Back to Journals » Journal of Pain Research » Volume 18
Efficacy of Acupuncture Assisted Anesthesia in Laparoscopic Cholecystectomy: A Systematic Review and Meta-Analysis
Authors Lv H, Xu J, Bian Z, Lu Y, Li X, Jiang Y, Fang J, Liu Y
Received 18 June 2025
Accepted for publication 17 October 2025
Published 25 October 2025 Volume 2025:18 Pages 5567—5585
DOI https://doi.org/10.2147/JPR.S547740
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Houman Danesh
Hengfeng Lv,1,* Jiayuan Xu,2,* Zhiyuan Bian,1 Yongyuan Lu,1 Xingzhen Li,1 Yurong Jiang,1 Jianqiao Fang,1 Yingjun Liu1
1The Third School of Clinical Medicine, Zhejiang Chinese Medical University, Hangzhou, Zhejiang, People’s Republic of China; 2Department of Nursing, The First Affiliated Hospital of Zhejiang Chinese Medical University, Hangzhou, Zhejiang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yingjun Liu; Jianqiao Fang, The Third School of Clinical Medicine, Zhejiang Chinese Medical University, 548 Binwen Road, Hangzhou, Zhejiang, 310053, People’s Republic of China, Email [email protected]; [email protected]
Purpose: Acupuncture assisted anesthesia (AAA) has received increasing attention in the procedure of laparoscopic cholecystectomy. Therefore, we conducted a systematic review and meta-analysis assessing the potential advantages and safety of AAA in patients undergoing laparoscopic cholecystectomy.
Methods: Randomized controlled trials (RCTs) on AAA in the procedure of laparoscopic cholecystectomy from 8 online databases were retrieved. Review Manager 5.3 software was used to merge and statistically analyze the extracted data, RoB 2.0 was used to assess the risk of bias, and GRADEprofiler was used to assess the quality of evidence.
Results: Twenty-three RCTs were included, with a total of 2031 participants. The meta-analysis results indicated that compared with the control group, AAA reduced postoperative pain intensity (P < 0.05) and the incidence of postoperative nausea and vomiting (P < 0.05), and shortened the time to first flatus (P = 0.002). AAA also reduced postoperative IL-6 (P = 0.01) and TNF-alpha (P < 0.00001) levels compared with the control group. However, no significant difference on IL-10 level was found (P = 0.09) between AAA and control group. Furthermore, AAA also reduced the use of intraoperative anesthetics (P < 0.05) and postoperative analgesics (P < 0.00001) compared to the control group.
Conclusion: This study demonstrates that AAA in the procedure of laparoscopic cholecystectomy has potential advantages on alleviating postoperative pain and gastrointestinal symptoms, reducing pro-inflammatory cytokines levels, and lowering the dosage of intraoperative and postoperative analgesics. This highlights the potential benefits of applying AAA in laparoscopic cholecystectomy to alleviate patient suffering.
Protocol and Registration: PROSPERO registration number: CRD42024549645.
Keywords: anesthesia, acupuncture, analgesia, safety, systematic review, meta-analysis
Introduction
In recent years, changes in lifestyle and dietary habits have led to a significant increase in the prevalence of gallbladder-related conditions, including gallstones, abdominal adhesions, acute cholecystitis, and Mirizzi syndrome.1 Laparoscopic cholecystectomy continues to be a primary clinical intervention for a range of benign gallbladder diseases, with an estimated 750,000 procedures conducted annually in the United States alone.2 Despite its widespread use, the procedure’s inherent challenges-such as the creation of pneumoperitoneum, anesthetic administration, and surgical trauma-predispose patients to a range of postoperative complications. These include incisional pain, nausea and vomiting, hemodynamic instability, and the risk of infection, all of which can impede recovery and result in extended hospitalization.3,4 Consequently, there is a pressing need to identify an optimal adjunctive anesthetic approach that mitigates perioperative risks and adverse events.
Acupuncture involves the insertion of filiform needles into specific points on the patient’s body, known as acupoints, at calculated angles and through deliberate manipulations with a minimally invasive approach.5 A literature review showed that acupuncture offers potential advantages in perioperative period, such as decreased incidence of postoperative gastrointestinal symptoms, and decreased postoperative analgesic use.6 In addition, extensive studies have reported the positive effects of different types of acupuncture and related therapies, such as electroacupuncture (EA) and transcutaneous electrical acupoint stimulation (TEAS), in the management of postoperative pain and gastrointestinal disturbances.7–9 In China, acupuncture assisted anesthesia (AAA) has been used in surgical procedures since the 1950s. And several potential mechanisms have been revealed, such as promoting the release of endogenous opioid peptides in the central nervous system, and inhibiting the secretion of pro-inflammatory cytokines in peripheral blood, thereby reducing the required dosage of analgesic medications while providing effective postoperative analgesia.10,11 This application has been considered as a significant milestone in the development of modern acupuncture practices and represents a notable advancement in the field.12,13
Previous clinical studies showed that the use of AAA in surgical operations can reduce the dose of intraoperative anesthetic and postoperative analgesics, as well as decrease the occurrence and severity of postoperative complications.14–16 In addition, acupuncture is considered as a minimal invasive treatment and is highly safe.17 Currently, the AAA technique has been applied in laparoscopic cholecystectomy. However, due to small sample sizes and the varying measurement indicators across different studies, its clinical value and safety are still controversial.18 Therefore, this study aim to summarize current evidence on the use of AAA in laparoscopic cholecystectomy.
Methods
The research protocol is retrievable from the PROSPERO International Systematic Review Database (https://www.crd.york.ac.uk/PROSPERO/view/CRD42024549645). The reporting of this study aligned with the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA)19 statement.
Search Strategies and Data Sources
A literature search was conducted to identify randomized controlled trials (RCTs) examining the efficacy and safety of AAA in improving postoperative adverse outcomes following laparoscopic cholecystectomy. The search encompassed major databases, including PubMed, Web of Science, Embase, Cochrane Central, CNKI, VIP, Wanfang Database, and Sinomed. The search period spanned from the inception of the databases to March 26, 2024. Clinical Trial Registries (ClinicalTrials.gov), International Clinical Trials registry Platform (trialsearch.who.int), and Chinese clinical trial registry (chictr.org.cn) were also included in the search to ensure the inclusion of ongoing or unpublished studies. The search strategy on 8 online databases is given in Supplementary Table S1. To identify additional studies, the reference lists of published systematic reviews and included RCTs were screened. No restrictions were placed on language, sample size, publication date, or country.
Inclusion and Exclusion Criteria
The following PICOS criteria were used to screen eligible trials: (1) Participants: Adults undergoing laparoscopic cholecystectomy, regardless of surgical technique; (2) Intervention: The use of AAA combined with drug anesthetics; (3) Comparison: standard drug anesthetics, with or without sham acupuncture; (4) The primary outcome was postoperative pain intensity measured using a visual analogue scale (VAS), and secondary outcomes were postoperative nausea and vomiting (PONV), time to first flatus (TFF), pro- and anti- inflammatory cytokines, intraoperative anesthesia use, and postoperative analgesic use; (5) Study Design: Only RCTs were included. (6) We excluded cross-over trials, quasi-RCTs, cluster RCTs or any other types of non-RCTs.
Articles Selection and Data Extraction
Two researchers (H.F. Lv and J.Y. Xu) independently screened the eligible literature according to the inclusion and exclusion criteria. Then, two researchers extracted the data and cross-checked it. Disagreements between the researchers were resolved by consulting a third reviewer (Z.Y. Bian) to reach a consensus. After the retrieved literature was imported into NoteExpress software for automatic duplicate screening, the title and abstract of each article were manually examined. After excluding articles that did not meet the inclusion criteria, the full text of each remaining article was independently screened to determine whether it was eligible for inclusion in the meta-analysis. The data extraction process utilized a standardized data extraction form to collect the required information. The extracted data included: (1) Characteristics of studies: author, country, year of publication, age and sex of participants, sample size, acupoint, EA waveform, and time of intervention; (2) Outcomes: VAS scores, PONV, TFF, pro- and anti- inflammatory cytokines, intraoperative anesthesia use, and postoperative analgesic use; (3) Information related to the risk of bias assessment and quality assessment.
For dichotomous variables such as the incidence of postoperative nausea and vomiting, the total number of cases in the observation and control groups, as well as the number of events, were extracted. For continuous variables like postoperative VAS scores, time to first flatus, pro/anti-inflammatory factors, and intra/postoperative drug usage, we extracted the mean, standard deviation, and total case count. During data extraction, when a study’s observation or control group comprised two or more subgroups, subgroup data were pooled using methods from the Cochrane Handbook for Systematic Reviews of Interventions (version 6.5).20 For dichotomous variables, data synthesis involved summing the sample sizes and event counts from each subgroup. For continuous variables, data synthesis involved using the equations


to merge two intervention groups into one. Combining multiple interventions for calculation was independently completed by two reviewers (H.F. Lv and J.Y. Xu), and inconsistencies were checked against the original text.
Quality of Included Studies
The methodological soundness of the enrolled studies was subjected to a rigorous dual-review process, employing the Cochrane Risk of Bias tool (RoB 2.0) tool as the standard for evaluation. These included the authenticity of the randomization process, any divergences from the planned interventions, the comprehensiveness of the reported outcome data, the precision of outcome assessments, the potential bias in the selection of reported findings, and the general susceptibility to bias. When disagreements arose between the two reviewers’ assessments (H.F. Lv and J.Y. Xu), the differences were resolved by reaching a consensus with a third researcher (Z.Y. Bian).
Certainty of Evidence
This study employed the Grades of Recommendation, Assessment, Development, and Evaluation (GRADE) approach to assess the overall quality of evidence for the outcomes. The GRADE system examines five domains: risk of bias, inconsistency, indirectness, imprecision, and potential publication bias. These domains collectively contribute to the evaluation of the quality of evidence, which is categorized into four levels: high, moderate, low, and very low. To ensure objectivity and reliability, two researchers (H.F. Lv and X.Z. Li) conducted the assessment independently, with a third researcher (Z.Y. Bian) reviewing the process. Any disagreements were resolved through discussions with the corresponding author (J.Q. Fang).
