Back to Journals » International Journal of Nanomedicine » Volume 21
Nanodynamic Therapy in Colorectal Cancer: Engineering Precision Immunotherapy and Multimodal Synergy
Authors Wang F, Zhang Z ![]() , Chen J
, Chen J ![]() , Qian L, Chen B, Zhai L, Zhao J
, Qian L, Chen B, Zhai L, Zhao J ![]() , Chen T, Zhou J
, Chen T, Zhou J ![]() , Gou K, Zhao Z
, Gou K, Zhao Z ![]() , Zhu X, Xiao Z
, Zhu X, Xiao Z
Received 22 January 2026
Accepted for publication 10 March 2026
Published 23 March 2026 Volume 2026:21 598076
DOI https://doi.org/10.2147/IJN.S598076
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Kamakhya Prakash Misra
Feng Wang,1,* Zhongsong Zhang,2,* Junhao Chen,3,* Lingrong Qian,1,* Bo Chen,4,* Lumei Zhai,5 Junxian Zhao,6 Tianze Chen,7 Jingfeng Zhou,2 Keyi Gou,2 Zihan Zhao,2 Xingcheng Zhu,8 Zhiyuan Xiao1
1Gastrointestinal Endoscopy Center, The Second People’s Hospital of Qujing City, Qujing, Yunnan, People’s Republic of China; 2School of Clinical Medicine, Chengdu Medical College, Chengdu, 610550, People’s Republic of China; 3Department of Urology, The Second Affiliated Hospital of Kunming Medical University, Kunming, Yunnan, People’s Republic of China; 4Department of Urology, Qujing Second People’s Hospital, Qujing, Yunnan, People’s Republic of China; 5Department of Ophthalmology, The Second People’s Hospital of Qujing City, Qujing, Yunnan Province, People’s Republic of China; 6Department of Urology, 920th Hospital of Joint Logistics Support Force of Chinese People’s Liberation Army, Kunming, Yunnan, People’s Republic of China; 7Center for Reproductive Medicine, Yangzhou Maternal and Child Health Care Hospital Affiliated to Yangzhou University, Yangzhou, 225000, People’s Republic of China; 8Department of Clinical Laboratory, The Second People’s Hospital of Qujing City, Qujing, Yunnan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xingcheng Zhu; Zhiyuan Xiao, Email [email protected]; [email protected]
Abstract: Colorectal cancer (CRC) is a common malignancy that remains difficult to control with surgery, chemotherapy, radiotherapy, and targeted therapy. These challenges arise from tumor heterogeneity, therapy resistance, and frequent relapse or metastasis, especially in advanced disease. In addition, precision approaches are limited by interpatient variability, evolving targets, and suboptimal biomarker performance. Nanodynamic therapy (NDT) is a modular, energy-activated strategy (e.g. PDT, SDT, CDT, and EDT). It can be systematically engineered using a “Structure–Energy Conversion–Reaction Dynamics” framework that links nanoplatform architecture to stimulus-transduction efficiency and spatiotemporally controlled cytotoxic reactions. NDT converts externally applied light, ultrasound, or electric fields into localized oxidative or catalytic cytotoxicity, potentially reducing off-target injury. This approach is particularly relevant to CRC because intracavitary or endoluminal energy delivery enables precise spatiotemporal control that is difficult to achieve with systemic targeting alone. However, NDT alone rarely addresses the full complexity of the heterogeneous, immunosuppressive CRC microenvironment. Efficacy is often limited by hypoxia, immunologically “cold” tumors, and suboptimal synchronization of treatment timing and delivery. These constraints motivate rational combinations with immunotherapy and microenvironment-targeted interventions. In this review, we summarize organ-specific design principles for CRC-focused NDT. Guided by the Structure–Energy Conversion–Reaction Dynamics paradigm, we describe how nanostructure design (e.g. composition, morphology, and interfaces) governs energy deposition and conversion. We then explain how these processes shape ROS/catalytic kinetics and diffusion, and how the resulting dynamics can be tuned for CRC-relevant activation routes. We further discuss how programmable, locally activated modules can be integrated into synergistic regimens that couple tumor debulking and immunogenic cell death with durable immune programming. We also highlight localized hydrogel- or depot-based “logistics layers” that maintain high drug concentrations at resection margins or intraperitoneal sites. These platforms enable repeated external triggering and coordinated multiagent release, helping to overcome systemic co-delivery barriers. Finally, we outline translational priorities, including patient stratification and biomarkers, clinically compatible energy delivery, manufacturability, and tumor access constraints. These considerations may guide the development of CRC-ready NDT platforms toward prospective validation.
Keywords: immunotherapy, colorectal cancer, multimodal synergistic therapy, nanodynamic therapy, nanomedicine, tumor microenvironment
Introduction
Colorectal cancer (CRC) is among the most prevalent malignancies worldwide and remains a leading cause of cancer-related mortality, representing a substantial burden on global public health.1–3 Current standard treatment modalities for CRC include surgical resection, chemotherapy, radiotherapy, and molecularly targeted therapies.4,5 Although these approaches have significantly improved patient survival, their therapeutic efficacy remains constrained by tumor heterogeneity, treatment resistance, local recurrence, and distant metastasis.6,7 Consequently, the 5-year survival rate for patients with advanced disease remains unsatisfactory.8 In parallel, although precision medicine strategies have emerged, such as tailoring therapeutic regimens to individual tumor molecular profiles, their clinical implementation remains limited by target heterogeneity, treatment tolerance, and suboptimal biomarker specificity.9–11 Therefore, to address these unmet clinical needs, innovative therapeutic strategies for CRC are urgently required to enhance radiotherapy sensitivity, overcome hypoxia-induced resistance, and maximize tumor eradication while preserving organ function.12
In recent years, nanotechnology has emerged as a cutting-edge tool in the biomedical field, offering novel perspectives and advanced technological platforms for the diagnosis and treatment of CRC.13,14 Among these advances, research on nanodynamic therapy (NDT) for CRC has expanded rapidly, encompassing the design of high-efficiency nanosensitizers, tumor-targeted delivery strategies, and integration with synergistic modalities such as immunotherapy and chemotherapy.14,15 These studies not only deepen the mechanistic understanding of NDT but also introduce novel strategies for the precision treatment of CRC, with the goal of improving therapeutic efficacy through enhanced tumor-selective cytotoxicity and reduced systemic toxicity.14,16 NDT represents a rapidly evolving paradigm in nanotechnology-based cancer treatment. In this approach, external energy sources such as light, ultrasound, heat, or electric fields are used to activate nanosensitizers, leading to localized generation of reactive oxygen species (ROS) or other cytotoxic intermediates for precise tumor cell eradication.17,18 NDT encompasses multiple therapeutic modalities, including photodynamic therapy (PDT), sonodynamic therapy (SDT), electrodynamic therapy (EDT), and chemodynamic therapy (CDT).19 The mechanistic diversity of NDT enables it to overcome the limitations of single-modality therapies and to better address the complexity of the tumor microenvironment.19,20 Unlike conventional radiotherapy, NDT allows selective activation of energy sources such as localized light or ultrasound to induce high levels of ROS/RNS generation within tumor tissues. This enhances tumor destruction while minimizing damage to surrounding normal tissues.21 Furthermore, because rectal tumors are anatomically proximal to the intestinal lumen, transrectal or intracavitary energy-activation approaches such as optical or acoustic stimulation can be used to achieve highly controllable energy delivery and spatially precise NDT at the tumor site. This may be more critical than reliance on systemic targeting alone.20–22 This cancer-specific, spatially confined energy delivery represents a distinct engineering opportunity beyond conventional targeting strategies and offers theoretical advantages in overcoming key barriers, including radiotherapy resistance and hypoxia-associated treatment insensitivity.
At present, several reviews have addressed nanotechnology-based and energy-dependent tumor therapies, focusing on the fundamental mechanisms and general strategies underlying modalities such as PDT and SDT.21,23,24 However, comprehensive reviews focused on organ-specific nanodynamic therapies for CRC remain scarce. Given substantial unmet clinical needs in CRC management, particularly in the context of total neoadjuvant therapy (TNT) and organ-preservation strategies, and the unique advantages of NDT in controllable energy activation and localized generation of reactive species, this review provides a systematic analysis of underlying mechanisms, engineering implementations, and key challenges for clinical translation. In particular, this review emphasizes cancer-type-specific engineering opportunities and therapeutic logic, and proposes a conceptual framework to guide the rational design and strategic evolution of NDT for precision treatment of CRC.
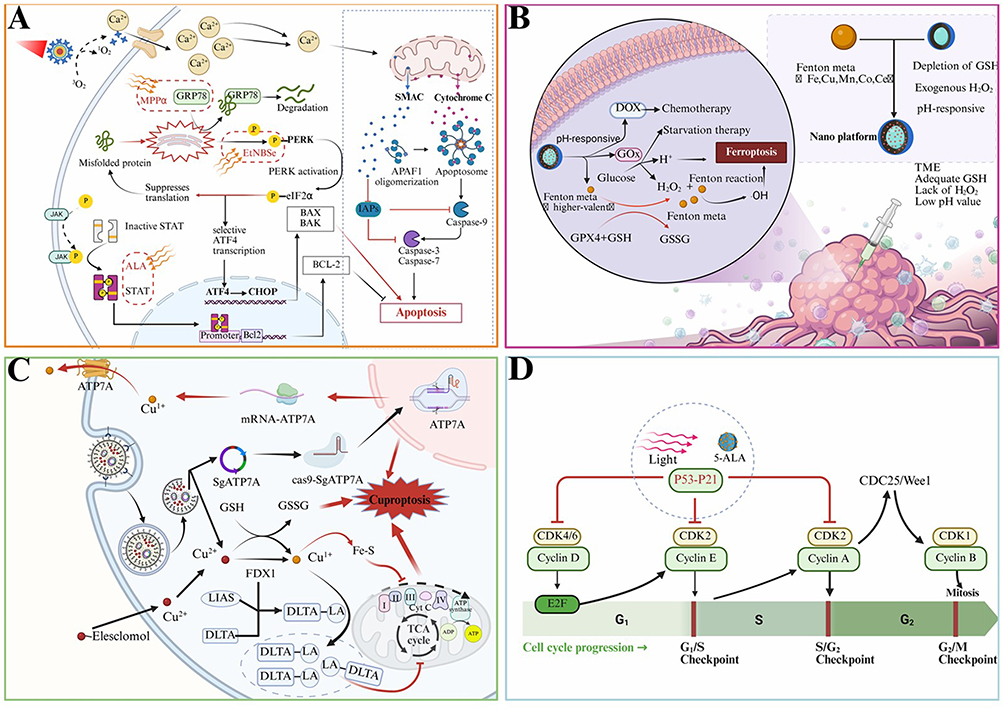 |
Figure 1 Molecular pathways involved in NDT-mediated tumor cell killing. (A) ROS-induced endoplasmic reticulum stress and mitochondrial apoptosis. (B) Ferroptosis triggered by Fenton/Fenton-like reactions and redox imbalance mediated by nano-platforms. In the tumor microenvironment (TME), the nano-platform releases catalytic metal ions (eg., Fe, Cu, Mn, Co, or Ce) that participate in Fenton or Fenton-like reactions. “Fenton metal” refers to redox-active transition metal ions capable of catalyzing H2O2 decomposition to generate highly reactive hydroxyl radicals (•OH), while “higher-valent metal species” denote oxidized metal intermediates produced during these catalytic cycles that further enhance ROS generation. The platform also promotes glucose oxidation via glucose oxidase (GOx), producing H2O2 and H⁺, while depletion of intracellular glutathione (GSH) and inhibition of GPX4 weaken antioxidant defenses, thereby amplifying lipid peroxidation and inducing ferroptosis. (C) Copper homeostasis disruption–mediated cuproptosis. (D) Cell cycle arrest regulated through p53-p21 and cyclin–CDK signaling pathways. Adapted from Li Y, Jin L, Tao Bet al Nanodynamic therapy for cancer: mechanistic innovations, targeting strategies and multimodal treatments. J Transl Med. Copyright © 2025 by authors.16 |
An Overview of the Design and Application of NDT Nanoplatforms in CRC
So far, we have gained a deep understanding of the challenges and potential advantages of NDT in the treatment of CRC (Figure 1). Although NDT has demonstrated controllable local effects and innovative treatment methods in tumor therapy, the design and application of nanoplatforms must be further optimized in order to successfully translate this therapy from basic research to clinical applications. In this process, how to construct an efficient and safe NDT nanoplatform, ensuring its superior targeting, drug loading capacity, and controllable release characteristics in the complex tumor microenvironment, has become a key factor for successful treatment.25,26 At present, the design of nanoplatforms is not limited to a single drug delivery function, but involves more multifunctional integration, including the synergistic effects of multiple modules such as intelligent response, immune activation, targeted delivery, and energy triggering.26,27 For example, through the precise design of nano platforms, the problems of oxygen deficiency and drug leakage in the tumor microenvironment can be effectively solved, and the therapeutic effect can be activated through external triggering mechanisms, making the treatment process more personalized and efficient.26 Therefore, this section will explore in detail the design principles, key technologies, and applications of different types of NDT nanoplatforms in the treatment of CRC, aiming to provide theoretical support and technical assurance for future clinical translational research.
NDT Nanoplatform Structure Energy Conversion Reaction Dynamics Triangle
Under the precise treatment of CRC, the reason why NDT is worth discussing separately is that it converts material structure into programmable energy conversion and quantifiable reaction kinetics, thereby making local tumor treatment a programmable, verifiable, and more clinically controllable thing.28,29 Maintaining consistency in focus from engineering to translation, we present NDT not only as a set of modalities but also as a design logic that links nanoplatform architecture, stimulus transduction, and measurable catalytic flux. The widely proposed “Structure–Energy Conversion–Reaction Dynamics” triangle provides a practical framework for NDT design.16,23 The structure axis governs active-site exposure, mass-transfer distances, interfacial electron or substrate transport, and targeted enrichment. The energy-conversion axis defines how inputs such as photons (NIR), ultrasound, electrons, or ionizing radiation are absorbed and converted into excited states, localized heat, charge separation, or secondary electrons.16,30 The reaction-dynamics axis determines key rate constants and the sustainability of catalytic flux for Fenton/Fenton-like reactions, enzyme-like catalysis, and free-radical chain reactions, including substrate selectivity and whether effective ROS/catalytic flux can be maintained under high GSH and a hypoxic TME.31,32 Importantly, CRC is not a monolithic disease. Its Consensus Molecular Subtypes (CMS) impose distinct microenvironmental constraints that can be rationally mapped onto the triangle.33,34 For example, CMS1 tumors are often immunogenic but remain constrained by immune suppression and metabolic stress. This profile suggests that NDT designs prioritizing reaction dynamics, such as sustaining ROS flux under hypoxia and high GSH and promoting immunogenic cell death, may be particularly relevant.35,36 By contrast, CMS4 tumors show a desmoplastic, stroma-rich phenotype and poor prognosis, implying that structure-end design, including improved penetration and retention, ECM-modulating interfaces, and diffusion-shortening architectures, and energy-end selection using deeper-penetrating stimuli are needed to overcome stromal transport barriers.37,38 For example, a semiconductor/metal oxide, TiO2–Ti3C2 (MXene) heterostructure, combines NIR-II photothermal efficiency with locally controllable tumor heating through the structural advantage of “layered interface carrier/phonon coupling”. This platform shows an energy-conversion window at 1064 nm that supports precise PTT and reproducible tumor suppression in human CRC cell lines and nude mouse subcutaneous tumor models. It also provides a materials-science rationale for combining radiotherapy or total neoadjuvant therapy (TNT) with local sensitization in RCR.39,40 However, because photonic penetration is intrinsically limited, the energy modality should be explicitly matched to lesion depth and clinical stage. NIR light typically penetrates on the millimeter scale, ultrasound can reach centimeter-scale depths with focusing, and X-rays offer essentially unrestricted penetration in tissue.41,42 In CRC, T3/T4 tumors frequently extend beyond the bowel wall and infiltrate perirectal or pericolic tissues. In such settings, deeper-penetrating energy sources, such as focused ultrasound or radiotherapy-compatible X-ray-activated platforms, may be more realistic for bulky or infiltrative disease. By contrast, endoluminal illumination may be advantageous for superficial lesions or tumors that are readily accessible from the lumen.43
Along the same metal oxide pathway, MnO2-modified hollow mesoporous SiO2 (HMSN@DHA@MnO2) links gate-controlled release at the structure end, defined by an HMSN reservoir and MnO2 shell, with reaction-dynamics tuning via GSH depletion, Mn2⁺ generation, and Fenton-like ROS production coupled to drugs and endogenous H2O2. The authors reported GSH-triggered degradation and an in vivo tumor inhibition rate of 52.6%, supporting the conclusion that reaction dynamics can be reshaped by TME substrate availability, particularly GSH. Such redox-adaptive design is particularly relevant in CRC, where the microenvironment is often highly reducing.44 In CRC, we further emphasize that reaction-dynamics tuning is not only a chemical problem but also a subtype-dependent biological one. For example, stromal hypoxia and redox buffering can be more prominent in aggressive phenotypes. This context reinforces why the triangle should be interpreted in a CMS-aware manner rather than as a purely materials-centric schematic.34,45 In MOF systems, the Cu PrIm three-in-one copper-based MOF nanoenzyme mimics the coordination microenvironment of natural copper enzymes via structurally twisted Cu-N4-like active centers. This design enables multiple enzyme-like activities and has been validated for antitumor efficacy and drug-resistance reversal in several CRC models. This example suggests that NDT is not simply the stacking of metal ions. Instead, coordination chemistry can render the catalytic cycle and substrate affinity programmable.46 In a setting closer to the clinical challenge of standard chemotherapy and drug resistance, Fe MOF nanoplatforms have been used to co-deliver oxaliplatin (OXA) and nitric oxide related substrates (L-Arg). This couples drug delivery with multipath resistance reprogramming, including NO-related regulation and TME remodeling, to target OXA-resistant CRC cells and improve efficacy. Such resistance-mechanism-oriented NDT design may align more readily with neoadjuvant therapy pathways.31 Because clinical translation requires more than mechanistic elegance, we also discuss Chemistry, Manufacturing, and Controls (CMC) considerations for multi-component MOF/COF platforms. Key issues include batch-to-batch compositional consistency, defect control, specifications for residual metals and ligands, and stability of catalytic activity during storage and sterilization.47–49 We also highlight that logistics layers, such as hydrogels and depots, face CRC-specific stability challenges in the gastrointestinal environment. Fecal enzymes, variable pH, and shear forces can compromise gel integrity and alter release profiles, and these factors should be addressed early to support reproducible manufacturing and regulatory alignment.50,51
Another materials-oriented example is surface engineering of a porphyrin-based MOF (PCN-224) loaded with Au nanoenzymes and copper peroxide nanodots. By leveraging the catalytic activity of Au and copper overload related triggering, this platform drives a cascade output that couples ROS-mediated apoptosis with cuprotosis. This behavior illustrates how structure-end features, including multiple interfaces and short-range electron or substrate transfer, can amplify the reaction-dynamics end by improving cascade efficiency and flux. This mechanistic narrative emphasizes a closed loop linking molecular death pathways to the material catalytic cycle in CRC.52 Complementary COF-based organic systems can also implement this triangular framework. For example, a disulfide-linked porphyrin COF undergoes triggered biodegradation and nanocrystallization under high GSH conditions. After loading with 5-Fu, it can further depolymerize and efficiently release the drug in tumor cells. In parallel, synergistic therapy can be achieved through a reaction sequence in which GSH depletion enhances PDT and amplifies ferroptosis and oxidative stress, indicating that purely organic frameworks can translate structural degradability into improved reaction kinetics.53 A more translational approach to drug delivery is to use pH sensitive carboxymethyl starch gelatin (CMS Gel) coated COF/5-Fu system, which utilizes the differences in pH and mucosal environment in the colorectal area to achieve better local delivery and reduce systemic exposure risk after oral administration. This integrated design of structure delivery kinetics is more friendly to the clinical reality of long-term, staged combination therapy for CRC.54 Given the dense and diverse colonic microbiome, we incorporate an organ-specific analysis of microbiome-NDT interactions. Pro-tumorigenic bacteria such as Fusobacterium nucleatum have been implicated in chemoresistance and TME shaping, raising two clinically relevant questions for NDT translation.55,56 First, can NDT-induced oxidative or catalytic stress selectively modulate pro-tumor microbes and improve therapy sensitivity.57 Second, can bacterial biofilms and microbial enzymes hinder nanoplatform penetration, alter catalytic substrates, or degrade logistics layers.58–60 We therefore add a subsection on microbiome-aware design opportunities, including biofilm-penetrating structure-end features, microbiota-responsive release, and combinations with microbiome-modulating strategies. Finally, the “energy conversion” end was truly connected to the clinical pathway of CRC: RA-PDT used radiation dose as an external energy to trigger photodynamic effects in the LARC (lymph node involvement) model, providing a more closely aligned NDT prototype with radiation therapy as the main line and local sensitization as the target, while X-PDT achieved X-ray triggered photodynamic chemotherapy synergy through folate modified lipid polymer nanoparticles co loaded with vitreofen and 5-Fu; Considering the crucial role of radiotherapy in neoadjuvant/TNT therapy for CRC, platforms that convert clinically available energy sources (RT) into nanoscale ROS kinetic outputs may be one of the most realistic approaches for NDT to move towards translational research.28,29,61
