Back to Journals » Patient Preference and Adherence » Volume 16
Development and Initial Validity of the Patients’ Literacy Scale Among Outpatients in Hangzhou City, China
Authors Jiang D, Sang T, Xiao X, Wu Z, Wang H ![]() , Yang Q
, Yang Q ![]()
Received 20 June 2022
Accepted for publication 26 August 2022
Published 7 September 2022 Volume 2022:16 Pages 2483—2496
DOI https://doi.org/10.2147/PPA.S379259
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Dongdong Jiang,1 Tian Sang,2 Xiaohua Xiao,1 Zhihua Wu,1 Hongmei Wang,3 Qian Yang1
1Center for Health Policy Studies, School of Public Health, The Children’s Hospital, and National Clinical Research Center for Child Health, Zhejiang University School of Medicine, Hangzhou, People’s Republic of China; 2Women’s Hospital, Zhejiang University School of Medicine, Hangzhou, People’s Republic of China; 3Department of Social Medicine of School of Public Health, and Department of Pharmacy of The First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, People’s Republic of China
Correspondence: Hongmei Wang, Department of Social Medicine of School of Public Health, and Department of Pharmacy of The First Affiliated Hospital, Zhejiang University School of Medicine, No. 866, Yuhangtang St, Hangzhou, Zhejiang Province, 310058, People’s Republic of China, Email [email protected] Qian Yang, Center for Health Policy Studies, School of Public Health, The Children’s Hospital, and National Clinical Research Center for Child Health, Zhejiang University School of Medicine, No. 866, Yuhangtang St, Hangzhou, Zhejiang Province, 310058, People’s Republic of China, Tel +86-187-5818-1126, Email [email protected]
Purpose: There are few studies on the intervention of the doctor–patient relationship (DPR) from patients’ perspective, because of lacking appropriate measurement instruments for the effect of the patient interveqntion. Understanding the status of patients’ literacy (the ability to initiatively obtain, read, and analyze health-related materials, make appropriate decisions, reduce risks of health-related problems) and developing the patients’ literacy scale (PLS) align with the interests of patients, doctors, and researchers.
Patients and Methods: This study was conducted in two stages: item building and item refinement. A total of 303 subjects were recruited from the outpatient hall in three hospitals with different levels in Hangzhou city, China. Twenty patients and seven experts determined the face and content validity, respectively. The construct validity, convergent, discriminant validity, and known-group validity of the scale were examined by exploratory and confirmatory factor analysis (EFA and CFA). Internal consistency, including Cronbach’s alpha, McDonald’s ω, split-half reliability, and composite reliability (CR), was also tested.
Results: The EFA of PLS showed that Kaiser–Meyer–Olkin (KMO) measure of sampling adequacy was 0.787, and Bartlett’s Test of Sphericity showed a significance of p < 0.001. The extracted four-factor (patient activation, knowledge, attitudes, practice) model explained 61.266% of the total variance. For the overall PLS, the Cronbach’s alpha, McDonald’s ω and split-half reliability coefficient were 0.815, 0.838 and 0.720, respectively. The CFA showed the goodness of fit (RMSEA = 0.065, CMIN/DF = 1.635, GFI = 0.900, CFI = 0.905, TLI = 0.909). The CR of each factor in this scale was 0.740, 0.732, 0.630, and 0.749, respectively.
Conclusion: This study showed that the PLS was valid and reliable to measure the patients’ literacy (PL). The 15-item PLS can help not only measure PL but also be used as a standard and advocacy target for patients’ behavioral model which can further improve the DPR.
Keywords: patients’ literacy, reliability, validity, outpatients, China
Introduction
It is almost universally acknowledged that the doctor–patient relationship (DPR) is tense in the world1–3 and receiving increasing attention from governments and scholars.4,5 Although the governments have legislated to prohibit violence against medical staff, the incidence of disputes between patients and medical workers is still rising.6,7 Existing research has manifested that the current tension between doctors and patients is not only caused by doctors8 but also by patients.9–11 There are few studies on the intervention of the DPR from patients’ perspective. This is because, there is a lack of appropriate measurement instruments for the effect of patient intervention. In addition, previous studies have clearly illustrated the responsibility and norms related to the role of doctors,12,13 while the responsibility and norms of patients were still undefined. Parsons first defined the sick role (or patients’ role) as a social role, in which patients were not only the sick individuals but also people with social expectations.12 A series of systems and social norms would strengthen these social expectations which lead patients to become more active to obtain health.12 However, the definition of patients’ role needs to be further improved for the theory of Parsons may not be applicable to changes in the current society.14
The initiative participation of patients in the doctor–patient-related matters has been regarded as a beneficial attempt for promoting DPR,15–17 which means that patients should be activated.18 Patient activation refers to patients with motivation, education, skills and confidence to make effective decisions to be responsible for their health.19 Patient activation requires the patients to believe the vital role in their health management and to actively obtain medical-related information and enhance their health literacy (HL). Therefore, patient activation would benefit for patients to seek medical treatment positively. It is worrying that patients’ performance cannot be determined. Relevant research has found that public adherence to control measures of some diseases was affected mainly by their knowledge, attitudes, and practices (KAP).20,21 People with great KAP may take positive efforts to avert the spread of disease20,22 and can also facilitate their course of diseases, especially those with chronic disease.23,24 The status of patients’ KAP is related to response to disease prevention and control, medical treatment, and personal health,25,26 which might be applicable in our study.
