Back to Journals » Journal of Pain Research » Volume 15
“I Still Suffer Every Second of Every Day”: A Qualitative Analysis of the Challenges of Living with Chronic Orofacial Pain
Authors Lovette BC ![]() , Bannon SM, Spyropoulos DC, Vranceanu AM
, Bannon SM, Spyropoulos DC, Vranceanu AM ![]() , Greenberg J
, Greenberg J ![]()
Received 27 April 2022
Accepted for publication 17 July 2022
Published 29 July 2022 Volume 2022:15 Pages 2139—2148
DOI https://doi.org/10.2147/JPR.S372469
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Robert Twillman
Brenda C Lovette,1,2 Sarah M Bannon,2,3 Daphne Catherine Spyropoulos,4 Ana-Maria Vranceanu,2,3 Jonathan Greenberg2,3
1Department of Rehabilitation Sciences, MGH Institute of Health Professions, Boston, MA, USA; 2Center for Health Outcomes and Interdisciplinary Research, Department of Psychiatry, Massachusetts General Hospital, Boston, MA, USA; 3Department of Psychiatry, Harvard Medical School, Boston, MA, USA; 4Graduate School of Education, Fordham University, New York, NY, USA
Correspondence: Jonathan Greenberg, Center for Health Outcomes and Interdisciplinary Research, Department of Psychiatry, Massachusetts General Hospital, Boston, MA, USA, Email [email protected]
Objective: Chronic orofacial pain is prevalent and debilitating. Psychological and social factors place a heavy burden on this population but are often overlooked. Here, we offer the first comprehensive qualitative conceptualization of the challenges of living with chronic orofacial pain through a biopsychosocial perspective to inform multifaceted care for this population.
Design: We employed a qualitative thematic analysis of open text responses using a hybrid inductive-deductive approach and a biopsychosocial framework.
Methods: Two hundred and sixty participants with chronic orofacial pain responded to an open-ended question: “What is the biggest challenge you face in managing your condition?” by typing their responses into a text box as part of an online survey. We mapped responses onto biomedical, psychological, and social themes (deductive) and concurrently identified findings within each theme that emerged directly from the data (inductive).
Results: Subthemes within the biomedical theme included challenges with biomedical pain management, medication side effects, sensory triggers, physical symptoms of stress/tension, and biological functions and related activities of daily living. Subthemes within the psychological theme included anxiety, depression, emotional symptoms of stress, unpredictability/uncertainty of pain, and psychological and cognitive aspects of medication management. Subthemes within the social theme included social relational, experience with providers, socioeconomics and access to care, and roles and responsibilities.
Conclusion: Chronic orofacial pain is associated with multifaceted challenges. Consideration of individuals’ experiences of biomedical, psychological, and social challenges in the assessment, referral, and treatment of chronic orofacial pain holds the potential to promote more comprehensive, patient-centered care for this population.
Keywords: chronic orofacial pain, biopsychosocial model, qualitative research, thematic analysis
Background
Chronic orofacial pain is one of the most common forms of chronic pain.1,2 It is defined by the International Classification of Orofacial Pain (ICOP) as pain in the face, mouth, or jaw that is present for at least 15 days in the past month and spans at least 3 months.3,4 Chronic orofacial pain often results in substantial disability1,5,6 and places a heavy burden on the healthcare system.7,8
Chronic orofacial pain is largely conceptualized through a biomedical lens.9–11 Treatments for chronic orofacial pain similarly focus primarily on biomedical factors. Such treatments typically have low success rates,12 adverse side-effects,13 and can include unnecessary and painful procedures (eg, tooth extractions, occlusal adjustment) that may result in permanent damage.9,12,14 Despite this biomedical dominance, a growing body of evidence illustrates the interplay between psychological and social factors and chronic orofacial pain symptoms and outcomes. These include psychological distress (eg, stress9 and hopelessness15 as both risk factors16 and consequences of chronic orofacial pain1,17 as well as known social effects (eg, negative impact on relationships18 and decreased social quality of life19). To date, with temporomandibular pain as an exception, psychosocial considerations in orofacial pain management have received limited attention.20 This highlights a need for a comprehensive approach to characterizing the multitude of challenges confronted by individuals with chronic orofacial pain to better understand the range of this population’s needs.
The biopsychosocial model is a widely accepted approach for conceptualizing treatment for chronic pain.21 This model provides a useful framework for a more integrative assessment of these individuals’ experiences, concerns, and priorities.20,22 Identifying specific biomedical, psychological, and social challenges is critical for informing comprehensive care for this population and working towards meeting the variety of its needs. Qualitative research methods can generate a nuanced understanding of these individuals’ lived experiences and perceived challenges,20 and using the biopsychosocial model as a framework in qualitative research is a promising means to inform implementation of psychosocial care.23
The aim of the current study is to gain insight into the most challenging aspects of living with chronic orofacial pain based on individuals’ own perspectives. We sought to organize reported challenges using the biopsychosocial framework to capture the multifaceted nature of these challenges, identify unmet needs within specific domains and offer recommendations to improve biopsychosocial care for this population.
