Back to Journals » International Journal of Nanomedicine » Volume 21
Nanoparticle-Based Targeted Drug Delivery Systems for Allergic Rhinitis: A Comprehensive Review
Authors Wang Y, Zhou Y, Liang B, Li S, Wang Z, Yan X, Gao Y, Li T, Qin Q, Yang S, Guo F, Nie J
Received 23 November 2025
Accepted for publication 9 March 2026
Published 27 March 2026 Volume 2026:21 581228
DOI https://doi.org/10.2147/IJN.S581228
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Jie Huang
Yuenan Wang,1,* Yang Zhou,2,3,* Boshen Liang,4,* Shuoming Li,1 Zhenning Wang,1 Xiaodong Yan,5 Yiqing Gao,1 Tiangang Li,1,6 Qiong Qin,7 Shaoli Yang,1,8 Fang Guo,1,7 Jian Nie1
1Basic Medical College, Yunnan University of Chinese Medicine, Kunming, Yunnan, People’s Republic of China; 2First Clinical Medical College, Yunnan University of Chinese Medicine, Kunming, Yunnan, People’s Republic of China; 3Joint Graduate School of Traditional Chinese Medicine of China, Suzhou, Jiangsu, People’s Republic of China; 4School of Public Health and Management, Guangzhou University of Chinese Medicine, Guangzhou, Guangdong, People’s Republic of China; 5Institute of Clinical Pharmacology, Nanchang University, Nanchang, Jiangxi, People’s Republic of China; 6Yunnan Provincial Key Laboratory of Integrated Traditional Chinese and Western Medicine for Chronic Disease in Prevention and Treatment, Kunming, Yunnan, People’s Republic of China; 7Department of Otolaryngology, The First Affiliated Hospital of Yunnan University of Chinese Medicine, Kunming, Yunnan, People’s Republic of China; 8Department of Specialist Outpatient, The Third Affiliated Hospital of Yunnan University of Chinese Medicine, Kunming, Yunnan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jian Nie, Basic Medical College, Yunnan Key Laboratory of Southern Medicinal Utilization, Yunnan University of Chinese Medicine, Kunming, Yunnan, People’s Republic of China, Email [email protected]
Abstract: Allergic rhinitis (AR) is an immunoglobulin E (IgE)-mediated immune response triggered by inhaled allergens, primarily involving type 2 cell-driven nasal mucosal inflammation. Current clinical management of AR relies on pharmacotherapy and immunomodulatory therapies but is limited by treatment time windows, bioavailability, and side effects. Rational design of nanodrug carriers can enhance drug bioavailability and enable targeted delivery. Nanoparticles (NPs) transport drugs or gene fragments to nasal tissues via passive or active targeting, thereby improving therapeutic efficacy while minimizing damage to healthy tissues. This review summarizes recent applications of NPs in preclinical and clinical AR treatment, highlighting strategies for targeted therapy using nanodrugs. It discusses the benefits and mechanisms of innovative drug delivery systems in the treatment of AR and provides a comprehensive catalog of such systems. Finally, it outlines future prospects for improved clinical translation.
Keywords: Allergic rhinitis, nanoparticles, nanodrug, drug delivery system, targeted therapy, passive targeting, active targeting
Introduction
Allergic rhinitis (AR), also known as hay fever, is an upper respiratory disease characterized by inflammation of the nasal mucosa, typically accompanied by symptoms such as nasal congestion, runny nose, sneezing, and nasal itching.1 Currently, approximately 500 million people worldwide are affected by AR.2 As a condition that often begins in childhood and may persist into adulthood, AR is among the most overlooked and poorly managed diseases. Research data indicate that the prevalence of AR among children and adolescents is 11.1% and 15.2%, respectively.3 The BAMSE study further reports that 75% of children with pollen-induced AR experience persistent symptoms into adulthood.4 AR often coexists with other diseases, such as asthma, chronic sinusitis and conjunctivitis. Beyond physical morbidity, AR significantly impacts mental health, increasing the risk of anxiety by 1.9 times and depression by 1.6 times,5 while elevating the risk of suicide attempts and suicide deaths.6 This considerable disease burden, coupled with annual healthcare costs reaching €4,827 per patient in a Dutch study,7 underscores the challenges in AR management and its economic impact on healthcare systems. Consequently, exploring effective treatment strategies that achieve long-term symptom control and improve patient quality of life remains a key focus in AR research.
Current treatment options for AR include environmental control, pharmacotherapy, and immunomodulatory therapy.8 First-line treatment for mild AR involves oral second-generation antihistamines or intranasal corticosteroids (INCS). For patients with moderate to severe persistent AR, a combination of intranasal antihistamines and INCS is recommended. However, antihistamines may cause adverse effects such as dryness, drowsiness, nasal irritation, and epistaxis. Long-term corticosteroid use may also lead to adrenal suppression, growth retardation in children, and osteoporosis.1,9 Although medication significantly alleviates symptoms and improves quality of life for most AR patients, some moderate-to-severe cases fail to achieve satisfactory outcomes even with high-dose therapy. Allergen-specific immunotherapy (AIT) is a proposed treatment strategy for such patients and remains the only option targeting the etiology of AR. It typically involves gradually increasing allergen doses via subcutaneous or sublingual routes to induce a sustained state of immune tolerance.10 While AIT’s unique immunomodulatory mechanism offers long-term benefits, its clinical application faces several challenges. The combination of local side effects from immunotherapy (eg injection site reactions with subcutaneous immunotherapy (SCIT)) or oral itching and gastrointestinal discomfort with sublingual immunotherapy (SLIT)) and a treatment duration of up to three years poses substantial barriers to patient compliance and therapeutic efficacy.11 Moreover, systemic reactions such as severe allergic responses, though rare, warrant heightened vigilance in pediatric populations or individuals with multiple allergen sensitivities.12,13
In recent years, nanoparticle-based drug delivery systems have progressively overcome the limitations of traditional therapies. Various organic, inorganic, and hydrogel nanoparticles (NPs) serve as carriers capable of directing therapeutic agents to specific cells or tissues, enhancing the solubility of hydrophobic drugs, prolonging drug retention time, and enabling controlled drug release.14 The application potential of NPs lies in their characteristics such as size, hydrophobicity, and surface parameters. When particle size reaches the nanoscale, the increased surface area enhances interactions between carriers and drugs. Surface charge or adhesive surface modifications can improve drug penetration through biological barriers and accumulation at target sites, thereby achieving passive targeting.15 Furthermore, by introducing specific ligands onto their surfaces, NPs can achieve active targeting through specific binding to cell surface antigens,16 thereby effectively enhancing drug cellular targeting and avoiding non-specific drug distribution. Consequently, NPs demonstrate potential in drug delivery for treating various diseases including AR.
This paper introduces the characteristics and advantages of NPs based on the pathogenesis and delivery strategies of AR. Building on this foundation, it focuses on targeted delivery strategies using NPs in AR therapy, categorizing them into passive and active targeting according to their mechanisms of action. It comprehensively summarizes and explores the application of therapeutic drugs combined with various functionalized NPs in AR, aiming to provide novel strategies and insights for AR treatment.
Literature Search Strategy and Methodology
This paper adopts a narrative review format to systematically organize relevant research literature. Literature searches were conducted in PubMed, Web of Science, SpringerLink, and Google Scholar databases. The following keywords were used individually or in combination: “Nanoparticles”, “Nanodrug delivery systems”, “Poly(lactic-co-glycolic acid)”, “Chitosan”, “Nanomicelles”, “Liposomes”, “Extracellular vesicles”, “Virus-like particles”, “Gold nanoparticles”, “Silver nanoparticles”, “Copper oxide nanoparticles”, “Silica nanoparticles”, “Aluminum oxide nanoparticles”, “Hydrogel nanoparticles”, “Active targeted delivery”, “Passive targeted delivery”, “Allergic rhinitis”, “Hay fever”, “Pollinosis”, and “Nasal mucosal inflammation”. Results encompass publications from 2020 to 2025. The objective was to gather data on the association between AR and NPs, as well as the role of nanodrug interventions in AR. Included articles are categorized according to following subsections of this review. To visually demonstrate the research intensity and development trends of different NPs during this period, we have plotted a trend chart based on the search results for the aforementioned keywords (Figure 1).
 |
Figure 1 Trend chart of research development related to nanodrugs for AR treatment. In the left graph, the Y-axis represents the number of articles published per year; the right graph shows the proportion of nanodrug types used for AR treatment. |
Pathogenesis of AR
AR is a T-helper type 2 inflammatory response triggered by allergens,2 involving two critical phases: sensitization phase and effector phase. During sensitization, allergens such as pollen or dust mites initially encountered penetrate the compromised nasal mucosal epithelial barrier. Antigen-presenting cells (APCs) engulf these allergens and present antigenic information to helper T cells, leading to T helper 1/T helper 2 (Th1/Th2) and regulatory T/T helper 17 (Treg/Th17) immune dysregulation.17 B cells differentiate into plasma cells and produce allergen-specific immunoglobulin E (IgE) antibodies. Upon subsequent exposure to the same allergen, it binds to IgE on the surface of mast cells and basophils, triggering IgE cross-linking and activating these cells. This leads to degranulation and the release of mediators such as histamine (early phase) and newly synthesized leukotrienes, prostaglandins, and cytokines (late phase), thereby initiating an allergic inflammatory response (effector phase). Collectively, this process results in the clinical manifestations of AR.18
The Sensitization Phase of AR
During the sensitization phase, proteases carried by the allergen damage the barrier function of the nasal epithelium and accelerate the production of pro-inflammatory factors. Simultaneously, the allergen induces immune cell activation through protease-dependent pathways, ultimately promoting IgE production and binding to the Fc epsilon receptor (FcεR). This process establishes a sensitized state in the body.
Damaged Nasal Epithelial Barrier
The nasal epithelium serves as the primary defense barrier of the respiratory tract, effectively resisting the pathogens, allergens, and other harmful substances.19 Studies indicate reduced expression of tight junction proteins such as occludin, claudins, and Zonula Occludens-1 (ZO-1) in AR patients resulting in damage to the epithelial barrier.20 Common allergens, such as pollen, house dust mites (HDM), and animal dander,8 contain specific proteases (eg Phl p 1, Der p 1, and Fel d 1) that activate receptors on nasal epithelial cells (NECs), initiating immune responses. This leads to downregulation of tight junction protein expression, compromising the nasal epithelial barrier integrity.21 Additionally, activated NECs release “alarm molecules” such as interleukin-25 (IL-25), interleukin-33 (IL-33), and thymic stromal lymphopoietin (TSLP), which further activate group 2 innate lymphoid cells (ILC2s) and Th2 cells, promoting the production of type 2 cytokines such as interleukin-4 (IL-4) and interleukin-13 (IL-13). These cytokines enhance inflammatory cell activation and disrupt tight junctions in epithelial cells to amplify immune responses.22
Antigen-Presenting
Upon initial contact with the body, allergens trigger the secretion of “alarm molecules” by damaged NECs, which recruit and activate APCs such as dendritic cells (DCs) and macrophages.21 Once activated, these APCs migrate to regional lymph nodes, where they present antigens via major histocompatibility complex class II (MHC-II) and deliver CD80/CD86 co-stimulatory signals. This process induces the differentiation of naïve CD4+ T cells into Th2 cells, which produce type 2 cytokines including IL-4, interleukin-5 (IL-5), and IL-13.23 Concurrently, these cytokines activate ILC2s to produce local type 2 cytokines, further promoting B cell differentiation into plasma cells and the production of specific IgE (sIgE), which then binds to FcεR on the surface of mast cells and basophils, establishing the sensitized state.24
The Effector Phase of AR
AR follows the sensitization phase, the inflammatory response triggered when the body is re-exposed to the same allergen, primarily driven by mast cell activation and Th2-type immune responses.
Early-Phase Reaction
Within minutes of subsequent allergen re-exposure in the nasal cavity, they directly bind to sensitized IgE-FcεR complexes on the surface of mast cells and basophils, triggering degranulation and the release of mediators such as histamine, prostaglandin D2, and leukotrienes.25 Next, histamine acts on H1 receptors at trigeminal nerve endings and transmits signals to the central nervous system, causing symptoms such as nasal itching and sneezing. It also stimulates mucous glands to secrete watery discharge, leading to rhinorrhea. Mediators like leukotrienes and prostaglandins induce nasal congestion by causing vascular leakage and nasal mucosal hyperemia.26 Additionally, the release of fibroblast growth factor-2 and vascular endothelial growth factor from mast cells further promotes vasodilation and inflammatory cell infiltration, exacerbating tissue edema and nasal mucosal swelling.27
Late-Phase Reaction
The late phase reaction occurs 4–12 hours after allergen challenge and is primarily characterized by infiltration of eosinophils, Th2 cells, and ILC2s into the nasal mucosa.28 Activation of these type 2 immune cells sustains the inflammatory response during the late phase of AR. As previously noted, epithelial cell-derived IL-25, IL-33 and TSLP mediate ILC2 secretion of IL-5 and IL-13. Concurrently, IL-33 binds to the ST2 receptor on Th2 cell surfaces, inducing production of IL-4, IL-5, and IL-13.29 These cytokines induce B cells to differentiate into plasma cells that generate increased amounts of allergen-sIgE. This sIgE binds to high-affinity Fc receptors on mast cells, leading to sustained mast cell activation and the release of inflammatory mediators such as histamine, leukotrienes, and prostaglandins, thereby exacerbating vasodilation and clinical symptoms.18 Leukotrienes can also further activate eosinophils by binding to cysLT receptors.30 Similarly, IL-5 induces eosinophil recruitment and activation, leading to the release of granule proteins such as major basic protein (MBP) and eosinophil peroxidase (EPO), which directly damage the nasal mucosal epithelium.31 Furthermore, Th2 cell-derived IL-4 downregulates tight junction proteins, disrupting the nasal epithelial barrier and exacerbating the host’s immune response to allergens.32
As a complex allergic inflammatory disease, the core pathogenesis of AR lies in the abnormal immune response to inhaled allergens. Multiple immune cells collectively drive the onset and progression of inflammation by secreting cytokines and chemokines and activating related signaling cascades. The underlying mechanism is illustrated in Figure 2.
 |
Figure 2 The pathogenesis of AR. When the human body first encounters allergens, these substances penetrate the damaged nasal mucosal epithelial barrier. Antigen-presenting cells engulf the allergens and present antigenic information to Th2 cells, thereby activating B cells to differentiate into plasma cells and produce allergen-specific IgE antibodies. Simultaneously, the allergen triggers NECs to produce IL-25, IL-33, and TSLP, which in turn activate ILC2s and Th2 cells to produce inflammatory mediators such as IL-4 and IL-13. This process drives B cell differentiation into plasma cells producing allergen-specific IgE antibodies and disrupts tight junctions in epithelial cells, further damaging the epithelial barrier. Upon re-exposure to the same allergen, the allergen binds to IgE on the surface of mast cells and basophils, triggering IgE-FcεRI cross-linking. This activates these cells and induces degranulation, releasing mediators such as histamine. Concurrently, ILC2s and Th2 cells produce IL-5, which recruits and activates eosinophils. These eosinophils release granular proteins such as MBP and EPO, damaging the nasal mucosal epithelium and ultimately leading to the manifestation of AR symptoms. |
Classification of NPs
NPs generally refer to particles with at least one dimension of 100 nm or smaller. As a versatile drug delivery platform, they enable targeted delivery of therapeutics to specific cells or tissues,14 owing to their large surface-to-volume ratio and unique chemical, electronic, optical, magnetic, and mechanical properties. Based on their characteristics, NPs are categorized into organic (Poly(lactic-co-glycolic acid) (PLGA), liposomes, chitosan, etc), inorganic (metals, non-metals, metal oxides, etc), and hydrogel NPs. NPs improve pharmacokinetic properties, prolong drug circulation time in vivo, and reduce potential toxicity; Additionally, they provide pathways for achieving precise targeted delivery, regulating drug release rates, and enhancing the solubility of poorly soluble drugs (Figure 3, Table 1).33
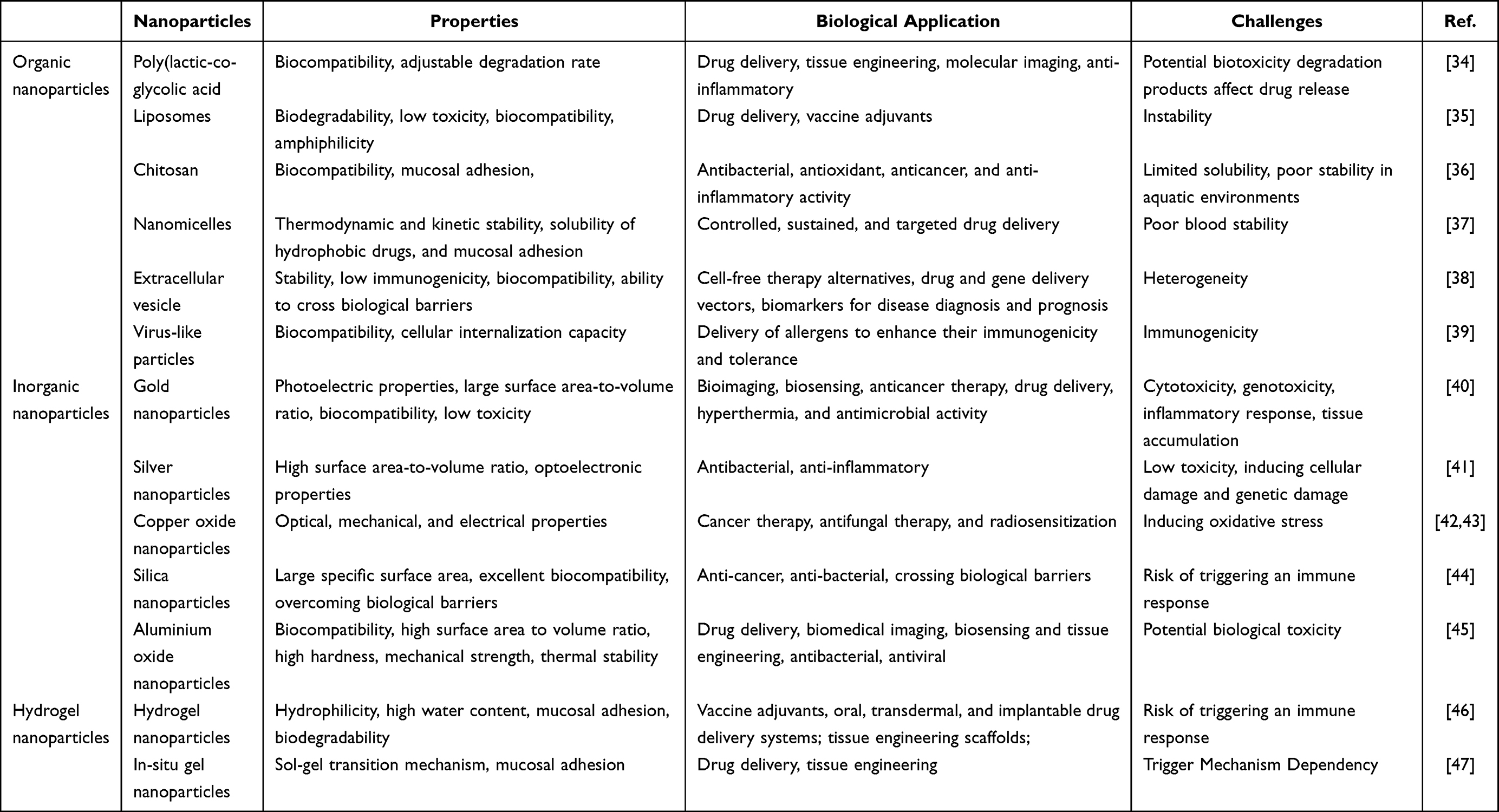 |
Table 1 Advantages and Challenges of Commonly Used NPs |
 |
Figure 3 Preparation and delivery of NPs. (A) Classification of organic and inorganic NPs. (B) NP preparation primarily involves three steps: selection of the nanocarrier, surface modification of the nanocarrier, and encapsulation of the payload. (C) NPs act on relevant targets in patients with AR. (D) NPs are delivered to targeted tissues via various administration routes, including intranasal, subcutaneous, and sublingual delivery. |
Organic NPs
Organic NPs are typically solid NPs composed of proteins, lipids, polymers, and carbohydrates, generally ranging from 10 to 100 nm in diameter but capable of reaching up to 1000 nm. They exhibit key properties such as non-toxicity and biodegradability, enabling their use across various biomedical fields, including targeted drug delivery, bioimaging, disease therapy, and biosensing.48 Currently, several types of organic NPs are available, such as liposomes, nanomicelles, PLGA, extracellular vesicles and virus-like particles,49 which have shown potential in treating AR (Table 2).