Nowadays, the threshold of seeing a doctor is higher for patients than before. On the one hand, the use of advanced medical technology has increased the information asymmetry between patients and doctors; on the other hand, social media (eg self-media, official account) has spread too much indiscriminate medical knowledge, which increased patients’ difficulties in making decisions on the contrary.27 All these new changes are urging patients to improve their comprehensive consulting abilities, such as the skills of communication, information acquisition and utilization, etc. To sum up, these abilities were collectively referred to as patients’ literacy (PL) in this study. In accordance with the theory of patients’ role, patient activation, and patients’ KAP, PL is defined as the ability to initiatively obtain, read, and analyze health-related materials, make appropriate decisions, reduce risks of health-related problems. To our knowledge, there are no specific scales for PL measurement. Most researchers use scales that measure HL to assess PL.28,29 They mainly test the ability of writing and reading or understand the prevalence among disease-specific HL of patients,29–31 rather than test patients’ comprehensive abilities. Moreover, these scales also exists several limitations: 1) focusing on only one dimension,32 2) focusing on only one specific disease,29,30 3) focusing on the awareness rate of medical knowledge,31,32 and 4) too many items to use conveniently.29–31
In China, the DPR is also facing the serious challenges. There were average 27 violence against medical workers per year recorded in each hospital in China in 2013.33 The Chinese government even has legislated to prohibit violence against medical staff in order to appeal to an end to infringement of the right of medical workers.6 However, laws and regulations, such as Regulation on the Prevention and Handling of Medical Disputes (RPHMD), only illustrate the ambiguous explanation regarding the rights of patients and lack the guidance of their responsibilities.34 RPHMD requires doctors to obey all laws and regulations to avoid risk, while it only requires patients to respect doctors and offer disease information honestly which is not enough. Moreover, research on DPR in China has found that the DPR in tertiary hospitals were worse than primary hospitals,35,36 and it is closely related to the lack of KAP among patients under the establishment of the National Hierarchical Medical System.37 Many Chinese scholars have introduced and developed several scales to measure HL, for example, Chinese version of health literacy survey tool European health literacy questionnaire (HLS-Asia-Q) for general Chinese population,38 cancer health literacy – 30/6 (CHLT-30/6-Chinese) for Chinese cancer patient population,39 short test of functional health literacy in adults (S-TOFHLA) for Chinese to assess functional health literacy,40 revised dental beliefs survey (DBS-R) for Chinese patients’ perception to dentist,41 etc. However, literature measuring the literacy (including KAP, activation) of patients is limited, especially outpatients. Therefore, this study combines the theory of KAP and patient activation, aiming to construct the indicator system of PL, develop the instrument of measuring PL, and prepare for future intervention studies from patients’ perspective. The specific objectives are to assess 1) internal consistency of the patients’ literacy scale (PLS), 2) item-total correlation, and 3) exploratory and confirmatory factor analysis.
Materials and Methods
Participants and Procedure
This study was conducted in two stages. The first stage was item building, which adopted the interview method; the second stage was item refinement, namely, primary evaluation of measurement properties, which included validity and reliability assessments.
Item Building
Interview
Using purposive sampling, participants (both patients and doctors) were selected in September 2019 from a comprehensive hospital in Hangzhou city of Zhejiang province in China. We organized 67 face-to-face interviews to obtain the initial items of PL, including 2 focus groups and 65 semi-structured interviews.27
Each focus group lasted about 1 hour and each semi-structured interview lasted about 30 minutes. The interviews mainly focus on these questions: 1) What should the patient prepare before seeing the doctor? 2) What can patients do to make the medical procedure more efficient? 3) What does the patient do that will hinder the doctor? 4) What can a patient do to be considered as a good patient? 5) What are the aspects of the health literacy of patients?
All interviews were recorded and transcribed into manuscripts. The texts of manuscripts were analyzed by selective coding. We adopted the thematic framework analysis method, including five stages (familiarization, identifying themes, indexing, charting and summarizing, interpretation), to process the text data in excel by two researchers. The text data was marked and summarized by citing the typical expressions of the interviewees.
Item Refinement
Based on the extracted codes, categories, and subcategories of the item building stage, 21 items were prepared from the item pool. The content of items was reviewed several times, and some contents of items were replaced and modified. Finally, the initial scale for PL has been finished. The scale had 20 items and a five-point Likert scale (1= completely disagree, 2 = disagree, 3 = neither agree nor disagree, 4 = agree, 5 = completely agree) was used in response options. Notably, item 2, 14, 17 on the first-version scale were designed for reverse scoring in order to screen out respondents who did not answer carefully.
Face Validity
The face validity refers to the transparency or relevance of the test from the perspective of test participants,42 which determines the ease of understanding of the item contents and the response rate. In this study, 20 patients of different genders (9 males vs 11 females), ages (22.90 ± 2.11 years old) and educational levels were inquired to check whether the expressions of the initial scale are easy to understand and comply with language habits. After the phase of the inquiry, researchers reworded several questions that participants raised (eg, item 1 “I have a high level of basic knowledge of the common disease” modified as “I know more about the basic knowledge of the common diseases.”). The process of face validity was repeated by those same patients, and no questions were raised.
Content Validity
Two-round assessments were carried out to confirm the content validity of the PLS. During the first round, 9 scholars, including 2 experts in the social medicine field, 2 senior physicians and 5 PhD candidates in Public Administration, were requested to evaluate the content validity of the initial version scale, such as the item grammar, wording and allocation. The second-round assessment was conducted after construct validity measurement, and we invited 7 experts (2 scholars in social medicine field, 2 linguists and 3 postgraduates in Public Administration) to check and modify the contents of the second version of PLS by conducting a focus group.
