Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
Parental Voices on Virtual Reality in Pediatric Oncology: Experiences, Needs, and Pathways for Co-Design
Authors Hélie C, Véronneau J, Desjardins O, Barada L, Lebeau J, Ogez D ![]()
Received 24 July 2025
Accepted for publication 8 November 2025
Published 19 November 2025 Volume 2025:18 Pages 7551—7565
DOI https://doi.org/10.2147/JMDH.S555927
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Pavani Rangachari
Charlotte Hélie,1,2 Jade Véronneau,1,3 Orly Desjardins,1,2 Léa Barada,1,2 Julie Lebeau,1 David Ogez1,4
1Research Center, Maisonneuve-Rosemont Hospital, Montreal, Quebec, Canada; 2Department of Psychology, Faculty of Arts and Sciences, University of Montreal, Montreal, Quebec, Canada; 3Department of Psychology, Faculty of Arts and Sciences, University of Quebec in Outaouais, Gatineau, Quebec, Canada; 4Department of Anesthesiology and Pain Medicine, Faculty of Medicine, University of Montreal, Montreal, Quebec, Canada
Correspondence: David Ogez, Research Center, Maisonneuve-Rosemont Hospital, 5415, boulevard de l’Assomption, Montréal, Québec, H1T 2M4, Canada, Tel +1 514 252-3400 X 4443, Email [email protected]
Introduction: Pediatric cancer treatments significantly affect children’s physical, emotional, and social well-being. Virtual reality (VR) is emerging as a promising non-pharmacological tool to enhance quality of life during hospitalization, yet little is known about parents perceive its potential role in supportive care.
Methods: This qualitative study used semi-structured interviews with five parents of children in remission from cancer. It explored their experiences during chemotherapy and their perspectives on how VR could help support children and families during treatment.
Results: Parents described multiple challenges during hospitalization, including emotional distress, physical side effects, social isolation, logistical difficulties, and communication issues. While most had limited prior exposure to VR, they expressed openness toward its use to reduce anxiety, boredom, and loneliness. Parents emphasized that VR should complement, not replace, human interaction, and suggested age-specific applications, interactive content for adolescent and calming, passive experiences for younger children.
Discussion: This study provides novel insights by integrating parental voices early in the co-design process of VR interventions for pediatric oncology. It identifies concrete psychosocial needs and offers recommendations to ensure future digital tools are developmentally appropriate and family-centered. While the small, homogeneous sample and absence of child participants limit generalizability, the in-depth qualitative approach offers valuable groundwork for future participatory research and VR intervention development in pediatric cancer care.
Plain Language Summary: When a child is hospitalized for cancer treatment, it can be a stressful experience for the entire family. Children often experience fear, loneliness, and pain. Their parents also face emotional and practical challenges, such as long hospital stays, lack of sleep, and concerns about their child’s well-being. In this study, we interviewed five parents whose children had undergone chemotherapy and were now in remission. We asked them to share what they went through during the treatment and how they feel about using virtual reality (VR) as a support tool for children during hospitalization. The parents described many difficulties their children faced: physical side effects, anxiety, boredom, and being cut off from school and friends. They also spoke about their own struggles, including emotional exhaustion and communication problems with hospital staff. Despite having little experience with VR, most parents were open to using it during treatment. They saw VR as a possible way to reduce anxiety, help children relax, and even keep in touch with friends. However, they were clear that VR should not replace human contact. Parents suggested ideas like calming virtual nature scenes for young children, or interactive games for teenagers. Their input helps us understand how to design VR tools that are both useful and acceptable for families. This study highlights the importance of involving parents in the development of new health technologies. By listening to their experiences, we can create better tools to support children with cancer and their families.
Keywords: pediatric oncology, chemotherapy, parental experiences, virtual reality, supportive care, qualitative research, thematic analysis
Introduction
Every year, thousands of children around the world are diagnosed with cancer, particularly hematological cancers such as leukemia, which are among the most common pediatric cancers. In Quebec, 233 children under the age of 14 were diagnosed with cancer in 2020, nearly 29% of whom had leukemia.1,2 Although survival rates have improved considerably following medical advances, the experience of cancer treatment, especially chemotherapy, remains a deeply disturbing and often traumatic event for young patients.2,3
Pediatric cancer treatment is associated with a wide range of physical side effects, including fatigue, nausea, neuropathic pain, and mucositis, alongside significant psychological and social burdens.4 Children frequently experience isolation, anxiety, fear related to treatment procedures and discouraged by being excluded from school and peer interactions.5 Studies show that quality of life (QoL) is significantly impacted during treatment, and emotional consequences can persist long after remission. Risk factors such as being older, female, or in an intensive treatment phase have been linked to worse outcomes in QoL.6–8 In response, psychosocial interventions have emerged globally to help alleviate these impacts. Programs including art therapy, mindfulness, cognitive behavioral therapy (CBT), and physical activity support have shown encouraging results in improving children’s psychological resilience and emotional well-being.9–13
At the same time, technology-based interventions have gained ground internationally, particularly the use of virtual reality (VR) to distract children during painful or anxiety-provoking medical procedures.14 VR has been shown to reduce the pain and anxiety associated with procedures in pediatric oncology settings.15–19 Applications range from immersive games and animated videos to software designed to help children cope with acute pain during medical procedures.16,18,19 However, most of these interventions are narrowly focused on momentary distraction and often lack integration into broader psychosocial care strategies. Very few studies have explored how VR could address challenges such as social isolation, loss of autonomy, or disrupted school connections, despite their critical role in children’s overall psychological adjustment.
