Back to Journals » International Medical Case Reports Journal » Volume 19
Mycobacterium abscessus Cervical Lymphadenitis Mimicking Tuberculosis in China: A Case Report
Authors Guo C ![]() , Guo Y, Tong J, Zhao G, Yao L, Pan Y, Zang M, Liu K
, Guo Y, Tong J, Zhao G, Yao L, Pan Y, Zang M, Liu K
Received 14 February 2026
Accepted for publication 1 April 2026
Published 14 April 2026 Volume 2026:19 600141
DOI https://doi.org/10.2147/IMCRJ.S600141
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Thomas E Hutson
Can Guo,1,* Yu Guo,2,* Jing Tong,3,* Guizeng Zhao,1 Linyan Yao,1 Yanjing Pan,1 Min Zang,1 Kewei Liu3
1Department of Tuberculosis, The First Affiliated Hospital of Henan Medical University, Xinxiang, People’s Republic of China; 2Health Management Center, The First Affiliated Hospital of Henan Medical University, Xinxiang, People’s Republic of China; 3Department of Tuberculosis, Beijing Chest Hospital, Capital Medical University, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Can Guo, Department of Tuberculosis, The First Affiliated Hospital of Henan Medical University, Xinxiang, 453100, People’s Republic of China, Email [email protected] Kewei Liu, Department of Tuberculosis, Beijing Chest Hospital, Capital Medical University, Beijing, 101149, People’s Republic of China, Email [email protected]
Abstract: Mycobacterium abscessus (Mab) is recognized as the most pathogenic mycobacterium affecting humans, comprising three phylogenetic subspecies: M. abscessus subsp. abscessus, M. abscessus subsp. bolletii, and M. abscessus subsp. massiliense. Its clinical manifestations are varied and frequently subject to misdiagnosis. Mab exhibits both intrinsic and acquired resistance to numerous antibiotics, which results in limited therapeutic options and poor clinical outcomes. This report details a case of cervical lymphadenitis caused by Mab, initially misdiagnosed as tuberculosis. During anti-tuberculosis therapy, the patient’s symptoms initially improved but subsequently deteriorated. Diagnosis of Mab infection was confirmed through high-throughput sequencing. However, due to the delay in accurate diagnosis and treatment missteps, the patient ultimately succumbed to a central nervous system (CNS) Mab infection. Consequently, early and precise diagnosis is imperative for the effective management of Mab infections.
Keywords: tuberculosis, Mycobacterium abscessus, diagnosis
Introduction
The incidence of human nontuberculous mycobacterial (NTM) infections has increased markedly in recent years. In Germany, the application of machine learning algorithms to health claims data revealed a significant underestimation of NTM infection cases. The study found that the actual prevalence and incidence rates in 2021 were fivefold and ninefold higher, respectively, than previously reported, highlighting the growing burden of NTM infections, which often go undiagnosed.1–3 Mab is the most pathogenic rapidly growing mycobacterium affecting humans, leading to pulmonary and extrapulmonary infections, such as lung, skin, soft tissue, CNS infections, as well as bacteremia, particularly in immunosuppressed individuals. This organism is notorious for its resistance to many antibiotics and its ability to form biofilms. The pathophysiology of Mab infections is complex and involves various host and microbial factors. The rising incidence of Mab infections and the emergence of strains with heightened virulence pose significant public health concerns.3
Mab is typically transmitted through contaminated water, dust, and inhaled or ingested aerosols.4 Its enhanced growth and survival in the presence of particulates such as kaolin, halloysite, silicon dioxide, and house dust suggest that contaminated fomites may also serve sources of transmission, underscoring the role of the environment in Mab spread.5 Consequently, the frequency and clinical presentation of Mab infections vary geographically due to environmental differences and population-specific susceptibilities.
