Back to Journals » OncoTargets and Therapy » Volume 19
Mechanisms and Emerging Strategies to Overcome Immunotherapy Resistance in Cold Tumours of Colorectal Cancer
Received 30 April 2026
Accepted for publication 6 June 2026
Published 15 June 2026 Volume 2026:19 621109
DOI https://doi.org/10.2147/OTT.S621109
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr John Maher
Xinqiang Zhu,1,* Beibei Ge,1,* Linchun Wen2
1Department of General Surgery The Affiliated Suqian Hospital of Xuzhou Medical University, Suqian, Jiangsu, 223800, People’s Republic of China; 2Department of Oncology, The Affiliated Suqian Hospital of Xuzhou Medical University, Suqian, Jiangsu, 223800, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xinqiang Zhu, Email [email protected]
Abstract: Immunotherapy in colorectal cancer (CRC) presents a striking dichotomy. MSS/pMMR tumors account for approximately 95% of metastatic CRC cases, representing a substantial global health burden. While immune checkpoint inhibitors (ICIs) have revolutionized treatment for mismatch repair-deficient/microsatellite instability-high (dMMR/MSI-H) metastatic CRC—achieving durable responses in tumors with high mutational burden and a T-cell-inflamed microenvironment—the majority of microsatellite stable (MSS) cases remain resistant. The MSS tumor microenvironment is typically “cold”, featuring low neoantigen load, poor T-cell infiltration, and dominant immunosuppressive networks. To overcome this resistance, extensive research is focused on combination strategies (ICIs with anti-angiogenic agents, targeted therapies, chemotherapy, radiotherapy) and next-generation modalities (adoptive cell therapies, bispecific antibodies, cancer vaccines). This review examines the biological basis for this dichotomy, summarizes clinical evidence in dMMR/MSI-H CRC, and critically assesses emerging strategies for MSS disease. We propose that future progress will likely depend on mechanism-based, biomarker-driven approaches that match specific immune evasion patterns with rationally designed interventions, with the goal of extending immunotherapy benefits to broader CRC populations. This narrative review synthesizes peer-reviewed literature from PubMed and clinical trial registries (2015– 2025), prioritizing Phase II/III trials and mechanistic studies.
Keywords: colorectal cancer, immunotherapy, immune checkpoint inhibitors, microsatellite instability, tumor microenvironment, combination therapy, biomarkers
Introduction
Colorectal cancer (CRC) remains a leading cause of cancer-related mortality worldwide.1 Globally, CRC accounts for nearly 1.9 million new cases and over 900,000 deaths annually,2 with metastatic disease carrying a 5-year survival rate below 15%.3,4 For decades, the therapeutic arsenal for metastatic CRC (mCRC) has been dominated by cytotoxic chemotherapy and biologic agents targeting angiogenesis and the epidermal growth factor receptor.5,6 While these treatments have improved outcomes, responses are often transient and long-term survival remains limited.
The emergence of cancer immunotherapy,7 particularly immune checkpoint inhibitors (ICIs),8 has reshaped treatment for many malignancies.9 However, in CRC, ICIs have revealed a striking dichotomy. Their efficacy is almost exclusively confined to the small subset (≈4–5%) of patients with mismatch repair-deficient/microsatellite instability-high (dMMR/MSI-H) tumors.10 These “immunologically hot” tumors are sensitive to PD-1/PD-L1 blockade, demonstrating durable responses. In contrast, the vast majority of patients with microsatellite stable (MSS) or mismatch repair-proficient (pMMR) tumors exhibit primary resistance to single-agent ICIs, their “cold” immunological landscape posing a formidable challenge.11,12
The biological basis of this dichotomy lies in distinct tumor microenvironment (TME) features. dMMR/MSI-H tumors have high mutational burden, abundant neoantigens, and dense CD8⁺ T-cell infiltration, whereas MSS/pMMR tumors are characterized by low mutational burden, T-cell exclusion, and dominance of immunosuppressive cells such as myeloid-derived suppressor cells and M2-polarized macrophages.12,13 Consequently, ICIs are standard of care in dMMR/MSI-H mCRC, while no immunotherapy has yet been approved for MSS/pMMR disease.
Methods:This narrative review searched PubMed and ClinicalTrials.gov for articles published between January 2015 and December 2025 using terms including “colorectal cancer”, “immunotherapy”, “immune checkpoint inhibitors”, “MSS”, “pMMR”, “tumor microenvironment”, and “combination therapy”. We prioritized phase II/III trials, high-impact mechanistic studies, and recent systematic reviews. References from selected articles were hand-searched for additional relevant studies.
This review dissects the biological basis for this dichotomy, summarizes landmark clinical data in dMMR/MSI-H CRC, and critically evaluates strategies to overcome resistance in MSS CRC.
The dMMR/MSI-H Subset: A Paradigm for Immunotherapy Success
Biological Rationale: An Immunogenic Phenotype
The profound efficacy of ICIs in dMMR/MSI-H CRC is underpinned by its distinct tumor biology.10 The dMMR system, responsible for correcting DNA replication errors, is functionally impaired, leading to a hypermutator phenotype. This results in a very high tumor mutational burden (TMB),12 with thousands of somatic mutations accumulating, particularly in coding microsatellite regions. These mutations frequently generate novel frameshift peptides, which serve as highly immunogenic neoantigens. These neoantigens are efficiently presented on major histocompatibility complex (MHC) molecules, leading to the priming and activation of a robust, tumor-specific T-cell response.14 Consequently, dMMR/MSI-H tumors are characterized by a pre-existing, T-cell-inflamed tumor microenvironment (TME), with dense infiltration of CD8+ cytotoxic T-cells15 and increased expression of immune checkpoint molecules like PD-1 and PD-L1. This adaptive immune resistance mechanism creates the perfect conditions for ICIs to act, by “releasing the brakes” on an already engaged anti-tumor immune response.16
Clinical Efficacy and Evolving Standards of Care
The translation of this biology into clinical practice has been transformative. Pivotal Phase II trials, such as KEYNOTE-164 and CheckMate-142,17,18 demonstrated unprecedented activity of pembrolizumab and nivolumab (alone or combined with ipilimumab) in previously treated metastatic dMMR/MSI-H CRC, with objective response rates (ORR) of 40–55% and, critically, remarkably durable responses.17,18 This led to regulatory approvals and established ICIs as the standard of care in the refractory setting.10
The paradigm was further shifted by the Phase III KEYNOTE-177 trial,19 which compared pembrolizumab to standard chemotherapy as first-line treatment.20 The study met its primary endpoint, demonstrating a significant improvement in median progression-free survival (16.5 vs. 8.2 months) with a more favorable toxicity profile.21 Based on these results, frontline pembrolizumab is now a standard first-line option, offering the potential for long-term disease control without the cumulative toxicities of chemotherapy.
