Back to Journals » Breast Cancer: Targets and Therapy » Volume 17
Naples Prognostic Score (NPS) as a Novel Prognostic Score for Stage III Breast Cancer Patients: A Real-World Retrospective Study
Authors Miao Y, Yang R, Zhang B, Yang J, Yao L, Wang W, Liu X, Guo X, Jia H
Received 3 February 2025
Accepted for publication 30 April 2025
Published 12 May 2025 Volume 2025:17 Pages 403—421
DOI https://doi.org/10.2147/BCTT.S519742
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Robert Clarke
Yongmin Miao,1– 3 Rui Yang,1– 3 Bo Zhang,1– 3 Jun Yang,1– 3 Liang Yao,1– 3 Wanfu Wang,1– 3 Xiaoqing Liu,1– 3 Xiangyang Guo,1– 3 Hongyan Jia4
1Department of Breast Surgery, Cancer Hospital Affiliated to Shanxi Medical University, Taiyuan, People’s Republic of China; 2Department of Breast Surgery, Shanxi Province Cancer Hospital, Taiyuan, People’s Republic of China; 3Department of Breast Surgery, Shanxi Hospital Affiliated to Cancer Hospital, Chinese Academy of Medical Sciences, Taiyuan, People’s Republic of China; 4Department of Breast Surgery, First Hospital of Shanxi Medical University, Taiyuan, People’s Republic of China
Correspondence: Hongyan Jia, Department of Breast Surgery, First Hospital of Shanxi Medical University, Taiyuan, People’s Republic of China, Email [email protected]
Objective: This study aims to explore whether Naples prognostic score (NPS) serves as a novel and original prognostic tool for predicting long-term survival in stage III breast cancer patients undergoing operation.
Methods: This retrospective study included 306 cases of stage III breast cancer patients hospitalized in our hospital from January 2014 to December 2018. In this study, NPS was based on five objective markers: (1) serum albumin level; (2) total cholesterol; (3) neutrophil to lymphocyte ratio; (4) lymphocyte to monocyte ratio. Survival curves of DFS and OS differences were visualized by Kaplan–Meier method and Log rank test. The variables with p < 0.05 in univariate analysis were performed in the multivariate Cox proportional hazard model analysis, and the p-values < 0.05 was considered the underlying independent variables. Nomogram was constructed by the multivariate Cox proportional hazard model analysis.
Results: Significant variations for DFS and OS categorized according to prognostic risk for the different NPS (DFS: χ2=24.926, P < 0.0001; OS: χ2=31.207, P < 0.0001). According to multivariable Cox analysis, NPS was an independent prognostic factor of DFS [Group 0 had significantly better prognosis than group 1 (HR = 2.733, 95% CI: 1.446– 5.166, P = 0.002) and group 2 (HR = 4.990, 95% CI: 2.555– 9.746), P < 0.001)] and OS [Group 0 had significantly better prognosis than group 1 (HR = 2.437, 95% CI: 1.288– 4.610, P = 0.006) and group 2 (HR = 5.707, 95% CI: 2.900– 11.231), P < 0.001)], respectively. Nomogram prognostic model exhibited excellent predictive performance on DFS [C-index: 0.692 (95% CI: 0.584– 0.782)] and OS [C-index: 0.711 (95% CI: 0.606– 0.797)] for stage III breast cancer.
Conclusion: NPS serves as a predictive tool for assessing the prognosis of stage III breast cancer after surgery. Nomogram prognostic model based on NPS show good prediction ability.
Keywords: breast cancer, Naples prognostic score, NLR, LMR, albumin
Introduction
According to recent statistics on cancer indicate that breast cancer is one of the common malignant tumors and the leading cause of cancer-related illnesses and death among females cancer all over the world.1 In addition to surgery as the major treatment, the increase in immunotherapy or radiotherapy on the basis of cytotoxic chemotherapy and endocrine therapy offers a new option to improve the prognosis of breast cancer patients.2 Although many cancer patients are successfully treated through early diagnosis and improved treatment strategies, about 20–25% of patients are diagnosed with locally advanced cancer.3 There is evidence to suggest that approximately 30–40% of invasive cancer patients will eventually develop metastatic cancer, and their 5-year survival rate may be lower than 30%.4,5 Stage III breast cancer is particularly common, with an incidence rate of about 30%.6 Although surgical resection significantly improves the survival rate of stage III breast cancer patients, postoperative prognosis monitoring for these patients remains a significant challenge due to the high heterogeneity of the disease. The overall prognosis of stage III breast cancer patients is still not promising. Nowadays, the widely accepted cancer prognosis assessment is based on postoperative pathological indicators, such as TNM stage, grade, hormone receptor status, HER2 status.7,8 Moreover, the genomic assays like Oncotype DX, PAM50 were also used to evaluate the prognosis of breast cancer patients. However, these emerging biomarkers were obtained after operation and not convenient. Therefore, the construction of preoperatively available prognostic marker can help clinicians in clinical decision-making and reasonable treatment decisions.
It is widely believed that the prognosis of breast cancer patients is not only influenced by cancer biology but also by host-related conditions.9,10 More and more evidence confirms that systemic inflammation plays a crucial biological role in the proliferation, metastasis, invasion, and angiogenesis of malignant tumors.11,12 The biochemical mechanism by which systemic inflammatory molecules affect the secretion of inflammatory cytokines by tumor cells may reflect the degree of biological response of tumor cells. The inflammatory, nutritional, and immune conditions of cancer patients are considered closely related to the outcome of breast cancer.13,14 Previous studies have shown that the inflammation-related prognostic indicators, such as neutrophil to lymphocyte ratio (NLR), lymphocyte to monocyte ratio (LMR), and fibrinogen-to-albumin ratio (FAR) were beneficial for assessing the outcome in breast cancer.15–17 Nevertheless, these predictive factors are still insufficient to fully reflect prognosis and overall patient condition through a single inflammation-related indicator. Additionally, several scoring systems for reflecting host nutritional or immunological condition, such as Nutritional risk index (NRI), systemic immune-inflammatory index (SII), are associated with tumor prognosis.18,19 However, the nutritional, inflammatory or immunological predictors are to some extent insufficient, and the results are still controversial. Therefore, there is an urgent need for an increasing number of comprehensive prognostic model associated with inflammation and nutrition.
Naples Prognostic Score (NPS), a new scoring system combining inflammatory with nutritional biomarkers, is consist of serum albumin (ALB), total cholesterol (CHOL), NLR and LMR.20 Albumin is a versatile serum protein synthesized by the liver, playing a key role in maintaining oncotic pressure, transporting hormones, and modulating inflammation, and its levels are influenced by nutritional status, systemic inflammation, and liver function. Cholesterol is a multifunctional lipid molecule essential for cell membrane integrity, steroid hormone synthesis, and bile acid production, also suppress Treg function, promoting autoimmunity. Tumor-associated neutrophils (TANs) promote immune evasion, and tumor associated macrophages (TAMs, M2 phenotype) promote metastasis. High NLR predicts poor prognosis in some cancers, and associated with resistance to immunotherapy. Low LMR correlates with worse survival, and may predict response to immunotherapy. This score has been widely used to study various gastrointestinal and other malignancies, such as colorectal cancer, gastric cancer, and esophageal carcinoma.21–23 The clinical significance of NPS in stage III breast cancer patients, particularly in those receiving radical resection, remains uncertain. Therefore, the present study aims to investigate the relationship of NPS with clinicopathologic characteristics, and evaluate the prognostic significance of NPS on the long-term survival in stage III breast cancer patients.
Methods
Patients Section
All of 306 stage III breast cancer patients were treated by curative surgical resection in Cancer Hospital Affiliated to Shanxi Medical University from January 2014 to December 2018 were enrolled in the current study. The data from electronic medical records were collected, such as clinical pathological data, follow up information. This study were received approval from Ethics Committee of Shanxi Cancer Hospital, and in accordance with the declaration of Helsinki. At the same comment, written informed consent was obtained from the enrolled patients, and authorizing the use of their data for scientific analysis.
