Back to Journals » Journal of Pain Research » Volume 18
Paravertebral Block versus Erector Spinae Plane Block for Postoperative Analgesia and Recovery: A Systematic Review and Meta-Analysis
Authors Ren D, Wang D, Zhang W, Lei L, He X, Yue H
Received 1 May 2025
Accepted for publication 19 August 2025
Published 2 September 2025 Volume 2025:18 Pages 4509—4526
DOI https://doi.org/10.2147/JPR.S537574
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Andrea Tinnirello
Dongqing Ren,1 Dabin Wang,1 Wenjuan Zhang,1 Linfeng Lei,1 Xiyan He,1 Haiyuan Yue2– 4
1Department of Anesthesiology, Gansu Provincial Hospital, Lanzhou, Gansu, 730000, People’s Republic of China; 2Department of Orthopaedics, Lanzhou University Second Hospital, Lanzhou, Gansu, 730000, People’s Republic of China; 3Orthopaedic Clinical Research Center of Gansu Province, Lanzhou, Gansu, 730000, People’s Republic of China; 4Intelligent Orthopaedic Industry Technology Center of Gansu Province, Lanzhou, Gansu, 730000, People’s Republic of China
Correspondence: Haiyuan Yue, Email [email protected]
Background: This systematic review and meta-analysis was performed to assess the relative efficacy of paravertebral block (PVB) and erector spinae plane block (ESPB) for postoperative analgesia and recovery.
Methods: Randomized controlled trials (RCTs) evaluating PVB and ESPB for postoperative analgesia and recovery were retrieved from databases, including PubMed, Embase, MEDLINE, Cochrane Library, Science-Direct, and Google Scholar, from inception to January 2025. The primary outcome included resting Visual Analogue Scale (VAS) at 6 h and quality of recovery (QoR) score in first 24 h. The meta-analysis was conducted using Stata 15.1 software. The certainty of the evidence was assessed utilizing the risk of bias and GRADE frameworks.
Results: We included 33 RCTs with 2256 patients. For resting VAS at 6 h, there was no significant difference between PVB and ESPB (mean difference [MD] = − 0.08, 95% confidence interval [CI]: − 0.44 to 0.27). For QoR, there was no significant difference between PVB and ESPB (MD = − 0.44, 95% CI: − 2.64 to 1.76). For resting VAS at 12 h, ESPB had a lower VAS than PVB. For resting VAS at 24 h, movement VAS at 6 h, 12 h, 24 h, time of first rescue analgesia, LOS, and postoperative nausea and vomiting (PONV), there were no significant differences between PVB and ESPB. However, PVB had a lower morphine consumption than ESPB.
Conclusion: There were no significant clinical differences between PVB and ESPB in terms of the VAS, QoR, time of first rescue analgesia, LOS, and PONV. Based on existing evidences, we recommended the application of ESPB in thoracic surgery, breast surgery, kidney surgery, and abdominal surgery.
Limitation: The included studies showed considerable variability in postoperative analgesia protocols, which increased heterogeneity in the results. There was a lack of data on long-term analgesia and functional outcomes.
Keywords: analgesia, erector spinae plane block, meta-analysis, paravertebral block, recovery
Introduction
Effective postoperative analgesia is essential for facilitating recovery, minimizing complications, and enhancing patient satisfaction after surgical procedures.1 Among various regional anesthesia techniques, paravertebral block (PVB) and erector spinae plane block (ESPB) have garnered significant attention for their potential in managing postoperative pain.2,3 Other nerve blocks such as intercostal nerve block, quadratus lumborum block, and transversus abdominis plane block are all derivatives of the ESPB and PVB. Both techniques offer distinct mechanisms and approaches to provide analgesia, yet comparative analyses of their effectiveness, safety profiles, and impact on recovery remain limited.
The PVB is a procedure that involves the injection of local anesthetics (LAs) into the paravertebral space.4 It has demonstrated significant efficacy in controlling postoperative pain, particularly in surgeries involving the chest and abdomen.4–6 Numerous studies have indicated that PVB can reduce opioid consumption, lower pain scores, and enhance pulmonary function.7–9 However, despite its benefits, PVB is not without limitations, potential complications such as pneumothorax, hematoma formation, and nerve injury, along with its technically demanding nature, create barriers to its widespread adoption.2 The ESPB is a relatively novel technique that involves depositing LAs in the fascial plane deep to the erector spinae muscle.10 Initial studies suggest that ESPB is associated with a favorable safety profile, simpler technique, and effective pain relief.11,12 The growing body of literature has highlighted its potential to spare the use of systemic opioids while providing adequate analgesia, thereby minimizing opioid-related side effects such as nausea, vomiting, and sedation.10 However, its requirement for large volumes of LAs to achieve an extensive and effective blockade, which raises concerns about potential toxicity and limits its safety in certain patient populations.11,12
Given the distinct characteristics of both PVB and ESPB, the precise comparative efficacy in terms of pain control, opioid-sparing effects, and overall recovery outcomes remains inadequately addressed in the literature. Our meta-analysis will compare the effectiveness of PVB with ESPB in providing postoperative analgesia and enhancing recovery outcomes. The findings will provide evidence-based recommendations for clinicians in selecting the optimal analgesic strategy tailored to individual patient and surgical needs.
Methods
Our study adhered to the guidelines of the PRISMA13 and the protocol was registered in the International Prospective Register of Systematic Reviews (CRD42025633254). This work started in 6 January 2025.
Inclusion and Exclusion Criteria
Eligibility criteria were designed according to PICOS criteria: patients undergoing surgeries for adults or children (P); interventions included single-injection PVB and ESPB (I); PVB or ESPB (C); resting and movement pain score, quality of recovery (QoR) scores, time of first rescue analgesia, total morphine consumption in first 24h, length of hospital stay, postoperative nausea and vomiting (PONV) (O); randomized controlled trials (RCTs) (S). Studies were excluded if they met the following criteria: (1) studies that did not report outcomes or the data can not be used for statistical analysis; (2) unpublished studies, parallel and crossover randomized design studies; (3) studies that appear to report the same data more than once.
Search Strategy
We searched PubMed, MEDLINE, Embase, Cochrane Library, Science-Direct, and Web of Science without language restriction from inception to January 2025. The search strategy was based on the PICOS framework and principles, the key words and Medical Subject headings (MESH) descriptor terms were as follows: “paravertebral block”, “erector spinae plane block”, “PVB”, and “ESPB”. There was no limitation on sample size, surgical types and language.
Data Extraction
Two researchers individually reviewed all titles, abstracts, and then full texts sequentially. The disagreements on eligibility were resolved by the third reviewer. The data extracted from each RCT included author, year of publication, country, blinding, surgical types, interventions description, sample size, postoperative analgesic regimens, and outcomes. The primary outcome included resting pain score at 6 h and QoR score in first 24 h. The secondary outcomes included resting pain score at 12 h, 24 h, movement pain score at 6 h, 12 h, 24 h, time of first rescue analgesia, total morphine consumption in first 24h, length of hospital stay (LOS), and PONV.
Certainty of Evidence
Two independent investigators assessed the certainty of evidence by using the Cochrane Collaboration’s tool, which included of sequence generation, allocation sequence concealment, blinding of participants and personal, blinding of outcome assessment, incomplete outcome data, selective outcome reporting and other potential sources bias.14 The result was shown by the risk of bias and GRADE framework.
Statistical Analysis
Statistical analysis was carried out in STATA 15.1 software, and the data were synthesized by random-effects model. Pain scores were converted to the 0–10 VAS, and opiates consumption was converted to intravenous morphine equivalent doses. Meanwhile, we used Luo’s and Wan’s formula to convert the data expressed as median and inter-quartile range to mean and standard deviations.15,16 The effect estimate was reported as the relative risk (RR) and 95% confidential intervals (CIs) for PONV. The effect estimate was reported as the mean difference (MD) and 95% CIs for pain score, QoR score, time of first rescue analgesia, total morphine consumption in first 24h, and LOS. Overall effect sizes were illustrated by forest plots, and the subgroup analysis was based on the surgical types. Heterogeneity was considered significant if I2 ≥ 50%,17 and then we performed sensitivity analysis and subgroup analysis to find the sources of heterogeneity. P value < 0.05 was considered as statistical significance in all analyses. The publication bias was usually assessed by funnel plot, but it was assessed by using Begg’s and Egger’s tests if the number of included studies was less than 10.18,19
Results
We obtained 260 potentially relevant records, 193 were excluded after reviewing titles and abstracts alone. We reviewed the full text of the remaining 67 potentially eligible studies, 33 RCTs with 2256 patients were included in this meta-analysis,20–52 between PVB (n = 1131 patients) and ESPB (n = 1125 patients) groups. Figure 1 showed the process of literature selection. Table 1 showed the basic characteristics of the included studies. The vast majority of trials used ropivacaine or bupivacaine alone, and a total volume between 20 and 30 mL. The most common types of surgeries included video-assisted thoracic surgery (8 RCTs) and modified radical mastectomy (8 RCTs). The resting VAS at 6 h was reported in 17 RCTs, and the QoR was reported in 5 RCTs.
