")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 17
Physical Restraint Experience of Patients with Mental Disorders in Mainland China: A Qualitative Study
Authors Chong Y , Wang C, Min H, Zhang L , Zhi T, Wu X, Wang Y
Received 1 September 2023
Accepted for publication 16 January 2024
Published 31 January 2024 Volume 2024:17 Pages 431—444
DOI https://doi.org/10.2147/JMDH.S438269
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Steve Campbell
Yue Chong,1 Can Wang,1 Haiying Min,1 Lei Zhang,1 Tingting Zhi,2 Xiaoning Wu,1 Yanbo Wang1
1Clinical Research Center for Mental Disorders, Shanghai Pudong New Area Mental Health Center, School of Medicine, Tongji University, Shanghai, 200124, People’s Republic of China; 2Shanghai Baoshan Mental Health Center, Shanghai, 201900, People’s Republic of China
Correspondence: Yanbo Wang, Clinical Research Center for Mental Disorders, Shanghai Pudong New Area Mental Health Center, School of Medicine, Tongji University, Shanghai, 200124, People’s Republic of China, Tel +86-21-65986226, Email [email protected]
Introduction: The use of physical restraint (PR) is considered a controversial practice and research in Western countries has demonstrated negative physical and psychological consequences for patients, as well as staff, family members/carers, organisations and society as a whole. However, there are few research reports on restraint experiences of patients with mental disorders in non-Western countries, especially in mainland China.
Aim: This study aims to explore the subjective experiences and perceptions of patients with psychiatric disorders who have experienced PR in mainland China.
Methods: Semi-structured interviews were conducted with 8 inpatients with mental disorders in convalescence at a specialized mental health hospital in Shanghai. Interviews were recorded on audiotape and transcribed verbatim. Transcripts were analyzed using thematic analysis.
Results: Five themes emerged: “perception and understanding of PR”, “response to PR”, “negative physical and psychological experiences”, “unmet care needs during PR” and “changes after PR”, which together characterize patients’ perceptions, experiences, feelings, and needs in PR.
Conclusion: The use of PR involves ethical issues and brings negative experiences to patients with mental disorders that cannot be ignored and should be used as a last resort. Different patients have different attitudes and reactions to PR. During PR, patients’ physical and psychological needs are not adequately met. Medical staff should give more attention to patients in PR, meet their physical and psychological needs, and actively seek PR alternatives and reduction options based on evidence-based resources on restraint reduction available in the West and the national context and culture of China.
Keywords: physical restraint, psychiatric nursing, thematic analysis, qualitative research
Introduction
In China, physical restraint (PR) refers to a measure imposed on patients with mental disorders to control and stop the occurrence or escalation of harmful behaviors, including the use of instruments and equipment such as restraining belts to immobilize the patient’s body so that he or she cannot control or easily remove.1 PR is considered an intervention of last resort, and the appropriate use of PR is described in the Mental Health Law of the People’s Republic of China. China outlined in Article 40 of the Mental Health Law of the People’s Republic of China from 2013 that “in the absence of alternative measures, medical institutions and their medical personnel may implement protective medical measures such as restraint and isolation when incidents occur or will occur in medical institutions among patients who may harm themselves, endanger the safety of others, or disrupt the medical order”.
A systematic review revealed that the use of PR ranged from 3.8% to 20% globally.2 The use of PR had given rise to various controversies. Various studies have reported that the application of PR can bring significant physical and psychological risks, interfere with the development of therapeutic relationships between patients and healthcare workers, and is inconsistent with the principles of trauma-informed, recovery-oriented care.3 From the perspective of patients, PR conflicts with their wishes, limiting their freedom. Additionally, PR can cause physical and psychological harm to patients. On the one hand, PR may lead to physical injuries including skin damage, circulatory disorders, limb dysfunction, lung diseases, pressure sores, physical pain, and even sudden death.4–6 On the other hand, restrained patients are susceptible to psychological trauma, including negative emotions such as depression, humiliation, anger, sadness, fear, and even post-traumatic stress disorder (PTSD).7,8
Reducing PR is an important measure of humanistic care for psychiatric patients. Many studies have shown that understanding patients’ subjective experiences and perceptions of PR in restraint situations is critical if the use of PR in psychiatry is to be reduced and PR care is to be optimized.9 To date, other countries have published a large number of studies on the qualitative experience of restraint in patients with mental disorders, and based on the findings, have developed PR reduction strategies that are suitable for their own national conditions, such as staff training, trauma-informed care, etc., which can reduce the use of PR and minimize trauma.7,10,11
However, few studies have explored the experience of restraint in patients with mental disorder in Chinese culture, resulting in a lack of evidence to support the development of PR alternatives and best practices for nursing care that are tailored to the Chinese context, and a scarcity of strategies to reduce PR in mainland China. And Ye et al12 concluded that the incidence rate of PR in China has exceeded the global average frequency. Studies in mainland China have shown that the frequency of PR varies from 27.2% (371/1364)13 to 51.3% (86/160).14 The use of PR is influenced by differences in national contexts, cultures of care and treatment, ethnic preferences, and legislation.15–17 The perceptions and experiences of PR of patients with mental disorders in mainland China cannot simply be replicated in the context of other countries. Therefore, it is necessary to understand the subjective experience of mental disorders in restraint situations and perceptions of physical restraint in mainland China.
The main purposes of this study are (1) to better understand the perceptions and experiences of patients regarding PR events in mainland China and (2) to further identify the unmet care needs of patients with mental disorders during PR in mainland China. We hope that this exploratory research can provide information about the restraint experience of patients with mental disorders in a multicultural context, and also provide a new perspective for Chinese mental health workers to find alternative strategies for restraint.
Methods
Design
The purpose of this study was to explore the personal lived experiences of patients with mental disorders who have undergone PR in mainland China by utilizing a qualitative thematic analysis design. A semi-structured, one-to-one and face-to-face interview was conducted with mental disorders in mainland China.