Inclusion and Exclusion Criteria
According to the histopathology, all enrolled patients were diagnosed by stage III breast cancer after surgery. Inclusion criteria were as follows: (1) diagnosed with stage III breast cancer by histopathology and immunohistochemistry; (2) confirmed by only breast cancer, and not in combination with other malignant tumors or distant organ metastasis; (3) patients with no prior anti-tumor treatment; (4) availability of complete blood routine, biochemical examination, tumor marker examination, and coagulation function within one week before surgery; (5) completely followed up data and medical records information. Exclusion criteria were as follows: (1) Insufficient heart, lung, brain, liver and renal function; (2) definite inflammatory, infectious, hematologic diseases, or other autoimmune diseases via electronic medical record affecting nutritional and immune condition; (3) accompanied by potential diseases that were difficult to control, and could not be treated surgically.
Definition of NPS
A common laboratory blood test was performed, and the results were obtained from department of breast cancer in Shanxi Cancer Hospital within one week before surgery. Naples prognostic score (NPS) was a scoring system applied to predict the prognosis of cancer patients. Peripheral neutrophil count was divided by lymphocyte count prior to surgery to calculate the NLR (neutrophil to lymphocyte ratio). Peripheral lymphocyte count was divided by monocyte count prior to surgery to calculate the LMR (lymphocyte to monocyte ratio). In our cohort, the best critical value for NLR and LMR by ROC with the highest sensitivity and specificity to predict OS. In this study, NPS was based on five objective markers: (1) serum albumin level (≤4.0 g/L = 1 point, >4.0 g/L = 0 point); (2) total cholesterol (≤3.9mmol/L = 1 point, >3.9mmol/L = 0 point); (3) neutrophil to lymphocyte ratio (≤1.8 = 0 point, >1.8 = 1 point); (4) lymphocyte to monocyte ratio (≤3.6 = 1 point, >3.6 = 0 point). Patients were categorized into three groups based on their NPS: 1) Group 1: NPS 0 group (0 point); Group 2: NPS 1 group (1 point); and Group 3: NPS 2–4 group (ranging from 2 to 4 points).
Treatment
All enrolled patients were received surgery, including breast conserving surgery and mastectomy. According to the pathological molecular typing after surgery, these patients were received chemotherapy (such as anthracycline and paclitaxel), radiotherapy, endocrine therapy (tamoxifen, anastrozole, letrozole), and targeted therapy (trastuzumab and pertuzumab).
Followed-Up
The enrolled patients were followed up by telephone interviews, inpatient services, or outpatient services to obtain their health status. The follow up deadline concluded in June 2023. The main outcome was specified as either disease free survival (DFS) or overall survival (OS). DFS was defined as time from the surgical procedure to the first disease recurrence, death or last follow-up. OS was defined as time from the surgical procedure to death or last follow-up. Patients were followed up every 3 months for the first 2 years, then every 6 months for the following 2 years and annually thereafter. Perform physical examination, laboratory examination, breast ultrasound, mammography, CT or MR on patients to evaluate primary tumors and distant metastases.
Statistical Methods
The IBM SPSS Statistics 22.0 (SPSS, Inc., Chicago, IL, USA) and R 4.2.2 (R Foundation for Statistical Computing, Vienna, Austria) were used to perform statistical analyses. The URL for R is: http://www.R-project.org/. Continuous variables were presented by median and interquartile range, and categorical variables were expressed as percentages with their corresponding numbers in parentheses. Fisher exact test and chi-square test were performed to assess the associations between NPS and clinicopathological characteristics. Survival curves of DFS and OS differences were visualized by Kaplan–Meier method and Log rank test. The variables with p < 0.05 in univariate analysis were performed in the multivariate Cox proportional hazard model analysis, and the p-values < 0.05 was considered the underlying independent variables. Receiver operating characteristic (ROC) and were assessed the cutoff value. Nomogram was constructed by the multivariate Cox proportional hazard model analysis. The concordance index (C-index) and the area under the AUC value were used to measure the degree of distinctiveness of the nomogram. Calibration curve was used to provides an intuitive evaluation of the calibration for the nomogram. Decision curve analysis was used to confirm the clinical benefit of the nomogram. Statistical tests with p-values < 0.05 were significantly difference.
Results
Construction and Evaluation of NPS with Survival
In the current study, NPS was constructed by serum albumin level (ALB), total cholesterol level (CHOL), NLR and LMR. Based on NPS, there were 74 cases for NPS 0 point divided into Group 1, 162 cases for NPS 1 point divided into Group 2, and 70 cases for NPS 2–4 points divided into Group 3, respectively. Among NPS groups, the mean duration of DFS was 68.86 months, while the mean OS was 79.67 months in Group 1 (NPS 0 point); the mean duration of DFS was 56.86 months, while the mean OS was 70.46 months in Group 2 (NPS 1 point); the mean duration of DFS was 49.25 months, while the mean OS was 55.78 months in Group 3 (NPS 2–4 point); respectively. Significant variations for DFS and OS categorized according to prognostic risk for the different NPS (DFS: χ2=24.926, P < 0.0001; OS: χ2= 31.207, P < 0.0001), and displayed in Figure 1A and B, respectively.
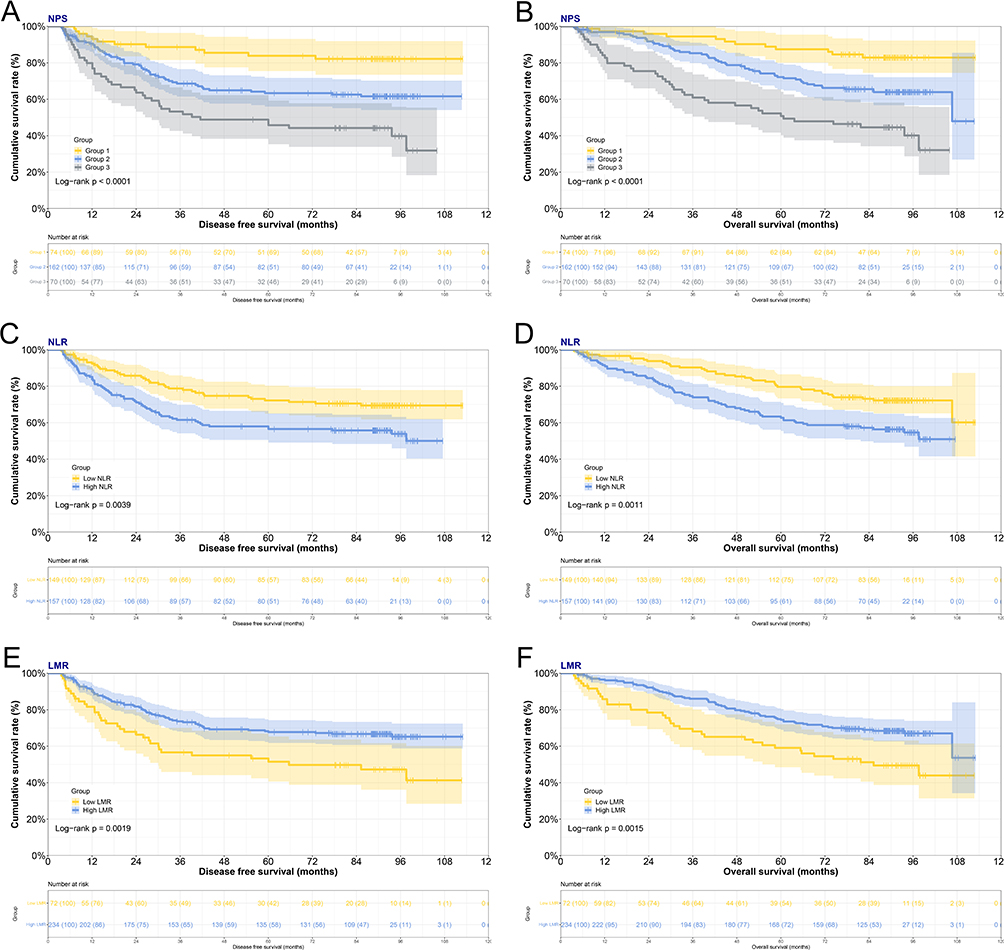 |
Figure 1 Kaplan-Meier survival analysis based on Naples Prognostic Score (NPS) / neutrophil to lymphocyte ratio (NLR) / lymphocyte to monocyte ratio (LMR) and group. (A) Significant differences in the disease free survival among stage III breast cancer patients were found with three groups by NPS (P < 0.0001). (B) Significant differences in the overall survival among stage III breast cancer patients were found with three groups by NPS (P < 0.0001). (C) Significant differences in the disease free survival among stage III breast cancer patients were found with two groups by NLR (P=0.0039). (D) Significant differences in the overall survival among stage III breast cancer patients were found with three groups by NPS (P=0.0011). (E) Significant differences in the disease free survival among stage III breast cancer patients were found with two groups by LMR (P=0.0019). (F) Significant differences in the overall survival among stage III breast cancer patients were found with three groups by LMR (P=0.0015). |
According to the NLR, 149 cases were in low NLR group, 157 cases were in high NLR group. In low NLR group, the mean duration of DFS was 61.20 months, while the mean OS was 74.74 months. By contrast, in high NLR group, the mean DFS was 55.00 months, and the mean OS was 64.19 months. Significant variations for DFS and OS categorized according to prognostic risk for the different NLR (DFS: χ2= 8.330, P = 0.0039; OS: χ2=10.574, P = 0.0011), and displayed in Figure 1C and D, respectively. According to the LMR, 72 cases were in low LMR group, 234 cases were in high LMR group. In low LMR group, the mean duration of DFS was 47.87 months, while the mean OS was 59.12 months. In comparison, in high LMR group, the mean DFS was 61.15 months, and the mean OS was 72.47 months. Significant variations for DFS and OS categorized according to prognostic risk for the different LMR (DFS: χ2=9.626, P = 0.0019; OS: χ2= 10.074, P = 0.0015), and displayed in Figure 1E and F, respectively.