Members of the Mab complex, particularly M. abscessus subsp. abscessus, are frequently misidentified as other bacterial infections, leading to delayed diagnosis and treatment.6 The occurrence of Mab cervical lymphadenitis is indeed a rare clinical phenomenon. This rarity is underscored by the limited number of documented cases and the challenges associated with its diagnosis. One case that highlights the diagnostic complexity involved is that of an immunocompetent female with Mab cervical lymphadenitis, which was initially suspected to be malignancy.7 The clinical presentation can closely resemble more common conditions, such as tuberculosis or even malignancies. In this study, we present a case of Mab cervical lymphadenitis mimicking tuberculosis, which led to death from central nervous system infection in China.
Case Presentation
A 23-year-old female patient from Xinxiang, Henan Province, China, presented with right cervical lymph node enlargement for one month (Figure 1A). The affected area did not exhibit tenderness or mobility and had a well-defined boundary. The local physician administered antibiotic treatment to the patient, but symptomatic improvement was not evident, which the specific plan is unknown. The patient was healthy, with no history of allergies, no family history, no long-term medication use, and no history of immunosuppressive agent use. The patient was a local college student with no travel history outside China.
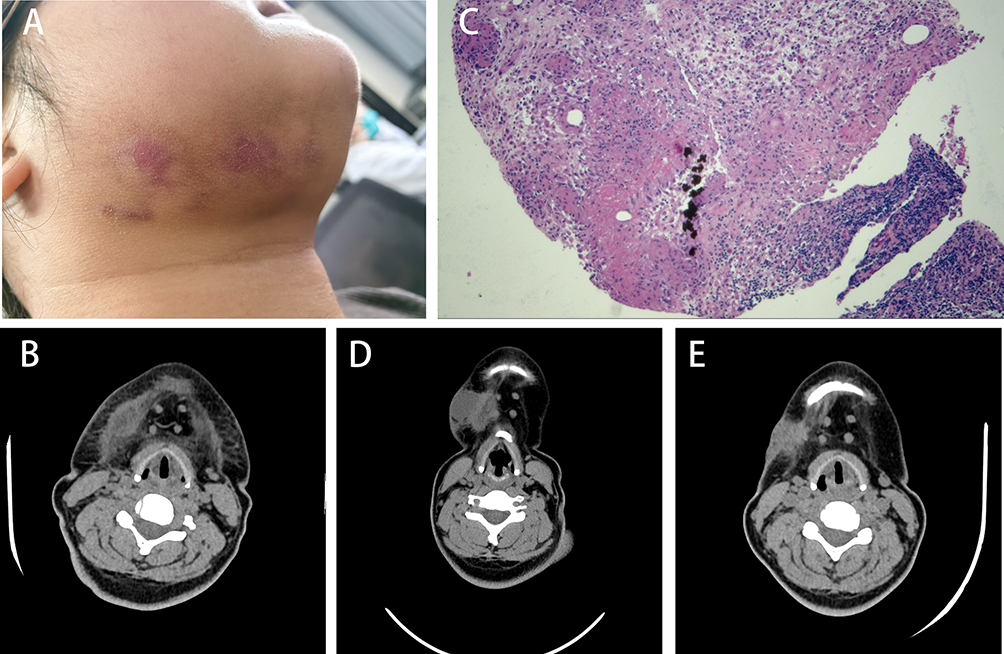 |
Figure 1 Right submaxillary lesions and pathological changes. (A) The right cervical lymph node enlargement. (B) Cervical CT revealed multiple nodular and clustered slightly low-density shadows with blurred boundaries and partial fusion into a mass was observed in the right submandibular region, reflecting tuberculosis infection. (C) The results of cervical lymph node puncture revealed focal caseous necrosis and epithelial-like cells, and tuberculosis was not excluded. (D) Cervical CT revealed multiple round low-density shadows, larger lesions than before, and more local soft tissue density shadows in the right submandibular region. (E) Cervical CT revealed a noticeable resolution of the right submandibular lesion and significantly reduced soft tissue density shadow. |
Cervical computed tomography (CT) revealed right cervical lymph node lesions, indicating a tuberculosis infection (Figure 1B). Serum tuberculosis antibody test results were positive. The erythrocyte sedimentation rate increased, but T-SPOT.TB (T-SPOT) was negative. Chest CT and pulmonary function tests revealed no obvious abnormalities. Examinations of Aspergillus galactomannan, β-D-glucans, respiratory viruses, complete blood count, tumor markers, autoimmune disease antibodies, and enzyme-linked immunosorbent assay (ELISA) tests for human immunodeficiency virus (HIV) were negative. Acid-fast staining and GeneXpert MTB/RIF tests of the puncture fluid were also negative. Nevertheless, tuberculosis could not be excluded, as cervical lymph node puncture displayed focal caseous necrosis and epithelioid cells (Figure 1C). Initially, a four-drug regimen (daily standard weight-based dosing of rifampicin [600 mg], ethambutol [1000 mg], isoniazid [300 mg], and pyrazinamide [1500 mg]) was prescribed for suspected tuberculosis of the cervical lymph nodes.
