Back to Journals » Journal of Pain Research » Volume 18
Pain Management Approaches for Robotic-Assisted Thoracic Surgery: A Retrospective Analysis
Authors Semyonov MA, Shmueli M ![]() , Smirnov A, Dubilet M
, Smirnov A, Dubilet M ![]() , Refaely Y, Ruderman LN, Maron P, Binyamin Y
, Refaely Y, Ruderman LN, Maron P, Binyamin Y ![]() , Brotfain E, Zlotnik A, Frank D
, Brotfain E, Zlotnik A, Frank D
Received 2 July 2025
Accepted for publication 22 October 2025
Published 14 November 2025 Volume 2025:18 Pages 6085—6093
DOI https://doi.org/10.2147/JPR.S547426
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jinlei Li
Michael Alexander Semyonov,1,2,* Moshe Shmueli,2,3,* Alexander Smirnov,1,2 Michael Dubilet,1,2 Yael Refaely,2,4 Leonid N Ruderman,2,4 Pavel Maron,1,2 Yair Binyamin,1,2 Evgeni Brotfain,1,2 Alexander Zlotnik,1,2 Dmitry Frank1
1Department of Anesthesiology and Critical Care, General Intensive Care Unit, Soroka Medical Center, Beer Sheva, Israel; 2Faculty of Health Sciences, Ben-Gurion University of the Negev, Beer Sheva, Israel; 3Clinical Research Center, Soroka University Medical Center, Beer Sheva, Israel; 4Department of Cardiothoracic Surgery, Soroka Medical Center, Beer Sheva, Israel
*These authors contributed equally to this work
Correspondence: Moshe Shmueli, Faculty of Health Sciences, Ben-Gurion University of the Negev, Beer Sheva, Israel, Tel +972-8 6403770, Fax +972-8-6403771, Email [email protected]
Purpose: Robotic-assisted thoracic surgery (RATS) is increasingly used for thoracic procedures; however, there are various regional anesthesia techniques for optimal pain management. This study aimed to compare the analgesic effectiveness and perioperative outcomes of different regional anesthesia techniques with those of general anesthesia (GA) in patients undergoing RATS.
Patients and Methods: We conducted a retrospective cohort study of adult patients undergoing elective RATS at Soroka University Medical Center from January 2018 to July 2024. Patients were grouped based on intraoperative pain management approach: thoracic epidural analgesia (TEA), thoracic paravertebral block (PVB), erector spinae plane (ESP) block, serratus anterior plane (SAP) block, or General anesthesia alone. Primary outcomes included postoperative pain (measured by Visual Analog Scale scores; VAS) and opioid consumption. Secondary outcomes included intraoperative hemodynamic stability, postoperative complications, and length of hospitalization.
Results: A total of 158 patients were analyzed: TEA (n=5), PVB (n=65), ESP (n=40), SAP (n=14), and GA alone (n=34). Demographics and surgical characteristics were similar across groups. Significant differences were observed in Post-Anesthesia Care Unit (PACU) morphine use (p < 0.001), with the lowest consumption in the ESP (3.75 ± 5.51 mg) and SAP (3.92 ± 4.00 mg) groups and the highest in the GA group (12.42 ± 6.01 mg). PACU VAS scores at 30 minutes and 1 hour were significantly lower in the PVB, ESP, and SAP groups compared to GA (p < 0.01). Hypotension and vasopressor use were most frequent with TEA and PVB, while SAP and ESP were associated with better hemodynamic profiles. No significant differences were observed in postoperative infection rates or hospital stay duration.
Conclusion: Regional pain management techniques, particularly ESP and SAP blocks, were associated with reduced pain and opioid use while maintaining hemodynamic stability compared to GA. Given the relatively small sample sizes in the TEA and SAP groups, these findings should be interpreted cautiously, and prospective studies are needed to confirm and refine these approaches.
Keywords: erector spinae plane block, opioid use, paravertebral block, postoperative pain, regional anesthesia, robotic-assisted thoracic surgery, thoracic epidural
Introduction
Robotic-assisted thoracic surgery (RATS) has become an established approach for managing a range of thoracic pathologies, particularly in lobectomies and other common interventions. With its enhanced visualization, precision, and ergonomic benefits, RATS offers several technical advantages over conventional open procedures. However, its benefits compared to video-assisted thoracoscopic surgery (VATS) remain a subject of ongoing debate. Studies comparing RATS and VATS have focused on metrics such as operative time, intraoperative blood loss, length of hospitalization, cost, complication rates, and, notably, postoperative pain control.1–3
Postoperative pain is a critical factor influencing recovery, respiratory function, and overall patient satisfaction following thoracic surgery. Regional anesthesia has recently become a cornerstone of multimodal analgesic strategies, aiming to reduce opioid consumption and enhance clinical outcomes, including lower pain levels as assessed by validated measurement tools. Various regional techniques, including thoracic paravertebral block (PVB), intercostal nerve block, erector spinae plane (ESP) block, serratus anterior plane (SAP) block, and thoracic epidural analgesia (TEA), are employed to optimize postoperative analgesia.4–9
Each of these techniques presents unique advantages and limitations. The paravertebral block is widely regarded as a first-line approach for thoracic surgery due to its proven efficacy and safety profile.10 Nonetheless, its success can be affected by technical difficulty and anatomical variability, with rare but reported complications including pneumothorax and vascular injury.11 The ESP block, a more recently described fascial plane technique, is easier to perform and generally safer, but may provide suboptimal visceral pain relief and requires larger volumes of local anesthetic, posing a potential risk for systemic toxicity.12,13 TEA remains the most comprehensive regional approach, capable of producing dense segmental anesthesia, particularly valuable in patients with compromised pulmonary reserve. However, it is associated with a higher incidence of hemodynamic side effects, requires greater technical expertise, and carries a risk of serious complications such as epidural hematoma.14
At our institution, we have accumulated five years of experience delivering anesthesia for RATS procedures utilizing a range of regional techniques. Despite the increasing adoption of these methods, no clear consensus has been established regarding the optimal regional block for patients undergoing RATS. The primary aim of this study is to assess the comparative effectiveness of regional anesthesia techniques versus general anesthesia alone on postoperative pain control and perioperative outcomes in patients undergoing RATS. Our secondary objective is to compare peripheral nerve blocks with each other in terms of analgesic efficacy and recovery parameters. By identifying differences in analgesic efficacy, complication profiles, and recovery metrics, we aim to contribute to ongoing research on a preferred regional anesthesia strategy for robotic thoracic surgery.