According to the ALB based on serum albumin level (≤4.0 g/L = 1 point, >4.0 g/L = 0 point), 18 cases were in low ALB group, 288 cases were in high ALB group. In low ALB group, the mean duration of DFS was 42.36 months, while the mean OS was 46.55 months. In comparison, in high ALB group, the mean DFS was 59.00 months, and the mean OS was 70.75 months. Significant variations for DFS and OS categorized according to prognostic risk for the different level of ALB (DFS: χ2= 10.221, P = 0.0014; OS: χ2=14.664, P = 0.0001), and displayed in Figure S1A and B, respectively. According to the CHOL based on total cholesterol (≤3.9mmol/L = 1 point, >3.9mmol/L = 0 point), 70 cases were in low CHOL group, 236 cases were in high CHOL group. In low CHOL group, the mean duration of DFS was 53.00 months, while the mean OS was 63.73 months. In comparison, in high CHOL group, the mean DFS was 59.51 months, and the mean OS was 70.99 months. Significant variations for DFS and OS categorized according to prognostic risk for the different level of CHOL (DFS: χ2= 5.830, P = 0.0158; OS: χ2= 7.138, P = 0.0075), and displayed in Figure S1C and D, respectively.
Patients’ Baseline Features and Association Between NPS and Clinicopathological Parameters of Stage III Breast Cancer Patients
This study ultimately enrolled 306 stage III breast cancer patients, who underwent curative surgical resection at the Department of Breast Surgery, Shanxi Cancer Hospital from January 2014 to December 2018 (Figure S2). Based on TNM stage, all patients were stage III breast cancer, including stage IIIA 176 (57.5%) cases, stage IIIB 3 (1.0%) cases, stage IIIC 127 (41.5) cases, respectively. According to molecular subtypes for breast cancer, there were five molecular subtypes, including Luminal A 52 (17.0%) cases, Luminal B HER2+ 50 (16.3%) cases, Luminal B HER2- 76 (24.8%) cases, HER2 enriched 63 (20.6%) cases, Triple negative subtype 65 (21.2%) cases, respectively. Of all clinicopathologic features, low expression of ER (P = 0.043), positive expression of E-cad (P = 0.014), no chemotherapy (P = 0.027) were associated with higher NPS (Table 1).
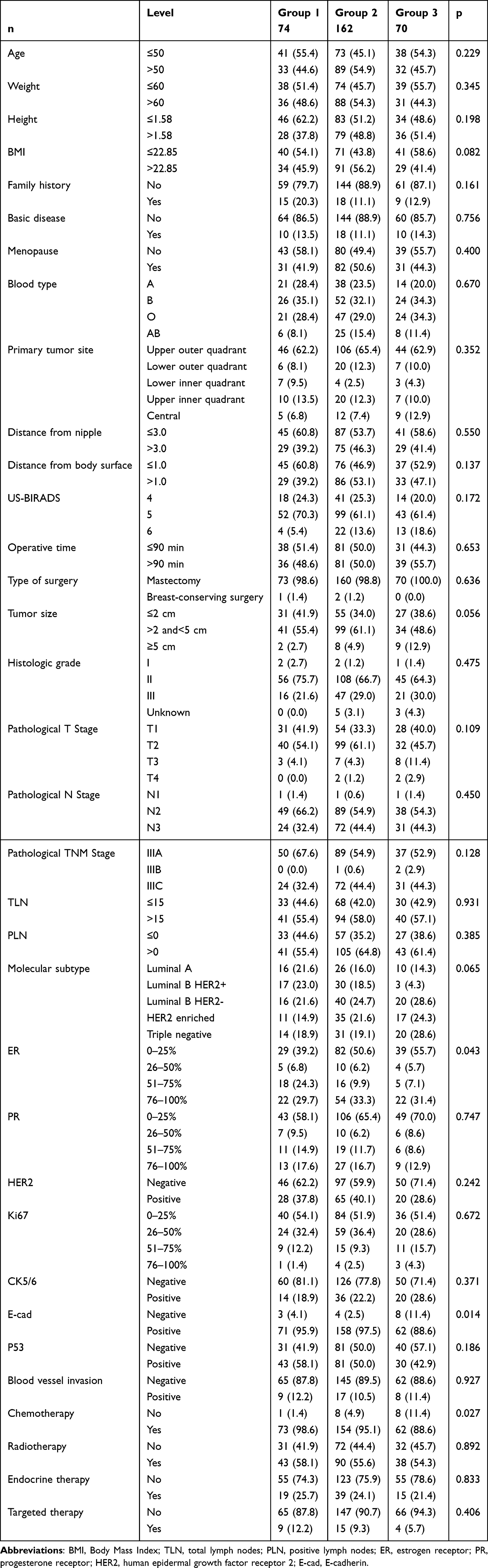 |
Table 1 Relationships Between Naples Prognostic Score (NPS) and Clinicopathological Characteristics for Stage III Breast Cancer |
Comparison of Performance of NPS Based on Hematological Parameters
The common laboratory blood test was performed and the results were obtained within one week before surgery. In our cohort, the best critical value for neutrophil to lymphocyte ratio (NLR 1.8) and lymphocyte to monocyte ratio (LMR 3.6) by ROC with the highest sensitivity and specificity to predict OS. High NLR level (P < 0.001) and low LMR level (P < 0.001), low ALB level (P < 0.001), low CHOL level (P < 0.001), were related to higher NPS. These enrolled hematological parameters were divided into two groups by median values. Of these hematological parameters, low ALT level (P = 0.027), IBIL (P = 0.029), CEA (P = 0.044), high D-Dimer level (P = 0.049), low red blood cell (P = 0.044), hemoglobin (P = 0.009), neutrophil (P < 0.001), lymphocyte (P = 0.029), basophil (P = 0.015) were associated with higher NPS (Table 2).