More recently, the power of ICIs has been demonstrated in the neoadjuvant setting. Several landmark studies in locally advanced dMMR rectal cancer have reported a 100% clinical complete response rate22 to neoadjuvant dostarlimab or other ICIs, allowing patients to avoid radical surgery and preserve organ function.22,23 This has ignited a new era of treatment for early-stage dMMR CRC.
The MSS/pMMR Majority: Confronting the “Cold” Tumor Challenge
It is important to note, however, that MSS CRC is not entirely homogeneous. Rare cases with POLE or POLD1 exonuclease domain mutations can exhibit ultra-high TMB and, despite being microsatellite stable, have shown responsiveness to immune checkpoint inhibitors in case series and small cohort studies. Similarly, a small fraction of MSS tumors with exceptionally high TMB through alternative mechanisms may also derive clinical benefit. Although these represent a minority of MSS cases, acknowledging this heterogeneity improves the scientific accuracy of the review.
The primary obstacle in CRC immunotherapy is the inherent resistance of MSS/pMMR tumors, which constitute over 95% of metastatic cases. The immunobiology of these tumors is characterized by multiple layers of immunosuppression12 (Table 1).
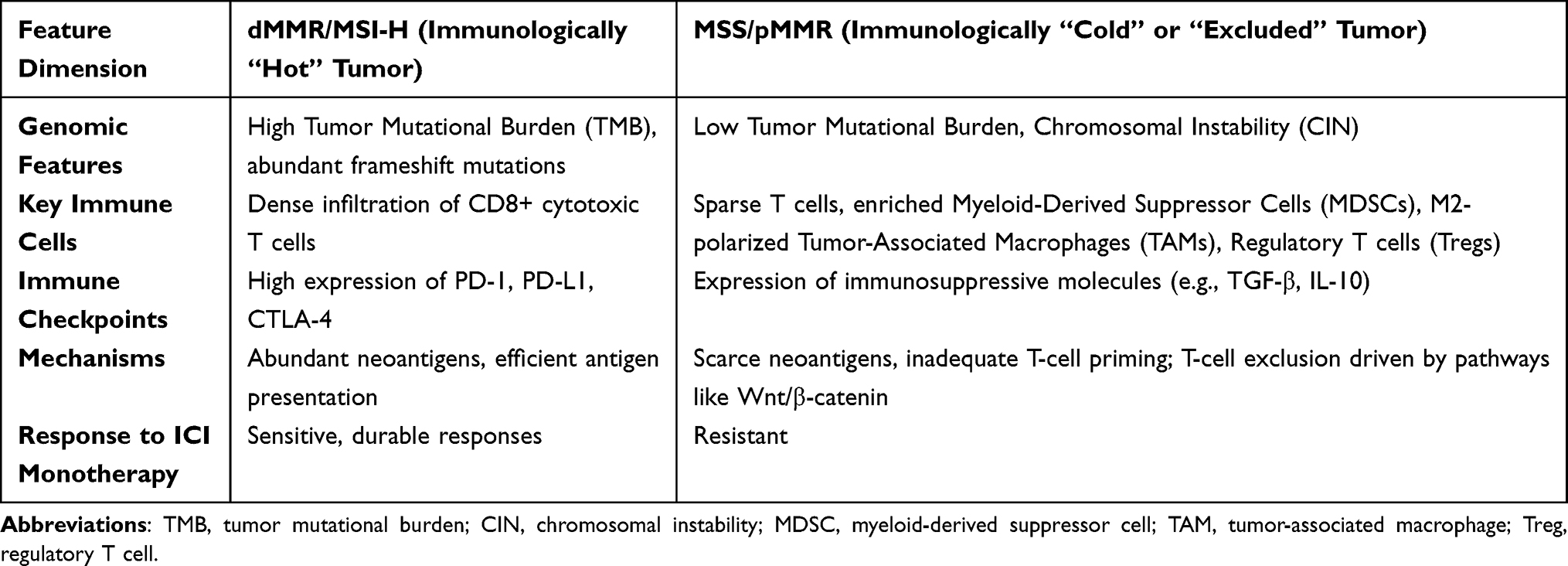 |
Table 1 Comparison of Tumor Immune Microenvironment Characteristics Between dMMR/MSI-H and MSS/pMMR Colorectal Cancer |
Mechanisms of Immunoresistance
The MSS phenotype is associated with low TMB and scarce neoantigens, resulting in inadequate T-cell priming.24 Beyond this lack of immunogenicity, the TME is profoundly immunosuppressive. It is often infiltrated by myeloid-derived suppressor cells (MDSCs)25 and M2-polarized tumor-associated macrophages (TAMs),12,13 which secrete inhibitory cytokines (IL-10, TGF-β) that suppress T-cell function.26,27 Regulatory T-cells (Tregs) are also abundant, contributing to local immune tolerance.12,28
A key feature of many MSS CRCs is T-cell exclusion, where cytotoxic T-cells are physically prevented from infiltrating the tumor core. This “immune-excluded” phenotype is often driven by Wnt/β-catenin activation, which may inhibit recruitment of CD103⁺ dendritic cells needed for T-cell priming and trafficking.29,30 Additionally, VEGF, commonly overexpressed in CRC, promotes abnormal vasculature that limits T-cell entry.
These resistance mechanisms often co-exist, creating a complex immunosuppressive landscape. Each mechanism represents a potential therapeutic vulnerability: T-cell exclusion may be targeted by pathway inhibitors or epigenetic modifiers; MDSC/M2 TAM dominance suggests a rationale for CSF-1R inhibitors or myeloid-targeting agents; and immunosuppressive cytokines like TGF-β may be neutralized by specific antibodies. This understanding underpins the rational combination strategies discussed below.
Established Immune Biomarkers in MSS CRC
Several immune-related biomarkers have prognostic value in CRC and may help guide immunotherapy patient selection.
Immunoscore® quantifies CD3⁺ and CD8⁺ T-cell densities in the tumor core and invasive margin; it has been validated as a strong prognostic factor in stage I–III CRC and is being explored for predicting ICI response in MSS tumors.31,32
Tumor-stroma ratio (TSR) assesses the proportion of stroma versus tumor cells; a stroma-rich phenotype correlates with immune exclusion, poor CD8⁺ infiltration, and worse prognosis in CRC.33,34
CD8⁺ T-cell localization classifies tumors as inflamed, excluded, or desert. Most MSS CRCs show excluded or desert phenotypes, which are associated with primary ICI resistance.35,36
Gut microbiome composition modulates systemic antitumor immunity. Specific bacteria (eg., Akkermansia) have been linked to improved ICI efficacy, and fecal profiling is emerging as a non-invasive biomarker in CRC.37,38
Integrating these complementary biomarkers into future trials may enable biologically guided patient stratification (Figure 1).
