Back to Journals » Journal of Inflammation Research » Volume 16
Naples Prognostic Score as an Independent Predictor of Survival Outcomes for Resected Locally Advanced Non-Small Cell Lung Cancer Patients After Neoadjuvant Treatment
Authors Zou Z, Li J, Ji X, Wang T ![]() , Chen Q, Liu Z, Ji S
, Chen Q, Liu Z, Ji S ![]()
Received 14 December 2022
Accepted for publication 16 February 2023
Published 23 February 2023 Volume 2023:16 Pages 793—807
DOI https://doi.org/10.2147/JIR.S401446
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Ning Quan
Zhonghua Zou,1 Jinping Li,2 Xiang Ji,2 Tingxing Wang,1 Qingqing Chen,1 Zhengcao Liu,1 Shengjun Ji1
1Department of Radiotherapy & Oncology, the Affiliated Suzhou Hospital of Nanjing Medical University, Gusu School, Nanjing Medical University, Suzhou, People’s Republic of China; 2Department of Gastroenterology, Fangzi People’s Hospital, Weifang, People’s Republic of China
Correspondence: Shengjun Ji, Department of Radiotherapy & Oncology, the affiliated Suzhou Hospital of Nanjing Medical University, Gusu School, Nanjing Medical University, No. 16 Baita Road, Suzhou, 215001, People’s Republic of China, Email [email protected]
Background: The Naples Prognostic Score (NPS) can reflect patient’s nutritional and inflammatory status, which is identified as a prognostic indicator for various malignant tumors. However, its significance in patients with resected locally advanced non-small cell lung cancer (LA-NSCLC) patients who receive neoadjuvant treatment remains unclear so far.
Methods: A total of 165 LA-NSCLC patients surgically treated from May 2012 to November 2017 were retrospectively investigated. The LA-NSCLC patients were divided into three groups according to NPS scores. The receiver operating curve (ROC) analysis was performed to reveal the discriminatory ability of NPS and other indicators for predicting the survival. The NPS and clinicopathological variables were further evaluated the prognostic value by univariate and multivariate Cox analysis.
Results: The NPS was related to age (P = 0.046), smoking history (P = 0.004), Eastern Cooperative Oncology Group (ECOG) score (P = 0.005), and adjuvant treatment (P = 0.017). Patients with high NPS scores had worse overall survival (OS) (group 1 vs 0, P = 0.006; group 2 vs 0, P < 0.001) and disease-free survival (DFS) (group 1 vs 0, P < 0.001; group 2 vs 0, P < 0.001). The ROC analysis demonstrated that NPS had better predictive ability than other prognostic indicators. Multivariate analysis revealed that NPS was independent prognostic indicator of OS (group 1 vs 0, hazard ratio [HR] =2.591, P = 0.023; group 2 vs 0, HR = 8.744, P = 0.001) and DFS (group 1 vs 0, HR =3.754, P < 0.001; group 2 vs 0, HR = 9.673, P < 0.001).
Conclusion: The NPS could be an independent prognostic indicator in patients with resected LA-NSCLC receiving neoadjuvant treatment and more reliable than the other nutritional and inflammatory indicators.
Keywords: surgery, locally advanced NSCLC, NPS, prognosis, neoadjuvant treatment
Introduction
The morbidity and mortality of lung cancer rank first in the world, which is a public problem worthy of our attention.1,2 Non-small cell lung cancer (NSCLC) is the main pathological type of lung cancer, accounting for about 80–85% of all lung cancers.3 The late clinical manifestations are the hidden symptoms of the NSCLC. Therefore, the outcome of NSCLC patients is extremely unfavorable compared with other solid malignancies.4,5 Surgery is a reliable and effective treatment for resected locally advanced non-small cell lung cancer (LA-NSCLC) patients.6,7 The 5-year survival rate of LA-NSCLC in the past few decades is about 30%, which is unsatisfactory.8,9 In recent years, with the rapid development of programmed cell death receptor-1 (PD-1) and programmed cell death ligand-1 (PD-L1) checkpoints, the application of immune checkpoint inhibitors (ICIs)in the treatment of malignant tumors has shown a promising prospect.10,11 Nevertheless, the value of ICIs is limited, and a considerable proportion of LA-NSCLC patients are resistant to ICIs.12,13 Therefore, exploring the convenient, economical and reliable prognostic indicators to help to optimize the treatment options is necessary.
According to previous reports, systemic inflammatory response is a hallmark that normal cells tend to malignant development, which is closely related to the occurrence and development of malignant tumors.14–16 Systemic inflammatory can promote local tumor cells infiltration, distant metastasis and treatment resistance.17,18 Systemic inflammatory related indicators have offered the utility value for predicting the tumor patient survival outcomes, such as neutrophil-to-lymphocyte ratio (NLR), lymphocyte-to-monocyte ratio (LMR), platelet-to-lymphocyte ratio (PLR), systemic immune-inflammation index (SII), and the C-reactive protein-to-albumin ratio (CAR).19–23 Additionally, nutritional status as host related factor, has attracted researchers’ interests in malignant tumors survival analysis.24,25 The systemic inflammation score (SIS), Glasgow prognostic score (GPS), and prognostic nutritional index (PNI) are related to the prognosis of NSCLC.26–28
Recently, Naples Prognostic Score (NPS) has attracted extensive attention as a new indicator of combining inflammatory and nutritional status. The NPS, proposed by Galizia et al, consists of serum albumin concentration (Alb), total blood cholesterol (TC), NLR, and LMR. And the predictive value of NPS in malignant tumors was firstly validated in colorectal cancer patients undergoing surgery by a clinical trial (NCT03272646).29 NPS has been reported to be significantly associated with survival outcomes in patients with ampullary carcinoma,30 gastric cancer,31 esophageal cancer,32 pancreatic cancer,33 stage I–II NSCLC34 and endometrial cancer.35 However, the relationship between NPS and long-term outcomes of resected LA-NSCLC patients after neoadjuvant treatment remains unclear.
The present study was designed to assess the predictive value of NPS in resected LA-NSCLC patients after neoadjuvant treatment. Meanwhile, based on the subgroup analysis, we also investigated the prognostic significance of NPS in stage IIIA and stage IIIB patients, respectively.
Materials and Methods
Patient Selection
We performed a retrospective study of 165 LA-NSCLC patients who underwent surgery in our hospital from May 2012 to November 2017. As shown in Figure 1, study flow diagram was identified. Clinicopathological variables including age, gender, smoking history, Eastern Cooperative Oncology Group (ECOG) score, pathological type, differentiation, TNM stage, surgery approach, adjuvant treatment, and postoperative complications were analyzed from the electronic medical record system of hospital.
 |
Figure 1 The flow chart of patient selection process. Abbreviation: NSCLC, non-small cell lung cancer. |
Evaluation of Inflammatory and Nutritional Indicators
The plasma laboratory examination was performed within seven days before neoadjuvant therapy. Laboratory examination included Alb, TC, absolute monocyte count, absolute neutrophil count, and absolute lymphocyte count. NLR was defined as absolute neutrophil count divided by absolute lymphocyte count. LMR was defined as absolute lymphocyte count divided by absolute monocyte count. The PNI was calculated as follows: 10 ×Alb value + 0.005 × total lymphocyte count.36 Patients with Alb ≥ 4g/dL and LMR level ≥ 4.44 were assigned a SIS score of 0, patients with Alb < 4g/dL and LMR < 4.44 were allocated a SIS score of 2, and patients with Alb < 4g/dL or LMR < 4.44 were allocated a SIS score of 1.37
Establishment of NPS
As described previously, the NPS was calculated from Alb, TC, NLR, and LMR.29 Alb <4 mg/dL, TC ≤ 180 mg/dL, NLR ≥ 2.96, or LMR ≤ 4.44 was scored as 1. Alb≥4 mg/dL, TC > 180 mg/dL, NLR < 2.96, or LMR > 4.44 was scored as 0. The NPS was evaluated as the sum of the above scores. Afterwards, these patients were divided into three groups based on respective NPS score: patients with a score of 0 were assigned to group 0; patients with a score of 1 or 2 were assigned to group 1; patients with a score of 3 or 4 were assigned to group 2.
