")
Back to Journals » Infection and Drug Resistance » Volume 15
Rapid Molecular Assays for the Diagnosis of Drug-Resistant Tuberculosis
Authors Nandlal L, Perumal R , Naidoo K
Received 12 July 2022
Accepted for publication 20 August 2022
Published 29 August 2022 Volume 2022:15 Pages 4971—4984
DOI https://doi.org/10.2147/IDR.S381643
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Louansha Nandlal,* Rubeshan Perumal,* Kogieleum Naidoo*
Centre for the AIDS Programme of Research in South Africa (CAPRISA), South African Medical Research Council (SAMRC)-CAPRISA-TB-HIV Pathogenesis and Treatment Research Unit, University of KwaZulu-Natal Nelson R Mandela School of Medicine, Durban, South Africa
*These authors contributed equally to this work
Correspondence: Rubeshan Perumal, Centre for the AIDS Programme of Research in South Africa (CAPRISA), South African Medical Research Council (SAMRC)-CAPRISA-TB-HIV Pathogenesis and Treatment Research Unit, University of KwaZulu-Natal Nelson R Mandela School of Medicine, Durban, South Africa, Email [email protected]
Abstract: The recognition that drug-resistant tuberculosis (DR-TB) poses a major threat to global tuberculosis (TB) control efforts has catalysed the development of new and urgently needed TB diagnostics. The full beneficial impact of the subsequent flood of new TB diagnostic tests into the market can only be realised if these diagnostic tests are readily accessible to TB programs and contribute to improved patient outcomes. Although phenotypic drug-susceptibility testing remains the gold standard, an improved understanding of the relationship between mutations and different levels of drug resistance coupled with the advantages of molecular diagnostics could result in rapid molecular diagnostic tests replacing phenotypic drug-susceptibility testing. Successful diagnostics need to diagnose all forms of drug-resistant TB prevalent in each geographic region. Given the finite number and often limited availability of effective drugs for DR-TB, the diagnostic test must be able to detect all clinically important types of resistance to available anti-TB drugs. However, less comprehensive resistance profiling may be sufficient in settings where extensively drug-resistant TB (XDR-TB) and pre-XDR are absent. Rapid molecular diagnostic tests for DR-TB detection suitable for DR-TB endemic settings should be accurate, inexpensive, suitable to be performed on an easily accessible sample, detect prevalent circulating drug-resistant strains, and provide results within a short turnaround time to enable timely treatment initiation. In this review, we appraise the wide range of molecular diagnostics for DR-TB endorsed by the World Health Organisation, discuss the challenges in the development and rollout of rapid molecular DR-TB tests in low- and middle-income countries, and highlight user perspectives and cost-effectiveness factors that influence their utility.
Keywords: tuberculosis, drug resistance, molecular assays, point of care, diagnosis
Corrigendum for this paper has been published.
Plain Language Summary
Drug-resistant TB is a major threat to global TB control. Rapid molecular diagnostic tests are crucial for earlier diagnosis, shortened time to treatment initiation, improved retention in care, and improved treatment outcomes. Rapid molecular tests must concord with phenotypic resistance and be capable of diagnosing resistance to a comprehensive list of available drugs for the treatment of DR-TB. In addition, these tests should be accurate, inexpensive, suitable for application on an easily accessible sample, and have a short turnaround time. In this review, we appraise the wide range of molecular diagnostics for DR-TB endorsed by the World Health Organisation, discuss the challenges in the development and rollout of rapid molecular DR-TB tests in low- and middle-income countries, and highlight user perspectives and cost-effectiveness factors that influence their utility.
Introduction
Drug-resistant Mycobacterium tuberculosis (Mtb) remains a significant challenge to global tuberculosis (TB) care and control efforts. According to the Global TB Report 2021, approximately 10 million people fell ill with TB, including ~50,000 incident cases of drug-resistant TB (DR-TB).1 Over 1.4 million people died from TB in 2020, with more than 95% of these deaths occurring in low- and middle-income countries.1 Despite a 20% decrease in TB mortality from 2015 to 2020, the prevalence rates of multidrug-resistant TB (MDR-TB) and extensively drug-resistant TB (XDR-TB) continue to rise among both new and previously treated TB cases.2 To a large extent, the COVID-19 pandemic has reversed years of gains in TB detection, notification, and treatment.1 More than 40% of the estimated 10 million TB cases in 2020 were not diagnosed, predominantly due to the globally reduced access to TB diagnostic services. Moreover, only 59% of the 4.8 million people diagnosed with TB in 2020 received a bacteriologically confirmed diagnosis, only half of whom were diagnosed by a WHO-endorsed rapid molecular test. The poor access to sensitive diagnostic tests is a major limitation to our ability to detect drug resistance. Recent data suggest that person-to-person transmission of MDR- and XDR-TB is now the driving force of the global DR-TB burden although acquired drug resistance continues to contribute to the evolution of drug resistance in the context of TB treatment mismanagement.1,2 In many high-burden settings, delays in access to rapid DR-TB diagnosis and effective treatment perpetuate transmission and fuel the epidemic.