Participants
This study was conducted from December 2021 to March 2022 at a specialized mental health hospital in Shanghai, China. Through purposive sampling strategy, participants were selected for inpatient psychiatric disorders who experienced PR and met inclusion criteria. Inclusion criteria were as follows: (i) having any disorder specified in the International Classification of Diseases and Related Health Problems, 10th Revision (ICD-10); (ii) being in the recovery phase (ie, basic remission of psychiatric symptoms and basic recovery of self-knowledge) as diagnosed by two psychiatrists; (iii) scoring ≥12 on the Insight and Treatment Attitudes Questionnaires (ITAQ)18 (having most self-knowledge or complete self-knowledge); (iv) being age 18–60 years, with normal intelligence, memory, comprehension and language expression; (v) signing the informed consent form and voluntarily participating in the study. Exclusion criteria were as follows: (i) mental disorder combined with serious organic diseases, substance abuse, and/or drug abuse; (ii) those with intellectual, audiovisual, and communication impairment; (iii) having severe dementia; or (iv) having changes in excitement, agitation, and miosis that prevent normal communication. Nurse practitioners and physicians were asked to identify eligible participants and to refer individuals with experience in PR to us. The number of participants enrolled was based on data saturation, which was achieved when no new topics could be found and the theoretical end point of saturation was reached. Finally, eight participants were recruited. After being asked if they would like to describe their experiences, all participants volunteered to participate in this study and signed informed consent. Confidentiality was maintained by using letters (ie, P1, P2, P3…) to identify participants (see Table 1).
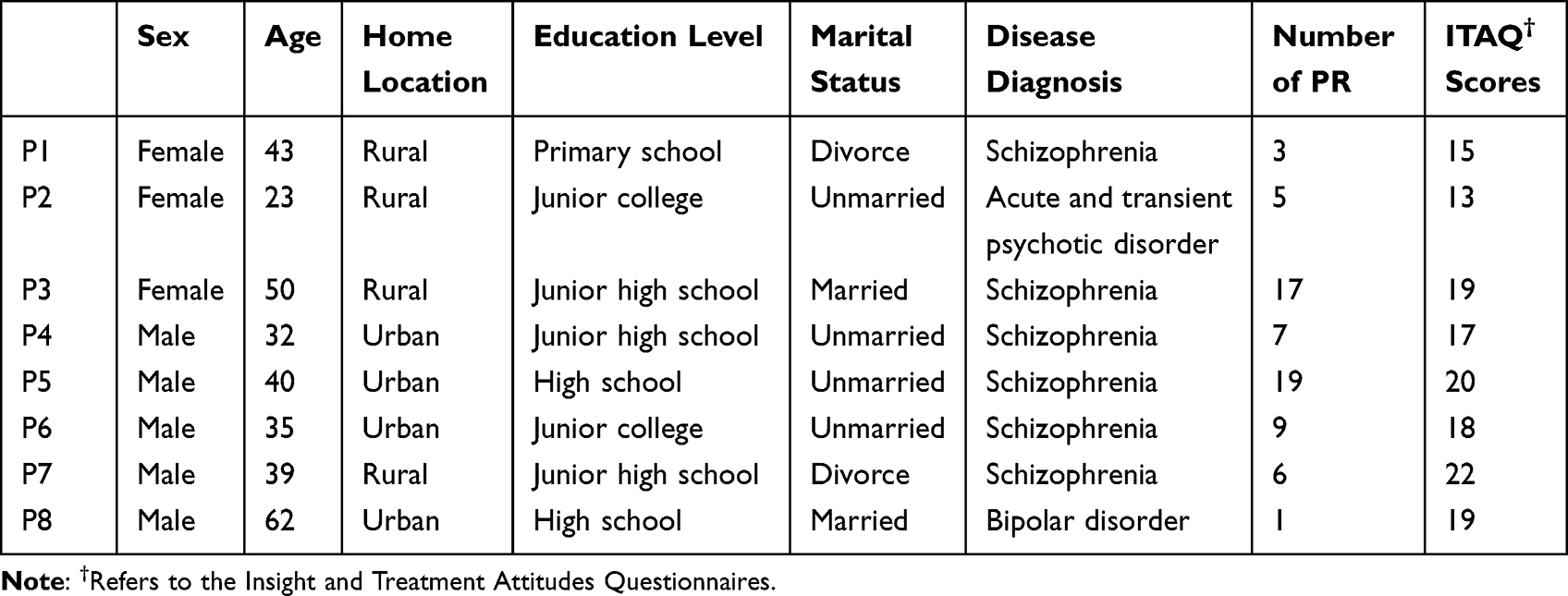 |
Table 1 Participant Information (n=8) |
Ethical Approval
The study protocol was carried out in compliance with the Helsinki Declaration. Before the interview, participants were informed of the purpose, procedures, and risks of the study. All participants signed an informed consent including publication of anonymized responses, there was no power or hierarchical relationship between this investigator and the patients, and both participation and withdrawal from the study were voluntary. Researchers are fully aware of the sensitivity of research related to physical restraint experiences, especially from the patient’s perspective. Participants were told that they did not have to answer any questions they did not want to answer and that they could stop the interview at any time or withdraw from the study at any time, but no one did so. If participants were distressed during the interview, patients in distress were directed to a nurse practitioner or clinician to lessen their anguish. We also provided contact information for the research team in the post-interview and study documents for guidance on: sensitive disclosure events (ie, risk of harm to self or others).
Data Collection
This study collected data through the use of one-on-one semistructured interviews in which participants were encouraged to share their experiences during PR, their perceptions of PR, and their expectations for future restraint use. The content of the patient interviews obtained in our study had a high degree of availability because the participants were questioned in a state of mind where they possessed most of their self-awareness or full self-awareness. Interviews lasted from 45–60 minutes, with an average of 53 minutes. All interviews were conducted by the primary author, anonymized, and transcribed verbatim. A semistructured interview schedule was used as a loose guideline during interviews:
- Can you tell us about the restraint you received during your hospitalization?