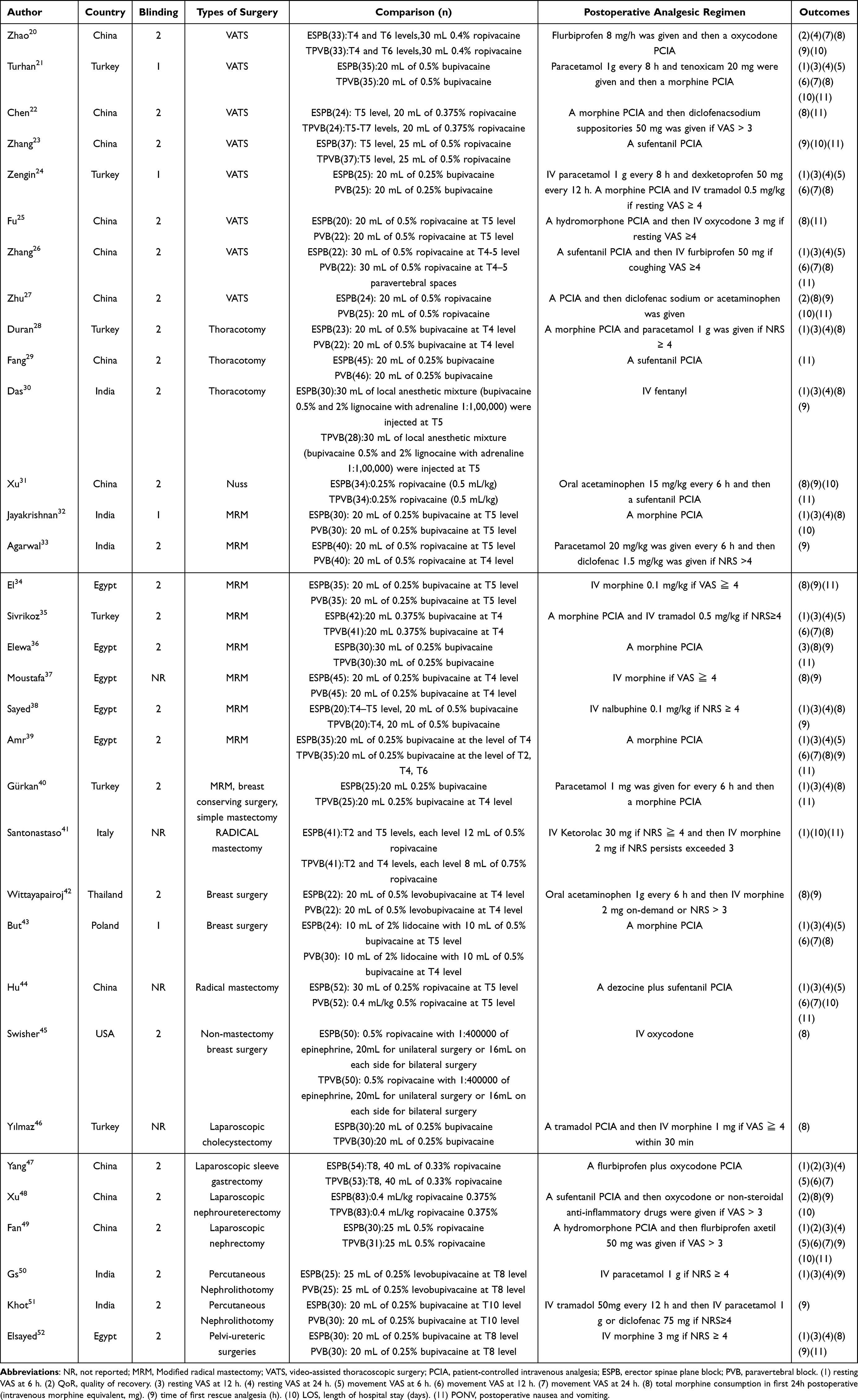 |
Table 1 Study Characteristics of Included Studies |
 |
Figure 1 PRISMA flow diagram of study selection. Notes: PRISMA figure adapted from Page MJ, Moher D, Bossuyt PM et al. PRISMA 2020 explanation and elaboration: updated guidance and exemplars for reporting systematic reviews. BMJ. 2021;372:n160. doi: 10.1136/bmj.n160.13. |
Assessment of Bias
Risk of bias of the primary outcomes were presented in Figures 2 and 3. The funnel plot of resting VAS at 6 h did not suggest any publication bias (Figure 4). For QoR, the results of Begg’s test and Egger’s test indicated that there were no publication bias (p=0.462 and p=0.378, respectively).
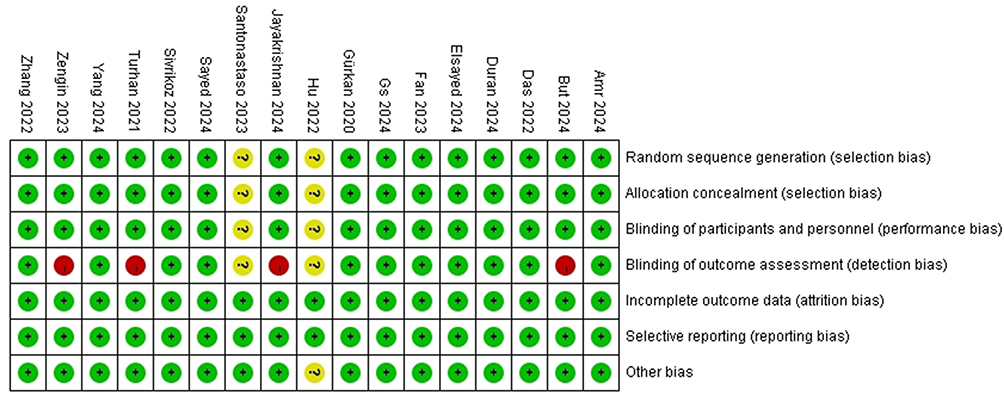 |
Figure 2 Risk of bias of resting VAS at 6 h. Data from these studies - Amr 2024.39 But 2024,43 Das 2022,30 Duran 2024,28 Elsayed 2024,52 Fan 2023,49 Gs 2024,50 Gürkan 2020,40 Hu 2022,44 Jayakrishnan 2024,32 Santonastaso 2023,41 Sayed 2024,38 Sivrikoz 2022,35 Turhan 2021,21 Yang 2024,47 Zengin 2023,24 Zhang 2022.26. |
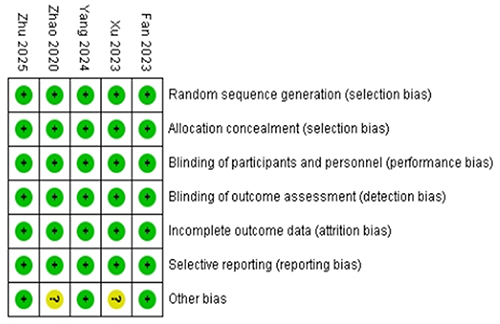 |
Figure 3 Risk of bias of QoR. Notes: Data from these studies - Fan 2023,49 Xu 2023,48 Yang 2024,47 Zhao 2020,20 Zhu 2025.27 |
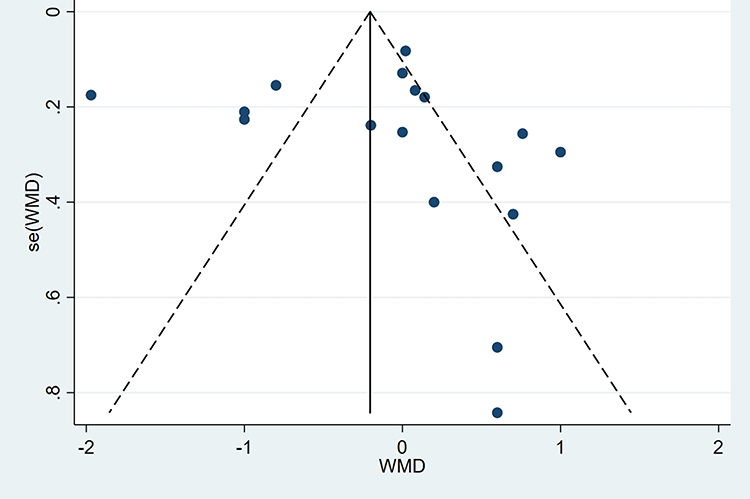 |
Figure 4 Funnel plot of resting VAS at 6 h. Abbreviation: WMD, weighted mean difference. |
Resting VAS at 6 h
The pooled data of seventeen studies did not suggest that PVB was superior to ESPB (MD = −0.08, 95% CI: −0.44 to 0.27; I2 = 92.2%; Figure 5). Due to the significant heterogeneity, we had to perform a sensitivity analysis and subgroup analysis. The sensitivity analysis demonstrated that the result was robust (Figure 6). The subgroup analysis showed that ESPB had a lower VAS than PVB in abdominal surgery (MD = −0.8, 95% CI: −1.1 to −0.5), but there were no significant differences in thoracic surgery, breast surgery, and kidney surgery (Figure 7).