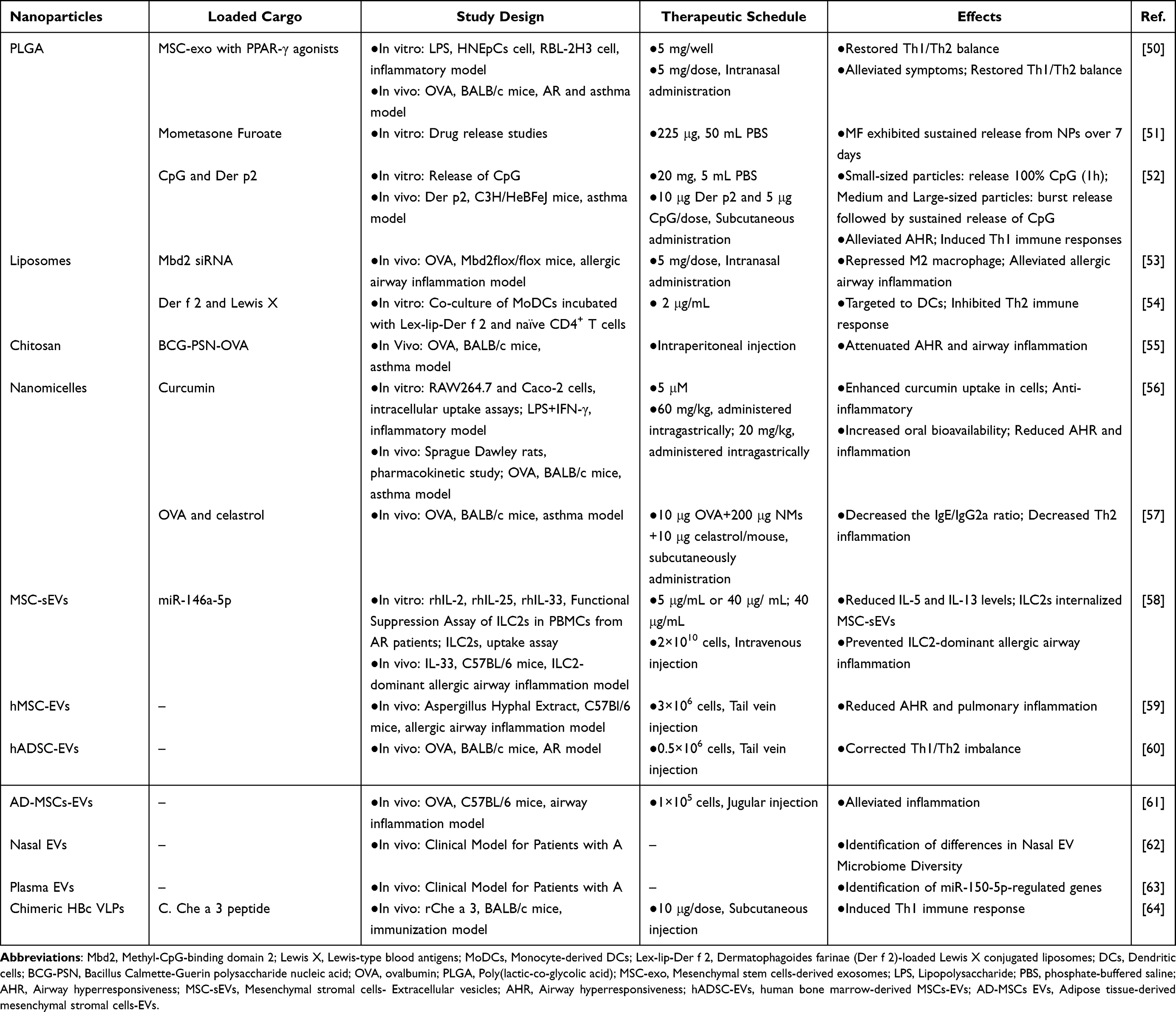 |
Table 2 Potential Applications of Organic Nanoparticles in AR |
PLGA
PLGA is a biodegradable copolymer synthesized from lactic acid and glycolic acid. Due to its excellent biocompatibility, tunable degradation rate, and versatile ability to encapsulate diverse therapeutic agents, it is widely used in biomedical applications.34 PLGA can encapsulate small molecules, proteins, nucleic acids, and inorganic nanoparticles, allowing controlled drug release from days to months depending on its molecular weight, particle size, and lactide-to-glycolide ratio.65
PLGA serves as a carrier to prolong drug release and enhance local drug retention. One study demonstrated that PLGA NPs could persist in the nasal cavity for up to 120 hours, enabling sustained release of mesenchymal stem cell-derived exosomes and peroxisome proliferator-activated receptor (PPAR)-γ agonists and effectively alleviating AR inflammation.50 Far et al further showed that PLGA NPs loaded with mometasone furoate achieved sustained drug release for up to 7 days, prolonging exposure to the nasal mucosa.51 In immunotherapy, PLGA NPs protect therapeutic agents from premature degradation while ensuring controlled and sustained release.66 A study found that small-sized PLGA NPs effectively protected encapsulated cytosine-phosphate-guanine (CpG) motifs from degradation, resulting in a stronger initial burst release and sustained delivery. Coating CpG-loaded PLGA with Der p 2 markedly reduced airway hyperresponsiveness and inflammation in asthma-prone mice.52 However, the hydrophobic surface of PLGA hinders the loading of hydrophilic protein antigens, restricting its application in immunotherapy.65 Nonetheless, PLGA remains a highly promising delivery system for AR due to its tunable release properties, safety, and multifunctionality.
Liposomes (LPs)
LPs are spherical lipid vesicles composed of amphiphilic molecules derived from phospholipids, cholesterol, non-toxic surfactants, or membrane proteins. Their biodegradability, biocompatibility, low immunogenicity, low toxicity, and amphiphilic nature make them excellent carriers for drug delivery.35
As an efficient drug delivery system, LPs can encapsulate various nucleic acid molecules.67 In respiratory RNA therapy, Wu et al found that Mbd2 siRNA-loaded liposomes protected mice from ovalbumin (OVA)-induced allergic airway inflammation and inhibited macrophage polarization toward the M2 phenotype.53 LPs are also promising carriers for intranasal vaccines, capable of enhancing immune responses through mucosal and cell-specific targeting. Peng et al designed a dendritic cell-targeted nanovaccine using liposomes loaded with recombinant dermatophagoides farinae allergen group 2 (Der f 2) and conjugated with the DC-SIGN ligand Lewis X. This nanovaccine significantly suppressed Th2-type immune responses.54 However, liposomes suffer from structural instability, which can be mitigated by surface modification or formulation into nanoemulsions.68 Overall, LPs offer significant advantages for treating allergic airway inflammatory diseases. Future research should focus on enhancing their stability and targeting precision to accelerate clinical translation.
Chitosan
Chitosan is a natural polysaccharide derived from chitin through deacetylation. It can self-assemble into NPs in the presence of hydrophobic components or under specific pH conditions and is primarily excreted via the renal pathway.36
Several studies have confirmed Chitosan’s molecular-level immunomodulatory and anti-inflammatory effects in respiratory inflammatory diseases. Yang et al demonstrated that chitosan NPs co-loaded with Bacillus Calmette-Guerin polysaccharide nucleic acid (BCG-PSN) and OVA effectively reduced airway hyperresponsiveness and inflammation in asthmatic mice.55 Their surface cationic groups form strong electrostatic interactions with anionic mucosal components, prolonging drug residence time and enhancing local bioavailability, offering a novel approach for intranasal drug delivery in AR.69
Nanomicelles (NMs)
NMs are self-assembled colloidal dispersions at the nanoscale, characterized by a hydrophobic core and a hydrophilic shell. They are commonly classified into regular micelles (eg polyethylene glycol–polylactic acid (PEG-PLA), PEG-PLGA micelles), reverse micelles (eg polycaprolactone (PCL)-P2VP micelles), and monolayer micelles (eg core-in-shell PEG micelles in aqueous media). NMs exhibit thermodynamic and kinetic stability, excellent solubilization capacity for hydrophobic drugs, and strong mucoadhesive properties, making them widely applied in drug delivery systems.37 Polymeric micelles, formed by the self-assembly of amphiphilic block copolymers such as PEG-PLA via hydrophobic interactions and hydrogen bonding, possess stable core-shell structures, controllable drug-loading capacity, and a narrow particle size distribution, which protect encapsulated drugs from oxidation and degradation.70 Recently, NMs have gained increasing attention as potential therapeutic tools for allergic airway diseases. They can be engineered to deliver anti-inflammatory drugs, bronchodilators, or immunomodulators directly to inflamed airway tissues.71 Wang et al developed hybrid nanomicelles by self-assembling two amphiphilic polymers for curcumin delivery. In an asthma mouse model, this nanodrug effectively alleviated OVA-induced airway hyperresponsiveness and inflammation.56 Similarly, Peng et al designed OVA-conjugated, celastrol-loaded NMs as a novel vaccine for AIT. This formulation reduced inflammatory cell infiltration in an OVA-induced allergic airway inflammation mouse model.57
Beyond PLGA, chitosan, and nanomicelles, protein-based materials (eg, albumin, gelatin, collagen) and synthetic polymers (eg, PLA, PEG, PCL) can also form diverse, stable polymeric nanostructures through self-assembly or chemical modification. These structures are used to encapsulate or adsorb active compounds, further expanding the potential of nanoparticle-based drug delivery systems.72
Extracellular Vesicles (EVs)
EVs are nanoscale, lipid-bound vesicles secreted by cells into the extracellular space, typically ranging from 30 to 200 nm in diameter. They can be produced by various cell types, including mesenchymal stem cells (MSCs), immune cells, and tumor cells. Based on their biogenesis mechanisms, release pathways, size, content, and functions, EVs are classified into types such as microvesicles, exosomes, and apoptotic bodies.38 EVs exhibit remarkable stability, low immunogenicity, high biocompatibility, extended circulation time, and exceptional ability to cross biological barriers. Consequently, they are widely investigated as cell-free therapeutic platforms, drug and gene delivery vehicles, diagnostic biomarkers, and vaccine development tools.73
EVs derived from different cellular sources show great promise in treating airway inflammation. Fang et al reported that small extracellular vesicles (sEVs) derived from MSC could reduce ILC2 populations, Th2 cytokine levels and airway hyperresponsiveness in an IL-33-induced-ILC2-dominant mouse model.58 Similarly, human bone marrow-derived sEVs improved severe refractory allergic airway inflammation induced by aspergillus mycelium extract in mice.59 Yang et al found that EVs derived from human adipose-derived stem cells (hADSC-EVs) alleviated AR symptoms by restoring Th1/Th2 balance.60 Beyond their intrinsic therapeutic effects, EVs function as drug delivery vehicles. In the same study, Fang’s group demonstrated that MSC-sEVs alleviated allergic airway inflammation by delivering miR-146a-5p.58 De Castro et al found that EVs derived from adipose tissue–derived MSCs (AD-MSCs) effectively reduced eosinophil infiltration in lung tissue and modulated airway remodeling.61 Additionally, EVs secreted by inflammatory and immune cells are valuable for studying AR pathogenesis. Chiang et al analyzed nasal EVs from AR patients and identified microbial communities such as acinetobacter, mycoplasma, escherichia coli, and fluorescentia within them, which may influence pathways like selenide metabolism and protein kinase signaling, thereby affecting AR progression.62 Fang et al also identified Der p 1 and antigen-presenting molecules in plasma EVs from AR patients, demonstrating their role in Th2 cell differentiation. Elevated miR-150-5p levels in plasma EVs were linked to increased Th2 and ILC2 differentiation.63 Despite these advantages, the complex biogenesis mechanisms and cellular heterogeneity of EVs pose challenges for accurately assessing therapeutic efficacy and may introduce potential safety concerns.74
Virus-Like Particles (VLPs)
VLPs are non-infectious nanoscale particles formed by the self-assembly of viral proteins encoding capsid, core, or envelope structures, but lacking viral genetic material.75 VLPs possess superior biocompatibility, cellular uptake capacity, ease of functionalization, and specific cellular targeting properties.39
Sani et al found chimeric HBc VLPs, which are fused with hepatitis B core antigen (HBc) and Che a 3 were capable of inducing antigen-specific immune responses.64 Interestingly, VLPs ranging from 20 to 200 nm can readily enter lymph nodes, facilitating efficient uptake by APCs.76 VLPs enriched with CpG motif DNA can be used in AR therapy, as CpG motifs activate Toll-like receptor 9 (TLR9), which can promote Th1 responses.77 Future research should further explore the therapeutic potential of VLPs and CpG motifs in AR immunotherapy, both as standalone interventions and in combination with allergen-specific immunotherapy strategies, to expand their clinical applicability.
Inorganic NPs
Inorganic NPs primarily include various metals (gold, silver, etc)., metal oxides (copper oxide, zinc oxide, etc)., and semiconductor nanoparticles. Due to their controllable size, unique optical properties, conductivity, magnetic behavior, catalytic activity, and excellent biocompatibility, they have been extensively studied in the biomedical field as therapeutic agents for disease treatment78 (Table 3).
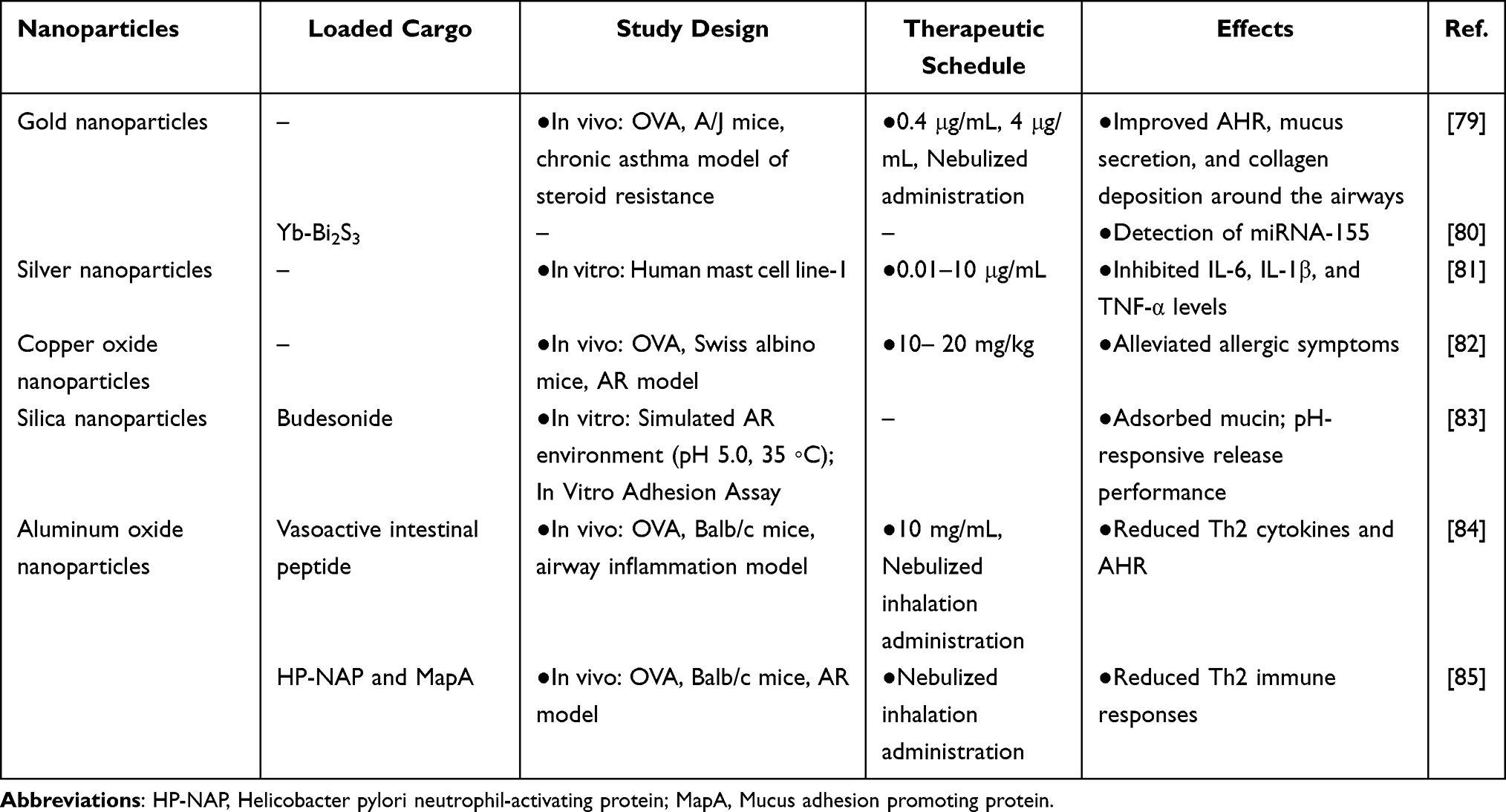 |
Table 3 Potential Applications of Inorganic Nanoparticles in AR |
Gold Nanoparticles (AuNPs)
Gold (Au) is one of the earliest studied metallic elements, with its inherent properties and stability widely utilized across various fields. AuNPs not only inherit the stability of gold86 but also exhibit optoelectronic properties, a high surface-to-volume ratio, excellent biocompatibility, and low toxicity, making them ideal materials for both medical and non-medical applications.40 Serra et al reported that AuNPs can alleviate airway inflammation in steroid-resistant asthma by protecting nuclear factor erythroid 2-related factor 2 (NRF2) and histone deacetylase 2 (HDAC2).79 Furthermore, AuNPs show promising applications in AR diagnostics. Liu et al created a Yb-Bi2S3/AuNP nanocomposite capable of specifically recognizing the AR biomarker miRNA-155.80 Regarding AuNP synthesis, biosynthetic approaches have emerged as a significant alternative to traditional chemical synthesis due to their environmental friendliness, low cost, high reproducibility, and avoidance of hazardous reagents.87 Therefore, further development of biosynthetic AuNPs warrants continued research.
