Validity of the Patients’ Literacy Scale Among Outpatients in Hangzhou City, China
Jiang D, Sang T, Xiao X, Wu Z, Wang H, Yang Q
Patient Preference and Adherence 2022, 16:2483-2496
Published Date: 7 September 2022
Research and Evaluation of a Cyberchondria Severity Scale in a Chinese Context
Wang D, Sun L, Shao Y, Zhang X, Maguire P, Hu Y
Psychology Research and Behavior Management 2023, 16:4417-4429
Published Date: 1 November 2023