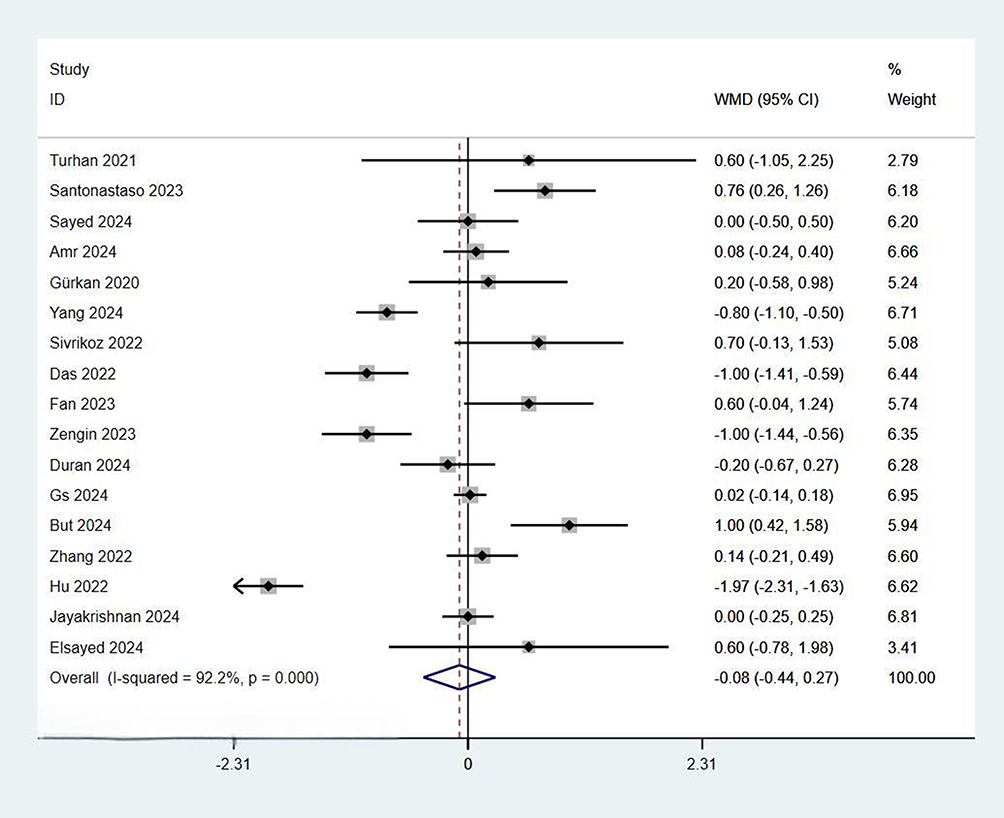 |
Figure 5 Forest plot of resting VAS at 6 h. Abbreviation: WMD, weighted mean difference. Notes: Weights are from random effects analysis. Turhan 2021,21 Santonastaso 2023,41 Sayed 2024,38 Amr 2024,39 Gürkan 2020,40 Yang 2024,47 Sivrikoz 2022,35 Das 2022,30 Fan 2023,49 Zengin 2023,24 Duran 2024,28 Gs 2024,50 But 2024,43 Zhang 2022,26 Hu 2022,44 Jayakrishnan 2024,32 Elsayed 2024.52 |
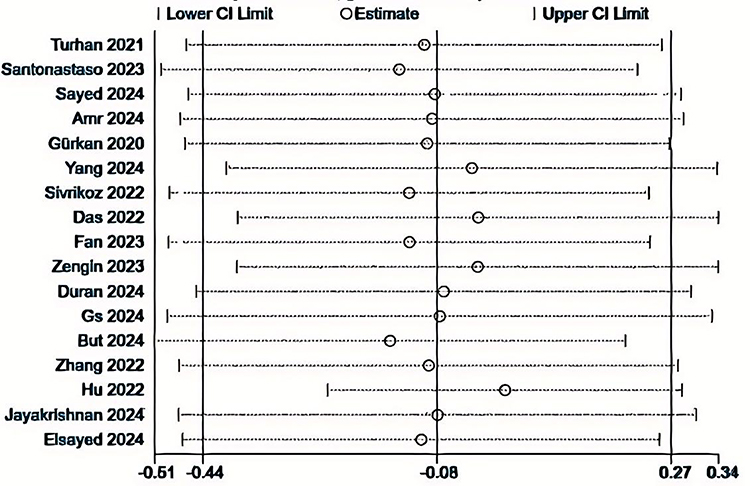 |
Figure 6 Sensitivity analysis of resting VAS at 6 h. Turhan 2021,21 Santonastaso 2023,41 Sayed 2024,38 Amr 2024,39 Gürkan 2020,40 Yang 2024,47 Sivrikoz 2022,35 Das 2022,30 Fan 2023,49 Zengin 2023,24 Duran 2024,28 Gs 2024,50 But 2024,43 Zhang 2022,26 Hu 2022,44 Jayakrishnan 2024,32 Elsayed 2024.52 |
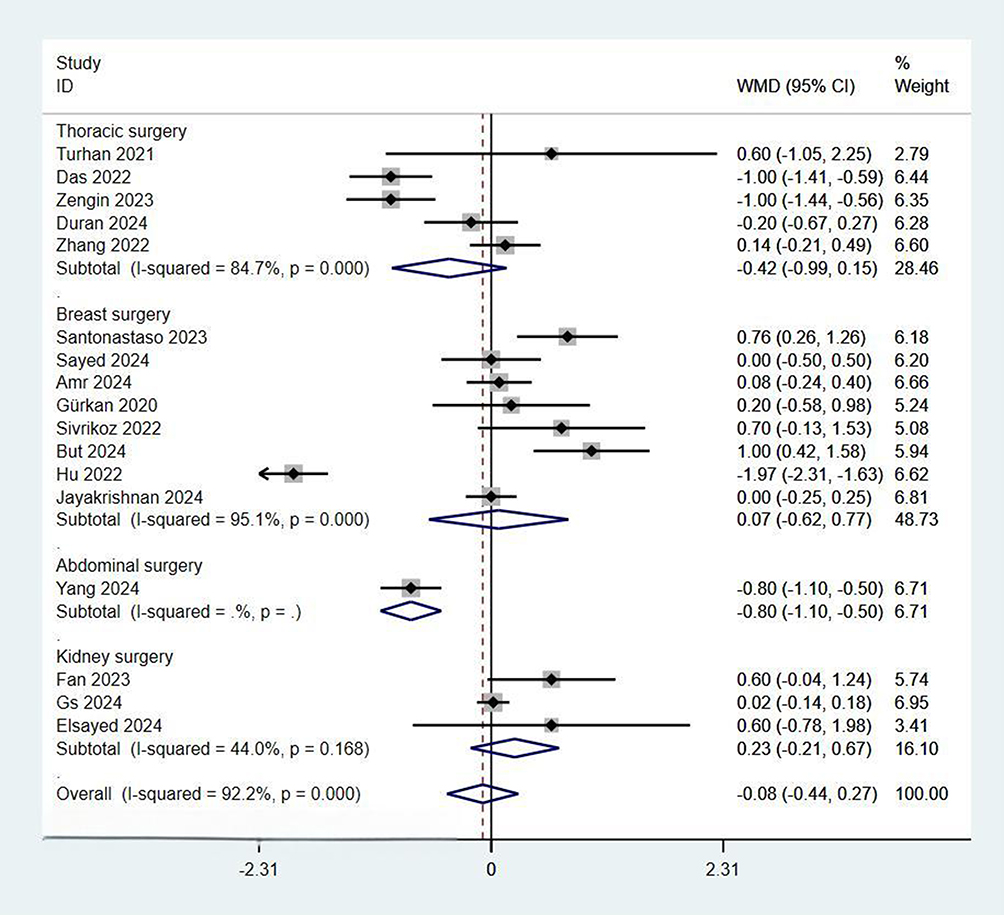 |
Figure 7 Subgroup analysis of resting VAS at 6 h. Abbreviation: WMD, weighted mean difference. Notes: Weights are from random effects analysis. Turhan 2021,21 Das 2022,30 Zengin 2023,24 Duran 2024,28 Zhang 2022,26 Santonastaso 2023,41 Sayed 2024,38 Amr 2024,39 Gürkan 2020,40 Sivrikoz 2022,35 But 2024,43 Hu 2022,44 Jayakrishnan 2024,32 Yang 2024,47 Fan 2023,49 Gs 2024,50 Elsayed 2024.52 |
QoR
The pooled data of five studies did not suggest that PVB was superior to ESPB (MD = −0.44, 95% CI: −2.64 to 1.76; I2 = 82.7%; Figure 8). The sensitivity analysis demonstrated that the result was not robust (Figure 9). The subgroup analysis showed the similar effects in thoracic surgery, kidney surgery, and abdominal surgery (Figure 10).