- For what reason were you restrained? What did you think when you were going to be restrained? How did you feel when the restraint was imposed?
- Before being restrained, did anyone tell you under what legal circumstances you would be subjected to such a measure? Would you have behaved differently if you had known this information?
- How has this experience affected you?
- If you were to return to that situation, what would have happened if PR had not been imposed on you at that time? What alternatives to PR do you think would have been more acceptable to you?
- Can you tell us how you feel and what you think about PR and seclusion?
- What do you think would happen if psychiatry did not have PR? What would happen to the ward environment if psychiatry reduced the use of PR?
- What care needs were not met during your stay, and if they had been met, would you still exhibit those behaviours?
Data Analysis
The transcribed interviews were analyzed using thematic analysis according to Braun and Clarke’s guidelines,19 which consisted of six steps. The first step was to familiarization by reading the transcripts repeatedly, thereby deepening understanding and insight into the information contained therein. At the same time, questions and ideas that emerged during the reading process were constantly recorded. The second step was to form an initial code, looking for word expressions related to the content of the physical restraint experience to form an initial code. The third step was to find themes and cluster analyze the initial codes to form theme clusters. The fourth step was checking the themes, verifying the consistency of the themes, codes, and the entire profile to form a thematic framework map. The fifth step was defining and naming each theme, consistently comparing and analyzing codes under and between different potential themes, and developing clear definitions and naming. Finally, the research report was written.
Several strategies were applied to guarantee trustworthiness and credibility. Authors 1 and 7 independently read and reread the transcripts to find themes, then coded and thematically organised the material. The findings were then compared and discussed by two authors until consensus on themes, theme clusters, and main themes was achieved. At the same time, an audit trail was maintained to ensure that all analytical steps could be traced back to the initial interviews. Finally, the results of the analysis were fed back to the participants to determine if the results were consistent with their true experiences.
Results
Analysis of the data revealed five main themes (each with sub-themes): perception and understanding of PR, response to PR, negative physical and psychological experiences, unmet care needs during PR, and changes after PR. The finalized thematic map is shown in Figure 1. All the sub-themes are discussed in turn in this section.
 |
Figure 1 The finalized thematic map. |
Perception and Understanding of PR
The first theme is about how patients view PR and their attitude towards PR. Some of them think that PR is discipline and punishment, and express strong antipathy to this measure. However, the others agree that this measure is necessary for the management of dangerous behaviors in psychiatric wards.
Discipline and Punishment
When talking about the past experience of being constrained, the two participants still showed strong emotional arousal. They thought that PR was a form of punishment and lead to their physical and psychological trauma. They complained that PR had become a “privilege” and “power” of the health care providers and was overused. They thought they did not need to be constrained under the current situation. When asked why they were restrained, P1 complained angrily:
In the name of PR, nurses are actually punishing and hurting patients in disguise. I went to fetch water yesterday, and a nurse wrongly accused me of splashing water downstairs. I said, ‘No, do not spoil a pot of porridge with a piece of mouse excrement.’ When I said something wrong and offended her, she restrained me! (P1)
Although P6 and P8 also consider PR as a punitive measure, they are neutral about PR and believe it is necessary. With the deterrence of such punitive measures, the participants’ bad behaviours are constantly being corrected, and thus, they are tamed into obedience according to hospital discipline and norms to maintain an orderly environment. P6 describes PR as “reminding” him and keeping him “well behaved”: “I used to knock on the door to be restrained, now I will not knock on the door”. P8 also affirms this role of PR but states that the use of PR should have clear preconditions.
PR is necessary. If nurses encounter patients who break the rules here and refuse to listen to repeated persuasion, they will implement restraint. However, like some patients who can communicate, nurses do not need to restrain them, and they can use other methods instead. (P8)
Safety Precautions
Five participants viewed PR as a management measure designed to maintain patient and staff safety by controlling aggressive and disruptive behaviour. They acknowledged that restraining patients in a timely manner minimized safety risks and maintain an orderly environment. Participants P2 and P7 described it this way:
If the patient smashes something or hits others, he must be restrained. If he is not restrained, he will hurt others and the hospital will become a mess. (P2)
PR has created an orderly ward environment, and I do not have to fear hurtful behaviour between patients. (P7)
When patients recalled the restraint by health care professionals, they revealed their understanding and recognition of the actions of the health care professionals, and they believed that the original purpose of PR by health care professionals was to protect and treat them. One of the patients with schizophrenia in this study, P1, strongly opposed to the use of PR initially, but when recalling the incident in which she was restrained as a result of a hunger strike, she revealed her approval of the use of PR by health care professionals. P1’s perceptions and attitudes toward PR differed in different scenarios.
Last time I was restrained because I didn’t eat. They restrained me to help me eat. They put a nasal tube in me and fed me. They were looking out for my survival and I can understand that. (P1)
Response to PR
Response to PR was the second theme that addressed how participants responds to the PR event. It demonstrated participants’ perceptions of how they behaved and reacted to PR. Participants reported a variety of coping method, with some engaging in overt resistance and others choosing passive compliance.
Overt Resistance
Three patients in this study talked about the lack of communication between nurses and patients, and expressed a deep sense of injustice that doctors and nurses restrained them were “make a big fuss over a minor issue”. P1 said angrily:
I don’t think this is fair! She asked me if I had poured water, and I said no, but she tied me up without giving me a chance to explain. There is really no place to cry out for injustice! (P1)
P2 expressed similar sentiments. She confesses that she does not have a mental illness, does not need to be dosed, and expresses her anger at being restrained for refusing to be dosed:
I was angry because they shouldn’t have given me medicine, and they added medicine to me. As soon as you come in, the doctor will treat you as a patient, and you have no right to communicate. I said I don’t take medicine, and then A lot of people came and tied me up, pried my mouth open, and poured medicine into my mouth. (P2)
Therefore, nurses should communicate the purpose and necessity of PR with patients before restraint so that patients can properly understand PR.