Silver Nanoparticles (AgNPs)
AgNPs possess a high surface area-to-volume ratio, reactivity, optoelectronic properties, and antibacterial characteristics, making them widely used in the medical field.41 AgNPs also exhibit potent anti-inflammatory properties, drawing attention for potential use in AR treatment. Gao et al reported that biosynthetic NPs derived from Ostericum koreanum extract inhibited mast cell production of IL-6, IL-1β, and TNF-α, potentially alleviating mast cell-mediated allergic inflammation by suppressing extracellular regulated protein kinases (ERK), caspase-1, and nuclear factor kappa-B (NF-κB) signaling pathways.81 Although research on AgNPs for AR remains limited, the available evidence highlights their therapeutic potential through anti-inflammatory effects. Biosynthetically prepared AgNPs not only enhance synthesis efficiency but also align with green chemistry principles. However, the biosafety of AgNPs requires careful evaluation. Studies indicate that AgNPs can induce apoptosis, oxidative stress, and genotoxicity in various cell types, with toxic effects typically inversely correlated with particle size.88 The conjugation of AgNPs with anticancer agents represents a novel strategy for targeted cancer cell therapy developed over the past decade, achieving synergistic effects and improved drug dosing.89 Future studies should further explore AgNP-drug conjugates, including systematic evaluation of their in vivo pharmacokinetics, biodistribution, metabolism, and toxicity mechanisms, to advance clinical translation.
Oxide Nanoparticles
Copper oxide NPs (CuO NPs) possess optical, mechanical, and electrical properties that enable them to interact with biological systems at the cellular level, regulating various biochemical reactions and physiological functions. They are currently applied in tumor therapy, antifungal treatments, and radiosensitization.42,43 Liu et al synthesized CuO NPs using Laurus nobilis extracts, such as eugenol, as reducing agents and stabilizers. This green synthesis approach alleviated allergic symptoms such as sneezing in OVA-induced AR mice.82 Plant-derived green-synthesized CuO NPs exhibit lower toxicity but may still induce oxidative stress-mediated toxicity through reactive oxygen species.90 Research on metal oxide NPs remains in its early stages; thus, addressing toxicity concerns while enhancing biomedical potential remains a key priority.
Silica NPs (SNPs) show significant potential in therapeutic and diagnostic applications due to their large surface area, ease of synthesis and surface modification, excellent biocompatibility, and ability to cross biological barriers such as the blood-brain and mucosal barriers.44,91 Peng et al developed a nasal delivery system based on diatomaceous earth-derived SNPs for loading the anti-inflammatory drug budesonide. The system significantly enhanced mucosal adhesion and enabled sustained drug release for up to 96 hours, with negligible cytotoxicity toward human skin fibroblasts (HSF) even at concentrations up to 1000 μg/mL, confirming excellent safety.83 These findings highlight the strong application potential of this nanoparticle system for rhinitis therapy. Moreover, optimized mesoporous silica NPs (MSNPs) with tunable pore structures act as effective drug carriers.92 However, other studies suggest that engineered silica NPs may exacerbate allergic airway diseases. Therefore, addressing long-term exposure safety and establishing comprehensive toxicological profiles across different delivery routes remain essential.93
Aluminum oxide (Al2O3) NPs (AlNPs) are porous nanomaterials with high surface area, mechanical strength, and thermal stability, widely used in industry but now attracting attention for biomedical use due to their biocompatibility and ease of surface functionalization.45 Conjugation of AlNPs with vasoactive intestinal peptide has demonstrated positive effects in treating allergic asthma, effectively reducing serum IgE levels and Th2 cytokines in OVA-induced allergic asthma mice.84 Another study demonstrated that peptide-conjugated AlNPs decreased inflammatory mediators such as IL-4, IL-33, IgE, and OVA-IgE, significantly alleviating allergic symptoms in AR mice.85 Collectively, these findings suggest that AlNPs, owing to their strong conjugation capacity with bioactive molecules and immunoregulatory effects, hold significant promise for treating nasal inflammation and offer new strategies for targeted rhinitis intervention.
Hydrogel Nanoparticles (HNPs)
Hydrogels are three-dimensional network structures formed by hydrophilic polymer chains through physical or chemical crosslinking, characterized by a high water content (over 90%).94 While conventional hydrogels are typically preformed, in situ gelation represents a specialized type that remains liquid in vitro but rapidly gels upon entering the body in response to physiological stimuli (eg, temperature, pH, or ionic concentration changes).46 This “sol-gel” transformation mechanism enables precise controlled drug release and significantly enhances treatment comfort and patient compliance. Based on their response mechanisms, in situ gels can be categorized as thermosensitive, ion-responsive, pH-sensitive, or multi-responsive.47 These systems show considerable potential for nasal and ocular drug delivery (Table 4). For example, Altuntaş et al developed an innovative thermosensitive mometasone furoate in situ gel that undergoes gelation upon temperature change during intranasal administration, achieving sustained local anti-inflammatory effects in a rat model of AR.95
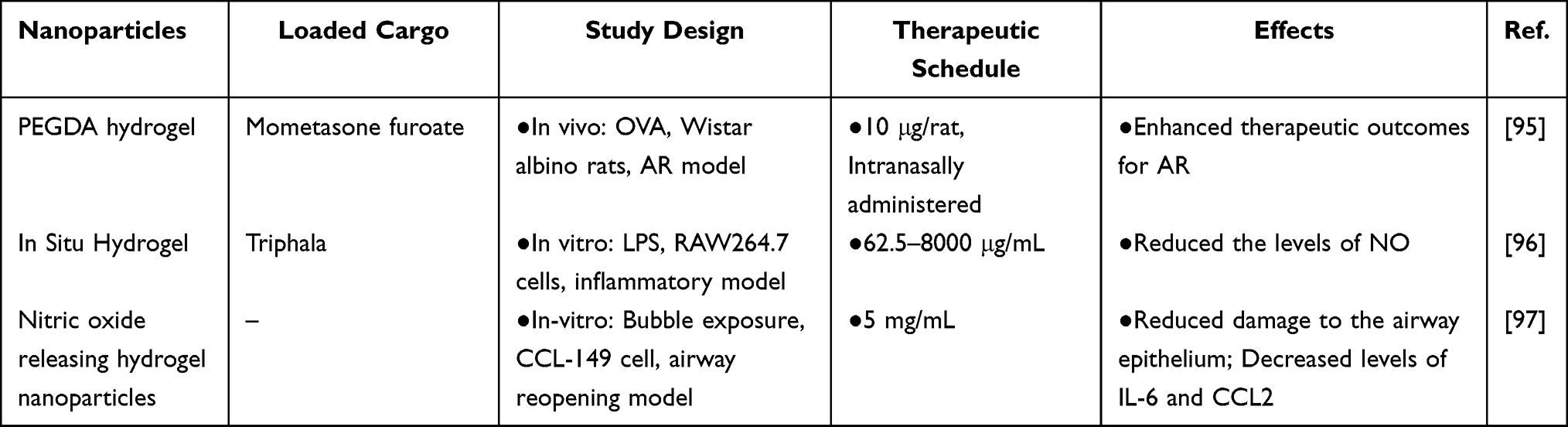 |
Table 4 Potential Applications of Hydrogel Nanoparticles in AR |
Owing to their excellent mucosal adhesion, hydrogels can significantly prolong drug retention time in the nasal cavity, making them highly promising nasal delivery carriers.98 Common strategies include preparing hydrogel NPs (often called nanogels or hydrogel NPs (HNPs) when submicron in size)99 or embedding NPs within a hydrogel matrix to form NP–hydrogel composite systems.100 The hydrogel component enhances tissue retention and biocompatibility, while the NPs facilitate sustained drug release.
Phongpradist et al designed a thermoresponsive in situ hydrogel system for delivering Triphala extract. Upon intranasal administration, this system gels at 34 °C, exerting antioxidant and anti-inflammatory effects to treat nasal disorders including AR, chronic sinusitis, and nasal polyps.96 Shurbaji et al designed nitric oxide (NO)-releasing hydrogel NPs with the ability to mitigate airway epithelial injury and reduce inflammatory mediators such as IL-6 and CCL2.97 While nano-hydrogels offer significant advantages for drug delivery, their application in rhinitis treatment remains in its infancy, lacking standardized in vitro evaluation models. Future research should focus on establishing more robust in vitro cellular and nasal mucosal models, developing standardized in vitro screening platforms, and systematically optimizing hydrogel nanoparticle preparation parameters to advance clinical translation.101
In summary, nanotechnology offers novel pathways for AR treatment that transcend conventional strategies. Various nanoparticle platforms, including organic nanoparticles, inorganic nanoparticles, and hydrogel nanoparticles, can enhance drug solubility, improve mucosal permeability, prolong intranasal retention, and enable targeted delivery to immune cells. These advantages make NPs an ideal platform for AR treatment (Supplementary Table 1).
Strategies for Nanodrug Targeting Delivery in AR Treatment
Targeting delivery strategies have been widely adopted in AR therapy. Observing that inflammatory sites exhibit enhanced permeability and retention (EPR) effect,102 NPs can exploit this pathological feature to achieve improved localization. In addition, NPs can be engineered with specific ligand modifications to create active targeted drug delivery systems, enabling precise drug delivery. Currently, nanodrugs based on both passive and active targeting strategies show significant potential in AR therapy (Figure 4). This section summarizes their design strategies and application progress to guide future research and promote clinical translation.
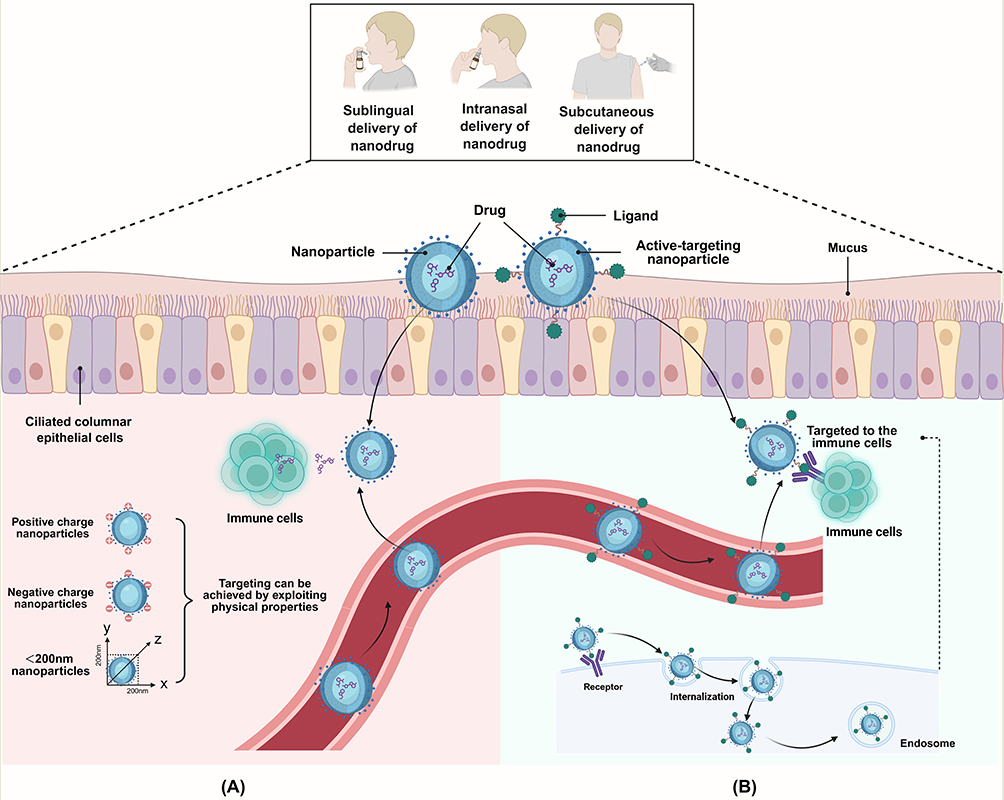 |
Figure 4 Passive and active targeting of nanodrug to the nasal cavity. (A) Nano drugs pass through the barrier, enter the nasal cavity, and reach the target cells. (B) Introducing specific functional groups or bioactive molecules, such as receptor and specific-adaptor for immune cells. |
Passive Targeting Delivery
Passive targeting relies on the physicochemical properties of nanocarriers such as particle size, surface charge, hydrophobicity, and non-specific adsorption capacity which enable them to accumulate selectively in specific tissues or organs, or be effectively delivered into the cytoplasm.103 Passive targeting strategies enhance drug accumulation at target sites through NPs, making them an ideal solution. The main delivery routes currently explored include intranasal, sublingual, and transdermal administration, all of which require drugs to traverse biological barriers and be absorbed via cellular or paracellular pathways. This places high demands on nanoparticle design.104–106 First, particle size. Appropriate size facilitates penetration through the mucus layer. For intranasal administration, NPs smaller than 150 nm are able to diffuse freely and permeate the mucosa more effectively. For transdermal and subcutaneous delivery, particle sizes between 20 and 200 nm are generally suitable. Second, surface charge. Neutral or slightly negatively charged NPs penetrate the mucus network more easily, whereas positively charged ones show stronger adhesion and uptake by mucosal epithelial cells. Third, surface hydrophilicity/hydrophobicity, rigidity, and the presence of targeting ligands also influence transmembrane transport efficiency.107 Pathological conditions involving thickened mucus, inflammatory cell infiltration, and elevated enzyme activity further alter barrier permeability. Therefore, NPs must adapt their physicochemical properties to the microenvironment to achieve efficient and precise delivery (Supplementary Table 2).
Commonly Used Clinical Drug Delivery
The primary clinical treatments for AR include glucocorticoids, antihistamines, leukotriene receptor antagonists, and mast cell stabilizers. However, these drugs generally suffer from low bioavailability, and long-term use may trigger adverse reactions such as osteoporosis, gastrointestinal discomfort, and headaches, severely limiting their clinical applicability and therapeutic efficacy. Therefore, developing efficient and safe NPs as carriers to deliver these drugs can help overcome these limitations (Table 5).
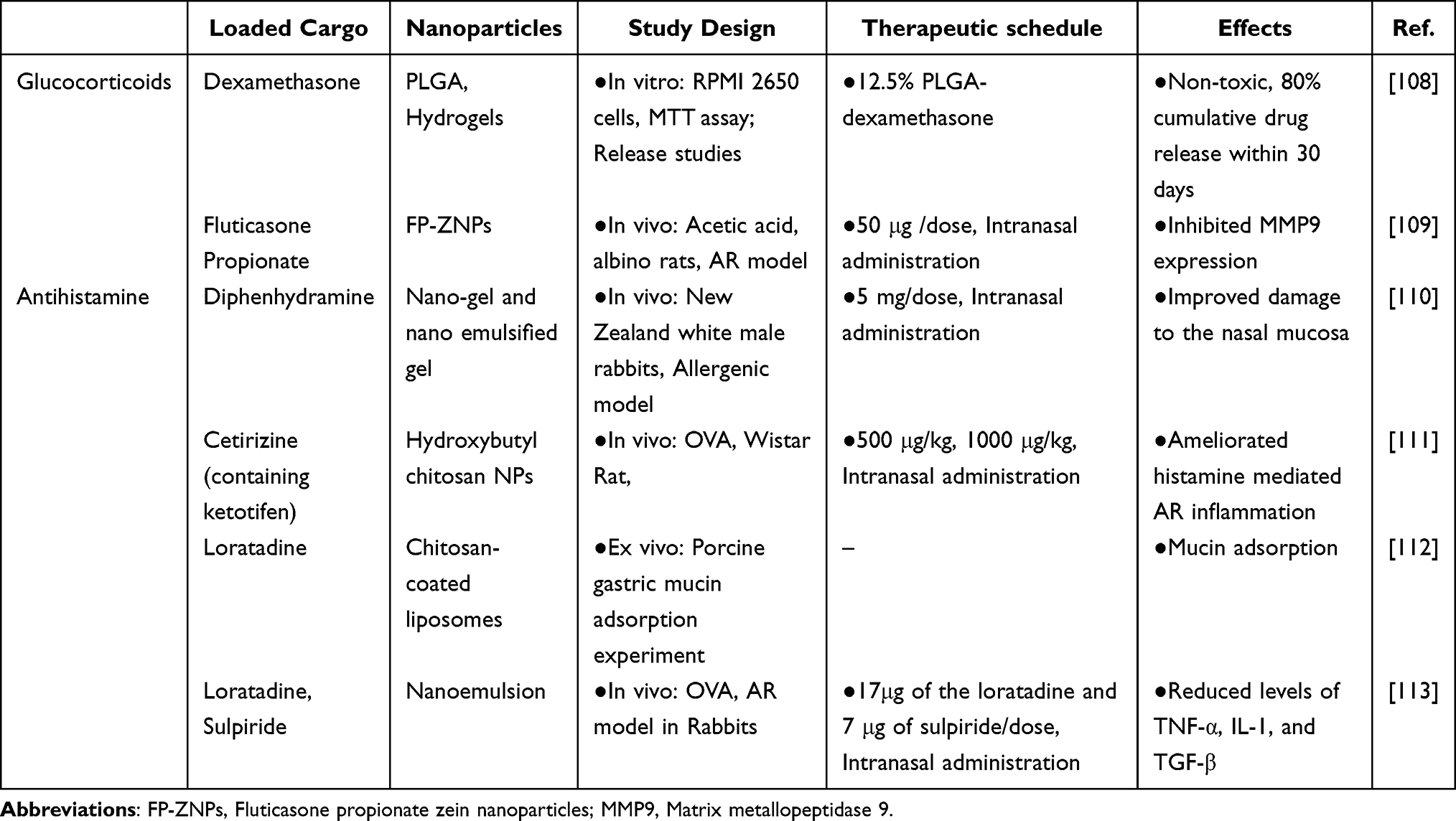 |
Table 5 Passive Targeted Delivery of Commonly Used Clinical Drug Delivery in AR |
Glucocorticoids
Glucocorticoids exert potent anti-inflammatory and immunomodulatory effects in AR. By binding to cytoplasmic glucocorticoid receptors, they inhibit NF-κB/AP-1 transcriptional activity and downregulate Th2 cytokines.114 One study demonstrated that dexamethasone (DEX) encapsulated in PLGA NPs and embedded in a chitosan/polyvinylpyrrolidone hydrogel exhibited no cytotoxicity toward RPMI-2650 nasal epithelial cells. This formulation enabled sustained DEX release, reaching a cumulative release of 80% within 30 days.108 El-Helaly et al prepared fluticasone propionate zein NPs (FP-ZNPs) via in situ gelation, with a zeta potential (ZP) of −32.6 ± 2.3 mV and an encapsulation efficiency (EE) of 98.8606 ± 0.0029%. These NPs enhanced the water solubility of fluticasone propionate, prolonged its residence time in the nasal cavity, improved intranasal absorption and healing rates, and showed superior performance in vitro release and permeability tests. In vivo experiments in an AR model demonstrated significant suppression of matrix metallopeptidase 9 (MMP9) levels.109
Antihistamines
Antihistamines can rapidly block H1 receptors, inhibit mast cell degranulation, and downregulate Th2-mediated inflammatory pathways to quickly relieve AR.115 Diphenhydramine hydrochloride (DPH), a first-generation antihistamine, exhibits strong sedative effects and may cause cardiac toxicity in overdose, leading to frequent clinical misuse.116 Javed’s team encapsulated DPH into a nasal nanogel and demonstrated that this nanodrug could rapidly penetrate the nasal mucosa, producing immediate therapeutic effects and alleviating histamine-induced symptoms in a New Zealand white rabbit AR model.110 Cetirizine (CTZ), a commonly used H1 antihistamine, has limited nasal application due to its hydrophobicity and mucosal irritation. A dual-antihistamine formulation incorporating ketotifen (KT) and cetirizine into chitosan NPs achieved the pH-responsive burst release of KT and lysozyme-mediated sustained release of CTZ. KT can inhibit histamine release by stabilizing mast cell membranes, while the combined KT–CTZ formulation specifically antagonized H1 receptors on epithelial cells, reducing nasal mucosal inflammation in AR rats.111 Liposomes coated with 0.05% and 0.1% chitosan showed loratadine release rates of 94±0.05% and 81±0.02%, respectively, over 24 hours, along with higher mucin adsorption.112 In another study, nanoemulsions co-loaded with loratadine and sulpiride, prepared using soybean lecithin and olive oil, showed small droplet size, low PDI, and optimal zeta potential, effectively downregulating TNF-α, TGF-β, and IL-1 expression. This significantly alleviated AR symptoms.113
Plant-Derived Extracts
Natural herbal medicines have become a current research focus due to their combined anti-inflammatory and anti-allergic properties, along with fewer side effects. However, their application is limited by enzymatic degradation and low bioavailability. NPs can effectively protect active components from degradation and improve solubility when loading natural herbal medicines. Through targeted delivery, they precisely deliver drug to nasal inflammation sites, enhancing local efficacy and reducing systemic exposure—offering a safer and more efficient strategy for AR treatment (Table 6).