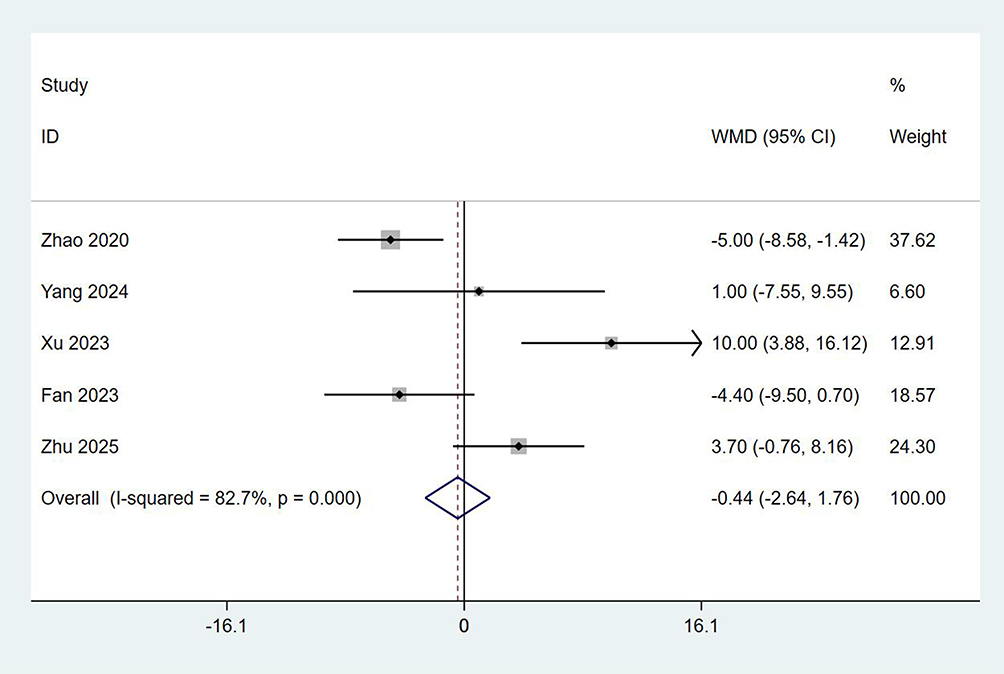 |
Figure 8 Forest plot of QoR. Zhao 2020.20 Yang 2024,47 Xu 2023,48 Fan 2023,49 Zhu 2025.27 Abbreviation: WMD, weighted mean difference. |
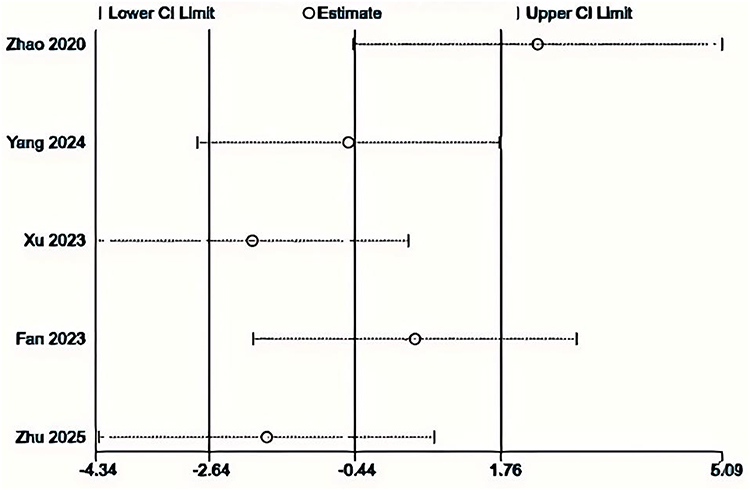 |
Figure 9 Sensitivity analysis of QoR. Zhao 2020.20 Yang 2024,47 Xu 2023,48 Fan 2023,49 Zhu 2025.27 |
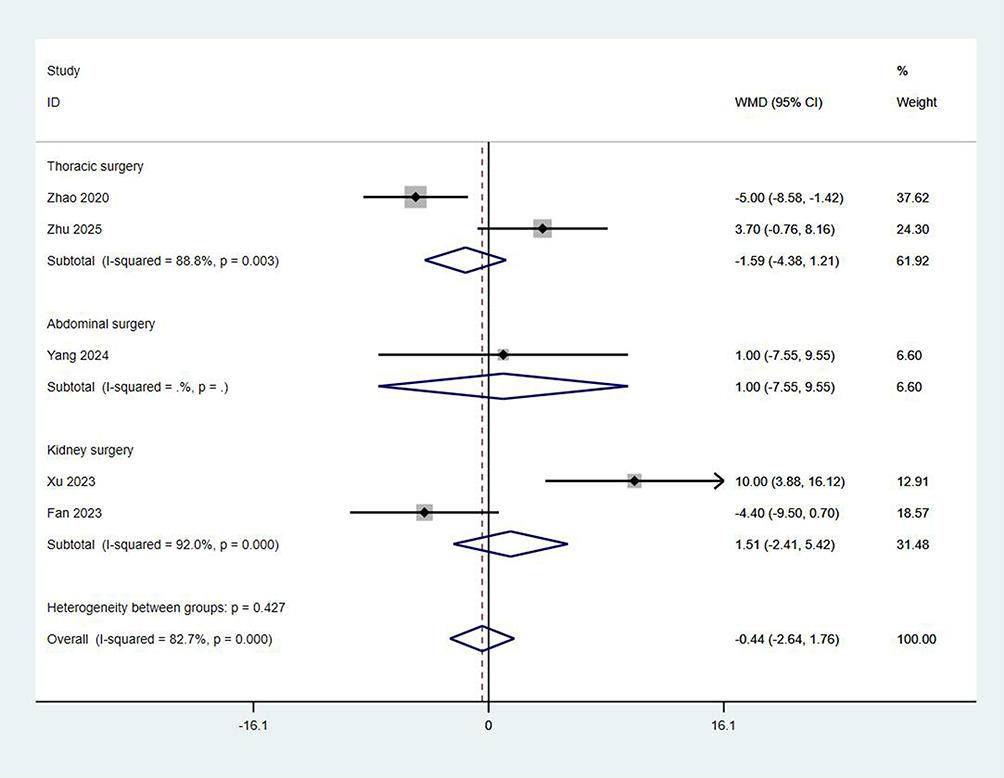 |
Figure 10 Subgroup analysis of QoR. Zhao 2020.20 Zhu 2025,27 Yang 2024,47 Xu 2023,48 Fan 2023.49 Abbreviation: WMD, weighted mean difference. |
Resting VAS at 12 h
The pooled data of seventeen studies suggested that ESPB had a lower VAS than PVB (MD = −0.15, 95% CI: −0.27 to 0.02; I2 = 87.1%; Table 2). The subgroup analysis showed that ESPB had a lower VAS than PVB in breast surgery, but there were no significant differences in thoracic surgery, abdominal surgery, and kidney surgery (Supplementary material: Figure 1).