Patients and Methods
Study Design and Setting
This retrospective cohort study was conducted at Soroka University Medical Center (SUMC), a tertiary referral hospital in Israel, between January 2018 and July 2024. The study was approved by the Institutional Review Board of SUMC (Approval No. 0195–24-SOR) and conducted in accordance with the principles of the Declaration of Helsinki. Given the retrospective design and use of de-identified data, the requirement for informed consent was waived by the ethics committee on the grounds of minimal risk to participants.
Patient Selection
We included all adult patients (aged ≥18 years) who underwent elective robotic-assisted thoracic surgery (RATS) under general anesthesia during the study period. Based on the intraoperative regional analgetic techniques used, patients were categorized into five groups: (1) general anesthesia with thoracic epidural analgesia (TEA), (2) general anesthesia with erector spinae plane block (ESP), (3) general anesthesia with paravertebral block (PVB), (4) general anesthesia with serratus anterior plane block (SAP), and (5) general anesthesia alone (GA).
Anesthesia Protocols
The choice of anesthesia technique was guided by institutional protocols, patient characteristics, and clinician preference. All patients received general anesthesia via total intravenous anesthesia (TIVA) with propofol (50–100 µg/kg/h), fentanyl (1 µg/kg), and rocuronium (0.8–1 mg/kg). One-lung ventilation was achieved using a standard double-lumen endobronchial tube. Local infiltration with 0.5% bupivacaine (3–10 mL) was performed at incision sites.
Regional anesthesia techniques were performed using ultrasound guidance by board-certified anesthesiologists. Thoracic epidural analgesia (TEA) was placed pre-induction while the patient was awake, with the catheter positioned at T5–T7. A test dose of 5–8 mL ropivacaine 0.2% was administered, followed by continuous infusion of ropivacaine 0.2% with fentanyl until postoperative day 2–3. Postoperatively, boluses of 10 mL ropivacaine were given every 8 hours for the first 24 hours.
All plane blocks (ESP and SAP) were performed post-induction, after intubation, with the patient in the tilt position prior to skin incision.
ESP block: Targeted the same dermatomal range as PVB (typically T5–T8) with a bolus of ropivacaine 3 mg/kg and postoperative boluses of 10 mL every 8 hours.
SAP block: Administered at the fifth rib along the mid-axillary line with intermittent boluses of ropivacaine 3 mg/kg and postoperative boluses of 10 mL every 8 hours.
Data Collection
Data were retrospectively extracted from institutional electronic medical records using the MetaVision® and Chameleon® platforms. Collected variables included patient demographics (age, sex, weight, and ASA physical status classification), surgical details (procedure type, operative time, time to chest tube removal, and time to discharge), and intraoperative parameters such as total opioid use (converted to intravenous morphine equivalents), vasopressor administration, and incidence of hypotension. Postoperative outcomes included visual analog scale (VAS) pain scores recorded at predefined intervals: 30 minutes, 1 hour, and 2 hours in the post-anesthesia care unit (PACU), and 1, 2, 4, 8, 16, 24, 48, and 72 hours postoperatively in the ward.Both static and dynamic pain were measured. Static VAS assessed pain at rest in the PACU, while dynamic VAS measured pain during movement or activity in the ward. VAS scores and complications were documented by trained PACU and ward nursing staff as part of routine clinical care and recorded in the electronic medical record. Additional outcomes comprised total postoperative opioid consumption, complication rates (nausea, respiratory depression, pruritus, urinary retention, and hypoxemia), time to ambulation, PACU length of stay, and total hospital length of stay. Acute pain service consultations were provided when clinically indicated, ensuring standardized assessment and management of postoperative pain.No catheter-related complications were observed; however, some cases required administration of morphine.
Outcomes
The primary outcomes were defined as follows: (1) postoperative pain intensity, measured using the Visual Analog Scale (VAS, 0–10) in the post-anesthesia care unit (PACU) at 30 minutes, 1 hour, and 2 hours postoperatively, and then at regular intervals during the first 72 hours after surgery; (2) total opioid consumption, calculated as the cumulative dose of opioids administered postoperatively, expressed in intravenous morphine equivalents; and (3) length of hospital stay, defined as the number of days from the day of surgery until patient discharge.
Secondary outcomes were defined to monitor complications and side effects associated with the different anesthesia techniques. These included: (1) hemodynamic instability, defined by the occurrence of intraoperative hypotension or the need for vasopressor support; (2) respiratory complications, including postoperative oxygen requirement, atelectasis, air leak, pneumonia, hypoxemia, and unplanned intensive care unit (ICU) admission; and (3) postoperative infections and other complications potentially related to regional anesthesia techniques, such as urinary retention, constipation, and nausea. All secondary outcomes were systematically recorded during the in-hospital postoperative period to assess the safety and tolerability of each anesthesia approach.