Methods
Participants and Procedures
This was a secondary analysis of data collected as part of a larger survey of individuals with chronic orofacial pain.24 We recruited participants via a newsletter to members of the Facial Pain Association (FPA), a non-profit organization serving individuals affected by facial pain, between March and June 2021. To be included in this study, participants had to be adults living in the United States, have an ability to read and write in English at a 6th grade level, and report having nonmalignant facial pain of any kind for more than 3 months. Participants indicated their consent on an electronic form prior to completing a series of questionnaires. All study procedures were approved by the Massachusetts General Hospital Institutional Review Board and comply with the Declaration of Helsinki.
Three hundred and three participants responded to an online battery of questionnaires,24 of which 260 responded to the single open-ended question we report on here: “What is the biggest challenge you face in managing your condition?” Participants typed their responses into a text box. Self-reported demographic and diagnostic information is detailed in Table 1. We classified reported diagnoses based on the International Classification of Orofacial Pain, 1st edition (ICOP).4 Final diagnosis categories included trigeminal neuralgia, other trigeminal neuropathic pain, classical trigeminal neuralgia with concomitant continuous pain, persistent idiopathic facial pain, and other less common diagnoses (eg, myofascial pain, glossopharyngeal neuralgia). Additionally, 22% of participants reported multiple cooccurring diagnoses.
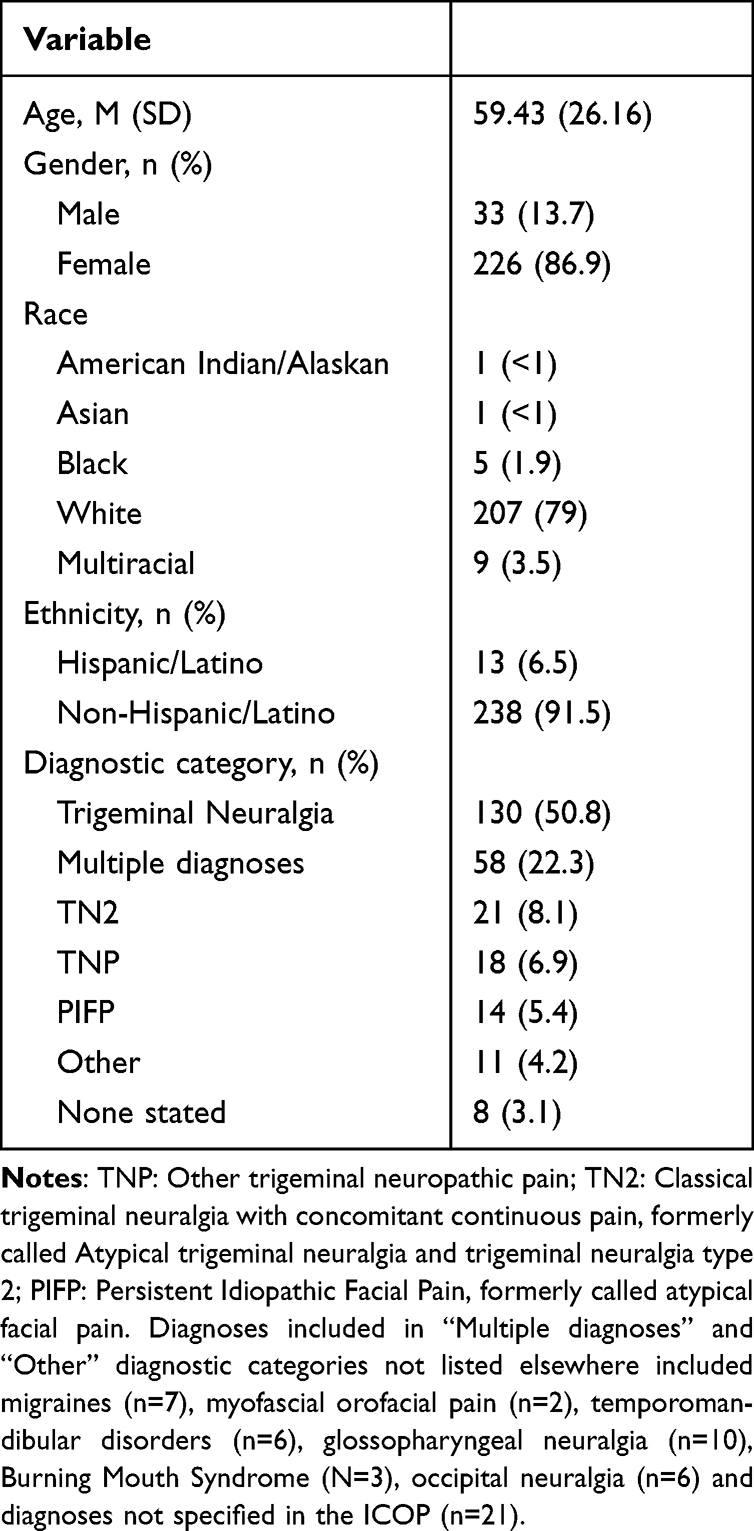 |
Table 1 Participant Demographics |
Data Analysis
We synthesized our findings utilizing a hybrid inductive-deductive thematic analysis approach.25,26 This methodological approach allows integration of data-driven codes with theory-driven ones based on the tenets of social phenomenology (ie, subjective perspective of individuals living in the world).26 Our approach was deductive in the sense that we mapped findings onto biomedical, psychological, and social themes that we selected a priori based on the theoretical framework of the biopsychosocial model.27 Our approach was also inductive in that we concurrently identified findings within each theme that emerged directly from the data. Specifically, we grouped and organized codes to allow novel findings within each a priori theme to develop. We defined a-priori themes based on the biopsychosocial model: 1) biomedical (ie, challenges relating to physical function and physiological aspects of injury), 2) psychological (ie, challenges relating to cognition, coping, emotion, and mental health or well-being) and 3) social (ie, challenges relating to interpersonal, socioeconomic, community and life participation factors).27,28