Neoadjuvant Treatment and Surgery
All patients were treated with neoadjuvant platinum-based chemotherapy regimens or chemoradiotherapy. The thoracic surgeons analyzed the patient’s condition and determined the surgical approaches, including thoracotomy or video-assisted thoracoscopic surgery (VATS) procedure.38 Thoracotomy was chosen to ensure the safety of patient when the preoperative imaging examination showed large tumor scope, obvious tumor invasion or unclear anatomy with the surrounding important vascular structure. Elderly patients with poor physique and weak immunity were treated with VAST. Of course, patients’ pain, economy and other factors were also taken into consideration when choosing surgical approaches. All patients were required to complete relevant pre-operative functional evaluation (blood examination, electrocardiograph test, heart Doppler ultrasound test, pulmonary function test). The specific scope of surgical resection included the complete lobectomy of the tumor and mediastinal lymph nodes dissection.39 The intercostal muscles, thymus, or pleura were sutured after the surgical excision. Chest tubes were placed in the chest to facilitate lung fluid drainage. Pneumonia, atelectasis, secondary tracheal intubation, bronchopleural fistula, and pulmonary embolism within 1 month after lung cancer resection were defined as the postoperative complication.40,41 The patients with respiratory failure post-surgery were excluded to ensure follow-up antitumor therapy.42 The thoracic surgeons encouraged patients to perform the early rehabilitation exercises and nutritional support. Sequentially, patients received adjuvant chemotherapy or chemoradiotherapy after surgery.
Follow-Up
The follow-up information included the assessment of disease status, identification of survival outcomes or last lost follow-up. The patients were regularly followed up every 3 months in the first two years after treatment and every 6 months thereafter. Each hospital follow-up examination included physical examination, tumor markers, chest computed tomography, and other examinations. Overall survival (OS) was considered as the duration from the date of neoadjuvant treatment to death from any cause or last follow-up. Disease-free survival (DFS) was considered as the time from the date of neoadjuvant treatment to the date of disease progression or the death from any cause.
Statistical Analysis
The SPSS 21.0 software and GraphPad Prism 8.0 were used to perform data analysis. The association between NPS and clinicopathological variables was analyzed using chi-square tests. Spearman correlation analysis was used to identify the associations among inflammatory indicators and nutritional indicators. Receiver operating characteristic (ROC) curves were performed to determine the predictive abilities of the different scoring systems. The Kaplan-Meier (KM) method was applied in conducting OS and DFS differences analysis and visualized by survival curves. The clinicopathological variables in univariate analysis with P values < 0.05 were included into the multivariate prognostic analysis. The hazard ratios (HRs) and corresponding 95% confidence intervals (CIs) of variables were assessed for relative risk. P < 0.05 was considered to be statistically significant.
Results
Patient Characteristics
Among the NSCLC patients, 165 LA-NSNCL patients met the screening criteria who underwent neoadjuvant treatment and surgery, including 74 (44.8%) males and 91 (55.2%) females. A total of 82 (49.7%) patients were older than 60 years old, and 80 (48.5%) patients had smoking history. 79 (47.9%) patients received a VATS, 86 (52.1%) received a thoracotomy. The majority of the LA-NSNCL patients received neoadjuvant chemotherapy (66.1%). The median follow-up time was 34 (interquartile range: 29–61) months.
Relationships Between NPS and Clinicopathological Variables
The relationships between NPS and clinicopathological variables are shown in Table 1. Thirty-five patients in the NPS groups 0, 108 patients in the NPS groups 1, and 22 patients in the NPS groups 2 were further analyzed. NPS significantly increased among patients having smoking history (P = 0.004). Moreover, NPS significantly increased among cases having the ECOG score of 1 (P = 0.005), neoadjuvant chemoradiotherapy (P = 0.017). However, no significant difference was observed in gender, pathological type, differentiation, TNM stage, surgery approach, and postoperative complications.
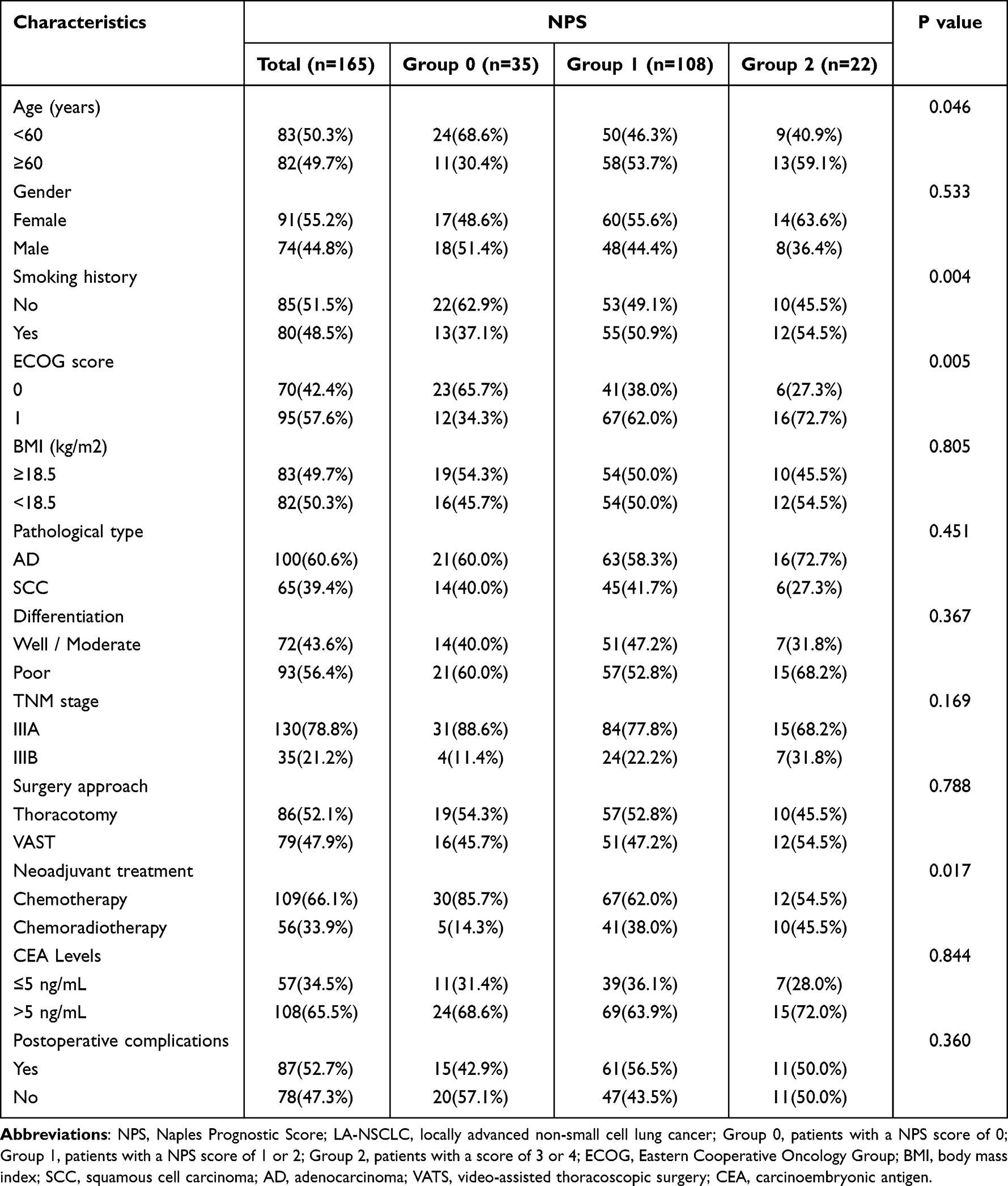 |
Table 1 Association of the NPS with LA-NSCLC Patient Clinicopathological Characteristics |
Prognostic Value of the Inflammatory and Nutritional Indicators
Kaplan-Meier curves were used to perform the OS analysis based on the Alb, TC, NLR, LMR, PNI and SIS. Compared with patients in the low LMR group and high SIS score group, those in the high LMR group and low SIS score group had better OS (Figure 2). We next used the Kaplan-Meier curves to evaluate the DFS differences in Alb, TC, NLR, LMR, PNI and SIS. We found that the patients in the high Alb group, high TC group, high LMR group and low SIS score group had better DFS compare with the low Alb group, low TC group, low LMR group, and high SIS score group (Figure 3).