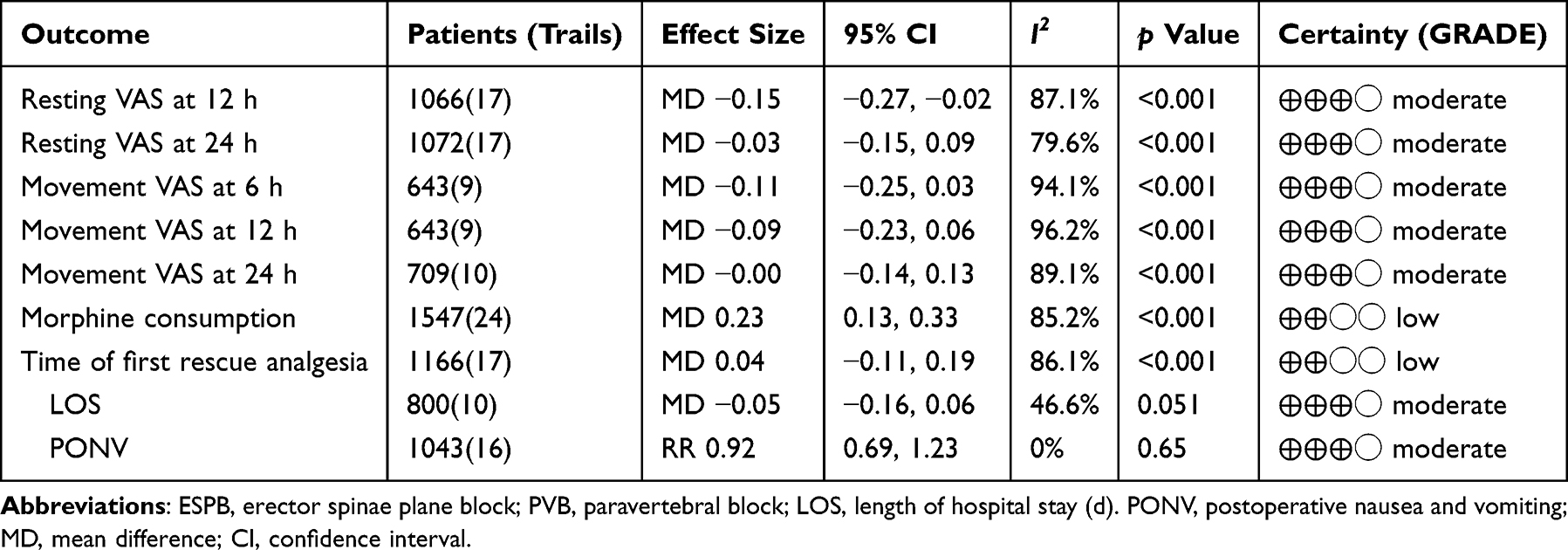 |
Table 2 Secondary Outcomes for ESPB versus PVB |
Resting VAS at 24 h
The pooled data of seventeen studies did not suggest that PVB was superior to ESPB (MD = −0.03, 95% CI: −0.15 to 0.09; I2 = 79.6%; Table 2). The subgroup analysis showed the similar effects in thoracic surgery, breast surgery, kidney surgery, and abdominal surgery (Supplementary material: Figure 2).
Movement VAS at 6 h
The pooled data of nine studies did not suggest that PVB was superior to ESPB (MD = −0.11, 95% CI: −0.25 to 0.03; I2 = 94.1%; Table 2). The subgroup analysis showed that ESPB had a lower VAS than PVB in thoracic surgery, abdominal surgery, and kidney surgery. However, PVB had a lower VAS than ESPB in breast surgery (Supplementary material: Figure 3).
Movement VAS at 12 h
The pooled data of nine studies did not suggest that PVB was superior to ESPB (MD = −0.09, 95% CI: −0.23 to 0.06; I2 = 96.2%; Table 2). The subgroup analysis showed the similar effects in thoracic surgery, breast surgery, kidney surgery, and abdominal surgery (Supplementary material: Figure 4).
Movement VAS at 24 h
The pooled data of ten studies did not suggest that PVB was superior to ESPB (MD = −0.00, 95% CI: −0.14 to 0.13; I2 = 89.1%; Table 2). The subgroup analysis showed the similar effects in thoracic surgery, breast surgery, kidney surgery, and abdominal surgery (Supplementary material: Figure 5).
Total Morphine Consumption in First 24 h (Mg)
The pooled data of twenty-four studies suggested that PVB had a lower morphine consumption than ESPB (MD = 0.23, 95% CI: 0.13 to 0.33; I2 = 85.2%; Table 2). The subgroup analysis showed the similar effects in thoracic surgery, breast surgery, and abdominal surgery. However, there was no significant difference in kidney surgery (Supplementary material: Figure 6).
Time of First Rescue Analgesia (h)
The pooled data of seventeen studies did not suggest that PVB was superior to ESPB (MD = 0.04, 95% CI: −0.11 to 0.19; I2 = 86.1%; Table 2). The subgroup analysis showed the similar effects in thoracic surgery, breast surgery, kidney surgery, and abdominal surgery (Supplementary material: Figure 7).
Length of Stay Hospital (d)
The pooled data of ten studies did not suggest that PVB was superior to ESPB (MD = −0.05, 95% CI: −0.16 to 0.06; I2 = 46.6%; Table 2). The subgroup analysis showed the similar effects in thoracic surgery, breast surgery, kidney surgery, and abdominal surgery (Supplementary material: Figure 8).
PONV
The pooled data of sixteen studies did not suggest that PVB was superior to ESPB (RR = 0.92, 95% CI: 0.69 to 1.23; I2 = 0%; Table 2). The subgroup analysis showed the similar effects in thoracic surgery, breast surgery, kidney surgery, and abdominal surgery (Supplementary material: Figure 9).
Discussion
Our meta-analysis demonstrated that PVB was not significantly better than ESPB in the primary outcomes, including resting VAS at 6 h and QoR. The similar results were shown in the secondary outcome, including other VAS, time of first rescue analgesia, LOS, and the incidence of PONV. The subgroup analysis showed similar results in thoracic surgery, breast surgery, kidney surgery, and abdominal surgery. Although there were slight differences in some outcomes, these effect sizes could not be considered as having clinical differences. Meanwhile, the degree of elevation in movement VAS markedly exceeded that of resting VAS within 12–24 hours postoperatively. This indicated a rising trend in inflammatory pain and visceral pain during this period, while nerve blockade appeared to have no inhibitory effect on these nociceptive modalities. For breast surgery, many meta-analysis also showed that there was no significant clinical difference between ESPB and PVB, and suggesting that the operation of ESPB was easier and safer.53–55 For thoracic surgery, however, the existing meta-analyses did not show consistent results. Xiong et al found the analgesic effect of PVB was better than ESPB for thoracic surgery.56 Capuano et al found ESPB was a safer technique than PVB and they had similar analgesic effects after thoracic surgery.57 Pang et al found two techniques had similar pain scores within 6 h and incidence of PONV after thoracic surgery, but PVB reduced pain scores at 12 h (SMD = 1.12; 95% CI 0.42 to 1.81) and postoperative anesthesia consumption (SMD = 1.27; 95% CI 0.30 to 2.23).58 A recent network meta-analysis suggested that ESPB was more effective and safer technique for analgesia after thoracic surgery, shortening the LOS and reducing the complications.59 These inconsistent conclusions required us to interpret the results with caution. Currently, there was limited meta-analysis on kidney surgery and abdominal surgery.
For thoracic surgery, these inconsistent conclusions could be explained by next reasons. Firstly, there were baseline differences among the populations undergoing thoracic surgery, which include variations in patients’ pain tolerance, the presence of chronic pain, and the extent of surgical resection. Secondly, there were inherent discrepancies in regional anesthesia techniques, including the types and dosages of LAs, the locations of needle insertion, the timing of drug administration (whether preoperative or postoperative), and the potential use of adjuncts. These two factors represented intrinsic limitations of our meta-analysis, as it is unlikely that the subjects and experimental designs would be identical across the two RCTs. Furthermore, there was considerable variability in postoperative analgesic protocols, including the types and dosages of baseline and rescue analgesics. This variability might be a primary contributor to the inconsistent conclusions observed and could also be a major source of heterogeneity in the results.