Statistical Analysis
Continuous variables were reported as mean ± standard deviation or median (interquartile range), as appropriate, and categorical variables were summarized as counts and percentages. Normality was assessed using the Kolmogorov–Smirnov test. Between-group comparisons for continuous variables were performed using one-way ANOVA for normally distributed data or Kruskal–Wallis tests for non-normally distributed data, with post hoc pairwise comparisons conducted using Tukey’s test or Dunn’s test, respectively. For categorical variables, Pearson’s χ2 or Fisher’s exact tests were applied as appropriate. To account for multiple comparisons, Bonferroni correction was applied when evaluating outcomes measured at multiple time points (eg, VAS scores at 30 min, 1 h, and 2 h postoperatively). A p-value <0.05 was considered statistically significant. All analyses were conducted using R Statistical Software (version 4.4.0).
Results
Patient Demographics and Operative Characteristics
A total of 158 patients were included in the analysis and divided Based on the intraoperative regional analgetic techniques used: thoracic epidural analgesia (TEA) (n=5), erector spinae plane (ESP) block (n=40), paravertebral (PVB) block (n=65), general anesthesia alone (GA) (n=34), and serratus anterior block (SAP) (n=14) (see Table 1). No statistically significant differences were found in age (p = 0.078), weight (p = 0.065), or gender distribution (p = 0.12) among groups. The SAP group had significantly lower ASA scores than the ESP, GA, and Paravertebral block groups, suggesting that SAP patients were generally healthier preoperatively.
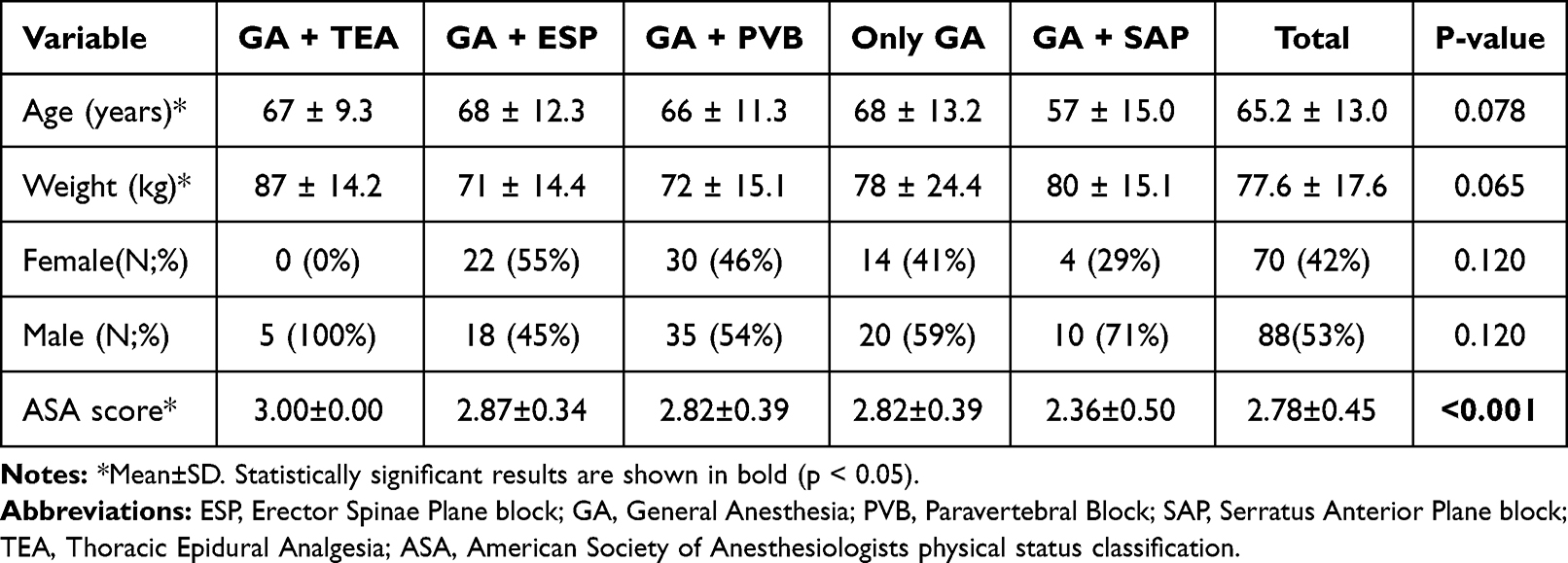 |
Table 1 Demographic and Clinical Characteristics of the Study Population by Regional Pain Management Technique |
The mean duration from admission to surgery ranged from 1.1 to 1.9 hours, with no significant differences (p = 0.9). Mean operative time ranged from 3.8 to 6.0 hours and did not differ significantly between groups (p = 0.3). Lobectomy was the most common surgical procedure in all groups, but differences in procedure types were not statistically significant (p = 0.54).
Intraoperative Management
Fluid balance varied across groups, with the highest volume recorded in the TEA group (2400 ± 894 mL) and the lowest in the SAP group (1736 ± 943 mL). However, the difference was not statistically significant (p = 0.4) (see Table 2).
