Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
The Subjective Will and Psychological Experience of Home-Based Exercise in Lung Cancer Patients During Interval of Chemotherapy: A Qualitative Study
Authors Hu Y ![]() , Chen X
, Chen X ![]() , Fan J
, Fan J ![]() , Huang Y, Ye J, Gu F
, Huang Y, Ye J, Gu F ![]() , Li Y
, Li Y
Received 30 December 2022
Accepted for publication 23 February 2023
Published 9 March 2023 Volume 2023:16 Pages 663—674
DOI https://doi.org/10.2147/JMDH.S403185
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Yachen Hu,1– 3,* Xinxin Chen,1,2,* Jiaxin Fan,1 Ying Huang,4 Junyan Ye,4 Fen Gu,5 Yumei Li1,2,*
1School of Medicine, Tongji University, Shanghai, People’s Republic of China; 2Department of Nursing, Shanghai Pulmonary Hospital, Tongji University, Shanghai, People’s Republic of China; 3Department of Respiratory Medicine, Shanghai Children’s Hospital, School of Medicine, Shanghai Jiao Tong University, Shanghai, People’s Republic of China; 4Department of Oncology Medicine, Shanghai Pulmonary Hospital, Tongji University, Shanghai, People’s Republic of China; 5Department of Nursing, Shanghai Ninth People’s Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yumei Li, Department of Nursing, Shanghai Pulmonary Hospital, Tongji University, Shanghai, 200433, People’s Republic of China, Email [email protected]
Purpose: This qualitative study explores the subjective will and psychological experience of home exercise in patients with lung cancer during the interval of chemotherapy.
Methods: Semi-structured interviews were conducted with 15 lung cancer patients undergoing chemotherapy. Following the Colaizzi 7-step analysis method, the interview data were read carefully, meaningful statements related to the research questions were extracted, coded, collected and described in detail, and the authenticity of the theme was verified.
Results: The analysis revealed the home-based exercise experience of patients’ in the interval period of chemotherapy, and identified three themes: 1) the perception experience of home-based exercise (beneficial home-based exercise experience, negative home-based exercise experience); 2) the influencing factors of home-based exercise (exercise rehabilitation knowledge, disease symptoms and adverse effects of chemotherapy, exercise history, exercise self-efficacy, social support, restrictions on objective conditions); 3) Patients with lung cancer expected to get professional guidance about home-based exercise rehabilitation knowledge from medical care providers.
Conclusion: Patients’ perception and attitude towards home-based exercise behavior is affected by many factors during the interval of chemotherapy, and they expect professional guidance from medical care providers. Medical care providers should know the problems and the influencing factors in the process of home-based exercise of patients, and formulate personalized exercise measures for patients based on their own characteristics and needs, so as to relieve the symptoms of discomfort and improve the quality of life of patients with lung cancer.
Keywords: lung cancer, chemotherapy, home-based exercise, psychological experience, qualitative research
Introduction
Lung cancer is one of the most common malignant tumors and the leading cause of cancer-related death. According to the global cancer statistics in 2020, lung cancer has the second highest incidence rate after breast cancer, and its mortality rate ranks the first in cancer deaths.1 The number of lung cancer cases and deaths in China accounts for 37% and 39.8% of the global total respectively, which is one of the countries with the highest incidence of lung cancer.2
Chemotherapy is one of the commonly used treatment methods for patients with lung cancer, often acting alone or in combination with other treatment methods. Some patients with lung cancer after surgery will also use chemotherapy to prolong their survival cycle. Lung cancer chemotherapy patients including postoperative chemotherapy will experience pain, cough, sleep disorders, shortness of breath, fatigue, loss of appetite, depression and anxiety and other complex and numerous discomfort symptoms.3,4 It seriously interferes with the daily activity function of lung cancer patients, including walking,5,6 reducing the quality of life. In addition, periodic hospitalization chemotherapy can also disrupt the daily life of patients with lung cancer.
The Clinical Oncology Society of Australia position statement that exercise should be a part of standard practice in cancer care and is viewed as an adjunct therapy that helps counteract the adverse effects of cancer and its treatment.7 Exercise has significant potential in reducing cancer associated symptoms and cancer treatment-related injuries,8 which can significantly alleviate cancer-related fatigue, depression, anxiety, sleep disorders and other adverse symptoms of patients with lung cancer, enhance physical fitness and improve the quality of life.9,10 Moderate- and high-intensity exercise intervention can be implemented for lung cancer patients.11 However, Avancini et al12 conducted a questionnaire survey on 329 patients in Italy, including patients with lung cancer, and found that 93% of cancer patients had insufficient exercise, and those patients given chemotherapy had even lower exercise.
At present, scholars have conducted a large number of quantitative studies on the effect of exercise intervention for patients with lung cancer13,14 or conducted interviews on the experience of patients after exercise intervention.15 However, there is a lack of qualitative research on the autonomous home-based exercise experience of patients with lung cancer undergoing chemotherapy. We want to explore the subjective willingness and psychological experience of home-based exercise of patients with lung cancer during chemotherapy interposition, and understand the perceived experience of home-based exercise of patients with lung cancer undergoing chemotherapy and various factors affecting home-based exercise and their inner needs.
Methods
Design
This is a qualitative study. Data were collected by interviewing lung cancer patients who were readmitted to the hospital for chemotherapy. Phenomenological research is a kind of qualitative research. In the field of nursing, it is mainly used to explore the subjective cognition or life experience related to health and disease, such as values and world outlook.16 Descriptive phenomenology can be used to describe individual expressed, superficial and obvious experiences through content analysis,17 which has been used in the research of patients with lung cancer chemotherapy18 and exercise rehabilitation behavior.19 In this study, descriptive phenomenology was used to describe the subjective will and psychological experience of patients with lung cancer chemotherapy to home-based exercise, in order to explore their substantive needs and provide guidance for the development of individualized intervention programs of home-based exercise.