Data Analysis
The meta-analysis was conducted using Review Manager (RevMan) 5.3 software. We categorized variables as risk ratios (RR) with a 95% confidence interval (CI). For continuous variables with consistent units, the mean difference (MD) with a 95% CI was used. In cases where units varied, the standardized mean difference (SMD) was employed. To avoid sample size overlap in studies with multiple intervention/control groups, we implemented a strategy of subdividing participants into distinct subgroups for comparison, as previously reported.21,22 This method ensures retention of means and standard deviations (SD) for continuous variables, while for categorical outcomes, the number of events and total number of participants were divided. We assessed the heterogeneity among the included studies by using the I² value and chi-square test. I² ≤ 50% and P > 0.1 indicated no significant heterogeneity, in which case the fixed-effects model was used. In contrast, I² > 50% and P ≤ 0.1 indicated significant heterogeneity. Subgroup analysis and sensitivity analysis were carried out for the primary outcomes. Sensitivity analyses were conducted by excluding one study at a time and pooling the remaining studies. Additionally, publication bias was evaluated using funnel plots. P < 0.05 was considered statistically significant.
Results
Search Results
A total of 767 studies were identified initially from 8 electronic databases and 3 clinical trial registries. After the removal of duplicates, 402 unique studies were assessed based on their titles and abstracts, and 308 were excluded because they did not meet the inclusion criteria. Finally, 23 RCTs were included after a full-text review. The detailed screening process was illustrated in Figure 1. Cumulatively, the analysis encompassed 23 randomized controlled trials conducted in China from 2008 to 2024, involving a total of 2,031 patients.23–45
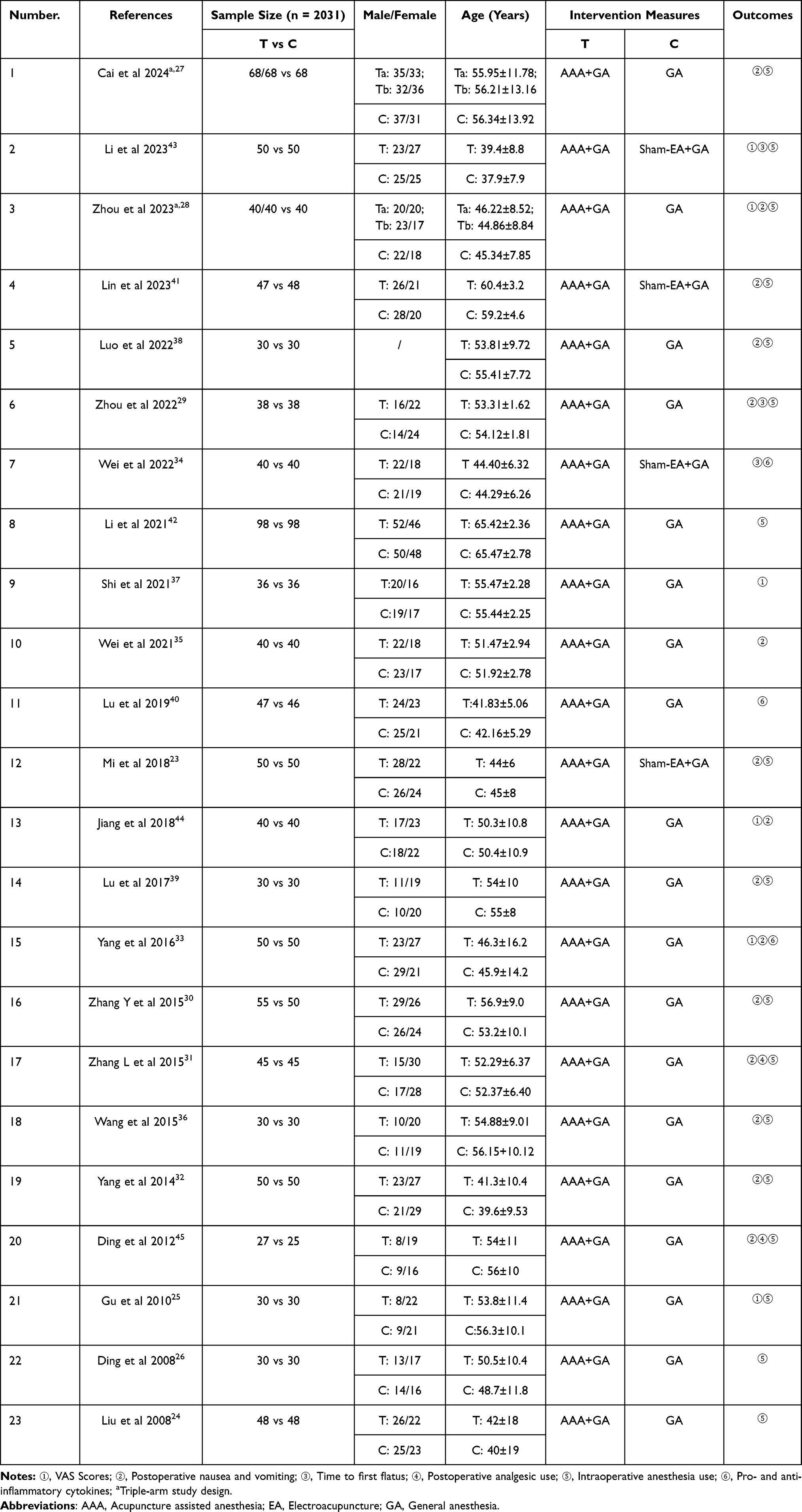 |
Table 1 Characteristics of Studies |
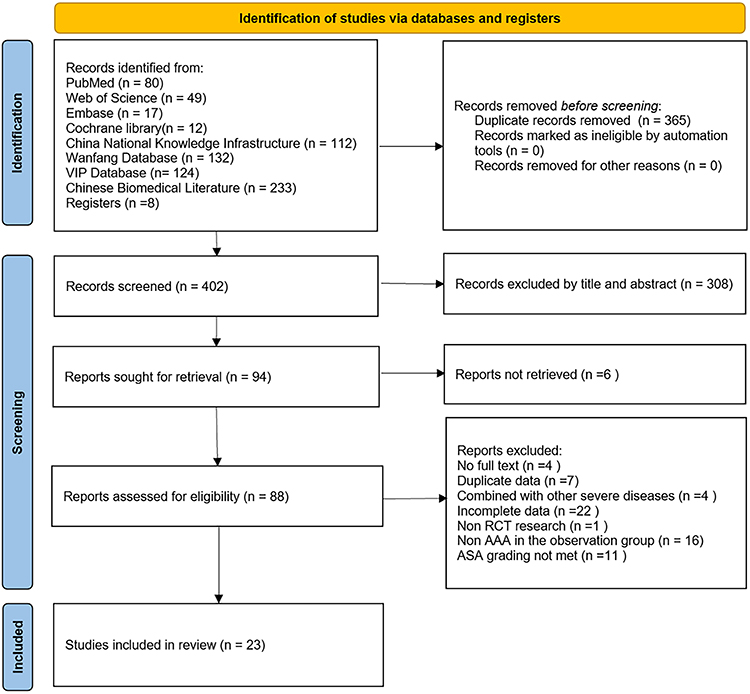 |
Figure 1 Flowchart for inclusion and exclusion of studies. |
Characteristics of Studies
The demographic and methodological features of the studies encompassed within this meta-analysis are delineated in Table 1. The fundamental patient characteristics, namely age and gender, were meticulously documented across the 23 studies. However, one study was noted to lack gender-specific data for both the intervention and control groups. Each of the 23 rigorously selected RCTs pertained to laparoscopic cholecystectomy procedures. The AAA group’s participant count varied from 27 to 98, while the control group’s size spanned from 25 to 98 individuals. Within these 23 trials, two featured a three-arm design.27,28
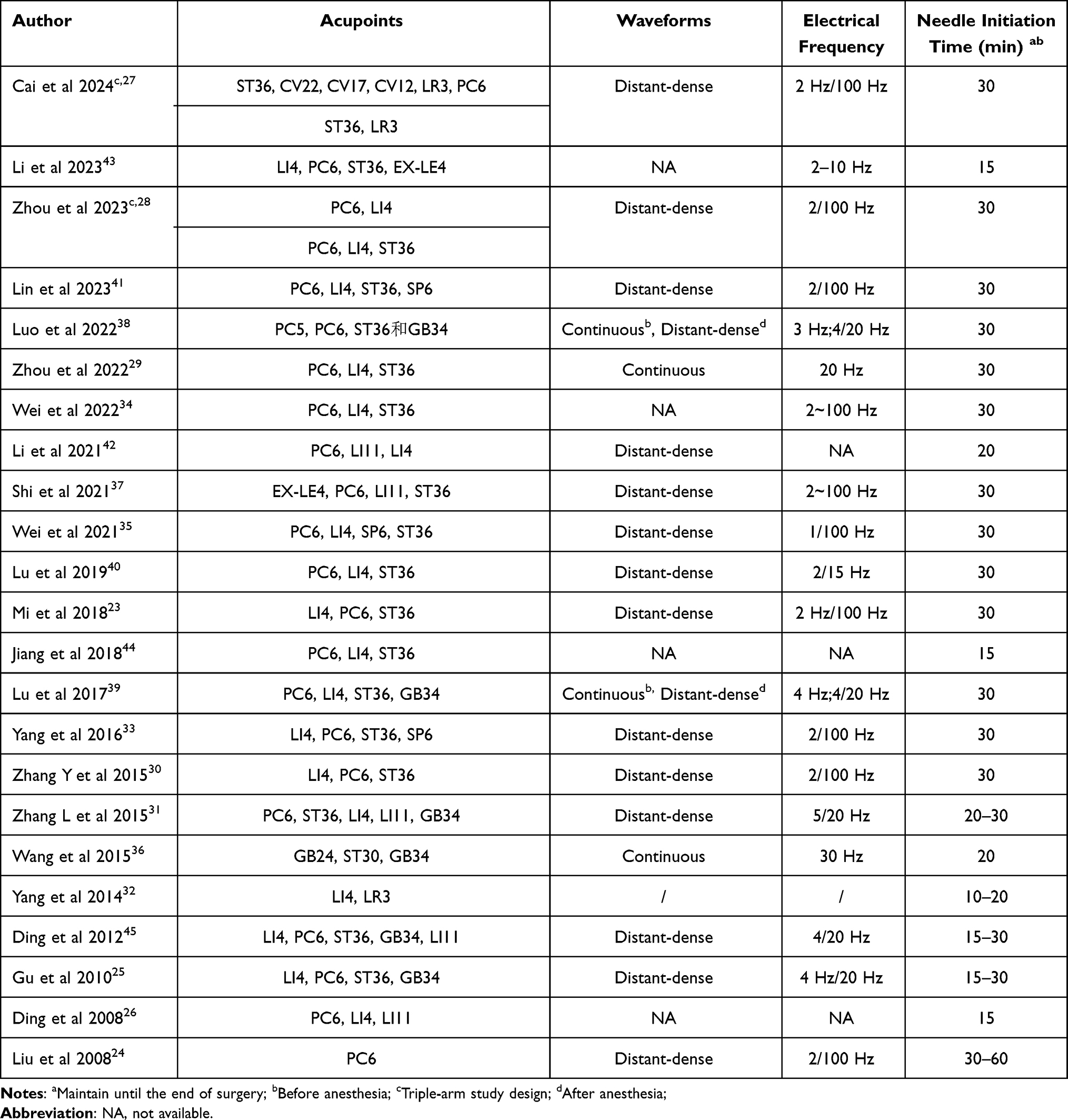 |
Table 2 Details of Acupoints |
Table 2 delineates a more nuanced view of the acupoints utilized across the studies under review. Within this corpus of 23 studies, a predominant trend emerges: 21 studies targeted the PC6 acupoint for intervention.23–31,33–35,37–45 Furthermore, a significant subset of 18 studies opted for a dual-acupoint approach, employing both ST36 and PC6.23,25,27–31,33–35,37–41,43–45 Beyond these primary foci, a constellation of additional acupoints was invoked in several studies, encompassing CV22, CV17, CV12, LR3, LI4, LI11, EX-LE4, SP6, PC5, and GB34. In the 23 studies on AAA, 22 used EA. For waveform selection of EA, the distant-dense waveform was the most frequently used, which was reported in 14 studies.23–25,27,28,30,31,33,35,37,40–42,45 This was contrasted by 2 studies that utilized a continuous wave and another 2 that initiated with a continuous wave before transitioning to a distant-dense pattern.29,36,38,39 Notably, 4 studies omitted details regarding their waveform selection.26,34,43,44 As for the temporal aspect of acupuncture intervention, a uniform approach was observed across all 23 studies, with interventions being initiated prior to surgical procedures. A specific temporal marker was identified in 13 studies, which initiated their intervention 30 minutes prior to anesthesia.23,27–30,33–35,37–41 While the remaining studies exhibited variability in the commencement of their interventions, a common thread was the continuation of acupuncture until the conclusion of surgery.