First, 2 coders (BL and DS) separately reviewed and open coded 15% of responses (n = 39). The team (BL, DS, JG, and SB) then met to discuss and agreed on a set of common codes. The data analysis team consisted of two clinical and research psychologists and two doctoral students in the fields of psychology and rehabilitation science. Next, the two coders reviewed another 15% of responses and met again to determine if any additional codes surfaced that were not previously conceptualized. Then, the two coders (BL and DS) coded all remaining responses and re-reviewed the first 30% of responses to ensure optimal fit to the final code list. Coders met again to discuss and resolve any discrepancies. Two members of the team (BL and JG) then met to review coded data, combine codes into broader parent codes, and identify sub-themes and representative exemplar quotes. We allowed partial overlap between the themes consistent with the view of the biopsychosocial model as a system of three interdependent factors, and in line with common practices in thematic analysis highlighting theme interconnectedness.29,30
Results
We organized codes of the challenges participants reported into biomedical, psychological, and social themes, and identified subthemes within each of these deductive themes, presented in Table 2 with exemplar quotes. Figure 1 depicts the distinct and overlapping subthemes across the model. Below, we describe nuances as occurring in “some” instances to present findings that were neither very rare nor highly frequent (occurred more than three but fewer than 20 times).
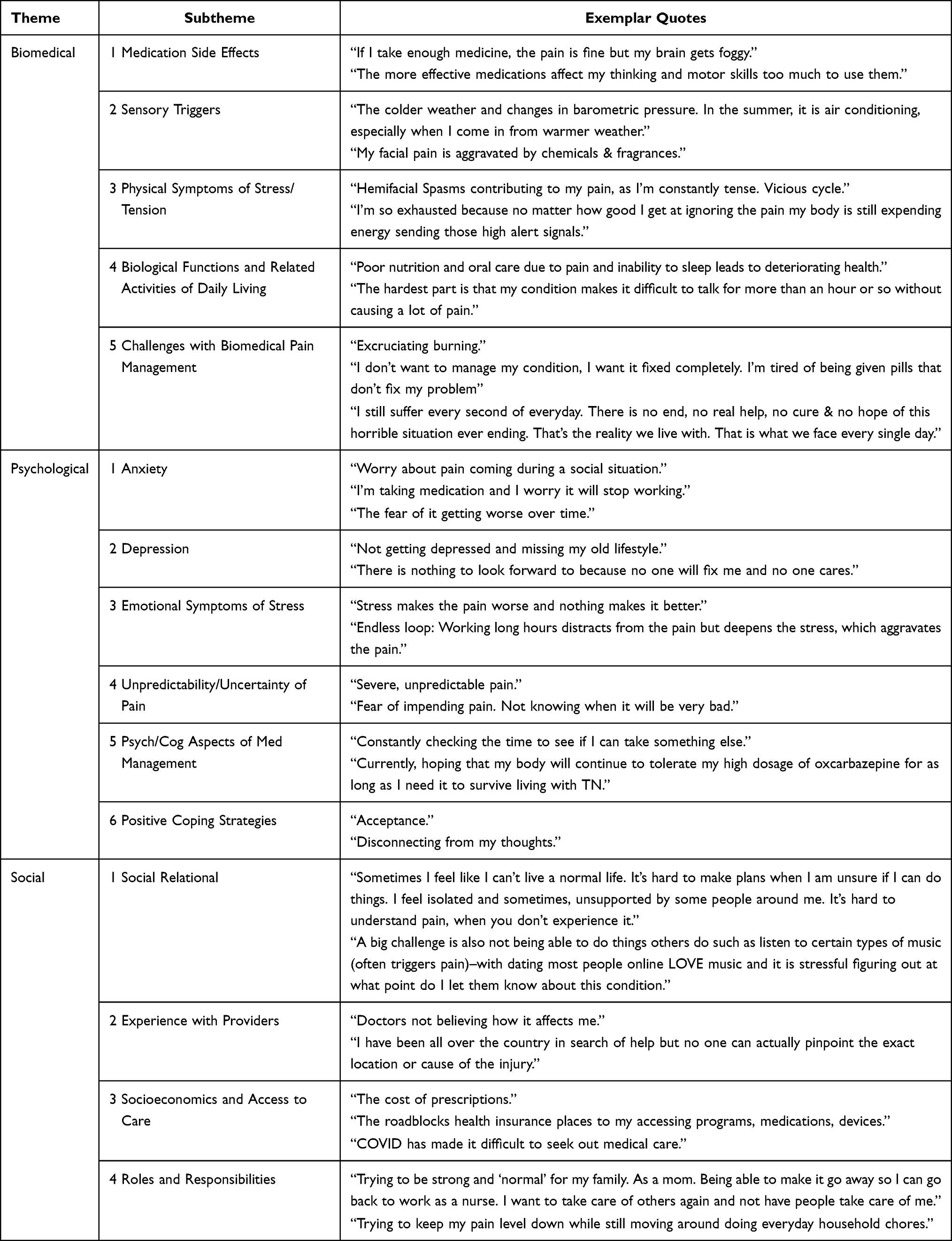 |
Table 2 Themes, Subthemes, and Exemplar Quotes |
 |
Figure 1 Biopsychosocial model: map of subthemes. |
Biomedical Challenges
We identified five subthemes within the biomedical theme including challenges with biomedical pain management, biological functions and related activities of daily living, medication side effects, sensory triggers, and physical symptoms of stress/tension. Challenges with biomedical pain management were the most common subtheme, reported by a third of participants. Participants described challenges relating to finding effective treatments and solutions, as well as the severity, constancy, progression, and/or chronicity of their pain. Participants described the uncontrollability of pain, in that pain did not respond to medications or other treatments, or that once breakthrough pain occurred it was long lasting and difficult to resolve.
The second most common subtheme was biological functions and related activities of daily living which included difficulty eating, sleeping, speaking, maintaining hygiene, and other daily activities. Some associated their poor sleep and nutrition with overall deterioration of health. Several participants described speech and communication as major challenges. For example, one reported “I am the grunt master. Hard to talk and sometimes text.” When describing medication side effects, participants often reported facing a dilemma choosing between experiencing pain and facing cognitive challenges, fogginess, fatigue, balance, dizziness, and motor issues caused by medication. Other medication side effects included allergies and problematic interactions between medications. Participants further noted challenges associated with sensory triggers of pain such as weather (eg, temperature and wind), and other aspects of the environment (eg, chemicals and fragrances). Two participants specifically described challenges with the typical climate in their home regions: fog in San Francisco, and cold in Minnesota winters. While sensory triggers are a hallmark of trigeminal neuralgia,4 participants in nearly all diagnostic categories identified environmental and sensory triggers as one of their greatest challenges. Challenges associated with physical symptoms of stress/tension included tense muscles, spasms, and high energy expenditure related to pain and resulting in exhaustion.