Participants
Purposive sampling was used to select the research objects from patients with lung cancer who were repeatedly hospitalized for chemotherapy from October 2022 to November 2022. According to the characteristics of patients such as age, gender, number of chemotherapy, course of disease, and exercise hobby, the inclusion and exclusion criteria of the research objects were formulated by using the maximum difference of sampling strategy as the selection principle. Inclusion criteria: (1) patients with stage II, III or IV lung cancer diagnosed by pathology and requiring repeat chemotherapy; (2) age ≥18 years old; (3) knowing their condition; (4) Good language skills; (5) KPS score ≥80; (6) having a history of exercise for at least one month; (7) Informed consent and voluntary participation in this study. Exclusion criteria were patients with lung cancer with cognitive impairment or brain or bone metastases.
Data Collection
The descriptive phenomenological method of qualitative research was used, and a semi-structured face-to-face interview outline was preliminarily formulated based on literature review and consultation with clinicians according to the purpose of the research. Three patients were interviewed prior to the main study to come up with the revised interview outline: (1) What physical exercise activities do you do at the end of each treatment? How to schedule the frequency? (2) What motivates you to exercise? What are the reasons for giving up continuing exercise? (3) How do you feel after exercise? (4) What do you think of the significance of exercise during the chemotherapy interval? (5) What is your family’s attitude towards exercises? What needs do you have or what kind of help do you want? The interview was conducted with the consent of the doctor and the head nurse. The whole interview process was recorded and centered on the outline of the interview. The order of questions was adjusted appropriately according to the actual situation of the interview, and repeated, cross-examined and summarized when necessary. Each interview lasted 30 to 45 minutes.
Data Analysis
The interview recordings were transcribed into text within 24 hours after the end of the interview, without any alteration or deletion of the recorded content, so as to ensure the authenticity of the data, and imported into QSR Nvivo 8.0 software for sorting and analysis. Colaizzi 7-step analysis method16 in phenomenology was used to analyze the data. The researchers Hu and Chen respectively through careful and repeated reading of the recording text to obtain the overall familiarity of lung cancer patients’ home-based exercise during intermittent chemotherapy, and then through word-by-sentence