Furthermore, these studies are often conducted outside of Canada, raising questions about their cultural and systemic relevance in specific contexts like Quebec.14 Health care systems, resource availability, and cultural values can shape how children and families respond to digital interventions. In Quebec, a publicly funded healthcare system coexists with limited access to pediatric psychosocial care. As of 2023, over 2400 children were on waiting lists for mental health services beyond the recommended 30-day delay.20 Hospitals are also facing critical staffing shortages, especially among psychologists and psychosocial professionals.21,22
These gaps present both a challenge and an opportunity. While psychosocial support is clearly needed, there is room to develop complementary and scalable tools like VR that could be tailored specifically to the needs and preferences of children and families in Quebec. Rather than simply adapting existing games or videos, there is a need to design immersive experiences that consider the broader emotional journey of children undergoing treatment, not only to distract them in moments of pain, but to support their sense of agency, connection, and well-being throughout the course of therapy. Mechanisms such as shared VR environments, interactive storytelling, or simulations of social situations could be used to reinforce social bonds and emotional engagement.
In this context, understanding the perspectives of families is essential Parents often serve as primary observers of their children’s emotional and psychological responses to treatment and can offer rich insights into what works, what’s missing, and what could help.23 They are also frequently involved in treatment decisions and thus play a key role in the acceptability and implementation of new interventions.15 However, most existing studies focus on children as users, and the parental perspective is often overlooked—despite its importance in both decision-making and home-based reinforcement of interventions. Consulting parents in the design phase of a VR-based tool can increase both its relevance and its impact.
Objectives
This study aims to explore parents’ perspectives related to their child’s experience of cancer treatment and hospitalization, as well as their views on potential supportive interventions. Specifically, it seeks to: 1) Understand parents’ perceptions of their child’s quality of life and emotional experience during chemotherapy; 2) Explore parents’ own experiences, challenges, and coping strategies throughout their child’s treatment and hospitalization; 3) Gather parents’ views, expectations, and openness toward the use of virtual reality (VR) and other technology-based interventions to support children’s well-being; 4) Generate preliminary recommendations for the development of developmentally appropriate, family-centered psychosocial and VR-based interventions tailored to pediatric oncology contexts.
Materials and Methods
This qualitative, exploratory study was conducted within a constructivist paradigm, which posits that knowledge emerges through individual lived experiences and that multiple subjective realities coexist.24 The goal was to explore how parents of children in remission from cancer perceive the potential role of VR in pediatric oncology, particularly during chemotherapy.
Participants and Procedures
Participants were recruited through callouts and flyers disseminated by two major Quebec-based foundations active in pediatric oncology (Leucan and the Cole Foundation). The study included five French-speaking parents of children in remission from pediatric cancer. All participants were required to have a child who had undergone chemotherapy within the past three years. Although the study protocol initially allowed for the inclusion of children, no children ultimately participated. Parents had discussed the study topic with their children prior to the interviews and shared insights based on those conversations, thereby indirectly conveying their children’s perspectives. No parent-child dyads were matched.
Inclusion criteria included being fluent in French and having a child who had received chemotherapy and was in remission. Exclusion criteria included any communication impairment that could interfere with the participant’s ability to engage in the interview process.
Although the sample size was limited to five participants, this reflects qualitative methodological standards prioritizing depth over breadth. In thematic analysis, rich and focused datasets from small, homogeneous groups are often sufficient to reach thematic saturation.25,26 In this study, saturation was determined inductively: after five interviews, no new codes or themes emerged during independent double coding, justifying the cessation of data collection.
The project received ethical approval from the institutional Research Ethics Committee (#2023-5239). Interested individuals received an information sheet and consent form via email. Written informed consent was obtained prior to the interview. Interviews were conducted virtually via Zoom to enhance accessibility and flexibility, particularly during COVID-19.
Before the interview, participants were asked to complete a brief sociodemographic form to verify eligibility and describe the sample. If the form was not returned in advance, it was completed during the first few minutes of the interview. Each participant was interviewed alone in a quiet setting. Interviews were audio-record. They lasted between 30 and 60 minutes and were conducted at the participant’s pace to ensure emotional comfort.
Each interview and moderated by two trained members of the research team: the principal investigator (DO, male, psychologist, PhD) and an undergraduate research assistant (CH, female, BSc student). A third team member (JV, female, MSc student) provided technical support and ensured secure audio recording. Interviews were transcribed verbatim in French and anonymized.
At the end of the interview, a summary of the responses was presented to the participant to ensure that they accurately reflected their intended meaning.
Data Collection
A semi-structured interview guide was developed based on the study objective. It included open-ended questions designed to elicit participants’ perceptions of their child’s quality of life during chemotherapy, their experiences as caregivers, and their views on how VR might be integrated into treatment to offer support. Flexibility was maintained during the interview process to allow for the exploration of emergent topics brought up by participants.
Data Analysis
The data were analyzed using an inductive thematic analysis approach.27 The analysis proceeded in three phases: data reduction, theme generation, and interpretation. In the first phase, the verbatim transcripts were segmented into meaningful units by sentence or paragraph. This reduction helped distill the content into analyzable pieces. In the second phase, descriptive coding was performed on each unit. Codes were initially kept close to the participants’ original wording and later grouped into thematic categories. A coding framework was developed and revised iteratively during the analysis. Two analysts (OD, LB, females, BSc students) independently coded the transcripts using QDA Miner software. This dual-coding process enhanced the internal validity and reproducibility of the analysis by ensuring inter-rater agreement and reducing subjectivity.28,29 Regular meetings with a third analyst (CH) and a healthcare professional (JL, female, nurse) were held to compare codes and resolve discrepancies through discussion and consensus. In the final phase, key themes were extracted and synthesized to generate insights related to the research question. Relevant participant quotations were retained to illustrate each theme and preserve the voice of those interviewed. The identified themes served as a foundation for developing practical recommendations for the design of a VR-based intervention intended to support pediatric oncology patients during chemotherapy. These recommendations will inform a follow-up phase in which items derived from the themes may be validated through a broader consultation process.