During this process, four items have been changed (items 1, 3, 6, 13). For example, item 3 “I know what the doctors who diagnose me are good at” was changed into “I will find out the specialty of my doctor in advance”. The detail is displayed in Table 1.
 |
Table 1 The Contents of the Patients’ Literacy Scale |
Construct Validity
This study used factor analysis to measure the construct validity of the scale. Bartlett’s sphericity test was performed to ascertain whether the data were suitable for exploratory factor analysis (EFA), and the Kaiser–Meyer–Olkin (KMO) index was used to test whether the sample is adequate for factor analysis (p < 0.05, KMO > 0.50).43 EFA was conducted to determine the underlying structure of variables. Principal component analysis and Promax rotation were used for factor extraction and rotation matrix, respectively. We adopted two criteria, Kaiser–Guttman’s rule and the Cattell’s scree test, to confirm the number of factors that would be retained. The eigenvalue >1 was considered as the main component. Items were reserved if the factor loadings were ≥0.40.44 After a pilot study completed by 306 patients in a comprehensive hospital in November 2020 in Hangzhou, China, item 2, 6, 7, 8, 18 was deleted (factor loadings <0.30). Therefore, the fourth version of the PLS has 15 items, and none of the items was set for the reverse scoring.
We checked and established the factor structure obtained from EFA by performing confirmatory factor analysis (CFA). The fit indices used in this study included the following: minimum discrepancy function divided by degrees of freedom (CMIN/DF, <3 good); root mean square error of approximation (RMSEA, <0.05 good; <0.10 acceptable); root mean square residual (RMR, <0.05 good); goodness-of-fit index (GFI, >0.90 acceptable; >0.95 good); comparative fit index (CFI, >0.90 good); Tucker–Lewis index (TLI, >0.90 acceptable).45
Convergent and Discriminant Validity
Convergent validity refers to using different variables to measure the degree of similar constructs.46 Average variance extracted (AVE) was used to assess the convergent validity, because it can explain the degree of items sharing between the construct in structural equation modeling (SEM).47 Generally, the ideal value of AVE should be >0.50, while the acceptable value of AVE should >0.36.48
Discriminant validity was used to test whether concepts or measurements should not be too high correlated.49 Discriminant validity could be established by correlating one latent construct to another and when the correlation value of each construct is <0.85, the discriminant validity exists.47
Known-Group Validity
Known-group validity is a form of construct validity in which hypotheses are pre-specified and then tested to reflect whether the tool can distinguish differences in a priori expectations.50 If a statistical discrepancy is found, it supports the effectiveness of the instrument and if the discrepancy is not significant, the tool/item is defective, the hypothesis is defective, or the power is insufficient.50 The one-way ANOVA with Tukey and Bonferroni post hoc analysis was conducted to evaluate the PLS among patients with different ages, genders, educational levels, and patients who went to the hospital with different levels, which included first-level, secondary and tertiary hospitals.
Reliability
The Cronbach’s alpha coefficient and McDonald’s ω were used to determine the reliability of the PLS. The value of Cronbach’s alpha >0.70 represents that scale meets the standard reliability,45 while >0.60 represent the acceptable outcome.51 Further, we examined split-half reliability by using the Spearman-Brown formula. Our study also tested composite reliability (CR). CR refers to the combination reliability of all latent constructs, which is similar to the Cronbach’s alpha. The higher the CR values represent the higher internal consistency.47 The ideal value of CR is >0.70, and the acceptable value of CR is >0.60.48,52
Sample Size and Setting
We assumed a 95% confidence interval, a 0.80 power and calculated the sample size of 211 with the Power Analysis & Sample Size (PASS) free trial (NCSS, LLC, USA) software. We conducted the study in three hospitals with different levels in December 2020. The participants were drawn by accidental sampling, and questionnaires were distributed face-to-face. The inclusion criteria of our study population were that 1) outpatients themselves; 2) individuals who were willing to be involved in the study, while the exclusion were that 1) patients aged below 16 years and over 80 years; 2) accompanying family members; 3) patients with audiology communication, vision, or cognitive disorder. All questionnaires were saved at an online dataset by Wenjuanxing, a platform providing functions equivalent to Amazon Mechanical Turk.
For the completeness of the questionnaire and the convenience of patients seeking medical treatment, this questionnaire is set with a breakpoint to continue answering. Our survey received 426 questionnaires. We conducted a logic error-check inference to ensure accuracy on all submitted questionnaires. There were 123 questionnaires excluded, including 44 who failed to complete within less than 60 seconds; 79 who failed to pass the attention test, with an eligibility rate of 71.13%. Given each item should include at least 10 samples,53 at least 150 respondents (15 items * 10) were considered for EFA and CFA. Finally, 152 samples were for EFA and 151 samples were for CFA by random allocation.
Ethical Statement
This study was conducted based on the Declaration of Helsinki. The Ethics Committee of Zhejiang University School of Public Health approved the protocol of this study (2019–066). All individuals voluntarily participated in our research, and each participant also signed informed consent before the interview and survey. Furthermore, the participants were informed that their names would be replaced by codes in the interview texts and questionnaire.
Statistical Analysis
Continuous variables are presented as mean and standard deviation (SD). Categorical variables are presented as numbers and frequency. Psychometric properties of the scale are reflected by validity and reliability. The random allocation and EFA were analyzed using Statistical Package for the Social Sciences (SPSS) version 22.0 (SPSS Inc., Chicago, IL, USA), with a significance level of 0.05. CFA was evaluated using Analysis of Moment Structure software (AMOS) version 21. McDonald’s ω was calculated by Jamovi software version 1.6.23.