Risk of Bias Assessment
The synthesis of the risk of bias assessment is presented herein. As shown in Figure 2, among the 23 studies scrutinized, all were identified to warrant “concerns” regarding the integrity of the randomization process, which is a critical component of study design. In terms of the risk of bias pertaining to the measurement of outcomes, two studies were flagged for raising “some concerns”, suggesting potential discrepancies in the accuracy or consistency of outcome assessments.28,39 With respect to the risk of bias associated with the selection of reported results, four studies were deemed to evoke “some concerns”, implying that there may be a selective reporting of findings which could skew the overall conclusions drawn from these studies.25,35,38,42 Upon evaluating the collective risk of bias across all studies, it was observed that “some concerns” were present in all studies, highlighting methodological limitations or issues that might compromise the reliability and validity of the results.23–45
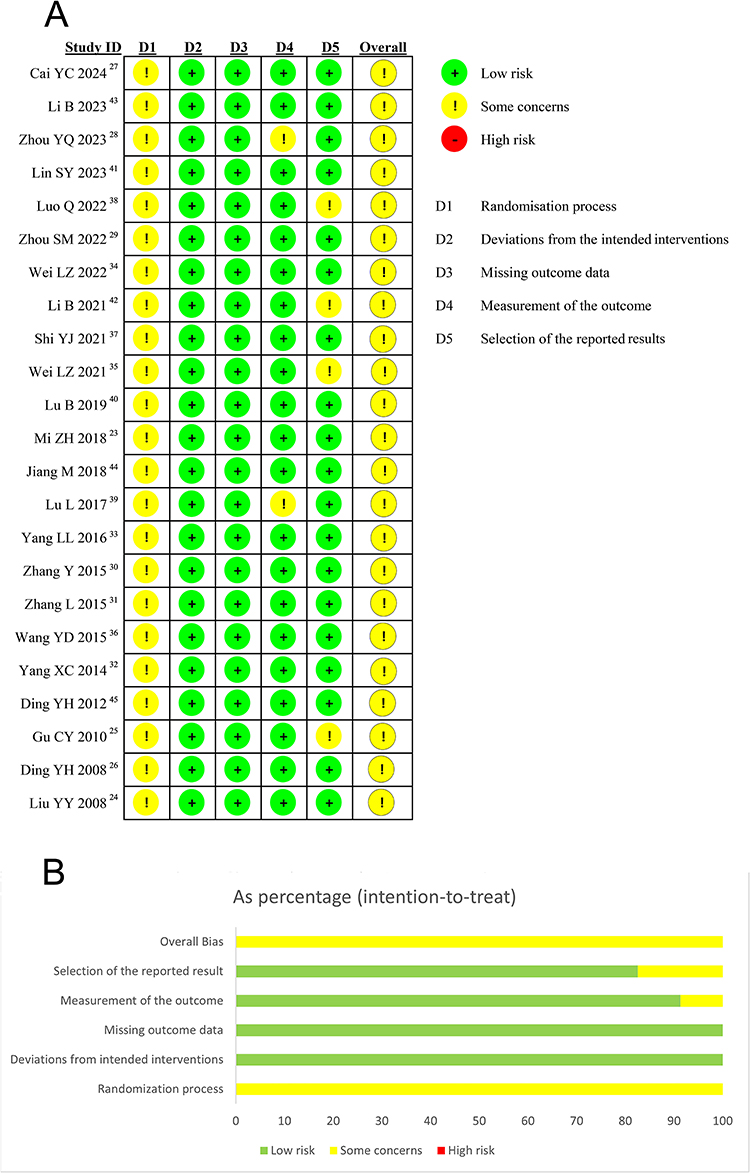 |
Figure 2 The risks of bias in (A) individual studies and (B) a summary. |
Primary and Secondary Outcomes
Primary Outcomes: Postoperative VAS Scores
In the analysis of VAS scores, the aggregation of pertinent subgroup data was focused at three critical postoperative time points (Figure 3): postoperative 2 hours, postoperative 12 hours, and postoperative 24 hours. The VAS scores at postoperative 2 hours encompassed data from a total of 160 participants, evenly divided between the AAA group and the control group. The meta-analysis demonstrated that patients in the AAA group experienced significantly reduced VAS scores at 2 hours compared to those receiving only standard care (MD: −0.75, 95% CI: −1.07 to −0.44, P < 0.00001, I² = 0%). Sensitivity analysis confirmed the consistency of these findings. For the VAS scores at postoperative 12 hours, a comprehensive analysis involving 432 participants revealed that the AAA group exhibited lower VAS scores than the control group (MD: −0.97, 95% CI: −1.10 to −0.84, P < 0.00001, I² = 16%), with sensitivity analysis again demonstrating consistent results. At the 24-hour postoperative mark, a pooled analysis of data from 532 patients indicated that VAS scores in the AAA group were lower than those of the control group (MD: −1.00, 95% CI: −1.47 to −0.53, P < 0.0001, I² = 96%), with sensitivity analysis showing consistency.