Results
As shown in Table 1, a total of five parents participated in the study, including four mothers and one father, all of whom had children in remission from pediatric cancer. The children were between the ages of 3 and 17 years at the time of diagnosis and had received chemotherapy as part of their treatment, primarily during hospitalizations.
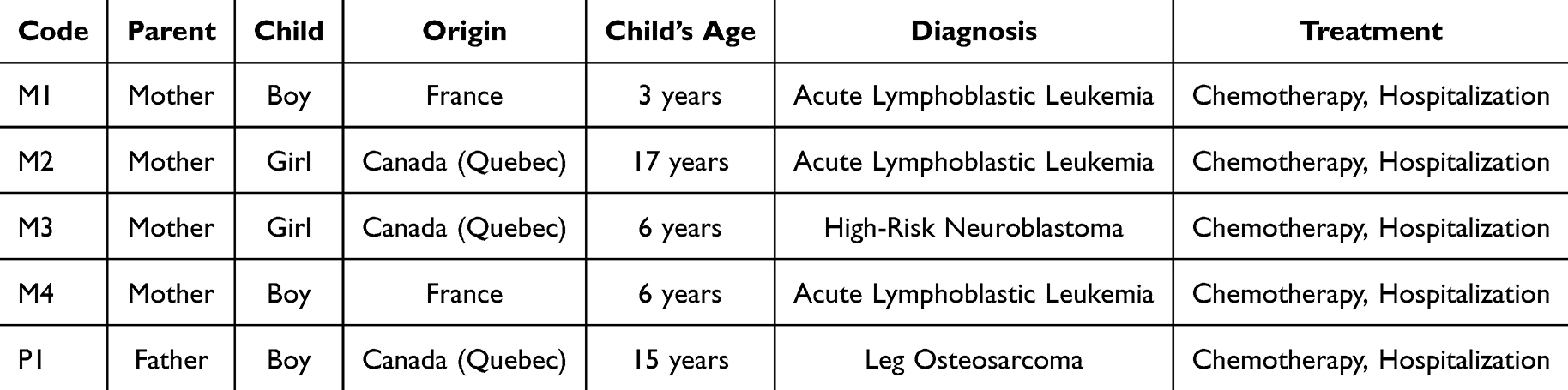 |
Table 1 Description of Participants |
Among the participants, three mothers were from Quebec and one from France. Their children had been diagnosed with either acute lymphoblastic leukemia (ALL) or high-risk neuroblastoma. The children ranged in age from 3 to 17 years and included both boys and girls. All had undergone chemotherapy in hospital settings. The participating father was from Quebec and had a 15-year-old son who had been treated for osteosarcoma of the leg. His son received chemotherapy exclusively during hospitalizations, including several extended inpatient stays.
The following results are organized into two main themes. Theme 1 describes the challenges and resources experienced during hospitalization for chemotherapy. Theme 2 explores how these experiences informed parents’ views on the potential value of virtual reality in pediatric oncology settings. The articulation of these themes reflects how existing needs and difficulties may be addressed through future VR-based interventions.
Theme 1-Experience During Hospitalization for Chemotherapy
Interviews with parents revealed several dimensions of the experience, including the difficulties encountered by the children, those experienced by the parents, and the resources mobilized to cope with treatment. These sub-themes are illustrated in Figure 1.
 |
Figure 1 Theme 1-Experience during hospitalization for chemotherapy. |
Children’s Difficulties
Children’s difficulties could be grouped into four main sub-themes. The first related to physical symptoms. Parents frequently mentioned challenges related to side effects and medical procedures. For example, P1 noted that his child was “weakened by the cancer”, while M1 observed
There are a lot of teens in wheelchairs during treatment… just from weakness.
She also explained how fatigue manifested in her son:
He barely walked anymore, he always wanted to be carried.
These physical symptoms fluctuated throughout the treatment cycle:
It’s not constant… At some point, the doctor explained that over time it hits harder. So the same chemo at the beginning, the child tolerates well, but later on, the body just takes it worse. (M1)
P1’s son also experienced discomfort, nausea, and had to relearn to walk following surgery:
He went into another round of rehab, he’s still doing physiotherapy, but it’s much better now.
M1’s son had a severe reaction to one treatment and became immunosuppressed. M1 also highlighted the pain associated with medical procedures:
Bandage changes were torture. We had to hold him down.
Routine medical checks triggered anxiety:
He’d see the cuff and start screaming.
M2 noted a similar distressing pattern with her daughter:
Every blood draw was a traumatic event. She knew the routine and already started crying when the nurse walked in.
Some procedures were done at night, affecting the sleep of both the child and the parents. M4 added, “She didn’t sleep at all that night, and I had to stay alert in case they needed me. We were both exhausted the next day”.
The second sub-theme concerned psychological aspects. For M1’s son, anticipation and panic associated with separation during procedures were major sources of distress. M1 recounted:
They had to hold him down with four or five people and stick both his arms to place catheters.
For P1’s son observed “a lot of boredom, a lot of anxiety, and sadness”, and noted signs of unspoken anger:
There was a sense of injustice.
M3 emphasized her daughter’s emotional withdrawal:
There were days she wouldn’t speak to anyone. She’d just stare, even when I tried to distract her.
The third sub-theme was social aspects. Hospitalization disrupted the children’s social lives and developmental experiences. Adolescents, such as M2’s daughter, missed school and social life:
She felt like life was going on without her. Her friends stopped visiting after a while.
For younger children like M1’s son, prolonged proximity to parents fostered dependency and separation anxiety:
Even today, it’s still a challenge because he’s not used to playing on his own. (M1)
M4 noted a similar trend:
He always wants to be with us now. He’s afraid something will happen if we’re not there.