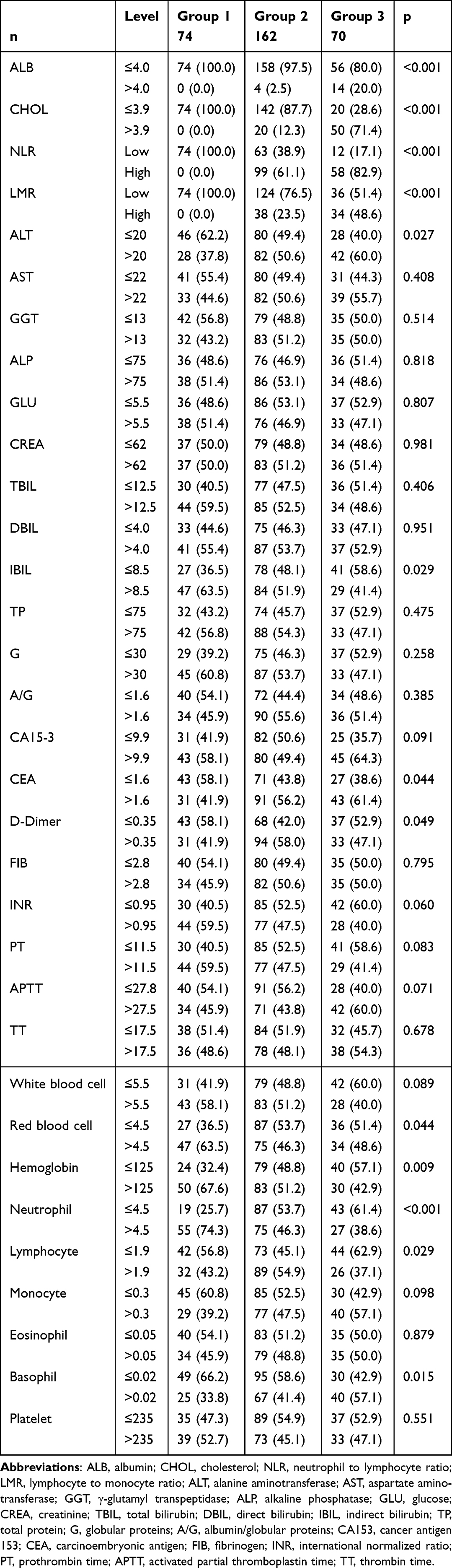 |
Table 2 Comparisons of Common Hematological Parameters Among the Three Groups According to Naples Prognostic Score (NPS) |
Univariate and Multivariate Analyses of Prognostic Factors for DFS and OS
We conducted univariate and multivariate Cox regression analysis on DFS and OS for stage III breast cancer. The potential prognostic factors affecting DFS and OS were demonstrated, as shown in Table 3 and 4. Univariate analysis demonstrated that family history, TLN, PLN, molecular subtype, radiotherapy, NPS, NLR, AST, D-D, white blood cell were significantly related to DFS. The multivariate analysis identified family history, molecular subtype, radiotherapy, NPS, and D-D were as potential prognostic factors for DFS in Table 3. At the same time, univariate analysis showed that family history, TLN, PLN, molecular subtype, radiotherapy, NPS, ALB, NLR, AST, D-D were dramatically correlated with OS. Additionally, the multivariate analysis revealed that family history, molecular subtype, radiotherapy, NPS, ALB, NLR, AST, D-D were prognostic factors for OS in Table 4.
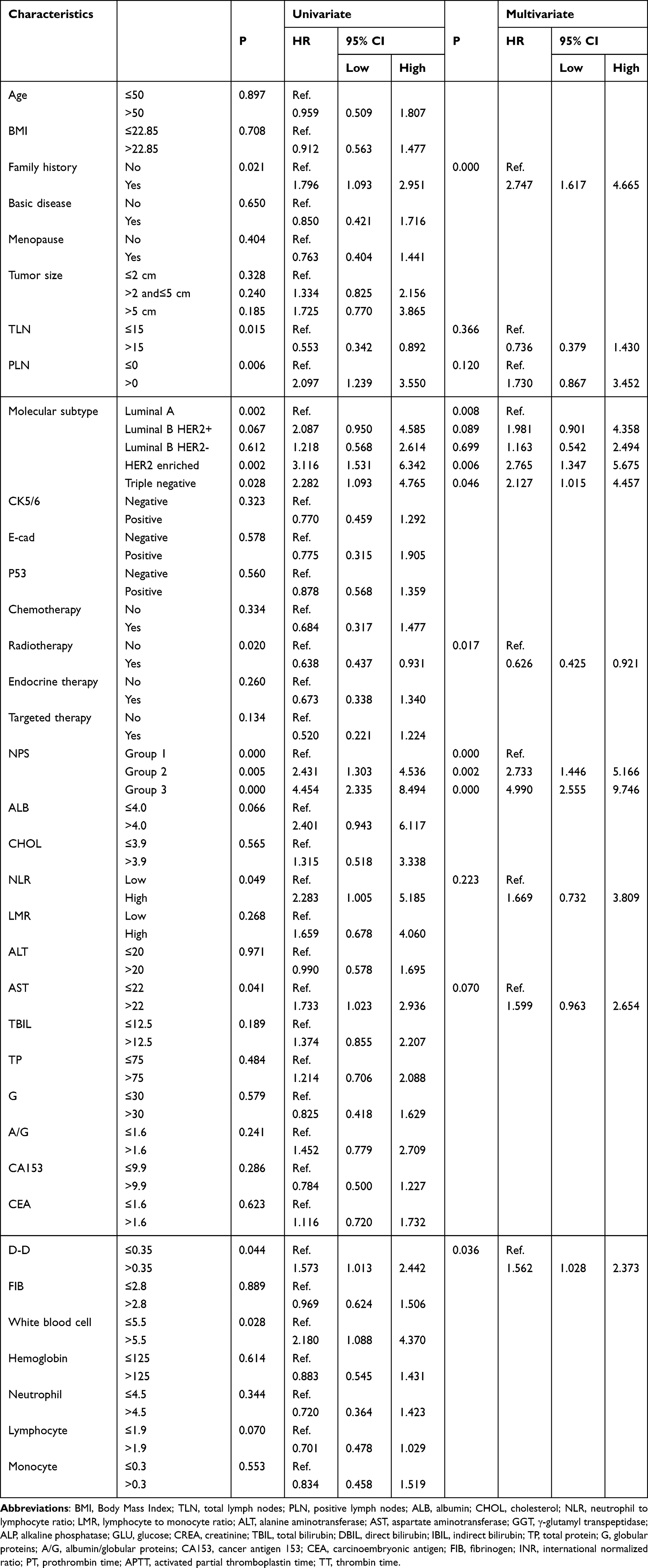 |
Table 3 The Prognostic Factors for Disease Free Survival According to Univariate and Multivariate Analyses |
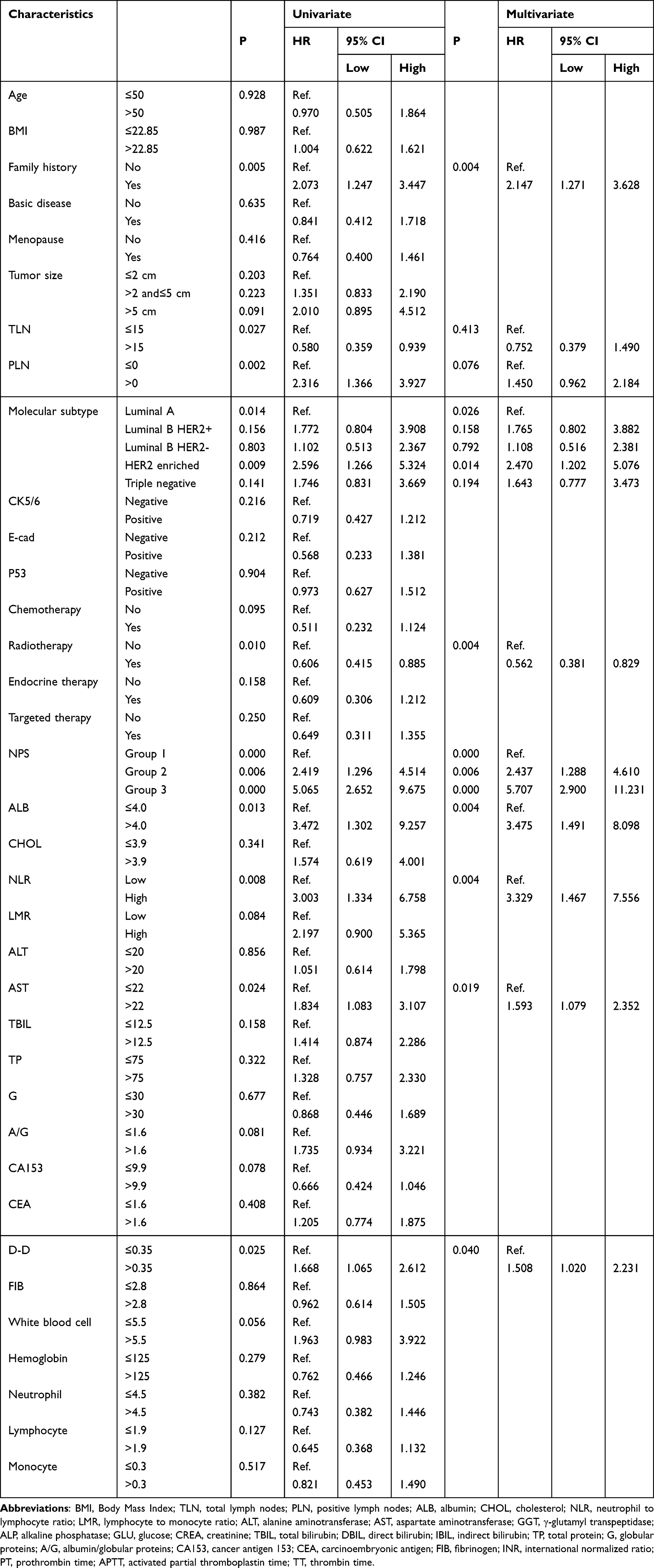 |
Table 4 The Prognostic Factors for Overall Survival According to Univariate and Multivariate Analyses |
NPS group was an independent prognostic factor of DFS [Group 0 had significantly better prognosis than group 1 (HR = 2.733, 95% CI: 1.446–5.166, P = 0.002) and group 2 (HR = 4.990, 95% CI: 2.555–9.746), P < 0.001)], as shown in Table 3. NPS group was also an independent prognostic factor of OS [Group 0 had significantly better prognosis than group 1 (HR = 2.437, 95% CI: 1.288–4.610, P = 0.006) and group 2 (HR = 5.707, 95% CI: 2.900–11.231), P < 0.001)], as shown in Table 4.
Building and Validating a Nomogram Prognostic Model
We conducted Nomogram prognostic model on DFS and OS for stage III breast cancer. The C-index for this Nomogram prognostic model predicting DFS and OS were 0.692 (95% CI: 0.584–0.782) and 0.711 (95% CI: 0.606–0.797). The parameters with P < 0.05, including family history, molecular subtype, radiotherapy, NPS, and D-D, were selected based on multivariate analyses to construct a Nomogram prognostic model of DFS in Figure 2A. Furthermore, the parameters with P < 0.05, including family.history, molecular subtype, radiotherapy, NPS, ALB, NLR, AST, and D-D by multivariate analyses were chose to comprise nomogram for Nomogram prognostic model of OS in Figure 2B. The Nomogram prognostic model shown that the breast cancer in Group 2 and Group 3 had a worse DFS and OS than those in Group 1. A calibration curve was conducted, and the multivariate Cox regression model was developed using 1000 re-samplings of the original data to predict the 3- and 5-year DFS and OS of stage III breast cancer patients, which was identified using R software. The 1-, 3- and 5-year DFS and OS predicted by Nomogram prognostic model and the actual DFS and OS in the predictions and actual observations demonstrated an acceptable degree of agreement, with the calibration curve essentially floating around 45° (Figure 3A-F). Decision curve analysis was applied to assess the extent of benefit. Furthermore, Nomogram prognostic model constructed showed a superior positive net benefit compared to the NPS in predicting 3- and 5-year DFS, and predicting 3- and 5-year OS (Figure 4A-D). Besides, Nomogram prognostic model indicated a better positive net benefit than NLR in predicting 3- and 5-year DFS or OS (Figure S3A-D), and LMR in predicting 3- and 5-year DFS or OS (Figure S4A-D). These results were demonstrated that its clinical applicability and net benefit over a broad range of thresholds.