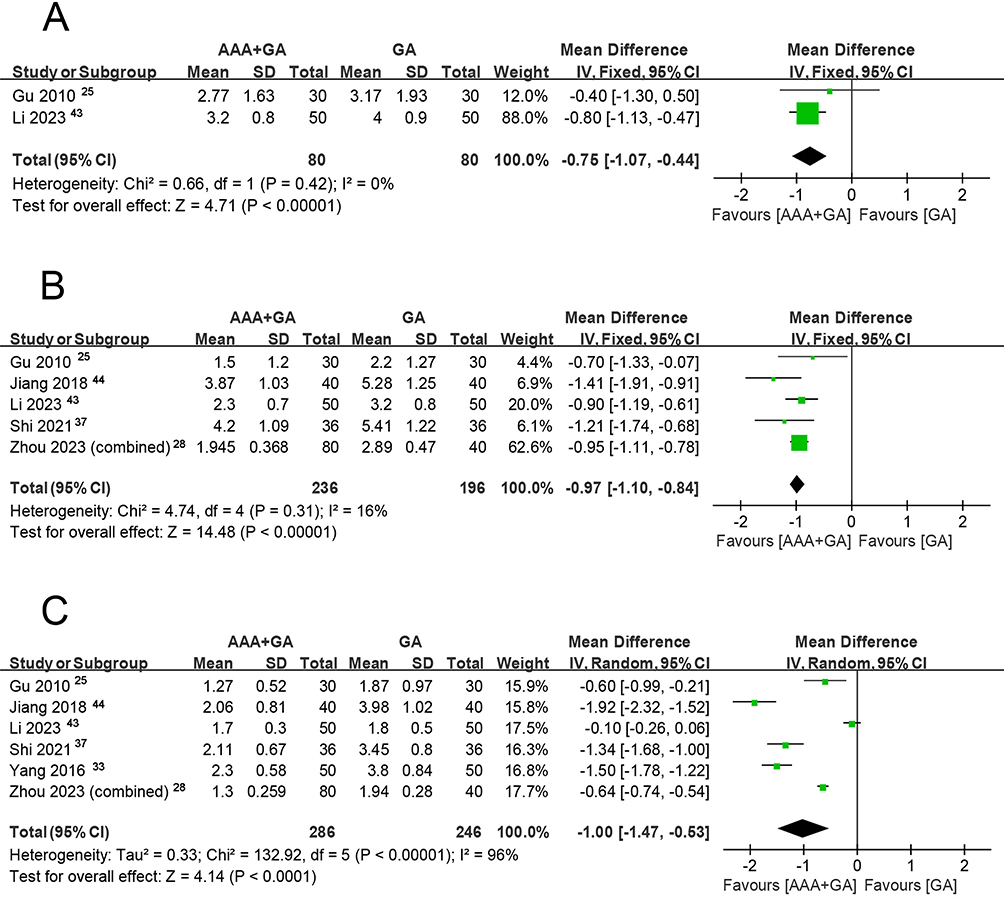 |
Figure 3 Forest plot showing the correlations of EA use with VAS scores at postoperative (A) 2 hours; (B) 12 hours; and (C) 24 hours. Abbreviations: IV, inverse variance; CI, confidence interval; SD, standard deviation. Notes: The results of the heterogeneity analysis showed that the I² values for (A and B) were less than 50%, indicating low heterogeneity, and a fixed-effects model was adopted. In contrast, a random-effects model was used for (C). |
Secondary Outcomes: Postoperative Nausea and Vomiting
The incidence of postoperative nausea and vomiting (PONV) was methodically stratified into four temporal categories for detailed subgroup analysis (Figure 4): postoperative 6 hours, postoperative 24 hours, postoperative 48 hours, and a general postoperative period without specific temporal designation (without specific temporal). In the subset of patients assessed within the first 6 hours postoperatively, those in the AAA group demonstrated a notably reduced incidence of PONV compared to the control group, with a mean difference (MD) of 0.65 and a 95% confidence interval (CI) from 0.50 to 0.85 (P = 0.001, I² = 0%), and sensitivity analysis affirmed the congruence of these findings across studies).When examining the 24-hour postoperative period, the AAA group maintained a significantly lower incidence of PONV relative to the control group, with an MD of 0.46 and a 95% CI ranging from 0.36 to 0.57 (P<0.00001, I² = 18%), and result of the sensitivity analysis showed consistency. At the 48-hour mark, the AAA group did not exhibit a statistically significant difference in PONV incidence compared to the control group, with an MD of 0.50 and a 95% CI from 0.21 to 1.22 (P = 0.13, I² = 0%). Sensitivity analysis maintained the consistency in study outcomes, yet hinted at a potential link between AAA intervention and the attenuation of PONV within the initial 48 hours postoperatively. In aggregate analysis of seven studies that lacked specific temporal data for PONV, AAA was associated with a reduced incidence of PONV (MD: 0.41, 95% CI: 0.25 to 0.68, P = 0.0005, I² = 59%). Nevertheless, the exclusion of the study by Zhang L et al 2015 from sensitivity analysis revealed inconsistent results, underscoring the complexity and the need for cautious interpretation of these findings.31
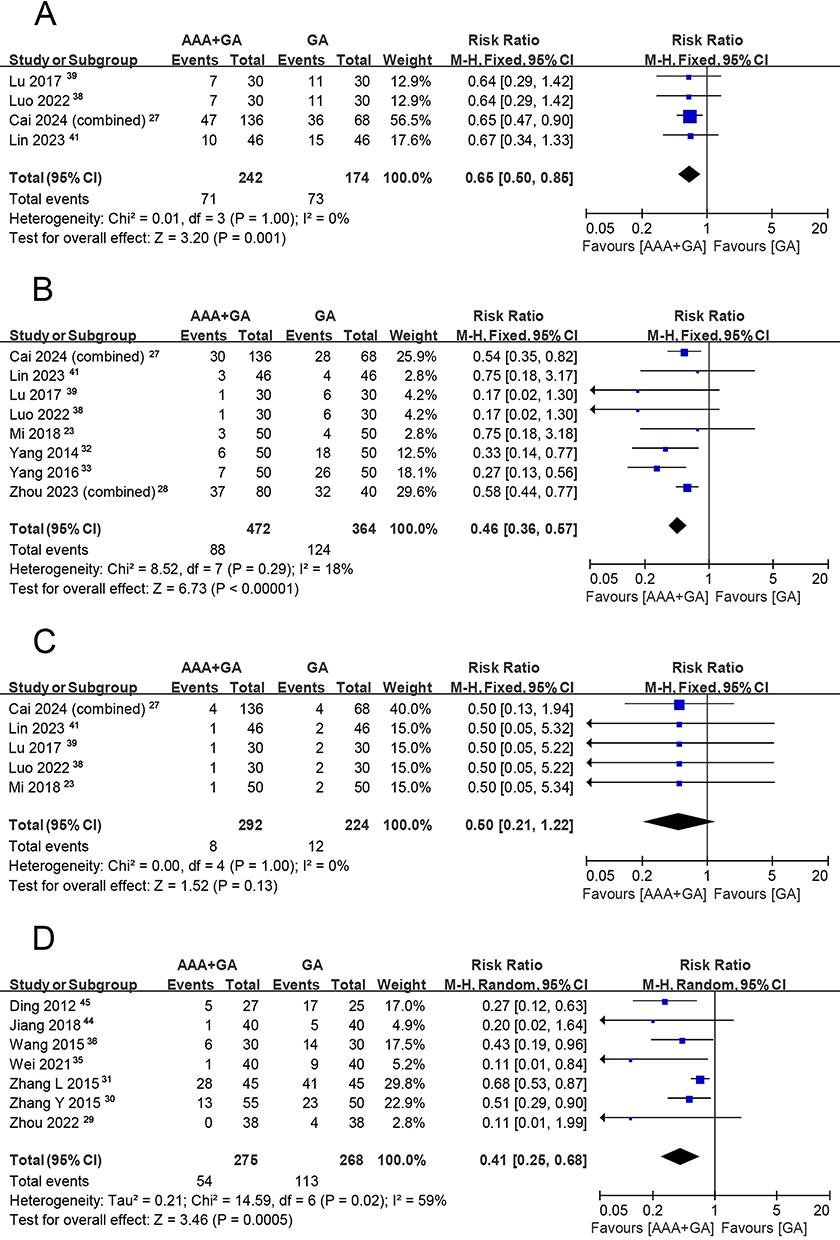 |
Figure 4 Forest plot showing the associations of EA use with PONV at (A) 6 hours; (B) 24 hours; (C) 48 hours; and (D) without specific tempora. Abbreviation: PONV, postoperative nausea and vomiting. Notes: The heterogeneity analysis results showed that the I² values for (A–C) were less than 50%, and a fixed-effects model was adopted. In contrast, due to significant heterogeneity, a random-effects model was used for (D). |
Secondary Outcomes: Pro- and Anti- Inflammatory Cytokines
This meta-analysis (Figure 5) also examined several physicochemical factors, including interleukin-6 (IL-6), interleukin-10 (IL-10), and tumor necrosis factor-alpha (TNF-alpha). The pooled data revealed that, postoperatively, the levels of IL-6 in the acupuncture intervention group were significantly lower than in the control group (MD: −11.15 pg/mL, 95% CI: −19.90 to −2.41, P = 0.01, I² = 89%). However, sensitivity analysis showed inconsistent results when the study by Lu et al 2019 was excluded.40 Regarding postoperative IL-10, the meta-analysis indicated no statistically significant difference between the two groups (MD: 3.35 pg/mL, 95% CI: −0.47 to 7.17, P = 0.09, I² = 91%). The meta-analysis results also demonstrated that TNF-alpha levels were effectively reduced under AAA intervention (MD: −2.71 pg/mL, 95% CI: −3.19 to −2.23, P<0.00001, I² = 0%), with sensitivity analysis confirming the consistency of the study outcomes.37,40
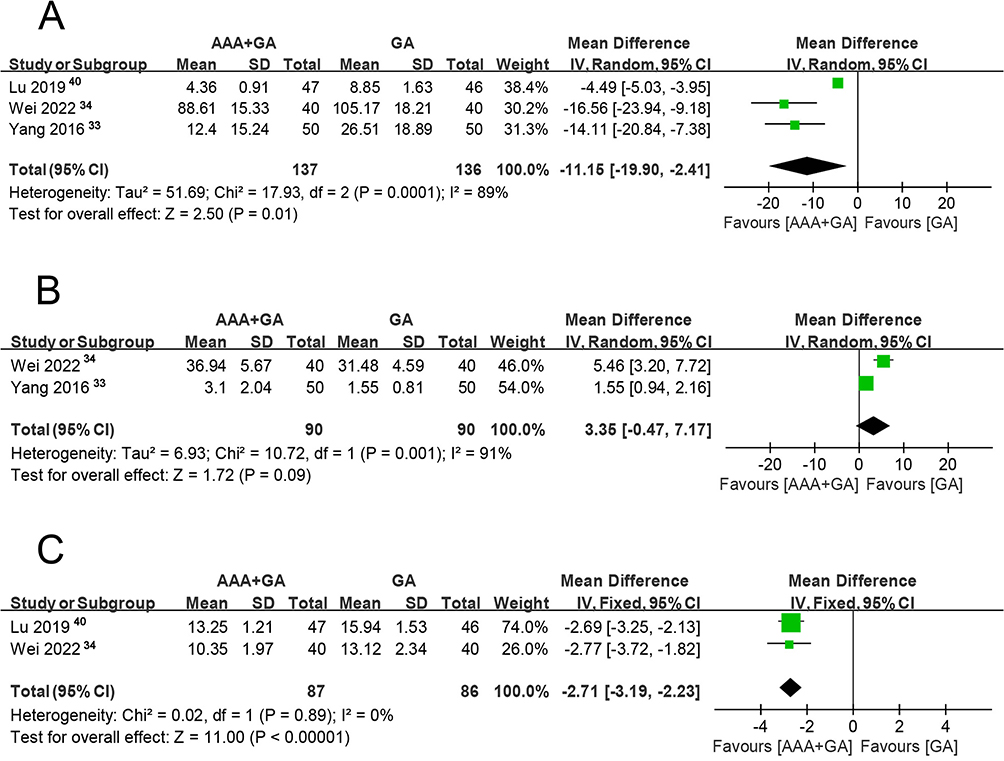 |
Figure 5 Forest plot showing the associations of EA use with pro-inflammatory and anti-inflammatory cytokines on (A) IL-6; (B) IL-10; and (C) TNF-alpha. Abbreviations: IL-6, interleukin-6; IL-10, interleukin-10; TNF- alpha, tumor necrosis factor-alpha. Notes: The heterogeneity analysis results showed that the I² values for (A and B) were greater than 50%, indicating significant heterogeneity, and a random-effects model was adopted. In contrast, a fixed-effects model was used for (C). |
Secondary Outcomes: Time to First Flatus
Regarding the time to first postoperative flatus, the analysis included data from 256 participants, with 128 in the AAA group and 128 in the control group (Figure 6). The combined data revealed that patients who received AAA intervention had an earlier time to first postoperative flatus compared to the control group (MD: −9.93 hours, 95% CI: −16.30 to −3.55, P = 0.002, I² = 98%) and sensitivity analysis showed consistent results across studies.