The fourth sub-theme concerned communication aspects. Parents highlighted issues with healthcare staff. Parents described inconsistency and lack of continuity in communication. “There’s a lot of incoherence” (P1). Some resources were not presented until late in the treatment process:
I didn’t even know that program existed. We’d already been there five months. (M1)
Certain staff interactions were perceived as cold and impersonal:
She wouldn’t even talk to us… She didn’t even say hello to the child. (M1)
M2 expressed concern about staff attitude:
Some staff were warm, but others were mechanical, like they were just doing their shift and not seeing the child as a person.
However, parents acknowledged that these behaviors may be related to staff overload.
Parents’ Difficulties
Parents also experienced significant difficulties throughout their child’s treatment. At a personal level, sleep disturbances, psychological strain, and relational impacts were frequently mentioned. M1 shared:
It was really hard emotionally, and on our relationship too. Really hard on the couple.
Parents struggled to hide their own suffering from their children. “We tried to pretend everything was fine, but we were so stressed when we saw him screaming” (M1). Time in the hospital was long and draining:
He didn’t feel like he was in prison, but we did. (M1)
Similarly, P1 added, “We just watched the hours pass by”. M3 also described emotional exhaustion and a feeling of being isolated in the experience:
We weren’t sleeping, we weren’t eating… you’re just not functioning anymore.
The psychological toll extended beyond the hospital:
Even now, I’m not sure I’ve recovered emotionally from that time. (M3)
M4 added, “I didn’t want to show him how scared I was… but inside, I was devastated”.
The logistical aspect was another important challenge, particularly for working parents. P1 had to leave his job:
There was no way I could work and do this at the same time.
Transportation was also a major source of stress:
Just the trips… it was extremely difficult. (P1)
Once at the hospital, accommodations were far from ideal:
I spent several weeks on a cot in a tiny hospital room.
M3 shared a similar burden, emphasizing the cumulative fatigue caused by back-and-forth travel:
It was exhausting, always packing and going back and forth… we had no break.
M2 also pointed out that managing family life during hospital stays was nearly impossible:
We were constantly torn between being with her at the hospital and trying to keep the house running.
The hospital system itself presented additional difficulties. Some staff were not experienced with pediatric oncology. M1 recalled an incident where the nurse had difficulty preparing the chemotherapy infusion. Overworked staff were frequently mentioned:
We needed to see him more, but he looked really overwhelmed. (M1)
P1 criticized the hospital’s lack of flexibility and poor infrastructure:
The buildings are outdated, the food is terrible, and there’s nothing for teens to do.
M4 shared this sentiment, describing the welcoming environment as “hostile and depressing”, adding, “It was not designed to make children feel safe or relaxed”. M2 emphasized the difficulty of adapting the schedule to the child’s rhythm:
There was no flexibility in the schedule. Sometimes she was too tired, but they came anyway for the procedures.
The communication surrounding care was also problematic. Parents expressed a need for clearer and more responsive dialogue with healthcare providers. “Some people just weren’t open to answering questions about our child’s care” (M1). M2 shared:
Sometimes we had to repeat everything because the staff hadn’t passed on information. It made us feel like we had to start over each time.
She added:
There were so many people involved; we never knew who to ask. It felt chaotic.
M3 also described feeling excluded from key decisions:
We weren’t really told what was going to happen. Often, we’d find out things at the last minute.
M4 echoed the importance of empathy in communication:
Sometimes they’d speak in front of him like he wasn’t there. It made him anxious. They forgot he was still just a child.
Resources Used During Hospitalization
To cope with the difficulties encountered during treatment, several resources were used, some more successfully than others. Among the effective tools, certain healthcare professionals made a meaningful difference for both parents and children. For instance, one nurse was particularly appreciated by P1 and his son:
He was known on the unit for connecting well with adolescents. (P1)
In M1’s son case, specific nurses and a psychosocial worker made a difference with their thoughtful gestures:
She came in with finger puppets and took her time. (M1)
Specialized educators were especially helpful, using age-appropriate techniques. One used “a little vibrating bee to desensitize the skin before injecting” (M1). A psychologist also played a key role in helping one child process their treatment experience.
The presence of parents was another crucial support mechanism. Parents often engaged in play with their children to pass the time. M2 said:
We played cards, board games… just to keep her distracted from everything else.
M3 highlighted the importance of parental presence:
Even when she was feeling awful, having me there helped her hold on.
Mobile phones served as another valuable tool, especially for older children. While initially unhelpful for the youngest child, they later offered distraction through videos or songs. M4 noted:
She found comfort in watching the same cartoon over and over. It became part of her routine.
Finally, Leucan, a non-profit pediatric cancer support organization, was mentioned as a major source of help by M1, providing emotional support, guidance, and practical resources like illustrated books explaining chemotherapy:
They were present, caring, and they made us feel less alone.
On the other hand, some resources proved ineffective or insufficient. Internet connection was often unreliable, particularly during peak hours, which affected P1’s son ability to stay connected with friends or use entertainment devices:
That would’ve made a huge difference, I think. (P1)
M2 added:
The Wi-Fi was spotty, and it frustrated her a lot, especially when she wanted to call her friends or stream something comforting.
Due to his young age, the smartphone was not useful for M1’s son at first:
It didn’t really change anything. (M1)
M3 added that distractions for younger kids were often inappropriate:
They had things for teens, but nothing that worked for a six-year-old.
Finally, even when individual staff members made a difference, the general shortage of staff was a barrier:
The nurses’ working conditions, the lack of personnel—it all meant they didn’t have 15 minutes to sit with a child and talk to them. (M1)
M4 also shared, “They were doing their best, but you could feel they were stretched too thin to offer anything beyond the basics”.