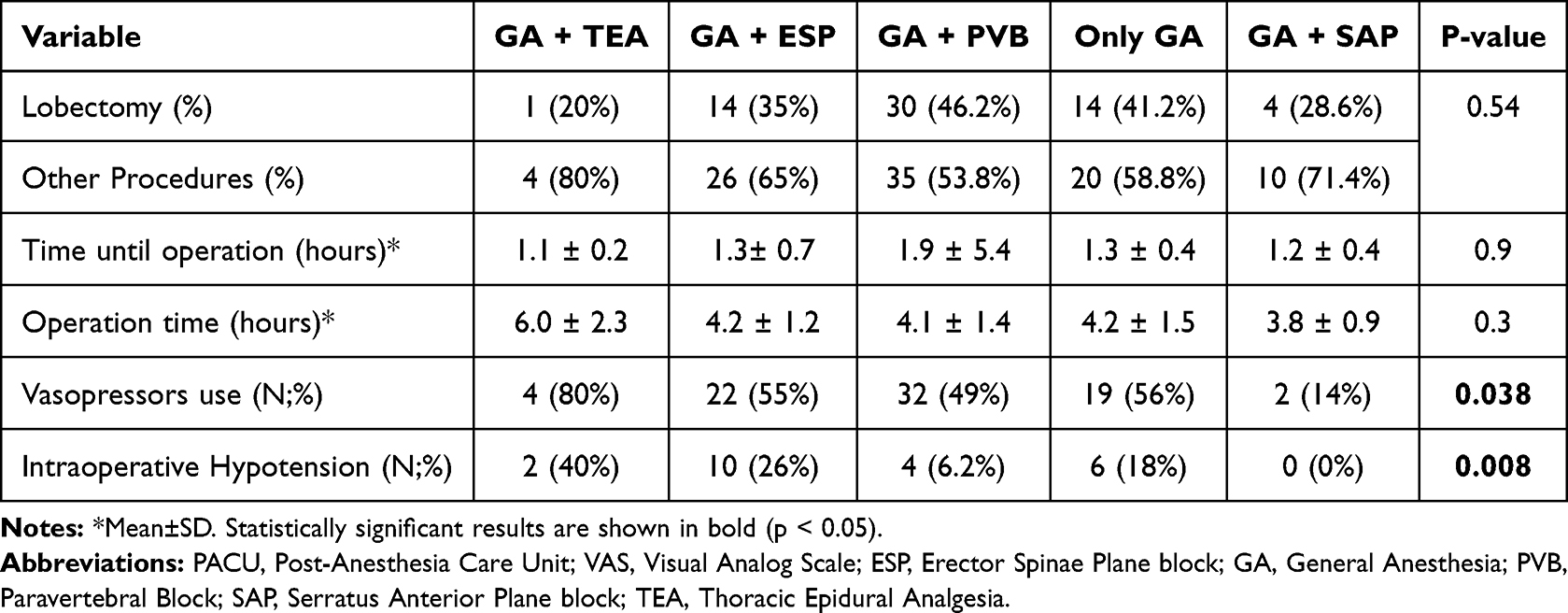 |
Table 2 Surgical Characteristics by Regional Pain Management Technique |
Intraoperative fentanyl use was highest in the ESP and PVB groups (265 ± 126 mcg and 257 ± 89 mcg, respectively), and lowest in the SAP group (193 ± 85 mcg), with no statistically significant difference (p = 0.12). Morphine use was uncommon and limited to the ESP and PVB groups (p = 0.2). Intraoperative vasopressor use differed significantly (p = 0.038), with 80% of patients in the TEA group requiring vasopressors, compared to only 14% in the SAP group. Intraoperative hypotension was also significantly more frequent in the PVB group (39%) and absent in the SAP group (p = 0.008).
Post-Operative Outcomes
Post-anesthesia care unit (PACU) stay duration varied significantly across groups (p < 0.001), with the GA group staying the longest (2.7 ± 0.9 hours), and the ESP group the shortest (1.4 ± 0.5 hours). (see Table 3). Mean morphine consumption in the PACU also showed significant variation (p < 0.001), with the highest levels in the GA group (12.4± 6.0 mg) and the lowest in the ESP (3.7 ± 5.5 mg) and SAP (3.9 ± 4.0 mg) groups.
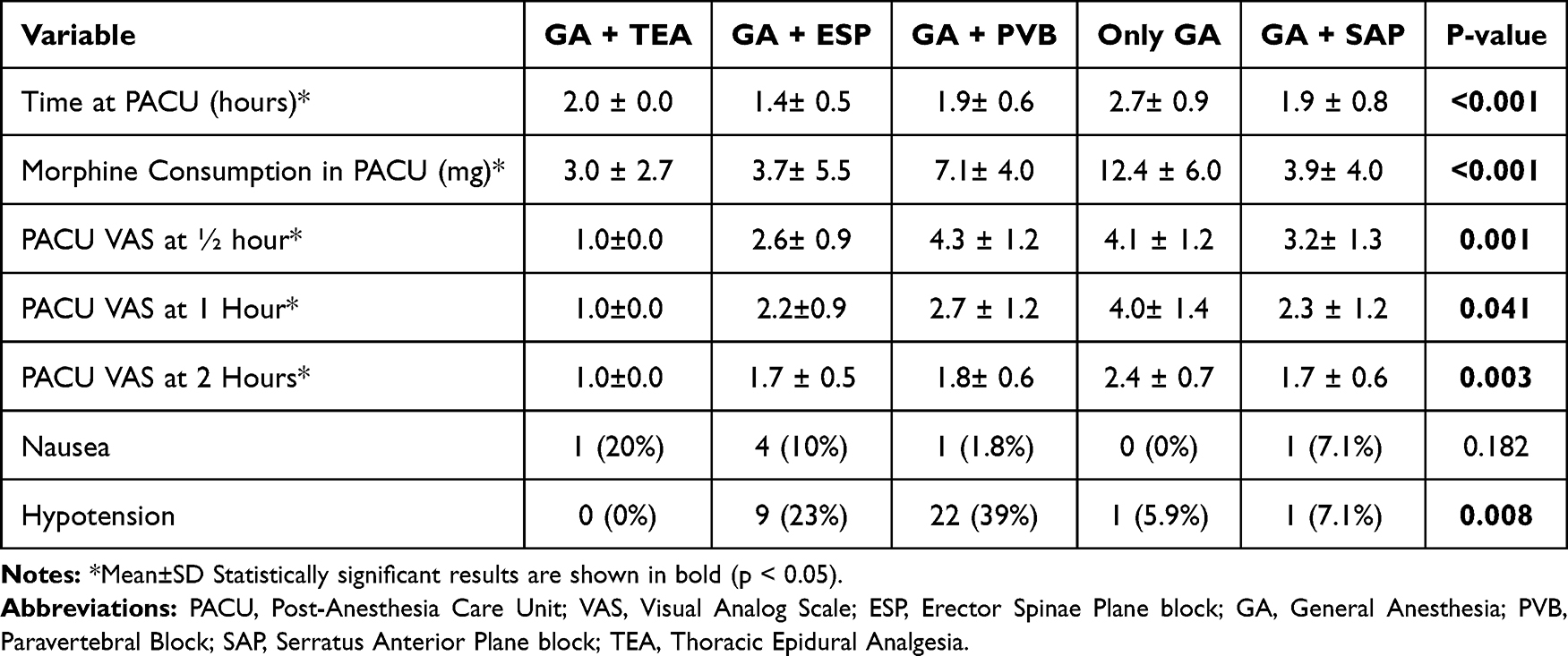 |
Table 3 Clinical Outcomes in the Post-Anesthesia Care Unit by Regional Pain Management Technique |
VAS scores recorded in the PACU at 30 minutes (p = 0.001), 1 hour (p = 0.041), and 2 hours (p = 0.003) demonstrated significantly better pain control in the TEA, ESP, and SAP groups compared to GA and PVB (see Figure 1). Postoperative PACU VAS scores differed across anesthesia groups. At 30 minutes, TEA, ESP, and SAP provided better analgesia than PVB and GA. At 1 