analysis, identify and extract the important and meaningful statements related to the subjective intention and psychological experience of lung cancer chemotherapy patients at home exercise, and the repeated views were coded. Subsequently, the members of the research team jointly analyzed and discussed, formed the initial topic by coding clustering, made repeated comparisons to identify and classify similar views, constructed the final topic, and verified the accuracy of the results to the interviewees. The detailed analysis steps are shown in Figure 1 below.
 |
Figure 1 Colaizzi 7-step analysis procedure. |
Ethical Considerations
This study complied with the requirements of the Declaration of Helsinki. The study was approved by the Ethics Committee of Shanghai Pulmonary Hospital Affiliated to Tongji University. The approval number was Q22-355Y. The interview time was determined to accord to the time of the patient’s hospitalization examination and treatment, and the criterion was not to interfere with the patient’s clinical treatment. Before the formal interview, the researchers introduced themselves, informed the purpose, content and process of the interview, and ensured that the interviewees would be anonymous. Finally, the informed consent was signed. The interview place was the ward talk room in a quiet environment. The whole interview process was completed in a natural state, and the participation of family members was not avoided, ensuring that the patients could accept communication and interview with a pleasant and open mind.
Results
In this interview, it was found that when the number of interviewees reached 13, no new themes were presented, and no new information appeared after continuing to interview 2 cases. It was considered that the interview data was saturated and the interview was stopped. Finally, 15 participants were selected. The basic information of the interviewees is shown in Table 1.
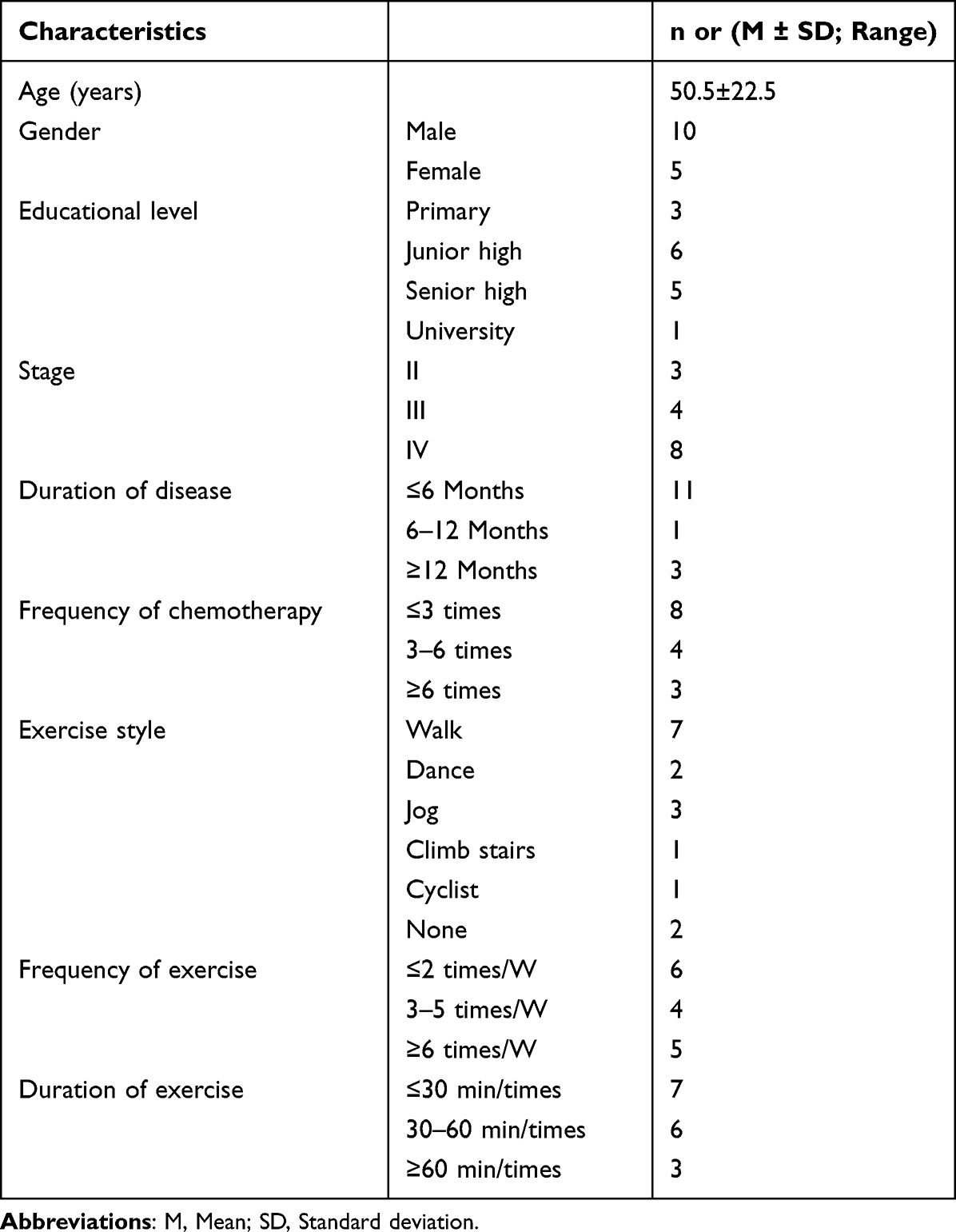 |
Table 1 Participant Characteristics (N = 15) |
Through the collation and analysis of the interview data, 3 themes and 8 sub-themes were obtained, The themes and sub-themes are shown in Table 2.
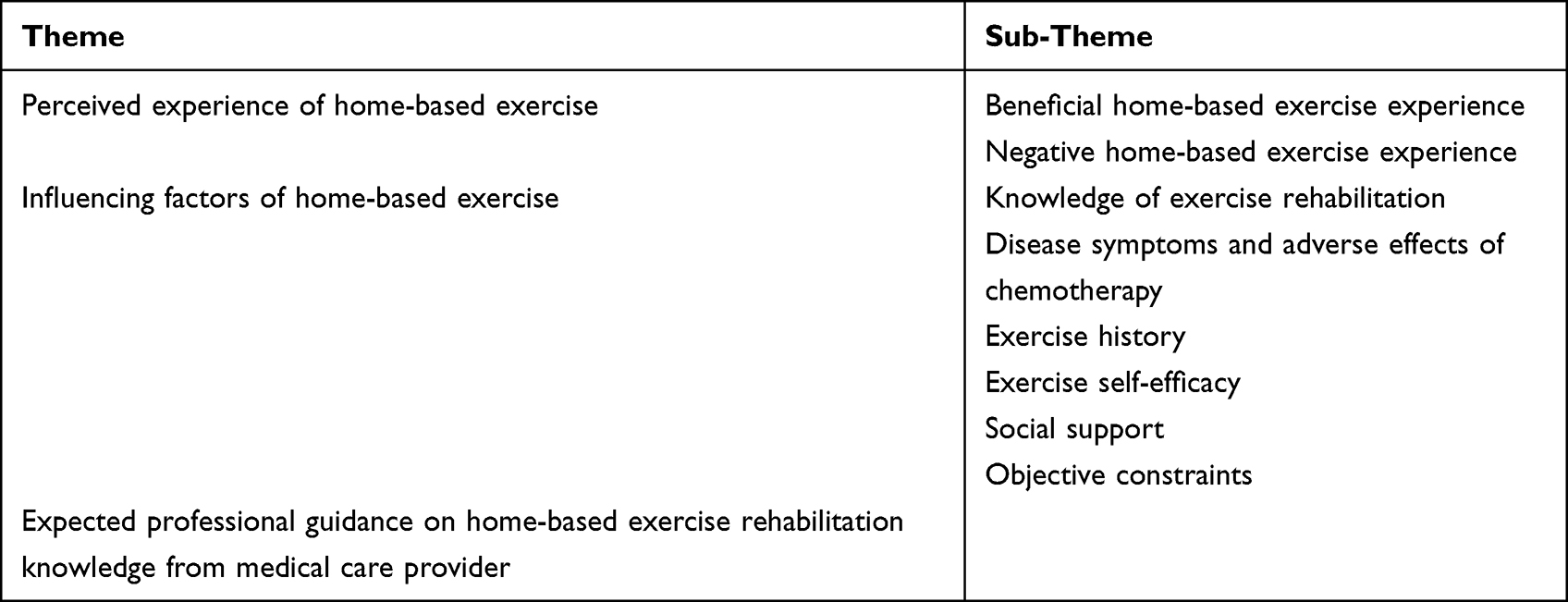 |
Table 2 Themes and Sub-Themes |
Perceived Experience of Home-Based Exercise
Patients’ perception of home-based experience is different, mainly divided into beneficial positive experiences and uncomfortable negative experiences.
Beneficial Home-Based Exercise Experience
When patients experience positive physical and mental experiences that are consistent with their expected goals, positive feedback will be formed and converted into motivation for subsequent active home-based exercise.