Theme 2-Virtual Reality in Pediatric Oncology Hospitalization
Another major theme that emerged from the interviews was parents’ perspectives on the use of VR during hospitalization for cancer treatment. Sub-themes are summarized in Figure 2.
 |
Figure 2 Theme 2-Virtual reality in the context of hospitalization in oncology. |
Parents had limited knowledge about VR. They were generally unfamiliar with VR prior to the interviews, and only one of the two children had previously used it:
He tried it, but didn’t really seem into it. (P1)
Nevertheless, throughout the discussions, both potential benefits and limitations of implementing VR during chemotherapy were identified.
Anticipated Benefits
In terms of anticipated benefits, the first related to social connection. For adolescents like P1’s son, VR could be used to maintain friendships—much like gaming consoles:
The console allowed him to socialize, to just talk to his friends. Kind of like FaceTime, but with more people. (P1)
For younger children like M1’s son, it could help foster autonomy and reduce parental overdependence:
Maybe it could allow for a daily moment where he plays alone… It might help with that kind of overly close attachment to us. (M1)
From a developmental perspective, educational content in VR could compensate for missed daycare activities:
For learning shapes, colors… it could be a substitute since he’s not going to daycare. (M1)
M3 reinforced this idea:
If it could have learning games—math, letters, stuff like that—it’d be useful during those long stays.
Parents also suggested that VR might promote relaxation and help with emotional regulation. M2 said, “When she was anxious, even simple breathing apps on a screen helped… If that was in VR, with nature sounds or visuals, I think it would work even better”.
Limitations
However, parents also identified limitations. M1 emphasized that VR use should not replace real human interaction:
Yes, it can help compensate when they just can’t have human contact for different reasons… but we shouldn’t lose touch, and all become robots either.
Another concern was the limited space in hospital rooms for active VR play, and the physical limitations due to medical equipment. M1 said “Often, he just couldn’t move much, especially when hooked up to machines”. M3 added:
The wires, the IV, the monitors… there wasn’t much freedom to move.
Intervention Proposals
Parents suggested several ideas for VR interventions, divided into two main categories: active and passive interventions.
Active interventions were seen as particularly beneficial for teens. P1 explained:
He prefers choosing, making decisions, progressing through a story… rather than being passive.
M1 reported that active content was appropriate in specific moments:
During the day, the game part could be interesting. (M1)
These could include physiotherapy exercises made more engaging through VR:
It must be hard to motivate some kids to do those exercises… but if they’re integrated in the headset, it could help. (M1)
Video games—adapted to the child’s age—were also proposed. M1 suggested simpler activities:
I think catching balls or something like that would be a good idea.
P1 mentioned console-style games like Minecraft or GTA. Chatroom-style features to connect with friends were also recommended. M4 also proposed mini-games with physical challenges adapted to kids with limited mobility. Another idea was the presence of a parent avatar to comfort children during procedures:
If he could see me in the headset, that would be reassuring when I’m not allowed to be beside him. (M1)
Finally, VR could help explain cancer and chemotherapy in age-appropriate ways:
I explained that there were ‘bad guys’ in his body and the treatment was to get rid of them… but it could be adapted with metaphors for different ages. (M1)
Passive interventions seemed better suited for younger children like M1’son. M1 proposed treatment simulations to reduce fear and anticipation:
Even for things like dressing changes… showing it in VR, showing that it hurts but then it’s over—that might help.
Animated nursery rhymes also helped during painful moments:
Those were what we watched most. They really helped during dressing changes. (M1)
Having visual content could also distract the child when parents were emotionally overwhelmed. M1 suggested pairing specific soothing content with recurring procedures:
If every time he had a dressing change, he got to watch a VR farm with animals… I think he’d really enjoy that and it would help distract him.
M2 suggested interactive breathing exercises with visuals. M3 proposed nature simulations:
Something with birds or forests… calming and immersive, but simple.
M4 emphasized using VR to explain treatment metaphors:
I told him the chemo was like little soldiers fighting inside. If VR could show that, it would make it real for him.
Discussion
This study aimed to gather the perspectives of parents of pediatric cancer survivors on the use of virtual reality (VR) during chemotherapy treatments, with the goal of formulating recommendations for the development of a VR-based intervention to improve quality of life during hospitalization. The findings highlight a range of experiences during chemotherapy and offer insights into potential intervention targets.
Children experienced various challenges across all dimensions of well-being, with differences noted depending on age. Physically, symptoms such as fatigue, discomfort, and nausea were common, aligning with previous findings.7 Medical procedures were particularly distressing for the youngest children. Psychologically, younger participants experienced fear and treatment-related anticipation, while adolescents reported boredom, sadness, anxiety, and feelings of injustice—consistent with research on acute lymphoblastic leukemia.7 Socially, prolonged isolation with caregivers during hospitalization was noted. Although depressive symptoms were not directly mentioned by parents, the isolation they described echoes prior studies linking it to emotional distress.6 Communication-related difficulties were also evident, including inconsistent messaging from healthcare providers and impersonal interactions.