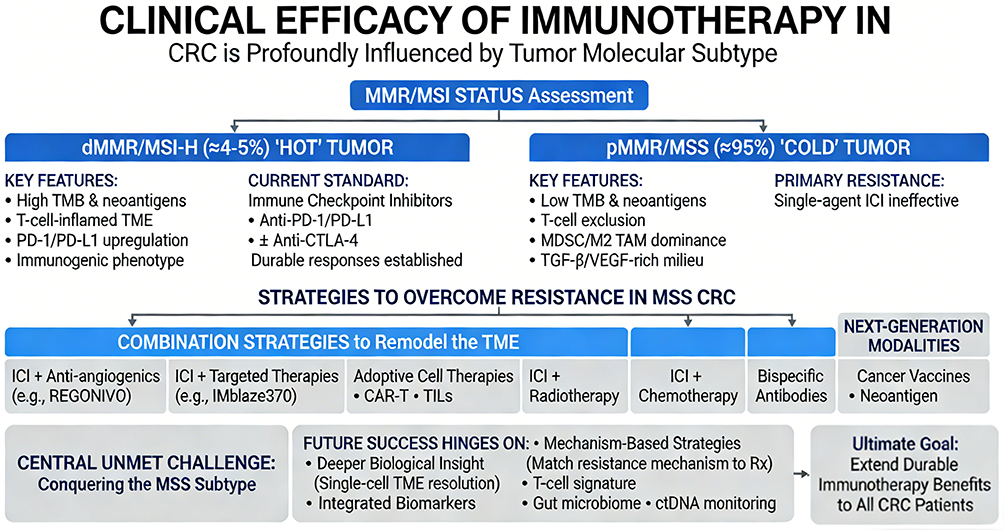 |
Figure 1 Immunotherapy landscape and therapeutic framework in colorectal cancer (CRC). Immunotherapy efficacy in CRC is dictated by MMR/MSI status. dMMR/MSI-H “hot” tumors (≈4–5%) are ICI-sensitive; pMMR/MSS “cold” tumors (≈95%) are resistant. Strategies to overcome resistance include combination TME-remodeling approaches and next-generation immunotherapies. |
Strategies to Sensitize MSS Colorectal Cancer to Immunotherapy
Overcoming the intrinsic resistance of MSS CRC requires a paradigm shift from empirical combination testing to mechanism-based strategies that target specific barriers within the immunosuppressive tumor microenvironment (TME). The heterogeneous nature of immune evasion in MSS tumors—ranging from T-cell exclusion and myeloid cell dominance to soluble immunosuppressive factors—demands a tailored approach that matches the dominant resistance mechanism with rationally selected interventions. This section systematically reviews emerging strategies organized by their primary mechanistic target, providing a framework for personalized immunotherapy in MSS CRC.
Targeting T-Cell Exclusion and Immune Desert Phenotypes
A subset of MSS CRCs exhibits an “immune-desert” or “immune-excluded” phenotype, characterized by the absence of T-cells within the tumor core despite their presence at the invasive margin or in surrounding stroma. This T-cell exclusion is often driven by oncogenic signaling pathways that actively prevent lymphocyte infiltration.
The Wnt/β-catenin pathway represents a prominent mechanism of immune exclusion. Constitutive activation of this pathway, frequently resulting from APC or CTNNB1 mutations, suppresses the production of CCL4, a chemokine essential for recruiting CD103+ dendritic cells. Without these dendritic cells, T-cell priming and subsequent trafficking into the tumor core are severely impaired.29,39 Preclinical studies have demonstrated that pharmacological inhibition of Wnt/β-catenin signaling can restore chemokine expression, enhance dendritic cell recruitment, and sensitize tumors to immune checkpoint blockade. Several small molecule inhibitors targeting this pathway are currently in early-phase clinical development, though their tolerability and efficacy in combination with ICIs remain to be established.
Epigenetic modifiers represent another avenue for reversing immune exclusion. DNA methyltransferase inhibitors (eg., decitabine) and histone deacetylase inhibitors (eg., vorinostat) have been shown to upregulate the expression of endogenous retroviral elements, triggering a viral mimicry response that enhances tumor immunogenicity and promotes T-cell infiltration.40 Early-phase trials combining epigenetic agents with ICIs in solid tumors have shown promising signals, though data specific to MSS CRC are still emerging.
For tumors with true immune-desert phenotypes—those lacking any evidence of a pre-existing T-cell response—therapeutic vaccines may be necessary to initiate de novo T-cell priming. Personalized neoantigen vaccines, generated by sequencing a patient’s tumor to identify mutation-derived immunogenic peptides, have demonstrated the ability to induce polyfunctional, tumor-specific T-cell responses in melanoma and other cancers.24,41 In MSS CRC, early-phase studies are exploring neoantigen vaccines alone or in combination with ICIs, with the goal of creating an initial T-cell infiltrate that can then be unleashed by checkpoint blockade.42
Remodeling the Immunosuppressive Myeloid Compartment
Myeloid cells dominate the immunosuppressive network in MSS CRC. MDSCs and M2-polarized TAMs accumulate abundantly and suppress T-cells via arginase, reactive oxygen species, and inhibitory cytokines.12,13,25
CSF-1R targeting aims to deplete or reprogram TAMs. Preclinical studies suggest CSF-1R inhibitors can reduce TAM density, shift macrophages toward an M1-like phenotype, and enhance ICI efficacy.13 Clinical trials of CSF-1R inhibitors (eg., cabiralizumab, pexidartinib) combined with ICIs in advanced solid tumors, including CRC, have shown mixed results, possibly reflecting redundancy within the myeloid network.
Inhibiting myeloid recruitment is an alternative. CCR2 and CCR5 on MDSC precursors mediate their trafficking into tumors. Small molecule inhibitors of these chemokine receptors are being evaluated to prevent MDSC accumulation and relieve T-cell suppression.27
PI3Kγ regulates macrophage polarization. PI3Kγ signaling promotes an M2-like phenotype; preclinical data indicate that PI3Kγ inhibition can reprogram TAMs toward an M1-like, immunostimulatory state, enhancing CD8⁺ T-cell activation and ICI sensitivity.43 Selective PI3Kγ inhibitors are entering clinical development as a strategy to “re-educate” rather than deplete myeloid cells.
Counteracting Soluble Immunosuppressive Factors
The MSS TME is rich in soluble factors that directly suppress effector immune cells and promote a tolerogenic milieu. Among these, transforming growth factor-beta (TGF-β) and vascular endothelial growth factor (VEGF) play particularly prominent roles.
TGF-β exerts pleiotropic immunosuppressive effects: it inhibits the proliferation and effector function of CD8+ T-cells and NK cells, promotes the differentiation of regulatory T-cells (Tregs), and drives the activation of cancer-associated fibroblasts (CAFs) that deposit extracellular matrix and create a physical barrier to T-cell infiltration.26 Preclinical studies have demonstrated that TGF-β blockade can reverse these effects, enhancing T-cell infiltration and synergizing with ICIs. Several TGF-β receptor kinase inhibitors and ligand-trapping molecules are in clinical development. Notably, a phase Ib trial combining the TGF-β inhibitor galunisertib with nivolumab in advanced solid tumors showed acceptable safety and signals of clinical activity, though dedicated studies in MSS CRC are needed.