hour, TEA and ESP continued to outperform GA, with ESP also better than PVB. By 2 hours, differences between groups diminished, suggesting analgesic effects converge over time. Departmental (DEP) VAS scores at 2 and 24 hours postoperatively also favored the regional anesthesia groups (p < 0.001 and p = 0.01, respectively). Across all time points, the GA group consistently exhibited the highest VAS scores, highlighting the superior analgesic efficacy of TEA, ESP, and SAP blocks during the first 24 hours after surgery.
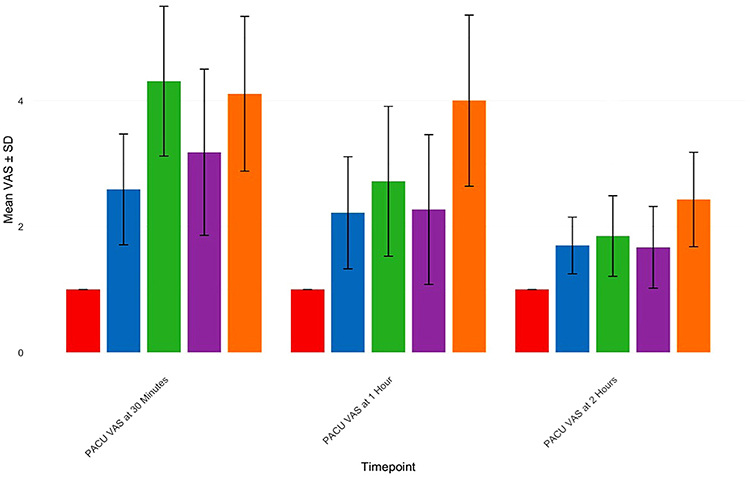 |
Figure 1 Mean VAS Scores in the Post-Anesthesia Care Unit by Regional Pain management Technique at 30 Minutes, 1 Hour, and 2 Hours Postoperatively. Red: GA + Thoracic Epidural Analgesia. Blue: GA + Erector Spinae Plane block. Green: GA + Paravertebral block. Purple: GA + Serratus Anterior Plane block. Orange: Only General Anesthesia. Abbreviations: PACU, Post-Anesthesia Care Unit; VAS, Visual Analog Scale (Static score)*. |
Postoperative Complications and Analgesic Use
The overall complication rate in the surgical department was significantly lower in the ESP and SAP groups compared to others (p = 0.029). Cardiovascular complications were highest in the TEA group (60%, p = 0.005), consistent with the known risk of hypotension associated with this technique. Incidences of urinary retention (p = 0.030) and constipation (p = 0.037) were also significantly higher in the GA group, with the lowest rate observed in the epidural group. Nausea was reported in a small subset of patients, primarily in the TEA and ESP groups, although the difference was not statistically significant (see Table 4).