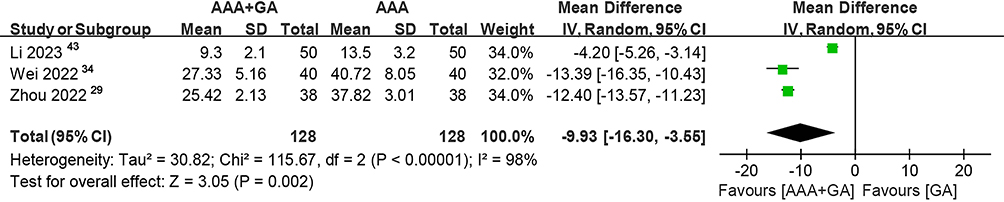 |
Figure 6 Forest plot showing the association of EA use with the TFF. Abbreviation: TFF, time to first flatus. Notes: The heterogeneity analysis results showed an I² value greater than 50%, indicating significant heterogeneity, and thus a random-effects model was adopted. |
Secondary Outcomes: Intraoperative Anesthesia and Muscle Relaxant Use
Owing to the heterogeneity in anesthetic protocols among the studies under review, a subgroup analysis was meticulously performed to assess the usage patterns of diverse anesthetics and muscle relaxants (Figure 7). The meta-analysis disclosed a markedly reduced propofol consumption in the AAA group relative to the control group during surgical procedures (MD: −89.65mg, 95% CI: −136.41 to −42.88, P = 0.0002, I² = 98%), with sensitivity analysis corroborating the uniformity of study outcomes. The fentanyl consumption in the AAA group was lower than in the control group (MD: −0.05mg, 95% CI: −0.07 to −0.03, P<0.0001, I² = 58%). However, sensitivity analysis revealed discordant results upon the exclusion of the study conducted by Zhang L et al 2015.31 The remifentanil consumption in the AAA group was likewise less than in the control group (MD: −89.09µg, 95% CI: −126.65 to −51.53, P<0.00001, I² = 90%), with sensitivity analysis maintaining consistency. The difference in sufentanil consumption between the AAA and control groups was not statistically significant (MD: −2.77µg, 95% CI: −8.48 to 2.95, P = 0.34, I² = 88%). Figure 7 also delineates the dosage of vecuronium bromide, suggesting that AAA may enhance muscle relaxation and decrease the intraoperative reliance on muscle relaxants (SMD: −1.36, 95% CI: −2.37 to −0.35, P = 0.008, I² = 0%). However, sensitivity analysis results became inconsistent upon exclusion of the Ding et al 2008 study.26
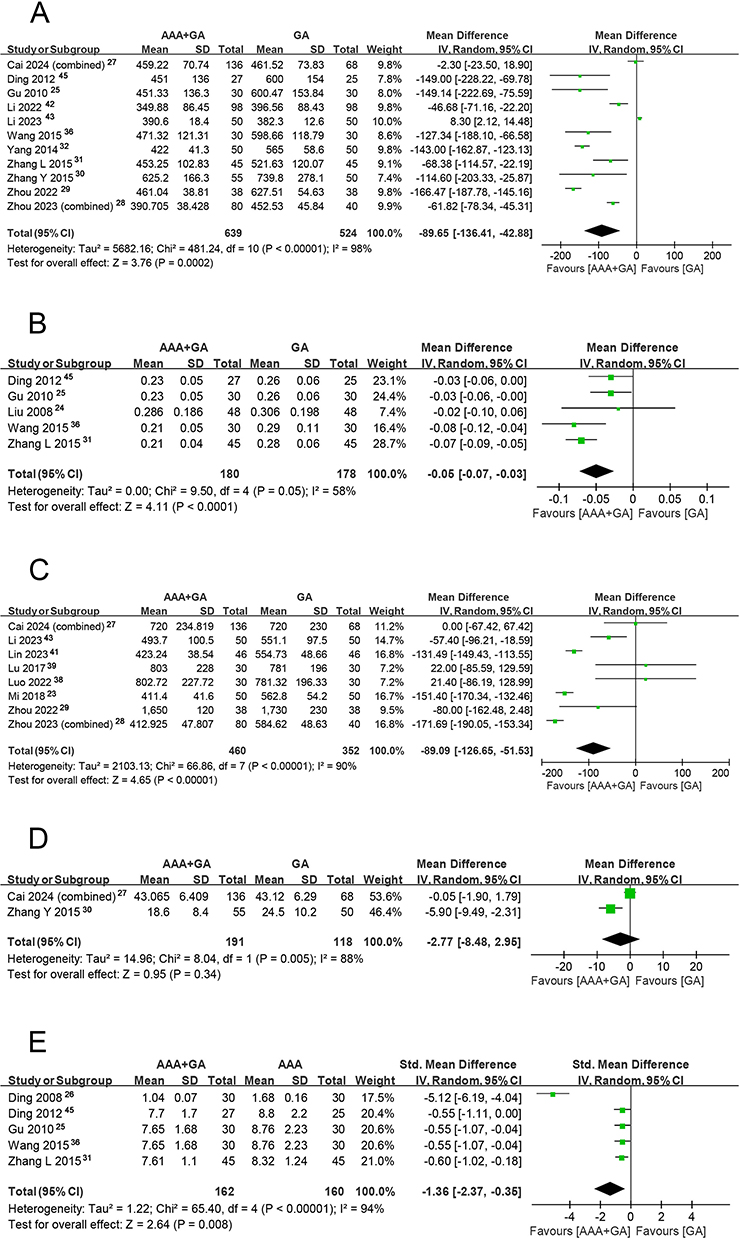 |
Figure 7 Forest plot showing the correlations of EA use with dosage of (A) Propofol; (B) Fentanyl; (C) Remifentanil; (D) Sufentanil; and (E) Vecuronium bromide. Abbreviation: SMD, standardized mean difference (can transform raw data into standardized units, allowing for the integration and comparison of results from various studies that utilized different measurement tools or scales). Notes: Heterogeneity analysis indicated that all subgroups had high heterogeneity, so the random effects model was adopted for all. |
Secondary Outcomes: Postoperative Analgesic Use
Due to the heterogeneity in analgesic formulations within pain pumps across the evaluated studies, the meta-analytic assessment for this particular outcome focused exclusively on the subgroup that utilized fentanyl as the sole postoperative analgesic (Figure 8). The findings indicated that AAA is associated with a reduction in the consumption of fentanyl for postoperative pain management (MD: −22.93mL, 95% CI: −32.00 to −13.86, P<0.00001, I² = 0%), and sensitivity analysis confirmed the homogeneity of the study outcomes.
 |
Figure 8 Forest plot showing the correlations of EA use with postoperative analgesic use (Fentanyl). Notes: No significant heterogeneity was found; a fixed-effects model was used. |
Adverse Events
Among included RCTs, six studies did not report adverse events related to AAA procedures. In other 17 studies, no serious adverse events (SAEs) were reported. In addition, no adverse events on local stimulated sites such as hematoma and infections were reported. Collectively, these findings support the favorable safety profile of AAA.