Results
General Demographic Characteristics of Participants
Table 2 shows the samples’ demographic characteristics. For the samples by EFA, the average age was 27.21 years and 76.32% were females. Most of them received university/college education. Over half individuals (54.60%) have more than 50,000 Yuan after-tax annual income. There were 54.61% respondents reporting first visit to the hospitals, and 32.89% and 26.32% of them visit the department of internal medicine and surgery, respectively. For the samples by CFA, 68.87% were females, averaging 27.58 years old. Most participants (49.67%) were undergraduate. The after-tax annual income of less than 30,000 yuan (39.07%) and over 90,000 yuan (31.13%) accounted for the majority of the sample. Nearly half of respondents (49.01%) reported first visiting the hospital, with 27.15% and 27.81% visiting the department of internal medicine and surgery, respectively.
 |
Table 2 Demographic Characteristics of Participants (N = 303) |
Exploratory Factor Analysis
Table 3 shows the exploratory factor loadings of the PLS. The KMO measurement of the samples’ adequacy was 0.787, which was higher than the commonly recommended value of 0.600. The Bartlett’s test of sphericity was significantly lower than 0.001, indicating that the data were suitable for factor analysis, and the variables were correlated. The four factors explained 61.266% of the total variance. Factor 1 loaded five items. Factor 2 and 4 both clustered three items. Factor 3 had included four items. All factor loadings of each item were above the 0.50.
 |
Table 3 Exploratory Factor Loadings of Patients’ Literacy Scale (n=152) |
Internal Consistency Reliability
Table 4 displays the results of the item analysis of PLS. The mean scores of all items were between 2.58 and 4.36. The corrected item-total correlation ranged from 0.342 to 0.633. The test to Cronbach’s alpha and McDonald’s ω if an item deleted did not significantly improve in the overall Cronbach’s alpha and McDonald’s ω of the scale.
 |
Table 4 Item Analysis for Patients’ Literacy Scale (n=152) |
Table 5 illustrates the reliability of the overall scale and its four factors. The overall Cronbach’s Alpha and McDonald’s ω of the 15-item scale was 0.815 and 0.838, respectively. The coefficient of split-half reliability was 0.720.
 |
Table 5 Reliability Test for Four Factors of Patients’ Literacy Scale (n=152) |
Confirmatory Factor Analysis
Table 6 demonstrates the convergent and discriminant validity indices of the PLS. All of the factors could meet the criteria of CR (>0.600) and AVE (>0.360). Factor 1 was estimated the highest CR value (0.749). While factor 3 was tested the lowest AVE value (0.365).
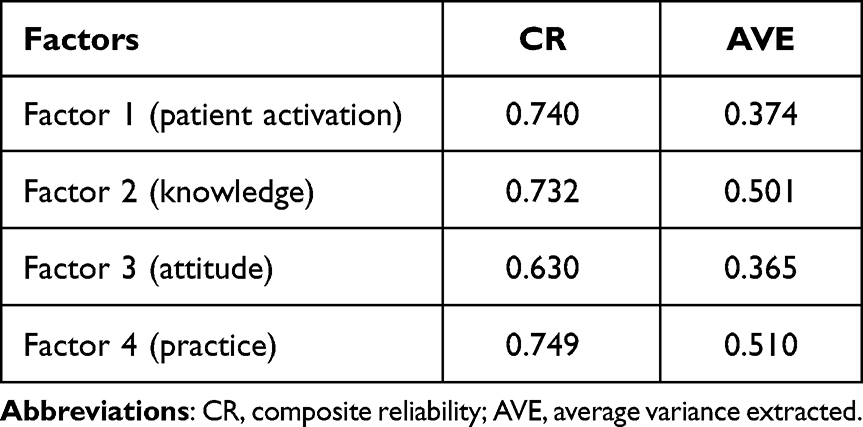 |
Table 6 The Indices of the Convergent and Discriminant Validity of Patients’ Literacy Scale |
Table 7 shows the model fit of five models (including four factor models and one full model) and the correlations among the factors. F1 was worse than the other models (RMSEA = 0.096, CMIN/DF = 2.389). Each item within the factors had a certain degree of correlation. The adjusted full model exhibited enough fit statistics (RMSEA = 0.065, CMIN/DF = 1.635, GFI = 0.900, CFI = 0.905, TLI = 0.909), after adjusting the crude model. The correlation value of all four factors was lower than 0.85, representing the discriminant validity existing.
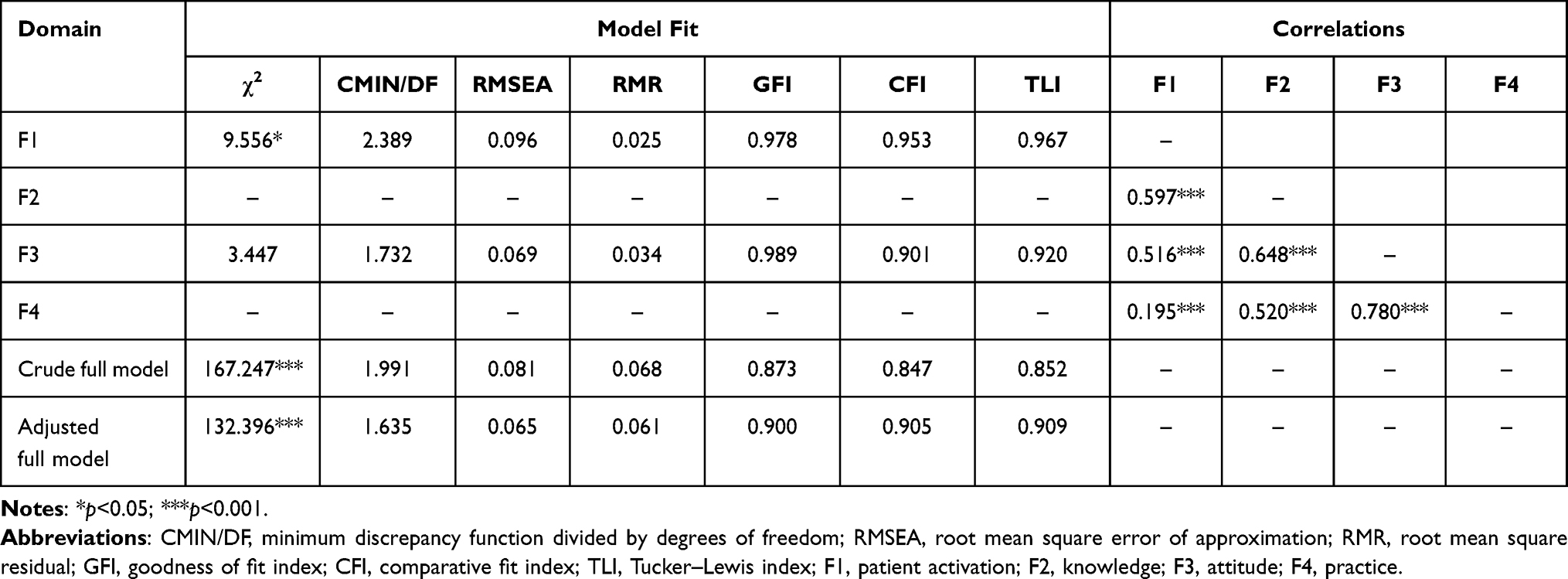 |
Table 7 Model Fit and Corrections Among Constructs of Patients’ Literacy Scale |
The final model had good known-group discriminant validity (Table 8). The total score had significant differences among patients of different ages, hospital levels and educational levels (p< 0.05). The PL was positively related to patients’ age. The gender difference between men and women is only reflected in F1. While patients who received high school or below education had higher PL than those who were undergraduate or graduate and over. Our study also found that the mean total score of PLS was positively correlated to patients’ age. Patients diagnosed in community hospitals or tertiary hospitals had higher patient literacy than those in secondary hospitals.