 |
Figure 2 Nomogram prognostic model for predicting 1-, 3- and 5-year (A) disease free survival (DFS) and (B) overall survival (OS) of stage III breast cancer patients using independent prognostic factors by multivariate COX analyses. |
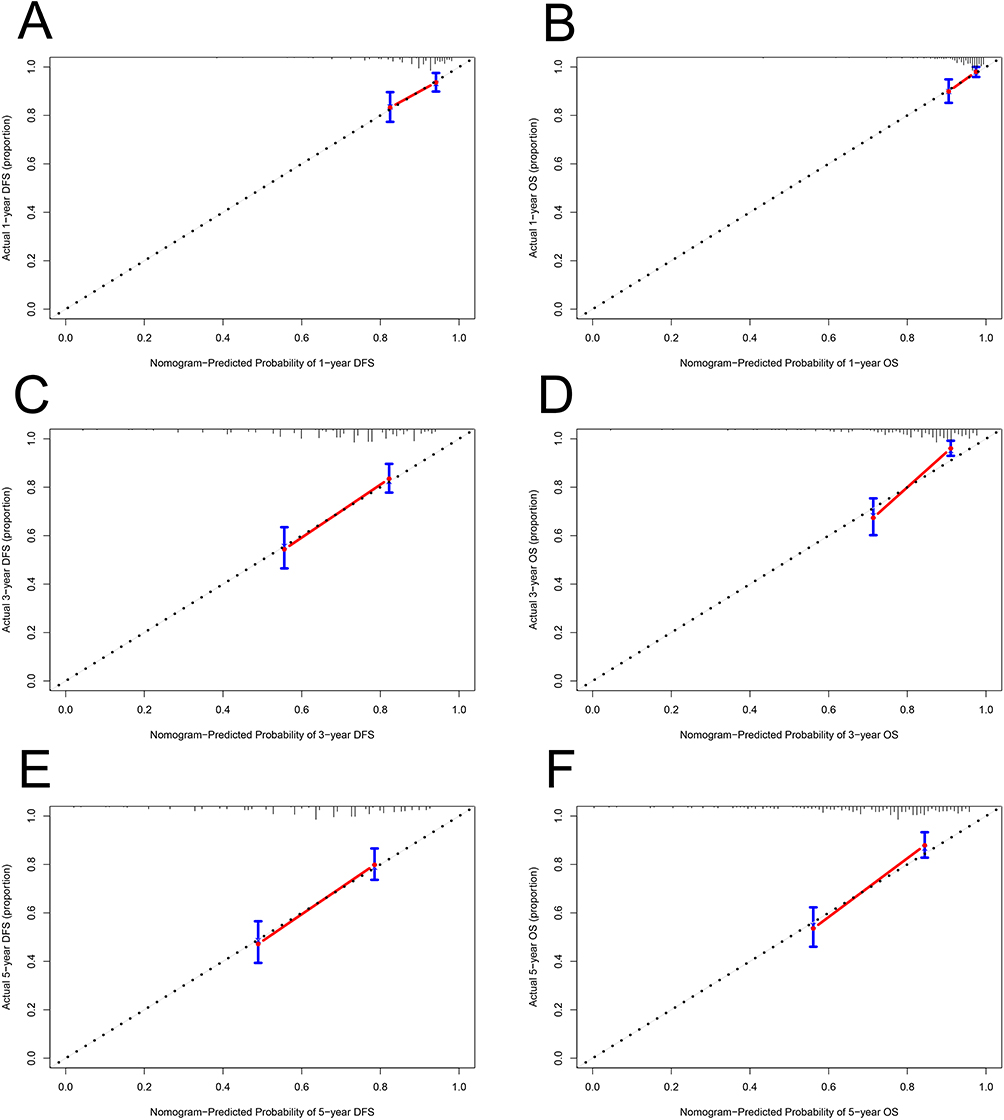 |
Figure 3 Calibration curves for predicting disease free survival (DFS) and overall survival (OS) at 1-, 3- and 5- year rates of stage III breast cancer patients using the nomogram closely matched the actual observed values. (A) Calibration curves for predicting DFS at 1-year rate. (B) Calibration curves for predicting OS at 1-year rate. (C) Calibration curves for predicting DFS at 3-year rate. (D) Calibration curves for predicting OS at 3-year rate. (E) Calibration curves for predicting DFS at 5-year rate. (F) Calibration curves for predicting OS at 5-year rate. |
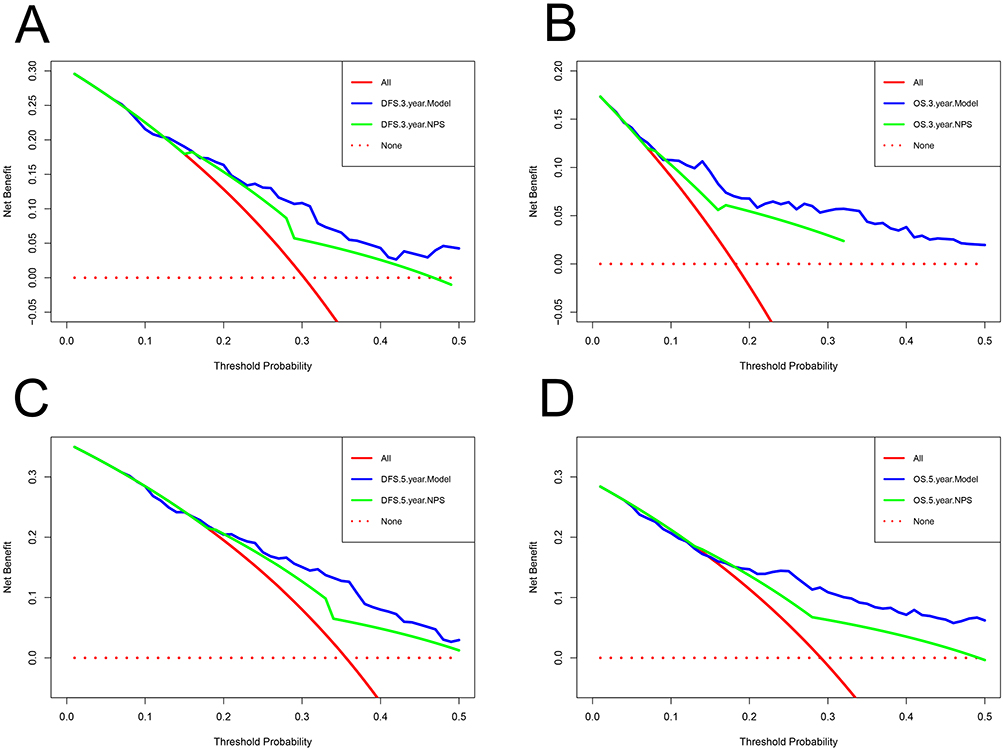 |
Figure 4 Decision curve analysis (DCA) curves for evaluating clinical usefulness of the condition survival Nomogram prognostic model and NPS for 3- and 5- year disease free survival (DFS) and overall survival (OS) rates. (A) DCA curves for evaluating clinical usefulness of the condition survival Nomogram prognostic model and NPS for 3- year DFS rate. (B) DCA curves for evaluating clinical usefulness of the condition survival Nomogram prognostic model and NPS for 3- year OS rate. (C) DCA curves for evaluating clinical usefulness of the condition survival Nomogram prognostic model and NPS for 5- year DFS rate. (D) DCA curves for evaluating clinical usefulness of the condition survival Nomogram prognostic model and NPS for 5- year OS rate. |
Discussion
Some traditional cancer predictors, including TNM stage, tumor size, histological type, NLR and LMR, reflect one-dimensional biological characteristics and have certain limitations. The nodal status, lymphovascular infiltration, and lymphotropic pattern (such as micropapillary element) are aslo uesd to evaluate the survival of breast cancer patients.24,25 Recently, studies have been established extensively on the application of NPS to predict the outcome of different malignant tumors due to the integration of multiple indicators of inflammation, nutrition, and immune condition. There is still controversy over the NPS threshold for different types of malignancies and treatment contexts. Systemic inflammatory and nutritional indicators are convenient for predicting the prognosis of breast cancer patients after operation. Although some researches demonstrated the preoperative condition, the current study evaluated that NPS can be applied to a predictive systemic inflammatory and nutritional biomarker in stage III breast cancer undergoing surgery compared to single inflammation related indicator, such as NLR or LMR. Despite its potential utility, limited researches have investigated the predictive value of NPS substantially in the context of stage III breast cancer. Eventually, 306 stage III breast cancer patients were enrolled and stratified into three groups according to the NPS. Our study demonstrated that NPS acted as a potential indicator of DFS and OS in stage III breast cancer, and the patients exhibiting a low NPS prolonged the survival time.