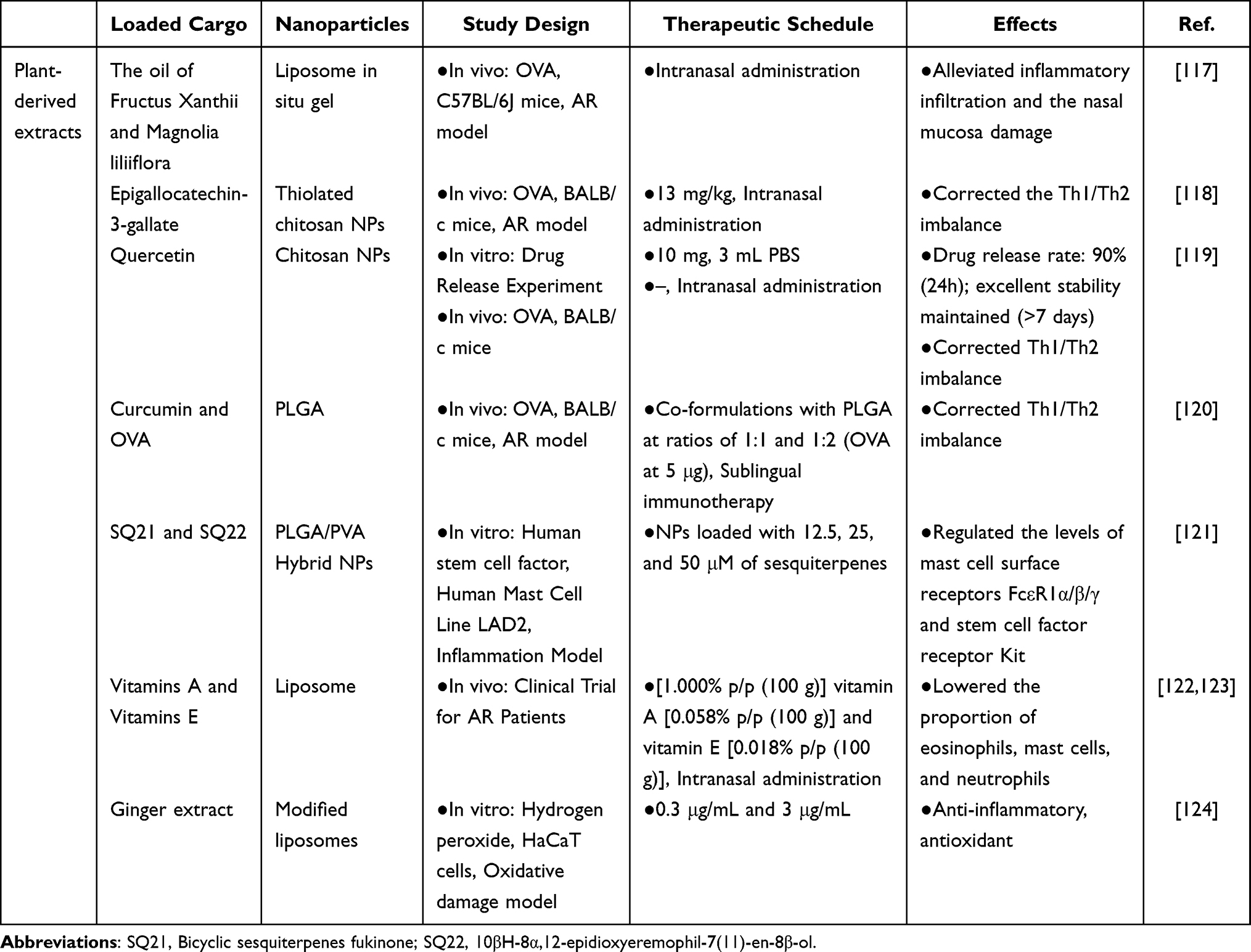 |
Table 6 Passive Targeted Delivery of Plant-Derived Extracts Delivery in AR |
Volatile Oils
Fructus xanthii is the fruit of Xanthium strumarium L., belonging to the Asteraceae family, and has been demonstrated to possess anti-inflammatory effects.125 Magnolia liliiflora belongs to the Magnolia family (Genus: Magnolia). Its flowers are an important medicinal ingredient.126 Using thin-film hydration technology, nano-liposomes containing volatile oils from Xanthium fruit and Magnolia liliiflora were prepared. A thermosensitive in-situ gel was obtained by incorporating Poloxamer as an excipient. This gel undergoes a solution-to-semi-solid transition at 34 °C and exhibits sustained-release properties. It effectively alleviated inflammatory infiltration and nasal mucosal damage in AR model mice.117
Polyphenols
Epigallocatechin gallate (EGCG), the main catechin in green tea, represents a major flavonoid polyphenol, accounting for about 50% of the total polyphenol content of green tea. It exhibits antioxidant, anti-inflammatory, cardioprotective, and antitumor properties.127 Zhang et al synthesized nanoscale polycyclodextrin (PCD) as a carrier to load EGCG, forming PCD@EGCG. Then combining thiolated chitosan (TCS) with it yielded TCS/PCD@EGCG, where the thiol groups in TCS formed disulfide bonds with cysteine residues in mucosal mucins, enhancing mucoadhesion and prolonging nasal retention time. In an AR mouse model, this system restored the Th1/Th2 balance, showing its promise as an excellent, long-lasting, and safe therapeutic agent for AR.118
Quercetin, a flavonoid polyphenol found in herbal plants such as Astragalus, mulberry bark, and ginkgo leaves, exerts antiallergic effects by improving Th1/Th2 balance.128 Loading quercetin onto chitosan NPs enhances its bioavailability by promoting dissolution. In an AR mouse model, quercetin-crosslinked chitosan NPs significantly suppresses allergic inflammation in AR mice, showing strong potential as a therapeutic candidate for AR.119
Curcumin is a polyphenolic compound and the primary active ingredient in Curcuma longa L., possesses potent antioxidant and anti-inflammatory properties,129 showing promise for AR treatment. Shahgordia et al encapsulated curcumin and OVA individually or together in PLGA could reduce IgE levels and increased the IFN-γ/IL-4 ratio in an AR mouse model. When combined with sublingual immunotherapy, curcumin–OVA co-loaded NPs further enhanced these regulatory effects, suggesting the potential to improve AR therapy.120
Sesquiterpenes
Bicyclic sesquiterpenes fukinone (SQ21) and 10βH-8α,12-epidioxyeremophil-7 (11)-en-8β-ol (SQ22), isolated from the rhizomes of Petasites tatewakianus (Asteraceae family) exhibit anti-inflammatory activity.130 Arizmendi’s team developed PLGA/PVA hybrid NPs to address the cytotoxicity and poor biocompatibility associated with sesquiterpene compounds, using them to deliver these two compounds. This nanodrug downregulated the expression of inflammatory receptors (FcεR1α/β/γ and Kit) on mast cell surfaces, effectively inhibiting tryptase secretion and degranulation. While maintaining cell viability and excellent biocompatibility, it regulated human mast cell phenotypic conversion and functional activation states.121
Meals
Vitamins A and E are fat-soluble vitamins closely linked to immune regulation. Vitamin A promotes the secretion of the anti-inflammatory factor IL-10 by regulating ILC2s, thereby suppressing Th2 immune responses, maintaining epithelial barrier function, and reducing IgE levels to inhibit allergic reactions in AR.131 The role of vitamin E in AR remains debated; however, evidence suggests that it can reduce IL-25, IL-33, Th2-type inflammatory mediators, and IgE levels in AR mice.132 Lauriello et al developed a vitamin A and E-loaded liposomal nasal spray that alleviated emotional distress symptoms in AR patients following intranasal administration.122 Further studies showed its ability to reduce eosinophil, mast cell, and neutrophil counts while relieving nasal congestion and other symptoms in AR patients.123
Ginger (Zingiber officinale Roscoe) is an herbaceous plant from the Zingiberaceae family, with its dried rhizome commonly used as medicine. Ginger extract is a multicomponent mixture containing various bioactive constituents, such as gingerol and zingerone. Studies show that it can alleviate AR symptoms but may occasionally cause drowsiness, fatigue, dizziness, and constipation.133 Casula et al developed a green nano-nasal spray by loading ginger extract into hyaluronic acid-modified phospholipid vesicles (modified liposomes) and enriching glycerol in the aqueous phase to form a multifunctional composite system. In vitro studies confirmed its excellent biocompatibility and strong antioxidant activity. Leveraging the combined advantages of liposomal mucosal barrier protection, hyaluronic acid moisturization and lubrication, and the anti-inflammatory and antioxidant effects of ginger extract, this formulation shows great potential for the prevention and treatment of rhinitis.124
Allergen
Allergens contain IgE epitopes that induce Type I allergic reactions.134 NPs offer several advantages, including allergen protection, enhanced immunomodulation, and targeted cellular delivery (Table 7). Therefore low-dose allergens such as Polcalcin (Che a 3) and OVA combined with NPs can improve AR symptoms. Sani’s team genetically fused the C. Che a 3 peptide with HBc VLPs. Compared with VLPs containing mixed antigens, this fusion induced stronger IgG production and shifted the immune response toward a Th1-dominant profile while suppressing Th2 immunity. This effect is attributed to the ability of VLPs to elicit humoral immune responses, efficiently enter lymph nodes, and inherently promote Th1-mediated immunity.64 Liu et al prepared sEVs loaded with CpG DNA and OVA (CpG–OVA–sEVs). Co-administration of CpG DNA with the allergen induced persistent allergen-specific immune tolerance maintained by immune memory. Studies demonstrated that intranasal delivery of CpG–OVA–sEVs to the nasopharyngeal-associated lymphoid tissue of AR model mice, where they were taken up by DCs and macrophages, corrected the Th1/Th2 immune imbalance.135
 |
Table 7 Passive Targeted Delivery of Allergen in AR |
Extracellular Vesicles
EVs derived from hypoxia-induced mesenchymal stem cells exhibit strong angiogenic and immunomodulatory properties.136 Wen et al developed an MXene-modified Gelatin Methacryloyl hydrogel (M-GelMA) as a sustained-release platform for intranasal delivery of hypoxia-induced MSC-EVs to treat AR. This hydrogel has a porous structure (swelling rate 140–180%) and excellent biocompatibility. In vitro, it significantly reduced IL-13-induced oxidative stress in nasal epithelial cells. In an AR mouse model, intranasal administration bypassed the first-pass effect and achieved prolonged nasal mucosal retention, ultimately restoring the Th1/Th2 immune balance. This formulation offers a novel therapeutic strategy for AR.137 Additionally, Xu et al found that MSC-sEVs upregulate claudin-1 expression, a tight junction protein in nasal epithelial cells, via the miR-143–GSK3B pathway, restoring nasal mucosal barrier integrity and alleviating AR.138 Yang et al showed that EVs derived from human adipose stem cells effectively reduce inflammatory infiltration in the nasal mucosa and restore the Th1/Th2 balance. They also observed that intranasal administration was more effective in mild rhinitis.139 Peng et al demonstrated that sEV-mDCs suppress Th2 immune responses by reducing IL-4, IL-9, and IL-13 production via secreting IL-10.140
Zhao et al developed an injectable thermosensitive chitosan hydrogel based on bone marrow-derived MSC-EVs (BMSC-EVs). This hydrogel undergoes a sol–gel transition at the nasal physiological temperature (34°C), allowing tight adhesion to the nasal mucosa and local retention of BMSC-EVs. In vitro experiments showed that it inhibited OVA-induced dendritic cell maturation and CCL21-mediated chemotaxis, blocking allergic response initiation. In vivo, this delivery system significantly alleviated AR symptoms and effectively restored immune balance by downregulating Th2/Th17-related factors while upregulating Th1/Treg-related factors.141
Using mechanical double emulsification, MSC-derived exosomes were encapsulated within PLGA NPs, significantly prolonging the nasal mucosal retention and preventing rapid clearance. In an OVA-induced AR mouse model, this nanoparticle formulation achieved passive targeting via intranasal delivery. Multi-omics analysis suggested that it remodels the immune microenvironment through IL-17/Th17, PPARγ, and glycolytic pathways, restoring Th1/Th2 balance, thereby markedly alleviating nasal inflammatory symptoms.142 (Illustrated in Table 8).
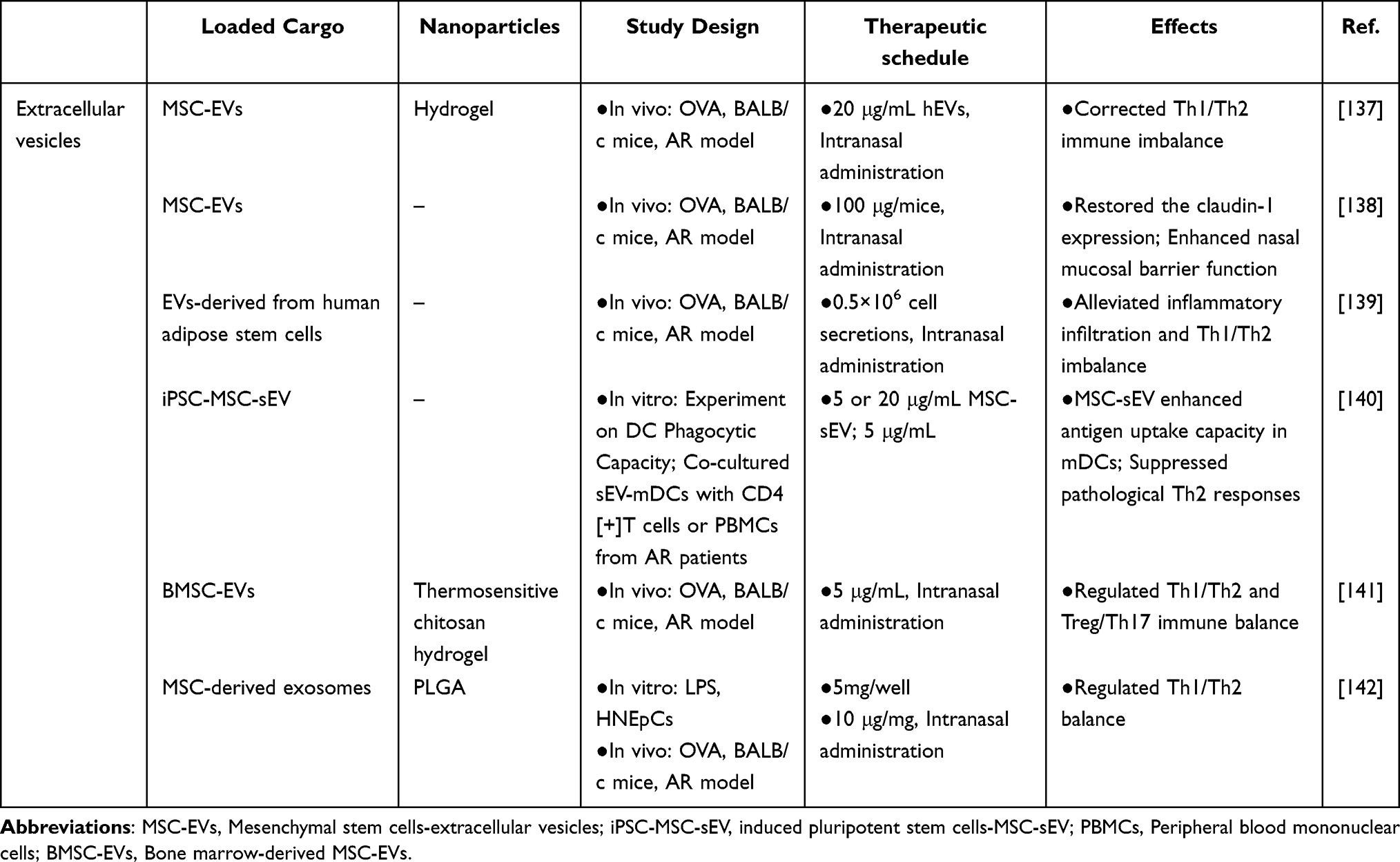 |
Table 8 Passive Targeted Delivery of Extracellular Vesicles in AR |
Gene
miR-146a-5p modulates the immune response in AR by suppressing ILC2 activation and Th2 cells differentiation via targeting molecules such as SERPINB2, IRAK6, and TRAF2.143 However, exposed nucleic acids generally struggle to penetrate extracellular barriers. Fang et al established an ILC2-dominant eosinophilic airway inflammation model and prepared MSC-sEVs, reduced ILC2 numbers, inflammatory cell infiltration in lung tissue, and mucus production, while alleviating IL-5 and IL-13 levels and airway hyperresponsiveness. They revealed that MSC-sEVs could reverse IL-5 and IL-13 levels from ILC2s in a dose-dependent manner. They also found delivery of miR-146a-5p enhanced the therapeutic efficacy of MSC-sEVs on ILC2s.58 As discussed previously, miR-146a-5p can target SERPINB2, IRAK6, and TRAF2 to inhibit ILC2 activation and Th2 cell differentiation. Additionally, studies indicate that miR-146a-5p can regulate cell proliferation and apoptosis by targeting Smad3.144 Li et al validated that miR-146a-5p directly binds the Smad3 3’UTR site, leading to a subsequent reduction in the Smad3/GATA-3 complex. Co-incubation of miR-146a-5p-containing EVs (EC-EVs miR-146a-5p) derived from NECs with CD4+ T cells promoted Th1 differentiation and suppressed Th2 responses, confirming that EC-EVs miR-146a-5p alleviates AR symptoms by modulating the Smad3/GATA-3 pathway. Furthermore, co-treatment with ephedrine polysaccharide Ephedra sinica polysaccharide B4 (ESP-B4) was found to enhance this effect.145
miRNA-146a is a non-coding single-stranded RNA that regulates the immune system and suppresses allergic inflammation. Considering the unique pH (5.5–7.8) and temperature (32–35°C) of the nasal cavity, Yu Su’s team designed a thermosensitive chitosan-based hydrogel that remains liquid at room temperature and prolongs drug retention in the nasal mucosa. By incorporating PEG-PLA, this system enables the intranasal delivery of miRNA-146a with sustained mucosal release. In vivo experiments showed that it inhibits the TLR4/NF-κB signaling pathway and reduces expression levels of IL-4, histamine, and other mediators.101 (Illustrated in Table 9).