 |
Table 8 The Known-Group Validity of Patients’ Literacy Scale |
Discussion
This study first discussed the concept of PL which was different from HL, because the trend of patients’ role is changing from passive recipients to active participants currently.54 The health system also places more and more emphasis on patients in order to design and offer better health services.55 Thus, the concept of PL should stress the initiative and importance of patients. Based on previous studies and the theory of patients’ role, we finally concluded that PL should include the individual’s ability to use healthcare resources wisely, choose appropriate and proportionate healthcare services, respect healthcare professionals, and beliefs and confidence for self-managing health, which refers broadly to the patient performance that deserves recognition. The PLS was developed based on the concept.
The PLS strictly followed the scale development and construction process. The final version of the scale with 15 items was confirmed by experts’ reviews. Moreover, the PLS is relatively easy to administer in 5 minutes, for it concerns all real situations that patients would encounter. The PLS can serve as a quick evaluation instrument to identify PL. To ensure the PLS’ content validity, we invited two-round experts to verify and employed two-round patients to identify the face validity. KMO and Bartlett’s test of sphericity demonstrated satisfactory sampling adequacy and suitability of data for EFA. Four factors with the eigenvalue higher than one were produced by EFA, with identified factors explained over 60% of the variance among all items in PLS. This finding demonstrates that PLS contains sufficient items to satisfactorily measure essential factors associated with PL.43 Thus, this scale has good validity and reliability.
According to EFA, the PLS included four dimensions, and we defined F1 to F4 as “patient activation”, “knowledge”, “attitudes”, “practice” by the theory of KAP and patient activation. The “patient activation” was identified by the theory of patient activation,18 which can reflect the proactive behavior, self-management intention and the self-care ability of patients before and in the process of seeing a doctor, affecting the patient’s experience of seeing a doctor. It has been proven that describing the condition accurately and empathizing with doctors are skills that patients can learn to help smooth doctor–patient communication.56,57 The “knowledge” was concluded by the KAP model, which reflects the knowledge level of participants, and can directly affect their attitudes to deal with medical practices. Proper knowledge, especially certain legal knowledge related to health and medical practice may help reduce the medical dispute, which is worth popularizing to patients. The “attitudes” was obtained by the KAP model, which reflects the degree of trust and understanding of patients to doctors. Trust is a fundamental component of the DPR and is related to increased satisfaction, adherence to treatment, and continuity of care.58 Therefore, it is essential to know and increase the trust of the patients in doctors. In addition, as the modern healthcare system shifts to digital platforms and channels, patients’ trust in the official health information from these sources is also crucial.59 The “practice” also concluded from the KAP model, reflecting the positive or negative attitudes of patients before seeking medical treatment. Previous studies have found that practice, like patients prepared before seeing the doctors can help doctors make better decisions and guidance.60,61 All these dimensions can not only measure PL but also evaluate the efficiency of doctor–patient communication.
In this study, the indicators of goodness-of-fit by CFA showed that the model fit of the structural equation model of PLS is appropriate. The known-group validity was supported among patients of different ages, who went to hospitals with different levels and patients with different educational levels. Understandably, PL becomes higher as the age increases, because people will become more experienced, mature, and accountable in coping with health-related problems as they get older. We found that there was no gender difference in PL. It is interesting that patients with higher education have lower PL. We speculated that it might result from psychological entitlement, which refers to a stable and universal subjective belief or perception that one feels entitled to preferential treatment and is exempt from social responsibility.62 People with higher psychological entitlement may be more likely to do negative actions.63 For example, people with higher education had a higher level of psychological entitlement.64 Therefore, higher educated people are more likely to think that they should receive preferential treatment compared to lower educated ones in the process of seeing a doctor, resulting in low scores in the “patient activation” and “practice” dimension of PL. They may also have higher expectation of medical outcomes, which means they can better understand the medical information obtained from doctors but ignore other information like medical entanglement, resulting in low scores in the PL dimension of “knowledge”. Moreover, patients with higher educational levels which are closer to the doctors’ educational levels, which shorten the entitlement distance with the doctor, and may lose the respect to doctors, resulting in low score in the “attitudes” dimension of PL. More studies should be conducted to confirm this speculation in the future. In this study, patients who go to the first-level hospital or the third-level hospital have higher PL than those who go to secondary hospitals, because most patients who go to the first-level hospitals are mildly ill, and they may consult for some medicines, while patients who go to the third-level hospitals usually have more severe illnesses, so they may know more about their diseases and prepare in advance.