Although not initially a focus, the study also brought forward the difficulties experienced by parents. These included fatigue, emotional strain, and relationship tensions. Parents reported having to remain strong while concealing their own distress during extended hospital stays. Logistical difficulties, such as quitting jobs, long travel times, and suboptimal accommodations, compounded the stress. Institutional issues such as understaffing, lack of pediatric oncology expertise, rigid procedures, outdated infrastructure, and inadequate food or entertainment also emerged. These findings mirror previous research on parental experiences during childhood cancer treatment.30,31
Some resources were identified as helpful, including certain medical staff, psychosocial professionals, specialized educators, and tools like mobile phones or support from Leucan. However, several resources were deemed ineffective, such as poor internet access, inability to use gaming consoles, or young children being unable to benefit from mobile content. These barriers align with current reports on healthcare resource limitations in Quebec.22
When discussing VR, parents were mostly unfamiliar with the technology but expressed openness. They anticipated social, emotional, and educational benefits. These attitudes are consistent with recent findings from similar studies.32 However, parents emphasized that VR should complement, not replace human interaction. They also expressed concerns about limited space in hospital rooms and physical constraints due to medical equipment. Active interventions were considered more suitable for adolescents, while younger children might benefit more from passive interventions during rest periods. This interest in gamified and interactive content aligns with other studies that highlight the therapeutic potential of play and interaction.33
This study has several limitations and considerations for future research. The small number of participants limits the possibilities for generalization. However, we referred to authors who argue that in qualitative studies, data richness takes precedence over sample size. The objective of this study was not statistical generalization, but an in-depth understanding of the experiences, perceptions and meanings attributed by participants to pediatric cancer.25,34
The absence of data triangulation with children or healthcare professionals may have limited the diversity of perspectives captured. Selection bias may have occurred, as participants who agreed to participate may have been particularly motivated to share their stories or had specific experiences of care. Although children were eligible to participate in the study, none ultimately did, which may have restricted the depth of insights into the child’s lived experience. In future studies, involving children and healthcare professionals would enrich understanding, provide complementary viewpoints, and strengthen the validity of emerging themes.
Although children were eligible to participate in the study, none ultimately did. However, some parents reported discussing the study themes with their children beforehand, meaning certain child perspectives may have been indirectly captured through the parental lens. Previous research has shown that parent-child assessments of healthcare experiences, while correlated, are not always aligned.15,35 Recruitment difficulties are not uncommon in this population; studies suggest this may be due to prior access to care, lack of perceived need, or a desire to move on from their illness.36 This was reflected in P1’s statement: “Anything related to cancer—he tends to want to leave that behind him.”
The study remains methodologically sound and transparent. Data collection was conducted between March and July 2023, allowing sufficient time to explore participants’ in-depth experiences. The semi-structured interview guide included open-ended questions addressing three domains: (1) the child’s quality of life and emotional experience during chemotherapy, (2) parents’ own psychological and logistical experiences, and (3) their views on the potential role of VR as a supportive tool. This flexible structure encouraged rich, detailed narratives and ensured coherence with the research objectives.
Despite these limitations, this study makes a valuable contribution by centering the voices of parents at the earliest stage of a VR intervention’s design process. Few studies have incorporated end-user feedback this early, especially within a French-speaking Canadian context. These findings offer culturally grounded, developmentally nuanced insights that can inform the co-construction of meaningful digital tools. It offers insights into the daily realities of hospital care from a parental perspective and helps anticipate logistical and emotional barriers to VR implementation. Including end-users from the start increases the likelihood that any developed tool will be adapted to real-world needs and settings. Although the sample was small, it captured a broad developmental range, adding valuable nuance to the findings.
These findings also have important implications for clinical practice, particularly for Pediatric and Pediatric-focused Family Nurse Practitioners. These professionals play a central role in managing pediatric oncology care and are ideally placed to recognize psychosocial distress, advocate for developmentally tailored interventions, and support the integration of VR into holistic care plans. Their involvement in co-design, testing, and implementation of VR interventions can ensure alignment with clinical workflows, enhance family engagement, and improve the emotional well-being of young patients.
Building on these preliminary findings, future research should engage a broader range of stakeholders, including pediatric patients, healthcare professionals, and digital developers, to co-design and pilot-test a prototype VR intervention. This next phase should also include data triangulation across children, parents, and health workers to capture complementary perspectives and strengthen the ecological validity of findings. The integration of children’s voices, in particular, will be essential to refine the content, usability, and emotional resonance of VR tools. Furthermore, testing prototypes developed from the insights of this study will allow assessment of their feasibility, acceptability, and preliminary impact on well-being and engagement during treatment.
Participatory workshops and iterative usability testing could further refine the tool’s acceptability and optimize its integration into clinical practice. Ultimately, feasibility studies and subsequent clinical trials will be required to evaluate real-world implementation and measure clinical outcomes.
In conclusion, this study provides an important basis for the development of a virtual reality intervention for children undergoing cancer treatment. Feedback and recommendations from parents will be useful for developing future VR interventions aimed at supporting young cancer patients.
Conclusion
This study highlights the perspectives of parents of pediatric cancer survivors on the use of virtual reality during chemotherapy, emphasizing both their openness to this technology and the challenges of importance of maintaining human connection during medical procedures. Parents identified key physical, emotional, and logistical needs that a VR intervention could address, offering valuable insights to guide the co-design of personalized and developmentally appropriate digital tools for children with cancer.
Future work should now directly involve children and healthcare professionals to capture their lived experiences and refine the intervention in real clinical settings. This participatory approach will make it possible to develop and test VR solutions that are both engaging and clinically feasible, ensuring that they meet the emotional and cognitive needs of children across different stages of treatment.
Beyond the individual level, these findings should inform institutional policies in pediatric psychosocial care and support the systematic integration of digital health technologies into hospital routines. By translating these results into clinical guidelines and innovation strategies, healthcare systems can promote equitable access to safe, evidence-based, and family-centered VR tools ultimately improving the quality of life of children and their families during cancer treatment.
Declaration of Generative AI and AI-Assisted Technologies in the Writing Process
During the preparation of this work the authors used DeepL to translate in English the manuscript. After using this tool, the authors reviewed and edited the content as needed and takes full responsibility for the content of the publication.
Ethics Approval and Informed Consent
This study was approved by the Research Ethics Committee of University of Montreal (approval number: #2023-5239). Written informed consent was obtained from all participants prior to the interviews. The consent process included permission for the publication of anonymized responses and direct quotes. All procedures were conducted in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki declaration and its later amendments.
Acknowledgment
We thank the parents who participated in this study, as well as the Leucan and Cole Foundations for their support in disseminating this study.