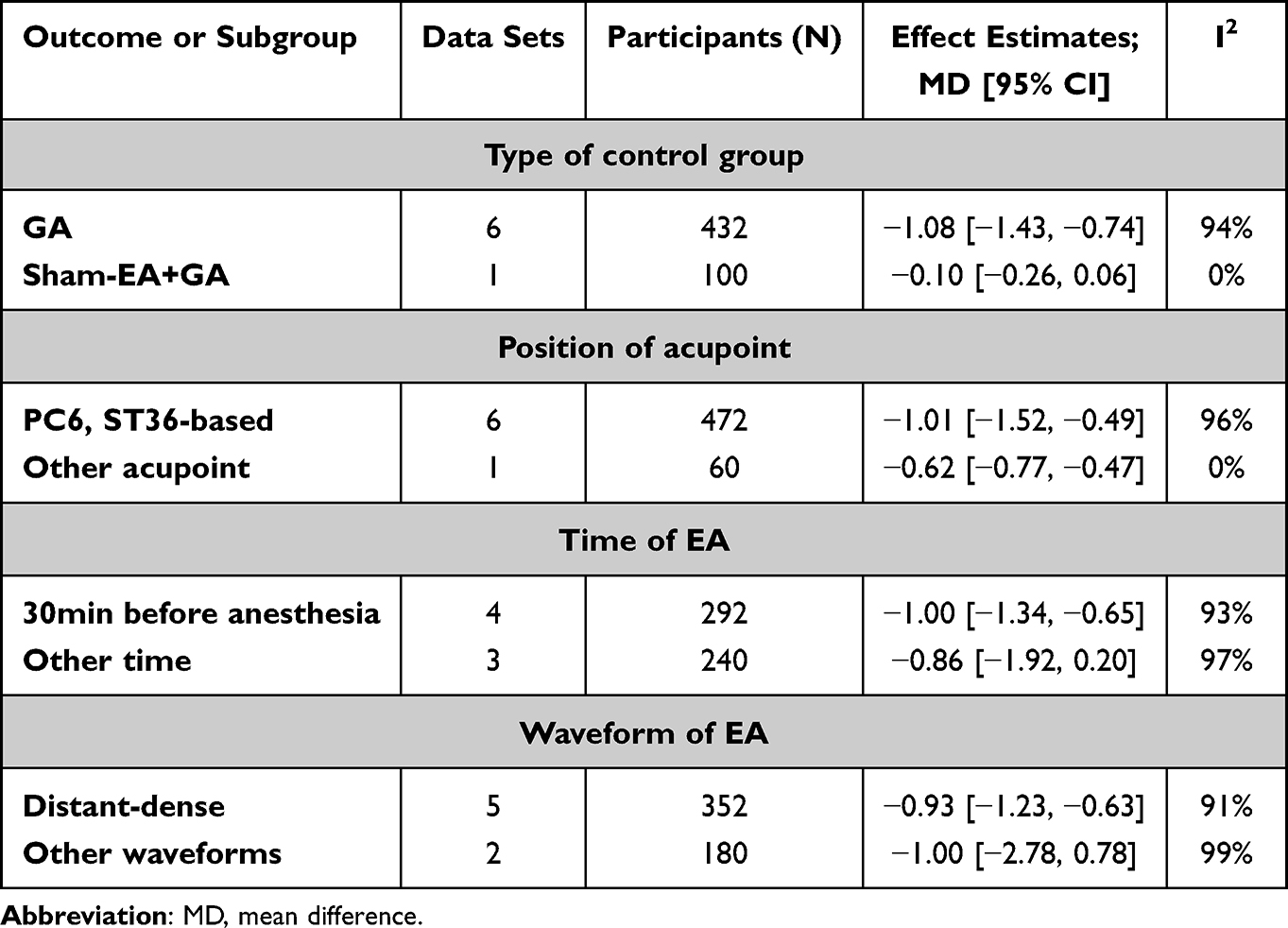 |
Table 3 Subgroup Analysis on Primary Outcome |
Sensitivity and Subgroup Analysis of the Primary Outcome
The findings from the subgroup analyses are concisely encapsulated in Table 3. The primary outcome measures of this study were analyzed through meta-analysis at three time points: 2 hours, 12 hours, and 24 hours postoperatively. Since the I² value was 0% at 2 hours and 12 hours (indicating no heterogeneity), but 96% at 24 hours (indicating significant heterogeneity), the sensitivity analysis was performed using the leave-one-out method. This involved sequentially excluding one study at a time from the meta-analysis to explore the sources of heterogeneity. The high heterogeneity in the 24 hours group remained unchanged, indicating that the results of the meta-analysis are relatively robust. Subgroup analyses were conducted for the 24 hours group to identify the sources of heterogeneity. Subgroup analyses, stratified by control group type (GA versus GA plus sham-EA), acupoints (PC6, ST36-based versus other acupoints), EA timing (30 minutes prior to anesthesia versus other timings), and EA waveform (distant-dense versus other waveforms), showed no significant effect of acupoint location on the primary outcome—the VAS scores. The other three subgroup analyses hinted at a modest, albeit statistically non-significant, influence of control group type, EA timing, and waveform on the outcomes, an effect potentially attributed to the limited sample sizes.
Publication Bias Assessment
The funnel plot was drawn using Manager 5.3 software, with MD as the abscissa and SEM (standard error of the mean difference) as the ordinate, based on the primary outcome measure, to detect publication bias. An uneven distribution of studies on either side suggests the possibility of publication bias. Upon visual inspection, the funnel plot for the 12 hours group showed a symmetrical distribution, with studies roughly evenly and centrally distributed on both sides of the pooled effect size (Figure S1). In contrast, the funnel plot for the 24 hours group was asymmetrical, indicating a potential publication bias (Figure S2). For the 2 hours group, only two studies were included, and thus, a funnel plot analysis was not performed. It is important to note that the validity of the funnel plot symmetry test was low because the cumulative number of RCTs included in the primary outcome measure was less than 10.
Certainty of Evidence
Supplementary Table S2 encapsulates an assessment of the evidentiary certainty across a spectrum of outcomes. The highest degree of confidence is accorded to eight outcomes, which include VAS scores at postoperative 2 hours and 12 hours, PONV at 6 hours, 24 hours and 48 hours, TNF-alpha, Dosage of Vecuronium bromide, postoperative analgesic use, indicating their robustness and reliability. A moderate level of certainty is assigned to nine additional outcomes, which encompass VAS scores at postoperative 24 hours, PONV without specific temporal, IL-6, IL-10, time to first flatus, dosage of propofol, dosage of fentanyl, dosage of sufentanil, dosage of remifentanil.
Discussion
This systematic review and meta-analysis, encompassing 23 studies with a patient population of 2,031, reveals several favorable outcomes associated with the application of AAA in laparoscopic cholecystectomy, including alleviation of postoperative pain, reduction in the incidence of postoperative nausea and vomiting, acceleration of the recovery of gastrointestinal function after surgery, reduction in the use of anesthetics, and decrease in dependence on postoperative analgesics. A schematic diagram summarizing these multifaceted effects of AAA is presented in Figure 9.
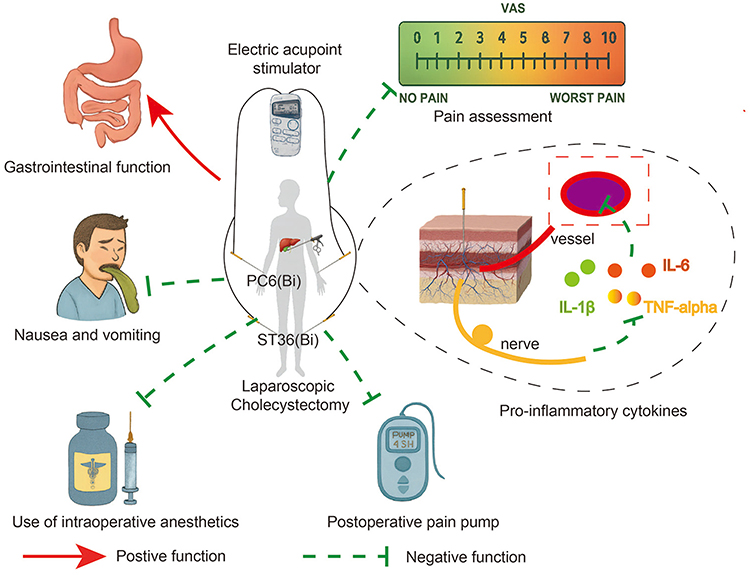 |
Figure 9 The diagram schematically represents the effects of acupuncture assisted anesthesia during laparoscopic cholecystectomy. Notes: Visual elements in the diagram were generated by ChatGPT, and the final figure was produced using Adobe Illustrator. |
The analgesic effect is one of the most widely recognized effects of acupuncture.46 Recent studies have shown that the application of AAA in gastrointestinal or gynecological surgery can reduce postoperative pain while decreasing the doses of intraoperative anesthetics and muscle relaxants.47–50 Our study indicated that patients who underwent acupuncture intervention had lower postoperative VAS scores than the control group (MD: −0.75 at 2 hours, −0.97 at 12hours, −0.94 at 24 hours). Acupuncture is reported to stimulate A-beta, A-delta and C fibers, and subsequently suppresses nociceptive signaling in the spinal dorsal horn through the dorsolateral descending inhibition system, exerting an analgesic effect.46,51,52 Furthermore, some studies suggest that electroacupuncture may elevate pain thresholds by modulating P2X3 receptor expression.10 Additionally, emerging research indicates that acupuncture stimulation can reduce the release of pro-inflammatory cytokines, such as TNF-alpha and IL-6, in venous blood samples when using enzyme-linked immunosorbent assay, while concurrently promoting an increase in the levels of the anti-inflammatory cytokine IL-10.53 Results of our study also showed that patients who received AAA exhibited reduced TNF- alpha and IL-6 levels compared to the control group (TNF-alpha, MD: −2.71 ng/mL; IL-6, MD: −11.15 ng/mL). However, the results of IL-10 did not show significant differences, which may be related to the relatively small sample size included. In terms of drug usage, the postoperative analgesic drug fentanyl consumption in the AAA group was lower than that in the control group. Moreover, the intraoperative anesthetic drug doses of fentanyl, remifentanil, and propofol in the AAA group were lower than those in the control group. However, there was no difference in sufentanil. This may be due to the stronger analgesic effect of sufentanil compared to other anesthetic drugs, resulting in a relatively smaller effect from acupuncture during surgery. Additionally, the dose of the intraoperative muscle relaxant vecuronium bromide in the AAA group was lower than that in the control group.
Postoperative gastrointestinal dysmotility, bowel movement cessation, and constipation are prevalent complications, particularly following open abdominal procedures.7 PONV and TFF are important outcomes for evaluating postoperative gastrointestinal function. Recent studies have reported that the application of AAA in gastrointestinal or gynecological surgery can help reduce the incidence of postoperative PONV and shorten the TFF.48,50 Our study also demonstrated that AAA has the same effect in laparoscopic cholecystectomy (TFF, MD: −9.93 hours; PONV, MD: 0.65 at 6 hours, 0.46 at 24 hours, 0.50 at 48 hours). This may be because acupuncture prevents PONV by modulating endogenous opioid neuropeptides and neurokinin ligands. Meanwhile, acupuncture exerts an analgesic effect and reduces the use of opioid drugs, thereby further lowering the risk of PONV. Additionally, in the included studies, the majority of AAA utilized EA. As reported in a prior literature review, EA can alleviate nausea and vomiting by augmenting the release of endogenous β-endorphins within the cerebrospinal fluid, thereby eliciting an antiemetic response through μ-opioid receptors.6 EA may exert its effects by stimulating adrenergic and noradrenergic nerve fibers, modulating the transmission of 5-hydroxytryptamine 3 (5-HT3), and thus preventing and managing PONV.54,55 Meanwhile, animal and clinical studies have demonstrated that EA can activate the vagus nerve in the spinal cord, thereby facilitating duodenal and distal colonic motility, leading to an earlier TFF in patients.56,57 In addition to this, the majority of AAA studies utilizing EA have employed the distant-dense waveform. This waveform generates stimulation at a relatively low frequency (usually < 30Hz) and a relatively high frequency (usually > 30Hz) alternatively. This waveform has been widely reported in studies for pain management.58
According to Traditional Chinese Medicine (TCM) theory, acupoints are identified as precise anatomical sites on meridians that reflect the operational status of the internal organs. The acupoint ST36, situated on the Stomach Meridian, is believed to help improve gastrointestinal function and have a good analgesic effect.59–61 PC6, located on the Pericardium Meridian, is thought to have antiemetic effects. Most of the included studies incorporated both ST36 and PC6. However, the results of the subgroup analysis indicated that for the primary outcome measure of pain, both the combination of ST36 and PC6 and other acupoint schemes were beneficial in reducing postoperative pain. This result indicated that the analgesic effects were not restricted to the most commonly used acupoints such as ST36 and PC6, and that other acupoints combination also produced certain therapeutic effects. Further comparisons of the effects of stimulating different acupoints can be made in future studies. Collectively, these insights suggested that electrical stimulation at both ST36 and PC6 possessed therapeutic potential for addressing postoperative gastrointestinal dysfunction and alleviating postoperative pain.