To quantitatively support the proposed “structure–energy transduction–reaction kinetics” triangle in CRC-relevant NDT, comparative studies of representative nanoplatforms show that structural manipulation can measurably alter energy deposition and transduction efficiency, as well as the sustainability of catalytic and ROS flux in the TME. These changes translate into differences in therapeutic output and translational feasibility. At the structure-to-energy interface, TiO2-coated Ti3C2 provides a quantitative example in CRC photothermal therapy. Under identical NIR-II irradiation (1064 nm, 0.5 W cm⁻2, 6 min, 100 µg mL⁻1), Ti3C2 alone heated to about 35 °C, whereas TiO2-coated Ti3C2 reached about 60 °C, with photothermal conversion efficiency (η) increasing to about 34.3%.34 These data quantify how interface engineering enhances energy ingestion and conversion into a clinically actionable thermal dose window.39 In electrically triggered NDT, where energy deposition depends on field-catalyst coupling, Fe3O4@Pt offers a quantitative readout across the triangle. Pt nanocrystal decoration at the structure end promotes electric-field-driven ROS formation at the energy end, while the Fe3O4 core releases iron under acidic conditions to drive Fenton chemistry. The authors reported that an AC square-wave electric field (5 mA, 10 min) markedly reduced cell viability, and the strongest synergy occurred when electric activation was combined with the Fenton substrate (H2O2) and GSH depletion. Mechanistically, Fe3⁺/Fe2⁺ cycling consumed intracellular GSH, measured by the Ellman assay, and restored ROS-mediated reactions that would otherwise be quenched by thiols, indicating that flux sustainability can be improved by reshaping the redox sink.62 The same study also reported translationally relevant quantitative endpoints, including tumor Pt accumulation of about 1.25% injected dose, a blood half-life of about 1.33 h, and efficacy even with initial tumor volumes of about 400 mm3. These metrics help connect measurable energy and flux outputs to biodistribution constraints that determine clinical controllability.62 A third CRC-relevant comparison shows that the choice of energy modality redefines transduction depth and dosimetry. An X-ray-activated PDT plus chemotherapy lipid-polymer nanoparticle system (FA-LPNPs-VP-5-FU, about 100 nm) generated ROS under a clinical 4 Gy X-ray fraction and induced apoptosis and necrosis in HCT116 cells, outperforming single modalities. In this design, the energy end is standardized by radiotherapy dosing, whereas the structure end, including a hybrid carrier, folate targeting, and co-loading, increases local reactant concentration and effective ROS yield per delivered dose.29 Importantly, RA-PDT has been evaluated in an in vivo rectal cancer context. One study reported that a single 4 Gy fraction activated verteporfin in a folate-functionalized lipid-polymer nanoplatform, generated ROS with minimal surrounding tissue injury, and inhibited primary tumors in orthotopic and subcutaneous models while suppressing lymph-node tumor progression. This example illustrates how clinically available RT can be converted into quantifiable ROS kinetics in anatomically relevant rectal settings.28 Finally, at the structure-to-kinetics vertex in a CRC-like reducing TME, MnO2-gated hollow mesoporous silica systems (HMSN@DHA@MnO2) used GSH-triggered degradation and Mn2⁺ generation to reprogram Fenton-like ROS kinetics. The authors reported an in vivo tumor inhibition rate of 52.6%, supporting the conclusion that substrate-adaptive structural gating can convert high GSH from a redox sink into a driver of catalytic flux.44
NDT Mediated TME Engineering of CRC
TME is often accompanied by hypoxia, high GSH reduction pressure, lactate accumulation/acidification, and immune suppression, which are unfavorable elements for tumor treatment. These factors not only determine the yield and diffusion radius of active species, but also determine whether the immune cycle can be ignited after treatment.63 For example, CRC cells enhance glycolysis and excrete lactate under hypoxia. Lactic acid not only shapes the acidic microenvironment, but also drives TAM polarization towards the M2 phenotype and induces HMGB1 related pro tumor signals, thereby amplifying the invasion and metastasis phenotype through the ERK/EMT/Wnt axis - meaning that “metabolic waste” itself is an engineered therapeutic target.63 Therefore, in recent years, NDT nano strategies have begun to use reaction substrates/inhibitors as programmable variables: for example, displaying lactate oxidase (LOX) and catalase (CAT) on the surface of protein nanoparticles (AalS), constructing AalS/LOX or AalS/LOX/CAT, which can continuously consume the lactate produced by CT26 colon cancer cells under normoxic and hypoxic conditions. The former generates H2O2 through LOX and triggers strong necrosis like killing, while the latter further regulates the supply and demand of H2O2/O2 through CAT to adapt to hypoxic TME, thus rewriting the lactate hypoxia immunosuppression chain into a more favorable reaction environment for ROS amplification.64 When oxygenation is proposed as a therapeutic mechanism, such as CAT mediated O2 supply, direct quantification of intratumoral oxygenation pO2 is recommended.65 Evidence should also be supported by hypoxia marker modulation, including HIF 1α, CAIX, and pimonidazole staining.66 When feasible, spatial or real time oxygen mapping methods such as photoacoustic imaging or BOLD MRI should be applied. These approaches are particularly important in orthotopic colorectal models, where vascular architecture and oxygen gradients differ markedly from those in subcutaneous systems.67,68
Correspondingly, chemical oxygen supplementation combined with reductive depletion on the material side is equally crucial. ZIF 90@CDDP@MnO2@HA employs an MnO2 shell as a TME responsive module. On the one hand, it exhausts GSH and weakens cisplatin detoxification and ROS clearance. On the other hand, it downregulates HIF-1 α through the decomposition of H2O2 to produce oxygen, alleviating hypoxia related drug resistance from the source. It also inhibits HK2/GLUT1 to suppress glycolysis energy supply. The released Mn2⁺ can participate in Fenton like reactions to achieve CDT amplification, which is equivalent to turning high GSH/hypoxia from resistance to reaction propulsion.69 Furthermore, the system also utilizes the Zn2 ⁺ released by the ZIF skeleton to induce mitochondrial damage and reduce ATP production, forming a dual channel cutoff with glycolysis inhibition, enabling the synergistic convergence of nanodynamic oxidative stress and metabolic starvation to cell death within the same TME window.69 On the immune dimension, TME engineering is pushing NDT from local chemical killing to scalable systemic immunotherapy: DOX@Zr-MOF Under acidic conditions, it can degrade and release drugs, triggering caspase-3/GSDME dependent pyroptosis. In the CT26 colon cancer model, it not only directly inhibits tumor growth, but also enhances systemic anti-tumor immunity by reshaping immunosuppressive TME, further significantly enhancing efficacy when combined with anti-PD-1. These findings suggest that immunogenic cell death and DME reprogramming represent an important interface for the clinical translation of NDT.70 The pH sensitive ZIF-8 nanoframe (CS/NPs) encapsulates mitoxantrone (MTX), a chemotherapy drug similar to mitoxantrone, and immunomodulatory peptide TP5 with chondroitin sulfate as the goal of immune cold tumor to heat. Firstly, the Zn2⁺ framework disrupts glycolysis and downregulates GLUT1, activating the AMPK axis to promote PD-L1 protein degradation, thereby reducing the immune checkpoint barrier; Secondly, MTX causes dsDNA damage, activates the cGAS STING pathway, and overlaps with TP5 to promote T cell/dendritic cell function, achieving stronger systemic immune response and lower systemic toxicity against CRC both in vitro and in vivo.71 We believe that from a translational perspective, these works collectively point towards a more clinically friendly design logic: using degradable frameworks (MOF/ZIF, protein nanoparticles) to carry enzyme/metal active centers, integrating oxygen supplementation, depletion of GSH, lactate metabolism reset, and STING/ICD activation into a set of TME response programs, thereby improving local control within the window of CRC radiotherapy/neoadjuvant therapy without significantly increasing systemic exposure and providing interpretable biomarker reads for immune combination (such as HIF-1 α, lactate, PD-L1, and T cell infiltration).70–72 To strengthen translational interpretability, oxygen generating designs should report whether the intervention measurably increases intratumoral pO2 rather than relying only on downstream inference.65 Reduced hypoxia associated signaling such as HIF 1α downregulation should also be demonstrated with independent hypoxia probes.73 Ideally, intratumoral oxygen mapping should be provided. This requirement is particularly important in orthotopic CRC models because vessel density, perfusion, and lumen adjacent oxygen diffusion are not accurately reproduced in subcutaneous xenograft models.74
Importantly, many CRC-NDT studies still rely on subcutaneous CT26 or MC38 models. Orthotopic and metastatic models can substantially reshape TME dependent treatment responses, including stromal architecture, immune infiltration, and perfusion or oxygen gradients. Therefore, these models can improve predictive validation for TME engineering related claims.68 For example, a direct comparison between subcutaneous and orthotopic MC38 implantation showed that the implantation site significantly alters the tumor immune microenvironment. It also changes the sensitivity and response trajectory to anti-PD-1 therapy. These findings indicate that the same therapeutic platform may produce different immunotherapy relevant outcomes depending on the tumor location.75 Consistent with this observation, location dependent profiling in murine colon cancer models has shown that orthotopic tumors display immune checkpoint and immune context features that differ from those of subcutaneous tumors. This suggests that conclusions regarding immune activation or relief of immune suppression should be validated in anatomically relevant settings.76 Methodologically, orthotopic CRC models established through cecal or colonic wall implantation better recapitulate local tumor invasion. These models also enable clinically relevant liver and lung metastatic spread. Such processes are difficult to reproduce in standard subcutaneous systems but are essential for evaluating NDT strategies intended for metastatic risk disease.77–79 Moreover, CRC development is strongly influenced by the intestinal microbiota. Emerging mechanistic evidence indicates that Fusobacterium nucleatum can colonize colonic crypt niches and promote tumor associated programs. Therefore, the microbiome context in orthotopic models may influence ROS and ICD outputs as well as downstream immune remodeling differently from ectopic sites.80 Notably, F. nucleatum promotes chemoresistance in CRC through innate immune signaling and autophagy associated pathways. This finding provides a rationale to examine how NDT, particularly ROS and ICD based regimens, may be hindered by or may modulate biofilm like bacterial burdens in the colon.55,56 Taken together, CRC focused NDT studies should prioritize validation in orthotopic models and, where appropriate, metastatic models. This recommendation is particularly relevant for studies claiming TME reprogramming, including oxygenation, GSH depletion, lactate metabolic rewiring, and immune cold to hot conversion. In addition, site dependent immune and microbiome variables should be explicitly reported to strengthen translational predictability.56,68
Local Delivery of Drugs in NDT in CRC
The local drug delivery of CRC is a huge advantage in the treatment of CRC, as the natural accessibility of the rectal cavity makes local drug delivery no longer just a dose reduction strategy. At the same time, it can lock the energy trigger and reaction site of NDT at the engineering entrance of the adjacent space of the lesion, providing a structural basis for the high local effect/low systemic exposure treatment window.28,81 We can understand the specific delivery methods as follows: enema/suppository achieves intracavitary coverage, endoscopic injection achieves precise placement under the mucosa or around the tumor, and in situ depot upgrades short resident drugs to long resident material depots (Table 1).82 However, rectal mucus barrier and erosion (peristalsis, defecation, and secretion dilution) will lead to rapid loss of nano drugs. Therefore, material countermeasures often start from anti-erosion: forming a wall attachment library through ionic cross-linking/rapid gel, improving local retention by using injectable viscoelastic network, and adapting endoscopic injection and complex intracavity mechanical environment with shear thinning/self-healing characteristics.83–85 In addition, a current research focus is the integration of local material libraries with NDT triggering strategies. In this approach, catalytic sites and precursor substrates are first immobilized around rectal lesions using functional materials. These components may include H2O2 sources, metal active sites, and modules for GSH depletion or oxygen supply. Subsequently, exogenous energy inputs such as ultrasound, light, or radiotherapy, or endogenous chemical gradients including pH, GSH, and glucose, are used to activate ROS, 1O2, or ·OH generation. This strategy enables spatially selective amplification of reaction kinetics.28,86 For example, AceGel (0.4% sodium alginate+2% calcium lactate) developed by Kang et al can be used as an endoscopic submucosal injection water cushion material to instantly gel and maintain mucosal lifting, and has also verified a good cushion effect in the rectum of animals. Moreover, small-scale clinical studies show that the mucous membrane heals well in postoperative follow-up, without serious adverse events, providing a direct reference for the feasibility of “endoscopic injection - local reservoir” in the clinical process.28 Once loaded with NDT active units (such as MnO2, Fe/Cu based Fenton like catalytic sites, or acoustic/photosensitive components), this injectable local library that has been validated by endoscopic procedures can converge the reaction site from the system distribution to the submucosal/tumor microenvironment.86 An example closer to the experimental system of CRC is the multi enzyme like hydrogel (MELH) constructed by Zhou et al, which provides a drug bank locally with an injectable network, and improves the therapeutic effect of 5-FU through multi-functional mechanisms (including the regulation of antioxidant barriers such as glutathione in tumors). It reflects the local rewriting of microenvironmental factors related to chemotherapy tolerance in CRC models, suggesting that local bank building can sustain the substrate/catalyst/depletion process required for NDT rather than pulse it once.87 In addition, the injectable composite hydrogel AMPS reported by Wang et al integrates MnO2 nanoparticles (Fenton like CDT) with sound sensitive components, and produces 1O2 and ·OH equivalent reactants triggered by ultrasound, reflecting the programmable path of local reservoir fixed reaction unit - exogenous energy triggered dynamics. This paradigm is particularly suitable for coupling with clinically available energy input modes such as transperineal/transluminal ultrasound in the rectal cavity.86 On the other hand, suppository formulations have demonstrated the feasibility of intracavitary delivery with prolonged local residence and sustained release in animal intestinal tumor models. For example, a sustained H2 and 5-FU releasing suppository developed by Chen et al showed high therapeutic efficiency with low toxicity in colon tumor models. This system provides a translational reference for local rectal administration from a pharmaceutical perspective.88 In the dimension of energy triggering, Sang et al proposed a radiation activated photodynamic strategy using folate modified lipid polymer hybrid nanoplatforms loaded with vitriprofen. ROS generation was achieved under low-dose radiation therapy (such as a single dose of 4 Gy), and the precision of tissue relative less collateral damage was demonstrated in the in situ rectal tumor and lymph node progression model. This suggests that combining it with the local rectal material library may further compress the non target distribution radius of the nanoplatform.28 From the perspective of clinical accessibility, Gu et al reported local tumor necrosis and increased immune cell infiltration in patients with advanced CRC treated with colonoscopic PDT using hematoporphyrin and 630 nm optical fiber irradiation in a retrospective study. These findings suggest that intracavitary energy delivery combined with local therapeutic amplification has a practical clinical basis. Registered clinical studies involving colon route local 5-FU administration and thermosensitive gel based formulations further support the exploratory development of local material platforms within regulatory and clinical research pathways. These efforts provide a clearer translational direction for the clinical implementation of local rectal delivery strategies for NDT.81
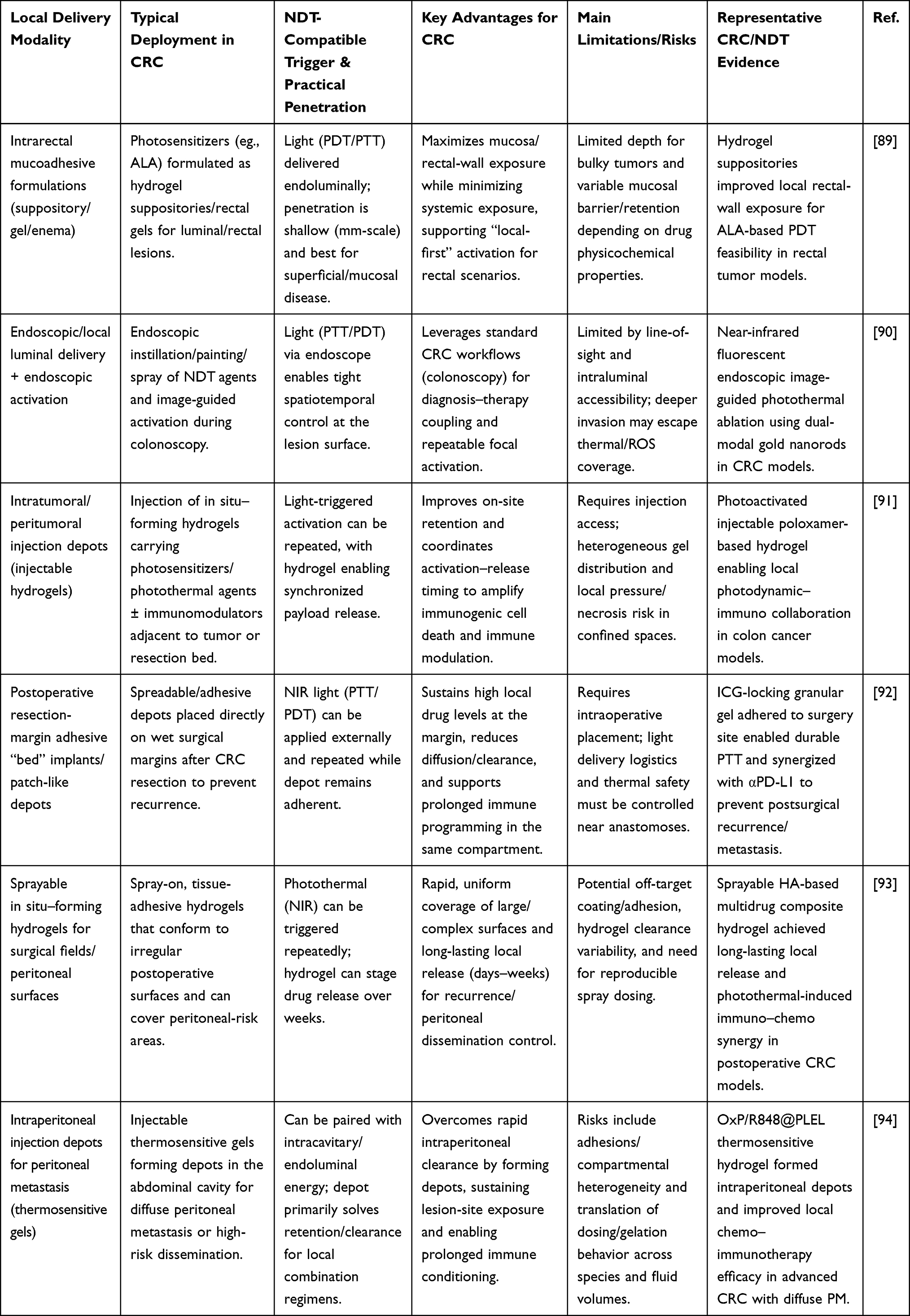 |
Table 1 Comparison of Local Delivery Strategies for CRC-Oriented NDT Platforms |
Application of Five Types of NDT in CRC
Although NDT has shown great potential in the treatment of CRC, the clinical efficacy of each NDT technique is still influenced by the tumor microenvironment, treatment mode, and nanoplatform characteristics. Different types of NDT, such as photodynamic therapy (PDT), sonodynamic therapy (SDT), chemodynamic therapy (CDT), etc., have different applications and effects in actual treatment due to their different mechanisms of action and indications (Figure 2).27,95 For example, PDT is mainly applicable to the surface or local area of tumors through the activation of specific photosensitizers, while SDT utilizes the deep penetration characteristics of ultrasound, especially suitable for tumors that are deep or difficult to reach.96 With the development of nanotechnology, these methods have also begun to integrate multiple treatment strategies, forming a new treatment model characterized by multimodal therapy, striving to provide more accurate and efficient solutions at different stages of cancer treatment.27 Therefore, this section will focus on discussing the specific applications of these five main NDT techniques in CRC, covering their design principles, preclinical and clinical research progress, and challenges faced, in order to better understand the advantages and limitations of each method in practical applications (Table 2).26
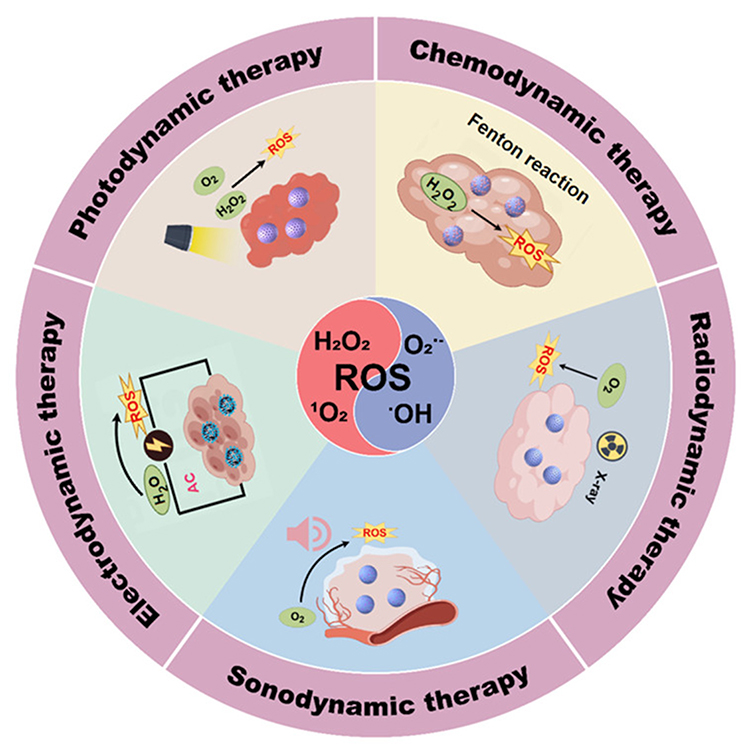 |
Figure 2 Application of five types of NDT in CRC. Schematic illustration of photodynamic, chemodynamic, radiodynamic, sonodynamic, and electrodynamic therapies, in which nanosensitizers are activated by distinct external or internal stimuli to generate reactive oxygen species (ROS) for tumor eradication. Adapted from Zhang, B., Huang, Y., and Huang, Y (2024). Advances in Nanodynamic Therapy for Cancer Treatment. Nanomaterials (Basel, Switzerland). Copyright © 2024 by authors.23 |
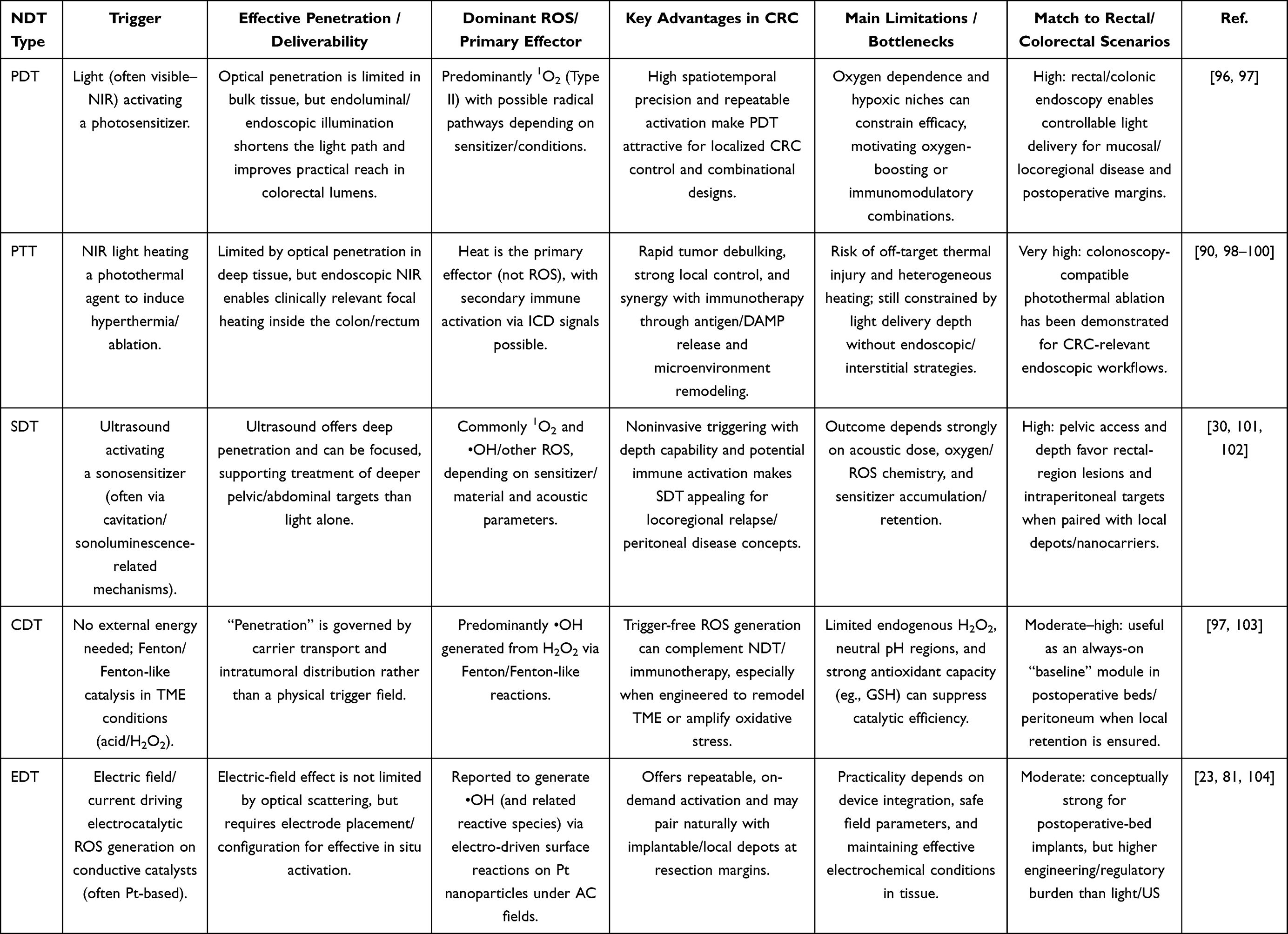 |
Table 2 Comparative Snapshot of Five NDT Modalities for CRC |
PDT for CRC Under The Advantage of Intracavity Illumination
The intracavitary radiogenicity of the rectum/distal colon gives PDT a natural advantage in temporal and spatial controllability within the framework of NDT, as optical fibers can be inserted through colonoscopy or intracavitary placement to precisely confine the light field to the tumor surface and infiltration front, thereby transforming the coupling of the three elements of light oxygen photosensitizer (PS) from an uncontrollable systemic process to an engineered local energy deposition process.81,104 At the mechanistic level, PDT induces cascade generation of ROS through PS light stimulation, and further induces direct damage to tumor cells, microvascular destruction, and release of immunogenic cell death signals. These effects can be manifested in clinical samples as increased infiltration of T cells, B cells, and macrophages in tumor tissue after treatment, suggesting its dual pathway potential of local ablation immune remodeling.105 The key value of nanoplatforms lies in integrating the enrichment, activation threshold, and imaging guidance of PS into the same material system. For example, the TCPP-Fe3+ metal organic framework (MOF) constructed by Li et al utilizes the CRC microenvironment H2S enrichment to trigger skeleton degradation, achieving a switch mode transition of TCPP from fluorescence/photosensitivity off to fluorescence/photosensitivity on, thereby supporting targeted PDT under real-time fluorescence imaging navigation and reducing the risk of non tumor phototoxicity.104 Another strategy that is closer to the transformation pathway is to stabilize and target PS that has been clinically applied or is close to clinical use: Khaled et al loaded the clinically relevant mTHPC liposome formulation Foslip, covered it with a silica shell, and coupled it with anti CEA Affimer to achieve CEA dependent uptake and phototoxicity of CRC cells such as LoVo/LS174T/HCT116. In the LS174T xenograft model, a single PDT can achieve about 4-fold tumor volume inhibition without significant organ toxicity, providing material level evidence for the precise scenario of “fluorescence tracing and intraoperative/intracavitary illumination”.106 Targeting CRC with a high proportion of “cold tumors” and limited immune therapy response, nano PDT can also complement the mechanism of immune checkpoint inhibition formation, as reported by Yuan et al mTHPC@VeC /T-RGD multifunctional nanoparticles mediate PDT under 660 nm laser, which can activate HIF-1 α and upregulate PD-L1 expression through PDT related hypoxia, making tumors more sensitive to PD-L1 therapy, thereby inhibiting primary and distant tumors and establishing immune memory, providing a clear dynamic explanatory framework for PDT to move from local controllability to systemic benefit107 In addition to carrier engineering, the structural design of PS molecules themselves can also serve the local irradiation window of the colon. For example, the novel chlorophyll derivative HCE6 synthesized by Chen et al showed low dark toxicity/high light toxicity in HT-29 and LoVo models, and could inhibit tumor proliferation and metastasis phenotype, suggesting that the molecular nano two routes can be used in parallel to optimize the therapeutic threshold under rectal irradiation conditions.108 The evidence for more rectal customization comes from Nguyen et al’s on photobleaching mediated charge convertible cyclodextrin nanoparticles: they first trigger charge conversion at 880 nm to promote cross cellular transport and deep penetration, and then initiate PDT/chemodynamic combination at 660 nm to achieve clearance of clinically relevant volume tumors in an in situ rectal tumor model, strengthening the combination logic of “local rectal illumination+nano penetration engineering”.109 At the clinical level, a retrospective analysis of stage III–IV CRC patients by Gu et al showed that intravenous injection of hemoglobin followed by 630 nm fiber segmented intracavitary irradiation (energy density of approximately 200 J/cm 2, continuous 3–4 days) can achieve high short-term remission and disease control rates, and prolong overall survival. At the same time, significant enrichment of local immune cells in the tumor after treatment and fewer serious adverse reactions were observed, directly proving the operability and safety boundary of intracavitary irradiation in the real world of CRC.109 However, some existing studies have shown that clinical evidence for CRC-PDT is still mainly based on small sample/case series, with significant differences in light dose and PS regimen (such as light dose spans of tens to hundreds of J/cm2). Therefore, a more convertible direction in the future is to use the rectal advantage of intracavity illumination as an entry point to incorporate imaging navigation, activatable switches, and immune synergistic mechanisms into nanomaterial design, and standardize light field dosimetry and local delivery processes in prospective trials to promote its entry into the evidence system of new adjuvant or organ preservation strategies.109,110