VEGF, in addition to its well-established role in promoting angiogenesis, is a potent immunosuppressive cytokine. VEGF inhibits dendritic cell maturation, promotes the expansion of MDSCs and Tregs, and contributes to the formation of abnormal, leaky vasculature that impedes effective T-cell trafficking.44,45 These observations provide a strong rationale for combining anti-angiogenic agents with ICIs—a strategy that aims to achieve “vascular normalization,” improving both drug delivery and immune cell infiltration while directly counteracting VEGF-mediated immunosuppression.
The clinical exploration of this approach has yielded both promise and complexity. The phase Ib REGONIVO trial evaluated regorafenib (a multi-kinase inhibitor with anti-angiogenic activity) in combination with nivolumab in patients with advanced gastric and colorectal cancer. In the MSS CRC cohort, the combination achieved an objective response rate of 33%, a striking signal given the historical resistance of MSS CRC to immunotherapy.46 However, subsequent larger studies have failed to consistently replicate this efficacy, suggesting that patient selection, dosing schedules, and the specific anti-angiogenic agent used may critically influence outcomes. Ongoing phase III trials, such as the LEAP-017 study evaluating lenvatinib plus pembrolizumab, will provide more definitive evidence.
The failure of the phase III IMblaze370 trial—which evaluated the MEK inhibitor cobimetinib combined with atezolizumab in previously treated MSS CRC—serves as an important cautionary tale.47 Despite a strong preclinical rationale (MEK inhibition was thought to enhance antigen presentation and reduce MDSC accumulation), the combination failed to improve survival compared to regorafenib alone. This outcome underscores several critical lessons: the complex, sometimes counterproductive immunomodulatory effects of targeted agents; the importance of patient selection; and the need for robust predictive biomarkers to guide combination development.48
Enhancing Effector Cell Function and Persistence
The ultimate goal of immunotherapy is to generate and maintain a robust, tumor-specific effector T-cell response. For tumors where such a response exists but is suppressed, ICIs alone may suffice. For MSS CRC, however, strategies that directly provide or enhance effector cells are increasingly being explored.
Adoptive cell therapy (ACT) represents one of the most powerful approaches to generate anti-tumor immunity. Tumor-infiltrating lymphocyte (TIL) therapy involves isolating T-cells from a patient’s resected tumor, expanding them ex vivo to large numbers, and reinfusing them following lymphodepleting chemotherapy.49,50 This approach has achieved remarkable success in melanoma, with durable response rates exceeding 50%. In MSS CRC, early-phase TIL trials are now showing promising signals of activity, with objective responses observed in a subset of patients with liver metastases.50 The major challenges include the technical complexity of TIL expansion and the variable presence of pre-existing tumor-reactive T-cells within individual tumors.51
Chimeric antigen receptor (CAR) T-cell therapy has transformed the treatment of hematologic malignancies but faces substantial hurdles in solid tumors like CRC.13 These challenges include: (1) a paucity of truly tumor-specific antigens that are uniformly expressed across all tumor cells; (2) on-target/off-tumor toxicity when targeting antigens shared with normal tissues; and (3) a hostile TME that rapidly inactivates infused CAR-T cells through immunosuppressive signals, metabolic restriction, and physical barriers.8,52
Despite these obstacles, early-phase clinical trials are providing initial evidence that CAR-T cells can exert biological activity in CRC with an acceptable safety profile. In a Phase I dose-escalation study reported by Zhang C et al 10 heavily pretreated CRC patients received CAR-T cell therapy targeting a tumor-associated antigen across five dose levels (1×105 to 1×108 CAR+ cells/kg). The therapy was well-tolerated with no severe treatment-related adverse events attributable to CAR-T cells. Notably, among the 7 patients who had experienced progressive disease on all prior standard therapies, CAR-T infusion resulted in disease stabilization, with 2 patients maintaining stable disease for over 30 weeks and 2 others showing objective tumor reduction on PET/CT and MRI.53 This emerging data, while preliminary, validates the potential of CAR-T therapy in CRC and provides proof-of-concept that adoptively transferred cells can traffic to tumors and exert anti-tumor effects even in the challenging MSS TME.
Strategies to enhance CAR-T cell efficacy in solid tumors include engineering “armored” CARs that constitutively secrete immunostimulatory cytokines (eg., IL-12, IL-18) to counteract the suppressive TME; designing logic-gated CARs that require recognition of two antigens for activation, thereby improving tumor specificity; and combining CAR-T cells with ICIs or TME-modulating agents to create a more permissive environment for their function.52
Bispecific T-cell engagers (BiTEs) offer an alternative strategy to redirect T-cell cytotoxicity without the need for ex vivo cell manipulation. These antibody-based molecules simultaneously bind a tumor-associated antigen (eg., carcinoembryonic antigen, CEA) and the CD3 complex on T-cells, effectively forcing the formation of an immunological synapse and inducing T-cell activation and tumor cell killing.54,55 The CEA-CD3 bispecific antibody cibisatamab has shown encouraging activity in early-phase trials, particularly when combined with atezolizumab, though cytokine release syndrome (CRS) remains a dose-limiting toxicity requiring careful management55 (Table 2).