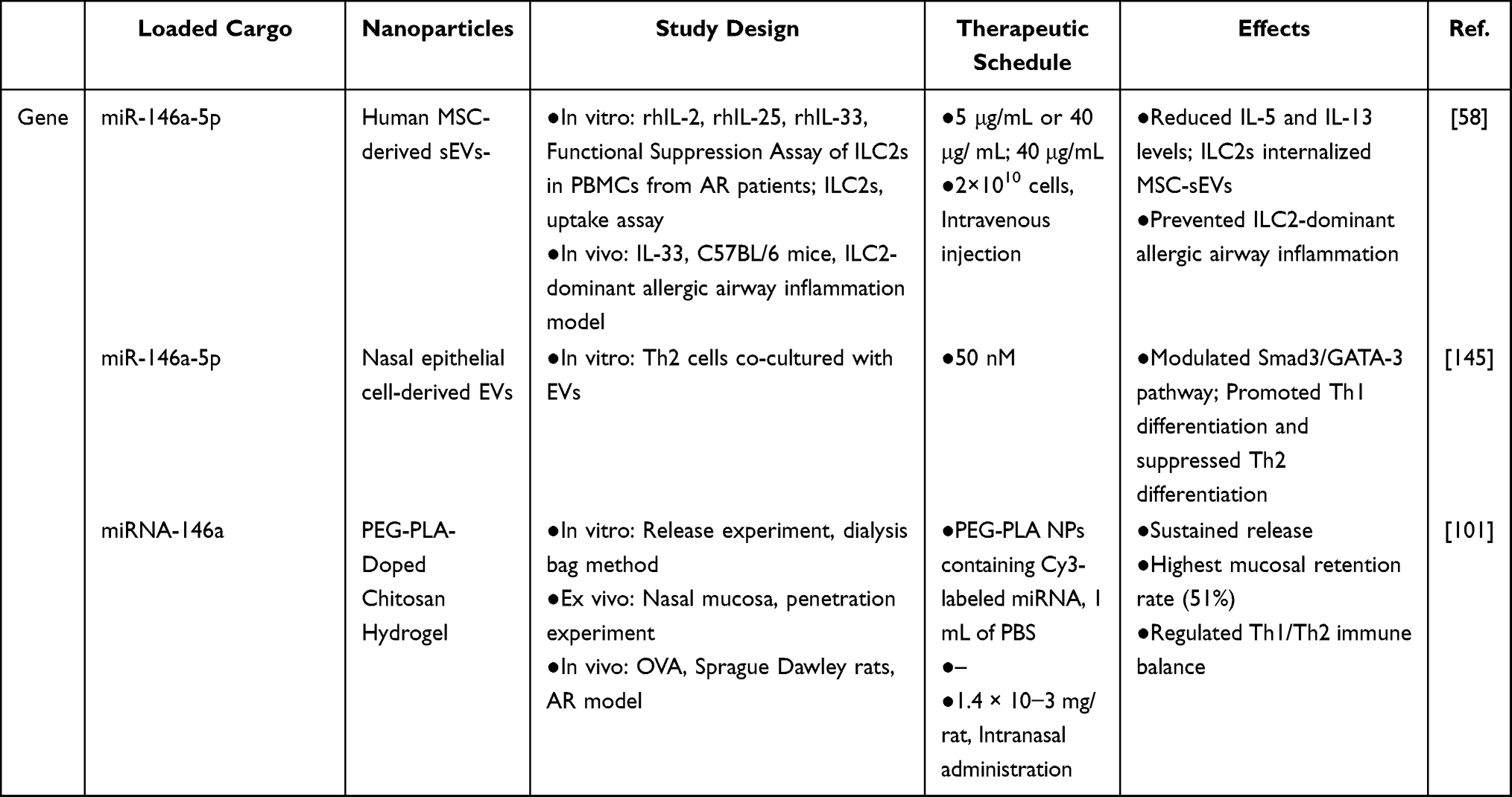 |
Table 9 Passive Targeted Delivery of Gene in AR |
Others
Monascin, a secondary metabolite derived from red yeast rice, exhibits potent anti-inflammatory, hypolipidemic, and antioxidant properties.146 Wang et al encapsulated monascin within PLGA (PLGA-MS) using mechanical techniques. In vitro and in vivo studies have demonstrated that PLGA-MS enhances drug stability and enables sustained release, reduces inflammatory cell infiltration in nasal tissue, and modulates cytokines such as IgE and histamine. Network pharmacology predicted potential signaling pathways involved, including NF-κB, neuroactive ligand–receptor interaction, TNF, and IL-17 pathways.147
Active Targeting Delivery
By introducing specific functional groups or bioactive molecules—such as receptor ligands for immune cells or targeting moieties on inflammatory cell surfaces—NPs can achieve enhanced affinity and targeting capability,148 enabling more effective interaction with nasal tissues (Figure 4). Utilizing NPs to actively target specific cells within nasal tissues offers the potential for more precise drug delivery and treatment, improving therapeutic efficacy, reducing systemic side effects, and providing new opportunities for breakthroughs and innovation in AR therapy (Supplementary Table 3).
Targeting of DCs
DCs are the primary antigen-presenting cells in the nasal mucosa. They recognize allergens, process them into antigenic peptides, and present these via MHC molecules to T cells. This process activates Th2-type immune responses, leading to excessive IgE antibody production and eosinophil infiltration.149 NGR is a disulfide-constrained cyclic peptide that specifically recognizes and binds to the CD13 marker on DCs. Liu et al developed PEG-PLGA micelles modified with NGR peptides. This system achieved active targeting of DCs with shikonin (SHI) through NGR–CD13-specific binding, effectively inhibiting DC maturation and NF-κB signaling pathway activation while regulating the Th1/Th2 immune balance. Experimental results showed that this delivery system enhanced the anti-inflammatory effects of SHI.150 Similarly, Zheng et al developed a polymeric micelle modified with NGR, and loaded with xanthatin (XT), enhancing XT’s water solubility and DC targeting. By specifically delivering XT to DCs and modulating the COX-2/PGE2 pathway, this approach effectively suppressed DC maturation and inflammatory responses, corrected Th1/Th2 imbalance, and achieved efficient treatment of refractory AR with a lower recurrence rate than the clinical drug budesonide.151 Research has shown that P-D2 can bind CD11c on the DC surface.152 Liu et al prepared P-D2 peptide-modified EVs (P-D2-EVs) derived from human umbilical cord MSCs. Compared to unmodified MSC-EVs, P-D2-EVs increased DC targeting from 22% to 52.1%. The study concluded that P-D2-EVs can alleviate AR symptoms by inhibiting the Fut1/ICAM1/P38MAPK signaling pathway, enhancing IL-10 expression in DCs, suppressing Th2 cell differentiation, and inhibiting ILC2 activation.153
DC-specific aptamers can specifically recognize and bind to molecules of specific receptors on the surface of DCs. AuNPs loaded with Platanus orientalis pollen extract and modified with DC-specific aptamers were employed for epidermal immunotherapy (EPIT) in AR. These NPs efficiently delivered Platanus orientalis pollen extract to DCs. Experiments demonstrated that a dose as low as 10 μg enhanced allergen delivery efficiency. This treatment achieved anti-inflammatory effects comparable to those in normal mice by reducing Th2-type immune responses and promoting Th1-type immune responses.154 Another study employed PLGA NPs modified with DC-specific aptamers for the targeted sublingual delivery of OVA. By recognizing receptors on oral mucosal Langerhans-like DCs, the system enhanced DC uptake, processing, and antigen presentation. This effectively modulated immune responses, enhanced immune tolerance, and alleviated AR symptoms in mice.155 A DC-specific aptamer (Apt)-modified MSC-derived exosomes (Apt-Exo) was also developed for sublingual delivery of OVA. Sadeghi et al addressed the high allergen dose required in conventional SLIT by using only Apt-Exo containing 5 μg OVA, improving allergic inflammation in OVA-allergic mice.156 The Koushki team developed a DC-targeted AuNP that enhanced stratum corneum penetration by incorporating transdermal peptide 1/polyarginine-7 skin-penetrating peptides (SPPs) while achieving precise targeting and enrichment of DCs in the skin and draining lymph nodes through DC-specific aptamers, thereby promoting allergen rChe a 2 uptake. Experimental results showed that even at a reduced rChe a 2 dose of 5 µg, this nanosystem significantly suppressed IgE production and eosinophil infiltration.157 In a subsequent study, the Koushki team applied the same DC-targeted AuNP for sublingual OVA delivery. This nanodrug effectively targeted oral mucosal DCs, alleviating OVA-induced AR and airway inflammation.158 These studies present an innovative, safe, and effective therapeutic strategy for SCIT and SLIT.
Haghnavaz et al synthesized OVA-loaded PLGA NPs via an emulsion–solvent evaporation method and modified them with D-mannose. Mannose targeted the mannose receptor (CD206) on DCs, significantly enhancing antigen uptake and presentation efficiency while reducing inflammation in AR mice even at a reduced OVA dose of 5 µg, showing superior immunomodulatory potential compared to conventional SLIT.159 (Illustrated in Table 10).
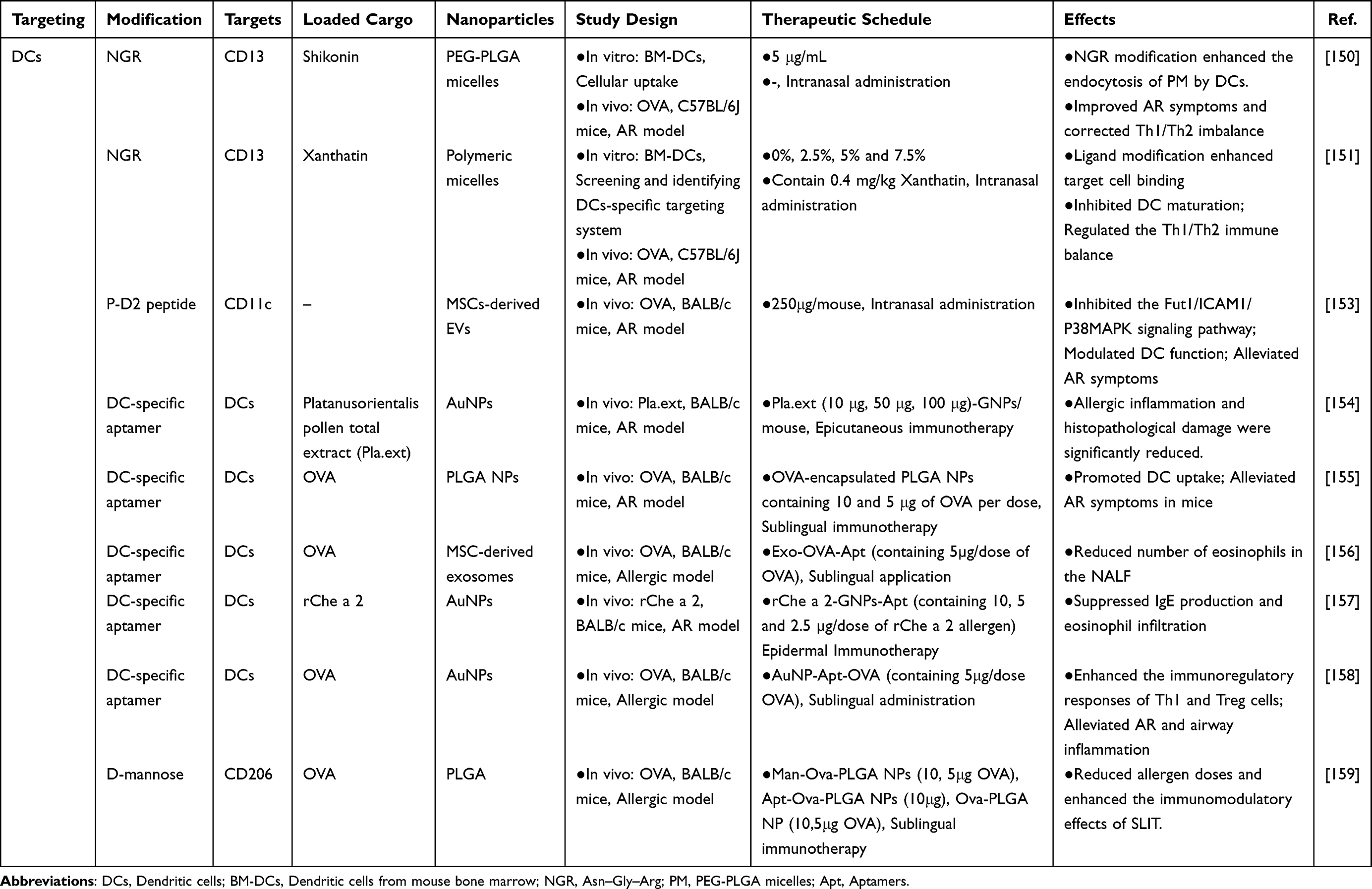 |
Table 10 Nanodrug Active Targeting of Dendritic Cells in AR |
Targeting of Mast Cells
Mast cells are the key effector cells in the early phase of allergic reactions. When the surface IgE receptor is activated, allergen cross-linking of FcεRI triggers a signaling cascade that ultimately leads to degranulation.160 Mast cells also overexpress CD300f, with ceramide serving as its ligand. Binding of ceramide to CD300f inhibits IgE-mediated mast cell activation and allergic reactions in mouse models.161
Ide et al developed ceramide-based liposomes using ceramide or phosphatidylserine as lipid materials. These liposomes bind to the CD300f receptor on mast cell surfaces, thereby inhibiting FcεRI-mediated mast cell degranulation and reducing the release of mediators such as histamine.162 Additionally, Shen et al developed a biodegradable diselenide-bridged mesoporous silica NP (SeMSNs) and modified it with an IgE aptamer (Ap) to deliver sodium cromoglycate (CS), ultimately forming SeMSNs@CS@Ap. The surface-modified Ap on these NPs specifically recognizes and binds to IgE antibodies on sensitized mast cell surfaces, preventing re-exposure to allergens. Meanwhile, the diselenide scaffold is degraded by ROS within mast cells, consuming excess ROS to restore redox homeostasis. This facilitates CS delivery to stabilize mast cell membranes, achieving therapeutic effects against AR. In vivo testing in AR mice demonstrated that SeMSNs@CS@Ap reduced eosinophil infiltration in nasal tissues and alleviated AR symptoms such as nasal itching and sneezing. Combined with passive skin allergy experiments, this nanoparticle showed superior therapeutic efficacy for AR intervention with minimal side effects.163 (Illustrated in Table 11).