As is well known, peripheral blood inflammation indicators can reflect the status of immune inflammation.26,27 Inflammation leads to the aggregation of neutrophils and monocytes, promoting the development of cancer by producing and releasing large amounts of inflammatory mediators, transforming factors, cytokines, and chemokines.28,29 Neutrophils are related to the severity of the disease, and low level of absolute neutrophil count is associated with improved prognosis after cancer treatment.30 Monocytes can differentiate into tumor associated macrophages (TAMs) in cancer tissue, which promote angiogenesis and tumor progression and can be used to predict tumor prognosis.31 On the contrary, the local immune response caused by inflammation leads to an increase in lymphocytes, which can play a significant role in anti-cancer activity to some extent.32 Therefore, changes in immune and inflammatory indicators, such as NLR and LMR, can undoubtedly provide a powerful reference for evaluating the prognosis of malignant tumors; and several studies have also explored the relationship between biomarkers and breast cancer prognosis.33,34 In our study, patients with low level of NLR or high level of LMR had survived longer than those with high level of NLR or low level of LMR, respectively. Moreover, the multivariate Cox analysis also showed that NLR was the prognostic factor for overall time. And this is generally consistent with previous research, such as Ethier JL’s study,35 Tokumaru Y’s study.36 Therefore, we hypothesize that elevated NLR may be used to predict the cancer prognosis, as it reflects the balance between inflammation and immune responses in tumor microenvironment.
As is known to all, nutritional status plays a crucial role in cancer progression, affecting the body’s oxidative stress levels and altering tissue metabolism.37 Nutritional predictors, such as ALB and CHOL, are closely related to the advancement of malignant tumors.38,39 The level of ALB is remarkable marker in clinical front-line of gastrointestinal surgery, which does not only effectively present the nutritional status of liver function and systemic inflammation, but also acts as a crucial indicator in cancer prognosis.40 Cholesterol inhibits transmembrane signaling and participates as an important immune component.41 One study has shown that low level of CHOL in patients with colorectal cancer (CRC) was an important prognostic factor for survival time after operation, and related to the poor prognosis of CRC.42 In our study, our study demonstrated that ALB acted as a potential indicator of OS in stage III breast cancer, and the patients exhibiting a high level of ALB prolonged the survival time. Although the level of CHOL was related to the prognosis of stage III breast cancer, CHOL was not the independent factor for the survival time. Additionally, studies have showed that the integrated assessment of cancer, inflammation, and nutrition highlights the importance of comprehensive assessment in guiding tumor treatment.