(I think) exercise is good, otherwise I can’t stick to the treatment for a year or two. As long as my health is good, I will continue to do Jiamusi dance every day. (P4, female, 50)
P14: In addition to the first two or three days after taking the medicine, I feel very tired, the other time I feel no difference from normal people, eat well, sleep well, I think this is a good foundation for regular exercise before, so now I continue to insist on exercise. (P14, male, 64)
Negative Home-Based Exercise Experience
Some patients with adverse home-based exercise experience will have a sense of withdrawal and hinder their home-based exercise.
I used to go out to square dance almost every day. Once when I danced, I breathed very fast, breathed hard, and my ribs hurt. Then I stopped dancing. (P8, female, 56)
I feel like I could walk fast, but I’m reluctant to try because I’ll be out of breath when I’m done. (P15, male, 73)
Once I insisted on walking seven times in a row in the community. After walking home, I felt very tired and did not want to take a walk. I still felt that I should take a rest instead of being too tired. (P2, male, 41)
Influencing Factors of Home-Based Exercise
Knowledge of Exercise Rehabilitation
The cognition of exercise rehabilitation knowledge was at the theoretical level, but the exercise of practice was insufficient. Most of the interviewed patients were aware of the benefits of exercise for their health, but their perceptions of the benefits of exercise were at a theoretical level. Most patients will participate in home-based exercise, but most of them do not have enough exercise, single form of exercise, and poor adherence.
Sometimes I go out for a walk, alone to think about something, nothing else. (P5, male, 51)
I usually go out for a walk for about 40 minutes, sometimes more than an hour. If the weather is bad or I feel sick, I will not move. (P13, male, 66)
Some patients or their caregivers lack the knowledge of exercise rehabilitation, and they think that they are no longer suitable for exercise when they have cancer, or they can only do some low-intensity exercise, and they worry that exercise will aggravate the disease or accelerate the progression of the disease.
The child is also afraid to let me move more, for fear that my body can not bear, will aggravate the disease. (P7, male, 56)
In addition, patients will also have fear of exercise, worried about the exercise aggravation of pain, chest tightness, asthma and other symptoms.
Exercise is good, but the lung disease can’t. The lung disease makes me unable to walk fast. When I walk fast, I pant and feel uncomfortable (P6, female, 55)
Disease Symptoms and Adverse Effects of Chemotherapy
Patients with lung cancer have symptoms such as fatigue, asthma, pain, and dyspnea. Some patients worry that they are not suitable for exercise because of shortness of breath after activity. Cancer-related fatigue is a unique symptom of patients with malignant tumors, and the fatigue after chemotherapy is more serious, which largely limits the patients’ home-based exercise. Some patients will also have a sense of stigma due to the diagnosis of lung cancer, and reduce or avoid outdoor activities.
We don’t have a course of treatment, in the hospital these days there is no place to run, after the drug home that a few days, all tired, do not want to move. (P10, female, 60)
I don’t want to go (to exercise), for fear that people will look at me in a different way, and I also feel that my coughing and expectoration will be rejected by others. (P1, female, 28)
I don’t want to go out, I prefer to stay at home and watch TV, I don’t want to meet acquaintances, their eyes make me uncomfortable. (P7, male, 56)
Repeated chemotherapy and various side effects after chemotherapy, such as poor appetite, poor appetite, fatigue, sleep disorders, etc., patients are prone to depression, anxiety, uncertainty about the prognosis and other negative emotions, and it is difficult to establish a positive attitude or insist on home exercise.
I know exercise is good, but now I just don’t want to move. My wife sometimes asks me to move more, and I don’t want to listen. (P2, male, 41)
I think since I have this disease, it means that my days are coming to an end, and there is no point in exercising. (P5, male, 51)
Exercise History
Patients who had exercise habits before the diagnosis of lung cancer would continue to exercise during the interval of chemotherapy, and also adjust the exercise mode and intensity timely according to their own conditions.
I used to weight-training, aerobic and anaerobic practice, but the illness did not practice (targeted aerobic and anaerobic exercise), and now, most of the time, will choose brisk walking or jogging. (P9, male, 57)
I used to do martial arts, but now I don’t practice. The intensity of martial arts is too high, and the range of action is also large, which is not suitable for me. Now I ride a bike and walk quickly to exercise. (P12, male, 64)
Exercise Self-Efficacy
Patients with good exercise self-efficacy will do home-based exercise every day if their physical condition allows, and will not give up exercise when they encounter some objective obstacles.
I like sports very much. Now I climb stairs for 20 minutes almost every day, jog for 40 minutes to 1 hour, and take a walk when I’m tired. (P14, male, 67)
I go out for a walk every day unless I’m in a bad condition. If it rains, I take an umbrella. (P3, male, 44)
Patients with poor exercise self-efficacy tend to lack initiative and transient enthusiasm in practice, even though they know that exercise is beneficial to health and have received guidance on the importance of home-based exercise many times.
Exercise is good for the body. After listening to (a science lecture), I feel that I need to move more, but after each chemotherapy, I have to feel tired for a week, and worry about accidents or aggravation in the process of activities, so I don’t run (step) for a while. (P10, female, 60)
I know exercise is good. Every time I sweat after exercise, I feel good, but I have other things or I break it when I’m admitted to the hospital for chemotherapy, and I can’t stick to it. (P11, male, 61)
Social Support
Effective social support Effective support can stimulate the motivation of patients to exercise, and even directly promote them to carry out home exercise, mainly including the support and company of family members, the encouragement and help of friends, the propaganda and education of exercise rehabilitation knowledge by medical staff, information support among patients, etc.