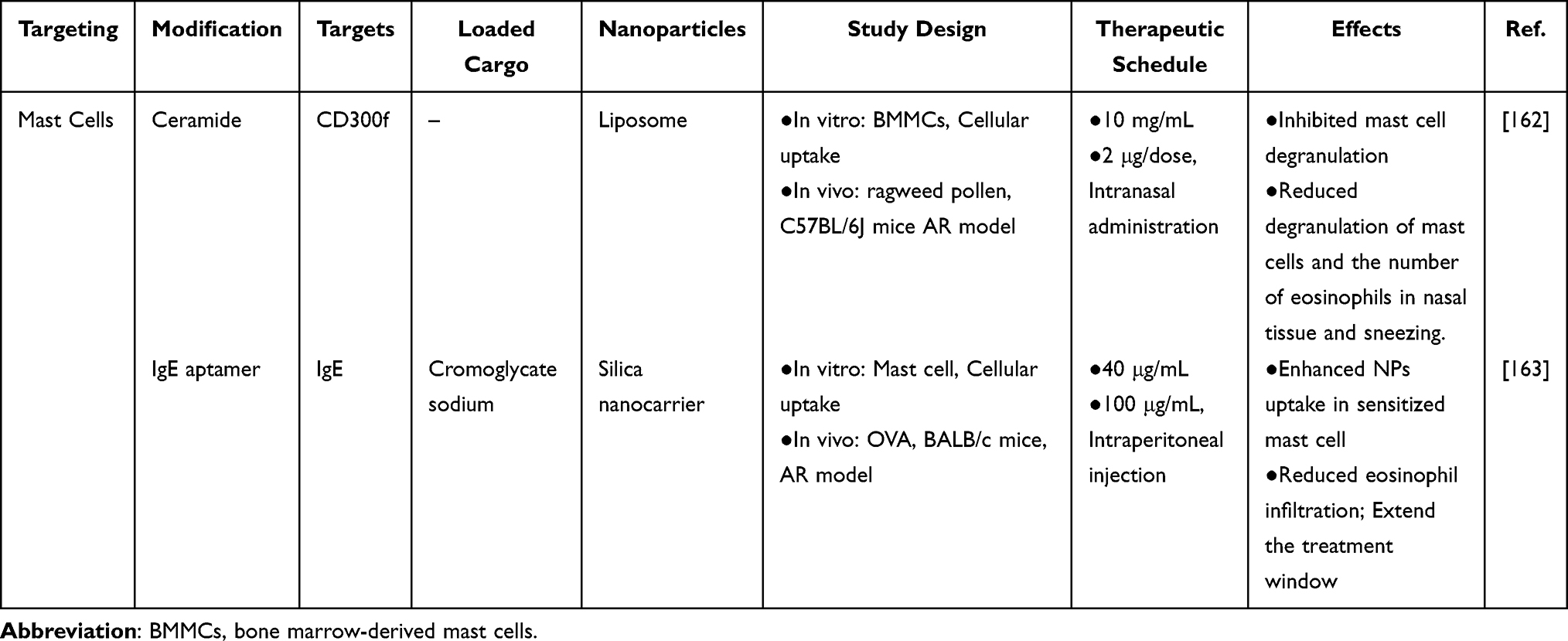 |
Table 11 Nanodrug Active Targeting of Mast Cells in AR |
Targeting of Eosinophils
Eosinophils are key immune cells in the pathogenesis of AR. Eosinophils with high CCR3 expression are induced by the chemokine CCL11 to infiltrate the nasal cavity, exacerbating the nasal inflammation.164 Based on these overexpressed proteins, targeting molecules were designed on the nanoparticle surface. Using the polymer PVA as the backbone, CCR3 antagonist peptides were chemically grafted along with pH-cleavable hydrophilic terminals (mPEG2000-Hyd-SH), while the antihistamine ketotifen fumarate was physically encapsulated, forming a self-assembling nanodrug. Under nasal acidic conditions, it undergoes fibrillation, enhancing CCR3-ligand binding blockade and prolonging its nasal retention time to 24 hours. This achieves sustained inhibition of mast cell degranulation and eosinophil chemotaxis.165
Targeting of T Cells
Tregs possess immunoregulatory properties, capable of suppressing Th2 cell activation. They can also directly act on mast cells, basophils, and eosinophils to inhibit allergic inflammation.166 Mo et al synthesized dendritic cell-derived EVs loaded with OVA, MHC-II, and tetramethylcurcumin (FLLL31), termed OFexo. The OVA/MHC-II complexes on their surface specifically recognize T cell receptors (TCRs), activate IL-10 secretion, and suppress Th2-type immune responses. Simultaneously, leveraging the immunomodulatory effects of FLLL31, they synergistically induce immunoregulatory cells and demonstrate excellent efficacy in suppressing allergic reactions.167
Challenges and Future Perspectives
Although nanodrugs offer new opportunities for treating AR, research on their application remains insufficient. First, we identified 8 common types of NPs, with current research hotspots including EVs, liposomes, chitosan, and PLGA (Figure 1), indicating significant room for innovation in materials. Furthermore, since the core target cells of AR (mast cells, eosinophils, DCs, etc) are dispersed within the submucosal layer of the nasal mucosa, existing NPs primarily rely on passive targeting with limited active targeting capabilities.111 Future research should enhance the understanding of AR immune microenvironment and develop patient-specific NPs tailored to inflammatory endotypes or genetic profiles for more personalized therapy. For instance, researchers could inhibit eosinophil degranulation or construct ligand-modified NPs targeting Siglec-8—a receptor co-expressed on eosinophils, basophils, and mast cells that can induce cell death. Furthermore, STAP-2 has been demonstrated to positively regulate FcεR-mediated basophil activation, positioning it as a promising novel therapeutic target for AR.168 Secondly, current NPs in AR primarily load allergens and/or immunomodulators. Future development may explore combined strategies that simultaneously load allergens, immunomodulators, and barrier repair agents (tight junction proteins), potentially achieving synergistic treatment for immune tolerance, inflammation suppression, and epithelial barrier repair. Additionally, smart NPs have emerged as a promising alternative to conventional NPs in disease treatment. Developing sensing/release feedback systems—such as pH-sensitive or temperature-sensitive carriers—allows for targeted drug release under the specific temperature and pH conditions of the nasal cavity, particularly within the inflammatory microenvironments.169
Nanodrugs are primarily delivered via intranasal, subcutaneous, and sublingual administration in AR treatment to achieve local or systemic immune modulation. Among these, intranasal administration is the primary route, delivering drugs directly to the affected nasal mucosa. It offers advantages such as bypassing the first-pass effect, enhancing local drug concentration, and modulating the nasal immune imbalance, thereby rapidly controlling nasal symptoms. However, its efficacy is often limited by the nasal mucociliary clearance mechanism. Therefore, to enhance the binding and penetration capacity of nanodrugs in the nasal mucosa, carrier designs often employ strategies such as surface positive charges, particle sizes below 150 nm, and thiolated polymer modifications.104 Subcutaneous and sublingual administration are primarily used for delivering allergens to establish immune tolerance in the body. For clinical selection, SCIT or SLIT is recommended for pollen allergens, while SLIT is generally preferred for dust mite allergies.170
Different routes of administration influence the absorption and distribution processes of NPs within the body. During intranasal administration, some NPs may enter the central nervous system via the nose-brain pathway and be taken up by neural cells, others remain in the nasal cavity and are taken up by nasal cells, and still others are rapidly degraded by nasal mucus and enzymes. Only a small fraction enters systemic circulation, where they undergo enzymatic degradation into biocompatible metabolites and are ultimately excreted by the kidneys.171 Subcutaneous administration primarily directs NPs into the lymphatic or systemic circulation, while sublingual delivery sends them directly into the systemic circulation. Both ultimately undergo metabolic degradation via enzymatic pathways.172 Notably, inorganic NPs exhibit poor biodegradability and tend to accumulate long-term in the body, potentially triggering toxic reactions—inducing cellular oxidative stress and membrane damage. Their toxicity typically increases with decreasing particle size.173 Furthermore, the environmental safety concerns they pose remain significant. Studies indicate that conventional synthesis methods for inorganic NPs often rely on toxic chemical reducing agents like sodium borohydride and citrate, as well as volatile organic solvents, posing hazards to the environment and living organisms. Therefore, NPs synthesized using bacteria, fungi, yeast, algae, and plants can eliminate the toxicity associated with traditional synthesis pathways, gradually emerging as alternative solutions to conventional methods. However, the potential for cellular toxicity remains unavoidable, necessitating comprehensive toxicological evaluation.174 Furthermore, most targeted nanodrugs for AR remain in preclinical stages. Nanodrug concentrations have been optimized to achieve desired therapeutic effects. The extent of bioaccumulation from long-term repeated administration remains unclear.175 Liposomes, synthetic polymers, and inorganic NPs exhibit low immunogenicity, which hinders their ability to effectively induce adaptive immune responses and generate corresponding antibodies. This limitation can lead to the activation and exacerbation of Type I allergic reactions.176 Simultaneously, the large-scale production and stable quality control of NPs constitute major bottlenecks in the industrialization process. Collectively, these factors present multiple obstacles to the clinical translation of nanodrugs.
In summary, nanodrugs are gaining increasing attention. Future research should focus on: determining and optimizing the particle size, surface chemistry, and targeted ligand modification of carriers; achieving personalized nanodrug and multifunctional drug combination therapies; verifying material biocompatibility; minimizing nanoparticle toxicity; and advancing nanodrugs from laboratory to clinical settings. This will provide more effective and safer treatment options for AR.
Conclusions
The ideal delivery system precisely transports drugs to the lesion site while allowing the carrier to degrade and metabolize under normal physiological conditions without accumulation. In most current studies, factors such as the first-pass effect, low bioavailability, and insufficient targeting limit drug application, suggesting that AR may benefit from nanodrugs. This review summarizes recent advances in nanodrugs for targeting treatment of AR. First, it outlines the types and characteristics of organic NPs, inorganic NPs, and hydrogel NPs, and then their potential applications in AR treatment. All NPs possess the capacity to load and transport drugs. Consequently, we also summarize nanodrug delivery strategies targeting AR, encompassing both active and passive targeting approaches. These nanodrugs exert anti-inflammatory effects by inhibiting inflammation, regulating immune balance to mitigate AR. In addition, certain nanodrugs provide supplementary therapeutic benefits by restoring tight junctions in nasal epithelial cells. Finally, the review discusses key challenges in translating nanodrugs from laboratory research to clinical practice, such as the large-scale production of nanocarriers, controlled release and targeting efficiency, and clinical safety assessment. Then this paper proposes potential solutions and outlines future research directions. These discussions provide valuable insights for the clinical application of nanodrugs in AR treatment and contribute to advancing precision medicine.
Abbreviations
AR, Allergic rhinitis; Ag NPs, Silver nanoparticles; AIT, Allergen immunotherapy; AlNPs, Aluminum oxide nanoparticles; APCs, Antigen-presenting cells; AD-MSCs, Adipose tissue–derived MSCs; BCG-PSN, Bacillus Calmette-Guerin polysaccharide nucleic acid; BMSC-EVs, Bone marrow-derived MSC-EVs; CpG, Cytosinephosphate-guanine motifs; CTZ, Cetirizine; DCs, Dendritic cells; DPH, Diphenhydramine hydrochloride; EGCG, Epigallocatechin gallate; EPO, Eosinophil peroxidase; ERK, Extracellular regulated protein kinases; ESP-B4, Ephedra sinica polysaccharide B4; EVs, Extracellular vesicles; FcεR, Fc epsilon receptor; FP-ZNPs, Fluticasone propionate zein nanoparticles; hADSC-EVs, Human adipose-derived stem cells; HDM, House dust mites; IgE, Immunoglobulin E; IgG-sIgE, IgG-specific IgE; IL-13, Interleukin-13; IL-25, Interleukin-25; IL-33, Interleukin-33; IL-4, Interleukin-4; IL-5, Interleukin-5; ILC2s, Group 2 innate lymphoid cells; INCS, Intranasal corticosteroids; KT, Ketotifen; LPS, Lipopolysaccharide; LPs, Liposomes; MHC-II, Major histocompatibility complex class II; MMP9, Matrix metallopeptidase 9; M-GelMA, MXene-modified Gelatin Methacryloyl; MBP, Major basic protein; MR, CD206, Mannose receptor; mRNA, Messenger RNA; MSCs, Mesenchymal stem cells; NALF, Nasal lavage fluid; NECs, Epithelial cells; NF-κB, Nuclear factor kappa-B; NMs, Nanomicelles; NPs, Nanoparticles; OVA, Ovalbumin; OVA-sIgE, OVA-specific IgE; PCD, Polycyclodextrin; PEG, Polyethylene glycol; PCL, Polycaprolactone; PLA, Polylactic acid; PLGA, Poly(lactic-co-glycolic acid); PMAA, Poly(methacrylate); PPAR-γ, Peroxisome proliferator-activated receptor; SCIT, Subcutaneous immunotherapy; sIgE, specific IgE; sEVs, Small extracellular vesicles; siRNA, Small interfering RNA; SLIT, Sublingual immunotherapy; SNPs, Silica nanoparticles; SQ21, Bicyclic sesquiterpenes fukinone; SPPs, Skin-penetrating peptides; SQ22, 10βH-8α,12-epidioxyeremophil-7(11)-en-8β-ol; SHI, Shikonin; TCS, Thiolated chitosan; Th1, T helper 1; Th2, T helper 2; Th17, T helper 17; Treg, Regulatory T; TSLP, Thymic stromal lymphopoietin; VLPs, Virus-like particles; XT, xanthatin; ZO-1, Zonula Occludens-1; ZP, Zeta potential.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work is supported by National Natural Science Foundation of China (82060883, 82360953); Yunnan Provincial Science and Technology Plan Project (Key Project of Traditional Chinese Medicine Joint Project, 202101AZ070001-162); Science and Technology Projects of Yunnan Universities Serving Key Industries (FWCY-BSPY2025089); Scientific Research Fund Project of Yunnan Provincial Department of Education (2025Y0613); Yunnan University of Chinese Medicine School of Basic Medical Sciences Institutional (2023CBMS014) and 2025 “Jiebangguashuai” Graduate Student Innovation Capacity Enhancement Project (A3-0317-25-429-005).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bousquet J, Anto JM, Bachert C, et al. Allergic rhinitis. Nat Rev Dis Primers. 2020;6(1):95. doi:10.1038/s41572-020-00227-0
2. Bernstein JA, Bernstein JS, Makol R, Ward S. Allergic rhinitis: a review. JAMA. 2024;331(10):866–32. doi:10.1001/jama.2024.0530
3. García-Marcos L, Asher MI, Pearce N, et al. The burden of asthma, hay fever and eczema in children in 25 countries: GAN Phase I study. Eur Respir J. 2022;60(3):2102866. doi:10.1183/13993003.02866-2021
4. Lindqvist M, Leth‐Møller KB, Linneberg A, et al. Natural course of pollen-induced allergic rhinitis from childhood to adulthood: a 20-year follow up. Allergy. 2024;79(4):884–893. doi:10.1111/all.15927
5. Rodrigues J, Franco-Pego F, Sousa-Pinto B, Bousquet J, Raemdonck K, Vaz R. Anxiety and depression risk in patients with allergic rhinitis: a systematic review and meta-analysis. Rhinology. 2021;59(4):360–373. doi:10.4193/Rhin21.087
6. Høj S, Nielsen FK, Chawes B, et al. Allergic rhinitis is associated with increased suicidality: a systematic review and meta-analysis. Clin Rev Allergy Immunol. 2025;68(1):52. doi:10.1007/s12016-025-09061-2
7. Avdeeva KS, Reitsma S, Fokkens WJ. Direct and indirect costs of allergic and non-allergic rhinitis in the Netherlands. Allergy. 2020;75(11):2993–2996. doi:10.1111/all.14457
8. Voelker R. What is allergic rhinitis? JAMA. 2024;332(19):1682. doi:10.1001/jama.2024.14237
9. Dykewicz MS, Wallace DV, Amrol DJ, et al. Rhinitis 2020: a practice parameter update. J Allergy Clin Immunol. 2020;146(4):721–767. doi:10.1016/j.jaci.2020.07.007
10. Penagos M, Durham SR. Allergen immunotherapy for long-term tolerance and prevention. J Allergy Clin Immunol. 2022;149(3):802–811. doi:10.1016/j.jaci.2022.01.007
11. De Filippo M, Votto M, Caminiti L, et al. Safety of allergen-specific immunotherapy in children. Pediatr Allergy Immunol. 2022;33(Suppl S27):27–30. doi:10.1111/pai.13622
12. Zhang P, Bian S, Wang X, et al. A real-world retrospective study of safety, efficacy, compliance and cost of combination treatment with rush immunotherapy plus one dose of pretreatment anti-IgE in Chinese children with respiratory allergies. Front Immunol. 2022;13:1024319. doi:10.3389/fimmu.2022.1024319
13. Bian S, Zhang P, Li L, et al. Anaphylaxis associated with allergen specific immunotherapy, omalizumab, and dupilumab: a real world study based on the US food and drug administration adverse event reporting system. Front Pharmacol. 2021;12:767999. doi:10.3389/fphar.2021.767999
14. Yusuf A, Almotairy ARZ, Henidi H, Alshehri OY, Aldughaim MS. Nanoparticles as drug delivery systems: a review of the implication of nanoparticles’ physicochemical properties on responses in biological systems. Polymers. 2023;15(7):1596. doi:10.3390/polym15071596
15. Qiu S, Zhu F, Tong L. Application of targeted drug delivery by cell membrane-based biomimetic nanoparticles for inflammatory diseases and cancers. Eur J Med Res. 2024;29(1):523. doi:10.1186/s40001-024-02124-8
16. Shang S, Li X, Wang H, et al. Targeted therapy of kidney disease with nanoparticle drug delivery materials. Bioact Mater. 2024;37:206–221. doi:10.1016/j.bioactmat.2024.03.014
17. Liu T, Zhang R, Jiang L, et al. The potential application and molecular mechanisms of natural products in the treatment of allergic rhinitis: a review. Phytomedicine. 2024;129:155663. doi:10.1016/j.phymed.2024.155663
18. Nur Husna SM, Tan H-TT, Md Shukri N, Mohd Ashari NS, Wong KK. Allergic rhinitis: a clinical and pathophysiological overview. Front Med. 2022;9:874114. doi:10.3389/fmed.2022.874114
19. Hellings PW, Steelant B. Epithelial barriers in allergy and asthma. J Allergy Clin Immunol. 2020;145(6):1499–1509. doi:10.1016/j.jaci.2020.04.010
20. Yuan J, Liao Z, Zhu X, et al. PM2.5 exacerbates nasal epithelial barrier dysfunction in allergic rhinitis by inducing NLRP3-mediated pyroptosis via the AhR/CYP1A1/ROS axis. J Hazard Mater. 2025;492:138145. doi:10.1016/j.jhazmat.2025.138145
21. Ouyang X, Reihill JA, Douglas LEJ, Martin SL. Airborne indoor allergen serine proteases and their contribution to sensitisation and activation of innate immunity in allergic airway disease. Euro Respirator Rev. 2024;33(172):230126. doi:10.1183/16000617.0126-2023
22. Siti Sarah CO, Md Shukri N, Mohd Ashari NS, Wong KK. Zonula occludens and nasal epithelial barrier integrity in allergic rhinitis. PeerJ. 2020;8:e9834. doi:10.7717/peerj.9834
23. Ronchese F, Webb GR, Ochiai S, Lamiable O, Brewerton M. How type-2 dendritic cells induce Th2 differentiation: instruction, repression, or fostering T cell-T cell communication? Allergy. 2025;80(2):395–407. doi:10.1111/all.16337
24. Molofsky AB, Locksley RM. The ins and outs of innate and adaptive type 2 immunity. Immunity. 2023;56(4):704–722. doi:10.1016/j.immuni.2023.03.014
25. Liva GA, Karatzanis AD, Prokopakis EP. Review of rhinitis: classification, types, pathophysiology. J Clin Med. 2021;10(14):3183. doi:10.3390/jcm10143183
26. Zoabi Y, Levi-Schaffer F, Eliashar R. Allergic rhinitis: pathophysiology and treatment focusing on mast cells. Biomedicines. 2022;10(10):10. doi:10.3390/biomedicines10102486