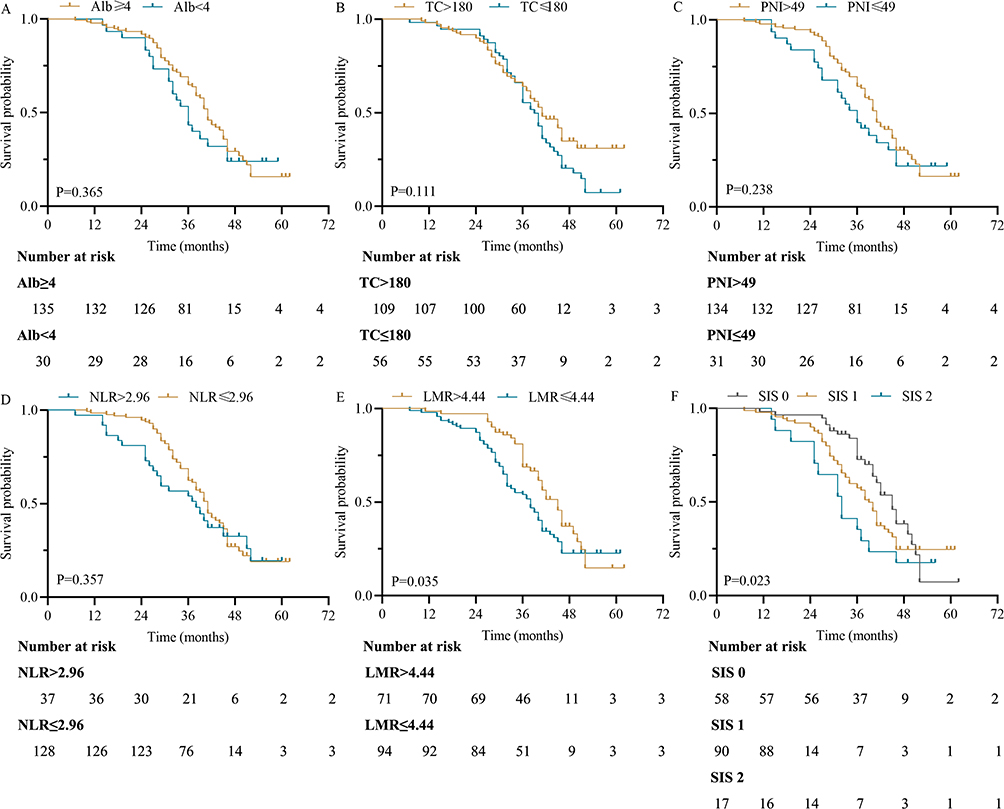 |
Figure 2 Kaplan-Meier curves for OS in patients with LA-NSCLC according to Alb (A), TC (B), PNI (C), NLR (D), LMR (E) and SIS (F). Abbreviations: OS, overall survival; LA-NSCLC, locally advanced non-small cell lung cancer; Alb, serum albumin concentration; TC, total blood cholesterol; PNI, prognostic nutritional index; NLR, neutrophil‐to‐lymphocyte ratio; LMR, lymphocyte‐to‐monocyte ratio; SIS, the systemic inflammation score. |
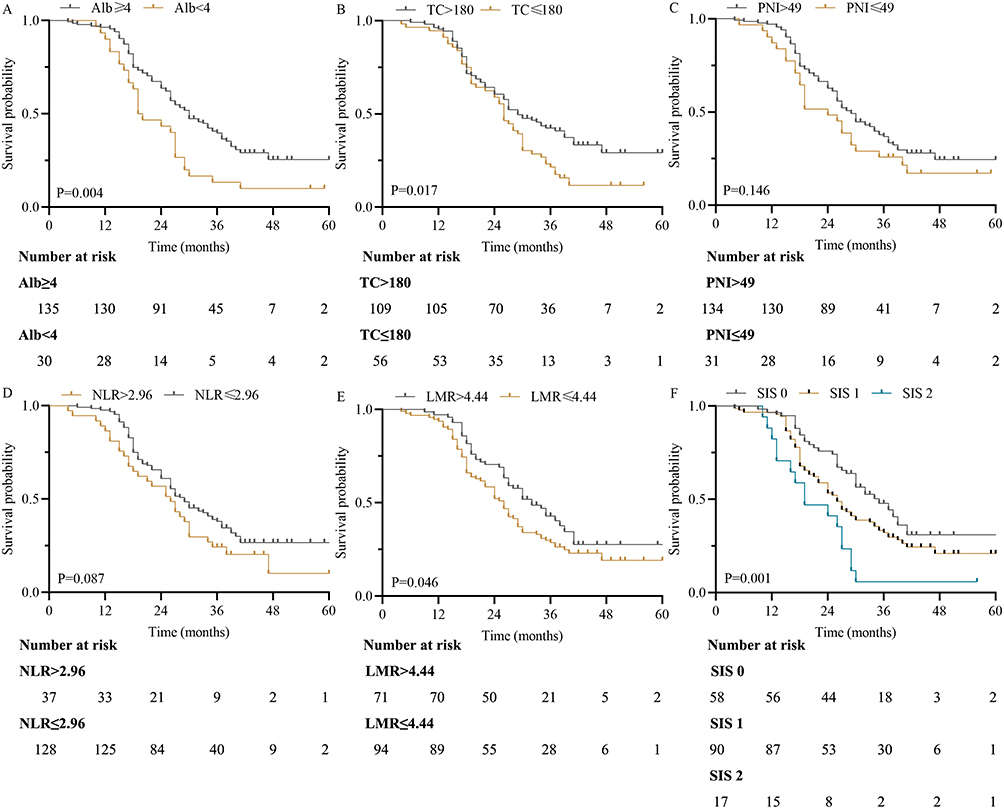 |
Figure 3 Kaplan-Meier curves for PFS in patients with LA-NSCLC according to Alb (A), TC (B), PNI (C), NLR (D), LMR (E) and SIS (F). Abbreviations: DFS, disease-free survival difference; LA-NSCLC, locally advanced non-small cell lung cancer; Alb, serum albumin concentration; TC, total blood cholesterol; PNI, prognostic nutritional index; NLR, neutrophil‐to‐lymphocyte ratio; LMR, lymphocyte‐to‐monocyte ratio; SIS, the systemic inflammation score. |
Prognostic Value of the NPS
We also explored the associations among inflammatory indicators and nutritional indicators. The results found that there were no significant correlations regarding Alb and NLR (r = 0.006, P = 0.337), Alb and LMR (r = 0.016, P = 0.109), TC and NLR (r = 0.006, P = 0.311), TC and LMR (r = 0.001, P = 0.680) (Figure 4). We used the ROC curves to determine the predictive abilities of the different scoring systems. As shown in Figure 5, the area under the curve (AUC) of NPS for predicting OS and DFS were 0.704 and 0.734, respectively. And the ROC results confirmed that the NPS had stronger discriminatory power for predicting the OS and DFS than Alb, TC, NLR, LMR, PNI and SIS (Table 2). OS analysis showed that the patients in NPS group 2 and group 1 had poorer survival benefits than those in NPS group 0 (group 1 vs 0, P = 0.006; group 2 vs 0, P < 0.001, Figure 6A). The Kaplan-Meier curves of DFS showed that patients in NPS group 2 and group 1 had significantly poorer DFS compared with those in NPS group 0 (group 1 vs 0, P < 0.001; group 2 vs 0, P < 0.001, Figure 6B).