They also all believed that PR escalated their aggression so that the original trigger became irrelevant and was replaced by reactive behavior in response to a sense of injustice.
Choosing to refuse and adopt an attitude of resistance was the response to PR in the vast majority of participants, especially those who experienced PR for the first time. Participants expressed intense anger and resistance to PR and acted on them because of their current disease state or their negative perceptions of PR. They described these coping behaviors as: Struggling and resisting, yelling.
One participant described an escalation in his aggressive behavior when surrounded by staff, who “fighted” against PR.
A Nurse Came in and Said She Was Going to Restrain Me, and Then I Threw Water on the Nurse. (P5)
During restraint, participants also responded in this way to get the attention of healthcare workers. P4 reported feeling frustrated and sad when staff did not actively communicate with him, and his reactive reactions were exacerbated.
Two years ago, I experienced restraint for the first time. I was tied up for about half a month that time. During that period, no one paid attention to me, and I was yelling and struggling every day. (P4)
P3 and P7 described how they had developed techniques to break free from the restraint straps, using an ingenious “unstrap” method to “fight” the health care workers to resist PR.
They tied me up, right? Sometimes they tied me up, and the people who tied me up had skills, but I could get my hands free. (P3)
I Would Resist, and I Just Remember I Unbuckled the Restraint Straps Myself a Few Times. (P7)
Passive Compliance
When repeated resistance to PR failed, participants began to change their coping strategies. Six participants stated that they gradually gave up their struggle against PR after experiencing multiple unsuccessful attempts to resist PR, and they chose to passively comply and accept PR as part of their role. They concluded that there was no point in continuing to resist PR because they would eventually be restrained, and they were prone to injury in the process of resisting PR. Because they did not want to go through the painful restraint experience again in the past, they chose passive submission. P1 and P3 described their acceptance of PR as follows:
You will only bring more harm to yourself if you resist PR. So I did not try to struggle or to abuse the staff. I just took PR with my usual mind. (P1)
It is useless to resist, I did resist before, and the end result was restraint. Now I have accepted the restraint. When I resisted before, I couldn’t succeed and I would get myself hurt because the medical staff would tie me up tighter. (P3)
For patients who had been in the hospital for a long time and had been restrained numerous times, they knew what they were doing and what the consequences would be, but they still wanted to do it. They did it to attract the attention of the nursing staff and knew that the nurses would eventually release them. For example, P3 (who had been restrained 17 times) and P5 (who had been restrained 19 times) were the “slippery fellows” of the unit and indicated that they had mastered the timing of PR, while P3 said she would utilise technique to undo the restraint herself. In this way, they were caught in a cycle of “restrain-unrestrain-restrain again”, as if they were playing a game with the medical staff, over and over again.
Your release the following morning follows a set schedule, with the constraint lasting around one day. They tied me up, right? Sometimes they tied me up, and the people who tied me up had skills, but I could get my hands free. (P3)
I usually didn’t resist. If you didn’t resist, you would be released soon. (P5)
P2 and P3 found that a meek and submissive approach was more likely to lead to positive results than a forceful and aggressive approach and that “compliance” with the hospital’s rules would speed up the end of PR.
I cannot keep being so tough, and it is torture to keep resisting, so I started using softer methods. As long as I did not resist PR and behaved well, I could basically be released the next day. (P2)
When you obey and don’t resist, the nurse will release you. (P3)
Negative Physical and Psychological Experiences
This theme presents the physical repression and psychological suffering that patients with mental disorders endure during PR.
Suffering from Somatic Discomfort
PR in China mainly consists of strapping the patient’s wrists and ankles to the bed with a belt or leather restraint. According to P1 and P4, under the control of restraint straps, they were “shackled” and “handcuffed” like prisoners, firmly bound to the bed, with no escape but to “face the wall” forever.
I felt like a prisoner in a cell. (P1)
I was tied to the bed like a hairy crab. I could not move my hands, and all I could do was look at the ceiling from the bed during that time. (P4)
From the participant’s perspective, PR puts the participant’s body in a state of coercion, deprivation, and restriction. In this state, participants are temporarily deprived of the right to make decisions about their own bodies, and they are unable to decide what their bodies experience. P4 describes the situation at that time:
I did not need to be restrained in that situation at the time, but medical staff insisted on binding me. (P4)
As a result of restraint, some participants’ physical abilities in the lifeworld were also disabled. Five participants described the experience of losing their ability to be free and control their actions due to PR. Take the description of P1 and P4 as examples:
If I wanted to drink water in normal times, I could pour it myself. If I wanted to pee, I could go to the toilet myself. However, after I was restrained in bed, I could not even pour water for myself and drink. I had to wait for my caregiver to come and ask me if I wanted to drink water. (P1)
I was tied to the bed and could not move. So, I couldn’t go to the toilet. I remember, once I peed on the bed. (P4)
Due to restricted movement during PR, the participants can only move in a small area, which changes their activity pattern. The inappropriate tightness of the restraint area and insufficient length of the restraint belt forces participants to maintain the same posture for long periods of time. They are unable to complete independent activities, often experiencing discomfort such as limb soreness, numbness, and pain. See these passages from Participants P2 and P7:
The nurses tied me so tightly that I was in pain. I was strangled here (pointing to her neck). It was particularly uncomfortable, and my neck hurt. (P2)
It is truly hard to be restrained. You can only lie in one position, cannot move, and your arms will be numb if you sleep for a while. (P7)
P4 described that he tried to break free from the restraint; however, instead of regaining freedom, this behaviour increased his physical discomfort.
I kept trying to free myself. But the more you struggle, the tighter the nurses tie you, and the more painful the tied parts become. (P4)
Five participants reported varying degrees of skin damage during restraint due to tight restraints and prolonged restraints. P2 alluded to the PR as being a torture chamber creating skin pain, as excerpted below.