The purpose of this study is not just developing the scale of PL but also intended to increase the PL of all kinds of patients. However, increasing PL is a form of mindset shifting, which expresses in many dimensions from patient activation to KAP. Mindset shifting relies on subjective information filtering (choosing what to accept or reject), indicating that it may be more beneficial for researchers to use the PLS supported by an information processing approach.65 To increase PL, governmental and public supports also can not be neglected.66 Currently, the PL of patients in China is worrying. Therefore, we should take the cost of future applications of PLS into consideration, in order to further improvement and promotion of PL among patients. The limitations of this study are as follows. First, the representation of samples was limited, because samples were collected in outpatient halls in three hospitals with different levels in Hangzhou. Thus, the scale still needs to verify in other regions. The scale’s validity and reliability also need more evidence in other countries with different cultures. Second, we did not measure the test–retest reliability of the scale, for it was hard to find the same respondents again. Third, our study used a self-report questionnaire with certain recall bias. Forth, we correlated the error terms to obtain the better model fit in the PLS, which is not recommended during model construction. We will collect more data samples to improve the model fit in the future. Fifth, we did not evaluate the concurrent validity, because there is no similar type of or related scale for comparison.
Conclusion
In conclusion, the PLS is the first to comprehensively measure the literacy of the patients. It is an instrument with acceptable validity and reliability. Future research could validate among large-scale samples, and further apply in clinical research and practice for better care. The 15-item PLS could not only benefit for researchers but also for both patients and doctors. On the one hand, researchers can evaluate the effects in design, implementation and interventions of patient-related studies by using PLS. On the other hand, it also can be used as a standard and advocacy target for patients’ behavioral model which can further improve the DPR.
Acknowledgments
The authors would like to thank all the participants in this study for their time and help.
Funding
This study was funded by the National Natural Science Foundation of China (71974170) and Leading Innovative and Entrepreneur Team Introduction Program of Zhejiang (2019R01007).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kuehn BM. Violence in health care settings on rise. J Amer Med Assoc. 2010;304(5):511–512. doi:10.1001/jama.2010.1010
2. Gates DM. The epidemic of violence against healthcare workers. Occup Environ Med. 2004;61(8):649–650. doi:10.1136/oem.2004.014548
3. Lancet T. Ending violence against doctors in China. Lancet. 2012;379(9828):1764. doi:10.1016/S0140-6736(12)60729-6
4. Zhang X, Sleeboom-Faulkner M. Tensions between medical professionals and patients in mainland China. Camb Q Healthc Ethics. 2011;20(3):458–465. doi:10.1017/S0963180111000144
5. Harrison N. Regressing or progressing: what next for the doctor-patient relationship? Lancet Respir Med. 2018;6(3):178–180. doi:10.1016/S2213-2600(18)30075-4
6. Lu S, Ren S, Xu Y, et al. China legislates against violence to medical workers. Lancet Psychiatry. 2020;7(3):e9. doi:10.1016/S2215-0366(20)30005-5
7. Phillips JP, Longo DL. Workplace violence against health care workers in the United States. N Engl J Med. 2016;374(17):1661–1669. doi:10.1056/NEJMra1501998
8. Yin DK. 依法规范行医,循证保护自己 [Law-regulated practice and evidence-based self-protection]. Chin J Evid Based Med. 2005;5:1–2. Chinese.
9. Wang XQ, Wang XT, Zheng JJ. How to end violence against doctors in China. Lancet. 2012;380(9842):647–648. doi:10.1016/S0140-6736(12)61367-1.
10. Nie JB, Cheng Y, Zou X, et al. The vicious circle of patient-physician mistrust in China: health professionals’ perspectives, institutional conflict of interest, and building trust through medical professionalism. Dev World Bioeth. 2018;18(1):26–36. doi:10.1111/dewb.12170
11. Zeng J, Zeng XX, Tu Q. A gloomy future for medical students in China. Lancet. 2013;382(9908):1878. doi:10.1016/S0140-6736(13)62624-0
12. Parsons T. The Social System. New York: The Free Press; 1951.
13. Remen RN, Rabow MW. The Healer’s Art: professionalism, service and mission. Med Educ. 2005;39(11):1167–1168. doi:10.1111/j.1365-2929.2005.02296.x
14. Buetow S, Elwyn G. Are patients morally responsible for their errors? J Med Ethics. 2006;32(5):260–262. doi:10.1136/jme.2005.012245
15. Yaffe MJ, Hovey RB, Rodriguez C. Use of patients’ unsolicited correspondence to a family doctor to describe and understand valued components of a doctor-patient relationship: a Hermeneutics approach. BMC Fam Pract. 2019;20(1):136. doi:10.1186/s12875-019-1024-6
16. Stevenson FA, Kerr C, Murray E, Nazareth I. Information from the Internet and the doctor-patient relationship: the patient perspective–a qualitative study. BMC Fam Pract. 2007;8:47. doi:10.1186/1471-2296-8-47
17. Loh KY, Sivalingam N. Enhancing doctor-patient relationship: the humanistic approach. Med J Malaysia. 2008;63(1):85–87.
18. Hibbard JH, Stockard J, Mahoney ER, Tusler M. Development of the Patient Activation Measure (PAM): conceptualizing and measuring activation in patients and consumers. Health Serv Res. 2004;39(4 Pt 1):1005–1026. doi:10.1111/j.1475-6773.2004.00269.x
19. Wagner EH. Chronic disease management: what will it take to improve care for chronic illness? Eff Clin Pract. 1998;1(1):2–4.
20. Zhong BL, Luo W, Li HM, et al. Knowledge, attitudes, and practices towards COVID-19 among Chinese residents during the rapid rise period of the COVID-19 outbreak: a quick online cross-sectional survey. Int J Biol Sci. 2020;16(10):1745–1752. doi:10.7150/ijbs.45221
21. Tachfouti N, Slama K, Berraho M, Nejjari C. The impact of knowledge and attitudes on adherence to tuberculosis treatment: a case-control study in a Moroccan region. Pan Afr Med J. 2012;12:52.