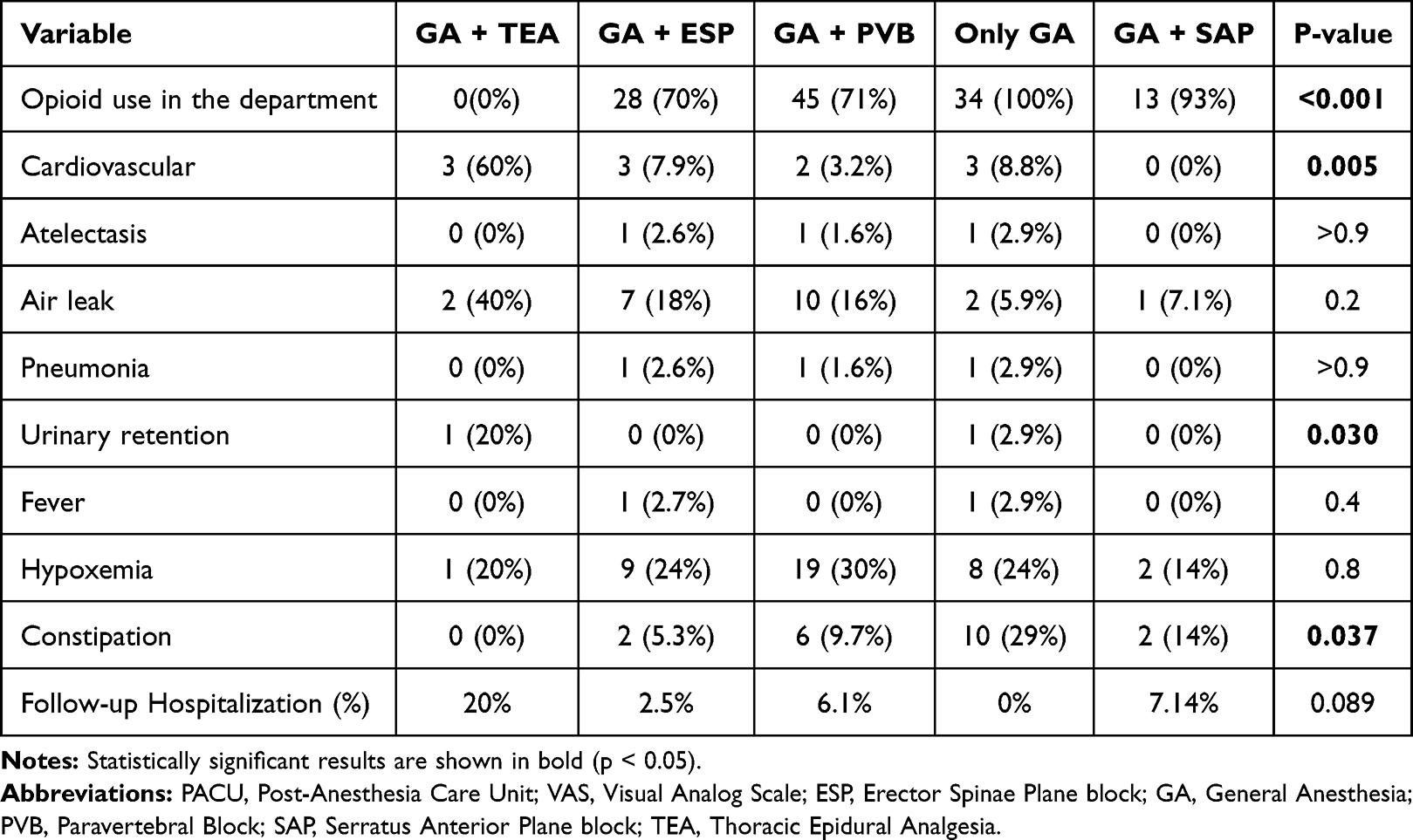 |
Table 4 Postoperative Clinical Outcomes and Complications in the Surgical Department by Regional Pain Management Technique |
Postoperative opioid use in the department was nearly universal in the GA group (100%) and significantly lower in all nerve block groups (p < 0.001). The lowest in-department opioid use was observed in the TEA group (0%), and lowest among block techniques in ESP (70%) and SAP (93%).
Functional Recovery and Hospitalization
No significant differences were found between groups in time to ambulation (mean range: 13–31 hours, p = 0.056), time to drainage removal (p = 0.2), or total length of hospital stay (mean 3.15–4.60 days, p = 0.2). Duration of oxygen therapy also did not differ significantly. No in-hospital mortality was observed in any of the groups. Follow-up hospitalization within 30 days occurred in a small number of patients, with no statistically significant difference between groups; the highest rate was observed in the paravertebral block group (6.2%) (p = 0.089).
Discussion
In this retrospective cohort study, we evaluated the impact of regional anesthesia techniques on postoperative pain control, opioid consumption, and perioperative outcomes in patients undergoing robotic-assisted thoracic surgery (RATS). Specifically, we compared general anesthesia alone with several regional block modalities, including thoracic epidural (TEA), paravertebral block (PVB), erector spinae plane (ESP) block, and serratus anterior plane (SAP) block. Our findings highlight the clinical value of regional pain management techniques in enhancing postoperative recovery and reducing opioid-related burden in thoracic robotic surgeries.
Patients who received general anesthesia alone demonstrated consistently worse outcomes in terms of analgesic requirements and early postoperative pain control. Morphine consumption in the PACU was highest in this group, averaging over 12 mg, and VAS scores remained significantly elevated at all recorded time points. These findings underscore the limitations of systemic analgesia alone in the context of RATS, especially when compared to the improved recovery observed in patients who received peripheral nerve blocks, as demonstrated in previous studies.15,16
Among the regional techniques, TEA offered the lowest VAS scores during the first hours postoperatively, affirming its efficacy in immediate pain control.17 However, one should consider the higher rates of intraoperative vasopressor use (80%). This is consistent with the known physiologic effects of thoracic epidural blockade, including sympathetic chain inhibition, which can lead to hypotension.18 PVB also demonstrated an increased incidence of intraoperative hypotension (39%), likely attributable to similar mechanisms involving sympathetic blockade.18 These hemodynamic effects should be weighed carefully against the analgesic benefits, particularly in patients with cardiovascular comorbidities.
When comparing the peripheral blocks (ESP, PVB, and SAP) with one another, ESP and SAP emerged as favorable options. Both techniques were associated with moderate VAS scores, low morphine requirements (3.75–3.92 mg in PACU), and shorter PACU stays. Notably, the ESP group demonstrated the shortest PACU time (1.41 ± 0.49 hours), indicating a potential advantage in early recovery metrics. Quantitative advantage of using Morphine in PVB group postoperative may explain the failure of block in any patients (7.1 mg vs 3.7 in ESP group vs 3.9 SAP group). PVB, while effective in pain control, was associated with higher rates of hypotension and greater variability in catheter management.