Although several advances have been made in diagnosing DR-TB, no reliable, simple point of care (POC) test exists to diagnose the disease. A POC test that readily detects active TB would reduce diagnostic delays, interrupt transmission with appropriate therapy, and address many current global TB control gaps.3 Improving existing testing means developing highly sensitive and specific assays to diagnose DR-TB and ensuring simplicity, affordability, technical robustness, and the capacity for rapid up-scaling at the most decentralised level by health care workers with minimal training.4 The critical advantage of a POC test is its potential ability to enable immediate treatment initiation at the point of presentation, thus circumventing the problem of patient dropout.5
Several nucleic acid-based assays that detect TB drug resistance have been developed over the years; however, significant shortcomings need to be addressed for optimal application. In this review, we appraise the wide range of molecular diagnostics for DR-TB endorsed by the World Health Organisation, discuss the challenges in the development and rollout of rapid molecular DR-TB tests in low- and middle-income countries, and highlight user perspectives and cost-effectiveness factors that influence their utility.
Methods
Manuscripts were identified through searches of PubMed using the terms: “Xpert”, “GeneXpert”, “point of care”, “tuberculosis”, “drug-resistant”, “diagnostics”, “line probe assay”, “NAATS”, and “implementation”. We included manuscripts published between 2000 and 2021 and limited the search to English-language publications. We manually searched all references of included articles to identify additional articles not captured by the electronic search. We included all manuscripts reporting on at least one diagnostic test for detection of Mtb and resistance to at least one TB drug. We excluded studies focused purely on culture-based techniques for the detection of Mtb or drug resistance.
Characteristics of Point of Care for DR-TB Diagnostic Tests
A minimum set of characteristics of future POC DR-TB diagnostic tests has previously been proposed (Table 1). Notably, POC tests require the ability to maintain high levels of sensitivity and specificity, irrespective of the local prevalence of TB, and must be capable of diagnosing TB, irrespective of the site of disease, type of specimen, or severity of the disease.6 Moreover, the test should simultaneously detect first- and second-line drug-resistance-conferring mutations. Overall, the main advantage of a POC diagnostic for DR-TB is the ability to detect TB and profile drug resistance without the support of laboratory infrastructure; this increases access to the test, eliminates the need to transport samples, and reduces travel time from weeks (or months) to hours. Same-day results from POC tests will enable single-visit treatment initiation, improved quality of care, and help mitigate pre-treatment loss to follow-up.7
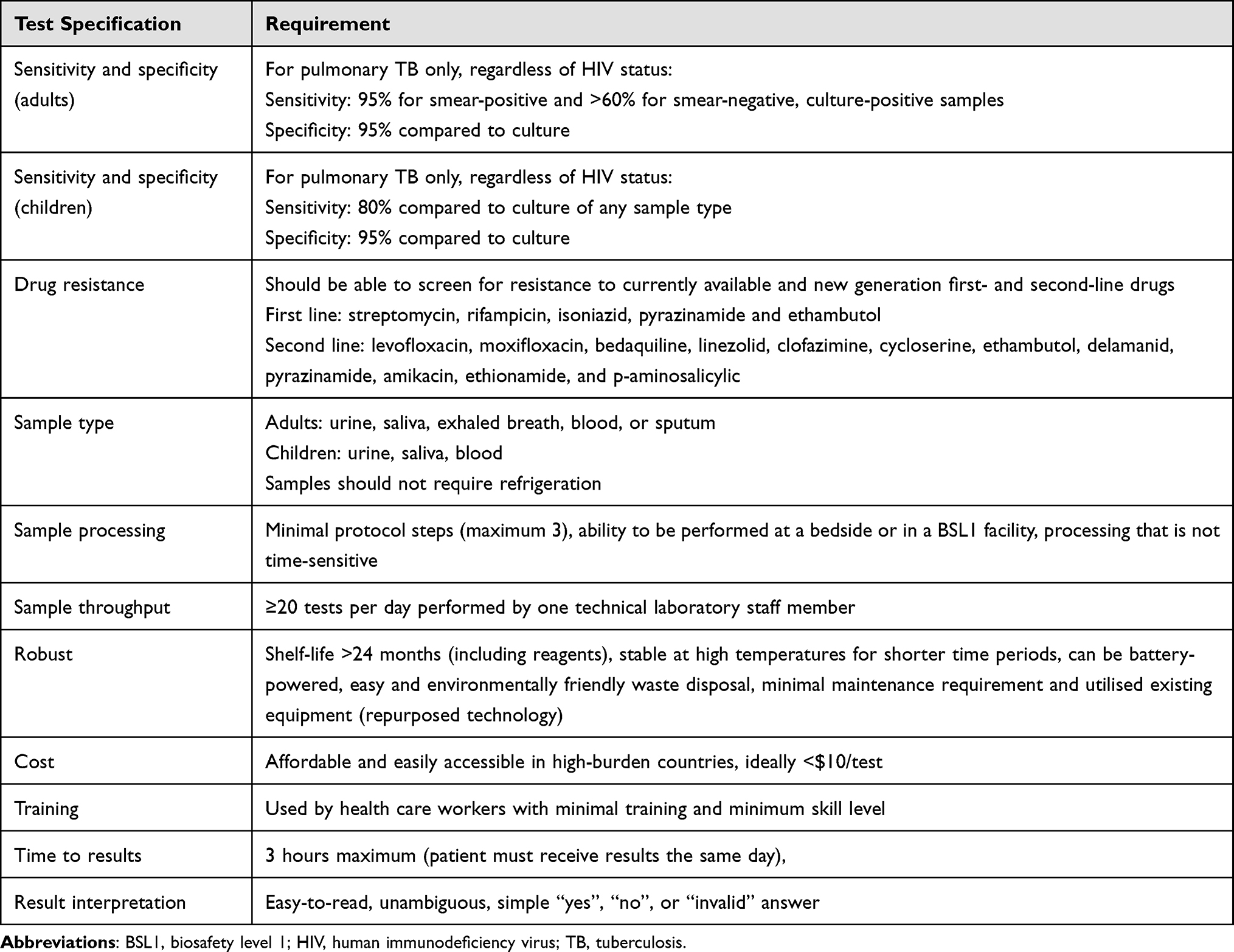 |
Table 1 Minimum Characteristics of a Future Point of Care DR-TB Diagnostic Test |