My husband often accompanies me to dance or watches me dance. I have been insisting (dance) nearly 2 years. (P4, female, 50)
I was diagnosed 2 months ago. At the beginning, I can’t eat well and can’t sleep. A doctor friend I know asked me to move more, saying that it could improve my immunity and improve my sleep. Now I can walk for about an hour every day. (P3, male, 44)
Through the mobile phone video and listening to some cases said by patients, I understand the benefits of exercise, and think it is feasible to carry out appropriate exercise. Try to walk slowly every day, about 40 minutes. (P6, female, 55)
Insufficient family support. Some family members do not support patients’ exercise, and think that they should take a rest when they are sick.
You can walk slowly, walk for 10 minutes, rest for 10 minutes, but jogging, fast walking is not good. I dare not try hard exercise for fear that my body will not be able to handle it. The two daughters also take good care of me. They think that what I need most is to eat well, drink well, sleep well, and the disease will recover well. They do not advise me to move too much, for fear that I will be tired. (P15, male, 73)
Objective Constraints
Through the interview, it was found that lung cancer patients were more inclined to outdoor exercise, and they believed that breathing more fresh outdoor air was good for the lungs, but outdoor exercise was easily limited by objective factors such as the site environment, weather and COVID-19 epidemic.
I thought about other ways of exercising, but I was too lazy to try because of my illness, limited space, time, and equipment. (P14, male, 67)
Recently the weather is very cold. I don’t go out much. When the weather is warm, I will go out for a walk, like in the summer, except the heavy rain or when it too hot to go out. (P13, male, 66)
Because of the outbreak and epidemic of COVID-19, I don’t go out dancing very much, and it’s not good to go to crowded places (for fear of getting infected). (P11, male, 61)
Expected Professional Guidance on Home-based Exercise Rehabilitation Knowledge from Medical Care Provider
It was learned from the interview that the patients expected to hear the health care workers’ knowledge education and exercise guidance about exercise for lung cancer patients.
If the doctor told me I could do more exercise, I would like to do more. (P1, female, 28)
When in hospital, if only the doctors and nurses could tell some knowledge about exercise. (P11, male, 61)
The doctor said to move more, but don’t tell me how exercise is good for my disease. I don’t dare to exercise hard anyway. (P15, male, 73)
Discussion
Patients with Lung Cancer Beneficial Cognition of Exercise Cannot Be Translated into Exercise Adherence Behavior
Patients’ preference for exercise comes from accidental or spontaneous behavior, and lack of professional guidance for exercise rehabilitation, so it is difficult to maintain exercise behavior despite knowing the benefits of exercise. Through interviews, this study found that patients’ cognition of the health benefits of exercise was mostly at the theoretical level, and there was a lack of exercise rehabilitation knowledge such as whether cancer patients can exercise and how to exercise. It is related to the traditional Chinese concept that cancer patients need to rest and rest. Most families think that lung cancer is a serious disease and needs to be raised. In clinical practice, the use of exercise as a strategy to prevent and manage tumors has received less attention. Considering that the main caregivers of lung cancer patients during the interval of chemotherapy are family members, family-centered exercise rehabilitation knowledge education for cancer patients can be carried out, using a variety of forms such as brochures, animated short films and popular science videos to correct the wrong perception of some patients or their families that cancer patients are not suitable for exercise and improve exercise rehabilitation knowledge literacy. By publicizing the benefits of home-based exercise in improving exercise endurance, reducing cancer-related fatigue, relieving negative emotions of depression and anxiety, improving the quality of life and relieving the pressure of resources, economy and travel,20,21 and the advantages of freely arranging exercise content on the premise of ensuring exercise volume and intensity,22 patients are promoted to change from cognition to behavior. In addition, this study found that lung cancer patients had a high degree of trust in medical staff and expected to receive education and guidance on exercise rehabilitation knowledge for lung cancer patients from medical staff, which was consistent with the study by Grange et al.23 It suggests that we need to focus on improving the knowledge level of medical staff about exercise rehabilitation of cancer patients and the awareness of exercise knowledge education and guidance for patients,24 and cultivate a professional team with a multidisciplinary cooperation model for the guidance of home exercise rehabilitation of cancer patients.
Individualized Exercise Program Was Developed According to Patients’ Symptom Characteristics and Exercise Preferences
The symptom burden and psychological burden of patients form the main hindering factors affecting the continuous exercise of patients. In addition, different patients have different preferences for exercise. To ensure that patients adhere to exercise, it is necessary to take into account the interest and hobbies of patients in exercise and form a dynamic factor to promote exercise, so as to reduce the symptom burden and psychological burden through continuous exercise. This study shows that patients with lung cancer have high participation in home-based exercise, but the amount of exercise is insufficient, and the main form of exercise is walking, which is consistent with the research results of Kartolo et al.25 In addition, it was also learned in the interview that patients with exercise habits would also reduce their exercise volume after the diagnosis of the disease, which was consistent with the research results of Titz et al.26 This may be related to the patient’s physical condition and side effects of chemotherapy. Therefore, disease - and treatment-related factors should also be considered when correcting the wrong perception of exercise rehabilitation in cancer patients. Patients’ physical function status is very important for their adherence to exercise.27 Patients with lung cancer have a heavy disease burden. In order to ensure the feasibility of home-based exercise plan, it is necessary to comprehensively evaluate the patient’s physical condition, exercise ability, exercise preference, the exercise environment, chemotherapy time, and promoting and hindering factors during home-based exercise before making a plan. According to the principle of step by step, before increasing the intensity, the duration is increased, and finally the kind.28 Attention should be paid to timely adjusting the mode, intensity, frequency and time of exercise according to the patient’s physical functional status. Patients should be encouraged to participate in physical activities in daily life such as housework and reduce sedentary behavior. Studies have shown that recreational exercise can improve the exercise compliance of patients with lung cancer,29 and it is suggested that the entertainment of exercise plan can be considered in the formulation of personalized home-based exercise plan.