I felt like I was in a torture chamber. The restraints kept torturing my body, which was bound and wounded. (P2)
The restraint straps left scars on the patients’ bodies, which faded with the passage of time.
Look, I Was Restrained Six Months Ago, and I Still Have the Marks on My Arm from the Restraint. (P5)
Participants P5, P7, and P8 had varying degrees of sleep deprivation during PR.
I could not sleep at night during the period of restraint. And, I thought nonsense, thinking about why my wife and children had put me in this hospital. (P8)
Experiencing Psychological Distress
Four participants expressed feelings of aggression and anger due to the imposition of restraint and the injustice of being restrained. P2 and P7 described feeling annoyed at being tied down:
I’ve been tied up four or five times. I’ve never been so angry, and it is the first time I’ve been so angry. (P2)
I was in an irrational state and did not want to be restrained, and I was definitely annoyed with the performance. (P7)
At present, Chinese psychiatric wards generally adopt an unaccompanied system, and restrained patients are generally placed alone in a primary care ward. Although nurses monitor patients in wards 24 hours a day, they are unable to do so for physically restrained patients due to the relatively large number of patients in the wards that require their attention. Feelings of loneliness and abandonment were pervasive for some participants. They claimed they were alone, abandoned in their rooms with little contact, as shown in the following excerpt:
Nurses restrained me and left me inside the small level one ward with the door closed and locked and just left me alone. I felt left out. (P1)
P6 reported that no staff talked to him during the time he was restrained, which left him with feelings of ambiguity and uncertainty, which added to his insecurity and fear. Similar sentiments were expressed by P7:
I was once restrained with a sense of fear inside. I was restrained for a long time, but none of the nurses came to tell me when I could be released from the restraint. I was a little scared. (P7)
During PR, participants are prone to suffer from psychological trauma that is difficult to resolve and leaves them in deep despair. As P1 said,
PR has been bogged down in my mind, and it is like a knot in my heart that I cannot untie. (P1)
When recalling the experience of PR, some of the interviewees viewed the use of physical force and coercion by the nursing staff during the restraint incident as an undeniable violation of the patient’s human rights. One of the participants recalled degrading behaviour from the nurse that caused her shame and humiliation.
One of the nurses wanted to give me medicine during the restraint, and I said, ‘You untie me, so I can take the medicine myself’, but she said no. She used a scoop to pry my mouth open. Do you think this is what people do? The greatest shame I’ve ever suffered in my life was this one. (P2)
Due to physical limitations during PR, two participants described being deprived of basic hygiene facilities, such as access to the toilet, which failed to protect their dignity while causing embarrassment and self-esteem to suffer. An excerpt from one participant is as follows:
You also need to pee after being restrained, but you can only solve it in bed. You cann’t even go to the toilet. It is so embarrassing. I feel like my dignity disappeared (P3)
Unmet Care Needs During PR
This theme captures the patient’s evaluation of the care provided by the nursing staff during PR and what help and support they expect.
Most study participants felt that they did not receive adequate physical and psychological support when they were restrained. Psychological support includes information and explanation, attention and a sense of security, while physical support includes the need for help with eating, drinking, toileting, and personal hygiene.
Desire for Psychological Comfort
After being restrained, three participants had doubts about why they were being restrained, their current situation, and when the restraint would end. However, health care providers did not communicate with patients in a timely manner and did not do a good job of comforting and explaining the process. Thus, the patients’ inner doubts were not dispelled, their thoughts and feelings went unshared, and their needs were not met. P7 described being in a panic because information about the duration of the constraint was not available in time.
I was once restrained with a sense of fear inside. I was restrained for a long time, but none of the nurses came to tell me what could be released from the restraint. I was a little scared. (P7)
It was clear that providing a thorough explanation is one of the main nursing objectives of the medical staff while the patient is being restrained, along with providing timely information about the reason for and length of the restraint after the patient has been restrained in order to allay any internal uncertainty and insecurity.
While patients were restrained, they felt they received less attention from caregivers and they felt neglected, which made them feel uneasy. Patients are also very vulnerable psychologically during PR, and most expressed a desire to be with others for psychological support and comfort, especially health care workers. They desired to maintain interactive communication with health care staff during PR and be asked more questions about their needs. As demands are expressed by P1:
I hope patients who are restrained are not left out in the cold. Nurses should care more about us, not leave us alone after restraining us. (P1)
Access to Physical Support
Two participants reported that nursing staff failed to meet their basic physical needs in a timely manner during PR. P1 complained that water and elimination needs were not addressed in a timely manner during PR, and P5 reported a lack of consideration by nursing staff for patients’ needs for warmth in winter.
I was tied up yesterday. I didn’t drink much water. No one asked me if I drank water. They restrained me and left me inside and left me alone. And, I only urinated once between 10 o’clock last night and this morning, and it was my caregiver aunt who went to ask for me. (P1)
Put a quilt on us in winter. Heat the water and then feed it to us; otherwise, we will catch cold easily. (P5)
Two study participants expressed their requests for life care, hoping that nursing staff would ensure food and water intake during PR, address excretion problems in a timely manner, and provide good personal hygiene for them.
Sometimes I want to drink water. The nurses can get me some water for me to drink. (P3)
I hope the nurses can deliver food on time, so that I can eat and take medicine. (P4)
They expressed gratitude when when staff did meet their basic physical needs. P5 recounted his experience when he was in restraint. A caregiver took care of him without failure, assisting him in going to the toilet in the middle of the night without a trace of impatience, and the patient gave the caregiver a book to express his gratitude.
There was a short master nurse named Zhao who was quite good to me. That nurse took care of me for 4 days and 4 nights. Once in the middle of the night, I wanted to urinate. He also helped me urinate. He was truly good to me, and later as a reward I sent a book to him. (P5)
Although some of the gestures of the health care workers may seem insignificant, for P5, who was restrained in a state of mental vulnerability, a thoughtful gesture was a cure. The satisfaction of some small needs made him feel respected and cared for, alleviating to some extent of the negative emotions caused by PR.