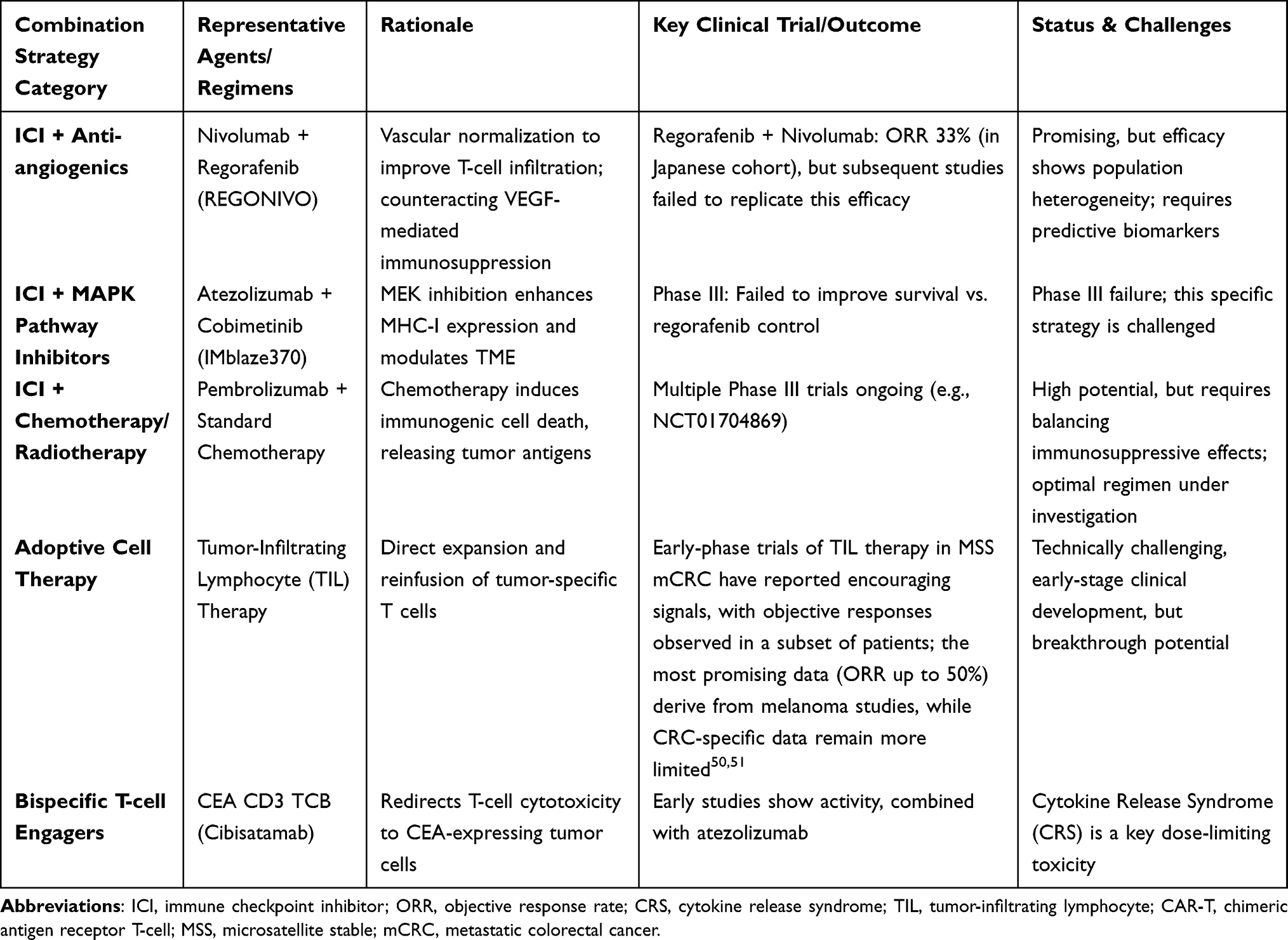 |
Table 2 Summary of Immunotherapy Combination Strategies and Key Clinical Trials for MSS Colorectal Cancer |
Other Emerging Modalities
STING agonists activate the cGAS-STING pathway to induce type I interferons and T-cell priming. In CRC, activation of this pathway can enhance anti-tumor immunity, but its dual role in promoting intestinal inflammation underscores the need for precise delivery.56 Preclinical studies have shown that combining a WIP1 inhibitor with a STING agonist synergistically enhances anti-tumor efficacy by amplifying IFNβ production to activate anti-tumor immune responses.57 Dazostinag (TAK-676), a STING agonist, is being evaluated with pembrolizumab for colorectal cancer (iintune-1, NCT04420884).58
Oncolytic viruses selectively replicate in malignant cells and mediate anti-tumor effects through direct oncolysis, immune activation, and modulation of tumor angiogenesis.59 In KRAS-mutant MSS mCRC, the oncolytic reovirus pelareorep combined with FOLFIRI/bevacizumab achieved partial responses in 3 of 6 patients, with median PFS of 65.6 weeks and OS of 25.1 months.60 IVX037, a bioselected oncolytic RNA picornavirus targeting CD55 and FcRn, has shown encouraging activity in MSS-CRC and is being evaluated in combination with sintilimab (anti-PD-1) in a Phase Ib trial.61
Antibody-drug conjugates (ADCs) are emerging as immuno-oncology agents that can induce immunogenic cell death and convert cold tumors into hot ones.62 In HER2-positive MSS CRC, trastuzumab deruxtecan (T-DXd) demonstrated an objective response rate of 45.3% in heavily pretreated patients in the DESTINY-CRC01 trial.63 The DESTINY-CRC02 trial subsequently established 5.4 mg/kg as the preferred dose with a favorable benefit-risk profile.64
Limitations and Future Challenges
Several important limitations must be honestly acknowledged. First, most combination strategies discussed in this review—including ICI plus anti-angiogenics (beyond the REGONIVO signal), ICI plus MEK inhibition (IMblaze370), and ICI plus chemotherapy—have failed to demonstrate consistent survival benefits in phase III trials.46,47 Second, the majority of emerging modalities (CAR-T, TILs, bispecific antibodies, cancer vaccines) remain in early-phase development, with limited CRC-specific data and no mature survival outcomes.50,53,55 Third, predictive biomarkers for patient stratification are still lacking; no validated biomarker panel is available for routine clinical use in MSS CRC.35,65 Fourth, the inherent heterogeneity of MSS tumors—including rare but clinically relevant POLE/POLD1-mutated or high-TMB subsets—means that a “one-size-fits-all” strategy is unlikely to succeed.66 Overcoming these barriers will require better preclinical models (eg., patient-derived organoids, immune-humanized mice), biomarker-driven basket trials, and international collaborative consortia.67
Beyond tumor-intrinsic mechanisms, emerging evidence from molecular pathological epidemiology (MPE) indicates that long-term exposures—including genetic variants, dietary factors, lifestyle habits, and environmental agents—can shape tumor immune phenotypes over decades.68,69 The prospective cohort incident-tumor biobank method (PCIBM), recently applied to large longitudinal studies such as the UK Biobank, enables integration of pre-diagnosis exposure data with detailed tumor molecular and immune profiling.70 This approach holds promise for identifying modifiable risk factors that influence immune evasion patterns in CRC and for discovering novel biomarkers that predict immunotherapy response. Future studies applying PCIBM to MSS CRC may uncover opportunities for prevention and personalized treatment that extend beyond traditional therapeutic paradigms.
Through continued translational research and innovative trial designs that embed these principles, extending durable immunotherapy benefits to a broader population of CRC patients represents an active area of investigation with incremental progress.
Conclusion and Future Perspectives
Immunotherapy has substantially changed the treatment landscape for dMMR/MSI-H CRC, establishing a powerful new pillar of cancer care. However, it is critical to acknowledge that, despite extensive ongoing investigation, no immunotherapy approach has yet received regulatory approval for MSS/pMMR metastatic colorectal cancer.46,47 The mission to extend these benefits to patients with MSS CRC therefore remains one of the most pressing challenges in oncology.
The path forward is not reliant on a single solution but on a mechanism-based, biomarker-driven approach that recognizes the heterogeneity of immune evasion within MSS tumors. We propose a three-pronged framework for future progress:
First, deeper biological insight is needed to deconvolute the heterogeneous immunosuppressive networks within the MSS TME at single-cell resolution.
Second, clinical trial design must evolve from empirical combinations to biology-guided strategies that match specific resistance mechanisms (eg., T-cell exclusion, myeloid dominance) with rationally selected interventions.