After two months of tuberculosis treatment, the patient complained of improved symptoms. However, the patient’s neck swelling symptoms worsened during the third month of anti-tuberculosis treatment. Cervical CT revealed re-expansion of the right submaxillary lesions (Figure 1D). The patient may have been misdiagnosed. Mab was identified in the cervical lymph node pus using high-throughput sequencing. The patient was switched to rifabutin, linezolid, amikacin, and clarithromycin for the treatment of nontuberculous mycobacteria for two months.
Cervical CT revealed resolution of the right submaxillary lesions (Figure 1E). However, the patient developed a worsening headache. After eight weeks, cerebrospinal fluid culture showed Mab. With the diagnosis of invasive CNS infection caused by Mab, antimicrobial therapy was adjusted to include tigecycline, linezolid, amikacin, and clarithromycin. However, the patient died from irreversible CNS involvement.
Discussion
The misdiagnosis of Mab as TB is a significant clinical challenge, particularly in regions where TB is endemic. This misdiagnosis often arises due to the overlapping clinical and radiological features of NTM infections and TB, as well as the limitations of conventional diagnostic methods. For instance, a study conducted in Mali highlighted the prevalence of NTM infections among patients initially treated for TB, emphasizing the need for high-throughput sequencing to accurately differentiate between these infections.8 Similarly, the challenges in distinguishing between NTM and TB were underscored in a case report in which a patient was misdiagnosed with TB for three years before NTM was correctly identified using high-throughput sequencing.9
The diagnostic conundrum is further complicated by the fact that NTM, including Mab, can present with non-specific symptoms that mimic TB, such as chronic cough and fever. The clinical manifestations of Mab infection include abscesses, panniculitis, nodules, cellulitis, ulcers, and sinus tract drainage.10 Diagnosis relies on isolating the organism from clinical specimens; however, Mab is challenging to detect using Gram staining and standard cultures. This was illustrated in a case in which Mab was initially misdiagnosed as TB, leading to ineffective treatment until the correct diagnosis was made through high-throughput sequencing.11 The importance of accurate species identification is underscored by studies emphasizing the role of high-throughput sequencing in distinguishing NTM from TB, thereby preventing misdiagnosis and ensuring appropriate treatment.12,13
The Ziehl-Neelsen staining technique is a cornerstone in the detection of acid-fast bacilli. The diagnostic insights rely on the presence of a sufficient bacterial load for visualization. However, in the context of Mab, which may present with atypical clinical manifestations and lower bacterial loads, the sensitivity of Ziehl-Neelsen staining can be suboptimal.14 Coupled with the long turnaround time for antimicrobial susceptibility testing, these challenges frequently delay accurate identification and timely initiation of appropriate therapy. This limitation underscores the importance of high-throughput sequencing, which offers enhanced sensitivity and specificity. It allows for the rapid and precise identification of specific mycobacterial DNA sequences, which might not be detectable through traditional staining methods.15
The process of Mab infection shares remarkable similarities with that of M. tuberculosis infection, including granuloma formation and persistent infection. After colonization, macrophages and neutrophils are recruited to phagocytose the bacteria, and the innate immune response initially contains the infection. However, Mab can resist phagosomal defenses and induce the generation of inflammatory cytokines, such as tumor necrosis factor (TNF), which promotes further immune-cell recruitment and granuloma formation.16 During persistent infection, Mab undergoes an irreversible transition from a smooth (S) to a rough (R) variant, leading to granuloma breakdown and the formation of large extracellular bacterial cords.17 The biological and environmental triggers driving this transition remain unknown.