27. Gelardi M, Giancaspro R, Cassano M, Ribatti D. The underestimated role of mast cells in the pathogenesis of rhinopathies. Int Arch Allergy Immunol. 2022;183(2):153–159. doi:10.1159/000518924
28. Drazdauskaitė G, Layhadi JA, Shamji MH. Mechanisms of allergen immunotherapy in allergic rhinitis. Curr Allergy Asthma Rep. 2021;21(1):2. doi:10.1007/s11882-020-00977-7
29. Zhou Y, Xu Z, Liu Z. Role of IL-33-ST2 pathway in regulating inflammation: current evidence and future perspectives. J Transl Med. 2023;21(1):902. doi:10.1186/s12967-023-04782-4
30. Thompson-Souza GA, Gropillo I, Neves JS. Cysteinyl leukotrienes in eosinophil biology: functional roles and therapeutic perspectives in eosinophilic disorders. Front Med. 2017;4:106. doi:10.3389/fmed.2017.00106
31. Ogulur I, Mitamura Y, Yazici D, et al. Type 2 immunity in allergic diseases. Cell Mol Immunol. 2025;22(3):211–242. doi:10.1038/s41423-025-01261-2
32. Steelant B, Seys SF, Van Gerven L, et al. Histamine and T helper cytokine–driven epithelial barrier dysfunction in allergic rhinitis. J Allergy Clin Immunol. 2018;141(3):951–963.e8. doi:10.1016/j.jaci.2017.08.039
33. Liu R, Luo C, Pang Z, et al. Advances of nanoparticles as drug delivery systems for disease diagnosis and treatment. Chin Chem Lett. 2023;34(2):107518. doi:10.1016/j.cclet.2022.05.032
34. Yang J, Zeng H, Luo Y, et al. Recent applications of PLGA in drug delivery systems. Polymers. 2024;16(18):2606. doi:10.3390/polym16182606
35. Antoniou AI, Giofrè S, Seneci P, Passarella D, Pellegrino S. Stimulus-responsive liposomes for biomedical applications. Drug Discovery Today. 2021;26(8):1794–1824. doi:10.1016/j.drudis.2021.05.010
36. El-Saadony MT, Saad AM, Alkafaas SS, et al. Chitosan, derivatives, and its nanoparticles: preparation, physicochemical properties, biological activities, and biomedical applications - A comprehensive review. Int J Biolog Macromole. 2025;313:142832. doi:10.1016/j.ijbiomac.2025.142832
37. Bose A, Roy Burman D, Sikdar B, Patra P. Nanomicelles: types, properties and applications in drug delivery. IET Nanobiotechnol. 2021;15(1):19–27. doi:10.1049/nbt2.12018
38. Yang C, Xue Y, Duan Y, Mao C, Wan M. Extracellular vesicles and their engineering strategies, delivery systems, and biomedical applications. J Controlled Release. 2024;365:1089–1123. doi:10.1016/j.jconrel.2023.11.057
39. Mejía-Méndez JL, Vazquez-Duhalt R, Hernández LR, Sánchez-Arreola E, Bach H. Virus-like particles: fundamentals and biomedical applications. Int J Mol Sci. 2022;23(15):8579. doi:10.3390/ijms23158579
40. Hammami I, Alabdallah NM, Jomaa AA, Kamoun M. Gold nanoparticles: synthesis properties and applications. J King Saud Univ Sci. 2021;33(7):101560. doi:10.1016/j.jksus.2021.101560
41. Bruna T, Maldonado-Bravo F, Jara P, Caro N. Silver nanoparticles and their antibacterial applications. Int J Mol Sci. 2021;22(13):7202. doi:10.3390/ijms22137202
42. Salman MD, Radzi YM, Salih EY, Oglat AA, Rahman AA, Dheyab MA. Synthesis techniques and modern applications of copper oxide nanoparticles in cancer treatment and radiotherapy: a review. J Mol Struct. 2025;1322:140301. doi:10.1016/j.molstruc.2024.140301
43. Pourmadadi M, Holghoomi R, Shamsabadipour A, Maleki-baladi R, Rahdar A, Pandey S. Copper nanoparticles from chemical, physical, and green synthesis to medicinal application: a review. Plant Nano Biology. 2024;8:100070. doi:10.1016/j.plana.2024.100070
44. Janjua TI, Cao Y, Kleitz F, Linden M, Yu C, Popat A. Silica nanoparticles: a review of their safety and current strategies to overcome biological barriers. Adv Drug Delivery Rev. 2023;203:115115. doi:10.1016/j.addr.2023.115115
45. Hassanpour P, Panahi Y, Ebrahimi‐Kalan A, Akbarzadeh A. Biomedical applications of aluminium oxide nanoparticles. Micro Nano Lett. 2018;13(9):1227–1231. doi:10.1049/mnl.2018.5070
46. Garg A, Agrawal R, Singh Chauhan C, Deshmukh R. In-situ gel: a smart carrier for drug delivery. Int J Pharm. 2024;652:123819. doi:10.1016/j.ijpharm.2024.123819
47. Vigani B, Rossi S, Sandri G, Bonferoni MC, Caramella CM, Ferrari F. Recent advances in the development of In situ gelling drug delivery systems for non-parenteral administration routes. Pharmaceutics. 2020;12(9):859. doi:10.3390/pharmaceutics12090859
48. Eker F, Duman H, Akdaşçi E, et al. A comprehensive review of nanoparticles: from classification to application and toxicity. Molecules. 2024;29(15):3482. doi:10.3390/molecules29153482
49. Vargas-Nadal G, Köber M, Nsamela A, et al. Fluorescent multifunctional organic nanoparticles for drug delivery and bioimaging: a tutorial review. Pharmaceutics. 2022;14(11):2498. doi:10.3390/pharmaceutics14112498
50. Shahzad KA, Wang Z, Cai B, et al. Novel pharmaco-exosomal immunotherapy for united airway diseases: PLGA-encapsulated, mesenchymal stem cell-derived exosomes with PPAR-γ agonist for allergic rhinitis and asthma. Stem Cell Res Ther. 2025;16(1):488. doi:10.1186/s13287-025-04624-8
51. Far J, Abdel-Haq M, Gruber M, Abu Ammar A. Developing biodegradable nanoparticles loaded with mometasone furoate for potential nasal drug delivery. ACS Omega. 2020;5(13):7432–7439. doi:10.1021/acsomega.0c00111
52. Joshi VB, Adamcakova-Dodd A, Jing X, et al. Development of a poly (lactic-co-glycolic acid) particle vaccine to protect against house dust mite induced allergy. AAPS J. 2014;16(5):975–985. doi:10.1208/s12248-014-9624-5
53. Wu G-R, Zhou M, Wang Y, et al. Blockade of Mbd2 by siRNA-loaded liposomes protects mice against OVA-induced allergic airway inflammation via repressing M2 macrophage production. Front Immunol. 2022;13:930103. doi:10.3389/fimmu.2022.930103
54. Peng X, Ge Y, Li W, et al. Targeting lewis X oligosaccharide-modified liposomes encapsulated with house dust mite allergen der f 2 to dendritic cells inhibits Th2 immune response. Eur J Pharm Sci. 2023;190:106570. doi:10.1016/j.ejps.2023.106570
55. Yang W, Dong Z, Li Y, Zhang Y, Fu H, Xie Y. Therapeutic efficacy of chitosan nanoparticles loaded with BCG-polysaccharide nucleic acid and ovalbumin on airway inflammation in asthmatic mice. Eur J Clin Microbiol Infect Dis. 2021;40(8):1623–1631. doi:10.1007/s10096-021-04183-9
56. Wang X, Wang Y, Tang T, et al. Curcumin-loaded RH60/F127 mixed micelles: characterization, biopharmaceutical characters and anti-inflammatory modulation of airway inflammation. Pharmaceutics. 2023;15(12):2710. doi:10.3390/pharmaceutics15122710
57. Peng X, Liang Y, Li J, et al. Preventive effects of “ovalbumin-conjugated celastrol-loaded nanomicelles’’ in a mouse model of ovalbumin-induced allergic airway inflammation. Eur J Pharm Sci. 2020;143:105172. doi:10.1016/j.ejps.2019.105172
58. Fang S-B, Zhang H-Y, Wang C, et al. Small extracellular vesicles derived from human mesenchymal stromal cells prevent group 2 innate lymphoid cell-dominant allergic airway inflammation through delivery of miR-146a-5p. J Extracell Vesicles. 2020;9(1):1723260. doi:10.1080/20013078.2020.1723260
59. Cruz FF, Borg ZD, Goodwin M, et al. Systemic administration of human bone marrow-derived mesenchymal stromal cell extracellular vesicles ameliorates aspergillus hyphal extract-induced allergic airway inflammation in immunocompetent mice. Stem Cells Transl Med. 2015;4(11):1302–1316. doi:10.5966/sctm.2014-0280
60. Yang W, Pan Z, Zhang J, et al. Extracellular vesicles from adipose stem cells ameliorate allergic rhinitis in mice by immunomodulatory. Front Immunol. 2023;14:1302336. doi:10.3389/fimmu.2023.1302336
61. De Castro LL, Xisto DG, Kitoko JZ, et al. Human adipose tissue mesenchymal stromal cells and their extracellular vesicles act differentially on lung mechanics and inflammation in experimental allergic asthma. Stem Cell Res Ther. 2017;8(1):151. doi:10.1186/s13287-017-0600-8
62. Chiang T-Y, Yang Y-R, Zhuo M-Y, et al. Microbiome profiling of nasal extracellular vesicles in patients with allergic rhinitis. World Allergy Organ J. 2022;15(8):100674. doi:10.1016/j.waojou.2022.100674
63. Fang S-B, Zhou Z-R, Sun Q, et al. Plasma extracellular vesicles regulate the functions of Th2 and ILC2 cells via miRNA-150-5p in patients with allergic rhinitis. Int Immunopharmacol. 2025;144:113644. doi:10.1016/j.intimp.2024.113644
64. Sani MZ, Bargahi A, Momenzadeh N, et al. Genetically engineered fusion of allergen and viral-like particle induces a more effective allergen-specific immune response than a combination of them. Appl Microbiol Biotechnol. 2021;105(1):77–91. doi:10.1007/s00253-020-11012-0
65. Horvath D, Basler M. PLGA particles in immunotherapy. Pharmaceutics. 2023;15(2):615. doi:10.3390/pharmaceutics15020615
66. Sadeghi M, Asadirad A, Koushki K, Keshavarz Shahbaz S, Dehnavi S. Recent advances in improving intranasal allergen-specific immunotherapy; focus on delivery systems and adjuvants. Int Immunopharmacol. 2022;113(Pt A):109327. doi:10.1016/j.intimp.2022.109327
67. Duong V-A, Nguyen T-T-L, Maeng H-J. Recent advances in intranasal liposomes for drug, gene, and vaccine delivery. Pharmaceutics. 2023;15(1):207. doi:10.3390/pharmaceutics15010207
68. Nsairat H, Khater D, Sayed U, Odeh F, Al Bawab A, Alshaer W. Liposomes: structure, composition, types, and clinical applications. Heliyon. 2022;8(5):e09394. doi:10.1016/j.heliyon.2022.e09394
69. Shim S, Yoo HS. The application of mucoadhesive chitosan nanoparticles in nasal drug delivery. Mar Drugs. 2020;18(12):605. doi:10.3390/md18120605
70. Perumal S, Atchudan R, Lee W. A review of polymeric micelles and their applications. Polymers. 2022;14(12):2510. doi:10.3390/polym14122510
71. Baidya M, Shilpi S, Bhatt S. Nanomicelles for the management of allergic airway diseases. In: Prasher P, Sharma M, Singh SK, MacLoughlin R, Pabreja K, Dua K, editors. Understanding Allergic Airway Diseases: Contemporary Treatment Paradigm. 2024:117–135. doi:10.1007/978-981-97-1953-2_7
72. Beach MA, Nayanathara U, Gao Y, et al. Polymeric nanoparticles for drug delivery. Chem Rev. 2024;124(9):5505–5616. doi:10.1021/acs.chemrev.3c00705
73. Su X, Wang H, Li Q, Chen Z. Extracellular vesicles: a review of their therapeutic potentials, sources, biodistribution, and administration routes. Int J Nanomed. 2025;20:3175–3199. doi:10.2147/ijn.s502591
74. Mizenko RR, Feaver M, Bozkurt BT, et al. A critical systematic review of extracellular vesicle clinical trials. J Extracell Vesicles. 2024;13(10):e12510. doi:10.1002/jev2.12510
75. Nooraei S, Bahrulolum H, Hoseini ZS, et al. Virus-like particles: preparation, immunogenicity and their roles as nanovaccines and drug nanocarriers. J Nanobiotechnol. 2021;19(1):59. doi:10.1186/s12951-021-00806-7
76. Tariq H, Batool S, Asif S, Ali M, Abbasi BH. Virus-like particles: revolutionary platforms for developing vaccines against emerging infectious diseases. Front Microbiol. 2022;12:790121. doi:10.3389/fmicb.2021.790121
77. Zepeda-Cervantes J, Ramírez-Jarquín JO, Vaca L. Interaction between virus-like particles (VLPs) and pattern recognition receptors (PRRs) from dendritic cells (DCs): toward better engineering of VLPs. Front Immunol. 2020;11:1100. doi:10.3389/fimmu.2020.01100
78. Ma X, Luan Z, Li J. Inorganic nanoparticles-based systems in biomedical applications of stem cells: opportunities and challenges. Int J Nanomed. 2023;18:143–182. doi:10.2147/IJN.S384343
79. Serra MF, Cotias AC, Pimentel AS, et al. Gold nanoparticles inhibit steroid-insensitive asthma in mice preserving histone deacetylase 2 and NRF2 pathways. Antioxidants. 2022;11(9):1659. doi:10.3390/antiox11091659
80. Liu Y, Gao J, Huo Y, Yang Y, Yue D, Lin X. A near-infrared photoelectrochemical aptasensor based on a Yb–Bi 2 S 3 /AuNP nanocomposite for determining miRNA-155, a biomarker for allergic rhinitis. Analytical Methods. 2025;17(24):4961–4969. doi:10.1039/d5ay00212e
81. Xiaoshang G, Murakonda GK, Mu Y. Biofabrication of silver nanoparticles using ostericum koreanum plant extract for treatment of allergic rhinitis in nursing care. Mater Res Express. 2021;8(1):15004. doi:10.1088/2053-1591/abd4b5
82. Liu T, Zhou C, Gao Y, Du X. An experimental mice model for ovalbumin-induced allergic rhinitis imbued with copper oxide green nanoparticles from leaf extract ofLaurus nobilis. Appl Organometallic Chem. 2025;39(1):e7755. doi:10.1002/aoc.7755
83. Peng G, Cai J, Wang Z, et al. Facile fabrication of diatomite biosilica-based nasal drug delivery vehicle for enhanced treatment of allergic rhinitis. Colloids Surf, B. 2024;234:113715. doi:10.1016/j.colsurfb.2023.113715
84. Athari SS, Pourpak Z, Folkerts G, et al. Conjugated alpha-alumina nanoparticle with vasoactive intestinal peptide as a nano-drug in treatment of allergic asthma in mice. Eur J Pharmacol. 2016;791:811–820. doi:10.1016/j.ejphar.2016.10.014
85. Li L, Wang J, Athari SS, Jiang C-W. Study on anti-inflammatory effect of peptides-conjugated alumina nanoparticle on allergic rhinitis mice model. Allergologia et Immunopathologia. 2023;51(3):111–116. doi:10.15586/aei.v51i3.819
86. Fan J, Cheng Y, Sun M. Functionalized gold nanoparticles: synthesis, properties and biomedical applications. The Chemical Record. 2020;20(12):1474–1504. doi:10.1002/tcr.202000087
87. Duman H, Akdaşçi E, Eker F, Bechelany M, Karav S. Gold nanoparticles: multifunctional properties, synthesis, and future prospects. Nanomaterials. 2024;14(22):1805. doi:10.3390/nano14221805
88. Ferdous Z, Nemmar A. Health impact of silver nanoparticles: a review of the biodistribution and toxicity following various routes of exposure. Int J Mol Sci. 2020;21(7):2375. doi:10.3390/ijms21072375
89. Gomes HIO, Martins CSM, Prior JAV. Silver nanoparticles as carriers of anticancer drugs for efficient target treatment of cancer cells. Nanomaterials. 2021;11(4):964. doi:10.3390/nano11040964
90. Sajjad H, Sajjad A, Haya RT, Khan MM, Zia M. Copper oxide nanoparticles: in vitro and in vivo toxicity, mechanisms of action and factors influencing their toxicology. Comp Biochem Physiol Part C. 2023;271:109682. doi:10.1016/j.cbpc.2023.109682
91. Li Z, Mu Y, Peng C, Lavin MF, Shao H, Du Z. Understanding the mechanisms of silica nanoparticles for nanomedicine. WIREs Nanomed Nanobiotechnol. 2021;13(1):e1658. doi:10.1002/wnan.1658
92. Kovtareva SY, Kopishev EE, Zhang H, Filippov SK. Exploring the physicochemical interactions and loading strategies of mesoporous silicon dioxide nanoparticles for drug delivery. Euro J Pharmaceu Biopharmaceu. 2025;208:114654. doi:10.1016/j.ejpb.2025.114654
93. Brandenberger C, Rowley NL, Jackson-Humbles DN, et al. Engineered silica nanoparticles act as adjuvants to enhance allergic airway disease in mice. Part Fibre Toxicol. 2013;10(1):26. doi:10.1186/1743-8977-10-26
94. Bashir S, Hina M, Iqbal J, et al. Fundamental concepts of hydrogels: synthesis, properties, and their applications. Polymers. 2020;12(11):2702. doi:10.3390/polym12112702
95. Altuntaş E, Yener G, Doğan R, Aksoy F, Şerif Aydın M, Karataş E. Effects of a thermosensitive In situ gel containing mometasone furoate on a rat allergic rhinitis model. Am J Rhinol Allergy. 2018;32(3):132–138. doi:10.1177/1945892418764951
96. Phongpradist R, Chittasupho C, Singh S, et al. Investigation of a thermoresponsive In situ hydrogel loaded with nanotriphala: implications for antioxidant, anti-inflammatory, and antimicrobial therapy in nasal disorders. Gels. 2025;11(2):106. doi:10.3390/gels11020106
97. Shurbaji S, El-Sherbiny IM, Alser M, et al. Nitric oxide releasing hydrogel nanoparticles decreases epithelial cell injuries associated with airway reopening. Front Bioeng Biotechnol. 2021;8:579788. doi:10.3389/fbioe.2020.579788
98. Salatin S, Barar J, Barzegar-Jalali M, Adibkia K, Milani MA, Jelvehgari M. Hydrogel nanoparticles and nanocomposites for nasal drug/vaccine delivery. Arch Pharmacal Res. 2016;39(9):1181–1192. doi:10.1007/s12272-016-0782-0
99. Gao W, Zhang Y, Zhang Q, Zhang L. Nanoparticle-hydrogel: a hybrid biomaterial system for localized drug delivery. Ann Biomed Eng. 2016;44(6):2049–2061. doi:10.1007/s10439-016-1583-9
100. Choi W, Kohane DS. Hybrid nanoparticle–hydrogel systems for drug delivery depots and other biomedical applications. ACS Nano. 2024;18(34):22780–22792. doi:10.1021/acsnano.4c06888
101. Su Y, Sun B, Gao X, Liu S, Hao R, Han B. Chitosan hydrogel doped with PEG-PLA nanoparticles for the local delivery of miRNA-146a to treat allergic rhinitis. Pharmaceutics. 2020;12(10):907. doi:10.3390/pharmaceutics12100907
102. Hua S. Targeting sites of inflammation: intercellular adhesion molecule-1 as a target for novel inflammatory therapies. Front Pharmacol. 2013;4:127. doi:10.3389/fphar.2013.00127
103. Rabanel JM, Aoun V, Elkin I, Mokhtar M, Hildgen P. Drug-loaded nanocarriers: passive targeting and crossing of biological barriers. Curr Med Chem. 2012;19(19):3070–3102. doi:10.2174/092986712800784702
104. Hua T, Li S, Han B. Nanomedicines for intranasal delivery: understanding the nano-bio interactions at the nasal mucus-mucosal barrier. Expert Opin Drug Delivery. 2024;21(4):553–572. doi:10.1080/17425247.2024.2339335
105. Liu L, Zhao W, Ma Q, et al. Functional nano-systems for transdermal drug delivery and skin therapy. Nanoscale Adv. 2023;5(6):1527–1558. doi:10.1039/D2NA00530A
106. Hua S. Advances in nanoparticulate drug delivery approaches for sublingual and buccal administration. Front Pharmacol. 2019;10:1328. doi:10.3389/fphar.2019.01328