Help Disease Symptoms Self-Management Skills, Strengthen Home Sports Confidence
The symptom burden of lung cancer patients undergoing chemotherapy is heavy. In addition to lung cancer specific symptoms such as cough, chest tightness and asthma, there are cancer-related fatigue, negative emotions such as depression and anxiety, fear of exercise, and stigma. The incidence of fatigue in lung cancer patients undergoing chemotherapy is high, and most of them are moderate to severe.30 Cancer-related fatigue and negative emotions can affect each other.31 Cancer-related fatigue can easily cause patients to produce negative emotions and refuse to carry out home exercise, and persistent negative emotions will aggravation fatigue symptoms and further hinder their home exercise behavior. Kinesiophobia refers to patients’ fear of functional rehabilitation exercise and daily activities due to fear of pain caused or aggravated by exercise.32 Patients who have experienced discomfort in the process of activity are more likely to develop kinesiophobia.33 The attention, support and help of medical staff in the management of patients’ disease symptoms can effectively improve the ability of patients to identify and deal with symptoms, and also let patients experience the feeling of being cared for and supported, which can then be transformed into the motivation to adhere to exercise.34 A regular follow-up plan led by the nursing team can be formulated, and patients’ disease symptoms and functional status can be given continuous attention and guidance with the help of patient-reported outcome measurement tools as the carrier of mobile health.35,36 The home exercise guidance plan can be adjusted through the feedback effect. At the same time, telemedicine technology was used to monitor the changes of patients’ exercise-related parameters and answer questions online. For example, portable mobile devices were used to monitor patients’ heart rate and blood oxygen indicators during home exercise, so as to provide guarantee for patients’ exercise safety. Patients were informed of their normal physiological reactions and abnormal symptoms during exercise, so as to reduce their kinesiophobia and enhance their confidence in home exercise. In addition, some patients refuse their favorite outdoor sports or group sports due to the stigma of cancer diagnosis. The level of stigma of patients can be reduced by group psychotherapy, self-confidence training, and patient mutual assistance,37–39 and they are encouraged to choose home sports according to their personal interests.
Give Full Play to the Advantages of Various Resources and Encourage Home-Based Exercise Behavior from Various Angles
This study shows that patients who have good exercise self-efficacy, can get effective support or benefit from exercise as well good compliance with home exercise behavior. Exercise self-efficacy refers to the individual’s belief, judgment and subjective feelings about their own exercise ability and the speculation of the expected results brought by their exercise behavior, which focuses on the individual’s confidence in the ability and results of exercise behavior.40 Studies have shown that the positive feedback formed in the process of exercise training can strengthen the exercise self-efficacy of patients,41 suggesting that family members and medical staff can guide patients to perceive the benign experience of home exercise and increase the motivation and confidence of patients to exercise at home during the interval of chemotherapy. In addition, in the family-centered coping model of cancer in China, the influence of family members on the home-based exercise behavior of patients should be considered, and family members can be encouraged to accompany patients to participate in home-based exercise to promote exercise behavior and ensure exercise safety. Regular patient communication meetings were organized, and patients with exercise habits were invited to share the positive experience of home exercise. Through the incentive effect of indirect experience, positive emotions were stimulated, and patients’ home exercise behavior compliance was promoted and improved. The knowledge of exercise rehabilitation can also be publicized and the experience of disease symptom management can be shared through the exchange platform. It is necessary to promote square dance, Tai Chi, Ba eight-section brocade, etc., which is widely based in the masses, to enrich the forms of exercise and reduce the restrictions of objective factors such as venues, weather and COVID-19 epidemic on patients’ home-based exercise.
Strengths and Limitations
This study strictly followed the guiding method of qualitative research, and fully reported the relevant matters of the study to ensure the rigor of the study and the transparency and credibility of the data. Most of the existing studies are quantitative studies on the exercise intervention of lung cancer patients. Chinese lung cancer patients are mostly at home during the interval of chemotherapy, and the research on their home exercise state and home exercise experience has not been found.
This study is a single directional study. In the future, qualitative and quantitative mixed studies can be carried out by expanding the sample size to explore the changes and characteristics of home-based exercise behavior trajectory of lung cancer patients during chemotherapy interval and analyze its potential influencing factors.
In addition, some of the patients who participated in the interview were accompanied by their family members, and they may not have fully expressed their views. However, in the data analysis stage, the interview data were returned to the interviewees for verification, and almost no patients expressed doubts about the description of the interview results.
Conclusion
Through descriptive qualitative research, this paper found that patients with lung cancer undergoing chemotherapy had different perceptions of experience of home-based exercise. The influencing factors of home-based exercise included exercise rehabilitation knowledge, disease symptoms and adverse reactions of chemotherapy, exercise habits, exercise self-efficacy, social support and objective factor restrictions, and the needs of patients for home-based exercise rehabilitation knowledge were not satisfied. It is expected to get professional guidance from medical staff on sports rehabilitation knowledge. In clinical work, medical staff can carry out family-centered exercise rehabilitation knowledge education and guidance for lung cancer patients through pamphlets and popular science videos, comprehensively evaluate the patient’s chemotherapy cycle, physical condition, exercise preference and other characteristics to formulate a personalized home-based exercise plan for them, and help patients with disease symptom self-management skills with the help of various forms of mobile medical platforms. Take advantage of the existing resources around patients to encourage exercise behavior and improve home exercise compliance.