Psychological Challenges
We identified six subthemes within the psychological theme including anxiety, depression, emotional symptoms of stress, unpredictability/uncertainty of pain, psychological and cognitive aspects of medication management, and positive coping strategies (including resilience and mindfulness).
Challenges depicting anxiety/worry typically focused on either disease progression (eg, worsening of pain and function over time, medications becoming ineffective) or were more general worry about the future. The constant vigilance about pain management and avoidance of triggers caused some to “drive [themselves] crazy dwelling on it.” Challenges pertaining to anxiety sometimes cooccurred with challenges relating to the unpredictability of pain. Participants worried about flairs occurring at inopportune times, such as during social activities, or for those who have found some relief, when their breakthrough pain might return. One participant described “always wondering when the next shock is going to come.”
Participants also described experiencing difficulties related to depression symptoms such as hopelessness and negative thinking. Some described these symptoms in connection to grief and loss of their “old lifestyle” and changes in their identity as well as their perception of having “nothing to look forward to”. One participant indicated experiencing suicidal ideation in the past.
Issues related to psychological and cognitive aspects of medication management dominated participants’ lives, requiring them to constantly check their clock and medication schedule or monitor and revise dosage. Some experienced mood fluctuations as the effects of their medications/treatments waned resulting in feeling “miserable and often irrational”. Some were concerned for their body’s ability to tolerate high doses of strong medication “for as long as [they] need it to survive living with [their diagnosis]”.
Some reported that emotional symptoms of stress were their greatest challenge, typically in that it contributed to the cycle of worsening pain resulting in increased stress. Rarely, participants complemented the challenges that they identified with positive coping strategies including resilience, acceptance, and mindfulness, and described attempting to keep a positive mindset or “living day to day”.
Social Challenges
We identified four subthemes within social theme including roles and responsibilities (including home, community, and employment), experience with providers (competence of providers, differential diagnosis), social relational (including social isolation and social identity/other social challenges), and socioeconomics and access to care.
The most common sub-theme within the social domain was challenges related to roles and responsibilities. Some participants described challenges related to loss of work and described difficulty obtaining and keeping a job due to the disruptive and debilitating nature of pain. Some described how pain and avoidance of triggers impacted ability to complete home and community level responsibilities including chores and shopping/errands. Participants also described challenges in their ability to parent, spend time with family, and serve as caregiver to others.