Patients undergoing thoracoscopic surgery may experience pain originating from thoracic incisional trauma, pleural irritation, inflammation of intercostal muscles, and manipulation of surrounding tissues.60 In the case of breast surgery, pain sources typically include surgical trauma to the breast tissue and surrounding structures.61 In laparoscopic surgery, sources of pain predominantly include incisional pain and visceral pain related to organ resection.62 Additionally, the potential neuropathic pain stemming from nerve damage during dissection and complications such as seroma or infection may contribute to prolonged pain experiences.63 The reason that ESPB and PVB can alleviate pain from the aforementioned surgeries lies in their unique mechanisms of action. The analgesic effect of ESPB is primarily attributed to the blockade of the dorsal rami of spinal nerves.64 By injecting LAs into the plane between the erector spinae muscle and the transverse processes of the vertebrae, the block eases pain by inhibiting nociceptive signals from the thoracic and abdominal structures.64 Other researches suggest that the spread of anesthetics can reach the anterior paravertebral space and the intercostal nerves.65–67 The analgesic effect of PVB is primarily attributed to the blockade of spinal nerve roots and sympathetic nerves.4 By injecting LAs into the paravertebral space, the afferent sensory pathways leading to the central nervous system are interrupted, effectively reducing nociceptive transmission.4 This mechanism not only diminishes pain perception but also provides a sympathetic block, contributing to decreased intraoperative stress responses.4
ESPB is increasingly recognized for its role in perioperative analgesia, providing effective pain relief while minimizing opioid consumption and associated side effects, which makes it an important consideration in the multimodal management of postoperative pain. LAs such as bupivacaine, ropivacaine, and levobupivacaine are commonly employed in ESPB. Typical dosages range from 0.25% to 0.5% bupivacaine, with volumes between 15 and 30 mL per side, depending on the surgical procedure and patient factors. The addition of adjuvants such as dexmedetomidine or dexamethasone can enhance the duration and quality of analgesia by prolonging the action of LAs.68 ESPB provides unilateral sensory coverage primarily across the dermatomes corresponding to the thoracic and upper abdominal areas.3 This targeted coverage helps alleviate pain from surgical sites while preserving motor function, crucial for early mobilization after surgery.3 The ESPB is generally regarded as easier to perform, often taking about 5 to 10 minutes per side.51 It has a relatively lower risk of complications, such as pneumothorax or inadvertent vascular puncture, due to the injection being executed in a more superficial plane.3 The fewer anatomical structures involved in the ESPB technique simplify the learning curve for clinicians, making it an attractive option for practitioners of varying skill levels.
The PVB typically provides unilateral sensory coverage, impacting dermatomes corresponding to the levels of blockade.2 A well-placed injection can cover multiple dermatomes, with the ability to extend from T2 to L3.69,70 A single injection of 10 mL LAs can provide sensory coverage of at least two segments.71 The PVB can be more time-consuming, often taking 10 to 15 minutes or longer, particularly for multi-level blocks.42 Identifying specific vertebral levels and accurately placing the needle in the paravertebral space requires a higher level of skill and experience. The complex anatomy of the paravertebral area, along with the need to confirm correct needle placement, can extend the procedure time. While ultrasound-guided PVB is generally considered safe, potential complications may arise, including pneumothorax, hematoma, and neural injury.2
Limitations
Our meta-analysis had several potential limitations. Firstly, as the included studies did not provide sufficient data, we did not evaluate the success rate, onset time and range of sensory blockade. Secondly, the included studies exhibited considerable variability in postoperative analgesia protocols. This increased the heterogeneity of the results and complicated direct comparisons between the PVB and ESPB. Thirdly, we made subgroup analysis for every outcome, but it was not ignored that the discrepancies in the implementation of both PVB and ESPB, including differences in the volume of LAs, the number of injection sites, and the specific techniques employed. These variations might impact the overall effectiveness and applicability of the findings. Additionally, some subgroup analyses include only a single study, so we need to interpret the results with caution. Fourthly, our study focused on short-term postoperative outcomes, such as pain relief and recovery within 24 hour. There was a lack of data on long-term analgesia and functional outcomes, which may be important for assessing the overall effectiveness of each block.
Conclusions
Our systematic review and meta-analysis suggested that ESPB and PVB provided similar effectiveness for analgesia and recovery. The ESPB was favored for its quicker execution time and greater ease of using, particularly for those less experienced in regional anesthesia. Further, high-quality, multicenter RCTs were needed to determine the long-term effectiveness of PVB and ESPB.
Funding
The study was supported by the Gansu Provincial Anesthesia and Brain Function Clinical Medical Research Center project (21JR7RA675) and the Gansu Provincial Health Industry project (GSWSKY2023-12).
Disclosure
The authors declare that they have no competing interests.
References
1. Beverly A, Kaye AD, Ljungqvist O, et al. Essential elements of multimodal analgesia in Enhanced Recovery After Surgery (ERAS) guidelines. Anesthesiol Clin. 2017;35(2):e115–e143. doi:10.1016/j.anclin.2017.01.018
2. Slinchenkova K, Lee K, Choudhury S, et al. A review of the paravertebral block: benefits and complications. Curr Pain Headache Rep. 2023;27(8):203–208. doi:10.1007/s11916-023-01118-1
3. De Cassai A, Bonvicini D, Correale C, et al. Erector spinae plane block: a systematic qualitative review. Minerva Anestesiol. 2019;85(3):308–319. doi:10.23736/S0375-9393.18.13341-4
4. Chenesseau J, Fourdrain A, Pastene B, et al. Effectiveness of surgeon-performed paravertebral block analgesia for minimally invasive thoracic surgery: a randomized clinical trial. JAMA Surg. 2023;158(12):1255–1263. doi:10.1001/jamasurg.2023.5228
5. Harkouk H, Fletcher D, Martinez V. Paravertebral block for the prevention of chronic postsurgical pain after breast cancer surgery. Reg Anesth Pain Med. 2021;46(3):251–257. doi:10.1136/rapm-2020-102040
6. Schreiber KL, Chelly JE, Lang RS, et al. Epidural versus paravertebral nerve block for postoperative analgesia in patients undergoing open liver resection: a randomized clinical trial. Reg Anesth Pain Med. 2016;41(4):460–468. doi:10.1097/AAP.0000000000000422
7. Sandeep B, Huang X, Li Y, et al. A comparison of regional anesthesia techniques in patients undergoing video-assisted thoracic surgery: a network meta-analysis. Int J Surg. 2022;105:106840. doi:10.1016/j.ijsu.2022.106840
8. Xu M, Hu J, Yan J, et al. Paravertebral block versus thoracic epidural analgesia for postthoracotomy pain relief: a meta-analysis of randomized trials. Thorac Cardiovasc Surg. 2022;70(5):413–421. doi:10.1055/s-0040-1722314
9. Heesen M, Klimek M, Rossaint R, et al. Paravertebral block and persistent postoperative pain after breast surgery: meta-analysis and trial sequential analysis. Anaesthesia. 2016;71(12):1471–1481. doi:10.1111/anae.13649
10. Oostvogels L, Weibel S, Meißner M, et al. Erector spinae plane block for postoperative pain. Cochrane Database Syst Rev. 2024;2(2):CD013763. doi:10.1002/14651858
11. Leong RW, Tan ESJ, Wong SN, et al. Efficacy of erector spinae plane block for analgesia in breast surgery: a systematic review and meta-analysis. Anaesthesia. 2021;76(3):404–413. doi:10.1111/anae.15164
12. Koo CH, Lee HT, Na HS, et al. Efficacy of erector spinae plane block for analgesia in thoracic surgery: a systematic review and meta-analysis. J Cardiothorac Vasc Anesth. 2022;36(5):1387–1395. doi:10.1053/j.jvca.2021.06.029
13. Page MJ, Moher D, Bossuyt PM, et al. PRISMA 2020 explanation and elaboration: updated guidance and exemplars for reporting systematic reviews. BMJ. 2021;372:160. doi:10.1136/bmj.n160
14. Higgins JP, Altman DG, Gøtzsche PC, et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011;343:5928. doi:10.1136/bmj.d5928
15. Luo D, Wan X, Liu J, et al. Optimally estimating the sample mean from the sample size, median, mid-range, and/or mid-quartile range. Stat Methods Med Res. 2018;27(6):1785–1805. doi:10.1177/0962280216669183
16. Wan X, Liu J, et al. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med Res Methodol. 2014;14:135. doi:10.1186/1471-2288-14-135
17. Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. 2002;21(11):1539–1558. doi:10.1002/sim.1186
18. Begg CB, Mazumdar M. Operating characteristics of a rank correlation test for publication bias. Biometrics. 1994;50(4):1088–1101.