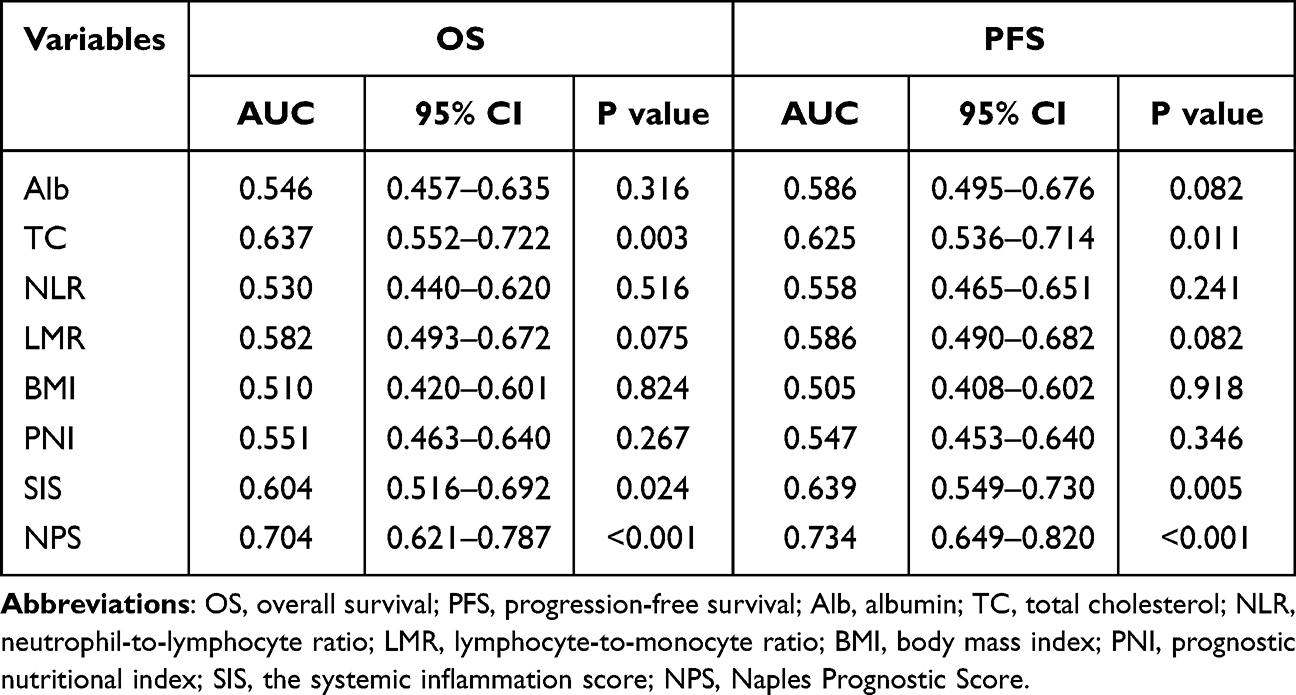 |
Table 2 ROC Analysis of Inflammatory or Nutritional-Related Indicators |
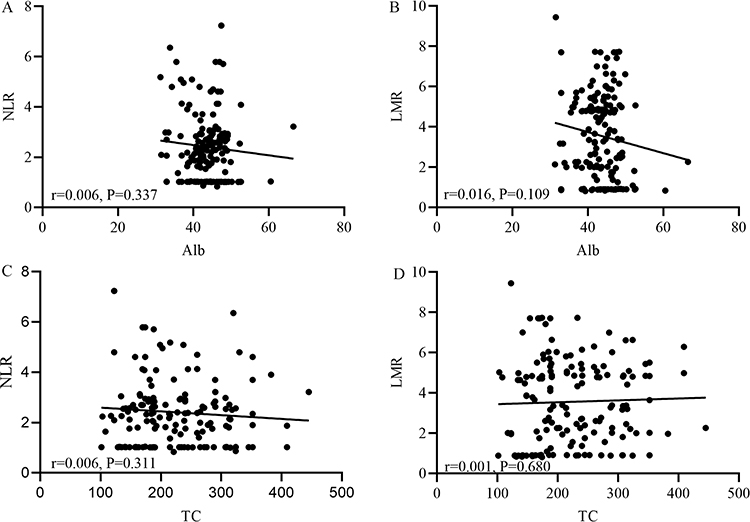 |
Figure 4 Correlation analysis between Alb and NLR (A), Alb and LMR (B), TC and NLR (C), TC and LMR (D). Abbreviations: Alb, serum albumin concentration; TC, total blood cholesterol; NLR, neutrophil‐to‐lymphocyte ratio; LMR, lymphocyte‐to‐monocyte ratio. |
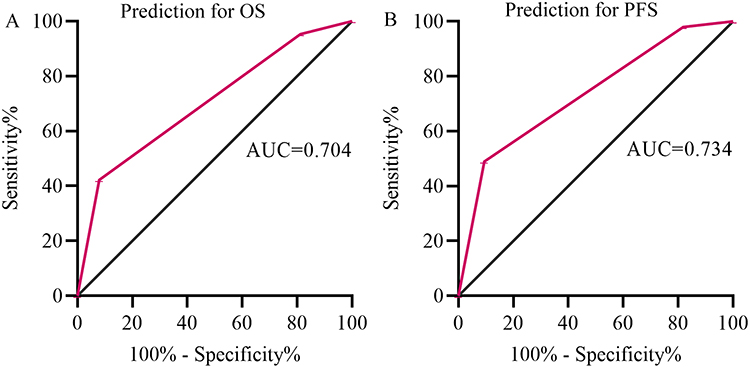 |
Figure 5 ROC curves of NPS for predicting OS (A) and DFS (B). Abbreviations: ROC, receiver operator characteristic curve; OS, overall survival; DFS, disease-free survival. |
 |
Figure 6 Kaplan-Meier survival curves in patients with LA-NSCLC. (A) OS based on NPS groups; (B) DFS based on NPS groups. Abbreviations: OS, overall survival; DFS, disease-free survival. |
We further performed subgroup analysis of TNM stage in LA-NSCLC patients (Figure 7). In the stage IIIA and stage IIIB, patients in NPS group 0 had significantly longer OS and DFS compared with those in NPS group 1 or 2 (P < 0.001; P < 0.001). In the stage IIIB, patients in NPS group 0 had significantly longer DFS compared with those in NPS group 1 or 2 (P = 0.017). However, no statistical significance was found between three groups in OS.