Third, the development of integrated biomarkers—combining T-cell-inflamed gene signatures, gut microbiome profiling, dynamic ctDNA monitoring, and emerging tools such as Immunoscore®—is essential to identify the subset of MSS patients most likely to benefit from specific immunotherapy approaches.31,67
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Project of Natural Science Foundation of Suqian City in 2025, Project Number K202522. “Suqian Talents” Project Achievement Contribution Award, Project No. SQCG202506.
Disclosure
The authors declare that they have no competing interests.
References
1. Hetta HF, Elkady A, Yahia R. et al. T follicular helper and T follicular regulatory cells in colorectal cancer: a complex interplay. J Immunol Methods. 2020;480:112753. doi:10.1016/j.jim.2020.112753
2. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–11. doi:10.3322/caac.21834
3. Emile SH, Horesh N, Wignakumar A, Boutros M, Wexner SD. Advanced T stage and nodal disease are independently associated with worse cancer-specific survival in stage IV colorectal cancer: a SEER-based survival analysis. Eur J Surg Oncol. 2026;52(2):111315. doi:10.1016/j.ejso.2025.111315
4. Zeineddine FA, Zeineddine MA, Yousef A, et al. Survival improvement for patients with metastatic colorectal cancer over twenty years. NPJ Precis Oncol. 2023;7(1):16. doi:10.1038/s41698-023-00353-4
5. Vincenzi B, Zoccoli A, Pantano F, Venditti O, Galluzzo S. Cetuximab: from bench to bedside. Curr Cancer Drug Targets. 2010;10(1):80–95. doi:10.2174/156800910790980241
6. González Astorga B, Salvà Ballabrera F, Aranda Aguilar E, et al. Patient profiles as an aim to optimize selection in the second line setting: the role of aflibercept. Clin Transl Oncol. 2021;23(8):1520–1528. doi:10.1007/s12094-021-02568-y
7. Rui R, Zhou L, He S. Cancer immunotherapies: advances and bottlenecks. Front Immunol. 2023;14:1212476. doi:10.3389/fimmu.2023.1212476
8. Zhao W, Jin L, Chen P, Li D, Gao W, Dong G. Colorectal cancer immunotherapy-Recent progress and future directions. Cancer Lett. 2022;545:215816. doi:10.1016/j.canlet.2022.215816
9. Kraehenbuehl L, Weng CH, Eghbali S, Wolchok JD, Merghoub T. Merghoub T: enhancing immunotherapy in cancer by targeting emerging immunomodulatory pathways. Nat Rev Clin Oncol. 2022;19(1):37–50. doi:10.1038/s41571-021-00552-7
10. Zhang X, Wu T, Cai X, et al. Neoadjuvant Immunotherapy for MSI-H/dMMR Locally Advanced Colorectal Cancer: new Strategies and Unveiled Opportunities. Front Immunol. 2022;13:795972. doi:10.3389/fimmu.2022.795972
11. Ooki A, Shinozaki E, Yamaguchi K. Immunotherapy in Colorectal Cancer: current and Future Strategies. J Anus Rectum Colon. 2021;5(1):11–24. doi:10.23922/jarc.2020-064
12. Zou D, Xin X, Xu Y, Xu H, Huang L, Xu T. Improving the efficacy of immunotherapy for colorectal cancer: targeting tumor microenvironment-associated immunosuppressive cells. Heliyon. 2024;10(16):e36446. doi:10.1016/j.heliyon.2024.e36446
13. Chen E, Zhou W. Immunotherapy in microsatellite-stable colorectal cancer: strategies to overcome resistance. Crit Rev Oncol Hematol. 2025;212:104775. doi:10.1016/j.critrevonc.2025.104775
14. Kawazu M. Abnormalities of Major Histocompatibility Complex in Microsatellite Instability-High Colorectal Cancer. Gan to Kagaku Ryoho. 2021;48(10):1185–1190.
15. Cai T, Liang Z, Chen Z, et al. KDM4A-induced tumor senescence enhances the efficacy of immunotherapy by inhibiting AGT-PHB1 axis-mediated mitophagy in colorectal cancer. Autophagy. 2025;2025:1–22.
16. Heregger R, Huemer F, Steiner M, Gonzalez-Martinez A, Greil R, Weiss L. Unraveling Resistance to Immunotherapy in MSI-High Colorectal Cancer. Cancers. 2023;15(20):5090. doi:10.3390/cancers15205090
17. Lenz HJ, Van Cutsem E, Luisa Limon M, et al. First-Line Nivolumab Plus Low-Dose Ipilimumab for Microsatellite Instability-High/Mismatch Repair-Deficient Metastatic Colorectal Cancer: the Phase II CheckMate 142 Study. J Clin Oncol. 2022;40(2):161–170. doi:10.1200/JCO.21.01015
18. Le DT, Diaz Jr LA, Kim TW, et al. Pembrolizumab for previously treated, microsatellite instability-high/mismatch repair-deficient advanced colorectal cancer: final analysis of KEYNOTE-164. Eur J Cancer. 2023;186:185–195. doi:10.1016/j.ejca.2023.02.016
19. Kanani A, Veen T, Alexeeva M, Lea D, Søreide K. Neoadjuvant immunotherapy in colorectal cancer beyond immune checkpoint inhibitors: emerging from bench to bedside. Minerva Surg. 2023;78(4):385–400. doi:10.23736/S2724-5691.23.09854-4
20. Tan E, Sahin IH. Defining the current role of immune checkpoint inhibitors in the treatment of mismatch repair-deficient/microsatellite stability-high colorectal cancer and shedding light on future approaches. Expert Rev Gastroenterol Hepatol. 2021;15(7):735–742. doi:10.1080/17474124.2021.1886077
21. Diaz Jr LA, Shiu KK, Kim TW, et al. Pembrolizumab versus chemotherapy for microsatellite instability-high or mismatch repair-deficient metastatic colorectal cancer (KEYNOTE-177): final analysis of a randomised, open-label, Phase 3 study. Lancet Oncol. 2022;23(5):659–670. doi:10.1016/S1470-2045(22)00197-8
22. Farzeen Z, Khan RRM, Chaudhry AR, et al. Dostarlimab: a promising new PD-1 inhibitor for cancer immunotherapy. J Oncol Pharm Pract. 2024;30(8):1411–1431. doi:10.1177/10781552241265058
23. Baz Y, Rassam M, Rhayem E, Zouein J, Gharios J, Kourie HR. The use of dostarlimab, a safe and efficient monotherapy in MSI-H rectal cancer patients, an alternative to surgery. Immunotherapy. 2023;15(10):699–701. doi:10.2217/imt-2022-0239
24. Chen H, Chen B, Yang Y, et al. Personalized Neoantigen Vaccine plus Regorafenib Increases Rgs2⁺CD8⁺ T Cells Infiltration and Reprograms the Tumor Microenvironment in Microsatellite Stable Colorectal Cancer Liver Metastases. Adv Sci (Weinh). 2025;12(36):e08040. doi:10.1002/advs.202508040
25. Varayathu H, Sarathy V, Thomas BE, Mufti SS, Naik R. Combination Strategies to Augment Immune Check Point Inhibitors Efficacy - Implications for Translational Research. Front Oncol. 2021;11:559161. doi:10.3389/fonc.2021.559161
26. Mariathasan S, Turley SJ, Nickles D, et al. TGFβ attenuates tumour response to PD-L1 blockade by contributing to exclusion of T cells. Nature. 2018;554(7693):544–548. doi:10.1038/nature25501
27. Nywening TM, Belt BA, Cullinan DR, et al. Targeting both tumour-associated CXCR2(+) neutrophils and CCR2(+) macrophages disrupts myeloid recruitment and improves chemotherapeutic responses in pancreatic ductal adenocarcinoma. Gut. 2018;67(6):1112–1123. doi:10.1136/gutjnl-2017-313738