19. Egger M, Davey Smith G, Schneider M, et al. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315(7109):629–634. doi:10.1136/bmj.315.7109.629
20. Zhao H, Xin L, Feng Y. The effect of preoperative erector spinae plane vs. paravertebral blocks on patient-controlled oxycodone consumption after video-assisted thoracic surgery: a prospective randomized, blinded, non-inferiority study. J Clin Anesth. 2020;62:109737. doi:10.1016/j.jclinane.2020.109737
21. Turhan Ö, Sivrikoz N, Sungur Z, et al. Thoracic paravertebral block achieves better pain control than erector spinae plane block and intercostal nerve block in thoracoscopic surgery: a randomized study. J Cardiothorac Vasc Anesth. 2021;35(10):2920–2927. doi:10.1053/j.jvca.2020.11.034
22. Chen N, Qiao Q, Chen R, et al. The effect of ultrasound-guided intercostal nerve block, single-injection erector spinae plane block and multiple-injection paravertebral block on postoperative analgesia in thoracoscopic surgery: a randomized, double-blinded, clinical trial. J Clin Anesth. 2020;59:106–111. doi:10.1016/j.jclinane.2019.07.002
23. Zhang L, Hu Y, Liu H, et al. Analgesic efficacy of combined thoracic paravertebral block and erector spinae plane block for video-assisted thoracic surgery: a prospective randomized clinical trial. Med Sci Monit. 2023;29:e940247. doi:10.12659/MSM.940247
24. Zengin M, Alagöz A, Sazak H, et al. Comparison of efficacy of erector spinae plane block, thoracic paravertebral block, and erector spinae plane block and thoracic paravertebral block combination for acute pain after video-assisted thoracoscopic surgery: a randomized controlled study. Minerva Anestesiol. 2023;89(3):138–148. doi:10.23736/S0375-9393.22.16639-3
25. Fu Z, Zhang Y, Zhou Y, et al. A comparison of paravertebral block, erector spinae plane block and the combination of erector spinae plane block and paravertebral block for post-operative analgesia after video-assisted thoracoscopic surgery: a randomised controlled trial. J Minim Access Surg. 2022;18(2):241–247. doi:10.4103/jmas.JMAS_277_20
26. Zhang JW, Feng XY, Yang J, et al. Ultrasound-guided single thoracic paravertebral nerve block and erector spinae plane block for perioperative analgesia in thoracoscopic pulmonary lobectomy: a randomized controlled trial. Insights Imaging. 2022;13(1):16. doi:10.1186/s13244-021-01151-x
27. Zhu Y, Yang Y, Zhang Q, et al. Comparison of ultrasound-guided single-injection erector spinae plane block, retrolaminar block, and paravertebral block for postoperative analgesia in single-incision video-assisted thoracoscopic surgery: a 3-arm, double-blind, randomized controlled noninferiority trial. Clin J Pain. 2025;41(1):e1259. doi:10.1097/AJP.0000000000001259
28. Duran M, Kuş A, Aksu C, et al. Comparison of postoperative opioid consumption of paravertebral block and erector spinae plane block after thoracotomy: a randomized controlled trial. Cureus. 2024;16(5):e59459. doi:10.7759/cureus.59459
29. Fang B, Wang Z, Huang X. Ultrasound-guided preoperative single-dose erector spinae plane block provides comparable analgesia to thoracic paravertebral block following thoracotomy: a single center randomized controlled double-blind study. Ann Transl Med. 2019;7(8):174. doi:10.21037/atm.2019.03.53
30. Das S, Saha D, Sen C. Comparison among ultrasound-guided thoracic paravertebral block, erector spinae plane block and serratus anterior plane block for analgesia in thoracotomy for lung surgery. J Cardiothorac Vasc Anesth. 2022;36(12):4386–4392. doi:10.1053/j.jvca.2022.08.022
31. Xu M, Zhang G, Wang R, et al. Erector spinae plane block provided comparable analgesia as thoracic paravertebral block post pediatric nuss procedure for pectus excavatum: a randomized controlled trial. Pain Physician. 2024;27(7):425–433.
32. Jayakrishnan S, Dua A, Kumar A. Comparison of fascial plane blocks (ESPB vs. TPVB) for pain relief following modified radical mastectomy. J Anaesthesiol Clin Pharmacol. 2024;40(3):410–415. doi:10.4103/joacp.joacp_90_23
33. Agarwal S, Bharati SJ, Bhatnagar S, et al. The comparison of the efficacy of ultrasound-guided paravertebral block versus erector spinae plane block for postoperative analgesia in modified radical mastectomy: a randomized controlled trial. Saudi J Anaesth. 2021;15(2):137–143. doi:10.4103/sja.sja_990_20
34. El Ghamry MR, Amer AF. Role of erector spinae plane block versus paravertebral block in pain control after modified radical mastectomy. A prospective randomised trial. Indian J Anaesth. 2019;63(12):1008–1014. doi:10.4103/ija.IJA_310_19
35. Sivrikoz N, Turhan Ö, Ali A, et al. Paravertebral block versus erector spinae plane block for analgesia in modified radical mastectomy: a randomized, prospective, double-blind study. Minerva Anestesiol. 2022;88(12):1003–1012. doi:10.23736/S0375-9393.22.16625-3
36. Elewa AM, Faisal M, Sjöberg F, et al. Comparison between erector spinae plane block and paravertebral block regarding postoperative analgesic consumption following breast surgery: a randomized controlled study. BMC Anesthesiol. 2022;22(1):189. doi:10.1186/s12871-022-01724-3
37. Moustafa MA, Alabd AS, Ahmed AMM, et al. Erector spinae versus paravertebral plane blocks in modified radical mastectomy: randomised comparative study of the technique success rate among novice anaesthesiologists. Indian J Anaesth. 2020;64(1):49–54. doi:10.4103/ija.IJA_536_19
38. Sayed JA, Hamed R, Abdelraouf AM, et al. A comparative study of respiratory effects of erector spinae plane block versus paravertebral plane block for women undergoing modified radical mastectomy. BMC Anesthesiol. 2024;24(1):262. doi:10.1186/s12871-024-02632-4
39. Amr SA, Othman AH, Ahmed EH, et al. Comparison between ultrasound guided erector spinae plane block and paravertebral block on acute and chronic post mastectomy pain after modified radical mastectomy: randomized controlled trial. BMC Anesthesiol. 2024;24(1):420. doi:10.1186/s12871-024-02810-4
40. Gürkan Y, Aksu C, Kuş A, et al. Erector spinae plane block and thoracic paravertebral block for breast surgery compared to IV-morphine: a randomized controlled trial. J Clin Anesth. 2020;59:84–88. doi:10.1016/j.jclinane.2019.06.036
41. Santonastaso DP, de Chiara A, Righetti R, et al. Efficacy of bi-level erector spinae plane block versus bi-level thoracic paravertebral block for postoperative analgesia in modified radical mastectomy: a prospective randomized comparative study. BMC Anesthesiol. 2023;23(1):209. doi:10.1186/s12871-023-02157-2
42. Wittayapairoj A, Sinthuchao N, Somintara O, et al. A randomized double-blind controlled study comparing erector spinae plane block and thoracic paravertebral block for postoperative analgesia after breast surgery. Anesth Pain Med. 2022;17(4):445–453. doi:10.17085/apm.22157
43. But M, Wernicki K, Zieliński J, et al. A comparison of the effectiveness of the serratus anterior plane block and erector spinae plane block to that of the paravertebral block in the surgical treatment of breast cancer-a randomized, prospective, single-blinded study. J Clin Med. 2024;13(16):4836. doi:10.3390/jcm13164836
44. Hu Y, Li M, Li J, et al. Effects of ultrasound-guided erector spinae plane block on the immune function and postoperative recovery of patients undergoing radical mastectomy. Gland Surg. 2021;10(10):2901–2909. doi:10.21037/gs-21-603
45. Swisher MW, Wallace AM, Sztain JF, et al. Erector spinae plane versus paravertebral nerve blocks for postoperative analgesia after breast surgery: a randomized clinical trial. Reg Anesth Pain Med. 2020;45(4):260–266. doi:10.1136/rapm-2019-101013
46. Yılmaz ET, Gülmez DD, Apan A, et al. A novel comparison of erector spinae plane block and paravertebral block in laparoscopic cholecystectomy. Rev Assoc Med Bras. 2024;70(3):e20231457. doi:10.1590/1806-9282.20231457
47. Yang G, Wang P, Yin Y, et al. Erector spinae plane block versus paravertebral block on postoperative quality of recovery in obese patients undergoing laparoscopic sleeve gastrectomy: a randomized controlled trial. PeerJ. 2024;12:e17431. doi:10.7717/peerj.17431
48. Xu ZZ, Li X, Chen BL, et al. A randomised controlled trial of the non-inferiority of erector spinae plane block vs. thoracic paravertebral block for laparoscopic nephro-ureterectomy. Anaesthesia. 2023;78(4):442–448. doi:10.1111/anae.15959
49. Fan Q, Liu H, Li Y, et al. Comparison of ultrasound-guided erector spinae plane block and thoracic paravertebral block for postoperative analgesia after laparoscopic nephrectomy: a randomized controlled non-inferiority clinical trial. Minerva Anestesiol. 2023;89(6):520–528. doi:10.23736/S0375-9393.22.16794-5
50. Gs K, Ramegowda S, Chandra M, et al. Comparison of the efficacy between ultrasound-guided paravertebral block and erector spinae block for postoperative analgesia in percutaneous nephrolithotomy using levobupivacaine: a prospective and randomized study. Cureus. 2024;16(8):e67401. doi:10.7759/cureus.67401
51. Khot PP, Desai SN, Bale SP, et al. Comparison of ultrasound-guided paravertebral block versus erector spinae plane block for postoperative analgesia after percutaneous nephrolithotomy - A randomised, double-blind, controlled study. Indian J Anaesth. 2023;67(12):1110–1115. doi:10.4103/ija.ija_355_23
52. Elsayed AA, Algyar MF, Arafa SK. Comparison of the analgesic efficacy of erector spinae plane block, paravertebral block and quadratus lumborum block for pelvi-ureteric surgeries: a randomized double-blind, noninferiority trial. Pain Physician. 2024;27(10):E1055–E1063.