Mab exhibits two phenotypically distinct morphotypes, S and R, defined by the presence or absence of glycopeptidolipids (GPLs) in the cell wall.18 Both variants can originate from the same isolate, coexist within the host, and evolve differently in response to host immunity, leading to distinct clinical outcomes and disease manifestations.19 The transition of Mab from a smooth (S) to a rough (R) morphotype is a critical factor in its pathogenicity, particularly in cases of lymphadenitis. This transition is characterized by a reduction in GPL production, which is well-documented as a key factor in the increased virulence associated with the R morphotype. The study titled “Loss of LpqM proteins in Mycobacterium abscessus is associated with impaired intramacrophage survival” provides insights into the genetic and molecular mechanisms underlying this transition.20
Treatment of Mab infections presents its own set of challenges due to the organism’s intrinsic resistance to many antibiotics commonly used for TB. Current treatment recommendations for Mab involve a combination of antibiotics, including macrolides like clarithromycin and aminoglycosides such as amikacin. The resistance to clarithromycin is a growing concern, as demonstrated by studies showing inducible resistance in Mab isolates.21 During treatment, this patient’s clinical symptoms improved, and cervical lymph node enlargement was reduced, however, she died a of CNS infection in the later stage, which may be related to inducible resistance and the S-to-R transition of the Mab. Various pathogenic factors confer upon Mab an exceptional ability to produce diverse infection patterns. Most of these determinants are related to the cell envelope structure and overall bacterial composition. The capacity of Mab to shift into more virulent morphotypes enables immune evasion and promotes systemic dissemination. Its distinctive mycobacterial outer membrane (MOM) and multiple efflux pumps create a robust barrier against both host defenses and many antibiotics. Moreover, the ESX-4 Type VII secretion system equips Mab with mechanisms to modulate host immunity, driving more aggressive infection progression.22 Therefore, it is necessary to pay greater attention to the cases of cervical lymph node involvement combined with central nervous system infection caused by Mab, and further explore the mechanisms by which Mycobacterium abscessus invades the central nervous system.
This study is subject to several limitations. Firstly, there was a lack of timely consideration by clinicians regarding the differential diagnosis between Mab and tuberculosis infections. Secondly, the initial treatment regimen for patients involved anti-tuberculosis therapy, which proved ineffective in controlling the condition and subjected patients to potential adverse effects of anti-tuberculosis medications, including hepatic and renal impairments. Thirdly, delays in the treatment of patients with CNS infections exacerbated their clinical conditions. Furthermore, numerous aspects of this organism’s infection mechanisms remain insufficiently understood, necessitating further research for comprehensive characterization.
Conclusion
In summary, this is an uncommon instance of Mab infection resembling tuberculosis. This article seeks to enhance comprehension of Mab diseases and address these neglected and significant global threats. It is crucial not only to prevent incorrect TB treatment but also to direct effective management of Mab infections. Developing new antibiotics and treatment plans, along with implementing systematic diagnostic protocols, is vital to tackle the increasing challenge of Mab infections in clinical settings.
Abbreviations
Mab, Mycobacterium abscessus; NTM, Nontuberculous mycobacteria; CT, Computed Tomography; TB, Tuberculosis; T-SPOT, T-SPOT.TB; ELISA, Enzyme-Linked Immunosorbent Assay; CNS, Central Nervous System; TNF, Tumor necrosis factor; GPLs, Glycopeptidolipids; S, Smooth; R, Rough; MOM, Mycobacterial outer membrane; HIV, Human Immunodeficiency Virus; ESX-4, Type VII secretion system-4.