Changes After PR
The last theme emerging from the patient interviews involved two aspects. One was their views on the doctor-nurse-patient relationship reflected behind PR, which included the self-positioning of the doctor-nurse-patient relationship in the eyes of the patients, and the impact of PR on the patient’s perceptions and attitudes toward the health care staff who restrained them. The second was the changes in their own behavior after restraint.
Repositioning the Doctor–Patient Relationship
Due to mental illness, especially in patients with psychiatric disorders without self-awareness, the diagnosis and treatment of patients often rely on health care professionals. In this relationship, the health care provider is in an extremely active and dominant position, while the patient is in a passive and receptive situation. Patients are similar to children who cannot be independent in a parent-child relationship, and medical staff are parents who take care of everything for their “children”.
Two patients accepted this paternalistic approach, while two patients wished to participate in shared restraint decision-making. P6 described being deprived of other options in PR decision-making, he had no choice, but this did not disturb him, and he stated that he was happy to defer to the professional decision-making of the medical staff.
It was a bit uncomfortable to be restrained for the first time. Later, when I thought about it, I should follow their instructions. In the hospital, I should listen to the doctors and nurses. (P6)
P1 represented a different case, for P1, this paternalistic model excluded her personal choices, she emphasized the importance of two-way dialogue in making PR decisions, and she felt that she was deprived of other options and co-participation.
I said you are unreasonable, but she said this is the rule. I walked to the door of this room from the nurse’s station, and she rushed out from the nurse’s station, and she said: What are you talking about? I said, ‘I didn’t say anything, can I go back and take the medicine now?’ She said: No! You go back to me. (P1)
The relationship between healthcare professionals and patients is a central aspect of mental health care, and four patients felt that PR jeopardized this, particularly the factor of trust.
PR made the patient lose confidence and trust in the nursing staff. For example, after experiencing the restraint incident, P2 harbored resentment and confessed that he was reluctant to approach the nursing staff. This deepened the gap between nurses and patients, which is not conducive to harmonious nurse-patient relationship development. To a certain extent, PR undermines the good therapeutic relationship that has been established between nurses and patients.
The trust was totally broken and I didn’t like to communicate with the nurses and care workers since then. (P2)
Improve Self-Management Skills
Six of the patients in this study reported positive changes regarding PR. Three participants described how PR had helped them to learn to curb their temper, manage and control their emotions, and become more mature. An excerpt from one of them is as follows:
Although I may be stubborn, since being restrained I try to restrain my temper. (P3)
Some participants reflected and summarized the reasons why they were restrained during PR. P2 conducted self-reflection during PR, rationalized his perceptions of his behaviours and recognized his mistakes in time. P3, P6, and P7 reflected on their previous bad behaviours and gradually improved their self-management skills.
Self-restraint of one’s own behaviour is somewhat improved because PR is a bit of a deterrent. (P7)
Discussion
The present study sought to provide a rich and detailed description of patient experiences of PR among patients with mental disorders using a qualitative descriptive approach. We aimed to gain a deeper understanding of the perceptions and physical and psychological experiences of psychiatric patients who have experienced PR to improve the implementation of PR and care of restrained patients. To our knowledge, this is the first qualitative study to explore physical restraint experience of patients with mental health in mainland China.
The participants in our study suffered varying degrees of physical and psychological distress, and they felt that PR had undermined their autonomy and dignity, which made them very angry. Some participants perceived PR as a punitive measure, a means of exerting control and power when they broke the health care provider’s rules, expressing their inner sense of injustice. Although the Mental Health Law of the People’s Republic of China has clearly defined the scope of application of PR, the descriptions of the indications listed in the Law, such as “disruptive behavior of the medical order”, are still vague and difficult to define, which may affect the implementation of PR by medical staff and put them in an ethical dilemma. If medical staff decide to impose PR on patients with mental disorders, it must be implemented after other alternative, non-restrictive methods have failed and in a way that maximizes the protection of their fundamental rights. Nurses should also communicate the purpose and necessity of PR with patients before restraint so that patients can properly understand PR. Furthermore, restraint review is necessary. Active listening, venting, reassurance, reviewing how events unfolded, discussing how staff and patients felt, and exploring ways in which patients and staff might respond to future escalating aggression situations are all restraint reviews important content.
Interestingly, the participants’ behaviours in response to PR were not uniform. Initially, the majority of participants responded to PR with “overt protest reactions”, in which they cried and struggled to resist PR, which may be related to the patient’s disease state or negative effects of the restraint. Our study also found that during PR, patients also respond in this way to get the nurse’s attention, which is consistent with the findings of Holmes et al.20 As the number of restraint episodes increases, participants gradually become passively compliant with the PR for three possible reasons. First, their condition improves, and self-knowledge returns after a period of medication; second, previous experience told them that resistance cannot lead to unrestrained results, and they also did not want to go through the painful restraint experience of the past again; and third, they gave up resistance to be released from PR sooner. The degree of patient cooperation is often used as an indicator for nurses to release from PR. However, their acceptance is not active, it is passive obedience, Holmes et al20 also said that it is still a subtle form of resistance.
Participants in this study reported unmet care needs during PR, such as neglect, lack of care and compassion by healthcare professionals, which is similar to findings in a number of related studies.8,10 In many cases, the main cause of patient dissatisfaction with PR is the lack of contact with the nurse and the feeling of abandonment.21 The lack of psychiatric nurses and lack of time make it difficult for staff to provide more time with restrained patients, which is the underlying cause of these feelings. Offering staff the necessary time and support through debriefing and training can help with understanding the patients’ needs. De-escalating situations before using restraint and, if RP is needed, how to support the individuals in distress are also issues that deserve attention. During PR, nurses should also focus on the subjective experience of the restrained patient, providing humane care by focusing on the living body, understanding the nature of human rights, interacting positively with the patient, and listening carefully to the patient’s needs.22,23 After PR, health care professionals should provide timely trauma-informed care to reduce the traumatic effects of restraint and to rebuild therapeutic alliance and trust.