The present study had several limitations. First, the included RCTs were homogeneous in terms of demographics, with all participants originating from China. This makes it impossible for us to rule out the potential biases that may arise from differences in ethnicity, geographical background, and healthcare settings and that may affect the results of the meta-analysis. Second, there are differences in the AAA protocols among the included studies, such as acupoint selection, electrostimulation parameters, and the duration of EA intervention, which makes it difficult to develop a generalizable AAA protocol. Lastly, the extended publication timeline of the included studies, spanning from 2008 to 2024, could engender potential biases associated with the evolution of acupuncture intervention strategies and the progression of surgical techniques.
Future studies should expand participant diversity to mitigate ethnic, geographical, and healthcare setting biases. Moreover, standardizing AAA protocols should be a priority. Consensus guidelines or large-scale collaborative studies could aid in creating a generalized protocol. Additionally, evolution of acupuncture and surgical techniques must also be considered. Future studies should control for these changes and conduct time-based subgroup analyses to understand their effects on outcomes. In this way, valid and reliable results can be ensured amid advancing medical practices. By addressing these limitations, addressing these limitations can provide stronger, more applicable evidence on AAA effectiveness and mechanisms.
Conclusion
The current evidence suggests that in laparoscopic cholecystectomy, AAA has potential advantages over general anesthesia, either with or without sham acupuncture, in alleviating postoperative pain, diminishing the incidence of postoperative nausea and vomiting, and expediting the restoration of gastrointestinal function. In addition, AAA may also reduce intraoperative anesthetic consumption, decrease postoperative dependence on analgesics, and lower postoperative levels of pro-inflammatory cytokines. However, considering the limitation on quality of current evidence and the heterogeneity in details of AAA methods among included studies, further high-quality studies focusing on specific AAA methods are needed to verify these conclusions and therefore contribute its clinical use.
Consent for Publication
The authors declare that all the content included in this review is suitable for publication.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author, Yingjun Liu, upon reasonable request.
Author Contributions
All authors have made significant contributions to the reported work, whether in terms of conception, research design, execution, data acquisition, analysis and interpretation, or in all these areas. Participate in drafting, revising or critically reviewing the article; The final version to be published was approved. And all authors agree to be responsible for all aspects of the work.
Funding
This research received funding from the Natural Science Foundation of China (No.82205269); Zhejiang Chinese Medical University Research Fund (No. 2023ZL476); Scientific Research Project of Zhejiang Traditional Chinese Medical University (No.2022JKZKTS47).
Disclosure
The authors declare that they have no conflicts of interest with regard to the content of this report.
References
1. Lammert F, Gurusamy K, Ko CW. et al. Gallstones. Nat Rev Dis Primers. 2016;2(1):16024. doi:10.1038/nrdp.2016.24
2. Brunt LM, Deziel DJ, Telem DA, et al. Safe Cholecystectomy Multi-society Practice Guideline and State of the Art Consensus Conference on Prevention of Bile Duct Injury During Cholecystectomy. Ann Surg. 2020;272(1):3–23. doi:10.1097/sla.0000000000003791
3. Henny CP, Hofland J. Laparoscopic surgery: pitfalls due to anesthesia, positioning, and pneumoperitoneum. Surg Endosc. 2005;19(9):1163–1171. doi:10.1007/s00464-004-2250-z
4. Oti C, Mahendran M, Sabir N. Anaesthesia for laparoscopic surgery. Br J Hosp Med (Lond). 2016;77(1):24–28. doi:10.12968/hmed.2016.77.1.24
5. Zhuang Y, Xing JJ, Li J, et al. History of acupuncture research. Int Rev Neurobiol. 2013;111:1–23. doi:10.1016/b978-0-12-411545-3.00001-8
6. Acar HV. Acupuncture and related techniques during perioperative period: a literature review. Complement Ther Med. 2016;29:48–55. doi:10.1016/j.ctim.2016.09.013
7. Cao LX, Chen ZQ, Jiang Z, et al. Rapid rehabilitation technique with integrated traditional Chinese and Western medicine promotes postoperative gastrointestinal function recovery. World J Gastroenterol. 2020;26(23):3271–3282. doi:10.3748/wjg.v26.i23.3271
8. Chen WT, Fu GQ, Shen WD. Progresses of studies on acupuncture analgesia for postoperative reaction. Acupunct Res. 2013;38(1):83–87.
9. Wang Y, Yang JW, Yan SY, et al. Electroacupuncture vs Sham Electroacupuncture in the Treatment of Postoperative Ileus After Laparoscopic Surgery for Colorectal Cancer: a Multicenter, Randomized Clinical Trial. JAMA Surg. 2023;158(1):20–27. doi:10.1001/jamasurg.2022.5674
10. XJ Z, Zhang H, Che J. Application and Mechanism of Acupuncture Assisted Analgesia in Perioperative Period. Journal of Practical Traditional Chinese Internal Medicine. 2024;38(10):129–132. doi:10.13729/j.issn.1671-7813.Z20232270
11. Zhou MT, ZHANG CJ, Fu JH, et al. Effects of Electroacupuncture on Postoperative Analgesia and Stress Reactions in Elderly Coronary Heart Disease Patients Undergoing Radical Gastrectomy. Shanghai Journal of Acupuncture and Moxibustion. 2020;39(08):1027–1032. doi:10.13460/j.issn.1005-0957.2020.08.1027
12. Han JS. THE FUTURE OF ACUPUNCTURE ANESTHESIA: from acupuncture anesthesia (AA) to acupuncture-assisted anesthesia (AAA). Chin J Pain Med. 1996;1996(01):1–5.
13. Zhou J, WX Z, Wang K, et al. Modern acupuncture anesthesia and its clinical practice. Acupunct Res. 2024;49(12):1310–1318. doi:10.13702/j.1000-0607.20230928
14. Xu TS, Qian HH. Clinical observation on the effect of acupuncture-assisted anesthesia for 40 cases of mixed hemorrhoids surgery. Zhen Ci Yan Jiu. 2009;34(6):403–405.
15. Ang JY, Bhojwani K, Chan HK, et al. A Malaysian retrospective study of acupuncture-assisted anesthesia in breast lump excision. Acupunct Med. 2021;39(1):64–68. doi:10.1177/0964528420920307
16. Hsu GL, Zaid UX, Hsieh CH, et al. Acupuncture assisted local anesthesia for penile surgeries. Transl Androl Urol. 2013;2(4):291–300. doi:10.3978/j.issn.2223-4683.2013.12.02
17. Kaptchuk TJ. Acupuncture: theory, efficacy, and practice. Ann Intern Med. 2002;136(5):374–383. doi:10.7326/0003-4819-136-5-200203050-00010
18. Wu Y, Yuan J, Feng XM. Effect of acupuncture-assisted anesthesia on stress response during laparoscopic cholecystectomy in aged patients. Chin Acupunct Moxibustion. 2011;31(2):155–157.
19. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71
20. Higgins JPT, Li T, JJ D, et al. Chapter 6: choosing effect measures and computing estimates of effect. In: Higgins JPT, Thomas J, Chandler J, editors. Cochrane Handbook for Systematic Reviews of Interventions. Version 6.5 Ed. 2024.
21. Chang CC, Yen WT, Lin YT, et al. Perioperative Pregabalin for Preventive Analgesia in Breast Cancer Surgery: a Meta-analysis of Randomized Controlled Trials. Clin J Pain. 2020;36(12):968–977. doi:10.1097/ajp.0000000000000883
22. Chen HT, Hung KC, Huang YT, et al. Efficacy of electroacupuncture in improving postoperative ileus in patients receiving colorectal surgery: a systematic review and meta-analysis. Int J Surg. 2024;110(2):1113–1125. doi:10.1097/js9.0000000000000848
23. Mi Z, Gao J, Chen X, et al. Effects of transcutaneous electrical acupoint stimulation on quality of recovery during early period after laparoscopic cholecystectomy. Chin Acupunct Moxibustion. 2018;38(3):256–260. doi:10.13703/j.0255-2930.2018.03.007
24. Liu YY, Duan SE, Cai MX, et al. Evaluation of transcutaneous electroacupoint stimulation with the train-of-four mode for preventing nausea and vomiting after laparoscopic cholecystectomy. Chin J Integr Med. 2008;14(2):94–97. doi:10.1007/s11655-008-0094-4
25. Gu CY, Shen LR, Ding YH, et al. Influence of acupuncture at acupoints and non-acupoints on the perioperative analgesic effect in patients with laparoscopic cholecystectomy. Chin Acupunct Moxibustion. 2010;30(8):675–678.
26. Ding YH, Gu CY. Effect of acupuncture--general anesthesia on hemodynamics in perioperative period of patients undergoing cholecystectomy. Chin J Integr Tradit West Med. 2008;28(3):206–208.
27. Cai YC, Lin YL, Yin SJ, et al. Effect of transcutaneous electrical acupoint stimulation based on the theory of “qi ascending and descending movement” on autonomic nervous system and gastrointestinal function in patients after general anesthesia laparoscopic cholecystectomy. Acupunct Res. 2024;49(3):283–288. doi:10.13702/j.1000-0607.20221402
28. Zhou YQ, Gao TS. Effect of TAES with Different Acupoint Compatibility Combined with General Anesthesia on Postoperative Adverse Reactions in Patients with Laparoscopic Cholecystectomy. J Emerg Tradit Chin Med. 2023;32(03):456–460.