CDT: Transforming CRC into in situ Chemical Reactors
CDT is a treatment modality that significantly affects the TME of CRC and has a crucial impact on the prognosis and quality of life of patients. The core of CDT lies in its ability to convert readily available weak acids, H2O2, and metal ion metabolic abnormalities in the TME into programmable in situ free radical reactions, amplifying therapeutic effects through reaction kinetics rather than single drug occupancy.30,111 At present, research mainly focuses on Fenton/Fenton like catalysts, using metal sites such as Fe/Cu/Mn to catalyze the generation of ROS such as •OH from H2O2 under weak acid conditions. However, unlike strongly acidic lysosomes, the extracellular pH of CRC lesions is typically neutral to mildly acidic and usually ranges from pH 6.5 to 7.4.112 In addition, intracellular redox buffering systems such as GSH and GPX4 remain strong.113 Therefore, mechanistic claims regarding CDT should be supported by kinetic analyses conducted under physiologically relevant pH conditions rather than relying solely on assumptions of acidic activation.30 Accordingly, three major bottlenecks remain for the implementation of CDT in CRC. These include insufficient catalytic kinetics, insufficient substrate availability, and reductive quenching.114 We recommend that future CDT studies explicitly report pH dependent kinetic parameters, including apparent rate constants and Michaelis Menten constants when applicable. In addition, studies should include in situ ROS flux quantification and experimental validation under neutral to mildly acidic conditions that better reflect CRC physiology, such as pH 6.8 to 7.4 and approximately pH 6.5.30,115
From a quantitative perspective, CDT performance in CRC should be benchmarked using standardized assays and kinetic frameworks.116 Key metrics include pseudo first order or second order rate constants for H2O2 decomposition and •OH generation, expressed as k_app or k2 across pH values of 7.4, 7.0, and 6.5. These parameters should ideally be normalized by the accessible metal site content of the catalyst.30,117 Direct identification and flux measurement of ROS should be performed using EPR spin trapping methods, such as DMPO for •OH detection.118 These measurements should be complemented by fluorescent probes, including terephthalic acid for •OH detection and DCFH DA for total ROS, together with time resolved calibration. Redox quenching resistance should also be evaluated.119,120 Relevant indicators include GSH consumption kinetics measured using Ellman or DTNB assays, changes in GPX4 activity, and ROS persistence under physiologic thiol concentrations.121 In addition, in situ validation should be conducted in CRC models with controlled pH microenvironments. Suitable systems include buffered media, 3D spheroids, or orthotopic models.67,68 These approaches help confirm that catalytic flux remains sufficient under mildly acidic conditions. This kinetic reporting framework enhances mechanistic interpretability and strengthens translational confidence. It directly links catalyst design to predictable ROS flux outputs under clinically relevant conditions.122
For example, Cu site engineering can regulate peroxidase like activity and reaction channels through coordination environment: the three in one Cu PrIm nanoenzyme constructed by Dong Shuohui et al distorts the Cu-N4 active center to simulate the natural copper enzyme structure, achieving ROS catalysis, copper ion stable disturbance, and promoting HIF-1 α degradation in various CRC in vivo models, thereby simultaneously suppressing the biological roots of chemotherapy tolerance on the three axes of oxidative stress cuprotosis hypoxia signal.32 To address the clinical challenge of oxaliplatin resistance, Wan et al used an Fe MOF carrier to co deliver OXA and the NO precursor L Arg. In the high GSH tumor environment, the Fe sites undergo reduction and the framework gradually disintegrates, which triggers drug release. At the same time, the Fe2⁺ mediated H2O2 Fenton reaction enhances ROS generation. In addition, NO related signaling pathways are introduced to achieve multi pathway reversal of drug resistance. This strategy reflects an integrated material design concept involving metal site dynamics, gas signal regulation, and chemotherapy sensitization.31 To strengthen mechanistic alignment with CRC physiology, we add that Fe-based systems should demonstrate sustained ROS/catalytic flux under mild acidity and high thiol pressure by quantifying (a) Fe2⁺/Fe3⁺ cycling and H2O2 consumption rates at pH 7.4/6.8/6.5, and (b) whether NO-related modulation reduces redox quenching or improves effective ROS lifetime—metrics that are directly tied to resistance-reversal robustness. Further triple efficiency enhancement strategies typically follow a cascade logic of acidification substrate (H2O2) - GSH consumption as designed by Zhang et al ZIF-90@CDDP @ MnO2 @ HA utilizes MnO2 to consume GSH and release Mn2⁺ to perform CDT in the CRC model, while downregulating HIF-1 α through in situ oxygen production, inhibiting glycolysis (such as the HK2/GLUT1 related axis), and inducing mitochondrial damage by superimposing Zn2⁺, thereby coupling ROS generation and energy metabolism suppression into a reactor level synergy on the same nanoplatform69 In the dimension of “substrate supply”, GOx and other enzyme consuming enzymes are used to convert glucose into H2O2 accompanied by acidification, thereby pushing the Fenton window from passive dependence on TME to active manufacturing reaction conditions. Specially, Li et al’s dual targeting GOx@FeNPs In the CT26 CRC model, GSH consumption and ROS amplification were achieved, and the combination with α PD-L1 significantly enhanced DC maturation and CD8⁺ T cell infiltration, indicating that CDT/nanozyme can not only kill tumor cells, but also provide bottom-up energy for immune checkpoint therapy through ICD/ferroptosis related antigen release.123 Another pathway that synergizes with immunity is to use nanozyme to alleviate hypoxia and immune suppression, thereby improving the interpretability of NDT combination therapy. For example, Chen et al used a tumor cell membrane coated sonosensitizer iron oxide coupling system for CRC, relying on the catalysis and sonodynamics of iron oxides to generate ROS and interact with anti-PD-1, demonstrating a transferable framework of catalyzing ROS local inflammation immune amplification.124 For such multimodal systems, it is important to separately quantify the chemical CDT component and the energy triggered SDT contribution.125 For example, ROS flux should be measured under conditions with and without ultrasound at matched pH values. This approach helps validate the proposed mechanistic framework and guides the development of clinically reproducible activation protocols.25 In another direction that emphasizes stable delivery and translational feasibility of material platforms, some studies loaded CDDP onto a Cu MOF through copper coordination. In a high GSH environment, Cu2⁺ and the drug are released simultaneously, which suppresses stemness related tolerance in cancer cells.126 In addition, copper ion chemistry and chemotherapy induced stress are integrated at the immune level to achieve combined sensitization. These results suggest that MOF based platforms can integrate catalysis, drug delivery, and immune regulation within a unified design framework while maintaining manufacturability.126,127 The latest trend in reactor upgrades is to make multiple reaction units controllable interfaces. For example, Chen et al surface engineered copper peroxide nanodots onto PCN-224 porphyrin MOF and combined them with Au nanozyme to achieve more efficient translation and multimodal coordination of TME trigger signals in the CRC model. This further proves that CDT/nanozyme is not only a ROS attachment, but can be designed as a core catalytic module that determines reaction selectivity and treatment window.52 Overall, the clinical translational value of CDT/nanozyme in CRC is shifting from supplementing ROS to rephrasing hypoxia, drug resistance, and immune suppression encountered in radiotherapy/chemotherapy/immunotherapy as engineering reaction kinetics problems, which is precisely the most convincing material science landing point of NDT system.128,129
SDT: Deep Precision Killing Triggered by Ultrasound
SDT uses low-intensity ultrasound as an external energy source to activate sonosensitizers, inducing ROS generation under the combined action of cavitation/sonoluminescence and sonochemical effects, thereby achieving better penetration and non-invasive, focusing spatiotemporal control of deep tissues. This gives SDT a more reachable energy advantage compared to PDT in CRC, and it is also the most suitable triggering mode for integration with clinical ultrasound equipment in the NDT system.95 Due to the widespread hypoxia and high GSH scavenging free radicals in CRC TME, the ROS flux of SDT alone is easily limited, thereby reducing the damage to CRC. Therefore, in recent years, basic research has tended to use nanomaterials to integrate sound sensing units, catalytic units, and TME regulatory units into a sound triggered original amplification reaction chain, and has shown many promising application opportunities. For example, Chen et al covalently or physically adsorbed Ce6 onto Fe3O4 nanoparticles. They further constructed MBFCs by coating the nanoparticles with CT26 tumor cell membranes. This design enabled homologous tumor targeting and the synergistic integration of Fe3O4 mediated Fenton like catalysis CDT with Ce6 induced ROS generation in SDT. This system significantly increased ROS levels, induced apoptosis, and inhibited tumor growth in CT26 cells and tumor bearing mice. These results demonstrate that combining material site engineering with biomimetic targeting can expand the effective dose window of SDT.124 To further address hypoxia dependence, Guo et al constructed a platelet membrane coated with C-TiO2 hollow nano shell (C-TiO2)/ AIPH@PM) TiO2 is used as the sound sensitive core, AIPH as the oxygen independent alkyl radical generator, and platelet membrane is used to prolong circulation and enhance tumor homing. AIPH decomposition releases N2, which can reduce cavitation threshold and improve acoustic field penetration/deposition efficiency, thereby achieving more thorough tumor clearance and good biosafety under both normoxic and hypoxic conditions. The key material strategy for CRC-SDT is emphasized as oxygen independent radical.130 In addition, in the direction of reaction cascade, Zhang et al proposed a biomimetic cascade nanoreactor (Pt nanozyme doped hollow polydopamine, tumor cell membrane coated and co loaded with Ce6 and chloroquine CQ), which enhances ROS generation through Pt nanoenzyme catalysis, while blocking autophagy clearance pathways with CQ, so that ultrasound triggered oxidative strikes are no longer recovered by cell stress. In a CRC model, multi omics suggests that apoptosis/ferroptosis related pathways are jointly activated, improving the reproducible efficacy of SDT from both the dynamic amplification and tolerance mechanism disassembly ends.131 Another type of material route that is closer to the local reachable scene of the rectum is the local library and acoustic triggering. Specifically, Wang et al constructed injectable AMPS hydrogel with alginate as the skeleton, in-situ gelled under the effect of Ca2+in the tumor microenvironment, and simultaneously loaded MnO2 (Fenton like CDT), organic sound sensitive polymer, and anti-metastasis drug SIS 3, to achieve SDT+CDT synergy and significantly inhibit the growth of subcutaneous tumors in mice, while achieving near complete inhibition of lung/liver metastasis, suggesting that fixed reaction sites in the material library can translate sound field triggering into more lasting local response flux.86 Furthermore, Zhao et al utilized pre drug micelles connected by diselenide bonds and introduced Pt nanozyme cascade enzyme like activity (such as SOD-CAT/SOD-POD) to alleviate hypoxia, enhance sonogenic ROS production, and achieve the reduction response release of Ce6 and paclitaxel in tumors, thereby improving the synergistic efficiency of “sonotherapy” for colon cancer in vitro and in vivo. This indicates that nanozyme can not only replenish ROS, but also systematically improve the therapeutic window of SDT through oxygen regulation and reaction selective engineering.132 From the current research perspective, the advantage of SDT lies not only in its deeper penetration, but also in its ability to naturally couple with clinical routine ultrasound imaging/localization and its low-cost, repeatable irradiation characteristics. The tumor homing, hypoxia/antioxidant barrier breaking, and immunogenic death amplification provided by the nano platform make it more likely to form an interpretable joint sensitization strategy with radiotherapy or immunotherapy, and approach the clinical goal of preserving CRC organs and improving local control rates.133,134 Given biological variability, we suggest that “hypoxia relief” claims in SDT-enhancement studies be supported by direct pO2 measurements and hypoxia-marker profiling before/after treatment, and that validation in orthotopic colorectal tumor models be prioritized to reflect clinically relevant vascular and perfusion features.65,66
RDT: Standard Radiotherapy Process Level Fusion Point for CRC
RDT can be seen as a secondary amplification of radiation energy onto a nanoplatform, transitioning to ROS/free radical chemistry. By utilizing the accessibility of X-rays in deep tissues, RDT converts local ionizing radiation in tumors into more controllable and high-density oxidative stress, providing a clinical entry point for nanodynamic gain in CRC, an already highly radiation dependent disease spectrum.135,136 RDT nanoplatforms typically enhance energy deposition through high-Z components, achieve energy transfer through organic/inorganic radiation response modules, and amplify ROS generation such as • OH/1O2 in the tumor microenvironment to complement the chemical killing deficiencies of conventional radiotherapy under hypoxia, sublethal repair, and dose limitation.137 Taking the work that directly corresponds to the cytological evidence of CRC as an example, Sang et al constructed folate targeted lipid polymer hybrid nanoparticles (FA-LPNPs-VP-5-FU) composed entirely of FDA approved ingredients. Under a clinically relevant dose of 4 Gy X ray irradiation, verteporfin triggered a burst of ROS. This ROS increase induced apoptosis and necrosis in HCT116 cells and caused cell cycle arrest at the G2/M and S phases. These findings reflect a chemodynamic enhancement effect within the radiation dose window.29 Furthermore, Rui Sang et al’s RA-PDT (radiation activated PDT) reported in eBioMedicine has advanced similar nanoplatforms to the in vivo scenario of locally advanced rectal cancer (LARC) with lymph node positive progression: a single 4 Gy division can activate VP and generate sufficient ROS, significantly inhibiting the growth of primary lesions in both local and subcutaneous models, while suppressing lymph node tumor progression with minimal involvement of surrounding tissues. This directly echoes the clinical demand for precise sensitization rather than simple dose escalation.28 This low segmentation trigger local high ROS tissue selective protection RDT logic has natural clinical alignment potential with the current guided practice of dose segmentation, treatment window, and organ preservation strategy in CRC radiotherapy: using nano RDT as a chemical gain module in conventional radiotherapy or TNT treatment sequences to increase effective biological dose and tumor control probability without changing the irradiation geometry.135,138 At the material level, clinically convertible sensitization designs are also moving from single high-Z to structurally engineered composite energy converters, such as Du et al through engineering Hf0.7Ti0.3O2@PEG Nanoparticles achieve enhanced radiotherapy response, emphasizing the use of material composition and surface engineering to obtain stronger tumor radiotherapy sensitization and better in vivo adaptability, providing a representative model for the manufacturability administration controllable toxicity route of rectal cancer radiotherapy sensitization materials.139 The common trend of nano radiation dynamics/nano sensitization for radiotherapy is to couple oxidative chemistry with microenvironmental regulation (such as oxygen supply/hypoxia relief, inhibition of antioxidant systems, or parallel with cell cycle regulation) to maintain the reaction kinetics advantage of ROS generation in real TME and reduce dependence on high-dose single irradiation, in response to the hypoxia immunosuppression bottleneck during radiotherapy.137 At the same time, the key pivot of RDT in pushing local radiotherapy towards systemic therapy lies in immunological amplification: stronger ROS and cell damage can enhance immunogenic cell death and antigen release, thereby providing higher quality in situ vaccine substrates for combined immune checkpoint inhibitors and theoretically increasing the probability of distant effects.137,140 It is worth noting that TNT strategies in rectal cancer are rapidly evolving. Increasing clinical evidence supports the integration of radiotherapy, chemotherapy, and immunotherapy. For example, Spring-01 evaluates the TNT regimen of short course radiotherapy (5 × 5 Gy) in locally advanced CRC and reports a higher pathological complete response rate signal in combination with cetuximab and CAPOX. This treatment framework provides a clear transformation path for embedding RDT nanoplatforms into segmented radiotherapy and immune combination timing in the future, from local sensitization to overall benefit.138,141 Because radiotherapy-relevant oxygen effects are highly context-dependent, studies proposing oxygen supplementation/hypoxia relief in RDT should include quantitative oxygen-tension readouts (pO2), hypoxia-marker modulation, and preferably spatial oxygen mapping, with emphasis on orthotopic rectal/colonic models for realistic vascular microarchitecture.65,142
EDT: A New Approach with Therapeutic Potential
EDT, as a new branch of NDT that deserves attention in recent years, focuses on converting programmable electric fields into in situ active species generation within tumors: electrode induced electrolysis products (especially chlorine containing active species) are reactivated on the surface of nanocatalysts, thereby amplifying oxidative stress and triggering tumor cell death without relying heavily on oxygen supply.97 At the mechanistic level, Lu et al pointed out from the perspective of heterogeneous catalysis that EDT is not simply electric field directly cracking water, but more likely to involve free chlorine/HOCl generated by electrolysis in key reactions, and undergo catalytic activation on the surface of Pt nanoparticles, producing strong oxidizing species such as superoxide anions.143 At the same time, it is accompanied by detectable processes such as Pt surface reactions/corrosion, providing an operable reactant site kinetics framework for subsequent material site engineering. Based on the idea of in-situ enrichment of reaction substrates, Chen et al utilized Pt Cu alloy nanoparticles to regulate the electronic structure through alloying and superimpose chloride ion transporters (CIT) to achieve intracellular Cl⁻ elevation, thereby significantly enhancing the generation of electrically driven ROS. At the same time, the Fenton like reactions mediated by Cu and Fe sites together with GSH consumption were utilized to enhance catalytic activity. This design established a multi pathway coupling strategy involving electrically driven ROS generation, •OH reinforcement, and release of antioxidant barriers. As a result, stronger antitumor effects were observed both in vitro and in vivo.144 Similarly, other researchers have utilized KCL-CaCO3 nanoclusters coated with Pt nanocrystals (KCCP) to integrate the “ion pool” with the electrocatalytic site: the release of Cl⁻ within tumor cells promotes the generation of Pt driven ROS, while Ca2 ⁺ overload and ROS form a self-amplifying cycle, resulting in higher levels of oxidative damage and deeper tumor inhibition under the same electrical stimulation.145 In addition, to address practical barriers such as high expression of GSH and fluctuations in acidic/peroxide substrates in the tumor microenvironment, Chen et al further integrated the logic of EDT and CDT nanoenzymes using Fe3O4@Pt. Pt is responsible for electrically driving ROS, while Fe sites participate in the Fenton reaction under acidic conditions and rapidly deplete GSH through the Fe3⁺/Fe2⁺ cycle, thereby reducing ROS clearance, improving overall reaction flux, and therapeutic window (Figure 3).62 However, the current mainstream validation of EDT nanomaterials still relies on models such as subcutaneous transplant tumors, and there is still limited systematic evidence in colorectal/rectal in situ models. However, the electrode accessibility within the rectal cavity is rapidly filling this transformation chain: endoscopic calcium electroporation has been completed for Phase I clinical studies of CRC, demonstrating that the intracavitary electric field can act on tumor tissue in a controllable manner and has a feasible safety profile.146 Furthermore, calcium electroporation has been explored as a potential neoadjuvant strategy for patients with curable CRC. This approach indicates that combining a local electric field with local material or substrate delivery may support clinical strategies aimed at organ preservation and treatment downstaging.147 The series of cases of palliative treatment for CRC with intracavitary calcium electroporation from the UK also demonstrates the feasibility of this type of intracavitary electrical therapy in late stage complex lesions from a real-world perspective, providing a clinical entry point for future grafting of local material libraries (such as EDT electrocatalytic nano platforms)+electric field triggering to local rectal treatment.148 At the same time, electroporation/electrochemical reactions can cause controllable pH and electrolytic microenvironment changes around the electrode, and have been shown to affect the state of immune cells (such as promoting macrophage activation towards a more anti-tumor phenotype), providing a verifiable biological lever for EDT to further form a local trigger immune amplification combination logic with immune checkpoint and other systemic therapies.149 In more engineering oriented electrochemical tumor therapy research, designs such as external anode/multi cathode arrays have been used to expand the effective reaction volume and pursue more thorough pathological reactions. This also suggests that in the future, if the electrode devices in the rectal cavity are optimized in conjunction with EDT nanocatalysts, the electric field may be upgraded from a simple energy input to a programmable reaction field, thereby promoting EDT from a conceptual new therapy to a more translational strategy that is closer to the clinical context of CRC.150