Based on the above biological mechanisms, it is completely feasible to anticipate expected cancer patient survival rates with NPS. NPS, as a new and original scoring system, has been widely used to construct the Nomogram prognostic model for some malignant tumors.43–45 This study demonstrated that patients with a high NPS exhibited a poorer prognosis and shorter survival time (DFS, HR = 4.990, 95% CI: 2.555–9.746, P < 0.001; OS: HR = 5.707, 95% CI: 2.900–11.231, P < 0.001) for stage III breast cancer. Studies also demonstrated that application of neutrophils, monocyte and lymphocytes was applied to immunotherapy. And NLR or LMR were couple of the comprised of NPS. Then, breast cancer patients with high level of NLR had worse prognosis and short survival time (OS: HR: 3.329, 95% CI: 1.467–7.556, P = 0.004). Moreover, the multivariate analysis identified family history, molecular subtype, radiotherapy, NPS, and D-D as potential prognostic factors. The application of NPS can provide reference for stage III breast cancer patients to choose optimal treatment and make optimal decisions. Furthermore, Nomograms were constructed by these multivariate prognostic factors. Additionally, Nomograms constructed by NPS performed superior predictive capabilities than NLR, LMR or only by NPS. The advantages of NPS include ease of use, cost-effectiveness, ability to capture host-related factors. According to these potential mechanisms, NPS might offer advantages over existing markers, such as NLR, LMR.
Certainly, there are still some limitations in the current study. Firstly, our research was a single-center retrospective study with relatively limited sample size, which provided it susceptible to some inherent bias, such as variables that could not be identified, without follow-up information. Secondly, as a result of limited study data, the heterogeneity of cancer-related features may not have been fully evaluated. Thirdly, the clinical significance of NPS may not reflect differences in individual studies by prospective multicenter trials.
Conclusions
In conclusion, NPS is an easy-to-use scoring system combined the inflammatory, immune, and nutritional indicators for predicting prognosis and treatment efficacy in stage III breast cancer patients. Our findings demonstrate a significant association between NPS and clinical outcomes. NPS, as a novel and original prognostic score, maybe as a valuable prognostic predictor for stage III breast cancer patients. We developed and validated a nomogram-based prognostic model using NPS, which provides an intuitive visualization tool for predicting 3- and 5-year survival rates. While this model shows promise, its generalizability may be limited to different patient populations and treatment settings. Comparative analyses with existing prognostic models (such as TNM stage) are warranted to determine whether the NPS-based nomogram offers improvements in accuracy, cost-effectiveness, or clinical utility.
Data Sharing Statement
The material supporting the conclusion of this article has been included within the manuscript.
Ethics Approval and Consent to Participate
This research received approval from the Ethics Committee of Cancer Hospital Affiliated to Shanxi Medical University. In the current study, all participants were thoroughly informed about the objectives, procedures, potential risks, and their rights related to the research. Specifically, written informed consent was obtained from each participant, documenting their agreement to participate in the research and authorizing the use of their data for scientific analysis.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors have declared that no competing interest exists.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–263. doi:10.3322/caac.21834
2. Yoon J, Oh DY. HER2-targeted therapies beyond breast cancer - an update. Nat Rev Clin Oncol. 2024;21(9):675–700. doi:10.1038/s41571-024-00924-9
3. Khan MS, Gowda BHJ, Nasir N, et al. Advancements in dextran-based nanocarriers for treatment and imaging of breast cancer. Int J Pharm. 2023;643:123276. doi:10.1016/j.ijpharm.2023.123276
4. Amgad M, Hodge JM, Elsebaie MAT, et al. A population-level digital histologic biomarker for enhanced prognosis of invasive breast cancer. Nat Med. 2024;30(1):85–97. doi:10.1038/s41591-023-02643-7
5. Thomas HR, Hu B, Boyraz B, et al. Metaplastic breast cancer: a review. Crit Rev Oncol Hematol. 2023;182:103924. doi:10.1016/j.critrevonc.2023.103924
6. Truong TKO, Vu HT, Bui VQ, Nguyen HB. Clinicopathological factors affecting response and survival in stage III breast cancer patients undergoing a dose-dense neoadjuvant regimen. Clin Ter. 2024;175(6):412–421. doi:10.7417/CT.2024.5148
7. Tarighati E, Keivan H, Mahani H. A review of prognostic and predictive biomarkers in breast cancer. Clin Exp Med. 2023;23(1):1–16. doi:10.1007/s10238-021-00781-1
8. Akrida I, Mulita F. The clinical significance of HER2 expression in DCIS. Med Oncol. 2022;40(1):16. doi:10.1007/s12032-022-01876-9
9. van Abbema DL, van den Akker M, Janssen-Heijnen ML, et al. Patient- and tumor-related predictors of chemotherapy intolerance in older patients with cancer: a systematic review. J Geriatr Oncol. 2019;10(1):31–41. doi:10.1016/j.jgo.2018.04.001
10. Chen N, He L, Zou Q, Deng H. HER2 targeted therapy in colorectal Cancer: current landscape and future directions. Biochem Pharmacol. 2024;223:116101. doi:10.1016/j.bcp.2024.116101
11. Diakos CI, Charles KA, McMillan DC, Clarke SJ. Cancer-related inflammation and treatment effectiveness. Lancet Oncol. 2014;15(11):e493–503. doi:10.1016/S1470-2045(14)70263-3
12. Candido J, Hagemann T. Cancer-related inflammation. J Clin Immunol. 2013;33 Suppl 1(S1):S79–84. doi:10.1007/s10875-012-9847-0
13. Xu T, Zhang SM, Wu HM, et al. Prognostic significance of prognostic nutritional index and systemic immune-inflammation index in patients after curative breast cancer resection: a retrospective cohort study. BMC Cancer. 2022;22(1):1128. doi:10.1186/s12885-022-10218-x
14. Kastora SL, Holmquist A, Valachis A, et al. Outcomes of different quality of life assessment modalities after breast cancer therapy: a network meta-analysis. JAMA Network Open. 2023;6(6):e2316878. doi:10.1001/jamanetworkopen.2023.16878
15. Grassadonia A, Graziano V, Iezzi L, et al. Prognostic relevance of neutrophil to lymphocyte ratio (NLR) in luminal breast cancer: a retrospective analysis in the neoadjuvant setting. Cells. 2021;10(7):1685. doi:10.3390/cells10071685
16. Song HN, Kim JY, Kim JM, et al. Sarcopenia using pectoralis muscle area and lymphocyte-to-monocyte ratio (LMR) are independent prognostic factors in patients for nonmetastatic breast cancer. Medicine. 2022;101(49):e32229. doi:10.1097/MD.0000000000032229
17. Wang Z, Shen X. Prognostic and clinicopathological significance of fibrinogen-to-albumin ratio (FAR) in patients with breast cancer: a meta-analysis. World J Surg Oncol. 2024;22(1):220. doi:10.1186/s12957-024-03506-2
18. Chen L, Qi Y, Kong X, et al. Nutritional risk index predicts survival in patients with breast cancer treated with neoadjuvant chemotherapy. Front Nutr. 2022;8:786742. doi:10.3389/fnut.2021.786742