Data Sharing Statement
Available upon request. The data is available from the correspondent author 1.
Ethics Approval
This investigation was reviewed and approved by the Institutional Review Board of The First Affiliated Hospital of Xinxiang Medical University.
Consent for Participation and Publication
Informed consent for participation was obtained from the patient during the hospitalization. Informed consent for publication was acquired from the patient during the hospitalization. Publishing the case details did not require institutional approval.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ringshausen FC, Ewen R, Multmeier J, et al. Predictive modeling of nontuberculous mycobacterial pulmonary disease epidemiology using German health claims data. Int J Infect Dis. 2021;104:398–6. doi:10.1016/j.ijid.2021.01.003
2. Dartois V, Dick T. Therapeutic developments for tuberculosis and nontuberculous mycobacterial lung disease. Nat Rev Drug Discov. 2024;23(5):381–403. doi:10.1038/s41573-024-00897-5
3. Desai AN, Hurtado R. Nontuberculous Mycobacterial Infections. JAMA. 2021;325(15):1574. doi:10.1001/jama.2020.19062
4. De Groote MA, Pace NR, Fulton K, et al. Relationships between Mycobacterium Isolates from Patients with Pulmonary Mycobacterial Infection and Potting Soils. Appl Environ Microbiol. 2006;72(12):7602–7606. doi:10.1128/AEM.00930-06
5. Malcolm KC, Caceres SM, Honda JR, et al. Mycobacterium abscessus Displays Fitness for Fomite Transmission. Appl Environ Microbiol. 2017;83(19):e00562–17. doi:10.1128/AEM.00562-17
6. Lange C, Böttger EC, Cambau E, et al. Consensus management recommendations for less common non-tuberculous mycobacterial pulmonary diseases. Lancet Infect Dis. 2022;22(7):e178–e190. doi:10.1016/S1473-3099(21)00586-7
7. Tan JYQ, Shafi H. An immunocompetent female with Mycobacterium abscessus cervical lymphadenitis mimicking malignancy. Int J Infect Dis. 2021;105:239–240. doi:10.1016/j.ijid.2021.02.044
8. Maiga M, Siddiqui S, Diallo S, et al. Failure to recognize nontuberculous mycobacteria leads to misdiagnosis of chronic pulmonary tuberculosis. PLoS One. 2012;7(5):e36902. doi:10.1371/journal.pone.0036902
9. Wu HH, Zhao YK, Lai Y, et al. Disseminated Mycobacterium avium and Talaromyces Marneffei coinfection in a patient of misdiagnosed tuberculosis and the challenges: a case report. BMC Infect Dis. 2025;25(1):1458. doi:10.1186/s12879-025-11895-2
10. Murillo J, Torres J, Bofill L, et al. Skin and wound infection by rapidly growing mycobacteria: an unexpected complication of liposuction and liposculpture. The Venezuelan Collaborative Infectious and Tropical Diseases Study Group. Arch Dermatol. 2000;136(11):1347–1352. doi:10.1001/archderm.136.11.1347
11. Zhao P, Zhang YY, Li YB, et al. Diagnosis of Pulmonary Disease Caused by Mycobacterium abscessus: a Case Report. J Int Med Res. 2011;39(3):968–975. doi:10.1177/147323001103900332
12. Biyang FI, Massi MN, Muslich LT, et al. Identification of Nontuberculous Mycobacterium and Mycobacterium tuberculosis Complex in Sputum Patients with Suspected Tuberculosis. Int J Mycobacteriol. 2024;13(4):436–442. doi:10.4103/ijmy.ijmy_206_24