28. Kang JH, Zappasodi R. Modulating Treg stability to improve cancer immunotherapy. Trends Cancer. 2023;9(11):911–927. doi:10.1016/j.trecan.2023.07.015
29. Spranger S, Bao R, Gajewski TF. Melanoma-intrinsic β-catenin signalling prevents anti-tumour immunity. Nature. 2015;523(7559):231–235. doi:10.1038/nature14404
30. Xue J, Yu X, Xue L, Ge X, Zhao W, Peng W. Intrinsic β-catenin signaling suppresses CD8(+) T-cell infiltration in colorectal cancer. Biomed Pharmacother. 2019;115:108921. doi:10.1016/j.biopha.2019.108921
31. Pagès F, Mlecnik B, Marliot F, et al. International validation of the consensus Immunoscore for the classification of colon cancer: a prognostic and accuracy study. Lancet. 2018;391(10135):2128–2139. doi:10.1016/S0140-6736(18)30789-X
32. Mlecnik B, Bifulco C, Bindea G, et al. Multicenter International Society for Immunotherapy of Cancer Study of the Consensus Immunoscore for the Prediction of Survival and Response to Chemotherapy in Stage III Colon Cancer. J Clin Oncol. 2020;38(31):3638–3651. doi:10.1200/JCO.19.03205
33. Huijbers A, Tollenaar RA, v Pelt GW, et al. The proportion of tumor-stroma as a strong prognosticator for stage II and III colon cancer patients: validation in the VICTOR trial. Ann Oncol. 2013;24(1):179–185. doi:10.1093/annonc/mds246
34. Polack M, Smit MA, van Pelt GW, et al. Results from the UNITED study. a multicenter study validating the prognostic effect of the tumor-stroma ratio in colon cancer. ESMO Open. 2024;9(4):102988. doi:10.1016/j.esmoop.2024.102988
35. Galon J, Bruni D. Approaches to treat immune hot, altered and cold tumours with combination immunotherapies. Nat Rev Drug Discov. 2019;18(3):197–218. doi:10.1038/s41573-018-0007-y
36. Chen DS, Mellman I. Elements of cancer immunity and the cancer-immune set point. Nature. 2017;541(7637):321–330. doi:10.1038/nature21349
37. Routy B, Le Chatelier E, Derosa L, et al. Gut microbiome influences efficacy of PD-1-based immunotherapy against epithelial tumors. Science. 2018;359(6371):91–97. doi:10.1126/science.aan3706
38. Gopalakrishnan V, Spencer CN, Nezi L, et al. Gut microbiome modulates response to anti-PD-1 immunotherapy in melanoma patients. Science. 2018;359(6371):97–103. doi:10.1126/science.aan4236
39. Grasso CS, Giannakis M, Wells DK, et al. Genetic Mechanisms of Immune Evasion in Colorectal Cancer. Cancer Discov. 2018;8(6):730–749. doi:10.1158/2159-8290.CD-17-1327
40. Jones PA, Ohtani H, Chakravarthy A, De Carvalho DD. Epigenetic therapy in immune-oncology. Nat Rev Cancer. 2019;19(3):151–161. doi:10.1038/s41568-019-0109-9
41. Yu YJ, Shan N, Li LY, et al. Preliminary clinical study of personalized neoantigen vaccine therapy for microsatellite stability (MSS)-advanced colorectal cancer. Cancer Immunol Immunother. 2023;72(7):2045–2056. doi:10.1007/s00262-023-03386-7
42. Dagher OK, Schwab RD, Brookens SK, Posey JAD. Advances in cancer immunotherapies. Cell. 2023;186(8):1814–1814.e1811. doi:10.1016/j.cell.2023.02.039
43. Kaneda MM, Messer KS, Ralainirina N, et al. PI3Kγ is a molecular switch that controls immune suppression. Nature. 2016;539(7629):437–442. doi:10.1038/nature19834
44. de Almeida PE, Mak J, Hernandez G, et al. Anti-VEGF Treatment Enhances CD8(+) T-cell Antitumor Activity by Amplifying Hypoxia. Cancer Immunol Res. 2020;8(6):806–818. doi:10.1158/2326-6066.CIR-19-0360
45. Xu M, Tsunedomi R, Kiyotani K, et al. Anti-VEGF and Anti-EGFR Antibody Therapy on T-Cell Infiltration and TCR Variation in Metastatic Colorectal Cancer. Anticancer Res. 2023;43(2):613–620. doi:10.21873/anticanres.16197
46. Fukuoka S, Hara H, Takahashi N, et al. Regorafenib Plus Nivolumab in Patients With Advanced Gastric or Colorectal Cancer: an Open-Label, Dose-Escalation, and Dose-Expansion Phase Ib Trial (REGONIVO, EPOC1603). J Clin Oncol. 2020;38(18):2053–2061. doi:10.1200/JCO.19.03296
47. Eng C, Kim TW, Bendell J, et al. Atezolizumab with or without cobimetinib versus regorafenib in previously treated metastatic colorectal cancer (IMblaze370): a multicentre, open-label, phase 3, randomised, controlled trial. Lancet Oncol. 2019;20(6):849–861. doi:10.1016/S1470-2045(19)30027-0
48. Schröder C, Lawrance M, Li C, et al. Building External Control Arms From Patient-Level Electronic Health Record Data to Replicate the Randomized IMblaze370 Control Arm in Metastatic Colorectal Cancer. JCO Clin Cancer Inform. 2021;5:450–458. doi:10.1200/CCI.20.00149
49. Quan Y, He J, Zou Q, et al. Low molecular weight heparin synergistically enhances the efficacy of adoptive and anti-PD-1-based immunotherapy by increasing lymphocyte infiltration in colorectal cancer. J Immunother Cancer. 2023;11(8). doi:10.1136/jitc-2023-007080
50. Albrecht HC, Gustavus D, Schwanemann J, et al. Generation of colon cancer-derived tumor-infiltrating T cells (TILs) for adoptive cell therapy. Cytotherapy. 2023;25(5):537–547. doi:10.1016/j.jcyt.2023.01.009
51. Tran E, Turcotte S, Gros A, et al. Cancer immunotherapy based on mutation-specific CD4+ T cells in a patient with epithelial cancer. Science. 2014;344(6184):641–645. doi:10.1126/science.1251102
52. Cao Y, Efetov SK, He M, et al. Updated Clinical Perspectives and Challenges of Chimeric Antigen Receptor-T Cell Therapy in Colorectal Cancer and Invasive Breast Cancer. Arch Immunol Ther Exp (Warsz). 2023;71(1):19. doi:10.1007/s00005-023-00684-x
53. Zhang C, Wang Z, Yang Z, et al. Phase I Escalating-Dose Trial of CAR-T Therapy Targeting CEA(+) Metastatic Colorectal Cancers. Mol Ther. 2017;25(5):1248–1258. doi:10.1016/j.ymthe.2017.03.010
54. Bacac M, Fauti T, Sam J, et al. A Novel Carcinoembryonic Antigen T-Cell Bispecific Antibody (CEA TCB) for the Treatment of Solid Tumors. Clin Cancer Res. 2016;22(13):3286–3297. doi:10.1158/1078-0432.CCR-15-1696
55. Segal NH, Melero I, Moreno V, et al. CEA-CD3 bispecific antibody cibisatamab with or without atezolizumab in patients with CEA-positive solid tumours: results of two multi-institutional Phase 1 trials. Nat Commun. 2024;15(1):4091. doi:10.1038/s41467-024-48479-8
56. Li WJ, Dong GH, Bi Y, et al. The cGAS‒STING pathway in colorectal cancer: bridging innate immunity and therapeutic strategies. J Exp Clin Cancer Res. 2025;44(1):286. doi:10.1186/s13046-025-03544-y
57. Chen L, Chen M, Yuan S, et al. Targeting WIP1 reprograms immunosuppressive tumor microenvironment to potentiate immunotherapy response in colorectal cancer. Cell Death Differ. 2026;2026:1.