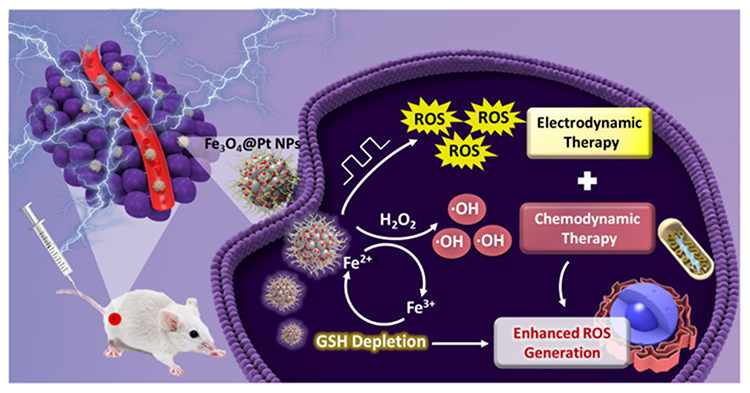 |
Figure 3 Schematic illustration of Fe3O4@Pt NPs for synergistic electrodynamic/chemodynamic tumor therapy with GSH depletion. The red dot on the mouse indicates the tumor site (intratumoral injection location) where Fe3O4@Pt NPs are administered. The lightning/electric field symbol represents electrodynamic therapy that promotes ROS production, while chemodynamic therapy is mediated by the Fe2⁺/Fe3⁺ redox cycle converting endogenous H2O2 into •OH via Fenton/Fenton-like reactions. “ROS” denotes reactive oxygen species and “•OH” denotes hydroxyl radicals. GSH depletion indicates the consumption of intracellular glutathione, which weakens antioxidant defenses and further enhances ROS accumulation for tumor killing. Adapted from Chen T, Chu Q, Li M, Han G, Li X. Fe3O4@Pt nanoparticles to enable combinational electrodynamic/chemodynamic therapy. J Nanobiotechnology. Copyright © 2021 by authors.62 |
To translate intracavitary activation strategies based on light, ultrasound, and electric fields into clinically executable rectal cancer workflows, patient specific dosimetric standardization is required. Such frameworks should explicitly model pelvic tissue heterogeneity, mucosal geometry, and organ level energy absorption rather than assuming homogeneous fields.151 For intracavitary or endoluminal PDT, established dosimetry principles indicate that treatment effects depend on geometry, tissue optical properties, photosensitizer distribution, and tissue oxygenation. Therefore, rectal implementations should combine applicator position tracking with optical property aware light transport calculations. This strategy helps prevent excessive local irradiation and insufficient dosing along curved mucosal surfaces.21,152 Clinical CRC and rectal PDT studies have historically shown large variation in light dose, irradiation methods, and sensitizer protocols. Therefore, standardized reporting is essential. Key parameters should include mucosal irradiance or fluence, exposure geometry, and oxygen related treatment dependence. Such standardization is critical for cross center reproducibility and for aligning NDT activation strategies with pelvic anatomy.152 For ultrasound triggered NDT and SDT, engineering feasibility improves when treatment centers adopt standardized parameter reporting and dosimetry guidelines. Important parameters include frequency, duty cycle, pressure or intensity, focal volume, and calibration methodology. These parameters should be integrated with acoustic modeling that accounts for pelvic anatomical structures. Such modeling helps address variations in attenuation and reflection across the bowel wall, mesorectum, and surrounding tissues.152,153 Electric field activation faces a similar challenge. Therapeutic thresholds depend on the spatial distribution of electric fields within heterogeneous tissues. Therefore, treatment planning should incorporate field mapping and monitoring approaches. These methods should account for nonlinear tissue changes during electroporation as well as the proximity of critical pelvic structures.154,155 Finally, pelvic anatomy is intrinsically heterogeneous and differs substantially from homogeneous phantom models in terms of absorption and attenuation. Therefore, heterogeneity aware quality assurance strategies derived from pelvic dosimetry should be incorporated into NDT trial SOPs. These approaches are particularly valuable when combined with image guidance and post treatment dose or field reconstruction.156
Synergistic Therapy in NDT to Enhance Immunotherapy in CRC
Although different types of NDT have their own advantages in the treatment of CRC, such as achieving locally efficient production of ROS, inducing tumor cell death, and reshaping the tumor microenvironment to some extent through light/sound/catalysis triggering, from a clinical decision-making perspective, a single NDT strategy is often difficult to simultaneously cover the highly heterogeneous biological characteristics and complex immunosuppressive network of CRC, and its efficacy is still limited by multiple bottlenecks such as tumor hypoxia, immune “cold” state, drug exposure spatiotemporal mismatch, and recurrence and metastasis risk.157,158 Therefore, it is still difficult to become the preferred monotherapy for clinical treatment. In contrast, the accumulated basic and translational research in recent years has shown that embedding NDT as a programmable local activation module into combination therapy systems can achieve tumor burden reduction and immune activation at a precise and controllable tissue scale, and further complement and cooperate with immune checkpoint blockade, innate immune agonists, metabolic/microenvironment regulation, or local delivery systems, thereby demonstrating more clinically significant potential in inhibiting recurrence, expanding systemic benefits, and prolonging the duration of therapeutic efficacy.158–160 When multimodal systems simultaneously integrate PDT, CDT, and immunotherapy, quantitative evaluation of synergistic effects should be included in the discussion. Such analysis helps distinguish true synergistic amplification from simple additive effects and improves the reproducibility and translational relevance of the conclusions.161,162 Because synergy definitions are model dependent, it is recommended to report synergy scores from multiple reference models. These may include Bliss, Loewe, HSA, and ZIP frameworks, together with visualization of synergy landscapes. For example, SynergyFinder can be used to standardize and visualize multidose combination data. This approach helps identify synergistic intervals within clinically feasible dose ranges rather than relying on apparent synergy observed only at extreme doses.163 For engineered platforms activated by light, sound, or electric fields, pharmacological frameworks such as MuSyC can further decompose synergy into efficacy and potency components. This analysis helps determine whether a combination increases maximal therapeutic efficacy or primarily reduces the effective dose. The latter scenario may support toxicity reduction and optimization of activation parameters. Such evaluation provides a more practical basis for clinical SOP development and cross center consistency.164 Based on these trends, this section focuses on the design logic and key evidence supporting NDT based synergistic therapies. It discusses how mechanism complementarity and optimization of timing and delivery engineering can transform local dynamic therapy into scalable antitumor immune responses. These strategies may provide promising treatment options for CRC, particularly for tumors with an immune cold phenotype.
NDT as an in situ Tumor Vaccine: ICD-Driven Antigen Cascade
The core synergistic logic of coupling NDT with immunotherapy in the “cold tumor” immune ecosystem of CRC is to reshape local tumor cell death from simple tumor reduction to an in situ vaccine process that can be read by the host immune system. Among them, NDT first produces measurable immunogenic cell death (ICD) signals, and then amplifies these signals into treatable immune activation and systemic anti-tumor memory through nanoadjuvants and microenvironment engineering.165,166 For example, built by Wan et al TIR@siRNA (TAT-IR780 self-assembled nanoparticles loaded with Nrf2 siRNA, particle size<60 nm) achieved sonosensitizer nuclear localization and inhibited Nrf2 mediated ROS clearance through TAT, transforming ultrasound triggered SDT from transient oxidative stress to accumulative lethal oxidative stress, and stronger tumor suppression and immune related changes were observed in the CT26 CRC model More importantly, this work has written ICD as a verifiable chain: at the cellular and tumor tissue levels, it reports a significant increase in ROS under ultrasound, activation of DNA damage and mitochondrial apoptosis pathways, and the appearance of ICD related phenotypes accompanied by increased DC recruitment and T cell infiltration. Ultimately, it synergizes with DPPA-1 peptide anti-PD-L1 to inhibit primary lesions and suppress intestinal metastases, reflecting a logical loop from in situ vaccination to checkpoint release.167 In a representative electrical NDT study, Chen et al constructed Pt-loaded with glutamine antagonist 6-diazo-5-oxo-L-nurleucine (DON) starting from the production of highly toxic ·OH by EDT Pd@DON Nanocarriers are designed to advance an EDT from short-term killing to long-term tumor suppression in the context of immune suppression, with a focus on the risk of tumor recurrence and metastasis.168 This work explicitly juxtaposes ROS mediated ICD and DON promoted CD8+T cell infiltration as a synergistic axis to achieve more robust systemic anti-tumor immune output in primary and metastatic models, emphasizing that metabolic intervention can serve as an ICD backend amplifier to enhance the immune transformation efficiency of EDT.168 More importantly, electric NDT should be regarded as a reliable in situ vaccine, not only by observing the ICD phenotype, but also by using a traceable causal chain to connect electrically triggered ·OH with immune initiation (such as establishing consistency through the generation of ·OH under electrically triggered conditions and changes in immune response), thus avoiding the explanatory bias of difficult to distinguish between cytotoxicity and immune contribution solely based on endpoint tumor suppression.16,168
Positioning NDT as an in situ tumor vaccine is most convincing when its local cytotoxicity is mechanistically linked to canonical ICD signaling. Key signals include ecto calreticulin exposure, extracellular ATP release, and HMGB1 release or translocation. These events enable dendritic cell cross priming and support durable T cell immunity.169,170 In CRC relevant NDT systems, ROS driven ER stress and membrane damage can initiate an antigen cascade. Tumor cell killing generates a synchronized release of tumor associated antigens together with DAMP signals. These signals promote DC maturation and antigen presentation rather than allowing antigen release to remain immunologically silent.169 The strongest immunological evidence arises from studies that quantify ICD biomarkers and functionally connect them with DC maturation and T cell priming. For example, photodynamic ER stress models in the CT26 colon carcinoma system have shown that CRT exposure and ATP secretion directly promote DC activation and a prophylactic vaccination effect.171 In this study, mice immunized with PDT treated CT26 cells were protected against subsequent live tumor rechallenge. This result directly demonstrated the presence of immune memory rather than transient inflammatory responses.171 More recent CRC oriented nanodynamic platforms have begun to report quantitative DAMP readouts together with DC maturation analysis. For example, a zirconium coordinated nanosonosensitizer for CRC increased CRT membrane translocation with MFI quantification, promoted HMGB1 release detected by imaging and quantification, and altered ATP levels. Conditioned medium from treated cells also induced BMDC maturation measured as CD11c⁺CD80⁺ and CD86⁺ populations by flow cytometry under defined ultrasound parameters. This experimental sequence more closely reflects the mechanistic requirements of in situ tumor vaccination.172 Conceptually similar PDT centered studies emphasize that ICD competence is not guaranteed by ROS generation alone. Therefore, ICD induction should be evaluated using standardized biomarker panels and functional assays. Different photosensitizer localizations and cellular stress programs can produce distinct immunogenic outputs even when the extent of tumor killing appears comparable.173 When antigen specific T cell activation is examined, cross presentation and antigen specific assays should be included together with DC maturation measurements. Examples include IFN γ ELISPOT, tetramer staining, and defined antigen models. These approaches ensure that CRT, ATP, and HMGB1 measurements are mechanistically linked to adaptive immune responses rather than remaining correlative observations.174,175 From a translational perspective, the sequential pathway linking ICD induction, DC activation, T cell priming, and immune memory suggests specific correlative endpoints for CRC NDT clinical trials. These may include peri treatment biopsies or organoid based assays that quantify CRT, HMGB1, and ATP related DAMP signatures together with DC activation markers and T cell clonality or expansion. Longitudinal monitoring of immune memory may also provide patient level evidence analogous to tumor rechallenge experiments. Such approaches are particularly relevant for MSS CRC, where insufficient.28,176
At the level of adjuvant engineering, what we hope to achieve is to amplify ICD from weak signals to immune activation. Often, instead of continuing to pile up ROS, we use nano platforms to decouple danger signals from innate immune switches/microenvironmental resistance, thereby increasing effective DC uptake and reducing immune suppression thresholds.145,165,177 For example, as an immunosuppressive axis releasing adjuvant, Huang et al prepared a nano drug NCG co loaded with a sound sensitive agent Ce6 and a TGF - β receptor inhibitor galunisterib. Under ultrasound, Ce6 produced ROS to induce ICD and release immune stimulation signals such as CRT/HMGB1, while the acidic microenvironment triggered Gal release to inhibit Smad2/3 signaling, thereby inhibiting MDSC differentiation, promoting TAM polarization towards M1, and weakening the tumor associated fibroblast barrier. This significantly improved effector T cell infiltration and enhanced the efficacy of anti-PD-L1 in CRC liver metastasis models. Essentially, this is the same nano prescription for ICD antigen production and relieving TGF-β-mediated immune rejection.165 On the other hand, the innate immune switch amplifying adjuvant is also an important component. For example, Liu et al assembled a supramolecular nanocarrier HCCSM using hyaluronic acid cyclodextrin as the host guest assembly, and co delivered the chemotherapy prodrug CPT with the STING agonist MSA-2 for in situ vaccination of CRC. The key point is to synchronize the tumor antigen released by cell death with the STING signal in time and space, thereby increasing the probability of triggering DC maturation and T cell initiation, and upgrading the death signal to a programmable vaccine adjuvant signal.177 In addition, in the impact study, researchers constructed the albumin nano delivery system FA-ICG& MnOx@HSA The co loading of ICG and MnOx aims to amplify anti-tumor immune responses by combining acoustic triggered ROS/sonodynamic effects with Mn related innate immune enhancement (accompanied by microenvironmental response behavior), providing a convertible design template for nanomedicine with sonodynamic+STING axis gain.134 Furthermore, Zhang et al proposed the biodegradable platform MMCH (MnOx@MIL-100 @ CDDP@HA) TME acid/GSH triggers the release of CDDP, Fe2⁺, and Mn2⁺. On the one hand, GSH consumption and · OH generation promote iron death and induce ICD. On the other hand, nuclear DNA and mitochondrial DNA damage drive the cGAS STING pathway. Mn2⁺ can increase the sensitivity of cGAS to dsDNA, achieve the synergy of the three pathways of ICD (adaptive immunity)+cGAS STING (innate immunity), and report persistent immune memory and recurrence inhibition.178 At the same time, the IrTe-x-Mn nano acoustic sensing system reported by Wu et al coupled Mn as an immune adjuvant/signal amplifier with acoustic sensing catalysis, and demonstrated the improvement path of nano adjuvant on the efficiency of in situ vaccines through a chain logic from material composition to ICD and then to tumor vaccination system immunity.179 We need to point out that in the precision treatment of CRC, the clinical significance of such in situ vaccine strategies lies in the fact that the vast majority of microsatellite stabilized (MSS) CRC is insensitive to PD-1/PD-L1 monotherapy. The goal of NDT-ICD and adjuvant engineering is to transform locally controllable energy deposition into a systemically amplified immune response, thereby creating a responsive immune background noise for immune checkpoint inhibitors and promoting our clinical treatment.165,167
Finally, in addition to ROS type ICD, material induced pyroptosis/inflammatory cell death can also serve as a strong adjuvant pathway for ICD. Specifically, Wang et al DOX@Zr-MOF Triggering caspase-3/GSDME dependent pyroptosis and reprogramming the immunosuppressive microenvironment significantly enhanced efficacy in the CT26 colon cancer model when combined with anti-PD-1 This suggests that we can consider dynamic ROS in the field and endogenous inflammatory death in the material as two convertible pathways for in situ vaccination of NDT.70 Electric fields/currents have the advantages of tissue penetration and spatial controllability, making the combination of locally accessible electrical stimulation with nano EDT materials and immune adjuvant modules theoretically easier to embed in neoadjuvant or local enhancement strategies. However, their clinical application still needs to establish stricter translational evidence around the safety window of electrical parameters, in vivo disposal and systemic toxicity of platinum/manganese based materials, and the repeatability of the kill ICD adjuvant T cell effect chain in the human immune suppressive microenvironment.16,134
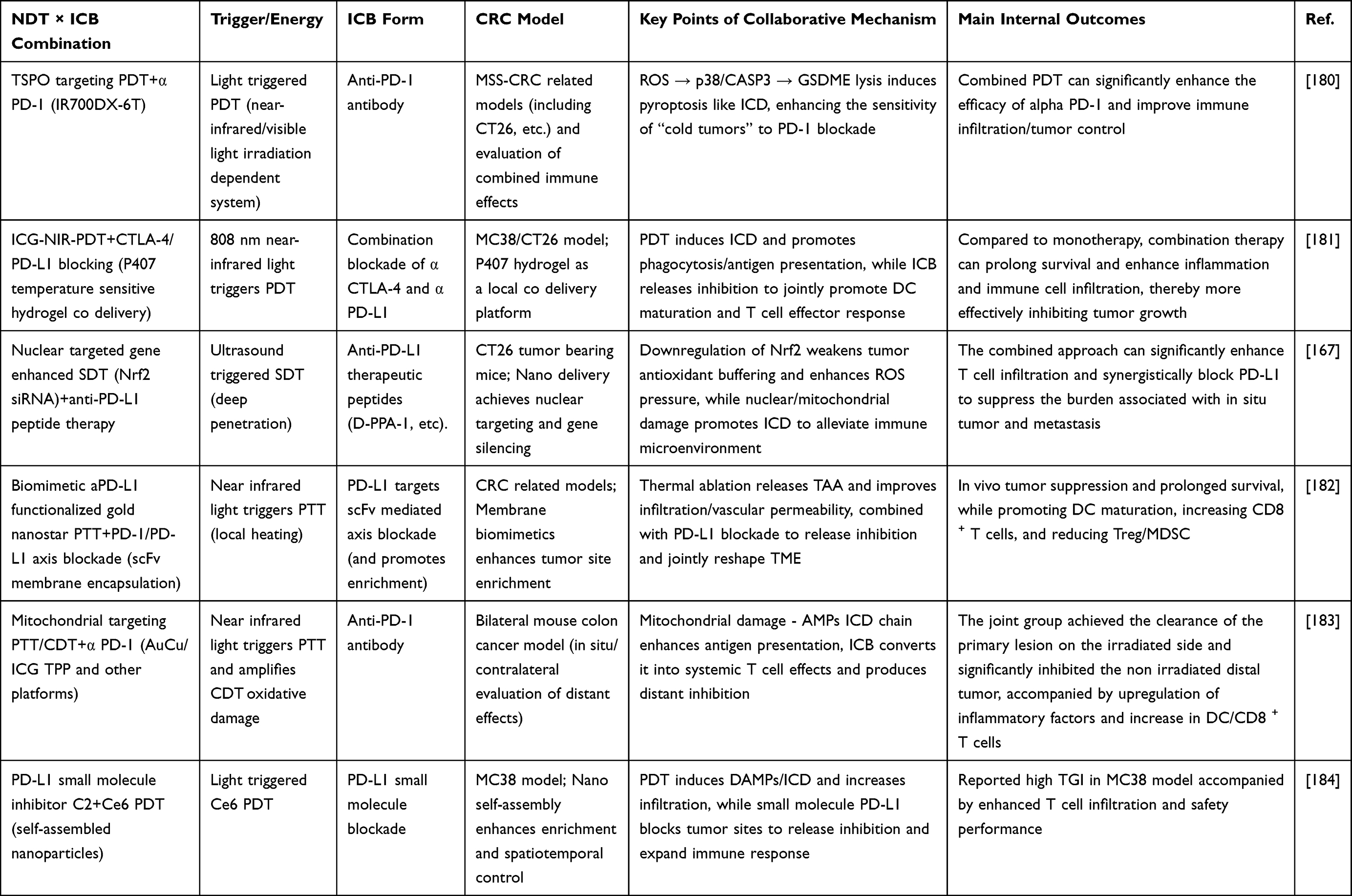 |
Table 3 Synergistic Integration of NDT with Immune Checkpoint Blockade for CRC |
NDT Collaborative Immune Checkpoint Blockade: Turning CRC from Cold to Hot
At present, in the actual clinical treatment of CRC, the long tail benefits brought by immune checkpoint inhibitors (ICIs) are mainly concentrated in the MSI-H/dMMR population, and the overall efficacy for MSS patients, who account for the vast majority, is still limited. Therefore, there is an urgent need for a controllable, locally triggered, and systematically reshaped immune pretreatment method to push “cold tumors” towards “hot tumors” (Table 3).159,185 Previous studies, represented by negative results such as IMblaze370, may suggest that in the absence of effective antigen release and T cell recruitment, it is often difficult to cross the primary tolerance threshold of tumors solely by relieving PD-1/PD-L1 axis inhibition.186,187 From the perspective of traditional systems engineering, NDT, Some methods that focus on precise delivery and controlled triggering of local dynamic therapies driven by ROS such as PDT/SDT using nano platforms are naturally suitable as synergistic treatment methods for ICI. Because ROS mediated local cell death and tissue stress can form an in situ vaccine effect in tumors, creating an entry point for subsequent T cell clone expansion and infiltration through antigen release and inflammation cascade. In addition, NDT has spatiotemporal programmability (light/sound triggering, dose segmentation), making the engineering trade-off between immune activation and toxicity more controllable, especially suitable for treatment scenarios that are locally accessible to the rectum.107 Typical examples from Yuan et al’s construction mTHPC@VeC /T-RGD multifunctional nanoparticles mediate PDT. PDT not only inhibits the primary lesion, but also induces systemic immune response and suppresses distant tumors. PD-L1 blockade further amplifies this effect and forms immune memory, thereby transforming local killing into systemic immune control. More importantly, this study reveals why NDT is suitable as an immune pretreatment for ICI in mechanism: the hypoxic stress caused by PDT can upregulate tumor PD-L1 through HIF-1 α, forming an adaptive immune escape induced by dynamic therapy. Introducing PD-L1 blockade during this window period can translate the original tolerance response into a therapeutic target that can be utilized by drugs, thereby achieving a closed-loop synergy from thermalization to amplification.107 Similarly, in the sound triggered path, Wan et al designed TIR@siRNA Realizing IR780 (sonosensitizer) nuclear localization and Nrf2 siRNA cytoplasmic delivery, utilizing gene enhanced nuclear targeted SDT to regulate redox balance and alleviate the immunosuppressive microenvironment, thereby significantly enhancing the therapeutic effect of DPPA-1 peptide based anti-PD-L1 therapy. In the CT26 model, not only the primary tumor is cleared, but also intestinal metastasis is inhibited and accompanied by enhanced T cell infiltration, reflecting the material immune synergistic logic of first igniting antigen/inflammation and then relieving checkpoint inhibition.167 Furthermore, in response to the key bottleneck of the lack of strong inflammatory cell death signals in the MSS context, Cao et al reported that mitochondrial targeted PDT can trigger GSDME mediated pyroptosis and enhance the efficacy of anti-PD-1 antibodies in microsatellite stable CRC, suggesting that a more immunostimulatory form of cell death (compared to simple apoptosis) may be more effective in enhancing antigen presentation and the probability of effector T cells entering the tumor, thereby providing a higher quality initiating signal for the “cold to hot” transition.180