53. Chen W, Zhou X, Li H, et al. Analgesic effectiveness of preoperative ultrasound-guided erector spinae plane block versus paravertebral nerve block for breast surgery: a systematic review and meta-analysis of four randomized controlled trials. Pain Pract. 2023;23(5):511–522. doi:10.1111/papr.13208
54. Weng WT, Wang CJ, Li CY, et al. Erector Spinae Plane Block similar to paravertebral block for perioperative pain control in breast surgery: a meta-analysis study. Pain Physician. 2021;24(3):203–213.
55. Wong HY, Pilling R, Young BWM, et al. Comparison of local and regional anesthesia modalities in breast surgery: a systematic review and network meta-analysis. J Clin Anesth. 2021;72:110274. doi:10.1016/j.jclinane.2021.110274
56. Xiong C, Han C, Zhao D, et al. Postoperative analgesic effects of paravertebral block versus erector spinae plane block for thoracic and breast surgery: a meta-analysis. PLoS One. 2021;16(8):e0256611. doi:10.1371/journal.pone.0256611
57. Capuano P, Hileman BA, Martucci G, et al. Erector spinae plane block versus paravertebral block for postoperative pain management in thoracic surgery: a systematic review and meta-analysis. Minerva Anestesiol. 2023;89(11):1042–1050. doi:10.23736/S0375-9393.23.17510-9
58. Pang J, You J, Chen Y, et al. Comparison of erector spinae plane block with paravertebral block for thoracoscopic surgery: a meta-analysis of randomized controlled trials. J Cardiothorac Surg. 2023;18(1):300. doi:10.1186/s13019-023-02343-w
59. Li J, Sun Q, Zong L, et al. Relative efficacy and safety of several regional analgesic techniques following thoracic surgery: a network meta-analysis of randomized controlled trials. Int J Surg. 2023;109(8):2404–2413. doi:10.1097/JS9.0000000000000167
60. Magoon R, Choudhary N. The nitty-gritty of pain research in thoracoscopic surgery. J Anesth. 2023;37(6):976–977. doi:10.1007/s00540-023-03249-6
61. Subedi A. Postsurgical events and persistent pain after breast cancer surgery. Anaesthesia. 2023;78(7):914. doi:10.1111/anae.15993
62. Macías AA, Finneran JJ. Regional anesthesia techniques for pain management for laparoscopic surgery: a review of the current literature. Curr Pain Headache Rep. 2022;26(1):33–42. doi:10.1007/s11916-022-01000-6
63. Baron R, Binder A, Wasner G. Neuropathic pain: diagnosis, pathophysiological mechanisms, and treatment. Lancet Neurol. 2010;9(8):807–819. doi:10.1016/S1474-4422(10)70143-5
64. Chin KJ, El-Boghdadly K. Mechanisms of action of the erector spinae plane (ESP) block: a narrative review. Can J Anaesth. 2021;68(3):387–408. doi:10.1007/s12630-020-01875-2
65. Rocha-Romero A, Fajardo-Perez M. Function of the sympathetic supply in the erector spinae plane block. Can J Anaesth. 2021;68(6):937–938. doi:10.1007/s12630-021-01960-0
66. Shan T, Zhang X, Zhao Z, et al. Spread of local anaesthetic after erector spinae plane block: a randomised, three-dimensional reconstruction, imaging study. Br J Anaesth. 2025;134(3):830–838. doi:10.1016/j.bja.2024.10.046
67. Bonvicini D, Boscolo-Berto R, De Cassai A, et al. Anatomical basis of erector spinae plane block: a dissection and histotopographic pilot study. J Anesth. 2021;35(1):102–111. doi:10.1007/s00540-020-02881-w
68. Yang J, Zhao M, Zhang XR, et al. Ropivacaine with dexmedetomidine or dexamethasone in a thoracic paravertebral nerve block combined with an erector spinae plane block for thoracoscopic lobectomy analgesia: a randomized controlled trial. Drug Des Devel Ther. 2022;16:1561–1571. doi:10.2147/DDDT.S366428
69. Xie PC, Zhang NN, Wu YM, et al. Comparison between ultrasound-guided paravertebral nerve block and subarachnoid block for elderly male patients under unilateral-opened inguinal hernia repair operation: a randomised controlled trial. Int J Surg. 2019;68:35–39. doi:10.1016/j.ijsu.2019.06.004
70. Kim YH, Kim SY, Lee YJ, et al. A prospective, randomized cross-over trial of T2 paravertebral block as a sympathetic block in complex regional pain syndrome. Pain Physician. 2019;22(5):E417–E424.
71. Okajima H, Tanaka O, Ushio M, et al. Ultrasound-guided continuous thoracic paravertebral block provides comparable analgesia and fewer episodes of hypotension than continuous epidural block after lung surgery. J Anesth. 2015;29(3):373–378. doi:10.1007/s00540-014-1947-y
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Neutrophil-to-Lymphocyte Ratio as an Indicator of Opioid-Induced Immunosuppression After Thoracoscopic Surgery: A Randomized Controlled Trial
Chen Q, Liang J, Liang L, Liao Z, Yang B, Qi J
Journal of Pain Research 2022, 15:1855-1862
Published Date: 30 June 2022
Ultrasound Guided Continuous Erector Spinae Plane Block versus Patient Controlled Analgesia in Open Nephrectomy for Renal Malignancies: A Randomized Controlled Study
Abdelgalil AS, Ahmed AM, Gamal RM, Elshal MM, Bakeer AH, Shaker EH
Journal of Pain Research 2022, 15:3093-3102
Published Date: 30 September 2022
Efficacy and Safety of Erector Spinae Plane Block for Perioperative Pain Management in Lumbar Spinal Surgery: A Systematic Review and Meta-Analysis of Randomized Controlled Trials
Fu MY, Hao J, Ye LH, Jiang W, Lv YW, Shen JL, Fu T
Journal of Pain Research 2023, 16:1453-1475
Published Date: 3 May 2023
Efficacy of Acupuncture Assisted Anesthesia in Laparoscopic Cholecystectomy: A Systematic Review and Meta-Analysis
Lv H, Xu J, Bian Z, Lu Y, Li X, Jiang Y, Fang J, Liu Y
Journal of Pain Research 2025, 18:5567-5585
Published Date: 25 October 2025
Pain Management Approaches for Robotic-Assisted Thoracic Surgery: A Retrospective Analysis
Semyonov MA, Shmueli M, Smirnov A, Dubilet M, Refaely Y, Ruderman LN, Maron P, Binyamin Y, Brotfain E, Zlotnik A, Frank D
Journal of Pain Research 2025, 18:6085-6093
Published Date: 14 November 2025