107. Kobayashi K, Wei J, Iida R, Ijiro K, Niikura K. Surface engineering of nanoparticles for therapeutic applications. Polym J. 2014;46(8):460–468. doi:10.1038/pj.2014.40
108. Saeedi Garakani S, Davachi SM, Bagher Z, et al. Fabrication of chitosan/polyvinylpyrrolidone hydrogel scaffolds containing PLGA microparticles loaded with dexamethasone for biomedical applications. Int J Biol Macromol. 2020;164:356–370. doi:10.1016/j.ijbiomac.2020.07.138
109. El-Helaly SN, Amr KA, Fadel M, Fahmy RH. Fluticasone propionate zein nanoparticles - loaded in situ gelling system: in vitro/ex vivo studies and associated in vivo nasal MMP9 suppressed effect. J Drug Delivery Sci Technol. 2024;96:105674. doi:10.1016/j.jddst.2024.105674
110. Javed H, Shah SNH, Iqbal FM, Javed N, Saeed B. A hematological and histopathological study on diphenhydramine nasal nano-gel and nano-emulgel for the management of allergic rhinitis in animal model. AAPS Pharmscitech. 2023;24(2):55. doi:10.1208/s12249-023-02515-w
111. Sun M, Qin D, Fan P, Chen X, Liu Y. Chitosan-centered nanosystems as sustained therapeutics for allergic rhinitis intervention: inhibition of histamine-induced cascades. J Controlled Release. 2021;335:422–436. doi:10.1016/j.jconrel.2021.05.048
112. Tamaddon L, Mohamadi N, Bavarsad N. Preparation and characterization of mucoadhesive loratadine nanoliposomes for intranasal administration. Turk J Pharm Sci. 2021;18(4):492–497. doi:10.4274/tjps.galenos.2020.33254
113. Mohamad SA, Safwat MA, Elrehany M, Maher SA, Badawi AM, Mansour HF. A novel nasal co-loaded loratadine and sulpiride nanoemulsion with improved downregulation of TNF-α, TGF-β and IL-1 in rabbit models of ovalbumin-induced allergic rhinitis. Drug Delivery. 2021;28(1):229–239. doi:10.1080/10717544.2021.1872741
114. Lockett J, Inder WJ, Clifton VL. The glucocorticoid receptor: isoforms, functions, and contribution to glucocorticoid sensitivity. Endocr Rev. 2024;45(4):593–624. doi:10.1210/endrev/bnae008
115. Linton S, Hossenbaccus L, Ellis AK. Evidence-based use of antihistamines for treatment of allergic conditions. Ann Allergy Asthma Immunol. 2023;131(4):412–420. doi:10.1016/j.anai.2023.07.019
116. Wolfson AR, Wong D, Abrams EM, Waserman S, Sussman GL. Diphenhydramine: time to move on? J Allergy Clin Immunol. 2022;10(12):3124–3130. doi:10.1016/j.jaip.2022.07.018
117. Jing Z, Li W, Liao W, et al. Fructus xanthii and magnolia liliiflora volatile oils liposomes-loaded thermosensitive in situ gel for allergic rhinitis management. Int J Nanomed. 2024;19:1557–1570. doi:10.2147/IJN.S445240
118. Zhang FZ, Tan M, Zeng J, et al. A supramolecular assembly of EGCG for long-term treatment of allergic rhinitis. ACS Biomater Sci Eng. 2024;10(4):2282–2298. doi:10.1021/acsbiomaterials.4c00091
119. Mu D, Zhou L, Shi L, et al. Quercetin-crosslinked chitosan nanoparticles: a potential treatment for allergic rhinitis. Sci Rep. 2024;14(1):4021. doi:10.1038/s41598-024-54501-2
120. Shahgordi S, Sankian M, Yazdani Y, et al. Immune responses modulation by curcumin and allergen encapsulated into PLGA nanoparticles in mice model of rhinitis allergic through sublingual immunotherapy. Int Immunopharmacol. 2020;84:106525. doi:10.1016/j.intimp.2020.106525
121. Arizmendi N, Qian H, Li Y, Kulka M. Sesquiterpene-loaded Co-polymer hybrid nanoparticle effects on human mast cell surface receptor expression, granule contents, and degranulation. Nanomaterials. 2021;11(4):953. doi:10.3390/nano11040953
122. Lauriello M, Di Rubbo V, Sinatti G, et al. Correlation between SNOT-22, nasal cytology, and mood disorders in patients with allergic rhinitis treated with a liposomal nasal spray. Allergy & Rhinology. 2019;10:2152656719866809. doi:10.1177/2152656719866809
123. Lauriello M, Di Marco GP, Necozione S, et al. Effetti dell’applicazione di spray liposomiale con vitamine A ed E nelle riniti allergiche. Acta Otorhinolaryngologica Italica. 2020;40(3):217–223. doi:10.14639/0392-100X-N0357
124. Casula E, Manca ML, Perra M, et al. Nasal spray formulations based on combined hyalurosomes and glycerosomes loading zingiber officinalis extract as green and natural strategy for the treatment of rhinitis and rhinosinusitis. Antioxidants. 2021;10(7):1109. doi:10.3390/antiox10071109
125. Jiang H, Yang L, Xing X, et al. A UPLC-MS/MS application for comparisons of the hepatotoxicity of raw and processed xanthii fructus by energy metabolites. RSC Adv. 2019;9(5):2756–2762. doi:10.1039/c8ra08272c
126. Atchudan R, Edison TNJI, Aseer KR, Perumal S, Lee YR. Hydrothermal conversion of Magnolia liliiflora into nitrogen-doped carbon dots as an effective turn-off fluorescence sensing, multi-colour cell imaging and fluorescent ink. Colloids Surf B. 2018;169:321–328. doi:10.1016/j.colsurfb.2018.05.032
127. Capasso L, De Masi L, Sirignano C, et al. Epigallocatechin gallate (EGCG): pharmacological properties, biological activities and therapeutic potential. Molecules. 2025;30(3):654. doi:10.3390/molecules30030654
128. Huang M, Liu X, Ren Y, et al. Quercetin: a flavonoid with potential for treating acute lung injury. Drug Des Dev Ther. 2024;18:5709–5728. doi:10.2147/DDDT.S499037
129. Brandes MS, Gray NE. NRF2 as a therapeutic target in neurodegenerative diseases. ASN NEURO. 2020;12(1):1759091419899782. doi:10.1177/1759091419899782
130. Arizmendi N, Hou C, Guo F, Li Y, Kulka M. Bicyclic eremophilane-type petasite sesquiterpenes potentiate peroxisome proliferator–activated receptor γ activator–mediated inhibition of dendritic cells. Int J Immunopathol Pharmacol. 2018;32:2058738418787739. doi:10.1177/2058738418787739
131. Luo H, Wang X, Kong H, Wang J, Zhou Q. Correlation between vitamin a, D, E, and K levels in children with allergic rhinitis: a propensity-matched analysis. BMC Pediatr. 2025;25(1):491. doi:10.1186/s12887-025-05855-7
132. Zhang P. The role of diet and nutrition in allergic diseases. Nutrients. 2023;15(17):3683. doi:10.3390/nu15173683
133. Zhang M, Zhao R, Wang D, et al. Ginger (Zingiber officinaleRosc.) and its bioactive components are potential resources for health beneficial agents. Phytotherapy Res. 2021;35(2):711–742. doi:10.1002/ptr.6858
134. Oeo‐Santos C, Navas A, Benedé S, et al. New insights into the sensitization to nonspecific lipid transfer proteins from pollen and food: new role of allergen ole e 7. Allergy. 2020;75(4):798–807. doi:10.1111/all.14086
135. Liu W, Ota M, Tabushi M, Takahashi Y, Takakura Y. Development of allergic rhinitis immunotherapy using antigen-loaded small extracellular vesicles. J Controlled Release. 2022;345:433–442. doi:10.1016/j.jconrel.2022.03.016
136. Niazi V, Ghafouri‐Fard S, Verdi J, et al. Hypoxia preconditioned mesenchymal stem cell-derived exosomes induce ex vivo expansion of umbilical cord blood hematopoietic stem cells CD133 + by stimulation of Notch signaling pathway. Biotechnol Prog. 2022;38(1):e3222. doi:10.1002/btpr.3222
137. Wen X, Zhao C, Zhao Y, Yang J, Cheng J, Wang Z. Multifunctional MXene-modified GelMA hydrogel loaded with hypoxia-induced mesenchymal stem cells derived extracellular vesicles alleviates allergic rhinitis in mice. Int J Biol Macromol. 2024;281:136485. doi:10.1016/j.ijbiomac.2024.136485
138. Xu M, Ren M, Zhang X, et al. Mesenchymal stem cell-derived small extracellular vesicles restored nasal barrier function in allergic rhinitis via miR-143–GSK3B in human nasal epithelial cells. J Allergy Clin Immunol. 2025;155(4):1236–1249.e5. doi:10.1016/j.jaci.2024.10.034
139. Yang W, Pan Z, Zhang J, et al. Administration strategy-dependent mechanisms and effects of human adipose tissue stem cell extracellular vesicles in mouse allergic rhinitis treatment. Cell Transplant. 2025;34:9636897251325673. doi:10.1177/09636897251325673
140. Peng Y-Q, Wu Z-C, Xu Z-B, et al. Mesenchymal stromal cells-derived small extracellular vesicles modulate DC function to suppress Th2 responses via IL-10 in patients with allergic rhinitis. Eur J Immunol. 2022;52(7):1129–1140. doi:10.1002/eji.202149497
141. Zhao C, Wei X, Kong W, et al. Mesenchymal stem cell derived extracellular vesicles loaded thermosensitive chitosan-based hydrogel alleviates allergic rhinitis in mouse model. Mater Des. 2023;233:112271. doi:10.1016/j.matdes.2023.112271
142. Shahzad KA, Wang Z, Li X, Li J, Xu M, Tan F. Immunomodulatory effect of PLGA-encapsulated mesenchymal stem cells-derived exosomes for the treatment of allergic rhinitis. Front Immunol. 2024;15:1429442. doi:10.3389/fimmu.2024.1429442
143. Ye Y-M, Zhao Y-X, Xiang L-R, et al. The immunomodulatory mechanism and research progress of mesenchymal stem cells in the treatment of allergic rhinitis. Stem Cell Res Ther. 2025;16(1):188. doi:10.1186/s13287-025-04333-2
144. Qiu M, Li T, Wang B, Gong H, Huang T. miR-146a-5p regulated cell proliferation and apoptosis by targeting SMAD3 and SMAD4. Protein Pept Lett. 2020;27(5):411–418. doi:10.2174/0929866526666190911142926
145. Li H, Wang Y, Han X. ESP-B4 promotes nasal epithelial cell-derived extracellular vesicles containing miR-146a-5p to modulate Smad3/GATA-3 thus relieving allergic rhinitis ESP-B4/miR-146a-5p in AR. Phytomedicine. 2023;108:154516. doi:10.1016/j.phymed.2022.154516
146. Adin SN, Gupta I, Panda BP, Mujeeb M. Monascin and ankaflavin—Biosynthesis from Monascus purpureus, production methods, pharmacological properties: a review. Biotechnol Appl Biochem. 2023;70(1):137–147. doi:10.1002/bab.2336
147. W Z, Ka S, L D, et al. PLGA-loaded monascin intranasal delivery system: sustained-release and immunomodulatory effect for treatment of allergic rhinitis by improving regulatory T cell function. ACS Appl Bio Mater. 2025;8(7). doi:10.1021/acsabm.5c00387
148. Ci Z, Wang H, Luo J, et al. Application of nanomaterials targeting immune cells in the treatment of chronic inflammation. Int J Nanomed. 2024;19:13925–13946. doi:10.2147/IJN.S497590
149. Lu L, Kong WY, Zhang J, et al. Utilizing murine dendritic cell line DC2.4 to evaluate the immunogenicity of subunit vaccines in vitro. Front Immunol. 2024;15:1298721. doi:10.3389/fimmu.2024.1298721
150. Liu C, Qi W, Teng Z, et al. NGR-modified PEG-PLGA micelles containing shikonin enhance targeting of dendritic cells for therapy of allergic rhinitis. Int Immunopharmacol. 2022;107:108649. doi:10.1016/j.intimp.2022.108649
151. Zheng X, Sun C, Yu R, et al. CD13-specific ligand facilitates xanthatin nanomedicine targeting dendritic cells for therapy of refractory allergic rhinitis. Int J Pharm. 2020;577:119034. doi:10.1016/j.ijpharm.2020.119034
152. Perera B, Wu Y, Nguyen N-T, Ta HT. Advances in drug delivery to atherosclerosis: investigating the efficiency of different nanomaterials employed for different type of drugs. Mater Today Bio. 2023;22:100767. doi:10.1016/j.mtbio.2023.100767
153. Liu J, Wang M, Tian X, et al. New insights into allergic rhinitis treatment: MSC nanovesicles targeting dendritic cells. J Nanobiotechnol. 2024;22(1):575. doi:10.1186/s12951-024-02748-2
154. Pordel S, Haghnavaz N, Rezaee M, et al. An epicutaneous therapeutic pollen-allergen extract delivery system in an allergic rhinitis mouse model: based on allergen loading on DC-specific aptamers conjugated nanogolds. Immunol Res. 2024;72(3):460–475. doi:10.1007/s12026-023-09445-6
155. Keshavarz Shahbaz S, Varasteh A-R, Koushki K, et al. Sublingual dendritic cells targeting by aptamer: possible approach for improvement of sublingual immunotherapy efficacy. Int Immunopharmacol. 2020;85:106603. doi:10.1016/j.intimp.2020.106603
156. Sadeghi M, Dehnavi S, Khodadadi A, et al. Immunomodulatory features of MSC-derived exosomes decorated with DC-specific aptamer for improving sublingual immunotherapy in allergic mouse model. Stem Cell Res Ther. 2024;15(1):481. doi:10.1186/s13287-024-04099-z
157. Koushki K, Varasteh A-R, Shahbaz SK, et al. Dc-specific aptamer decorated gold nanoparticles: a new attractive insight into the nanocarriers for allergy epicutaneous immunotherapy. Int J Pharmaceu. 2020;584:119403. doi:10.1016/j.ijpharm.2020.119403
158. Sadeghi M, Koushki K, Mashayekhi K, et al. DC-targeted gold nanoparticles as an efficient and biocompatible carrier for modulating allergic responses in sublingual immunotherapy. Int Immunopharmacol. 2020;86:106690. doi:10.1016/j.intimp.2020.106690
159. Haghnavaz N, Rezaee MA, Pordel S, et al. Mannose targeting of poly(lactic-co-glycolic acid): a promising approach for improving sublingual allergen-specific immunotherapy. Immunopharmacol Immunotoxicol. 2024;46(6):815–828. doi:10.1080/08923973.2024.2410291
160. Costanzo G, Marchetti M, Ledda AG, et al. Mast cells in allergic and non-allergic upper airways diseases: sentinel in the watchtower. Int J Mol Sci. 2024;25(23):12615. doi:10.3390/ijms252312615
161. Shiba E, Izawa K, Kaitani A, et al. Ceramide-CD300f binding inhibits lipopolysaccharide-induced skin inflammation. J Biol Chem. 2017;292(7):2924–2932. doi:10.1074/jbc.M116.768366
162. Ide T, Izawa K, Diono W, et al. Intranasal administration of ceramide liposome suppresses allergic rhinitis by targeting CD300f in murine models. Sci Rep. 2024;14(1):8398. doi:10.1038/s41598-024-58923-w
163. Shen Q, Cao M, Yu C, et al. Biodegradable mesoporous organosilica-based nanostabilizer targeting mast cells for long-term treatment of allergic diseases. ACS Nano. 2024;18(26):16934–16946. doi:10.1021/acsnano.4c03069
164. Zhang Y, Wang M, Liu Z, et al. CCR3 gene knockout inhibits proliferation, differentiation, and migration of eosinophils in allergic rhinitis model mice. Mol Immunol. 2023;162:1–10. doi:10.1016/j.molimm.2023.08.004
165. Teng Z, Yang J, Chen X, Liu Y. Intranasal morphology transformation nanomedicines for long-term intervention of allergic rhinitis. ACS Nano. 2023;17(24):25322–25334. doi:10.1021/acsnano.3c08752
166. Hung L, Zientara B, Berin MC. Contribution of T cell subsets to different food allergic diseases. Immunol Rev. 2024;326(1):35–47. doi:10.1111/imr.13368
167. Mo L-H, Han H-Y, Jin Q-R, et al. T cell activator-carrying extracellular vesicles induce antigen-specific regulatory T cells. Clin Exp Immunol. 2021;206(2):129–140. doi:10.1111/cei.13655
168. González-Fernández Á, Maietta I. The forgotten innate immune cells: unraveling their prospective interactions with nanomaterials. Int J Nanomed. 2025;20:8173–8189. doi:10.2147/IJN.S517249
169. Trehan K, Saini M, Thakur S. Stimuli-responsive material in controlled release of drug. In: Engineered Biomaterials. Singapore: Springer;2023:535–561. doi:10.1007/978-981-99-6698-1_18
170. Pavón-Romero GF, Parra-Vargas MI, Ramírez-Jiménez F, Melgoza-Ruiz E, Serrano-Pérez NH, Teran LM. Allergen immunotherapy: current and future trends. Cells. 2022;11(2):212. doi:10.3390/cells11020212
171. Chen Y, Zhang C, Huang Y, et al. Intranasal drug delivery: the interaction between nanoparticles and the nose-to-brain pathway. Adv Drug Delivery Rev. 2024;207:115196. doi:10.1016/j.addr.2024.115196
172. Bahraminejad S, Almoazen H. Sublingual and buccal delivery: a historical and scientific prescriptive. Pharmaceutics. 2025;17(8):1073. doi:10.3390/pharmaceutics17081073
173. Jakic K, Selc M, Razga F, et al. Long-term accumulation, biological effects and toxicity of BSA-coated gold nanoparticles in the mouse liver, spleen, and kidneys. Int J Nanomed. 2024;19:4103–4120. doi:10.2147/IJN.S443168
174. Osman AI, Zhang Y, Farghali M, et al. Synthesis of green nanoparticles for energy, biomedical, environmental, agricultural, and food applications: a review. Environ Chem Lett. 2024;22(2):841–887. doi:10.1007/s10311-023-01682-3
175. Lee WT, Lee H, Kim J, et al. Alveolar macrophage phagocytosis-evading inhaled microgels incorporating nintedanib-PLGA nanoparticles and pirfenidone-liposomes for improved treatment of pulmonary fibrosis. Bioact Mater. 2024;33:262–278. doi:10.1016/j.bioactmat.2023.11.005
176. Alsaleh NB, Brown JM. Engineered nanomaterials and type I allergic hypersensitivity reactions. Front Immunol. 2020;11:222. doi:10.3389/fimmu.2020.00222
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Current Strategies and Potential Prospects for Nanoparticle-Mediated Treatment of Diabetic Nephropathy
Liu C, Wu K, Gao H, Li J, Xu X
Diabetes, Metabolic Syndrome and Obesity 2022, 15:2653-2673
Published Date: 31 August 2022
Recent Research Advances in Nano-Based Drug Delivery Systems for Local Anesthetics
Ma H, Pan Z, Lai B, Zan C, Liu H
Drug Design, Development and Therapy 2023, 17:2639-2655
Published Date: 30 August 2023
Biomimetic Nano-Drug Delivery System: An Emerging Platform for Promoting Tumor Treatment
Han X, Gong C, Yang Q, Zheng K, Wang Z, Zhang W
International Journal of Nanomedicine 2024, 19:571-608
Published Date: 18 January 2024
Nanotechnology for the Diagnosis and Treatment of Liver Cancer
Cai Y, Wang W, Jiao Q, Hu T, Ren Y, Su X, Li Z, Feng M, Liu X, Wang Y
International Journal of Nanomedicine 2024, 19:13805-13821
Published Date: 24 December 2024
Mannosamine-Engineered Nanoparticles for Precision Rifapentine Delivery to Macrophages: Advancing Targeted Therapy Against Mycobacterium Tuberculosis

Luan H, Peng C, Yasin P, Shang Q, Xiang W, Song X
Drug Design, Development and Therapy 2025, 19:2081-2102
Published Date: 19 March 2025