Acknowledgments
The authors acknowledge the invaluable contribution from the lung cancer patients who shared their thoughts and experiences in the individual interviews. Thanks are also given to the medical staff of the second and third departments of Oncology in Shanghai Pulmonary Hospital Affiliated to Tongji University for their important inputs and comments along the process.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Natural Science Foundation of China (grant number: 71904144), Scientific Clinical research project of Tongji University (grant number: JS2210319).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021. doi:10.3322/caac.21660
2. He J, Li N, Chen WQ, et al. Chinese guidelines for the screening, early diagnosis and early treatment of lung cancer (2021, Beijing). Chin J Cancer. 2021;30:81–111. Chinese. doi:10.11735/j.issn.1004-0242.2021.02.A001
3. Li NN, Wu J, Xu M, et al. To analyze symptom clusters and influencing factors in lung cancer patients undergoing chemotherapy. J Adv Nurs Educ. 2018;2018:2029–2032. Chinese.
4. Liao J, Wang Y, Dai W, et al. Profiling symptom burden and its influencing factors at discharge for patients undergoing lung cancer surgery: a cross-sectional analysis. J Cardiothorac Surg. 2022;17:1–229. doi:10.1186/s13019-022-01974-9
5. Wang DD, Fu JF, Zuo XP, et al. Symptom clusters and their effects on daily life in patients with lung cancer during chemotherapy. J Nurs Manag. 2013;13:156–158. Chinese.
6. Wei X, Yu H, Dai W, et al. Discrepancy in the perception of symptoms among patients and healthcare providers after lung cancer surgery. Support Care Cancer. 2022;30:1169–1179. doi:10.1007/s00520-021-06506-0
7. Newton RU, Taaffe DR, Galvao DA. Clinical oncology society of Australia position statement on exercise in cancer care. Med J Aust. 2019;210. doi:10.5694/mja2.12043
8. Mugele H, Freitag N, Wilhelmi J, et al. High-intensity interval training in the therapy and aftercare of cancer patients: a systematic review with meta-analysis. J Cancer Surviv. 2019;13:205–223. doi:10.1007/s11764-019-00743-3
9. Rutkowska A, Jastrzebski D, Rutkowski S, et al. Exercise training in patients with non–small cell lung cancer during in-hospital chemotherapy treatment. J Cardiopulm Rehabil. 2019;39:127–133. doi:10.1097/HCR.0000000000000410
10. Murley B, Haas B, Hermanns M, Wang YT, Stocks E. Influence of Tai Chi on self-efficacy, quality of life, and fatigue among patients with cancer receiving chemotherapy: a pilot study brief. J Holist Nurs. 2019;37:354–363. doi:10.1177/0898010119867557
11. Luan X, Tian XY, Zhang HX, et al. Exercise as a prescription for patients with various diseases. J Sport Health Sci. 2019;8:422–441. doi:10.1016/j.jshs.2019.04.002
12. Avancini A, Pala V, Trestini I, et al. Exercise levels and preferences in cancer patients: a cross-sectional study. Int J Environ Res Public Health. 2020:17. doi:10.3390/ijerph17155351
13. Zhang LF, Zhou CF, Luo JN, et al. To explore the effects of aerobic exercise combined with resistance exercise on cancer-related fatigue and sleep quality in elderly lung cancer patients undergoing chemotherapy after surgery. Chin J Mod Nurs. 2020;26:2452–2455. Chinese. doi:10.3760/cma.j.cn115682-20200220-00890
14. Quist M, Langer SW, Lillelund C, et al. Effects of an exercise intervention for patients with advanced inoperable lung cancer undergoing chemotherapy: a randomized clinical trial. Lung Cancer. 2020;145:76–82. doi:10.1016/j.lungcan.2020.05.003
15. Ji H, Sha ML, Ke QH, Huang HB. The perspectives and lived experience of postoperative patients with lung cancer participating in a home-based exercise intervention. Semin Oncol Nurs. 2022;38. doi:10.1016/j.soncn.2021.151235
16. Liu M. The application of Colaizzi’s seven steps in data analysis of phenomenological research. Chin J Nurs. 2019;34:90–92. Chinese.
17. Willis DG, Sullivan-Bolyai S, Knafl K, Cohen MZ. Distinguishing features and similarities between descriptive phenomenological and qualitative description research. West J Nurs Res. 2016;38:1185–1204. doi:10.1177/0193945916645499
18. Tian L, Chen Y, Long YH, et al. Qualitative research on self-management experience of home fall prevention in cancer patients after chemotherapy. Chin J Nurs. 2020;55:1648–1652. Chinese.
19. Tong JT, Wang Y, Ni P, et al. Qualitative research on limb function rehabilitation behavior of breast cancer patients after surgery. Chin J Nurs. 2022;57:711–717. Chinese.
20. He X, Zheng W, Liu Y. Demand for “internet +” pulmonary rehabilitation in elderly patients after lung cancer surgery: a qualitative study. China Med Guide. 2021;18:56–59. Chinese.
21. Yang M, Liu L, Gan CE, et al. Effects of home-based exercise on exercise capacity, symptoms, and quality of life in patients with lung cancer: a meta-analysis. Eur J Oncol Nurs. 2020;49:101836. doi:10.1016/j.ejon.2020.101836
22. Li DF, Li H, Ma JJ, et al. To explore the application of family-based voluntary exercise in patients with lung cancer. Chin J Mod Nurs. 2020;26:3326–3329. Chinese. doi:10.3760/cma.j.cn115682-20191114-04143
23. Wu E, Lu T, Ni J. Research progress of family-based rehabilitation of lung cancer patients. Chin Rehabil. 2021;36:432–436. Chinese. doi:10.3870/zgkf.2021.07.011