Recently, more conversion-oriented material schemes have begun to nanoize and antibody free the blockade itself. For example, the chimeric peptide engineered photodynamic PD-L1 degradation agent NPPM (PpIX-PD-L1 targeting peptide CVRARTR forms an amphiphilic skeleton and is loaded with macitentan) developed by Wei et al Under light irradiation, it not only triggers ICD but also achieves PD-L1 photodynamic degradation in tumor cells. At the same time, macitentan synergistically reduces the expression of PD L1 in extracellular vesicles. This effect leads to increased T cell infiltration and a reduction in Treg populations. As a result, both primary tumors and metastatic lesions are effectively suppressed. These findings highlight the potential to simultaneously disrupt PD L1 mediated immune suppression at the cell membrane and extracellular vesicle levels through materials based strategies.188 Similarly, Zhang et al self-assembled small molecule PD-L1 inhibitor C2 and photosensitizer Ce6 into C2-Ce6 nanoparticles, achieving up to 94.7% tumor growth inhibition in the MC38 model, accompanied by increased T cell infiltration and enhanced evidence of DAMPs, suggesting that small molecule blockade and PDT-ICD co delivery at the nanoscale can provide a more manufacturable and iterative joint paradigm for CRC with antibody tolerance or insufficient infiltration.184 However, for clinical translation, given the overall lack of stable benefits of MSS mCRC for ICI and the urgent need for interpretable and stratable sensitization strategies, NDT has the advantages of local temporal and spatial controllability (such as accessible rectal/colon cavity illumination, ultrasound coverage of deep lesions) and material programmability (targeting, organelle localization, death mode regulation, extracellular vesicle immune suppression intervention). We hope to form an engineered synergistic treatment unit with PD-1/PD-L1 blockade as an immune pretreatment module. However, its clinical implementation still needs to align with existing evidence systems in patient stratification, biomarker and combination design, and be validated through prospective studies.159,189,190
In addition, ROS bursts and oxygen dynamics can transiently reshape checkpoint biology. Therefore, NDT pulses may modulate PD L1 expression through hypoxia and HIF 1 signaling pathways. This effect makes the temporal synchronization between NDT and ICB treatment nontrivial.191,192 For example, a CRC nanoplatform study combining PDT with PD L1 blockade reported that PDT mediated hypoxia activated HIF 1α signaling and increased PD L1 expression. This finding explained why the timing of anti PD L1 administration relative to the PDT pulse influenced therapeutic efficacy.107 In addition to tumor cells, ROS can also reprogram myeloid cell compartments. ROS inducing agents have been shown to increase PD L1 expression in macrophages through NF κB dependent transcription. These findings suggest that NDT generated oxidative stress may transiently alter PD L1 levels in both tumor and immune cells. Consequently, the optimal window for checkpoint inhibition may shift over time.193 Collectively, these findings support a practical translational recommendation for CRC NDT and ICB combination protocols. PD L1 and HIF 1α kinetics should be measured over time after each NDT pulse, together with local oxygenation when possible. These measurements help determine when checkpoint upregulation peaks and when antigen release and DC priming are maximal. ICB dosing should then be aligned with this empirically defined therapeutic window rather than assuming that concurrent treatment is always optimal.107,191
Engineering Localized Hydrogel and Depot Systems to Coordinate NDT with Immunomodulation
Localized co-delivery depots (injectable/sprayable hydrogels, in situ–forming matrices, or “postoperative bed” implants) are increasingly used as a logistics layer for nanodynamic therapies (NDT, eg., photodynamic/photothermal/chemodynamic modules) combined with immunomodulators, because a single platform can simultaneously solve tissue retention, spatiotemporal triggering, and multi-agent release mismatches that commonly limit systemic combination regimens (Figure 4).194–196 In CRC scenarios where surgery and locoregional relapse or peritoneal dissemination remain major barriers, a depot placed directly at the resection margin or intraperitoneal sites can sustain high on-site drug levels while reducing systemic exposure, thereby enabling repeated external triggering (light/heat) and prolonged immune modulation within the same anatomical compartment (Figure 5).93,197 Mechanistically, these depots are designed to synchronize tumor debulking plus antigen/alarmin generation by NDT with a longer immune programming window delivered by adjuvants or checkpoint blockade, a concept emphasized in recent injectable hydrogel immunotherapy frameworks.195,198,199 A representative colon cancer example is the thermosensitive poloxamer 407 (P407) hydrogel used as a co-delivery reservoir for indocyanine green (ICG) and checkpoint antibodies, where near-infrared PDT induced reactive oxygen species–mediated cytotoxicity and immunogenic cell death, while the same depot enabled effective intratumoral exposure to anti-PD-L1 and anti-CTLA-4 to extend survival in CT26/MC38-bearing mice compared with monotherapies.181 Importantly, the study directly connected material choice (P407 gelation and intratumoral retention) with immune readouts, showing that ICG-PDT promoted dendritic cell handling of tumor debris and maturation, and that adding checkpoint blockade amplified leukocyte infiltration and antitumor control, illustrating why depot-based colocalization can convert a transient photoreaction into a durable immune cascade.181
 |
Figure 4 Local CRC therapy–immunotherapy combinations enabled by localized co-delivery depots. Schematic overview of local cancer therapy in which a peritumoral/intratumoral depot serves as a logistics layer to integrate immunotherapy alone or in combination with chemotherapy, radiotherapy, phototherapy (photodynamic/photothermal), and gene/DNA-based interventions to elicit synergistic antitumor immunity. Localized co-delivery depots (eg., injectable/sprayable hydrogels, in situ–forming matrices, or postoperative-bed implants) improve tissue retention and enable spatiotemporally controlled activation of NDT modules while coordinating multi-agent release kinetics, thereby mitigating delivery and dosing mismatches that often limit systemic combination regimens. Adapted from Liu C, Liao Y, Liu Let al Application of injectable hydrogels in cancer immunotherapy. Front Bioeng Biotechnol. Copyright © 2023 by authors.194 |
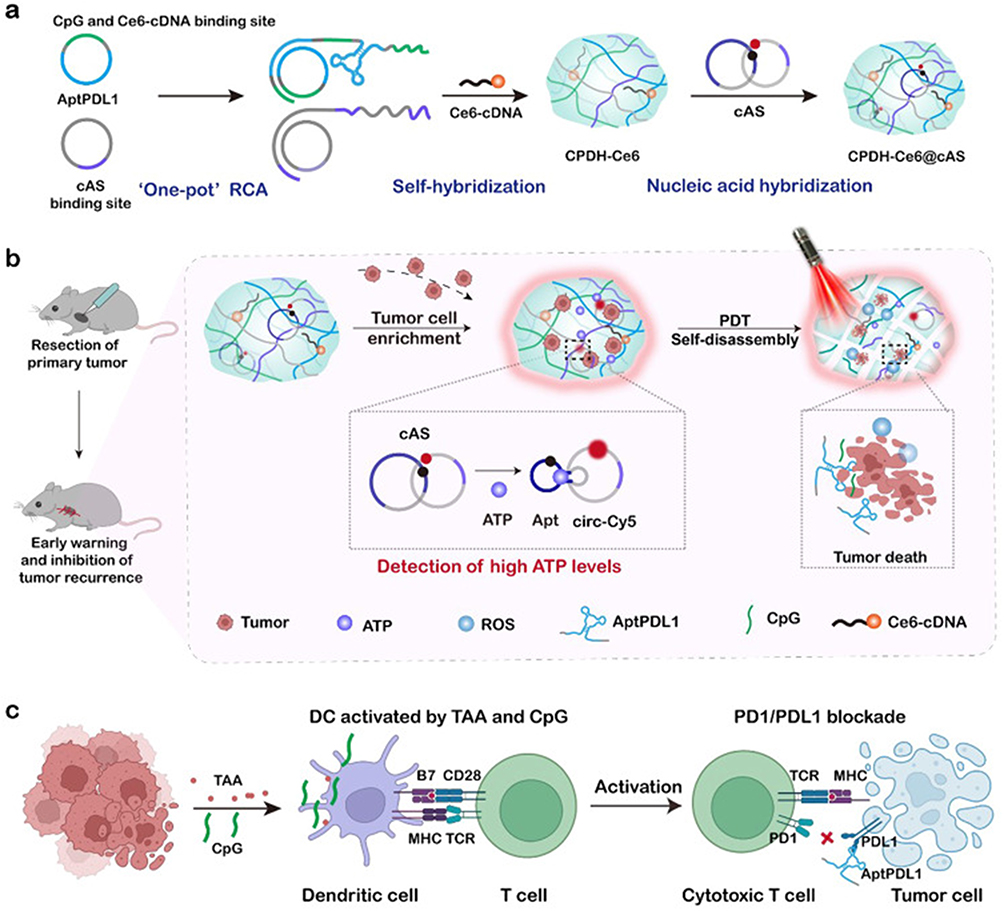 |
Figure 5 Mechanism schematic of a postoperative, triggerable immunomodulatory hydrogel depot for tumor recurrence monitoring and locoregional control. (a) Construction of CPDH-Ce6@cAS: aptPDL1 and CpG/Ce6-cDNA binding sites are introduced via a “one-pot” RCA process, followed by self-hybridization and nucleic-acid hybridization to assemble CPDH-Ce6 and further load cAS, yielding the final CPDH-Ce6@cAS complex. (b) Postoperative implantation and on-demand activation: a locally embedded CPDH-Ce6@cAS depot is placed at the CRC resection margin and/or intraperitoneal sites to sustain high on-site exposure with reduced systemic burden. Elevated ATP associated with locoregional relapse/peritoneal dissemination restores cAS fluorescence for early warning, while repeated external triggering (light) activates Ce6 to generate ROS, induces depot self-disassembly, and enables release/availability of immunomodulators for locoregional tumor control. (c) Immunomodulation mechanism: CpG and tumor-associated antigens (TAA) promote dendritic cell (DC) maturation and T-cell activation, while the released PD-L1 aptamer blocks the PD-1/PD-L1 checkpoint, thereby enhancing cytotoxic T-cell–mediated tumor killing.Adapted from Wang D, Liu J, Duan J et al Enrichment and sensing tumor cells by embedded immunomodulatory DNA hydrogel to inhibit postoperative tumor recurrence. Nat Commun. Copyright © 2023 by authors.197 |
Beyond simple loading, advanced depots embed stimulus-responsive logic so that NDT itself controls immunomodulator release. For example, Wang et al developed a DNA hydrogel, which encodes PD-L1 aptamer and CpG through rolling circular amplification, carries dihydroporphyrin e6 (Ce6), captures tumor cells with early recurrence after surgery, and then uses laser triggered PDT to damage the captured cells and generate ROS. ROS decomposes the matrix to release PD-L1 blocker (aptamer) and CpG in situ adjuvant.181 This design is notable from a combination-logistics perspective because the depot couples a local recurrence event with on-demand irradiation and an automatically “unlocked” immunotherapy payload, leading to systemic antitumor immunity and inhibition of metastasis in the authors’ postoperative recurrence-mimicking model, while also acknowledging translational constraints such as hydrogel/probe in vivo stability and model fidelity that must be engineered for clinical feasibility.181 A clinically relevant extension in postoperative CRC is a sprayable, hyaluronic-acid–based adhesive composite hydrogel embedding multifunctional nanoparticles (OXA–Mn(II)–Cur coordination polymer core with polydopamine shell), which achieved segmented pH-responsive release for >20 days, maintained high local concentration with reduced systemic toxicity, and produced long-lasting multi-stage immune activation that synergized with chemotherapy to eliminate residual disease and suppress peritoneal metastasis in mice.93 Although that platform emphasizes chemo–immuno synergy, its materials logic (tissue adhesion, sustained regional pharmacokinetics, and externally reinforced NDT-like photothermal contributions via PDA) directly informs how “rectal bed” depots could be engineered to host NDT sensitizers alongside immune agonists or checkpoint agents for prolonged local control.93 At the antigen-supply level, a complementary strategy is to use thermoresponsive F-127/gelatin hydrogels as a tumor-antigen depot by mixing tumor cells into the gel and applying PDT-associated ROS monitoring (Cy7 functionalization), conceptually positioning the hydrogel as a local vaccine-like template to mechanistically limit postsurgical relapse through antigen release coupled to phototherapy.200 In the future, modular immunostimulatory nanocomponents that integrate NDT with innate immune agonism—such as manganese-coordinated nanoparticles co-packaging Ce6 with the STING agonist MSA-2—provide plug-in payloads that are particularly compatible with depot placement, because depots can mitigate systemic off-target innate activation while preserving repeated triggerability and durable local exposure.201 Overall, these studies support a translationally grounded engineering principle for CRC: hydrogel/depot selection is not merely a carrier decision but a system-design variable that governs co-localization, trigger timing, and dose density of NDT plus immunomodulators, thereby shaping whether locoregional immune activation can be sustained long enough to prevent recurrence and metastatic escape.91,202,203
Challenges and Future Directions
Clinical Translational Challenges
Although NDT has shown various unique advantages compared to traditional treatments in CRC, there is still a critical gap between it and conventional clinical protocols. The core issue is not the insufficient performance of a single material, but the uncertainty and non-standardization of the full chain synergy of delivery triggering immune effects manufacturing and regulation.204,205 From a translational perspective, the lack of real exposure of nanoplatforms in vivo, limited cross model reproducibility, and gaps in evidence of biocompatibility and long-term safety are common bottlenecks that limit the entry of nanomedicine into clinical practice.206,207 NDT, relying on dynamic catalysis/energy triggering and ROS cascades, is more likely to amplify these uncertainties.208 Meanwhile, tumor vascular permeability and cell-mediated transport mechanisms are highly heterogeneous between different patients and lesions, leading to significant deviations in tumor accumulation and distribution of the same nano formula in clinical settings from animal models, thereby directly affecting the local response threshold and immune post effects required for NDT.81,209 For the indication of CRC, which is a more locally operable anatomical site, how to truly translate the advantages of local delivery into a controllable engineering loop of dose and exposure is still a clinical problem that needs to be prioritized.209 In addition, in terms of triggering and dosimetry, NDT of PDT/class PDT is constrained by the depth of light penetration, tissue optical heterogeneity, and hypoxia, especially in locally advanced CRC or deep infiltrating lesions, where uneven light field distribution can cause “edge residue” and insufficient immune stimulation, thereby weakening the synergistic window with immunotherapy.27 At the same time, clinical evidence also suggests that PDT research on CRC is still mainly based on early case series or retrospective evidence, with significant differences in treatment parameters (light dose, photosensitizer, irradiation method) across studies, making it difficult to form a replicable standard pathway. This makes it even more necessary to have a strict dosimetric framework when NDT approaches prospective trials.110 Even though there have been clinical explorations showing changes in the peripheral and tumor local immune cell spectrum after PDT accompanied by therapeutic signals, the queue size and study design are still insufficient to answer the key translational questions of optimal trigger intensity, repetition rate, and immune combination timing.81,210 For SDT/ultrasound triggered NDT, the acoustic field parameters (frequency, intensity, duty cycle, focusing mode) are highly coupled with cavitation effects and are related to tissue acoustic properties, tumor location, and gas/blood flow status. This leads to a greater dependence on equipment and operational standardization for efficacy and toxicity windows, which must be addressed through an engineering quality control system before multi-center clinical promotion.81,166,210
Furthermore, considering the biocompatibility of nanomaterials, NDT often achieves immune activation through ROS induced cell death and DAMPs release. However, ROS generation relies on oxygen supply and local antioxidant buffering. The hypoxia and metabolic/inflammatory fluctuations in the CRC microenvironment can cause individual differences in the intensity of immunogenic cell death (ICD), which in turn affects the predictability of subsequent immunotherapy.211 In addition, the active ingredient carrier boundary of NDT nanoplatforms is often not clear (such as metal/semiconductor nanostructures with both carrier and catalytic functions), and their protein crown, immunogenicity, reticuloendothelial system uptake, and long-term clearance pathways may be completely different from traditional small molecules. Therefore, more systematic immunotoxicology and chronic exposure assessment are needed, not just short-term blood biochemistry and major organ H&E.212 Notably, glutathione GSH depletion is widely used as a catalytic amplification strategy to sustain ROS flux. However, GSH is a central redox buffer in normal tissues, particularly in the liver and kidney, and it participates in detoxification and redox signaling pathways. Therefore, systemic perturbation of GSH can disrupt whole body redox homeostasis and increase susceptibility to off target oxidative injury.213–215 Accordingly, CRC oriented NDT and CDT systems that rely on GSH depletion should clearly distinguish local intratumoral depletion from systemic depletion. Longitudinal oxidative safety monitoring should also be incorporated. Relevant indicators include blood or tissue GSH to GSSG ratios, lipid peroxidation products such as MDA and 4 HNE, protein oxidation markers, and antioxidant enzyme activities. These measurements should be evaluated together with standard organ function panels and extended histopathological analyses.213–215 This safety consideration is closely related to biodistribution. After systemic administration, a substantial fraction of nanoparticles may be captured by the liver through RES and Kupffer cell pathways. This process can concentrate metal or catalytic components in hepatic tissue. If GSH reactive chemistry is not adequately confined, this accumulation may amplify redox related toxicity.216,217 Therefore, hepatic accumulation and clearance as well as potential hepatobiliary elimination should be reported as part of a translation oriented evaluation package. Design strategies should prioritize degradable chemistries and circulation stable inactive states. In addition, local delivery approaches such as intrarectal depots, hydrogels, or postoperative implants can spatially confine redox modulation and reduce systemic oxidative burden.216,217 For metal based catalytic agents, long term biodistribution and clearance kinetics should be quantitatively evaluated. Measurements should include RES organs such as the liver and spleen as well as CRC relevant sites. These sites include the intestinal mucosa, particularly under endoluminal or intrarectal exposure conditions, and metastatic liver lesions. Hepatic sinusoidal structures and Kupffer cell uptake can dominate nanoparticle fate and may generate clinically meaningful off target exposure.218,219 Accordingly, translation ready NDT studies should report time resolved organ burden measurements. These may include elemental quantification by ICP MS for metal catalysts or radiotracer imaging such as PET or SPECT when feasible. Studies should also quantify biological half life and excretion routes. In addition, dose exposure toxicity relationships should be defined to establish practical safety thresholds for CRC patients with compromised liver function or liver metastases.218–220 For mucosa facing strategies, nanoparticle interactions with mucus and epithelial barriers as well as local immune responses can influence retention and safety profiles. Therefore, mucosal accumulation, barrier perturbation, and local inflammatory responses should be evaluated together with systemic PK measurements.221,222 From the perspectives of regulation and chemistry, manufacturing and controls, the key quality attributes of nanomedicine (particle size distribution, surface chemistry, morphology, impurities, and inter batch consistency) need to be linked to the mechanism of action and risk benefit logic in the early stages, otherwise they are often forced to rework after entering the IND/clinical stage due to the inability to prove controllability and comparability.223 European regulatory authorities also emphasize that the development of nanomedicine should be aligned with regulatory scientific advice as early as possible, and a consistent classification and quality data package should be established throughout the lifecycle to reduce registration uncertainty caused by differences in the definition of active ingredients/excipients in different regions.224,225
Future Directions
In the near future, we believe that the breakthrough of NDT in precision treatment of CRC should shift from stronger materials to clinically executable system solutions. The primary direction is to reconstruct the delivery path with local accessibility as the core, such as using endoscopy, intracavitary/intraoperative light sources, and focused ultrasound to achieve spatial dose control, and coupling with imaging or optical monitoring to form a closed-loop dosimetry, thereby improving the coverage and consistency of deep or irregular lesions.27,157,226 Secondly, based on the objective reality of heterogeneity in tumor delivery mechanisms, there is a greater need for the development of interpretable patient stratification and biomarker strategies in the future (such as histological/vascular and immune structural feature prediction of nano accumulation and immune plasticity) to reduce the dilution of the true beneficiary population by averaging experimental designs.208,226 To make this stratification clinically actionable, we propose a biomarker framework aligned with the mechanistic logic of NDT involving trigger activation, ROS flux generation, and immune responses. The first category includes hypoxia associated indicators such as HIF 1α and CAIX expression or hypoxia PET tracers including 18F FMISO. These biomarkers help evaluate oxygen dependent PDT or ROS kinetics and hypoxia associated immune escape. The second category includes metabolic markers reflecting lactate accumulation and tumor acidity. Representative examples include lactate transport signatures such as MCT4 and SLC16A3. These markers have been associated with immune suppression and may correlate with responsiveness to ICB therapy. The third category involves dynamic PD L1 expression trajectories, including hypoxia driven coupling between HIF signaling and PD L1 regulation. These dynamics can guide the temporal synchronization between pulsatile NDT treatment and checkpoint blockade therapy.192,227–229 In parallel, immune infiltration profiles should be standardized using clinically validated frameworks such as the Immunoscore. This system evaluates CD3 and CD8 T cell densities within the tumor core and invasive margin. Additional profiling of myeloid and Treg related signatures, including MDSC and TAM polarization states, can further characterize the capacity for immune cold to hot conversion. These parameters also provide cross center comparable immune readouts.230–232 Thirdly, in terms of immune transformation, it is recommended to position NDT as a programmable immune preprocessing module, systematically designing the timing, frequency, and intensity of ICIs/immunomodulators through controllable local inflammation and antigen release windows, and establishing a transferable readout system with tumor infiltrating T cells, Treg/MDSC lineage, PD-L1 dynamics, and memory T cells to support cross center comparability.81,233 Fourthly, at the industrialization level, following the transformation framework such as DELIVER, the design, characterization, manufacturing, non-clinical models, and clinical endpoints will be moved forward and coordinated. Priority will be given to selecting scalable and scalable synthesis routes, degradable/removable material systems, and trigger schemes compatible with existing equipment platforms, which will significantly improve the success probability of NDT entering clinical validation.27,204,233 Future development of multilayer MOF, COF, and nanozyme based NDT systems should prioritize manufacturing feasibility. Designs should move beyond proof of concept complexity toward scalable, reproducible, and stability validated architectures. Regulatory agencies require developers to define critical quality attributes (CQAs), control process variability, and demonstrate product comparability when nanomaterials are incorporated into finished drug products.234,235 Continuous manufacturing strategies can help reduce process drift and improve batch to batch consistency. Examples include microfluidics enabled synthesis and scalable downstream drying or solidification processes. In addition, long term physicochemical stability programs should incorporate stress testing relevant to clinical handling conditions. When gastrointestinal delivery layers are involved, these logistics related components should also be evaluated. Such measures allow multifunctional nanoplatforms to remain compatible with a translation ready CMC development framework.27,225,234 By vigorously combining basic experiments with clinical translation and promoting each other, we believe that NDT will greatly improve the outcomes of CRC treatment in the future.