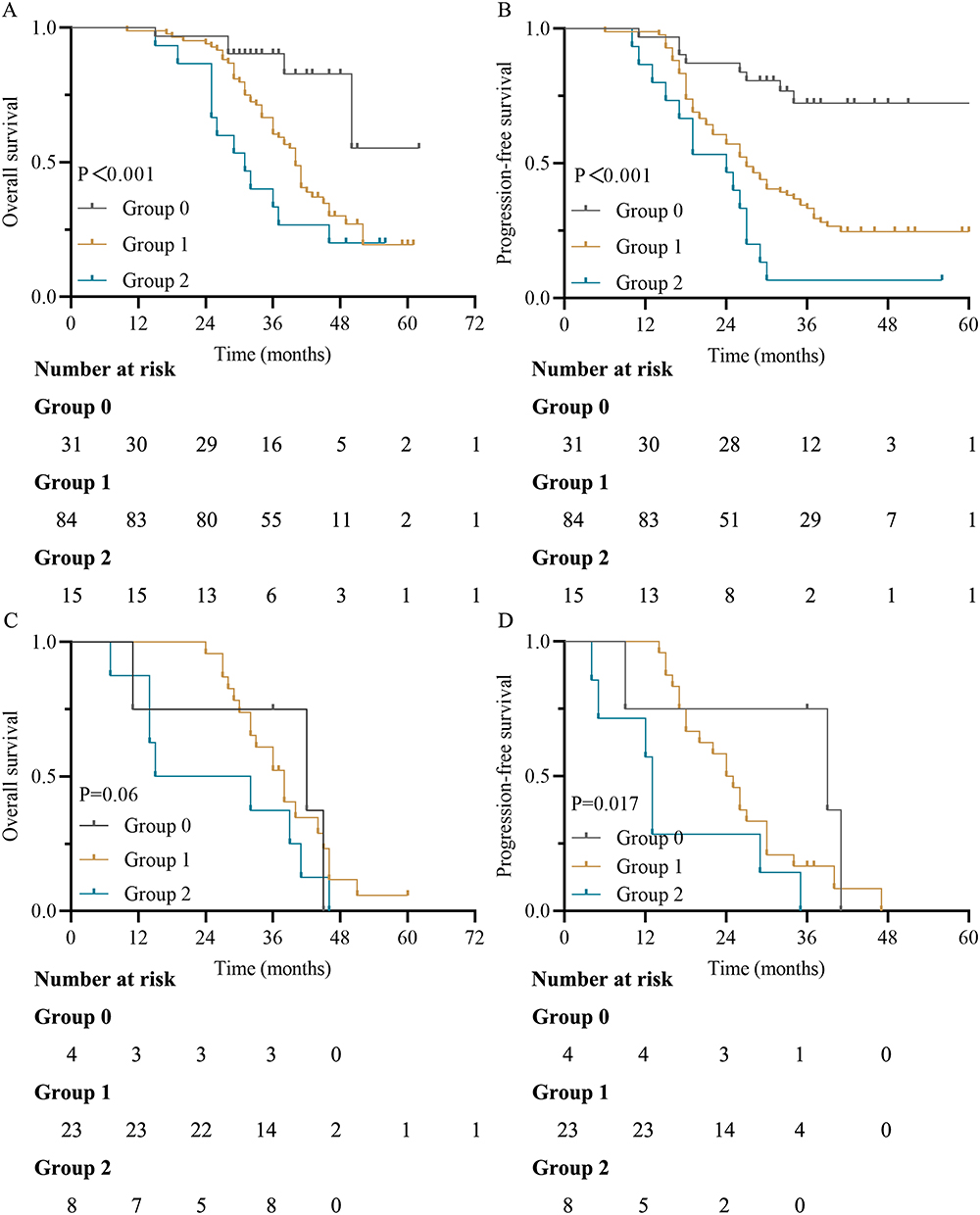 |
Figure 7 Kaplan-Meier survival curves in patients with LA-NSCLC according to the TNM stage. (A and B) OS and DFS based on NPS groups in stage IIIA; (C and D) OS and DFS based on NPS groups in stage IIIB. Abbreviations: OS, overall survival; DFS, disease-free survival. |
Cox Regression Analysis on Prognostic Factors
The univariate survival analysis of this study was shown in Table 3. Univariate Cox regression analysis was performed in age, gender, smoking history, ECOG score, body mass index (BMI), pathological type, differentiation, TNM stage, surgery approach, adjuvant treatment, CEA levels, postoperative complications, PNI, SIS and NPS. The results demonstrated that age, ECOG score, TNM stage, surgery approach, SIS, and NPS were closely associated with OS and DFS. Based on above results of univariate Cox regression analysis, multivariate analysis demonstrated that NPS was independent prognostic factor of poor OS (group 1 vs 0, hazard ratio [HR] =2.591, P = 0.023; group 2 vs 0, HR = 8.744, P = 0.001) and DFS (group 1 vs 0, HR =3.754, P < 0.001; group 2 vs 0, HR = 9.673, P < 0.001) (Table 4).
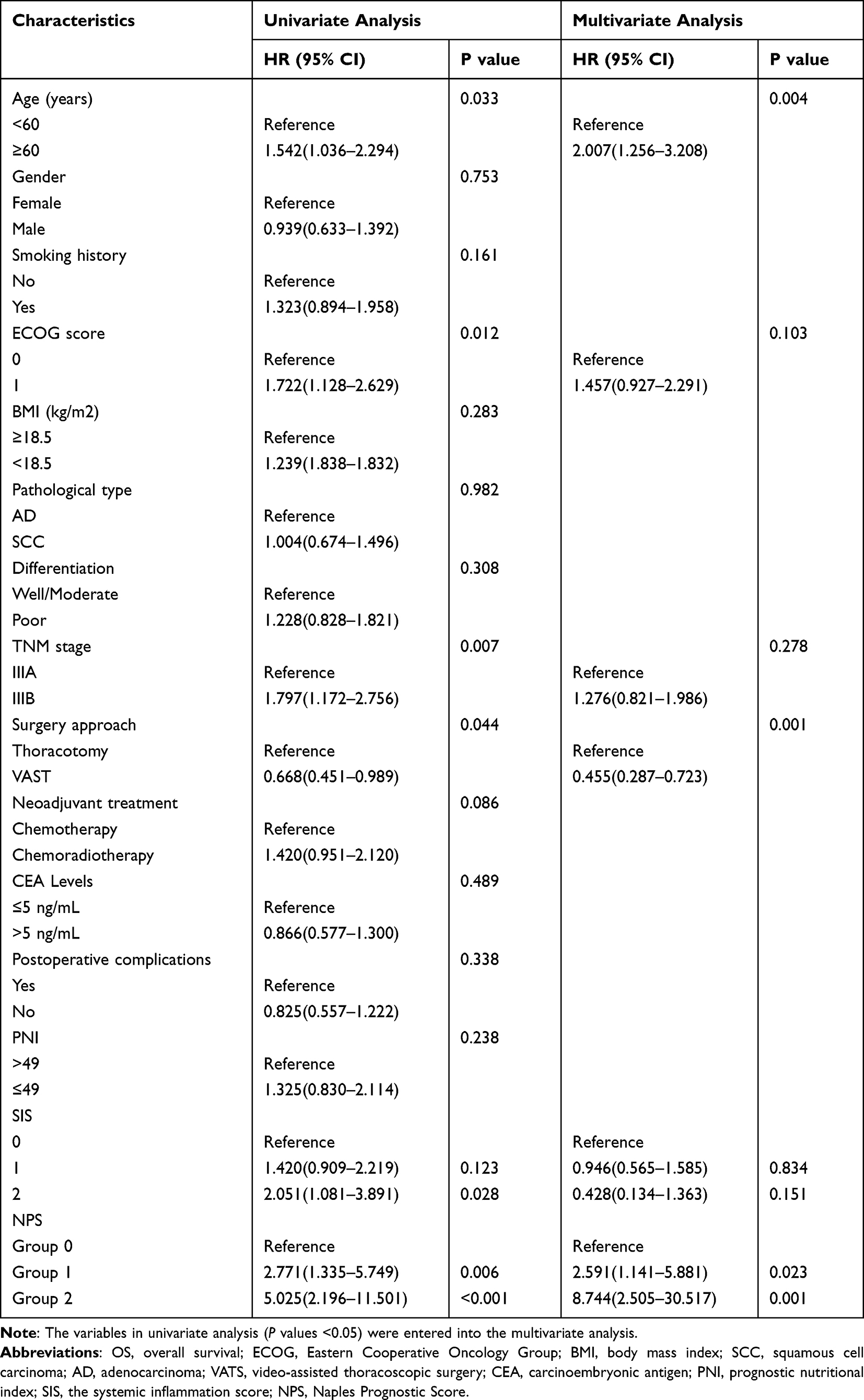 |
Table 3 Univariate and Multivariate Analyses of OS |
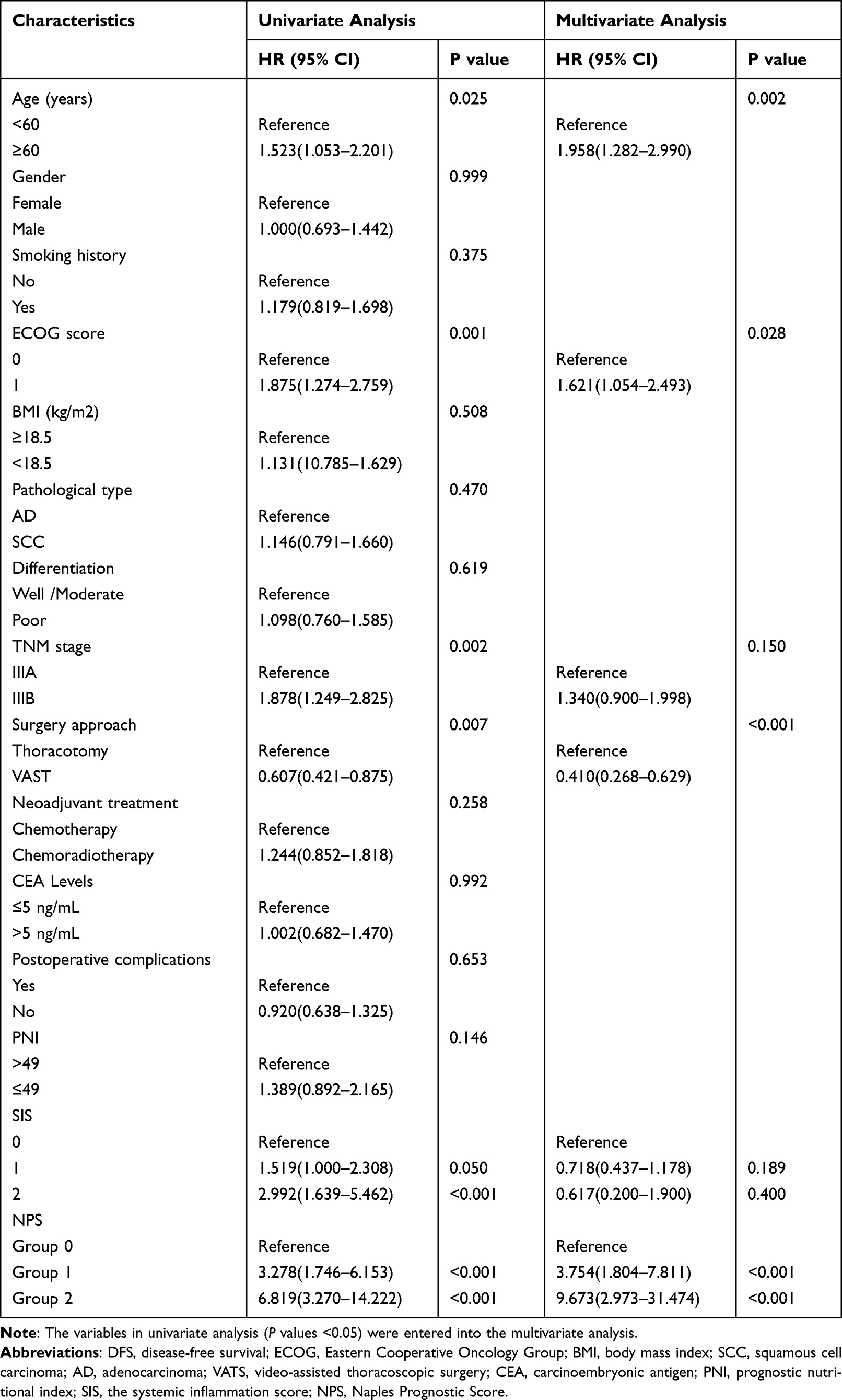 |
Table 4 Univariate and Multivariate Analyses of DFS |
Discussion
Though people’s awareness of cancer prevention is increasing year by year, the incidence rate of NSCLC was gradually increasing in China.43 TNM staging is often used by clinicians to evaluate the prognosis of NSCLC patients and guide treatment decisions. However, TNM staging is not so accurate and reliable for NSCLC patients in clinical practice. Even if NSCLC patients are in the same stage, their survival outcomes are different. Scholars generally believe that the occurrence of tumor is a complicated biological process,44,45 and a single prognostic index is easily influenced by the arbitrary cut-off value. Therefore, we should focus on the clinical application of multidimensional prognostic evaluation systems, such as the NPS. This present study firstly assessed the prognostic value of NPS in resected LA-NSCLC patients after neoadjuvant treatment. Our results demonstrated that the NPS can accurately predict survival outcomes for resected LA-NSCLC patients after neoadjuvant treatment, and high NPS score implied a poor OS and DFS.
Increasing evidences have revealed that the malignant tumor cells formation is associated with inflammatory mediators.46 Systemic inflammation is the characteristic of tumor microenvironment, which can promote tumor cells invasion, metastasis, and weaken the host antitumor immunity. Researchers have made adequate work on the effect of inflammation on tumors, and have obtained the theoretical consensus.47,48 Systemic inflammation-related blood cells include neutrophils, platelets, monocytes and so on. Only by fully grasping the mechanism of inflammatory cells acting on tumor, can we better comprehend the systemic inflammation-related prognostic indicators.
First, we analyze these mechanisms from the perspective of neutrophils. Neutrophils play stable roles not only in anti-infection but also in promoting role of cancer.49 Specifically, neutrophils specifically release the matrix metalloproteinase (MMPs) and vascular endothelial growth factor (VEGF), which induce tumor metastasis and tumor-associated angiogenesis.50 In terms of body immunity, neutrophils suppress the immune T-cell activation to weaken anti-tumor immune effect, which destroy the immune balance of the body, resulting in the tumorigenesis.51 Secord, the potential of monocytes to differentiate into tumor-associated macrophages (TAMs) has attracted much attention. TAMs are found as key controlling factors in tumor microenvironment, and enhance cancer rapidly multiplying in size and cancer cells migration.52 More interestingly, monocytes can promote the blood circulation of tumor cells, thus increasing the risk of distant metastasis.53 Considering these, the elevated monocytes may represent a high tumor burden status. Last, lymphocytes are the essential cornerstone of the immune system, which effectively reduce the risk of tumor cell invasion and metastasis. Given the above findings, elevated NLR and decreased LMR reveal the pro-inflammatory and weak immune status.