Second most common were challenges regarding participants’ experience with providers. Participants found it difficult or “impossible” to find doctors with the knowledge and skills needed. Some expressed frustration at the lack of empathy and attention they received from providers. Others reported their difficulty with establishing a differential diagnosis and described traveling the country seeking answers.
Social relational challenges included social isolation, social activity, and identity. Participants expressed a sense of isolation due to living with an “invisible” illness. Others reported opting out of social engagements due to pain or fear of onset of pain. Participants reported feeling misunderstood by family, friends, and others who do not live with chronic pain. Some reported challenges with making plans, dating, maintaining relationships, and generally “being normal.”
Participants also noted challenges related to socioeconomics and access to care. Some participants described struggling to live on reduced income from disability and social security. Several experienced difficulty affording their medications and/or lacked adequate insurance coverage for programs and treatments (eg alternatives to pharmacological treatments such as supplements, therapies, and acupuncture). Additionally, the societal impact of the COVID-19 pandemic impacted access to orofacial pain care due to barriers such as cancelled appointments and surgeries, and limited seating in pharmacies.
Discussion
We conducted the first qualitative thematic analysis of individuals’ perceived challenges due to chronic orofacial pain. We utilized a hybrid inductive-deductive approach and synthesized findings using a biopsychosocial framework in order to promote a comprehensive understanding of challenges experienced by impacted individuals. We summarize findings and offer specific recommendations for each challenge in the sections below.
We identified biomedical subthemes including challenges with biomedical pain management, medication side effects, biological functions and related activities of daily living, sensory triggers, and physical symptoms of stress/tension. The most frequently identified sub-theme was challenges with biomedical pain management. Individuals often described a lengthy and frustrating search for pain relief, and many failed treatment attempts. This is consistent with previous research on efficacy of treatments for chronic orofacial pain indicating a success rate of less than 25%.12 Participants reported ubiquitous use of pharmacological treatment with unpleasant and debilitating motor, cognitive, and mood related side effects. Consistent with previously published studies,15 participants identified pervasive difficulty with biological functions and related activities of daily living which ultimately negatively impacted overall health and wellness. Additionally, participants reported challenges with sensory triggers and described physical symptoms of stress/tension as both a cause and effect of their pain. To address the aforementioned challenges with medication side effects, providers may consider integrating discussion of these common side effects into standard care to empower patients to make conscious choices about the cost benefit of their medications. Providers may also consider opioid rotation, changing administration route,31 dietary changes (increased fiber),31 or complementary treatments such as acupuncture32 to help manage medication side effects. To address challenges with biological functions and related activities of daily living, providers should include assessment and treatment of sleep, communication, nutrition, or other aspects of self-care to optimize patients’ health and function despite their pain.33 Patients may benefit from referrals including occupational therapy for modifications to activities of daily living,34 speech language pathology for treatment of speech, communication, and swallowing function, and nutrition and dietetics to address patients’ nutritional needs in the setting of odynophagia. Additionally, patients who experience sensory triggers could benefit from counseling to identify their unique environmental triggers, develop predictive awareness to avoid them, and establish a toolkit of strategies to manage them. Finally, patients who experience physical symptoms of stress/tension could benefit from pain-informed mind-body interventions to develop skills around interrupting patterns of stress, tension, energy expenditure, and pain.35
We identified psychological challenges including anxiety, depression, emotional symptoms of stress, unpredictability/uncertainty of pain, psychological and cognitive aspects of medication management, and positive coping strategies (resilience/mindfulness). Participants described the interplay of depression, anxiety, and general mental suffering with the severity of their pain condition. They additionally mentioned the unpredictability of their pain as a source of anxiety which impacted their ability or willingness to participate in social activities and work. Results are consistent with previous work indicating that psychological factors can play a role in the manifestation of chronic orofacial pain.9,36 Several psychosocial interventions have demonstrated feasibility and potential utility of use among people living with chronic orofacial pain including: Cognitive Behavioral Therapy, relaxation, and biofeedback.36–40 However, prior research notes limited discussion between providers and patients of such opportunities, resulting in limited access to these interventions.9 Our results indicate a need for accessible programs to be more commonly embedded in standard care to address the specific psychological experiences of people with chronic orofacial pain. Providers who have contact with people with orofacial pain, particularly those directing care plans (dentists, neurologist, and primary care physicians) should be aware of these psychological challenges and screen patients for emotional distress and make referrals to psychosocial care when indicated.
We identified subthemes within the social theme including social relational challenges, roles and responsibilities, experiences with providers, and socioeconomics and access to care. Our findings are consistent with prior research that suggests that experiences of not being understood by friends, family, and society at large are common among people living with all types of chronic pain.41 Participants in this study linked their isolation and change in social roles and responsibilities to feelings of depression and overall decreased participation in society contributing to a troubling cycle of isolation, hopelessness, grief, and changes to identity roles. To address these social challenges, patients with orofacial pain may benefit from dyadic and systemic approaches to treatment which involve spouses and family members. Clinicians may additionally provide patients with information about resources such as orofacial pain support groups, online forums, and orofacial pain advocacy organizations (eg, the Facial Pain Association).