Conclusion
Nanodynamic therapy provides a promising locally controllable strategy for CRC. It enables on demand generation of cytotoxic species and modulation of the tumor microenvironment. Because CRC lesions are anatomically accessible, externally triggered activation and localized delivery are particularly feasible. These features offer advantages in precision and safety compared with purely systemic approaches. Increasing evidence indicates that the therapeutic potential of NDT extends beyond direct tumor ablation. NDT can function as an immune priming modality that synergizes with immunotherapy and other treatment strategies. This process may convert immunologically cold CRC lesions into immune active tumors and enhance responsiveness to immune checkpoint blockade. Nevertheless, successful clinical translation will require standardized activation protocols, robust patient stratification strategies, and scalable manufacturing systems that meet regulatory requirements. To accelerate cross center reproducibility, future CRC focused NDT trials should establish practical Standard Operating Procedures SOPs. These procedures should harmonize stimulus dosimetry and reporting parameters. Examples include light wavelength, irradiance, fluence, and exposure geometry, as well as ultrasound frequency, duty cycle, acoustic pressure or intensity, and focal volume. When applicable, RT dose and spatial mapping should also be reported. In addition, SOPs should standardize intraluminal or intracavitary delivery logistics, including applicator positioning, treatment margins, and motion management. Prespecified pharmacokinetic and retention controls for local depots or hydrogels should also be defined. Finally, response assessment timelines and immune monitoring panels related to ICD induction and systemic immune memory should be incorporated. Standardized dosimetry, particularly for optical and ultrasound fields, should be treated as a field level priority. Lack of standardization remains a major bottleneck that limits inter institutional comparability and delays regulatory acceptance. Addressing these challenges will be essential for translating NDT from experimental platforms into clinically impactful therapies for CRC. Finally, the anatomical accessibility of rectal tumors and the increasing emphasis on organ preservation create a favorable context for NDT based strategies. NDT induced local immune priming and durable complete clinical responses may support Watch and Wait strategies in selected rectal cancer patients. Such approaches could reduce the need for radical surgery while maintaining oncologic safety and would highlight the clinical significance of CRC oriented NDT platforms.
Data Sharing Statement
No new data has been generated, all references are cited in the manuscript.
Consent for Publication
All the authors were consent for publication.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by Scientific Research Fund Project of Yunnan Provincial Department of Education (2023J1768).
Disclosure
The authors declare that there are no competing interests associated with the manuscript.
References
1. Bray F, Laversanne M, Sung H. et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–36. doi:10.3322/caac.21834
2. Zhang J, Ou D, Xie A, Chen D, Li X. Global burden and cross-country health inequalities of early-onset colorectal cancer and its risk factors from 1990 to 2021 and its projection until 2036. BMC Public Health. 2024;24(1):3124. doi:10.1186/s12889-024-20624-4
3. Wang K, Ning S, Zhang S, et al. Extracellular matrix stiffness regulates colorectal cancer progression via HSF4. J Exp Clin Cancer Res. 2025;44(1):30. doi:10.1186/s13046-025-03297-8
4. Liu B, Zhou H, Tan L, Siu KTH, Guan XY. Exploring treatment options in cancer: tumor treatment strategies. Signal Transduct Target Ther. 2024;9(1):175. doi:10.1038/s41392-024-01856-7
5. Cañellas-Socias A, Sancho E, Batlle E. Mechanisms of metastatic colorectal cancer. Nat Rev Gastroenterol Hepatol. 2024;21(9):609–625. doi:10.1038/s41575-024-00934-z
6. Zeineddine FA, Zeineddine MA, Yousef A, et al. Survival improvement for patients with metastatic colorectal cancer over twenty years. Npj Precis Oncol. 2023;7(1):16. doi:10.1038/s41698-023-00353-4
7. Goey KKH, Lam-Boer J, de Wilt JHW, Punt CJA, van Oijen MGH, Koopman M. Significant increase of synchronous disease in first-line metastatic colorectal cancer trials: results of a systematic review. EurJ Cancer. 2016;69:166–177. doi:10.1016/j.ejca.2016.09.028
8. Valdeolivas A, Amberg B, Giroud N, et al. Profiling the heterogeneity of colorectal cancer consensus molecular subtypes using spatial transcriptomics. Npj Precis Oncol. 2024;8(1):10. doi:10.1038/s41698-023-00488-4
9. Jia H, Liu X, Wang G, et al. Spatial and single‐cell transcriptomic analysis reveals fibroblasts dependent immune environment in colorectal cancer. BioFactors. 2025;51(2):e70012. doi:10.1002/biof.70012
10. He B, Wang L, Zhou W, et al. A fusion model to predict the survival of colorectal cancer based on histopathological image and gene mutation. Sci Rep. 2025;15(1):9677. doi:10.1038/s41598-025-91420-2
11. Kao TW, Bai GH, Wang TL, et al. Novel cancer treatment paradigm targeting hypoxia-induced factor in conjunction with current therapies to overcome resistance. J Exp Clin Cancer Res. 2023;42(1):171. doi:10.1186/s13046-023-02724-y
12. Wang B, Hu S, Teng Y, et al. Current advance of nanotechnology in diagnosis and treatment for malignant tumors. Signal Transduct Target Ther. 2024;9(1). doi:10.1038/s41392-024-01889-y
13. Song G, Zeng C, Li J, et al. Exosome-based nanomedicines for digestive system tumors therapy. Nanomed. 2025;20(10):1167–1180. doi:10.1080/17435889.2025.2493037
14. Guan L, Tao S, Lu X, et al. A Lysosome-Targeted Iridium(III) Complex Inducing Pyroptosis for Enhanced Sonodynamic Therapy of Colorectal Cancer. J Med Chem. 2025;68(13):14008–14018. doi:10.1021/acs.jmedchem.5c01106
15. Lin S, Yang M, Chen J, Feng W, Chen Y, Zhu Y. Two-Dimensional FePS3 Nanosheets as an Integrative Sonosensitizer/Nanocatalyst for Efficient Nanodynamic Tumor Therapy. Small. 2023;19(8):2204992. doi:10.1002/smll.202204992
16. Li Y, Jin L, Tao B, et al. Nanodynamic therapy for cancer: mechanistic innovations, targeting strategies and multimodal treatments. J Transl Med. 2025;23(1):1300. doi:10.1186/s12967-025-07277-6
17. Wen D, Feng J, Deng R, Li K, Zhang H. Zn/Pt dual-site single-atom driven difunctional superimposition-augmented sonosensitizer for sonodynamic therapy boosted ferroptosis of cancer. Nat Commun. 2024;15(1):9359. doi:10.1038/s41467-024-53488-8
18. Wu S, Wang Q, Du J, et al. Bi-Pt Heterojunction Cascade Reaction Platform for Sono-Immunotherapy of Tumors via PANoptosis and Ferroptosis. Adv Healthc Mater. 2024;13(30):e2401697. doi:10.1002/adhm.202401697
19. Ding Q, Li W, Mei L, et al. Tailoring Advanced Metal-Based Nanomedicines for Adaptable Nanodynamic Disease Therapies and Theranostics. Adv Mater. 2026;38(1):e13609. doi:10.1002/adma.202513609
20. Hu H, Feng W, Qian X, Yu L, Chen Y, Li Y. Emerging Nanomedicine-Enabled/Enhanced Nanodynamic Therapies beyond Traditional Photodynamics. Adv Mater. 2021;33(12):e2005062. doi:10.1002/adma.202005062
21. Rodrigues JA, Correia JH. Photodynamic Therapy for Colorectal Cancer: an Update and a Look to the Future. Int J Mol Sci. 2023;24(15):12204. doi:10.3390/ijms241512204
22. Janas K, Boniewska-Bernacka E, Dyrda G, Słota R. Porphyrin and phthalocyanine photosensitizers designed for targeted photodynamic therapy of colorectal cancer. Bioorg Med Chem. 2021;30:115926. doi:10.1016/j.bmc.2020.115926
23. Zhang B, Huang Y, Huang Y. Advances in Nanodynamic Therapy for Cancer Treatment. Nanomaterials. 2024;14(7). doi:10.3390/nano14070648
24. Chen Q, Zhang M, Huang H, et al. Single Atom-Doped Nanosonosensitizers for Mutually Optimized Sono/Chemo-Nanodynamic Therapy of Triple Negative Breast Cancer. Adv Sci. 2023;10(6):e2206244. doi:10.1002/advs.202206244
25. Jiang T, Tang Z, Tian S, et al. Metal-organic nanostructures based on sono/chemo-nanodynamic synergy of TixOy/Ru reaction units: for ultrasound-induced dynamic cancer therapy. J Nanobiotechnology. 2025;23(1):533. doi:10.1186/s12951-025-03599-1
26. Wang X, Peng J, Meng C, Feng F. Recent advances for enhanced photodynamic therapy: from new mechanisms to innovative strategies. Chem Sci. 2024;15(31):12234–12257. doi:10.1039/D3SC07006A
27. Zhang S, Zhang H, Song P, Wang D, Wang Y. Colorectal cancer therapy mediated by nanomedicines. Chem Commun. 2023;59(30):4423–4435. doi:10.1039/d2cc06212g
28. Sang R, Nixdorf S, Hung T, et al. Unlocking the in vivo therapeutic potential of radiation-activated photodynamic therapy for locally advanced rectal cancer with lymph node involvement. eBioMedicine. 2025;116:105724. doi:10.1016/j.ebiom.2025.105724
29. Sang R, Deng F, Engel A, Goldys E, Deng W. Lipid-polymer nanocarrier platform enables X-ray induced photodynamic therapy against human colorectal cancer cells. Biomed Pharmacother Biomedecine Pharmacother. 2022;155:113837. doi:10.1016/j.biopha.2022.113837
30. Cao C, Wang X, Yang N, Song X, Dong X. Recent advances of cancer chemodynamic therapy based on Fenton/Fenton-like chemistry. Chem Sci. 2022;13(4):863–889. doi:10.1039/d1sc05482a
31. Wan X, Zhang Y, Zheng T, et al. Fe-MOF nanoplatform: specifically overcoming oxaliplatin resistance in colorectal cancer through multifaceted pathways. Mater Today Nano. 2024;26:100484. doi:10.1016/j.mtnano.2024.100484
32. Dong S, Cao H, Yuan Y, et al. A Novel “Three-in-One” Copper-Based Metal-Organic Framework Nanozyme Eradicates Colorectal Cancer and Overcomes Chemoresistance for Tumor Therapy. Adv Sci. 2025;12(6):e2413422. doi:10.1002/advs.202413422
33. Ding X, Huang H, Fang Z, Jiang J. From Subtypes to Solutions: integrating CMS Classification with Precision Therapeutics in Colorectal Cancer. Curr Treat Options Oncol. 2024;25(12):1580–1593. doi:10.1007/s11864-024-01282-5
34. Guinney J, Dienstmann R, Wang X, et al. The consensus molecular subtypes of colorectal cancer. Nat Med. 2015;21(11):1350–1356. doi:10.1038/nm.3967
35. Sehgal M, Ramu S, Vaz JM, et al. Characterizing heterogeneity along EMT and metabolic axes in colorectal cancer reveals underlying consensus molecular subtype-specific trends. Transl Oncol. 2024;40:101845. doi:10.1016/j.tranon.2023.101845
36. Zhang Y, Zhu J, Sun H, Li J. Modulation of tumor hypoxia and redox microenvironment using nanomedicines for enhanced cancer photodynamic therapy. Appl Mater Today. 2022;29:101687. doi:10.1016/j.apmt.2022.101687
37. Han X, Xu Y, Geranpayehvaghei M, Anderson GJ, Li Y, Nie G. Emerging nanomedicines for anti-stromal therapy against desmoplastic tumors. Biomaterials. 2020;232:119745. doi:10.1016/j.biomaterials.2019.119745
38. Cressey P, Abd Shukor SB, Thanou M. Sonodynamic therapy: transforming sound into light for hard-to-treat tumours. Adv Drug Deliv Rev. 2025;226:115696. doi:10.1016/j.addr.2025.115696
39. Wang Z, Run Z, Wang H, He X, Li J. TiO2-Ti3C2 Nanocomposites Utilize Their Photothermal Activity for Targeted Treatment of Colorectal Cancer. Int J Nanomed. 2024;19:1041–1054. doi:10.2147/IJN.S446537
40. Wo JY, Anker CJ, Ashman JB, et al. Radiation Therapy for Rectal Cancer: executive Summary of an ASTRO Clinical Practice Guideline. Pract Radiat Oncol. 2021;11(1):13–25. doi:10.1016/j.prro.2020.08.004
41. Lin L, He H, Xue R, et al. Direct and quantitative assessments of near-infrared light attenuation and spectroscopic detection depth in biological tissues using surface-enhanced Raman scattering. Med-X. 2023;1(1):9. doi:10.1007/s44258-023-00010-2
42. Bachu VS, Kedda J, Suk I, Green JJ, Tyler B. High-Intensity Focused Ultrasound: a Review of Mechanisms and Clinical Applications. Ann Biomed Eng. 2021;49(9):1975–1991. doi:10.1007/s10439-021-02833-9
43. Mushtaq A, Iqbal MZ, Tang J, Sun W. The wonders of X-PDT: an advance route to cancer theranostics. J Nanobiotechnology. 2024;22(1):655. doi:10.1186/s12951-024-02931-5
44. Liu Z, He Y, Ling J, Yi G, Ouyang XK, Wang N. MnO2 modified hollow mesoporous silica nanoparticles for enhanced chemodynamic therapy. J Drug Deliv Sci Technol. 2024;95:105604. doi:10.1016/j.jddst.2024.105604
45. Leonard NA, Corry SM, Reidy E, et al. Tumor-associated mesenchymal stromal cells modulate macrophage phagocytosis in stromal-rich colorectal cancer via PD-1 signaling. iScience. 2024;27(9). doi:10.1016/j.isci.2024.110701
46. Dong S, Cao H, Yuan Y, et al. A Novel “Three-in-One” Copper-Based Metal-Organic Framework Nanozyme Eradicates Colorectal Cancer and Overcomes Chemoresistance for Tumor Therapy. Adv Sci Weinh Baden-Wurtt Ger. 2025;12(6). doi:10.1002/advs.202413422
47. Bernal-Chávez SA, Prado-Audelo MLD, Caballero-Florán IH, et al. Insights into Terminal Sterilization Processes of Nanoparticles for Biomedical Applications. Molecules. 2021;26(7):2068. doi:10.3390/molecules26072068
48. Portillo-Vélez NS, Obeso JL, De Los Reyes JA, Peralta RA, Ibarra IA, Huxley MT. Benefits and complexity of defects in metal-organic frameworks. Commun Mater. 2024;5(1):247. doi:10.1038/s43246-024-00691-1
49. Costa C, Padrela L. Progress on drug nanoparticle manufacturing: exploring the adaptability of batch bottom-up approaches to continuous manufacturing. J Drug Deliv Sci Technol. 2025;111:107120. doi:10.1016/j.jddst.2025.107120
50. Yang Z, McClements DJ, Li C, et al. Targeted delivery of hydrogels in human gastrointestinal tract: a review. Food Hydrocoll. 2023;134:108013. doi:10.1016/j.foodhyd.2022.108013
51. Huai M, Pei M, Pan J, et al. Oral colon-targeted responsive alginate/hyaluronic acid-based hydrogel propels the application of infliximab in colitis. Int J Biol Macromol. 2023;249:125952. doi:10.1016/j.ijbiomac.2023.125952
52. Chen H, Liu R, Fu J, et al. Surface engineering of copper peroxide nanodots and Au nanozyme on porphyrin-based metal-organic frameworks induces cascade reactions for colorectal cancer treatment. Chem Eng J. 2025;518:164764. doi:10.1016/j.cej.2025.164764
53. Li WY, Wan JJ, Kan JL, et al. A biodegradable covalent organic framework for synergistic tumor therapy. Chem Sci. 2023;14(6):1453–1460. doi:10.1039/d2sc05732h
54. Pooresmaeil M, Namazi H. pH-sensitive carboxymethyl starch-gelatin coated COF/5-Fu for colon cancer therapy. Ind Crops Prod. 2023;202:117102. doi:10.1016/j.indcrop.2023.117102
55. Yu T, Guo F, Yu Y, et al. Fusobacterium nucleatum Promotes Chemoresistance to Colorectal Cancer by Modulating Autophagy. Cell. 2017;170(3):548–563.e16. doi:10.1016/j.cell.2017.07.008
56. Dadgar-Zankbar L, Elahi Z, Shariati A, Khaledi A, Razavi S, Khoshbayan A. Exploring the role of Fusobacterium nucleatum in colorectal cancer: implications for tumor proliferation and chemoresistance. Cell Commun Signal CCS. 2024;22(1):547. doi:10.1186/s12964-024-01909-y
57. Li H, Zhou X, Huang Y, Liao B, Cheng L, Ren B. Reactive Oxygen Species in Pathogen Clearance: the Killing Mechanisms, the Adaption Response, and the Side Effects. Front Microbiol. 2020;11:622534. doi:10.3389/fmicb.2020.622534
58. Fulaz S, Vitale S, Quinn L, Casey E. Nanoparticle-Biofilm Interactions: the Role of the EPS Matrix. Trends Microbiol. 2019;27(11):915–926. doi:10.1016/j.tim.2019.07.004
59. Chen C, Su Q, Zi M, Hua X, Zhang Z. Harnessing gut microbiota for colorectal cancer therapy: from clinical insights to therapeutic innovations. NPJ Biofilms Microbiomes. 2025;11(1). doi:10.1038/s41522-025-00818-3
60. Cho YS, Han K, Xu J, Moon JJ. Novel strategies for modulating the gut microbiome for cancer therapy. Adv Drug Deliv Rev. 2024;210:115332. doi:10.1016/j.addr.2024.115332
61. Narang AK, Meyer J. Neoadjuvant Short-Course Radiation Therapy for Rectal Cancer: trends and Controversies. Curr Oncol Rep. 2018;20(9):68. doi:10.1007/s11912-018-0714-x
62. Chen T, Chu Q, Li M, Han G, Li X. Fe3O4@Pt nanoparticles to enable combinational electrodynamic/chemodynamic therapy. J Nanobiotechnology. 2021;19(1):206. doi:10.1186/s12951-021-00957-7
63. Gao X, Zhou S, Qin Z, Li D, Zhu Y, Ma D. Upregulation of HMGB1 in tumor-associated macrophages induced by tumor cell-derived lactate further promotes colorectal cancer progression. J Transl Med. 2023;21(1):53. doi:10.1186/s12967-023-03918-w
64. Choi H, Yeo M, Kang Y, et al. Lactate oxidase/catalase-displaying nanoparticles efficiently consume lactate in the tumor microenvironment to effectively suppress tumor growth. J Nanobiotechnology. 2023;21(1):5. doi:10.1186/s12951-022-01762-6