Additionally, Alb and TC were incorporated into NPS scoring systems. Alb and TC serve as nutritional indicators, their mechanisms of action on tumor are also gradually clear.54 Previous reports indicated that patients with hypoalbuminemia had poorer outcomes in advanced gastrointestinal cancer.55 More importantly, Alb is also an indicator of systemic inflammation, because some pro-inflammatory cytokines can reduce the concentration of Alb.56 TC has been identified to correlate with tumorigenesis and survival in gastric cancer patients.57
Given the significance of neutrophils, monocytes, lymphocytes, Alb and TC in cancer, we have sufficient evidences to believe that NPS is a reliable prognostic evaluation system in clinical practice. Galizia et al firstly proposed the NPS as a prognostic indicator, and found that preoperative NPS was closely associated with long-term outcomes in colorectal cancer patients.29 Importantly, Galizia et al’s conclusion has also been confirmed in cancers other than colon cancer. Jin and colleagues found that NPS can independently predict the incidence of postoperative complications after pancreatoduodenectomy, and demonstrated the predictive value of NPS for short- and long-term outcomes in ampullary carcinoma patients.30 Similarly, Lieto et al found the predictive value of NPS in gastric cancer with a retrospective study in Italy. NPS mirrored the immune-nutritional conditions, and showed a trustworthy power in predicting tumor regression grade and survival.58 Besides, a relevant study about gastrointestinal stromal tumors also revealed that NPS was associated with tumor progression and long-term survival.59
The application of incorporating multimodal prognostic indicators in the management of cancers is still challenging. As we have seen, we are trying our best to explore the predictive value of NPS in resected LA-NSCLC patients after neoadjuvant treatment. The optimal cut-off values of NLR, LMR, Alb and TC were determined according to Galizia’s study, which did not reflect the heterogeneity of individual research. However, this does not affect our conclusions. In terms of the correlation between NPS and clinicopathological variables, we found that NPS was significantly associated to the age (P = 0.046), smoking history (P = 0.004), ECOG score (P = 0.005), and neoadjuvant treatment (P = 0.017). Although the number of group 0 and group 2 patients who were included in this study was small, we still obtained the positive results. In addition, the OS and DFS of LA-NSCLC patients in NPS 0 group was significantly longer than that in NPS 1 group and 2 group. In the present study, univariate analysis confirmed that age, ECOG score, TNM stage, surgery approach, SIS, and NPS were prognostic risk factors for the LA-NSCLC patients. As we expected, the results of multivariate analysis showed that NPS was independent risk factors for the OS (group 1 vs 0, HR =2.591, P = 0.023; group 2 vs 0, HR = 8.744, P = 0.001) and DFS (group 1 vs 0, HR =3.754, P < 0.001; group 2 vs 0, HR = 9.673, P < 0.001) of LA-NSCLC patients. In addition, age and surgery approach were independent risk factors for the OS and DFS of LA-NSCLC patients. These findings are consistent with those previously reported, and further verified the clinical application value of NPS in tumors. We firmly believe that the NPS can be served as a reliable index for recurrence surveillance and prognosis evaluation for LA-NSCLC. The poorer the nutritional status and physical inflammation, the higher the risk of disease progression will be.
Our study has several limitations. First, due to the nature of single-center and retrospective study with limited cohort size, the findings might be inevitably affected by selection bias. Second, the cutoff value for NLR, LMR, Alb and TC were determined through Galizia et al’s method,29 which makes these findings lack certain specificity. Third, although all patients received neoadjuvant and surgical treatment, patients had different postoperative adjuvant treatment, which may affect the long-term survival. Therefore, a larger, multicenter and prospective study is needed to verify our findings.