Participants emphasized their difficult experiences with providers and navigating care (eg, distress around not being “believed”, difficulty obtaining a definitive diagnosis, and perceived lack of knowledgeable providers). These findings are consistent with prior research on chronic orofacial pain9,42 and suggest a need for more training and resources for providers who manage these cases. Trainings could include building communication skills and strategies for complex cases, and raising awareness of the prevalence of idiopathic presentation of orofacial pain. Difficulty accessing care due to the cost of treatment and insurance coverage issues is consistent with the broader literature on disparities in access to care, and may be particularly pronounced for those who are uninsured, experiencing financial insecurity, or who have less financial resources.43 Patients could benefit from increased access to social work to assist in navigating financial and social resources and establish vocational accommodations when indicated. This may also inform potential changes in policy such as reduced cost for effective pharmaceuticals, and expansion of coverage to evidence-based complementary therapies.
Overall, these results offer a novel perspective emphasizing the co-occurring and interdependent challenges associated with chronic orofacial pain and underscore the importance of assessing and addressing biomedical, psychological and social aspects of living with orofacial pain. As depicted in Figure 1, some of the subthemes identified fall close to the intersection of multiple domains of the biopsychosocial model, suggesting notable implications for treatment planning and delivery. Challenges associated with chronic orofacial pain may be distributed across a bio-psycho-social continuum, and challenges in one domain may produce challenges in another domain. This interplay has implications for case conceptualization and intervention. For example, when prescribing medications for pain management, providers should be aware of psychological and cognitive factors important to successful medication management and provide education and resources as needed.
This study has several strengths. First, we included a relatively large number of participants from a national association with a geographically broad area, which enabled us to gather diverse perspectives comprehensively capture a wide range of challenges associated with chronic orofacial pain across individuals. Second, we included individuals with a variety of orofacial pain diagnoses. While most previous research on orofacial pain silos participants based on their different diagnoses, the current findings reveal more similarities than differences in challenges experienced among the diagnoses represented in our sample. This supports a transdiagnostic approach to management of orofacial pain which may increase scalability of treatments for this population.44 Third, this paper focused on patients’ perspectives and lived experiences, which are often overlooked in quantitative literature in general, and in orofacial pain research in particular, and are important to inform treatment priorities.
Limitations
Several limitations of this study should also be considered. First, participants responded by typing in a text box as part of an online survey. As such, we may have not gathered as in-depth responses as those gathered by other qualitative methods, such as semi-structured interviews. Second, while our sample included individuals with several of orofacial pain conditions, approximately half of the sample reported trigeminal neuralgia as their primary diagnosis. All demographics were self-reported, including pain diagnosis, which may be limited by participants’ awareness of their diagnosis or willingness to disclose. Our sample was predominantly white (79%). Thus, the perspectives of some diagnostic and racial identity groups may be underrepresented in this sample. This is of particular importance given the difference in pain outcomes and treatment disparities between ethnic and racial groups.43
Conclusions
Individuals with chronic orofacial pain face a range of challenges across the biopsychosocial continuum. Multimodal programs for people with chronic orofacial pain may be particularly suitable for targeting these heterogeneous challenges. Consideration of biomedical, psychological, and social factors in the assessment, referral, and treatment of individuals with chronic orofacial pain holds potential to considerably improve care for this population. Further research is warranted to clarify differential challenges associated with specific orofacial pain conditions.
Data Sharing Statement
The data that support the findings of this study are available on request from the corresponding author.
Acknowledgment
We would like to thank the Facial Pain Association for their contribution to data collection in this study.
Funding
This study was funded by grants from the National Center for Complementary and Integrative Health to JG (1K23AT01065301A1) and AMV (1K24AT011760-01).
Disclosure
Authors declare that they have no conflicts of interest.
References
1. Macfarlane TV, Blinkhorn AS, Davies RM, Kincey J, Worthington HV. Oro-facial pain in the community: prevalence and associated impact. Community Dent Oral Epidemiol. 2002;30(1):52–60. doi:10.1034/j.1600-0528.2002.300108.x
2. National Institute of Dental and Craniofacial Research. Facial pain; 2018. Available from: https://www.nidcr.nih.gov/research/data-statistics/facial-pain.