Although many studies have been conducted to reduce the use of PR in psychiatric wards, restraint measures continue to occur.24 Participants in our study expected that PR was not the preferred measure and that the use of PR would be minimized and reduced. Participants made a number of recommendations based on their own PR experiences to help mental health personnel reduce PR.
The recommendations are summarized as follows: 1. Conducting de-escalation interventions, including temporarily meeting patients’ needs and establishing verbal contact with patients; 2. Educating and training of staff and patients; 3. Improving the environment of the ward by achieving a reasonable allocation of patients to medical resources, making the ward spacious and quiet; providing various forms of work and recreational activities and playing soothing music according to patients’ conditions; and 4. Prescribing individualized medication to control patients’ symptoms and restore stability. These suggestions have been proposed and addressed in many studies in the West.11,24,25 Bowers et al24 implemented ten “Safewards” interventions in psychiatric wards, which reduced the incidence of conflict incidents in patients with mental disorders by 15% and the rate of restraint use by 26.4%, showing promising success in reducing restraints. Chinese psychiatric medical staff can combine practical resources to carry out operable and easy-to-accept safety interventions to reduce the use of PR.
Meanwhile, this study adds two new recommendations, enabling a good family support system and advancing community mental health services, which are important to complement the existing evidence base. Due to China’s long-term cultural and national conditions, many patients with mental disorders are “abandoned” by their families in the hospital. Patients crave a closer bond with their family for support, but the family members do not come to visit for a long time. The blunt indifference to the patients will lead to the depression of the patients. To a certain extent, the patient may erupt and, in severe cases, violent aggressive behaviors may occur. A strong family support system can play an important role in facilitating the relief of patients’ agitation symptoms and help promote the effectiveness and outcome of treatment, while violent aggression is often the main cause of patients being restrained. In a Chinese mental health center, Feng et al26 used systematic family therapy in the treatment and rehabilitation process of patients with mental disorders, but its effectiveness has not been proven.
Overall, the construction and development of mental health services in China is not as mature as in Western countries due to many factors. At present, specialized mental health hospitals in mainland China have a high density of patients and medical pressure in their wards, with many patients who have met the discharge criteria but cannot be discharged, and some patients are repeatedly admitted to the hospitals, which brings a heavy burden to the hospitals and a great pressure on the originally insufficient resources for mental health services. In these mental health care facilities, noisy and crowded wards and unsafe environments can increase agitated behaviours, leading to increased PR use. The shortage of psychiatric nurses and the heavy burden of care leave nurses with limited resources and time to cope with aggressive patient behaviour, making them more inclined to use PR. If these patients can return to the community, there will be more space resources available in the hospital, and at the same time, the nurse-patient ratio will be balanced, so that health care workers can spend more time and energy on the psychological care of patients. Therefore, hospitals and communities need cooperation to provide empowerment for patients with mental disorders and to train patients with mental disorders to return to the community, achieving the goal of comprehensive, community-based services.
Limitations
This study has several limitations. First, the majority of the participants in this study were patients with schizophrenia, and the sample size should be expanded in the future to enrich the types of psychiatric disorders studied. Second, some participants had been away from PR events for a long time. The interview content was inevitably subject to memory bias, and their perceptions of PR were subject to change due to other experiences (eg, psychotherapy). The third limitation is the issues of generalizability of research findings. Differences in national circumstances, cultures of care and treatment, ethnic preferences, and legislation can make use of the PR variable from country to country.15–17 This study was conducted within one specialized mental health hospital in Shanghai, China. In the future, the study can be conducted jointly with multi-regional and multi-center and investigate how similar or different these perceptions might be in different areas or institutions in mainland China.
Conclusions
Patients with mental disorders in mainland China have negative physical and psychological experiences of PR, which are almost inevitably associated with negative, harmful or even traumatic experiences. Healthcare professionals must acknowledge and address this situation. Participants have different perceptions of and reactions to PR, all of which remain resistant in nature. Patients’ physical and psychological needs are not adequately met during PR. Offering staff the necessary time and support through debriefing and training can help with understanding the patients’ needs. De-escalating situations before using restraint and, if RP is needed, support the individuals in distress as well as reduce post restraint trauma. It is imperative to explore other less restrictive alternatives to PR. In Western nations, interventions for reducing PR have been researched and successfully used in clinical settings, such as ten “Safewards” interventions. Chinese mental health professionals can draw on the evidence-based resources available in the West and explore intervention strategies for restraint reduction in psychiatry that are appropriate for China based on the Chinese medical context, culture, and practice experience.
Data Sharing Statement
The data are not available due to privacy or ethical restrictions.
Ethical Approval
The study protocol was approved by the Ethics Committee of Pudong New Area Mental Health Center (PDJWLL2022006) and Science and Technology Ethics Committee of Tongji University (2021tjdx065). It was carried out in compliance with the Helsinki Declaration. After being fully informed about the purpose, procedures, and risks of the study, all participants signed an informed consent. And codes rather than personally identifiable information were used in the study.
Acknowledgments
We thank all of the persons who participated in this study and Shanghai Pudong New Area Mental Health Center.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was funded by the General Project of Shanghai Teaching and Scientific Research (C2021333) and the Outstanding Clinical Discipline Project of Shanghai Pudong (Grant No. PWYgy2021-02).
Disclosure
All authors declare no conflicts of interest in this work.
References
1. Mental Health Professional Committee of Chinese Nursing A. Expert consensus on the implementation and removal of protective restraints in psychiatry. Chin J Nurs. 2022;57(2):146–151.