65. Cao X, Rao Allu S, Jiang S, et al. Tissue pO2 distributions in xenograft tumors dynamically imaged by Cherenkov-excited phosphorescence during fractionated radiation therapy. Nat Commun. 2020;11(1):573. doi:10.1038/s41467-020-14415-9
66. Rademakers SE, Lok J, van der Kogel AJ, Bussink J, Kaanders JHAM. Metabolic markers in relation to hypoxia; staining patterns and colocalization of pimonidazole, HIF-1α, CAIX, LDH-5, GLUT-1, MCT1 and MCT4. BMC Cancer. 2011;11:167. doi:10.1186/1471-2407-11-167
67. Kucherlapati MH. Mouse models in colon cancer, inferences, and implications. iScience. 2023;26(6):106958. doi:10.1016/j.isci.2023.106958
68. Greenlee JD, King MR. A syngeneic MC38 orthotopic mouse model of colorectal cancer metastasis. Biol Methods Protoc. 2022;7(1):bpac024. doi:10.1093/biomethods/bpac024
69. Zhang S, Zhang H, Song P, et al. A biodegradable nanodrug with highly efficient treatment effect by remodeling tumor microenvironment and manipulating energy metabolism against colorectal cancer. Sci China Mater. 2023;67(1):331–342. doi:10.1007/s40843-023-2693-7
70. Wang X, Lu X, Yang X, et al. Engineering metal-organic framework nanoparticles trigger pyroptosis to boost colon cancer immunotherapy. Mater Des. 2024;238:112731. doi:10.1016/j.matdes.2024.112731
71. Zhang X, Tian H, Chen Y, et al. A metal-organic nanoframework for efficient colorectal cancer immunotherapy by the cGAS-STING pathway activation and immune checkpoint blockade. J Nanobiotechnology. 2024;22(1):592. doi:10.1186/s12951-024-02836-3
72. Xiao Y, Guo G, Wang H, et al. Curcumin/L-OHP co-loaded HAP for cGAS-STING pathway activation to enhance the natural immune response in colorectal cancer. Bioeng Transl Med. 2024;9(1):e10610. doi:10.1002/btm2.10610
73. Sivasubramanian M, Lo LW. Assessment of Nanoparticle-Mediated Tumor Oxygen Modulation by Photoacoustic Imaging. Biosensors. 2022;12(5):336. doi:10.3390/bios12050336
74. Shang T, Zhang R, Liu Y, Shi S. Intestinal oxygen and microbiota crosstalk: implications for pathogenesis of gastrointestinal diseases and emerging therapeutic strategies. Gut Pathog. 2025;17(1):100. doi:10.1186/s13099-025-00783-4
75. Denis M, Mathé D, Micoud M, et al. Impact of mouse model tumor implantation site on acquired resistance to anti-PD-1 immune checkpoint therapy. Front Immunol. 2022;13:1011943. doi:10.3389/fimmu.2022.1011943
76. Zhao X, Li L, Starr TK, Subramanian S. Tumor location impacts immune response in mouse models of colon cancer. Oncotarget. 2017;8(33):54775–54787. doi:10.18632/oncotarget.18423
77. Zhang L, Bu P. Generation of an orthotopic mouse model to study colorectal cancer metastasis. STAR Protoc. 2021;2(4):100792. doi:10.1016/j.xpro.2021.100792
78. Chicote I, Martínez-Quintanilla J, Cámara JA, Palmer HG. Orthotopic Implantation of Patient-Derived Cancer Cells in Mice Recapitulates Advanced Colorectal Cancer. J Vis Exp. 2023;(192). doi:10.3791/64629
79. Lee SB, Jeon HJ, Hyun H, Jeon YH. Establishment of an Orthotopic and Metastatic Colorectal Cancer Mouse Model Using a Tissue Adhesive-Based Implantation Method. Cancers. 2025;17(13):2266. doi:10.3390/cancers17132266
80. Wang Q, Hu T, Zhang Q, et al. Fusobacterium nucleatum promotes colorectal cancer through neogenesis of tumor stem cells. J Clin Invest. 2025;135(3):e181595. doi:10.1172/JCI181595
81. Gu B, Wang B, Li X, et al. Photodynamic therapy improves the clinical efficacy of advanced colorectal cancer and recruits immune cells into the tumor immune microenvironment. Front Immunol. 2022;13:1050421. doi:10.3389/fimmu.2022.1050421
82. Kang JW, Chen PJ, Chen CY, et al. Development of a hybrid hydrogel for submucosal injection in endoscopic resection of gastrointestinal neoplasm: from laboratory to clinical trial. Endosc Int Open. 2023;11(11):E1026–E1034. doi:10.1055/a-2161-2100
83. Gan R, Ni E, Li G, Chen W. A New Paradigm for Precision Drug Delivery in Inflammatory Bowel Disease: effective Transfer, Enhanced Retention, and Pathology‐Targeting Treatment via Biomaterials and Engineered Platforms. MedComm – Biomater Appl. 2025;4(3):e70022. doi:10.1002/mba2.70022
84. Muñoz Taboada G, Dahis D, Dosta P, Edelman E, Artzi N. Sprayable Hydrogel Sealant for Gastrointestinal Wound Shielding. Adv Mater. 2024;36(24):e2311798. doi:10.1002/adma.202311798
85. Liang C, Dudko V, Khoruzhenko O, et al. Stiff and self-healing hydrogels by polymer entanglements in co-planar nanoconfinement. Nat Mater. 2025;24(4):599–606. doi:10.1038/s41563-025-02146-5
86. Wang X, Zhu L, Zhou J, Zhao L, Li J, Liu C. Drug-loaded hybrid hydrogels for sonodynamic-chemodyanmic therapy and tumor metastasis suppression. Front Bioeng Biotechnol. 2023;11:1281157. doi:10.3389/fbioe.2023.1281157
87. Zhou J, Jia D, Jin L, et al. An injectable hydrogel for synergistic therapy in colorectal cancer by targeting glutathione. Cell Rep Phys Sci. 2025;6(2):102399. doi:10.1016/j.xcrp.2024.102399
88. Chen D, Wu Z, Xia C, Yang H, Ding W, He Q. A Sustained H2/Fluorouracil-Releasing Suppository for High-efficacy and Low-Toxicity Hydrogenochemotherapy of Colon Cancer. Adv Healthc Mater. 2025;14(7):e2404054. doi:10.1002/adhm.202404054
89. Ye X, Yin H, Lu Y, Zhang H, Wang H. Evaluation of Hydrogel Suppositories for Delivery of 5-Aminolevulinic Acid and Hematoporphyrin Monomethyl Ether to Rectal Tumors. Molecules. 2016;21(10):1347. doi:10.3390/molecules21101347
90. Gournaris E, Park W, Cho S, Bentrem DJ, Larson AC, Kim DH. Near-Infrared Fluorescent Endoscopic Image-Guided Photothermal Ablation Therapy of Colorectal Cancer Using Dual-Modal Gold Nanorods Targeting Tumor-Infiltrating Innate Immune Cells in a Transgenic TS4 CRE/APC loxΔ468 Mouse Model. ACS Appl Mater Interfaces. 2019;11(24):21353–21359. doi:10.1021/acsami.9b04186
91. Kim J, Choi Y, Kim DH, Yoon HY, Kim K. Injectable Hydrogel-Based Combination Cancer Immunotherapy for Overcoming Localized Therapeutic Efficacy. Pharmaceutics. 2022;14(9):1908. doi:10.3390/pharmaceutics14091908
92. Zeting Y, Shuli M, Yue L, et al. Tissue adhesive indocyanine green-locking granular gel-mediated photothermal therapy combined with checkpoint inhibitor for preventing postsurgical recurrence and metastasis of colorectal cancer. Bioeng Transl Med. 2023;8(6):e10576. doi:10.1002/btm2.10576
93. Wang Y, Zhang X, Zhang Y, et al. Sprayed hyaluronic acid based multidrug composite hydrogel for postoperative colorectal cancer ultra-efficient long-lasting multi-stage immuno-chemo synergistic therapy. Mater Horiz. 2025;12(12):4317–4335. doi:10.1039/d5mh00108k
94. Wang M, Hu D, Yang Y, et al. Enhanced Chemo-Immunotherapy Strategy Utilizing Injectable Thermosensitive Hydrogel for The Treatment of Diffuse Peritoneal Metastasis in Advanced Colorectal Cancer. Adv Sci. 2023;10(35):e2303819. doi:10.1002/advs.202303819
95. Huang Y, Ouyang W, Lai Z, et al. Nanotechnology-enabled sonodynamic therapy against malignant tumors. Nanoscale Adv. 2024;6(8):1974–1991. doi:10.1039/d3na00738c
96. Chen Y, Tang D. Precision nanomaterials in colorectal cancer: advancing photodynamic and photothermal therapy. RSC Adv. 2025;15(33):26583–26600. doi:10.1039/d5ra03996g
97. Gu T, Wang Y, Lu Y, et al. Platinum Nanoparticles to Enable Electrodynamic Therapy for Effective Cancer Treatment. Adv Mater Deerfield Beach Fla. 2019;31(14):e1806803. doi:10.1002/adma.201806803
98. Abreu MM, Chocron AF, Smadja DM. From cold to hot: mechanisms of hyperthermia in modulating tumor immunology for enhanced immunotherapy. Front Immunol. 2025;16:1487296. doi:10.3389/fimmu.2025.1487296
99. Chen P, Zhang P, Shah NH, Cui Y, Wang Y. A Comprehensive Review of Inorganic Sonosensitizers for Sonodynamic Therapy. Int J Mol Sci. 2023;24(15):12001. doi:10.3390/ijms241512001
100. Qu X, Yin F, Pei M, et al. Modulation of Intratumoral Fusobacterium nucleatum to Enhance Sonodynamic Therapy for Colorectal Cancer with Reduced Phototoxic Skin Injury. ACS Nano. 2023;17(12):11466–11480. doi:10.1021/acsnano.3c01308
101. Lyons NJ, Giri R, Begun J, et al. Reactive Oxygen Species as Mediators of Disease Progression and Therapeutic Response in Colorectal Cancer. Antioxid Redox Signal. 2023;39(1–3):186–205. doi:10.1089/ars.2022.0127
102. Yan X, Liu H, Guo L, et al. Multifunctional drug delivery nanoparticles for combined chemotherapy/chemodynamic/photothermal therapy against colorectal cancer through synergistic cuproptosis/ferroptosis/apoptosis. Mater Today Bio. 2025;30:101427. doi:10.1016/j.mtbio.2024.101427
103. Shi J, Tian H, Peng L, et al. A nanoplatform reshaping intracellular osmolarity and redox homeostasis against colorectal cancer. J Control Release off J Control Release Soc. 2022;352:766–775. doi:10.1016/j.jconrel.2022.11.003
104. Li H, Huang M, Wei Z, et al. Hydrogen sulfide activatable metal-organic frameworks for Fluorescence Imaging-Guided Photodynamic Therapy of colorectal cancer. Front Bioeng Biotechnol. 2022;10:1032571. doi:10.3389/fbioe.2022.1032571
105. Liu J, Liang L, Gan P, et al. Development of a Highly Efficient NIR-II Phototherapeutic Agent for Fluorescence Imaging-Guided Synergistic PTT/PDT/Chemotherapy of Colorectal Cancer. J Med Chem. 2025;68(7):7592–7604. doi:10.1021/acs.jmedchem.5c00066
106. Khaled YS, Khot MI, Aiyappa-Maudsley R, et al. Photoactive imaging and therapy for colorectal cancer using a CEA-Affimer conjugated Foslip nanoparticle. Nanoscale. 2024;16(14):7185–7199. doi:10.1039/d3nr04118b
107. Yuan Z, Fan G, Wu H, et al. Photodynamic therapy synergizes with PD-L1 checkpoint blockade for immunotherapy of CRC by multifunctional nanoparticles. Mol Ther J Am Soc Gene Ther. 2021;29(10):2931–2948. doi:10.1016/j.ymthe.2021.05.017
108. Chen J, Chen Z, Tan L, et al. Synthesis of a new chlorin photosensitizer for photodynamic therapy against colon cancer. Mater Chem Front. 2022;6(9):1129–1136. doi:10.1039/D2QM00046F
109. Nguyen DT, Baek MJ, Lee SM, et al. Photobleaching-mediated charge-convertible cyclodextrin nanoparticles achieve deep tumour penetration for rectal cancer theranostics. Nat Nanotechnol. 2024;19(11):1723–1734. doi:10.1038/s41565-024-01757-4
110. Guidolin K, Ding L, Yan H, et al. Photodynamic Therapy for Colorectal Cancer: a Systematic Review of Clinical Research. Surg Innov. 2022;29(6):788–803. doi:10.1177/15533506221083545
111. Mohammed DF, Madlool HA, Faris M, et al. Harnessing inorganic nanomaterials for chemodynamic cancer therapy. Nanomed. 2022;17(24):1891–1906. doi:10.2217/nnm-2022-0187
112. Anemone A, Consolino L, Arena F, Capozza M, Longo DL. Imaging tumor acidosis: a survey of the available techniques for mapping in vivo tumor pH. Cancer Metastasis Rev. 2019;38(1–2):25–49. doi:10.1007/s10555-019-09782-9
113. Liu J, Tang D, Kang R. Targeting GPX4 in ferroptosis and cancer: chemical strategies and challenges. Trends Pharmacol Sci. 2024;45(8):666–670. doi:10.1016/j.tips.2024.05.006
114. Li Y, Wang J, Zhu T, et al. A ROS storm generating nanocomposite for enhanced chemodynamic therapy through H2O2 self-supply, GSH depletion and calcium overload. Nanoscale. 2024;16(17). doi:10.1039/d3nr06422k
115. Pan X, Lin Y, Lin C, et al. Enhanced cGAS-STING Activation and Immune Response by LPDAM Platform-Based Lapachone-Chemical-Photothermal Synergistic Therapy for Colorectal Cancer. Adv Healthc Mater. 2025;14(11):e2403309. doi:10.1002/adhm.202403309
116. Jiang B, Duan D, Gao L, et al. Standardized assays for determining the catalytic activity and kinetics of peroxidase-like nanozymes. Nat Protoc. 2018;13(7):1506–1520. doi:10.1038/s41596-018-0001-1
117. Stolik S, Delgado JA, Pérez A, Anasagasti L. Measurement of the penetration depths of red and near infrared light in human “ex vivo” tissues. J Photochem Photobiol B. 2000;57(2–3):90–93. doi:10.1016/s1011-1344(00)00082-8
118. Suzen S, Gurer-Orhan H, Saso L. Detection of Reactive Oxygen and Nitrogen Species by Electron Paramagnetic Resonance (EPR) Technique. Molecules. 2017;22(1):181. doi:10.3390/molecules22010181
119. LeBel CP, Ischiropoulos H, Bondy SC. Evaluation of the probe 2’,7’-dichlorofluorescin as an indicator of reactive oxygen species formation and oxidative stress. Chem Res Toxicol. 1992;5(2):227–231. doi:10.1021/tx00026a012
120. Charbouillot T, Brigante M, Mailhot G, Maddigapu PR, Minero C, Vione D. Performance and selectivity of the terephthalic acid probe for OH as a function of temperature, pH and composition of atmospherically relevant aqueous media. J Photochem Photobiol Chem. 2011;222(1):70–76. doi:10.1016/j.jphotochem.2011.05.003
121. Niu B, Liao K, Zhou Y, et al. Application of glutathione depletion in cancer therapy: enhanced ROS-based therapy, ferroptosis, and chemotherapy. Biomaterials. 2021;277:121110. doi:10.1016/j.biomaterials.2021.121110
122. Imai H, Nakagawa Y. Biological significance of phospholipid hydroperoxide glutathione peroxidase (PHGPx, GPx4) in mammalian cells. Free Radic Biol Med. 2003;34(2):145–169. doi:10.1016/s0891-5849(02)01197-8
123. Li Y, Chen J, Xia Q, et al. Photothermal Fe3O4 nanoparticles induced immunogenic ferroptosis for synergistic colorectal cancer therapy. J Nanobiotechnology. 2024;22(1):630. doi:10.1186/s12951-024-02909-3
124. Chen X, Cheng D, Ding M, et al. Tumor-targeting biomimetic sonosensitizer-conjugated iron oxide nanocatalysts for combinational chemodynamic-sonodynamic therapy of colorectal cancer. J Mater Chem B. 2022;10(24):4595–4604. doi:10.1039/d2tb00872f
125. Zhang K, Meng X, Yang Z, Dong H, Zhang X. Enhanced cancer therapy by hypoxia-responsive copper metal-organic frameworks nanosystem. Biomaterials. 2020;258:120278. doi:10.1016/j.biomaterials.2020.120278
126. Huang Y, Tian H, Yue Z, et al. Copper-coordination driven nano-frameworks for efficient colorectal cancer chemo-immunotherapy by suppression of cancer cell stemness. Mater Today Bio. 2025;32:101707. doi:10.1016/j.mtbio.2025.101707
127. Qian Y, Wang C, Xu R, et al. Copper-based metal-organic frameworks for antitumor application. J Nanobiotechnology. 2025;23(1):135. doi:10.1186/s12951-025-03220-5
128. Ji M, Liu H, Gou J, et al. Recent advances in nanoscale metal-organic frameworks for cancer chemodynamic therapy. Nanoscale. 2023;15(20):8948–8971. doi:10.1039/d3nr00867c
129. Zhang L, Forgham H, Shen A, Qiao R, Guo B. Recent Advances in Single Fe-Based Nanoagents for Photothermal-Chemodynamic Cancer Therapy. Biosensors. 2022;12(2):86. doi:10.3390/bios12020086
130. Guo W, Wang T, Huang C, et al. Platelet membrane-coated C-TiO2 hollow nanospheres for combined sonodynamic and alkyl-radical cancer therapy. Nano Res. 2022;16(1):782–791. doi:10.1007/s12274-022-4646-2
131. Zhang Y, Zhao J, Zhang L, et al. A cascade nanoreactor for enhancing sonodynamic therapy on colorectal cancer via synergistic ROS augment and autophagy blockage. Nano Today. 2023;49:101798. doi:10.1016/j.nantod.2023.101798
132. Zhao Y, Xu J, Zhang Y, et al. Biomimetic redox-responsive prodrug micelles with diselenide linkage for platinum nanozymes augmented sonodynamic/chemo combined therapy of colon cancer. Chem Eng J. 2023;472:144911. doi:10.1016/j.cej.2023.144911
133. Wang T, Peng W, Du M, Chen Z. Immunogenic sonodynamic therapy for inducing immunogenic cell death and activating antitumor immunity. Front Oncol. 2023;13:1167105. doi:10.3389/fonc.2023.1167105
134. Huang H, Du L, Su R, et al. Albumin-based co-loaded sonosensitizer and STING agonist nanodelivery system for enhanced sonodynamic and immune combination antitumor therapy. J Control Release off J Control Release Soc. 2024;375:524–536. doi:10.1016/j.jconrel.2024.09.023
135. Wo JY, Ashman JB, Bhadkamkar NA, et al. Radiation Therapy for Rectal Cancer: an ASTRO Clinical Practice Guideline Focused Update. Pract Radiat Oncol. 2025;15(2):124–143. doi:10.1016/j.prro.2024.11.003
136. Benson AB, Venook AP, Adam M, et al. NCCN Guidelines® Insights: rectal Cancer, Version 3.2024. J Natl Compr Cancer Netw JNCCN. 2024;22(6):366–375. doi:10.6004/jnccn.2024.0041
137. He M, Chen S, Yu H, et al. Advances in nanoparticle-based radiotherapy for cancer treatment. iScience. 2025;28(1):111602. doi:10.1016/j.isci.2024.111602
138. Kagawa Y, Smith JJ, Fokas E, et al. Future direction of total neoadjuvant therapy for locally advanced rectal cancer. Nat Rev Gastroenterol Hepatol. 2024;21(6):444–455. doi:10.1038/s41575-024-00900-9
139. Du J, Ye YL, Xie CX, et al. Engineered Hf0.7Ti0.3O2 nanoparticles for efficient radiotherapy on rectal cancer via synergistically enhanced radiation deposition and ROS production. Rare Met. 2025; 1–14. doi:10.1007/s12598-025-03595-2.