3. Ananthan S, Benoliel R. Chronic orofacial pain. J Neural Transm. 2020;127(4):575–588. doi:10.1007/s00702-020-02157-3
4. Orofacial Pain Classification Committee. International classification of orofacial pain, 1st edition (ICOP). Cephalalgia. 2020;40(2):129–221. doi:10.1177/0333102419893823
5. Haviv Y, Zini A, Etzioni Y, et al. The impact of chronic orofacial pain on daily life: the vulnerable patient and disruptive pain. Oral Surg Oral Med. 2017;123(1):58–66. doi:10.1016/j.oooo.2016.08.016
6. Zakrzewska JM, Wu J, Mon-Williams M, Phillips N, Pavitt SH. Evaluating the impact of trigeminal neuralgia. Pain. 2017;158(6):1166–1174. doi:10.1097/j.pain.0000000000000853
7. Breckons M, Shen J, Bunga J, Vale L, Durham J. DEEP study: indirect and out-of-pocket costs of persistent orofacial pain. J Dent Res. 2018;97(11):1200–1206. doi:10.1177/0022034518773310
8. Durham J, Shen J, Breckons M, et al. Healthcare cost and impact of persistent orofacial pain: the DEEP study cohort. J Dent Res. 2016;95(10):1147–1154. doi:10.1177/0022034516648088
9. Peters S, Goldthorpe J, McElroy C, et al. Managing chronic orofacial pain: a qualitative study of patients’, doctors’, and dentists’ experiences. Br J Health Psychol. 2015;20(4):777–791. doi:10.1111/bjhp.12141
10. Zakrzewska JM, Akram H. Neurosurgical interventions for the treatment of classical trigeminal neuralgia. Cochrane Database Syst Rev. 2011;2011(9). doi: 10.1002/14651858.CD007312.pub2
11. Obermann M, Katsarava Z. Update on trigeminal neuralgia. Expert Rev Neurother. 2009;9(3):323–329. doi:10.1586/14737175.9.3.323
12. Beecroft EV, Durham J, Thomson P. Summary of: retrospective examination of the healthcare ‘journey’ of chronic orofacial pain patients referred to oral and maxillofacial surgery. Br Dent J. 2013;214(5):236–237. doi:10.1038/sj.bdj.2013.221
13. Furlan AD, Sandoval JA, Mailis-Gagnon A, Tunks E. Opioids for chronic noncancer pain: a meta-analysis of effectiveness and side effects. Cmaj. 2006;174:1589–1594. doi:10.1503/cmaj.051528
14. Pfaffenrath V, Rath M, Pöllmann W, Keeser W. Atypical facial pain-application of the IHS criteria in a clinical sample. Cephalalgia. 1993;13(12_suppl):84–88. doi:10.1177/0333102493013S1218
15. Wolf E, Birgerstam P, Nilner M, Petersson K. Nonspecific chronic orofacial pain: studying patient experiences and perspectives with a qualitative approach. J Orofac Pain. 2008;22(4):349–358.
16. Aggarwal VR, Macfarlane GJ, Farragher TM, McBeth J. Risk factors for onset of chronic oro-facial pain–results of the North Cheshire oro-facial pain prospective population study. Pain. 2010;149(2):354–359. doi:10.1016/j.pain.2010.02.040
17. Alrashdan MS, Alkhader M. Psychological factors in oral mucosal and orofacial pain conditions. Eur J Dent. 2017;11(4):548–552. doi:10.4103/ejd.ejd_11_17
18. Garro LC, Stephenson KA, Good BJ. Chronic illness of the temporomandibular joints as experienced by support-group members. J Gen Intern Med. 1994;9(7):372–378. doi:10.1007/BF02629516
19. Di Fabio RP. Physical therapy for patients with TMD: a descriptive study of treatment, disability, and health status. J Orofac Pain. 1998;12(2):24–135.
20. Durham J, Raphael KG, Benoliel R, Ceusters W, Michelotti A, Ohrbach R. Perspectives on next steps in classification of oro-facial pain - part 2: role of psychosocial factors. J Oral Rehabil. 2015;42(12):942–955. doi:10.1111/joor.12329
21. Gatchel RJ, McGeary DD, McGeary CA, Lippe B. Interdisciplinary chronic pain management: past, present, and future. Am Psychol. 2014;69(2):119–130. doi:10.1037/a0035514
22. Penlington C, Ohrbach R. Biopsychosocial assessment and management of persistent orofacial pain. Oral Surg. 2019;13(4):349–357.
23. Vranceanu AM, Bakhshaie J, Reichman M, et al. Understanding barriers and facilitators to implementation of psychosocial care within orthopedic trauma centers: a qualitative study with multidisciplinary stakeholders from geographically diverse settings. Implement Sci Commun. 2021;2(1):102. doi:10.1186/s43058-021-00208-8
24. Greenberg J, Bakhshaie J, Lovette BC, Vranceanu AM. Association between coping strategies and pain-related outcomes among individuals with chronic orofacial pain. J Pain Res. 2022;11(15):431–442. doi:10.2147/JPR.S350024
25. Bingham A, Witkowsky P. Qualitative analysis: deductive and inductive approaches. In: Vanover C, Mihas P, Saldaña Jeditors. Analyzing and Interpreting Qualitative Data: After the Interview. SAGE Publications; 2022:133–146. Available from: https://www.andreajbingham.com/resources-tips-and-tricks/deductive-and-inductive-approaches-to-qualitative-analysis.