Funding
This work was supported by the Foundation Cole. The funder of this study didn’t and won’t have any influence on the methodology of this study nor on the analysis and interpretation of results. DO is the recipient of a salary grant from the Fonds de recherche du Québec – Santé (https://doi.org/10.69777/329980).
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper. This paper has been uploaded to SSRN as a preprint: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=5223239
References
1. Registre québécois du cancer. Incidence du cancer: gouvernement du Québec. 2023. Available from: https://app.powerbi.com/view?r=eyJrIjoiNjc2ZTAxNmMtMWFiMi00NDIwLTg0MzYtOTY2OTIzMDliYjA2IiwidCI6IjA2ZTFmZTI4LTVmOGItNDA3NS1iZjZjLWFlMjRiZTFhNzk5MiJ9.
2. Ellison LF, Xie L, Sung L. Trends in paediatric cancer survival in Canada, 1992 to 2017. Health Reports. 2021;32(2):3–16. doi:10.25318/82-003-x202100200001-eng
3. Vlachioti E, Matziou V, Perdikaris P, et al. Assessment of quality of life of children and adolescents with cancer during their treatment. Jpn J Clin Oncol. 2016;46(5):453–461. doi:10.1093/jjco/hyw009
4. Anthony SJ, Selkirk E, Sung L, et al. Considering quality of life for children with cancer: a systematic review of patient-reported outcome measures and the development of a conceptual model. Qual Life Res. 2014;23(3):771–789. doi:10.1007/s11136-013-0482-x
5. Dupuis LL, Milne-Wren C, Cassidy M, et al. Symptom assessment in children receiving cancer therapy: the parents’ perspective. Support Care Cancer. 2010;18(3):281–299. doi:10.1007/s00520-009-0651-1
6. Li HC, Chung OK, Chiu SY. The impact of cancer on children’s physical, emotional, and psychosocial well-being. Cancer Nursing. 2010;33(1):47–54. doi:10.1097/NCC.0b013e3181aaf0fa
7. Dupuis LL, Lu X, Mitchell HR, et al. Anxiety, pain, and nausea during the treatment of standard-risk childhood acute lymphoblastic leukemia: a prospective, longitudinal study from the children’s oncology group. Cancer. 2016;122(7):1116–1125. doi:10.1002/cncr.29876
8. Fardell JE, Vetsch J, Trahair T, et al. Health-related quality of life of children on treatment for acute lymphoblastic leukemia: a systematic review. Pediatr Blood Cancer. 2017;64(9). doi:10.1002/pbc.26489
9. Abdulah DM, Abdulla BMO. Effectiveness of group art therapy on quality of life in paediatric patients with cancer: a randomized controlled trial. Complement Ther Med. 2018;41:180–185. doi:10.1016/j.ctim.2018.09.020
10. Leucan. L’art-thérapie 2019. Available from: https://www.leucan.qc.ca/fr/art-therapie/#:~:text=Leucan%20et%20la%20Fondation%20qu%C3%A9b%C3%A9coise,plus%20de%20d%C3%A9velopper%20sa%20cr%C3%A9ativit%C3%A9.
11. Ozturk CS, Toruner EK. Effectiveness of technology-based psychosocial interventions for child, adolescents and young adults undergoing cancer treatment: a meta-analysis of randomised controlled trials. Eur J Cancer Care. 2022;31(1):1–14. doi:10.1111/ecc.13515
12. Coughtrey A, Millington A, Bennett S, et al. The effectiveness of psychosocial interventions for psychological outcomes in pediatric oncology: a systematic review. J Pain Sympt Manag. 2018;55(3):1004–1017. doi:10.1016/j.jpainsymman.2017.09.022
13. Pathrose SP, Everett B, Patterson P, et al. Mindfulness-based interventions for young people with cancer: an integrative literature review. Cancer Nursing. 2021;44(5):349–360. doi:10.1097/NCC.0000000000000821
14. Czech O, Rutkowski S, Kowaluk A, Kiper P, Malicka I. Virtual reality in chemotherapy support for the treatment of physical functions, fear, and quality of life in pediatric cancer patients: a systematic review and meta-analysis. Frontiers in Public Health. 2023;11:1039720. doi:10.3389/fpubh.2023.1039720
15. Gerceker GO, Bektas M, Aydinok Y, Oren H, Ellidokuz H, Olgun N. The effect of virtual reality on pain, fear, and anxiety during access of a port with Huber needle in pediatric hematology-oncology patients: randomized controlled trial. Eur J Oncol Nurs. 2021;50:101886. doi:10.1016/j.ejon.2020.101886
16. Gold JI, SooHoo M, Laikin AM, Lane AS, Klein MJ. Effect of an immersive virtual reality intervention on pain and anxiety associated with peripheral intravenous catheter placement in the pediatric setting: a randomized clinical trial. JAMA Netw. 2021;4(8):e2122569. doi:10.1001/jamanetworkopen.2021.22569
17. Hundert AS, Birnie KA, Abla O, et al. A pilot randomized controlled trial of virtual reality distraction to reduce procedural pain during subcutaneous port access in children and adolescents with cancer. Clin J Pain. 2022;38(3):189–196. doi:10.1097/AJP.0000000000001017
18. Semerci R, Akgün Kostak M, Eren T, Avci G. Effects of virtual reality on pain during venous port access in pediatric oncology patients: a randomized controlled study. J Pediatr Oncol Nurs. 2021;38(2):142–151. doi:10.1177/1043454220975702
19. Wong CL, Li CK, Chan CWH, et al. Virtual reality intervention targeting pain and anxiety among pediatric cancer patients undergoing peripheral intravenous cannulation: a randomized controlled trial. Cancer Nursing. 2021;44(6):435–442. doi:10.1097/NCC.0000000000000844
20. Gouvernement du Québec. Tableau de bord - Performance du réseau de la santé et des services sociaux 2023. Available from: https://app.powerbi.com/view?r=eyJrIjoiOTFmZjc4NzAtMTBkMS00OTE5LWE4YjQtZTIzOTc5NDZjNmZlIiwidCI6IjA2ZTFmZTI4LTVmOGItNDA3NS1iZjZjLWFlMjRiZTFhNzk5MiJ9.