Beyond efficacy, successful implementation of ESP and SAP blocks requires adequate training and experience for anesthesiologists, as proper ultrasound guidance and anatomical knowledge are essential. These techniques are relatively feasible for adoption in other institutions, given appropriate resources and staff familiarity, and may offer potential cost-effectiveness by reducing opioid consumption and PACU duration.19–21 Our findings support the safe use of ESP and SAP blocks in thoracic surgery and align with emerging recommendations for multimodal pain management, highlighting their advantages compared to other regional anesthesia techniques.19,22,23
Postoperative opioid use was nearly universal in the GA group (100%), whereas all regional anesthesia groups required markedly less, demonstrates the efficacy of targeted regional blocks into perioperative protocols for RATS.24 As for post-anesthesia complications were most frequent in the TEA and PVB groups. PACU hypotension occurred in 23% of ESP and 39% of PVB patients, consistent with sympathetic blockade. Nausea and urinary retention (Known side effect of opioid use) were concentrated in the TEA group, while constipation was most prominent in the GA group (29%). Urinary retention was observed only in TEA and GA. The reduction in opioid use observed with regional techniques was associated with fewer complications.
An important clinical endpoint, hospital discharge time, did not differ significantly across groups, although a trend toward earlier discharge was observed in the SAP group (mean, 3.15 days). This outcome may reflect more stable hemodynamic profiles and improved pain control; however, this result was likely influenced by variations in patient characteristics and procedural complexity.
This study has several limitations. As a retrospective analysis from a single tertiary care center, generalizability is limited. Some patient subgroups (particularly TEA and SAP) were relatively small, which may have underpowered certain comparisons and made it more difficult to draw firm conclusions or fully learn from these findings. We acknowledge this have highlighted it to ensure careful interpretation. Nevertheless, the overall cohort was robust, and the distribution of lobectomies and other procedures was comparable between groups, minimizing procedural bias. Additionally, the study reflects real-world clinical practice across a 5-year period and provides a valuable comparative framework for regional anesthesia in the context of robotic thoracic surgery.
Conclusion
Our findings support the routine use of regional anesthesia techniques in patients undergoing robotic-assisted thoracic surgery (RATS), highlighting the potential benefits of Erector Spinae Plane (ESP) and Serratus Anterior Plane (SAP) blocks compared to general anesthesia alone. These techniques were associated with lower VAS scores, reduced opioid consumption, and improved perioperative recovery profiles, without the hemodynamic instability often observed with thoracic epidural analgesia (TEA) or thoracic paravertebral block (PVB).
The ESP block, in particular, can offer practical advantages: it is relatively simple to perform, has a low complication and failure rate, and allows for safe and stable continuous catheter placement. Moreover, it causes minimal hemodynamic disturbance compared to TPVB and TEA, an important consideration for intraoperative management in thoracic robotic procedures.
The SAP block demonstrated results comparable to the ESP block, likely reflecting its effective analgesic coverage of the lateral branches of the intercostal nerves, which innervate the regions commonly involved in thoracic drain placement. These findings also underscore the contribution of thoracic drains to postoperative pain following thoracic surgeries.
While these results are encouraging, the relatively small sample sizes in the TEA and SAP groups should be considered when interpreting their apparent advantages. Future prospective multicenter trials are warranted to validate these findings and to establish standardized regional anesthesia protocols for minimally invasive thoracic surgery.
Abbreviations
ASA, American Society of Anesthesiologists; AUC, Area under the curve; ESP, Erector spinae plane (block); GA, General anesthesia; ICU, Intensive care unit; IQR, Interquartile range; LS, Least squares; PACU, post-anesthesia care unit; PVB, Paravertebral block; RATS, Robotic-assisted thoracic surgery; SAP, Serratus anterior plane (block); SD, Standard deviation; SUMC, Soroka University Medical Center; TEA, Thoracic epidural analgesia; TIVA, Total intravenous anesthesia; VAS, Visual analog scale.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Nagano H, Suda T. Advantages and disadvantages of robotic and uniportal video-assisted thoracoscopic surgery. Video Assist Thorac Surg. 2021;6:14. doi:10.21037/VATS-20-34
2. Veronesi G. Robotic lobectomy and segmentectomy for lung cancer: results and operating technique. J Thorac Dis. 2015;7(Suppl 2):S122. doi:10.3978/J.ISSN.2072-1439.2015.04.34
3. Novellis P, Bottoni E, Voulaz E, et al. Robotic surgery, video-assisted thoracic surgery, and open surgery for early stage lung cancer: comparison of costs and outcomes at a single institute. J Thorac Dis. 2018;10(2):790–798. doi:10.21037/JTD.2018.01.123
4. Louie BE, Farivar AS, Aye RW, Vallières E. Early experience with robotic lung resection results in similar operative outcomes and morbidity when compared with matched video-assisted thoracoscopic surgery cases. Ann Thorac Surg. 2012;93(5):1598–1605. doi:10.1016/J.ATHORACSUR.2012.01.067
5. Duclos G, Charvet A, Resseguier N, et al. Postoperative morphine consumption and anaesthetic management of patients undergoing video-assisted or robotic-assisted lung resection: a prospective, propensity score-matched study. J Thorac Dis. 2018;10(6):3558. doi:10.21037/JTD.2018.05.179