19. Tong L, Wang S, Zhang R, Wu Y, Xu D, Chen L. High levels of SII and PIV are the risk factors of axillary lymph node metastases in breast cancer: a retrospective study. Int J Gen Med. 2023;16:2211–2218. doi:10.2147/IJGM.S411592
20. Galizia G, Lieto E, Auricchio A, et al. Naples prognostic score, based on nutritional and inflammatory status, is an independent predictor of long-term outcome in patients undergoing surgery for colorectal cancer. Dis Colon Rectum. 2017;60(12):1273–1284. doi:10.1097/DCR.0000000000000961
21. Park SH, Woo HS, Hong IK, Park EJ. Impact of postoperative Naples prognostic score to predict survival in patients with stage II-III colorectal cancer. Cancers. 2023;15(20):5098. doi:10.3390/cancers15205098
22. Wang H, Fang T, Yin X, et al. Prognostic importance of the preoperative New-Naples prognostic score for patients with gastric cancer. Cancer Med. 2023;12(2):1358–1375. doi:10.1002/cam4.5017
23. Demir M, Demircan NC. The Naples prognostic score in esophagus cancer: prognostic and beyond. Bull Cancer. 2023;110(10):1027–1040. doi:10.1016/j.bulcan.2023.06.007
24. Verras GI, Mulita F, Tchabashvili L, et al. A rare case of invasive micropapillary carcinoma of the breast. Prz Menopauzalny. 2022;21(1):73–80. doi:10.5114/pm.2022.113834
25. Akrida I, Michalopoulos NV, Lagadinou M, Papadoliopoulou M, Maroulis I, Mulita F. An updated review on the emerging role of indocyanine green (ICG) as a sentinel lymph node tracer in breast cancer. Cancers. 2023;15(24):5755. doi:10.3390/cancers15245755
26. Kiely M, Lord B, Ambs S. Immune response and inflammation in cancer health disparities. Trends Cancer. 2022;8(4):316–327. doi:10.1016/j.trecan.2021.11.010
27. Arifuzzaman M, Collins N, Guo CJ, Artis D. Nutritional regulation of microbiota-derived metabolites: implications for immunity and inflammation. Immunity. 2024;57(1):14–27. doi:10.1016/j.immuni.2023.12.009
28. Prame Kumar K, Nicholls AJ, Wong CHY. Partners in crime: neutrophils and monocytes/macrophages in inflammation and disease. Cell Tissue Res. 2018;371(3):551–565. doi:10.1007/s00441-017-2753-2
29. Patel AA, Ginhoux F, Yona S. Monocytes, macrophages, dendritic cells and neutrophils: an update on lifespan kinetics in health and disease. Immunology. 2021;163(3):250–261. doi:10.1111/imm.13320
30. Shaul ME, Fridlender ZG. Tumour-associated neutrophils in patients with cancer. Nat Rev Clin Oncol. 2019;16(10):601–620. doi:10.1038/s41571-019-0222-4
31. Wang Y, Li C, He J, et al. Multi-omics analysis and experimental validation of the value of monocyte-associated features in prostate cancer prognosis and immunotherapy. Front Immunol. 2024;15:1426474. doi:10.3389/fimmu.2024.1426474
32. Brummel K, Eerkens AL, de Bruyn M, Nijman HW. Tumour-infiltrating lymphocytes: from prognosis to treatment selection. Br J Cancer. 2023;128(3):451–458. doi:10.1038/s41416-022-02119-4
33. Cupp MA, Cariolou M, Tzoulaki I, Aune D, Evangelou E, Berlanga-Taylor AJ. Neutrophil to lymphocyte ratio and cancer prognosis: an umbrella review of systematic reviews and meta-analyses of observational studies. BMC Med. 2020;18(1):360. doi:10.1186/s12916-020-01817-1
34. Ma Y, Zhang J, Chen X. Lymphocyte-to-monocyte ratio is associated with the poor prognosis of breast cancer patients receiving neoadjuvant chemotherapy. Cancer Manag Res. 2021;13:1571–1580. doi:10.2147/CMAR.S292048
35. Ethier JL, Desautels D, Templeton A, Shah PS, Amir E. Prognostic role of neutrophil-to-lymphocyte ratio in breast cancer: a systematic review and meta-analysis. Breast Cancer Res. 2017;19(1):2. doi:10.1186/s13058-016-0794-1
36. Tokumaru Y, Oshi M, Murthy V, et al. Low intratumoral genetic neutrophil-to-lymphocyte ratio (NLR) is associated with favorable tumor immune microenvironment and with survival in triple negative breast cancer (TNBC). Am J Cancer Res. 2021;11(11):5743–5755.
37. De Cicco P, Catani MV, Gasperi V, Sibilano M, Quaglietta M, Savini I. Nutrition and breast cancer: a literature review on prevention, treatment and recurrence. Nutrients. 2019;11(7):1514. doi:10.3390/nu11071514
38. Nakazawa N, Sohda M, Tateno K, et al. Albumin-derived neutrophil-to-lymphocyte ratio score as a marker of nivolumab treatment sensitivity in gastric cancer: a multicenter study. Vivo. 2023;37(2):818–824. doi:10.21873/invivo.13147
39. Amjad W, Qureshi W, Singh RR, Richter S. Nutritional deficiencies and predictors of mortality in diabetic and nondiabetic gastroparesis. Ann Gastroenterol. 2021;34(6):788–795. doi:10.20524/aog.2021.0660
40. Xie H, Yuan K, Ruan G, et al. Improving the assessment of malnutrition in cancer: using systemic inflammation markers as a supplement to the inflammation items of the GLIM criteria. Clin Nutr. 2023;42(10):2036–2044. doi:10.1016/j.clnu.2023.08.020
41. Chen Y, Zhu Y, Li X, et al. Cholesterol inhibits TCR signaling by directly restricting TCR-CD3 core tunnel motility. Mol Cell. 2022;82(7):1278–1287.e5. doi:10.1016/j.molcel.2022.02.017
42. Bai Y, Li T, Wang Q, et al. Shaping immune landscape of colorectal cancer by cholesterol metabolites. EMBO Mol Med. 2024;16(2):334–360. doi:10.1038/s44321-023-00015-9
43. Lieto E, Auricchio A, Tirino G, et al. Naples prognostic score predicts tumor regression grade in resectable gastric cancer treated with preoperative chemotherapy. Cancers. 2021;13(18):4676. doi:10.3390/cancers13184676
44. Gu J, Deng S, Jiang Z, et al. Modified Naples prognostic score for evaluating the prognosis of patients with obstructive colorectal cancer. BMC Cancer. 2023;23(1):941. doi:10.1186/s12885-023-11435-8
45. Li J, Yang W, Yuan Y, et al. Preoperative Naples prognostic score is a reliable prognostic indicator for newly diagnosed glioblastoma patients. Front Oncol. 2022;12:775430. doi:10.3389/fonc.2022.775430
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Neutrophil-to-Lymphocyte Ratio and Platelet-to-Lymphocyte Ratio Can Predict the Severity in COVID-19 Patients from Ethiopia: A Retrospective Study
Ayalew G, Mulugeta B, Haimanot Y, Adane T, Bayleyegn B, Abere A
International Journal of General Medicine 2022, 15:7701-7708
Published Date: 7 October 2022
Prognostic Significance of Preoperative Lactate Dehydrogenase to Albumin Ratio in Breast Cancer: A Retrospective Study
He J, Tong L, Wu P, Wu Y, Shi W, Chen L
International Journal of General Medicine 2023, 16:507-514
Published Date: 8 February 2023
Clinical Significance and Diagnostic Utility of NLR, LMR, PLR and SII in the Course of COVID-19: A Literature Review

Kosidło JW, Wolszczak-Biedrzycka B, Matowicka-Karna J, Dymicka-Piekarska V, Dorf J
Journal of Inflammation Research 2023, 16:539-562
Published Date: 11 February 2023
Neutrophil/Lymphocyte Ratio (NLR) and Lymphocyte/Monocyte Ratio (LMR) – Risk of Death Inflammatory Biomarkers in Patients with COVID-19
Dymicka-Piekarska V, Dorf J, Milewska A, Łukaszyk M, Kosidło JW, Kamińska J, Wolszczak-Biedrzycka B, Naumnik W
Journal of Inflammation Research 2023, 16:2209-2222
Published Date: 23 May 2023
Pretreatment Circulating Albumin, Platelet, and RDW-SD Associated with Worse Disease-Free Survival in Patients with Breast Cancer
Chen CC, Tang WH, Wu CC, Lee TL, Tsai IT, Hsuan CF, Wang CP, Chung FM, Lee YJ, Yu TH, Wei CT
Breast Cancer: Targets and Therapy 2024, 16:23-39
Published Date: 16 January 2024