Conclusion
This study indicated that NPS is a superior predictor of survival outcomes compared with Alb, TC, NLR, LMR, BMI, PNI, and SIS. Besides, NPS could be utilized to guide the individualized treatment in resected LA-NSCLC patients after neoadjuvant treatment.
Data Sharing Statement
The data used to support to the findings of this study are available from the corresponding author upon request.
Ethics Approval and Consent to Participate
This study was approved by the ethics committee of the affiliated Suzhou Hospital of Nanjing Medical University. All authors confirmed that this study complied with the Declaration of Helsinki. And all individuals participating in this study signed written informed consent.
Acknowledgments
The authors would like to thank the patients who participated in this study as well as the research groups who played an important role in analyzing the data.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by Grant (GSWS2020067) from the Gusu Health Talent Program.
Disclosure
The authors declare no competing interests.
References
1. Ferlay J, Soerjomataram I, Dikshit R, et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer. 2015;136(5):E359–386. doi:10.1002/ijc.29210
2. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2019. CA Cancer J Clin. 2019;69(1):7–34.
3. Ettinger DS, Bepler G, Bueno R, et al. Non-small cell lung cancer clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2006;4(6):548–582.
4. Vansteenkiste J, Crino L, Dooms C, et al. 2nd ESMO Consensus Conference on Lung Cancer: early-stage non-small-cell lung cancer consensus on diagnosis, treatment and follow-up. Ann Oncol. 2014;25(8):1462–1474.
5. Blandin Knight S, Crosbie PA, Balata H, Chudziak J, Hussell T, Dive C. Progress and prospects of early detection in lung cancer. Open Biol. 2017;7(9):548.
6. David EA, Canter RJ, Chen Y, Cooke DT, Cress RD. Surgical Management of Advanced Non-Small Cell Lung Cancer Is Decreasing But Is Associated With Improved Survival. Ann Thorac Surg. 2016;102(4):1101–1109.
7. Roy MS, Donington JS. Management of locally advanced non small cell lung cancer from a surgical perspective. Curr Treat Options Oncol. 2007;8(1):1–14.
8. Chansky K, Detterbeck FC, Nicholson AG, et al. The IASLC Lung Cancer Staging Project: external Validation of the Revision of the TNM Stage Groupings in the Eighth Edition of the TNM Classification of Lung Cancer. J Thorac Oncol. 2017;12(7):1109–1121.
9. Segawa Y, Kiura K, Takigawa N, et al. Phase III trial comparing docetaxel and cisplatin combination chemotherapy with mitomycin, vindesine, and cisplatin combination chemotherapy with concurrent thoracic radiotherapy in locally advanced non-small-cell lung cancer: OLCSG 0007. J Clin Oncol. 2010;28(20):3299–3306.
10. Puri S, Shafique M, Gray JE. Immune Checkpoint Inhibitors in Early-Stage and Locally Advanced Non-Small Cell Lung Cancer. Curr Treat Options Oncol. 2018;19(8):39.
11. Rossi G, Pezzuto A, Sini C, et al. Concomitant medications during immune checkpoint blockage in cancer patients: novel insights in this emerging clinical scenario. Crit Rev Oncol Hematol. 2019;142:26–34.
12. Mok TSK, Wu YL, Kudaba I, et al. Pembrolizumab versus chemotherapy for previously untreated, PD-L1-expressing, locally advanced or metastatic non-small-cell lung cancer (KEYNOTE-042): a randomised, open-label, controlled, Phase 3 trial. Lancet. 2019;393(10183):1819–1830.
13. Tamayo-Bermejo R, Del Rio-Valencia JC, Mora-Rodriguez B, Munoz-Castillo I. Effectiveness and safety of pembrolizumab monotherapy in patients with locally advanced or metastatic non-small-cell lung cancer. J Oncol Pharm Pract. 2021;10781552211061117.
14. Diakos CI, Charles KA, McMillan DC, Clarke SJ. Cancer-related inflammation and treatment effectiveness. Lancet Oncol. 2014;15(11):e493–503.
15. Roxburgh CS, McMillan DC. Cancer and systemic inflammation: treat the tumour and treat the host. Br J Cancer. 2014;110(6):1409–1412.
16. Hainaut P, Plymoth A. Targeting the hallmarks of cancer: towards a rational approach to next-generation cancer therapy. Curr Opin Oncol. 2013;25(1):50–51.
17. Noble F, Hopkins J, Curtis N, et al. The role of systemic inflammatory and nutritional blood-borne markers in predicting response to neoadjuvant chemotherapy and survival in oesophagogastric cancer. Med Oncol. 2013;30(3):596.
18. Zhang X, Moriwaki T, Kawabata T, et al. Nicaraven Attenuates Postoperative Systemic Inflammatory Responses-Induced Tumor Metastasis. Ann Surg Oncol. 2020;27(4):1068–1074.
19. Barbetta A, Nobel TB, Sihag S, et al. Neutrophil to Lymphocyte Ratio as Predictor of Treatment Response in Esophageal Squamous Cell Cancer. Ann Thorac Surg. 2018;106(3):864–871.
20. Huang Q, Diao P, Li CL, et al. Preoperative platelet-lymphocyte ratio is a superior prognostic biomarker to other systemic inflammatory response markers in non-small cell lung cancer. Medicine. 2020;99(4):e18607.
21. Miyazaki T, Yamasaki N, Tsuchiya T, et al. Ratio of C-reactive protein to albumin is a prognostic factor for operable non-small-cell lung cancer in elderly patients. Surg Today. 2017;47(7):836–843.
22. Wang Y, Huang D, Xu WY, Wang YW, Che GW. Prognostic Value of Pretreatment Lymphocyte-to-Monocyte Ratio in Non-Small Cell Lung Cancer: a Meta-Analysis. Oncol Res Treat. 2019;42(10):523–531.
23. Guo D, Zhang J, Jing W, et al. Prognostic value of systemic immune-inflammation index in patients with advanced non-small-cell lung cancer. Future Oncology. 2018;14(25):2643–2650.
24. Sanabria A, Carvalho AL, Kowalski LP. Is nutrition support related to a poor prognosis in head and neck cancer patients? Thoughts about the secondary analysis of RTOG trial 90-03. Head Neck. 2007;29(5):518–519.
25. Sanchez-Lara K, Turcott JG, Juarez E, et al. Association of nutrition parameters including bioelectrical impedance and systemic inflammatory response with quality of life and prognosis in patients with advanced non-small-cell lung cancer: a prospective study. Nutr Cancer. 2012;64(4):526–534.
26. Imai H, Kishikawa T, Minemura H, et al. Pretreatment Glasgow prognostic score predicts survival among patients with high PD-L1 expression administered first-line pembrolizumab monotherapy for non-small cell lung cancer. Cancer Med. 2021;10(20):6971–6984.
27. Li W, Qu Y, Wen F, et al. Prognostic nutritional index and systemic immune-inflammation index are prognostic biomarkers for non-small-cell lung cancer brain metastases. Biomark Med. 2021;15(13):1071–1084.
28. Ohba T, Takamori S, Toyozawa R, et al. Prognostic impact of the Controlling Nutritional Status score in patients with non-small cell lung cancer treated with pembrolizumab. J Thorac Dis. 2019;11(9):3757–3768.
29. Galizia G, Lieto E, Auricchio A, et al. Naples Prognostic Score, Based on Nutritional and Inflammatory Status, is an Independent Predictor of Long-term Outcome in Patients Undergoing Surgery for Colorectal Cancer. Dis Colon Rectum. 2017;60(12):1273–1284.
30. Jin J, Wang H, Peng F, et al. Prognostic significance of preoperative Naples prognostic score on short- and long-term outcomes after pancreatoduodenectomy for ampullary carcinoma. Hepatobiliary Surg Nutr. 2021;10(6):825–838.
31. Xiong J, Hu H, Kang W, et al. Prognostic Impact of Preoperative Naples Prognostic Score in Gastric Cancer Patients Undergoing Surgery. Front Surg. 2021;8:617744.