140. Nelson BE, Adashek JJ, Lin SH, Subbiah V. The abscopal effect in patients with cancer receiving immunotherapy. Med. 2023;4(4):233–244. doi:10.1016/j.medj.2023.02.003
141. Tian F, Dai H, Sha D, et al. Total neoadjuvant treatment with short-course radiotherapy followed by sintilimab plus capecitabine-oxaliplatin versus short-course radiotherapy followed by capecitabine-oxaliplatin in patients with locally advanced rectal cancer (SPRING-01): a single-centre, open-label, Phase 2, randomised controlled trial. Lancet Oncol. 2025;26(8):1043–1054. doi:10.1016/S1470-2045(25)00286-4
142. Russell J, Carlin S, Burke SA, Wen B, Yang KM, Ling CC. Immunohistochemical detection of changes in tumor hypoxia. Int J Radiat Oncol Biol Phys. 2009;73(4):1177–1186. doi:10.1016/j.ijrobp.2008.12.004
143. Lu Z, Zhou L, Yao Y, et al. Reaction Mechanisms in Platinum-Mediated Electrodynamic Therapy. Adv Funct Mater. 2023;33(24):2214749. doi:10.1002/adfm.202214749
144. Chen T, Han G, Li X. Platinum–copper alloy nanoparticles armored with chloride ion transporter to promote electro-driven tumor inhibition. Bioact Mater. 2022;12:143–152. doi:10.1016/j.bioactmat.2021.10.012
145. C T, F Y, Z R, H G, L X. KCl-CaCO3 nanoclusters armoured with Pt nanocrystals for enhanced electro-driven tumor inhibition. Biomater Sci. 2022;10(2). doi:10.1039/d1bm01464a
146. Broholm M, Vogelsang R, Bulut M, et al. Endoscopic calcium electroporation for colorectal cancer: a phase I study. Endosc Int Open. 2023;11(5):E451–E459. doi:10.1055/a-2033-9831
147. Broholm M, Vogelsang R, Bulut M, et al. Neoadjuvant calcium electroporation for potentially curable colorectal cancer. Surg Endosc. 2024;38(2):697–705. doi:10.1007/s00464-023-10557-1
148. Adeyeye A, Olabintan O, Ayubi H, et al. Palliative Luminal Treatment of Colorectal Cancer Using Endoscopic Calcium-Electroporation: first Case Series from United Kingdom. J Clin Med. 2025;14(12):4138. doi:10.3390/jcm14124138IF:2.9Q1
149. Salameh ZS, Aycock KN, Alinezhadbalalami N, et al. Harnessing the Electrochemical Effects of Electroporation-Based Therapies to Enhance Anti-tumor Immune Responses. Ann Biomed Eng. 2024;52(1):48–56. doi:10.1007/s10439-023-03403-x
150. Miripour ZS, Ghahremani A, Karimi K, et al. Electrochemical therapy (EChT) of cancer tumor with an external anode, a way to achieve pathological complete response. Med Oncol. 2023;40(4):117. doi:10.1007/s12032-023-01979-x
151. Pogue BW, Elliott JT, Kanick SC, et al. Revisiting photodynamic therapy dosimetry: reductionist & surrogate approaches to facilitate clinical success. Phys Med Biol. 2016;61(7):R57–89. doi:10.1088/0031-9155/61/7/R57
152. Nompumelelo Simelane NW, Kruger CA, Abrahamse H. Photodynamic diagnosis and photodynamic therapy of colorectal cancer in vitro and in vivo. RSC Adv. 2020;10(68):41560–41576. doi:10.1039/d0ra08617g
153. Li X, Liu Y. Focused ultrasound in modern medicine: bioengineering interfaces, molecular effects, and clinical breakthroughs. Front Bioeng Biotechnol. 2025;13:1610846. doi:10.3389/fbioe.2025.1610846
154. Perera-Bel E, Yagüe C, Mercadal B, et al. EView: an electric field visualization web platform for electroporation-based therapies. Comput Methods Programs Biomed. 2020;197:105682. doi:10.1016/j.cmpb.2020.105682
155. Corovic S, Lackovic I, Sustaric P, Sustar T, Rodic T, Miklavcic D. Modeling of electric field distribution in tissues during electroporation. Biomed Eng Online. 2013;12:16. doi:10.1186/1475-925X-12-16
156. Yadav N, Singh M, Mishra SP, Ansari S. Development of an Anthropomorphic Heterogeneous Female Pelvic Phantom and Its Comparison with a Homogeneous Phantom in Advance Radiation Therapy: dosimetry Analysis. Med Sci. 2023;11(3):59. doi:10.3390/medsci11030059
157. Rodrigues JA, Correia JH, Rodrigues JA, Correia JH. Photodynamic Therapy for Colorectal Cancer: an Update and a Look to the Future. Int J Mol Sci. 2023;24(15):12204. doi:10.3390/ijms241512204
158. Huang L, Zhao S, Wu J, et al. Photodynamic therapy for hypoxic tumors: advances and perspectives. Coord Chem Rev. 2021;438:213888. doi:10.1016/j.ccr.2021.213888
159. Hamid MA, Pammer LM, Lentner TK, et al. Immunotherapy for Microsatellite-Stable Metastatic Colorectal Cancer: can we close the Gap between Potential and Practice? Curr Oncol Rep. 2024;26(10):1258–1270. doi:10.1007/s11912-024-01583-w
160. Xiao BY, Zhang X, Cao TY, et al. Neoadjuvant Immunotherapy Leads to Major Response and Low Recurrence in Localized Mismatch Repair-Deficient Colorectal Cancer. J Natl Compr Cancer Netw JNCCN. 2023;21(1):60–66.e5. doi:10.6004/jnccn.2022.7060
161. Chou TC. Drug Combination Studies and Their Synergy Quantification Using the Chou-Talalay Method. Cancer Res. 2010;70(2):440–446. doi:10.1158/0008-5472.CAN-09-1947
162. Chou TC, Talalay P. Quantitative analysis of dose-effect relationships: the combined effects of multiple drugs or enzyme inhibitors. Adv Enzyme Regul. 1984;22:27–55. doi:10.1016/0065-2571(84)90007-4
163. Ianevski A, He L, Aittokallio T, Tang J. SynergyFinder: a web application for analyzing drug combination dose-response matrix data. Bioinformatics. 2017;33(15):2413–2415. doi:10.1093/bioinformatics/btx162
164. Meyer CT, Wooten DJ, Paudel BB, et al. Quantifying Drug Combination Synergy along Potency and Efficacy Axes. Cell Syst. 2019;8(2):97–108.e16. doi:10.1016/j.cels.2019.01.003
165. Huang S, Ding D, Lan T, et al. Multifunctional nanodrug performs sonodynamic therapy and inhibits TGF-β to boost immune response against colorectal cancer and liver metastasis. Acta Biomater. 2023;164:538–552. doi:10.1016/j.actbio.2023.04.001
166. Liang Y, Zhang M, Zhang Y, Zhang M. Ultrasound Sonosensitizers for Tumor Sonodynamic Therapy and Imaging: a New Direction with Clinical Translation. Molecules. 2023;28(18):6484. doi:10.3390/molecules28186484
167. Wan G, Chen X, Wang H, et al. Gene augmented nuclear-targeting sonodynamic therapy via Nrf2 pathway-based redox balance adjustment boosts peptide-based anti-PD-L1 therapy on colorectal cancer. J Nanobiotechnology. 2021;19(1):347. doi:10.1186/s12951-021-01094-x
168. Chen G, Xu Q, Feng Z, et al. Glutamine Antagonist Synergizes with Electrodynamic Therapy to Induce Tumor Regression and Systemic Antitumor Immunity. ACS Nano. 2022;16(1):951–962. doi:10.1021/acsnano.1c08544
169. Fucikova J, Kepp O, Kasikova L, et al. Detection of immunogenic cell death and its relevance for cancer therapy. Cell Death Dis. 2020;11(11):1013. doi:10.1038/s41419-020-03221-2
170. Alzeibak R, Mishchenko TA, Shilyagina NY, Balalaeva IV, Vedunova MV, Krysko DV. Targeting immunogenic cancer cell death by photodynamic therapy: past, present and future. J Immunother Cancer. 2021;9(1):e001926. doi:10.1136/jitc-2020-001926
171. Garg AD, Krysko DV, Verfaillie T, et al. A novel pathway combining calreticulin exposure and ATP secretion in immunogenic cancer cell death. EMBO J. 2012;31(5):1062–1079. doi:10.1038/emboj.2011.497
172. Yang S, Jiao X, Lou X, et al. Image-guided therapy of colorectal cancer using a zirconium coordinated nanosensitizer. J Nanobiotechnology. 2025;23(1):732. doi:10.1186/s12951-025-03757-5
173. Turubanova VD, Balalaeva IV, Mishchenko TA, et al. Immunogenic cell death induced by a new photodynamic therapy based on photosens and photodithazine. J Immunother Cancer. 2019;7(1):350. doi:10.1186/s40425-019-0826-3
174. Miao X, Zhang Y, Li Z, et al. Inhibition of indoleamine 2,3-dioxygenase 1 synergizes with oxaliplatin for efficient colorectal cancer therapy. Mol Ther Methods Clin Dev. 2021;20:442–450. doi:10.1016/j.omtm.2020.12.013
175. De Silva M, Tse BCY, Diakos CI, Clarke S, Molloy MP. Immunogenic cell death in colorectal cancer: a review of mechanisms and clinical utility. Cancer Immunol Immunother. 2024;73(3):53. doi:10.1007/s00262-024-03641-5
176. Ou P, Wen L, Ni H, Yang CY. In Vivo and In Vitro Assay to Address Dendritic Cell Antigen Cross-Presenting Capacity. Methods Mol Biol. 2023;2618:239–249. doi:10.1007/978-1-0716-2938-3_17
177. Liu X, Chen F, Saeed M, et al. In-situ vaccination immunotherapy of colorectal cancer with STING agonist-integrated supramolecular nanovectors. Nano Today. 2024;56:102273. doi:10.1016/j.nantod.2024.102273
178. Zhang S, Zhang H, Cao Y, et al. Triple-pathway cGAS-STING activation collaborated with ferroptosis-induced immunogenic cell death for boosting systemic colorectal cancer immunotherapy. Nano Today. 2024;59:102484. doi:10.1016/j.nantod.2024.102484
179. Wu Q, Ren H, Xi B, Zhang J, Chen Y, Yu M. Sono-catalytic nanorod-adjuvanted in situ cancer vaccines augment antitumor T cell immunity through potentiated immunomodulation. Mater Chem Front. 2026;10(5):790–799. doi:10.1039/D5QM00746A
180. Zhou Y, Zhang W, Wang B, et al. Mitochondria-targeted photodynamic therapy triggers GSDME-mediated pyroptosis and sensitizes anti-PD-1 therapy in colorectal cancer. J Immunother Cancer. 2024;12(3):e008054. doi:10.1136/jitc-2023-008054
181. Hao Y, Chung CK, Gu Z, et al. Combinatorial therapeutic approaches of photodynamic therapy and immune checkpoint blockade for colon cancer treatment. Mol Biomed. 2022;3(1):26. doi:10.1186/s43556-022-00086-z
182. Xiao Y, Zhu T, Zeng Q, Tan Q, Jiang G, Huang X. Functionalized biomimetic nanoparticles combining programmed death-1/programmed death-ligand 1 blockade with photothermal ablation for enhanced colorectal cancer immunotherapy. Acta Biomater. 2023;157:451–466. doi:10.1016/j.actbio.2022.11.043
183. Zheng B, Wang H, Zhai S, Li J, Lu K. Mitochondria-targeted photothermal-chemodynamic therapy enhances checkpoint blockade immunotherapy on colon cancer. Mater Today Bio. 2025;31:101542. doi:10.1016/j.mtbio.2025.101542
184. Zhang J, Lu T, Jia R, et al. Nano-enabled combinatorial immunotherapy of colorectal cancer via small molecular PD-L1 blockade and photodynamic therapy. Mater Des. 2025;260:115185. doi:10.1016/j.matdes.2025.115185
185. Diaz LA, Shiu KK, Kim TW, et al. Pembrolizumab versus chemotherapy for microsatellite instability-high or mismatch repair-deficient metastatic colorectal cancer (KEYNOTE-177): final analysis of a randomised, open-label, Phase 3 study. Lancet Oncol. 2022;23(5):659–670. doi:10.1016/S1470-2045(22)00197-8
186. Bracken-Clarke D, Pastor DM, Marté JL, et al. The quadruple immunotherapy for colorectal cancer (QuICC) trial for mismatch repair-proficient metastatic colorectal cancer. oncologist. 2026;31(3):oyag008. doi:10.1093/oncolo/oyag008
187. Chen S, Wang Z, Sun P, Liu Y. Succinate-mediated SUCNR1 activation in tumor-associated macrophages promotes M2 polarization and cetuximab resistance in colorectal cancer: in vitro and in vivo insights. Apoptosis Int J Program Cell Death. 2026;31(1):22. doi:10.1007/s10495-025-02239-1
188. Wei Y, Chen Z, Zhu W, et al. Chimeric peptide-engineered photodynamic PD-L1 degrader for activating colorectal cancer immunity in combination with exosomal PD-L1 inhibition. Sci China Mater. 2025;68(8):2928–2939. doi:10.1007/s40843-025-3431-y
189. Guven DC, Kavgaci G, Erul E, et al. The Efficacy of Immune Checkpoint Inhibitors in Microsatellite Stable Colorectal Cancer: a Systematic Review. oncologist. 2024;29(5):e580–e600. doi:10.1093/oncolo/oyae013
190. Zhao Z, Dong S, Liu Y, et al. Tumor Microenvironment-Activable Manganese-Boosted Catalytic Immunotherapy Combined with PD-1 Checkpoint Blockade. ACS Nano. 2022;16(12):20400–20418. doi:10.1021/acsnano.2c06646
191. Mortezaee K, Majidpoor J, Kharazinejad E. The impact of hypoxia on tumor-mediated bypassing anti-PD-(L)1 therapy. Biomed Pharmacother. 2023;162:114646. doi:10.1016/j.biopha.2023.114646
192. Shurin MR, Umansky V. Cross-talk between HIF and PD-1/PD-L1 pathways in carcinogenesis and therapy. J Clin Invest. 2022;132(9):e159473. doi:10.1172/JCI159473
193. Roux C, Jafari SM, Shinde R, et al. Reactive oxygen species modulate macrophage immunosuppressive phenotype through the up-regulation of PD-L1. Proc Natl Acad Sci U S A. 2019;116(10):4326–4335. doi:10.1073/pnas.1819473116
194. Liu C, Liao Y, Liu L, et al. Application of injectable hydrogels in cancer immunotherapy. Front Bioeng Biotechnol. 2023;11:1121887. doi:10.3389/fbioe.2023.1121887
195. Norouzi M, Nazari B, Miller DW. Injectable hydrogel-based drug delivery systems for local cancer therapy. Drug Discov Today. 2016;21(11):1835–1849. doi:10.1016/j.drudis.2016.07.006
196. Xiao Y, Gu Y, Qin L, et al. Injectable thermosensitive hydrogel-based drug delivery system for local cancer therapy. Colloids Surf B Biointerfaces. 2021;200:111581. doi:10.1016/j.colsurfb.2021.111581
197. Wang D, Liu J, Duan J, et al. Enrichment and sensing tumor cells by embedded immunomodulatory DNA hydrogel to inhibit postoperative tumor recurrence. Nat Commun. 2023;14(1):4511. doi:10.1038/s41467-023-40085-4
198. Mohaghegh N, Ahari A, Zehtabi F, et al. Injectable hydrogels for personalized cancer immunotherapies. Acta Biomater. 2023;172:67–91. doi:10.1016/j.actbio.2023.10.002
199. Fan DY, Tian Y, Liu ZJ. Injectable Hydrogels for Localized Cancer Therapy. Front Chem. 2019;7:675. doi:10.3389/fchem.2019.00675
200. Khaliq NU, Lee J, Kim Y, et al. Tumor cell loaded thermosensitive hydrogel for photodynamic therapy associated tumor antigens release. Biochim Biophys Acta Gen Subj. 2024;1868(11):130703. doi:10.1016/j.bbagen.2024.130703
201. Chen H, Qu H, Pan Y, Cheng W, Xue X. Manganese-coordinated nanoparticle with high drug-loading capacity and synergistic photo-/immuno-therapy for cancer treatments. Biomaterials. 2025;312:122745. doi:10.1016/j.biomaterials.2024.122745
202. Yin M, Mao L, Zhang X, et al. Biodegradable 3D Injectable Amino Acid Hydrogels Delivering Immune Adjuvant for Enhancing Immunotherapy in Colon Cancer. Cancer Sci. 2025;116(10):2846–2857. doi:10.1111/cas.70156
203. Marques AC, Costa PC, Velho S, Amaral MH. Injectable Poloxamer Hydrogels for Local Cancer Therapy. Gels. 2023;9(7):593. doi:10.3390/gels9070593
204. Joyce P, Allen CJ, Alonso MJ, et al. A translational framework to DELIVER nanomedicines to the clinic. Nat Nanotechnol. 2024;19(11):1597–1611. doi:10.1038/s41565-024-01754-7
205. Đorđević S, Gonzalez MM, Conejos-Sánchez I, et al. Current hurdles to the translation of nanomedicines from bench to the clinic. Drug Deliv Transl Res. 2022;12(3):500–525. doi:10.1007/s13346-021-01024-2
206. Song Y, Huang Y, Zhou F, Ding J, Zhou W. Macrophage-targeted nanomedicine for chronic diseases immunotherapy. Chin Chem Lett. 2022;33(2):597–612. doi:10.1016/j.cclet.2021.08.090
207. Lu JY, Zhou X, Yang J, et al. Migration inhibition and selective cytotoxicity of cobalt hydroxide nanosheets on different cancer cell lines. New J Chem. 2022;46(21):10289–10298. doi:10.1039/D2NJ01466A
208. Dasgupta A, Sofias AM, Kiessling F, Lammers T. Nanoparticle delivery to tumours: from EPR and ATR mechanisms to clinical impact. Nat Rev Bioeng. 2024;2(9):714–716. doi:10.1038/s44222-024-00203-3
209. Simelane NWN, Kruger CA, Abrahamse H. Targeted Nanoparticle Photodynamic Diagnosis and Therapy of Colorectal Cancer. Int J Mol Sci. 2021;22(18):9779. doi:10.3390/ijms22189779
210. Dudzik T, Domański I, Makuch S. The impact of photodynamic therapy on immune system in cancer - an update. Front Immunol. 2024;15:1335920. doi:10.3389/fimmu.2024.1335920
211. Lu S, Feng W, Yao X, et al. Microorganism-enabled photosynthetic oxygeneration and ferroptosis induction reshape tumor microenvironment for augmented nanodynamic therapy. Biomaterials. 2022;287:121688. doi:10.1016/j.biomaterials.2022.121688
212. Fan D, Cao Y, Cao M, Wang Y, Cao Y, Gong T. Nanomedicine in cancer therapy. Signal Transduct Target Ther. 2023;8(1):293. doi:10.1038/s41392-023-01536-y
213. Bonet-Aleta J, Hueso JL, Mosseri A, Santamaria J. Nanomedical approaches to deplete intracellular glutathione in oncology. Chem Sci. 2026;17(4):1911–1931. doi:10.1039/d5sc09556e
214. Xiong Y, Xiao C, Li Z, Yang X. Engineering nanomedicine for glutathione depletion-augmented cancer therapy. Chem Soc Rev. 2021;50(10):6013–6041. doi:10.1039/d0cs00718h
215. Han D, Hanawa N, Saberi B, Kaplowitz N. Mechanisms of liver injury. III. Role of glutathione redox status in liver injury. Am J Physiol Gastrointest Liver Physiol. 2006;291(1):G1–7. doi:10.1152/ajpgi.00001.2006
216. He Y, Wang Y, Wang L, Jiang W, Wilhelm S. Understanding nanoparticle-liver interactions in nanomedicine. Expert Opin Drug Deliv. 2024;21(6):829–843. doi:10.1080/17425247.2024.2375400
217. Zhang YN, Poon W, Tavares AJ, McGilvray ID, Chan WCW. Nanoparticle-liver interactions: cellular uptake and hepatobiliary elimination. J Control Release off J Control Release Soc. 2016;240:332–348. doi:10.1016/j.jconrel.2016.01.020
218. Skorzynski M, Krol M, Braniewska A. Hepatotoxicity of Nanoparticle-Based Anti-Cancer Drugs: insights into Toxicity and Mitigation Strategies. Int J Nanomed. 2025;20:11697–11715. doi:10.2147/IJN.S543433
219. Jiang S, Zhang Z, Mao Y, et al. Emerging nano-immunotherapeutic strategies achieve metastatic colorectal cancer precision therapy. J Nanobiotechnology. 2026;24(1):111. doi:10.1186/s12951-025-03933-7
220. Pallares RM, Consolino L, Wang A, et al. Targeting metastasis with nanomedicine. Nat Rev Bioeng. 2026;4(1):47–66. doi:10.1038/s44222-025-00358-7
221. Wang Y, Mo Y, Sun Y, et al. Intestinal nanoparticle delivery and cellular response: a review of the bidirectional nanoparticle-cell interplay in mucosa based on physiochemical properties. J Nanobiotechnology. 2024;22(1):669. doi:10.1186/s12951-024-02930-6
222. Qiao X, Bao L, Liu G, Cui X. Nanomaterial journey in the gut: from intestinal mucosal interaction to systemic transport. Nanoscale. 2024;16(41). doi:10.1039/d4nr02480j
223. O’Brien Laramy M, Foley DA, Pak RH, et al. Chemistry, manufacturing and controls strategies for using novel excipients in lipid nanoparticles. Nat Nanotechnol. 2025;20(3):331–344. doi:10.1038/s41565-024-01833-9
224. Emily M, Ioanna N, Scott B, Beat F. Reflections on FDA Draft Guidance for Products Containing Nanomaterials: is the Abbreviated New Drug Application (ANDA) a Suitable Pathway for Nanomedicines? AAPS J. 2018;20(5):92. doi:10.1208/s12248-018-0255-0
225. Kara A, Ongoren B, Anaya BJ, Lalatsa A, Serrano DR. Continuous manufacturing of nanomedicines using 3D-printed microfluidic devices. Appl Mater Today. 2025;43:102672. doi:10.1016/j.apmt.2025.102672
226. Ye LY, Li YS, Ge T, et al. Engineered Luminescent Oncolytic Vaccinia Virus Activation of Photodynamic-Immune Combination Therapy for Colorectal Cancer. Adv Healthc Mater. 2024;13(17):e2304136. doi:10.1002/adhm.202304136
227. Babl N, Decking SM, Voll F, et al. MCT4 blockade increases the efficacy of immune checkpoint blockade. J Immunother Cancer. 2023;11(10):e007349. doi:10.1136/jitc-2023-007349
228. Reeves KM, Song PN, Angermeier A, et al. 18F-FMISO PET Imaging Identifies Hypoxia and Immunosuppressive Tumor Microenvironments and Guides Targeted Evofosfamide Therapy in Tumors Refractory to PD-1 and CTLA-4 Inhibition. Clin Cancer Res. 2022;28(2):327–337. doi:10.1158/1078-0432.CCR-21-2394
229. Sun J, Zhao Z, Lu J, et al. The Tumor Microenvironment Mediates the HIF-1α/PD-L1 Pathway to Promote Immune Escape in Colorectal Cancer. Int J Mol Sci. 2024;25(7):3735. doi:10.3390/ijms25073735
230. Pagès F, Mlecnik B, Marliot F, et al. International validation of the consensus Immunoscore for the classification of colon cancer: a prognostic and accuracy study. Lancet. 2018;391(10135):2128–2139. doi:10.1016/S0140-6736(18)30789-X
231. Angell HK, Bruni D, Barrett JC, Herbst R, Galon J. The Immunoscore: colon Cancer and Beyond. Clin Cancer Res. 2020;26(2):332–339. doi:10.1158/1078-0432.CCR-18-1851
232. Bruni D, Angell HK, Galon J. The immune contexture and Immunoscore in cancer prognosis and therapeutic efficacy. Nat Rev Cancer. 2020;20(11):662–680. doi:10.1038/s41568-020-0285-7
233. Winifred Nompumelelo Simelane N, Abrahamse H. Nanoparticle-Mediated Delivery Systems in Photodynamic Therapy of Colorectal Cancer. Int J Mol Sci. 2021;22(22):12405. doi:10.3390/ijms222212405
234. de Vlieger JSB, Crommelin DJA, Tyner K, et al. Report of the AAPS Guidance Forum on the FDA Draft Guidance for Industry: “Drug Products, Including Biological Products, that Contain Nanomaterials. AAPS J. 2019;21(4):56. doi:10.1208/s12248-019-0329-7
235. de Souza Cardoso Delfino C, de Paula Pereira MC, Dos Santos Oliveira M, et al. Scaling nanopharmaceutical production for personalized medicine: challenges and strategies. J Nanopart Res. 2025;27(4):108. doi:10.1007/s11051-025-06293-3
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Overexpression of TREM1 is Associated with the Immune-Suppressive Microenvironment and Unfavorable Prognosis in Pan-Cancer
Zhou X, Lin K, Fu L, Liu F, Lin H, Chen Y, Zhuang B, Liang H, Deng Q, Wang Z, Chen W, Luo J, Cao J, Li P
Journal of Inflammation Research 2023, 16:1375-1391
Published Date: 27 March 2023
Exploring the Correlation Between GPR176, a Potential Target Gene of Gastric Cancer, and Immune Cell Infiltration
Gu X, Shen H, Xiang Z, Li X, Zhang Y, Zhang R, Su F, Wang Z
Pharmacogenomics and Personalized Medicine 2023, 16:519-535
Published Date: 1 June 2023
Integrating Bulk and Single-Cell RNA Sequencing Reveals Heterogeneity, Tumor Microenvironment, and Immunotherapeutic Efficacy Based on Sialylation-Related Genes in Bladder Cancer
Tan Z, Chen X, Zuo J, Fu S, Wang J, Wang H
Journal of Inflammation Research 2023, 16:3399-3417
Published Date: 14 August 2023
The Role of Bacterial Outer Membrane Vesicles in Tumor Development: Facts, Potential Applications and Future Perspectives
Gu Z, Zhang M, Shen F, Chen J, Gu Y, Gong Y, Xue Q, Zhou H, Liu Y, Shao S, Zhang Y, Bai J, Hua K, Zhou G, Ding J
International Journal of Nanomedicine 2026, 21:582600
Published Date: 11 March 2026
Mechanisms and Emerging Strategies to Overcome Immunotherapy Resistance in Cold Tumours of Colorectal Cancer
Zhu X, Ge B, Wen L
OncoTargets and Therapy 2026, 19:621109
Published Date: 15 June 2026