26. Fereday J, Muir-Cochrane E. Demonstrating rigor using thematic analysis: a hybrid approach of inductive and deductive coding and theme development. Int J Qual Methods. 2006;5(1):80–92. doi:10.1177/160940690600500107
27. Engel GL. The need for a new medical model: a challenge for biomedicine. Science. 1977;196(4286):129–136.
28. Blackwell B, Galbraith JR, Dahl DS. Chronic pain management. Hosp Community Psychiatry. 1984;35(10):999–1008. doi:10.1176/ps.35.10.999
29. Pope C, Ziebland S, Mays N. Analysing qualitative data. BMJ. 2000;320(7227):114–116. doi:10.1136/bmj.320.7227.114
30. Nowell LS, Norris JM, White DE, Moules NJ. Thematic analysis: striving to meet the trustworthiness criteria. Int J Qual Methods. 2017;16(1):1609406917733847. doi:10.1177/1609406917733847
31. Rogers E, Mehta S, Shengelia R, Reid MC. Four strategies for managing opioid-induced side effects in older adults. Clin Geriatr. 2013;21(4). Available from: http://www.consultant360.com/articles/four-strategies-managing-opioid-induced-side-effects-older-adults.
32. Han C, Liu Y, Fan H, Li D, Guo N. Acupuncture relieves opioid-induced constipation in clinical cancer therapy – a meta-analysis and systematic review. Clin Epidemiol. 2021;2(13):907–919. doi:10.2147/CLEP.S324193
33. Dueñas M, Salazar A, de Sola H, Failde I. Limitations in activities of daily living in people with chronic pain: identification of groups using clusters analysis. Pain Pract. 2020;20(2):179–187. doi:10.1111/papr.12842
34. Robinson K, Kennedy N, Harmon D. Is occupational therapy adequately meeting the needs of people with chronic pain? Am J Occup Ther. 2011;65(1):106–113. doi:10.5014/ajot.2011.09160
35. Greenberg J, Popok PJ, Lin A, et al. A mind-body physical activity program for chronic pain with or without a digital monitoring device: proof-of-concept feasibility randomized controlled trial. JMIR Form Res. 2020;4(6):e18703. doi:10.2196/18703
36. Goldthorpe J, Peters S, Lovell K, McGowan L, Aggarwal V. “I just wanted someone to tell me it wasn’t all in my mind and do something for me”: qualitative exploration of acceptability of a CBT based intervention to manage chronic orofacial pain. Br Dent J. 2016;220(9):459–463. doi:10.1038/sj.bdj.2016.332
37. Litt MD, Shafer DM, Kreutzer DL. Brief cognitive-behavioral treatment for TMD pain: long-term outcomes and moderators of treatment. Pain. 2010;151(1):110–116. doi:10.1016/j.pain.2010.06.030
38. Tan G, Glaros A, Sherman R, Wong C. Integrative approaches to orofacial pain: role of biofeedback and hypnosis. In: Orofacial Disorders: Current Therapies in Orofacial Pain and Oral Medicine. Cham: Springer; 2017:317–24.
39. Bergdahl J, Anneroth G, Perris H. Cognitive therapy in the treatment of patients with resistant burning mouth syndrome: a controlled study. J Oral Pathol Med. 1995;24(5):213–215. doi:10.1111/j.1600-0714.1995.tb01169.x
40. Noma N, Watanabe Y, Shimada A, et al. Effects of cognitive behavioral therapy on orofacial pain conditions. J Oral Sci. 2020;63(1):4–7. doi:10.2334/josnusd.20-0437
41. Bannon S, Greenberg J, Mace RA, Locascio JJ, Vranceanu AM. The role of social isolation in physical and emotional outcomes among patients with chronic pain. Gen Hosp Psychiatry. 2021;69:50–54. doi:10.1016/j.genhosppsych.2021.01.009
42. Durham J, Steele J, MAdel M, Wassell R, Robinson P, Exley C. Temporomandibular disorder patients’ journey through care: TMD patients’ journey through care. Community Dent Oral Epidemiol. 2011;39(6):532–541. doi:10.1111/j.1600-0528.2011.00608.x
43. Morales ME, Yong RJ. Racial and ethnic disparities in the treatment of chronic pain. Pain Med Malden Mass. 2021;22(1):75–90. doi:10.1093/pm/pnaa427
44. Wessely S, Nimnuan C, Sharpe M. Functional somatic syndromes: one or many? Lancet Lond Engl. 1999;354(9182):936–939. doi:10.1016/S0140-6736(98)08320-2
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Physical Restraint Experience of Patients with Mental Disorders in Mainland China: A Qualitative Study
Chong Y, Wang C, Min H, Zhang L, Zhi T, Wu X, Wang Y
Journal of Multidisciplinary Healthcare 2024, 17:431-444
Published Date: 31 January 2024
Perspectives of People with Type 2 Diabetes Mellitus Towards a Decision Aid Assessing Preferences of Glucose-Lowering Drugs: The Dilemma of Choosing
Roldan Munoz S, Mol PGM, de Vries F, van Dijk PR, Hillege H, Postmus D, de Vries ST
Patient Preference and Adherence 2025, 19:215-234
Published Date: 25 January 2025
Parental Voices on Virtual Reality in Pediatric Oncology: Experiences, Needs, and Pathways for Co-Design
Hélie C, Véronneau J, Desjardins O, Barada L, Lebeau J, Ogez D
Journal of Multidisciplinary Healthcare 2025, 18:7551-7565
Published Date: 19 November 2025