32. Feng JF, Zhao JM, Chen S, Chen QX. Naples Prognostic Score: a Novel Prognostic Score in Predicting Cancer-Specific Survival in Patients With Resected Esophageal Squamous Cell Carcinoma. Front Oncol. 2021;11:652537.
33. Nakagawa N, Yamada S, Sonohara F, et al. Clinical Implications of Naples Prognostic Score in Patients with Resected Pancreatic Cancer. Ann Surg Oncol. 2020;27(3):887–895.
34. Li S, Wang H, Yang Z, et al. Naples Prognostic Score as a novel prognostic prediction tool in video-assisted thoracoscopic surgery for early-stage lung cancer: a propensity score matching study. Surg Endosc. 2021;35(7):3679–3697.
35. Li Q, Cong R, Wang Y, et al. Naples prognostic score is an independent prognostic factor in patients with operable endometrial cancer: results from a retrospective cohort study. Gynecol Oncol. 2021;160(1):91–98.
36. Wang Z, Wang Y, Zhang X, Zhang T. Pretreatment prognostic nutritional index as a prognostic factor in lung cancer: review and meta-analysis. Clin Chim Acta. 2018;486:303–310.
37. Li S, Zhang W, Yang Z, Li Y, Du H, Che G. Systemic Inflammation Score as a Novel Prognostic Indicator for Patients Undergoing Video-Assisted Thoracoscopic Surgery Lobectomy for Non-Small-Cell Lung Cancer. J Invest Surg. 2021;34(4):428–440.
38. Cheng X, Li C, Huang J, Lu P, Luo Q. Three-arm robot-assisted thoracoscopic surgery for locally advanced N2 non-small cell lung cancer. J Thorac Dis. 2018;10(12):7009–7013.
39. Iwasaki A, Shirakusa T, Maekawa T, Enatsu S, Maekawa S. Clinical evaluation of systemic inflammatory response syndrome (SIRS) in advanced lung cancer (T3 and T4) with surgical resection. Eur J Cardiothorac Surg. 2005;27(1):14–18.
40. Batchelor TJP, Rasburn NJ, Abdelnour-Berchtold E, et al. Guidelines for enhanced recovery after lung surgery: recommendations of the Enhanced Recovery After Surgery (ERAS(R)) Society and the European Society of Thoracic Surgeons (ESTS). Eur J Cardiothorac Surg. 2019;55(1):91–115.
41. Benker M, Citak N, Neuer T, Opitz I, Inci I. Impact of preoperative comorbidities on postoperative complication rate and outcome in surgically resected non-small cell lung cancer patients. Gen Thorac Cardiovasc Surg. 2022;70(3):248–256.
42. Pezzuto A, Trabalza Marinucci B, Ricci A, et al. Predictors of respiratory failure after thoracic surgery: a retrospective cohort study with comparison between lobar and sub-lobar resection. J Int Med Res. 2022;50(6):3000605221094531.
43. Sun KX, Zheng RS, Zeng HM, et al. The incidence and mortality of lung cancer in China, 2014. Chinese journal of oncology. 2018;40(11):805–811.
44. Abrams JM. Competition and compensation: coupled to death in development and cancer. Cell. 2002;110(4):403–406.
45. Salehi-Rad R, Li R, Paul MK, Dubinett SM, Liu B. The Biology of Lung Cancer: development of More Effective Methods for Prevention, Diagnosis, and Treatment. Clin Chest Med. 2020;41(1):25–38.
46. Alifano M, Mansuet-Lupo A, Lococo F, et al. Systemic inflammation, nutritional status and tumor immune microenvironment determine outcome of resected non-small cell lung cancer. PLoS One. 2014;9(9):e106914.
47. Fernandes JV, Cobucci RN, Jatoba CA, Fernandes TA, de Azevedo JW, de Araujo JM. The role of the mediators of inflammation in cancer development. Pathol Oncol Res. 2015;21(3):527–534.
48. Weitzman SA, Gordon LI. Inflammation and cancer: role of phagocyte-generated oxidants in carcinogenesis. Blood. 1990;76(4):655–663.
49. Zhou N, Liu L, Li D, Zeng Q, Song X. VCS parameters of neutrophils, monocytes and lymphocytes may indicate local bacterial infection in cancer patients who accepted cytotoxic chemotherapeutics. Eur J Clin Microbiol Infect Dis. 2016;35(1):41–48.
50. Abu-Shawer O, Abu-Shawer M, Hirmas N, et al. Hematologic markers of distant metastases and poor prognosis in gynecological cancers. BMC Cancer. 2019;19(1):141.
51. Shaul ME, Eyal O, Guglietta S, et al. Circulating neutrophil subsets in advanced lung cancer patients exhibit unique immune signature and relate to prognosis. FASEB J. 2020;34(3):4204–4218.
52. Vasiljeva O, Papazoglou A, Kruger A, et al. Tumor cell-derived and macrophage-derived cathepsin B promotes progression and lung metastasis of mammary cancer. Cancer Res. 2006;66(10):5242–5250.
53. Xu F, Cui WQ, Wei Y, et al. Astragaloside IV inhibits lung cancer progression and metastasis by modulating macrophage polarization through AMPK signaling. J Exp Clin Cancer Res. 2018;37(1):207.
54. Huang H, Zhang L, Chen DB, et al. Validation of Prognosis Value of Cumulative Prognostic Scores Based on Serum High-Density Lipoprotein Cholesterol and Albumin Levels in Patients with Colorectal Cancer. J Cancer. 2019;10(1):35–42.
55. Elahi MM, McMillan DC, McArdle CS, Angerson WJ, Sattar N. Score based on hypoalbuminemia and elevated C-reactive protein predicts survival in patients with advanced gastrointestinal cancer. Nutr Cancer. 2004;48(2):171–173.
56. Tokunaga R, Sakamoto Y, Nakagawa S, et al. CONUT: a novel independent predictive score for colorectal cancer patients undergoing potentially curative resection. Int J Colorectal Dis. 2017;32(1):99–106.
57. Kang R, Li P, Wang T, et al. Apolipoprotein E epsilon 2 allele and low serum cholesterol as risk factors for gastric cancer in a Chinese Han population. Sci Rep. 2016;6:19930.
58. Lieto E, Auricchio A, Tirino G, et al. Naples Prognostic Score Predicts Tumor Regression Grade in Resectable Gastric Cancer Treated with Preoperative Chemotherapy. Cancers. 2021;13(18):548.
59. Wu H, Fu M, Xie X, et al. Naples prognostic score, a novel prognostic score for patients with high- and intermediate-risk gastrointestinal stromal tumours after surgical resection. World J Surg Oncol. 2022;20(1):63.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Fibrinogen/Albumin Ratio Index as an Independent Prognostic Biomarker for Patients with Combined Hepatocellular Cholangiocarcinoma After Surgery
Xu J, Li S, Feng Y, Zhang J, Peng Y, Wang X, Wang H
Cancer Management and Research 2022, 14:1795-1806
Published Date: 23 May 2022
Associations Between Morphological Phenotypes of COPD and Clinical Characteristics in Surgically Resected Patients with COPD and Concomitant Lung Cancer
Suzuki Y, Kitaguchi Y, Ueno F, Droma Y, Goto N, Kinjo T, Wada Y, Yasuo M, Hanaoka M
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:1443-1452
Published Date: 21 June 2022
Identification of High-Risk Patients for Postoperative Myocardial Injury After CME Using Machine Learning: A 10-Year Multicenter Retrospective Study
Liu Y, Song C, Tian Z, Shen W
International Journal of General Medicine 2023, 16:1251-1264
Published Date: 7 April 2023
The Association of Cerebral Oxygen Desaturation with Postoperative Cognitive Dysfunction in Older Patients: A Review
Zhang CY, Yang YS, Pei MQ, Chen XL, Chen WC, He HF
Clinical Interventions in Aging 2024, 19:1067-1078
Published Date: 17 June 2024
Follow-up of Surgical and Nonsurgical Patients With Pulmonary Aspergillosis: A Real-World Study
Chen Z, Shang Y, Wasti B, Ou Y, Gong S, Xiang X, Ouyang R
Infection and Drug Resistance 2025, 18:1059-1070
Published Date: 21 February 2025