29. Zhou SM, Suo JF, Sun YX, et al. Effects of transcutaneous electrical acupoint stimulation assisted general anesthesia on anesthetic management and efficacy in laparoscopic gallbladder surgery. China Med Pharm. 2022;12(12):
30. Zhang Y, Zhu L, Lou JY, et al. The Application of Acupuncture Anesthesia in Obese Patients Undergo Elective laparoscopic Cholecystectomy. J Emerg Tradit Chin Med. 2015;24(06):1079–1081.
31. Zhang L, Wu C. Clinical Comparative Study of Two Methods of Acupuncture Assisted with Anesthesia for Patients Undergoing Laparoscopic Cholecystectomy. Chin Arch Tradit Chin Med. 2015;33(04):826–828. doi:10.13193/j.issn.1673-7717.2015.04.017
32. Yang XC, Xu HM, Wang YH, et al. Clinical Study on Acupuncture-Assisted General Anesthesia for Laparoscopic Cholecystectomy. Chin J Integr Tradit West Med. 2014;34(07):883–886.
33. Yang LL, Mo YC, Wang LL, et al. Effects of Transcutaneous Electrical Acupoint Stimulation on Postoperative Complications and Inflammatory Factors after Laparoscopic Cholecystectomy. J Zhejiang Tradit Chin Med. 2016;51(01):9–10. doi:10.13633/j.cnki.zjtcm.2016.01.005
34. Wei LZ, Qu N, Guan YM. Intervention effect on acupoint electrical stimulation of postoperative nausea and vomiting(PONV) after laparoscopic cholecystectomy. J Xinjiang Med Univ. 2022;45(03):339–344.
35. Wei LZ. Transcutaneous Electrical Acupoint Stimulation for the Prevention of Postoperative Nausea and Vomiting (PONV) After Laparoscopic Cholecystectomy. Pharm Wkly. 2021;30(36):161–162.
36. Wang YD, Zhou J, Han G, et al. Clinical Observation of the Efficacy of Combined Acupuncture and Drug Anesthesia in Laparoscopic Cholecystectomy. Chin J Basic Med Tradit Chin Med. 2015;21(06):728–730. doi:10.19945/j.cnki.issn.1006-3250.2015.06.040
37. Shi YJ, Zhang H, Cao XW. Effect of acupuncture assisted anesthesia on pain and hemodynamics in patients undergoing laparoscopic cholecystectomy. China Mod Med. 2021;28(23):
38. Luo Q, Lu L. Clinical observation on the effect of electroacupuncture combined with dizocine on perioperative hemodynamic changes for patients undergoing laparoscopic cholecystectomy. China Med Pharm. 2022;12(19):
39. Lu L, Zhu HS. Effect of electroacupuncture combined with dezocine on postoperative hyperalgesia induced by remifentanil. Chin J Anesthesiol. 2017;37(12):1434–1437. doi:10.3760/cma.j.issn.0254-1416.2017.12.007
40. Lu B, Wang Q, Ding LL. Effect of transcutaneous acupoint electrical stimulation on early recovery quality of patients after laparoscopic cholecystectomy. China Med Her. 2019;16(13):
41. Lin SY, Yin ZL, Gao J, et al. Effect of Percutaneous Acupoint Electrical Stimulation on Postoperative Fatigue Syndrome in Patients Undergoing Daytime Laparoscopic Cholecystectomy. Chin J Integr Tradit West Med. 2023;43(03):365–368.
42. Li B, Yu FL. Analysis of the practical effect of acupuncture assisted anesthesia in elderly patients undergoing laparoscopic cholecystectomy. China Prac Med. 2021;16(25):18–20. doi:10.14163/j.cnki.11-5547/r.2021.25.006
43. LI B, Zhao ZQ, Liu SY, et al. Effects of transcutaneous electrical acupoint stimulation on stress response and gastrointestinal function after laparoscopic cholecystectomy. J Clin Anesthesiol. 2023;39(04):379–383.
44. Jiang M, Zhou M, Shen FY. A Clinical Study on the Analgesic Effect of Acupuncture as an Adjunct to Anesthesia in Patients Undergoing Laparoscopic Cholecystectomy—With 40 Case Reports. Jiangsu J Tradit Chin Med. 2018;50(03):67–68.
45. Ding YH, Gu CY, Shen LR, et al. Effects of acupuncture on neuromuscular block of vecuronium and analgesia under general anesthesia. Chin J Anesthesiol. 2012;32(6):762–765. doi:10.3760/cma.j.issn.0254-1416.2012.06.033
46. Zhao ZQ. Neural mechanism underlying acupuncture analgesia. Prog Neurobiol. 2008;85(4):355–375. doi:10.1016/j.pneurobio.2008.05.004
47. Lu Z, Dong H, Wang Q, et al. Perioperative acupuncture modulation: more than anaesthesia. Br J Anaesth. 2015;115(2):183–193. doi:10.1093/bja/aev227
48. Zhu J, Li S, Wu W, et al. Preoperative electroacupuncture for postoperative nausea and vomiting in laparoscopic gynecological surgery: a randomized controlled trial. Acupunct Med. 2022;40(5):415–424. doi:10.1177/09645284221076517
49. Zhong Y, Deng J, Pan T, et al. Buccal Acupuncture Reduces the Dose of Sufentanil Needed in Laparoscopic Gynecological Surgery. Med Sci Monit. 2025;31:e947088. doi:10.12659/msm.947088
50. Hou Y, Yan Q, An H, et al. The use and protective effects of transcutaneous electrical acupoint stimulation during abdominal surgery: study protocol for a multicenter randomized parallel controlled trial. Trials. 2019;20(1):462. doi:10.1186/s13063-019-3558-2
51. Association MISCotCRH. Expert consensus on day-case laparoscopic cholecystectomy. World J Laparosc Surg. 2023;28(08):
52. Kehlet H, Jensen TS, Woolf CJ. Persistent postsurgical pain: risk factors and prevention. Lancet. 2006;367(9522):1618–1625. doi:10.1016/s0140-6736(06)68700-x
53. Wang M, Liu W, Ge J, et al. The immunomodulatory mechanisms for acupuncture practice. Front Immunol. 2023;14:1147718. doi:10.3389/fimmu.2023.1147718
54. Stoicea N, Gan TJ, Joseph N, et al. Alternative Therapies for the Prevention of Postoperative Nausea and Vomiting. Front Med (Lausanne). 2015;2:87. doi:10.3389/fmed.2015.00087
55. Streitberger K, Ezzo J, Schneider A. Acupuncture for nausea and vomiting: an update of clinical and experimental studies. Auton Neurosci. 2006;129(1–2):107–117. doi:10.1016/j.autneu.2006.07.015
56. Imai K, Ariga H, Chen C, et al. Effects of electroacupuncture on gastric motility and heart rate variability in conscious rats. Auton Neurosci. 2008;138(1–2):91–98. doi:10.1016/j.autneu.2007.11.003
57. Lu MJ, Yu Z, He Y, et al. Electroacupuncture at ST36 modulates gastric motility via vagovagal and sympathetic reflexes in rats. World J Gastroenterol. 2019;25(19):2315–2326. doi:10.3748/wjg.v25.i19.2315
58. Liang Y, Zhou J, Sun J, et al. The dose-effect relationship of electroacupuncture analgesia and its stimulus parameters: progress in the last 3 decades. World Journal of Acupuncture-Moxibustion. 2023;33(01):12–19. doi:10.1016/j.wjam.2022.12.001
59. Han X, Chen X, Wang X, et al. Electroacupuncture at ST36 Improve the Gastric Motility by Affecting Neurotransmitters in the Enteric Nervous System in Type 2 Diabetic Rats. Evid Based Complement Alternat Med. 2021;2021:6666323. doi:10.1155/2021/6666323
60. Meng JB, Jiao YN, Xu XJ, et al. Electro-acupuncture attenuates inflammatory responses and intraabdominal pressure in septic patients: a randomized controlled trial. Medicine (Baltimore). 2018;97(17):e0555. doi:10.1097/md.0000000000010555
61. Wang X, Lu L, Zi L, et al. Electroacupuncture at Acupoint ST36 (Zusanli) Improves Intestinal Motility Dysfunction Via Increasing the Proportion of Cholinergic Neurons in Rat Ileal Myenteric Ganglia after Severe Acute Pancreatitis. Evid Based Complement Alternat Med. 2022;2022:7837711. doi:10.1155/2022/7837711
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Efficacy and Safety of Acupuncture for Tinnitus-Associated Insomnia: A Protocol for a Systematic Review and Meta-Analysis
Fan L, Gao Y, Zhou J, Hu H, Gao H
Journal of Pain Research 2022, 15:2957-2965
Published Date: 21 September 2022
Tezepelumab for Patients with Severe Uncontrolled Asthma: A Systematic Review and Meta-Analysis
Zoumot Z, Al Busaidi N, Tashkandi W, Aljohaney AA, Isse S, Vidyasagar K, Ukwaja KN
Journal of Asthma and Allergy 2022, 15:1665-1679
Published Date: 18 November 2022
The Analgesic Effect and Potential Mechanisms of Acupuncture for Migraine Rats: A Systematic Review and Meta-Analysis
Sun S, Liu L, Zhou M, Liu Y, Sun M, Zhao L
Journal of Pain Research 2023, 16:2525-2542
Published Date: 24 July 2023
Efficacy of Acupuncture in Acute Exacerbation of Chronic Obstructive Pulmonary Disease: A Systematic Review and Meta-Analysis
Yang C, Tian H, Xu G, Luo Q, Sun M, Liang F
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:707-720
Published Date: 11 March 2024
Acupuncture and Moxibustion in the Treatment of Gynecological Perioperative Anxiety: A Systematic Review and Meta-Analysis
Wang X, Yu Q, Zhu J, Liu J, Gao X, Wang X, Wang L, Xu X
Journal of Pain Research 2024, 17:3515-3538
Published Date: 31 October 2024