6. Huang L, Shen Y, Onaitis M. Comparative study of anatomic lung resection by robotic vs. video-assisted thoracoscopic surgery. J Thorac Dis. 2019;11(4):1243. doi:10.21037/JTD.2019.03.104
7. McCall P, Steven M, Shelley B. Anaesthesia for video-assisted and robotic thoracic surgery. BJA Educ. 2019;19(12):405. doi:10.1016/J.BJAE.2019.09.002
8. Slinger P, Blank RS, Campos J, Lohser J, McRae K. Principles and practice of anesthesia for thoracic surgery: second edition. Principles Pract Anesthesia Thoracic Surg. 2019;1–1081. doi:10.1007/978-3-030-00859-8/COVER
9. La Via L, Cavaleri M, Terminella A, Sorbello M, Cusumano G. Loco-regional anesthesia for pain management in robotic thoracic surgery. J Clin Med. 2024;13(11):3141. doi:10.3390/JCM13113141
10. Feray S, Lubach J, Joshi GP, et al. PROSPECT guidelines for video-assisted thoracoscopic surgery: a systematic review and procedure-specific postoperative pain management recommendations. Anaesthesia. 2022;77(3):311–325. doi:10.1111/ANAE.15609
11. D’Ercole F, Arora H, Kumar PA. Paravertebral block for thoracic surgery. J Cardiothorac Vasc Anesth. 2018;32(2):915–927. doi:10.1053/J.JVCA.2017.10.003
12. Tulgar S, Selvi O, Senturk O, Ermis MN, Cubuk R, Ozer Z. Clinical experiences of ultrasound-guided lumbar erector spinae plane block for Hip joint and proximal femur surgeries. J Clin Anesth. 2018;47:5–6. doi:10.1016/J.JCLINANE.2018.02.014
13. Krishna SN, Chauhan S, Bhoi D, et al. Bilateral erector spinae plane block for acute post-surgical pain in adult cardiac surgical patients: a randomized controlled trial. J Cardiothorac Vasc Anesth. 2019;33(2):368–375. doi:10.1053/J.JVCA.2018.05.050
14. Khan IA, Siddiqui NH, Ramachandra SS, Nair A. Indications and technique for thoracic segmental spinal anesthesia in clinical practice: a narrative review. Cureus. 2025;17(5). doi:10.7759/CUREUS.84118
15. Kawagoe I, Hayashida M, Satoh D, Kochiyama T, Fukuda M, Kishii J. Postoperative analgesia in patients undergoing robot-assisted thoracic surgery: a comparison between thoracic epidural analgesia and intercostal nerve block combined with intravenous patient-controlled analgesia. Ann Palliat Med. 2021;10(2):1985–1993. doi:10.21037/APM-20-1607
16. Kanani F, Nugzar R, Shimonov M, Akar FA. Comparative analysis of perioperative analgesia methods in thoracic surgery: a literature systemic review. J Clin Med. 2025;14(7):2484. doi:10.3390/JCM14072484
17. Sagiroglu G, Meydan B, Copuroglu E, et al. A comparison of thoracic or lumbar patient-controlled epidural analgesia methods after thoracic surgery. World J Surg Oncol. 2014;12(1):96. doi:10.1186/1477-7819-12-96
18. Hopf HB, Schlaghecke R, Peters J. Sympathetic neural blockade by thoracic epidural anesthesia suppresses renin release in response to arterial hypotension. Anesthesiology. 1994;80(5):992–999. doi:10.1097/00000542-199405000-00007
19. But M, Wernicki K, Zieliński J, Szczecińska W. A comparison of the effectiveness of the serratus anterior plane block and erector spinae plane block to that of the paravertebral block in the surgical treatment of breast cancer—a randomized, prospective, single-blinded study. J Clin Med. 2024;13(16):4836. doi:10.3390/JCM13164836
20. Muhammad QUA, Sohail MA, Azam NM, et al. Analgesic efficacy and safety of erector spinae versus serratus anterior plane block in thoracic surgery: a systematic review and meta-analysis of randomized controlled trials. J Anesthesia Analgesia Critical Care. 2024;4(1):3. doi:10.1186/S44158-023-00138-Y
21. Rim G, Park HJ, Kang S, et al. Serratus anterior plane block for acute pain management after pectus excavatum repair. Front Surg. 2023;10:1305326. doi:10.3389/FSURG.2023.1305326/BIBTEX
22. Van Den Broek RJC, Postema JMC, Koopman JSHA, et al. Continuous erector spinae plane block versus thoracic epidural analgesia in video-assisted thoracoscopic surgery: a prospective randomized open-label non-inferiority trial. Reg Anesth Pain Med. 2025;50(1):11–19. doi:10.1136/RAPM-2023-105047
23. Galande MV, Mahajan HC, Shastri R. Comparing erector spinae plane block with serratus anterior plane block for coronary bypass graft surgery. European J Cardiovasc Med. 2025;15:787–792. doi:10.61336/EJCM/25-08-142
24. Kusano Y, Kawagoe I, Yamaguchi A, et al. Postoperative analgesia following robot-assisted thoracic surgery for mediastinal disease: retrospective comparative study of general anesthesia alone, combined with epidural analgesia, and with ultrasound-guided thoracic paraspinal block. Ann Transl Med. 2023;11(5):206. doi:10.21037/ATM-22-4258
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Case Report: Erector Spinae Block in Perforated Viscus
Rauf J, A M Haji MM
Local and Regional Anesthesia 2023, 16:19-23
Published Date: 16 February 2023
Utility of Ultrasound-Guided Erector Spinae Plane Blocks for Postoperative Pain Management Following Thoracolumbar Spinal Fusion Surgery
Zelenty WD, Li TY, Okano I, Hughes AP, Sama AA, Soffin EM
Journal of Pain Research 2023, 16:2835-2845
Published Date: 16 August 2023
Clinical Value of Continuous Fascia Iliaca Compartment Block in Perioperative Management of Elderly Patients with Intertrochanteric Fracture: A Propensity Score-Matched Retrospective Study
Xu G, Deng Y, Gao H, Wang B, Wang G, Ma J
Therapeutics and Clinical Risk Management 2025, 21:817-827
Published Date: 30 May 2025
Paravertebral Block versus Erector Spinae Plane Block for Postoperative Analgesia and Recovery: A Systematic Review and Meta-Analysis
Ren D, Wang D, Zhang W, Lei L, He X, Yue H
Journal of Pain Research 2025, 18:4509-4526
Published Date: 2 September 2025
Erector Spinae Plane versus Pectoralis Nerve Block for Mastectomy in Cancer Patients: A Retrospective, Multicenter Cohort Study
Yap EN, Wei J, Darling C, Linehan E, Behrends M, Ng KP
Journal of Pain Research 2025, 18:4775-4785
Published Date: 16 September 2025