22. Ajilore K, Atakiti I, Onyenankeya K. College students’ knowledge, attitudes and adherence to public service announcements on Ebola in Nigeria: suggestions for improving future Ebola prevention education programmes. Health Educ J. 2017;76:001789691771096. doi:10.1177/0017896917710969
23. Niroomand M, Ghasemi SN, Karimi-Sari H, Kazempour-Ardebili S, Amiri P, Khosravi MH. Diabetes knowledge, attitude and practice (KAP) study among Iranian in-patients with type-2 diabetes: a cross-sectional study. Diabetes Metab Syndr. 2016;10(1 Suppl 1):S114–119. doi:10.1016/j.dsx.2015.10.006
24. Ramchandani SR, Mehta SH, Saple DG, et al. Knowledge, attitudes, and practices of antiretroviral therapy among HIV-infected adults attending private and public clinics in India. AIDS Patient Care STDS. 2007;21(2):129–142. doi:10.1089/apc.2006.0045
25. Haq IU, Liu Y, Liu M, et al. Association of smoking-related Knowledge, Attitude, and Practices (KAP) with nutritional status and diet quality: a cross-sectional study in China. Biomed Res Int. 2019;2019:5897478. doi:10.1155/2019/5897478
26. Matsumoto-Takahashi EL, Tongol-Rivera P, Villacorte EA, Angluben RU, Jimba M, Kano S. Patient knowledge on malaria symptoms is a key to promoting universal access of patients to effective malaria treatment in Palawan, the Philippines. PLoS One. 2015;10(6):e0127858. doi:10.1371/journal.pone.0127858
27. Sang T, Wu Zh, Kou Y, Ye LX, Yang Q. 患方就医素养的定性研究 [Qualitative research on connotation of patient’s literacy (in press)]. Chinese J Social Med. 2022;39(3):278–281. Chinese.
28. Baker DW. The meaning and the measure of health literacy. J Gen Intern Med. 2006;21(8):878–883. doi:10.1111/j.1525-1497.2006.00540.x
29. Hussein SH, Almajran A, Albatineh AN. Prevalence of health literacy and its correlates among patients with type II diabetes in Kuwait: a population based study. Diabetes Res Clin Pract. 2018;141:118–125. doi:10.1016/j.diabres.2018.04.033
30. Jovanić M, Zdravković M, Stanisavljević D, Jović Vraneš A. Exploring the importance of health literacy for the quality of life in patients with heart failure. Int J Environ Res Public Health. 2018;15(8):1761. doi:10.3390/ijerph15081761
31. Kim MT, Song HJ, Han HR, et al. Development and validation of the high blood pressure-focused health literacy scale. Patient Educ Couns. 2012;87(2):165–170. doi:10.1016/j.pec.2011.09.005
32. Gordon MM, Hampson R, Capell HA, Madhok R. Illiteracy in rheumatoid arthritis patients as determined by the Rapid Estimate of Adult Literacy in Medicine (REALM) score. Rheumatology. 2002;41(7):750–754. doi:10.1093/rheumatology/41.7.750
33. China Medical News. Chinese Hospital Association: 27 incidents of violent injuries in hospitals per year; 2013. Available from: http://rs.yiigle.com/CN115178201316/584135.htm.
34. State Council of the People’s Republic of China. Regulation on the prevention and handling of medical disputes; 2018. Available from: http://www.gov.cn/zhengce/content/2018-08/31/content_5318057.htm.
35. Yu Yi HY, Libo L, Qunhong W, et al. Analysis of medical staff perspective factors influencing a harmonious doctor-patient relationship: based on 27 public hospitals of Heilongjiang province. Chin J Health Policy. 2016;9(6):15–19.
36. Liu Li XZ, Zeqi Q, Tuohong Z. Doctor-patient relationship in different level hospitals and influencing factors from doctor side. Med Philos. 2009;30(8):30–31.
37. Liu X, Hou Z, Towne SD
38. Or PP, Wong BY, Chung JW. To investigate the association between the health literacy and hand hygiene practices of the older adults to help them fight against infectious diseases in Hong Kong. Am J Infect Control. 2020;48(5):485–489. doi:10.1016/j.ajic.2019.12.021
39. Chan WL, Pun J, Dong D, Siminoff L, Dumenci L. Reliability and validity of the Cancer Health Literacy Test - Chinese versions: CHLT-30-Chinese and CHLT-6-Chinese. Asia Pac J Clin Oncol. 2022;18(3):279–286. doi:10.1111/ajco.13621
40. Mantwill S, Schulz PJ. Health literacy in Mainland China: validation of a functional health literacy test in simplified Chinese. Health Promot Int. 2016;31(4):742–748.
41. Wu L, Buchanan H. Translation and validation of the Revised Dental Beliefs Survey (DBS-R) in China. Psychol Health Med. 2020;25(7):812–823. doi:10.1080/13548506.2019.1668568
42. Holden RB. The Corsini Encyclopedia of Psychology.
43. Abounoori M, Maddah MM, Sharif Nia H, et al. Development and validation of the knowledge and attitude scale toward COVID-19 pandemic breaking transmission chain (KA-C) among Iranian population. Front Public Health. 2021;9(61). doi:10.3389/fpubh.2021.627013
44. Bao C, Yu Z, Yin X, et al. The development of the social health scale for the elderly. Health Qual Life Outcomes. 2018;16(1):67. doi:10.1186/s12955-018-0899-6