2. Beghi M, Peroni F, Gabola P, Rossetti A, Cornaggia CM. Prevalence and risk factors for the use of restraint in psychiatry: a systematic review. Rivista Di Psichiatria. 2013;48(1):10–22. doi:10.1708/1228.13611
3. Allen DE, Fetzer S, Siefken C, Nadler-Moodie M, Goodman K. Decreasing physical restraint in acute inpatient psychiatric hospitals: a systematic review. J Am Psychiatric Nurses Assoc. 2019;25(5):405–409. doi:10.1177/1078390318817130
4. Hirose N, Morita K, Nakamura M, Fushimi K, Yasunaga H. Association between the duration of physical restraint and pulmonary embolism in psychiatric patients: a nested case-control study using a Japanese nationwide database. Arch Psychiatric Nurs. 2021;35(5):534–540. doi:10.1016/j.apnu.2021.07.009
5. Bellenger EN, Ibrahim JE, Lovell JJ, Bugeja L. The nature and extent of physical restraint-related deaths in nursing homes: a systematic review. J Aging Health. 2018;30(7):1042–1061. doi:10.1177/0898264317704541
6. Steinberg A. Response to: response to: prone restraint cardiac arrest: a comprehensive review of the scientific literature and an explanation of the physiology. Med Sci Law. 2022;62(1):79–80. doi:10.1177/00258024211025226
7. Hawsawi T, Power T, Zugai J, Jackson D. Nurses’ and consumers’ shared experiences of seclusion and restraint: a qualitative literature review. Int J Ment Health Nurs. 2020;29(5):831–845. doi:10.1111/inm.12716
8. Gleerup CS, Ostergaard SD, Hjuler RS. Seclusion versus mechanical restraint in psychiatry - A systematic review. Acta Neuropsychiatr. 2019;31(5):237–245. doi:10.1017/neu.2019.22
9. Tingleff EB, Hounsgaard L, Bradley SK, Gildberg FA. Forensic psychiatric patients’ perceptions of situations associated with mechanical restraint: a qualitative interview study. Int J Ment Health Nurs. 2019;28(2):468–479. doi:10.1111/inm.12549
10. Hansen A, Hazelton M, Rosina R, Inder K. What do we know about the experience of seclusion in a forensic setting? An integrative literature review. Int J Ment Health Nurs. 2022;31(5):1109–1124. doi:10.1111/inm.13002
11. Wilson C, Rouse L, Rae S, Ray MK. Mental health inpatients’ and staff members’ suggestions for reducing physical restraint: a qualitative study. J Psychiatric Ment Health Nurs. 2018;25(3):188–200. doi:10.1111/jpm.12453
12. Ye JR, Xiao AX, Yu L, et al. Staff training reduces the use of physical restraint in mental health service, evidence-based reflection for China. Arch Psychiatric Nurs. 2018;32(3):488–494. doi:10.1016/j.apnu.2017.11.028
13. An FR, Sha S, Zhang QE, et al. Physical restraint for psychiatric patients and its associations with clinical characteristics and the National Mental Health Law in China. Psychiatry Res. 2016;241:154–158. doi:10.1016/j.psychres.2016.04.101
14. Zhu XM, Xiang YT, Zhou JS, et al. Frequency of physical restraint and its associations with demographic and clinical characteristics in a Chinese Psychiatric Institution. Perspect Psychiatric Care. 2014;50(4):251–256. doi:10.1111/ppc.12049
15. Bak J, Aggernaes H. Coercion within Danish psychiatry compared with 10 other European countries. Nordic J Psychiatry. 2012;66(5):297–302. doi:10.3109/08039488.2011.632645
16. McLaughlin P, Giacco D, Priebe S, McKenna PJ. Use of coercive measures during involuntary psychiatric admission and treatment outcomes: data from a prospective study across 10 European countries. PLoS One. 2016;11(12):e0168720. doi:10.1371/journal.pone.0168720
17. Georgieva I, Mulder CL, Wierdsma A. Patients’ preference and experiences of forced medication and seclusion. Psychiatr Q. 2012;83(1):1–13. doi:10.1007/s11126-011-9178-y
18. McEvoy JP, Hartman M, Gottlieb D, Godwin S, Apperson LJ, Wilson W. Common sense, insight, and neuropsychological test performance in schizophrenia patients. Schizophrenia Bull. 1996;22(4):635–641. doi:10.1093/schbul/22.4.635
19. Braun V, Clarke VJQRi P. Using thematic analysis in psychology. Qual Res Psychol. 2008;3(2):77–101. doi:10.1191/1478088706qp063oa
20. Holmes D, Kennedy SL, Perron A. The mentally ill and social exclusion: a critical examination of the use of seclusion from the patient’s perspective. Issues Ment Health Nurs. 2004;25(6):559–578. doi:10.1080/01612840490472101
21. Meehan T, Vermeer C, Windsor C. Patients’ perceptions of seclusion: a qualitative investigation. J Adv Nurs. 2000;31(2):370–377. doi:10.1046/j.1365-2648.2000.01289.x
22. Kottow M. Some thoughts on phenomenology and medicine. Med Health Care Philos. 2017;20(3):405–412. doi:10.1007/s11019-017-9763-4
23. Kong B. Merleau-Ponty’s phenomenology of body and the experience of illness in nursing. Philos Phenomenol Res. 2009;40:57–81.
24. Bowers L, James K, Quirk A, et al. Reducing conflict and containment rates on acute psychiatric wards: the Safewards cluster randomised controlled trial. Int J Nurs Stud. 2015;52(9):1412–1422. doi:10.1016/j.ijnurstu.2015.05.001
25. Goulet MH, Larue C, Dumais A. Evaluation of seclusion and restraint reduction programs in mental health: a systematic review. Aggress Violent Behav. 2017;34:139–146. doi:10.1016/j.avb.2017.01.019
26. Feng VY, Qin H, Chen Y-H, et al. Application of SYMPA project in the whole process of rehabilitation of mental disorder (in Pudong of Shanghai, China). Notch Forum Social Psychiatry. 2023;1(1):4–8.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.