24. Zhang J. Analysis and prospect of tumor rehabilitation in China. Chin J Rehabil Med. 2018;33:4–6. Chinese.
25. Kartolo A, Cheng S, Petrella T. Motivation and preferences of exercise programmes in patients with inoperable metastatic lung cancer: a need assessment. Support Care Cancer. 2016;24:129–137. doi:10.1007/s00520-015-2767-9
26. Titz C, Hummler S, Schmidt ME, Thomas M, Steins M, Wiskemann J. Exercise behavior and physical fitness in patients with advanced lung cancer. Support Care Cancer. 2018;26:2725–2736. doi:10.1007/s00520-018-4105-5
27. Denehy L, Granger C, Edbrooke L. Who is able to adhere to exercise during non-surgical treatment for lung cancer? Eur Respir J. 2020;56. doi:10.1183/13993003.congress-2020.3237
28. Cancer Nutrition Committee, China anti-Cancer Association, State Key Laboratory for Market Regulation of Cancer Special Medical Foods, Oncology Palliative Care Committee, Beijing Cancer Society. Chinese expert consensus on exercise therapy for cancer patients. Electron J Cancer Metab Nutr. 2022;9:298–311. Chinese. doi:10.16689/j.cnki.cn11-9349/r.2022.03.006
29. Ma XR, Dong GY, Meng AF, et al. Formulation and practice of perioperative recreational exercise plan for patients with lung cancer. Chin J Nurs. 2019;54:1313–1317. Chinese.
30. Xu HB, Jiang LP, Yin ZQ, et al. Investigation of cancer-related fatigue in lung cancer patients undergoing chemotherapy. Chin J Nurs. 2010;45:332–335. Chinese.
31. Li XX. Study on Influencing Factors of Lung Cancer Related Fatigue and Its Relationship with quality of Life [D]. Liaoning: Dalian Medical University; 2014. Chinese.
32. Mas S, Quantin X, Ninot G. Barriers to, and facilitators of physical activity in patients receiving chemotherapy for lung cancer: an exploratory study. J Palliat Care. 2015;31:89–96. doi:10.1177/082585971503100204
33. Velthuis MJ, Peeters PH, Gijsen BC, et al. Role of fear of movement in cancer survivors participating in a rehabilitation program: a longitudinal cohort study. Arch Phys Med Rehabil. 2012;93:332–338. doi:10.1016/j.apmr.2011.08.014
34. Edbrooke L, Denehy L, Granger CL, Kapp S, Aranda S. Home-based rehabilitation in inoperable non-small cell lung cancer—the patient experience. Support Care Cancer. 2019;28:99–112. doi:10.1007/s00520-019-04783-4
35. Basch E, Deal AM, Kris MG, et al. Symptom monitoring with patient-reported outcomes during routine cancer treatment: a randomized controlled trial. J Clin Oncol. 2016;34:557. doi:10.1200/JCO.2015.63.0830
36. Dai W, Feng W, Zhang Y, et al. Patient-reported outcome-based symptom management versus usual care after lung cancer surgery: a multicenter randomized controlled trial. J Clin Oncol. 2022;40:988–996. doi:10.1200/JCO.21.01344
37. Wang YK, Li Q, Hou JH. To explore the effect of group psychotherapy on stigma and quality of life in patients with lung cancer. Chin J Mod Nurs. 2018;24:3186–3189. Chinese. doi:10.3760/cma.j.issn.1674-2907.2018.26.020
38. Liu Q, Pan HF. To explore the effects of remote support exercise combined with self-confidence training on stigma and fatigue in elderly patients undergoing radical resection of lung cancer. Chin J Gerontol. 2021;41:3570–3573. Chinese. doi:10.3969/j.issn.1005-9202.2021.16.050
39. Li H, Guo YN. To study the effect of patient mutual assistance nursing model on the stigma and social function of patients with lung cancer. J Nurs Manag. 2017;17:660–661. Chinese.
40. Zhang XM. Development of Exercise Self-Efficacy Scale for Lung Cancer Patients [D]. Anhui: Anhui Medical University; 2020. Chinese.
41. Ha FJ, Hare DL, Cameron JD, Toukhsati SR. Heart failure and exercise: a narrative review of the role of self-efficacy. Heart Lung Circ. 2018;27:22–27. doi:10.1016/j.hlc.2017.08.012
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Patient Perspectives and Side-Effects Experience on Chemotherapy of Non-Small Cell Lung Cancer: A Qualitative Study
Zubair HM, Khan MA, Gulzar F, Alkholief M, Malik A, Akhtar S, Sharif A, Akhtar MF, Abbas M
Cancer Management and Research 2023, 15:449-460
Published Date: 25 May 2023
Nursing Dilemmas in Chemotherapy-Induced Peripheral Neuropathy: A Qualitative Study of a Tertiary Hospital in China
Fan JX, Hu YC, Chen X, Li Y
Journal of Pain Research 2023, 16:2299-2308
Published Date: 6 July 2023
Adolescent Patients’experiences of Mental Disorders Related to School Bullying
Chu ZJ, Yin X, Zhu GY, Yu SS, Li HY
Journal of Multidisciplinary Healthcare 2024, 17:2911-2919
Published Date: 19 June 2024
Perspectives of People with Type 2 Diabetes Mellitus Towards a Decision Aid Assessing Preferences of Glucose-Lowering Drugs: The Dilemma of Choosing
Roldan Munoz S, Mol PGM, de Vries F, van Dijk PR, Hillege H, Postmus D, de Vries ST
Patient Preference and Adherence 2025, 19:215-234
Published Date: 25 January 2025
Estimating the Cost-Effectiveness of Tumor Treating Fields (TTFields) Therapy with an Immune Checkpoint Inhibitor or Docetaxel in Metastatic Non-Small Cell Lung Cancer
Furnback W, Wu E, Koh CYC, Nino de Rivera Guzman JF, Kruhl C, Kotecha R, Wang BC
ClinicoEconomics and Outcomes Research 2025, 17:55-68
Published Date: 5 February 2025