58. Ding K, Tong X, Ramesh R, et al. Abstract 7143: development of a peripheral dazostinag (TAK-676) activation RNASeq signature to evaluate STING pharmacodynamic modulation in human solid tumor clinical trials. Cancer Res. 2025;85(8_Suppl_1):
59. Salameh H, Naseem N, Chattha MA, et al. Oncolytic Virotherapy in Colorectal Cancer: mechanistic Insights, Enhancer Strategies, and Translational Combinations. Cells. 2025;14(24):2006. doi:10.3390/cells14242006
60. Goel S, Ocean AJ, Parakrama RY, et al. Elucidation of Pelareorep Pharmacodynamics in A Phase I Trial in Patients with KRAS-Mutated Colorectal Cancer. Mol Cancer Ther. 2020;19(5):1148–1156. doi:10.1158/1535-7163.MCT-19-1117
61. Liu J, Frentzas S, Kichenadasse G, et al. Abstract CT183: phase Ib clinical evaluation of a novel CD55- and FcRn-bioselected RNA oncolytic virus, IVX037, combined with sintilimab (anti-PD-1) in advanced microsatellite-stable colorectal cancer. Cancer Res. 2026;86(8_Suppl):CT183. doi:10.1158/1538-7445.AM2026-CT183
62. Wang Y, Lu K, Xu Y, Xu S, Chu H, Fang X. Antibody-drug conjugates as immuno-oncology agents in colorectal cancer: targets, payloads, and therapeutic synergies. Front Immunol. 2025;16:1678907. doi:10.3389/fimmu.2025.1678907
63. Siena S, Di Bartolomeo M, Raghav K, et al. Trastuzumab deruxtecan (DS-8201) in patients with HER2-expressing metastatic colorectal cancer (DESTINY-CRC01): a multicentre, open-label, Phase 2 trial. Lancet Oncol. 2021;22(6):779–789. doi:10.1016/S1470-2045(21)00086-3
64. Raghav K, Siena S, Takashima A, et al. Trastuzumab deruxtecan in patients with HER2-positive advanced colorectal cancer (DESTINY-CRC02): primary results from a multicentre, randomised, phase 2 trial. Lancet Oncol. 2024;25(9):1147–1162. doi:10.1016/S1470-2045(24)00380-2
65. Marliot F, Chen X, Kirilovsky A, et al. Analytical validation of the Immunoscore and its associated prognostic value in patients with colon cancer. J Immunother Cancer. 2020;8(1):e000272. doi:10.1136/jitc-2019-000272
66. El Hajj J, Reddy S, Verma N, Huang EH, Kazmi SM. Immune Checkpoint Inhibitors in pMMR/MSS Colorectal Cancer. J Gastrointest Cancer. 2023;54(4):1017–1030. doi:10.1007/s12029-023-00927-2
67. Helmink BA, Khan MAW, Hermann A, Gopalakrishnan V, Wargo JA. The microbiome, cancer, and cancer therapy. Nat Med. 2019;25(3):377–388. doi:10.1038/s41591-019-0377-7
68. Ogino S, Chan AT, Fuchs CS, Giovannucci E. Molecular pathological epidemiology of colorectal neoplasia: an emerging transdisciplinary and interdisciplinary field. Gut. 2011;60(3):397–411. doi:10.1136/gut.2010.217182
69. Ogino S, Stampfer M. Lifestyle factors and microsatellite instability in colorectal cancer: the evolving field of molecular pathological epidemiology. J Natl Cancer Inst. 2010;102(6):365–367. doi:10.1093/jnci/djq031
70. Ogino S, Ugai S, Hamada T, Ugai T. The early-onset cancer epidemics: evidence synthesis using the prospective cohort incident-tumor biobank method. Eur J Epidemiol. 2025;40(12):1405–1417. doi:10.1007/s10654-025-01322-w
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Immune Checkpoint Inhibitor-Based Combination Therapy for Colorectal Cancer: An Overview
Li J, Xu X
International Journal of General Medicine 2023, 16:1527-1540
Published Date: 26 April 2023
Advances of Drug-Loaded Microsphere Technology for Targeted Immunotherapy Against Prostate Cancer
Feng W
International Journal of Nanomedicine 2025, 20:11479-11489
Published Date: 20 September 2025
Advances in the Use of Immune Checkpoint Inhibitors for Colorectal Cancer Treatment
Li J, Fu T, Wen Z, Liang J, Qiu Y, Li K, Yang J, Tong Y, Cai H
OncoTargets and Therapy 2025, 18:1159-1168
Published Date: 15 October 2025
DNA Methylation in Lung Cancer: Predictive Biomarkers for Effective Immunotherapy
Kumari K, Kumar V, Verma C, Hsu PC, Singh A
International Journal of General Medicine 2025, 18:7893-7910
Published Date: 31 December 2025
Immune Checkpoint Inhibitors in Breast Cancer: Mechanisms, Biomarkers, and Future Therapeutic Strategies
Deng QC, Kuang WB, Yang YJ, Gong CP, Zhang YP, Luo Q, Luo LP, Wang GM
Therapeutics and Clinical Risk Management 2026, 22:547154
Published Date: 9 July 2026