21. Coalition des psychologues du réseau public québécois. Commission parlementaire sur l’augmentation préoccupante de la consommation de psychostimulants chez les enfants et les jeunes en lien avec le trouble déficitaire de l’attention avec hyperactivité (TDAH): assemblée nationale du Québec. 2019. Available from: https://www.assnat.qc.ca/Media/Process.aspx?MediaId=ANQ.Vigie.Bll.DocumentGenerique_155641&process=Default&token=ZyMoxNwUn8ikQ+TRKYwPCjWrKwg+vIv9rjij7p3xLGTZDmLVSmJLoqe/vG7/YWzz.
22. Institut de la statistique du Québec. Les postes vacants au Québec par trimestre 2023. Available from: https://statistique.quebec.ca/fr/produit/publication/postes-vacants-au-quebec-par-trimestre.
23. Matza LS, Swensen AR, Flood EM, Secnik K, Leidy NK. Assessment of health-related quality of life in children: a review of conceptual, methodological, and regulatory issues. Value Health. 2004;7(1):79–92. doi:10.1111/j.1524-4733.2004.71273.x
24. Ponterotto JG. Qualitative research in counseling psychology: a primer on research paradigms and philosophy of science. J Counseling Psychol. 2005;52(2):126–136. doi:10.1037/0022-0167.52.2.126
25. Braun V, Clarke V. Using thematic analysis in psychology. qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
26. Guest G, Bunce A, Johnson L. How many interviews are enough?: an experiment with data saturation and variability: an experiment with data saturation and variability. Field Method. 2006;18(1):59–82. doi:10.1177/1525822X05279903
27. Braun V, Clarke V. Is thematic analysis used well in health psychology? A critical review of published research, with recommendations for quality practice and reporting. Health Psychol Rev. 2023;17(4):695–718. doi:10.1080/17437199.2022.2161594
28. Miles MB, Huberman AM. Analyse des données qualitatives.
29. Boyatzis RE. Transforming Qualitative Information: Thematic Analysis and Code Development. Sage Publications, Inc; 1998.
30. Lundgren J, Thiblin E, Lutvica N, et al. Concerns experienced by parents of children treated for cancer: a qualitative study to inform adaptations to an internet‐administered, low‐intensity cognitive behavioral therapy intervention. Psycho-Oncology. 2022;32(2):237–246. doi:10.1002/pon.6074
31. Enskär K, Carlsson M, Golsäter M, Hamrin E, Kreuger A. Parental reports of changes and challenges that result from parenting a child with cancer. J Pediatr Oncol Nurs. 1997;14(3):156–163. doi:10.1016/S1043-4542(97)90051-5
32. Tennant M, McGillivray J, Youssef GJ, McCarthy MC, Clark TJ. Feasibility, acceptability, and clinical implementation of an immersive virtual reality intervention to address psychological well-being in children and adolescents with cancer. J Pediatr Oncol Nurs. 2020;37(4):265–277. doi:10.1177/1043454220917859
33. Li WH, Chung JO, Ho EK. The effectiveness of therapeutic play, using virtual reality computer games, in promoting the psychological well-being of children hospitalised with cancer. J Clin Nurs. 2011;20(15–16):2135–2143. doi:10.1111/j.1365-2702.2011.03733.x
34. Patton M. Qualitative Research and Evaluation Methods.
35. Rodriguez EM, Dunn MJ, Zuckerman T, Vannatta K, Gerhardt CA, Compas BE. Cancer-related sources of stress for children with cancer and their parents. J Pediatr Psychol. 2011;37(2):185–197. doi:10.1093/jpepsy/jsr054
36. van Lankveld J, Fleer J, Schroevers MJ, Sanderman R, den Oudsten BL, Dekker J. Recruitment problems in psychosocial oncology research. Psycho-Oncology. 2018;27(9):2296–2298. doi:10.1002/pon.4792
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
“I Still Suffer Every Second of Every Day”: A Qualitative Analysis of the Challenges of Living with Chronic Orofacial Pain
Lovette BC, Bannon SM, Spyropoulos DC, Vranceanu AM, Greenberg J
Journal of Pain Research 2022, 15:2139-2148
Published Date: 29 July 2022
The Subjective Will and Psychological Experience of Home-Based Exercise in Lung Cancer Patients During Interval of Chemotherapy: A Qualitative Study
Hu Y, Chen X, Fan J, Huang Y, Ye J, Gu F, Li Y
Journal of Multidisciplinary Healthcare 2023, 16:663-674
Published Date: 9 March 2023
Patient Perspectives and Side-Effects Experience on Chemotherapy of Non-Small Cell Lung Cancer: A Qualitative Study
Zubair HM, Khan MA, Gulzar F, Alkholief M, Malik A, Akhtar S, Sharif A, Akhtar MF, Abbas M
Cancer Management and Research 2023, 15:449-460
Published Date: 25 May 2023
Physical Restraint Experience of Patients with Mental Disorders in Mainland China: A Qualitative Study
Chong Y, Wang C, Min H, Zhang L, Zhi T, Wu X, Wang Y
Journal of Multidisciplinary Healthcare 2024, 17:431-444
Published Date: 31 January 2024
Perspectives of People with Type 2 Diabetes Mellitus Towards a Decision Aid Assessing Preferences of Glucose-Lowering Drugs: The Dilemma of Choosing
Roldan Munoz S, Mol PGM, de Vries F, van Dijk PR, Hillege H, Postmus D, de Vries ST
Patient Preference and Adherence 2025, 19:215-234
Published Date: 25 January 2025