45. Rong TS. AMOS 与研究方法 [AMOS and Its Research Methods]. Chongqing: Chongqing University Press; 2010. Chinese.
46. Kenny D, Kashy D. Analysis of the multitrait-multimethod matrix by confirmatory factor analysis. Psychol Bull. 1992;112:165–172. doi:10.1037/0033-2909.112.1.165
47. Hair JP, Black JP, Babin JP, Anderson RE. Multivariate Data Analysis.
48. Fornell C, Larcker D. Evaluating structural equation models with unobservable variables and measurement error. J Mark Res. 1981;18:39–50. doi:10.1177/002224378101800104
49. Campbell DT, Fiske DW. Convergent and discriminant validation by the multitrait-multimethod matrix. Psychol Bull. 1959;56(2):81–105. doi:10.1037/h0046016
50. Rodrigues IB, Adachi JD, Beattie KA, Lau A, MacDermid JC. Determining known-group validity and test-retest reliability in the PEQ (personalized exercise questionnaire). BMC Musculoskelet Disord. 2019;20(1):373. doi:10.1186/s12891-019-2761-3
51. Wu S. SPSS 实战与统计思维 [SPSS and Statistical Thinking]. Beijing: Tsinghua Press; 2018. Chinese.
52. Zhang Z, Zheng L. Consumer community cognition, brand loyalty, and behaviour intentions within online publishing communities: an empirical study of Epubit in China. Learn Publ. 2020;34:116–127.
53. BH Munro. Statistical Methods for Health Care Research. Philadelphia, PA: LippincottWilliams &Wilkins; 2005.
54. Brady TJ. The patient’s role in rheumatology care. Curr Opin Rheumatol. 1998;10(2):146–151. doi:10.1097/00002281-199803000-00011
55. Hansen HP, Draborg E, Kristensen FB. Exploring qualitative research synthesis: the role of patients’ perspectives in health policy design and decision making. Patient. 2011;4(3):143–152. doi:10.2165/11539880-000000000-00000
56. Gáspárik AI, Ábrám Z, Ceana D, Sebesi S, Fărcaş D, Gáspárik AC. Shortages of doctor-patient communication. teaching patients to communicate effectively. Procedia Soc Behav Sci. 2014;142:376–379. doi:10.1016/j.sbspro.2014.07.693
57. Lin CS, Hsu MY, Chong CF. Differences between emergency patients and their doctors in the perception of physician empathy: implications for medical education. Educ Health. 2008;21(2):144.
58. Rolfe A, Cash-Gibson L, Car J, Sheikh A, McKinstry B. Interventions for improving patients’ trust in doctors and groups of doctors. Cochrane Database Syst Rev. 2014;2014(3):Cd004134.
59. Vuong QH, Le TT, La VP, Nguyen MH. The psychological mechanism of internet information processing for post-treatment evaluation. Heliyon. 2022;8(5):e09351. doi:10.1016/j.heliyon.2022.e09351
60. Stacey D, Kryworuchko J, Bennett C, Murray MA, Mullan S, Légaré F. Decision coaching to prepare patients for making health decisions: a systematic review of decision coaching in trials of patient decision aids. Med Decis Making. 2012;32(3):E22–E33. doi:10.1177/0272989X12443311
61. Grande SW, Faber MJ, Durand MA, Thompson R, Elwyn G. A classification model of patient engagement methods and assessment of their feasibility in real-world settings. Patient Educ Couns. 2014;95(2):281–287. doi:10.1016/j.pec.2014.01.016
62. Campbell WK, Bonacci AM, Shelton J, Exline JJ, Bushman BJ. Psychological entitlement: interpersonal consequences and validation of a self-report measure. J Pers Assess. 2004;83(1):29–45. doi:10.1207/s15327752jpa8301_04
63. Zitek EM, Jordan AH, Monin B, Leach FR. Victim entitlement to behave selfishly. J Pers Soc Psychol. 2010;98(2):245–255. doi:10.1037/a0017168
64. Sarshar M, Farley F, Fiorello C, DuCette J. T behavior: psychological implications of thrill-seeking/risk-taking. Curr Psychol. 2019;40(8):3840–3847. doi:10.1007/s12144-019-00338-2
65. Vuong Q-H, Napier N. Acculturation and global mindsponge: an emerging market perspective. Int J Intercult Relat. 2015;49:354–367. doi:10.1016/j.ijintrel.2015.06.003
66. Vuong QH. The (ir) rational consideration of the cost of science in transition economies. Nat Hum Behav. 2018;2(1):5. doi:10.1038/s41562-017-0281-4
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Validation of the Connor-Davidson Resilience Scale-10 in South Africa: Item Response Theory and Classical Test Theory
Pretorius TB, Padmanabhanunni A
Psychology Research and Behavior Management 2022, 15:1235-1245
Published Date: 16 May 2022
Validity and Reliability of the Thai Version of the 19-Item Compliance-Questionnaire-Rheumatology
Panichaporn S, Chanapai W, Srisomnuek A, Thaweeratthakul P, Katchamart W
Patient Preference and Adherence 2022, 16:2149-2158
Published Date: 17 August 2022
Psychometric Properties of the Montreal Cognitive Assessment (MoCA) to Detect Major Neurocognitive Disorder Among Older People in Ethiopia: A Validation Study
Daniel B, Agenagnew L, Workicho A, Abera M
Neuropsychiatric Disease and Treatment 2022, 18:1789-1798
Published Date: 22 August 2022
Development and Validation of the Patient/Caregiver Reported Hydroxyurea Evaluation of Adherence for Life (HEAL) Scale
Janson IA, Bloom EM, Hampton KC, Meier ER, Rampersad AG, Kronenberger WG
Patient Preference and Adherence 2022, 16:3229-3239
Published Date: 10 December 2022
Research and Evaluation of a Cyberchondria Severity Scale in a Chinese Context
Wang D, Sun L, Shao Y, Zhang X, Maguire P, Hu Y
Psychology Research and Behavior Management 2023, 16:4417-4429
Published Date: 1 November 2023