13. Ustinova VV, Smirnova TG, Sochivko DG. New assay to diagnose and differentiate between Mycobacterium tuberculosis complex and nontuberculous mycobacteria. Tuberculosis (Edinb). 2019;114:17–23. doi:10.1016/j.tube.2018.10.004
14. Fujii W, Chang L, Inui TA, et al. Cervical lymphadenitis caused by Mycobacterium avium in a patient treated with Janus kinase inhibitors. Int J Infect Dis. 2023;133:57–59. doi:10.1016/j.ijid.2023.05.006
15. Zhang W, Xu J, Zhang L, et al. The value of histopathologic examination and Xpert (MTB/RIF) assay in diagnosis of cervical lymph node tuberculosis after coarse needle biopsy guided by CEUS: a retrospective analysis of 612 cases. Eur J Clin Microbiol Infect Dis. 2024;43(10):1951–1957. doi:10.1007/s10096-024-04913-9
16. Bernut A, Nguyen-Chi M, Halloum I, et al. Mycobacterium abscessus-Induced Granuloma Formation Is Strictly Dependent on TNF Signaling and Neutrophil Trafficking. PLoS Pathog. 2016;12(11):e1005986. doi:10.1371/journal.ppat.1005986
17. Bernut A, Herrmann JL, Kissa K, et al. Mycobacterium abscessus cording prevents phagocytosis and promotes abscess formation. Proc Natl Acad Sci USA. 2014;111(10):E943–E952. doi:10.1073/pnas.1321390111
18. Johansen MD, Herrmann JL, Kremer L. Non-tuberculous mycobacteria and the rise of Mycobacterium abscessus. Nat Rev Microbiol. 2020;18(7):392–407. doi:10.1038/s41579-020-0331-1
19. Boudehen YM, Kremer L. Mycobacterium abscessus. Trends Microbiol. 2021;29(10):951–952. doi:10.1016/j.tim.2021.06.006
20. Boudehen Y-M, Daher W, Roquet-Baneres F, et al. Loss of LpqM proteins in Mycobacterium abscessus is associated with impaired intramacrophage survival. Microbiol Spectr. 2024;12(5):e0383723. doi:10.1128/spectrum.03837-23
21. Chu HS, Chang SC, Shen EP, et al. Nontuberculous mycobacterial ocular infections--comparing the clinical and microbiological characteristics between Mycobacterium abscessus and Mycobacterium massiliense. PLoS One. 2015;10(1):e0116236. doi:10.1371/journal.pone.0116236
22. Parmar S, Tocheva EI. The cell envelope of Mycobacterium abscessus and its role in pathogenesis. PLoS Pathog. 2023;19(5):e1011318. doi:10.1371/journal.ppat.1011318
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Duration and Determinants of Delayed Diagnosis with Tuberculosis in Shenzhen, China: A Cross-Sectional Study
Jiang Y, Luo L, Gui M, Liu L, Lin Y, Deng G, Chen J, Zhang P
Risk Management and Healthcare Policy 2022, 15:1473-1481
Published Date: 29 July 2022
Rapid Molecular Assays for the Diagnosis of Drug-Resistant Tuberculosis
Nandlal L, Perumal R, Naidoo K
Infection and Drug Resistance 2022, 15:4971-4984
Published Date: 29 August 2022
Nontuberculous Mycobacteria Lung Disease (NTM-LD): Current Recommendations on Diagnosis, Treatment, and Patient Management
Pathak K, Hart S, Lande L
International Journal of General Medicine 2022, 15:7619-7629
Published Date: 1 October 2022
Application of Adenosine Deaminase and γ-Interferon Release Assay in Pleural Fluid for the Diagnosis of Tuberculous Pleural Effusion in Patients Over 40 Years Old
Li Z, Chen J, Zeng J, Shi P, Xiong X, Wang M, Zheng D, Zhao R, Dong L
Infection and Drug Resistance 2023, 16:1009-1018
Published Date: 17 February 2023
Advances in the Diagnosis of Latent Tuberculosis Infection
Zhang H, Guan W, Zhou J
Infection and Drug Resistance 2025, 18:483-493
Published Date: 25 January 2025