An adequate expectorated sputum sample is required at the primary care level to diagnose pulmonary TB.8 However, in up to a third of TB cases, an adequate biological sample is not readily available or has a deficient concentration of TB bacilli rendering the sample smear-negative.9 The availability of alternative techniques such as sputum induction, bronchoscopy, gastric aspiration and organ biopsy is limited in TB endemic settings. Therefore, on the one hand, attention has been focused on other biological samples, such as exhaled breath, blood and urine, which are easy to collect and process.6 On the other hand, improved sensitivity and specificity of existing tests will improve TB detection even in paucibacillary samples. Urine as a biological fluid for diagnostic testing is particularly attractive because it is easy to collect compared to other fluids such as sputum and serum, is readily available, and contains TB-specific proteins and DNA in patients with TB.10–15 The collection of exhaled breath condensate is a completely non-invasive method of sampling the respiratory tract, which can be performed with minimal patient effort using portable equipment, and which can be repeated several times within short intervals.16 Breath analysis has predominantly focused on the detection of volatile organic compound with TB-specific signatures.17 Recent advances have focused on novel exhaled breath aerosol collection and analysis techniques, which may demonstrate the potential to detect Mtb proteins and lipids.17,18
WHO-Endorsed Molecular Diagnostics for Detection of TB and Drug-Resistance
The WHO recommends that TB Programmes transition from microscopy as the initial TB diagnostic test to rapid molecular diagnostics that allow for the simultaneous detection of Mtb and drug resistance.2 Sputum smear is one of the oldest front-line diagnostic techniques currently used to detect acid-fast bacilli directly from sputum.19 This is a simple and inexpensive technique, but its sensitivity is limited, requiring 10000 bacilli per mL of sputum to reliably detect Mtb,20 and results are subject to interpretation by the reader, which can result in variability of results.21 Moreover, smear microscopy cannot differentiate between Mtb and non-tuberculous mycobacteria, viable and nonviable organisms, or drug-susceptible and drug-resistant strains.22 Mtb can also be cultured from clinical specimens using various solid and liquid culture media such as (i) Lowenstein – Jensen, (ii) Middlebrook 7H10/11, and (iii) Middlebrook 7H9.23 The cultivation and susceptibility testing of Mtb has evolved from solid culture to automated systems, ie, BACTEC-Mycobacteria Growth Indicator Tube (MGIT) and other liquid media, and represents a significant advance in TB culture-based diagnostics. The BACTEC-MGIT 960 method overcame many drawbacks of the BACTEC 460 TB system, such as the need for radioactive substances and needles.24 However, phenotypic DST still has several limitations, including costly, time-consuming culture-based methods that generate results 2–8 weeks after specimen collection, increased risk of culture contamination, and the need for complex laboratory infrastructure.25
During the last decade, the WHO has endorsed a range of highly sensitive and specific molecular diagnostic techniques for detecting Mtb nucleic acids and drug resistance to overcome these challenges (Table 2). Currently, the molecular diagnostic assays, including Xpert MTB/RIF Ultra and Xpert MTB/XDR (Cepheid, Sunnyvale, CA), Truenat MTB-RIF Dx (Molbio), line probe assays (LPA) (GenoType MTBDRplus, MTBDRsl and GenoScholar NTM+MDRTB II; Hain Lifescience GmbH, Nehren, Germany), and moderate complexity automated NAATS, can rapidly identify a limited number of mutations in first-line and second-line antibiotic resistance-conferring genes.2 These assays have significantly improved Mtb detection and drug susceptibility testing (DST) and support rapid turnaround times.
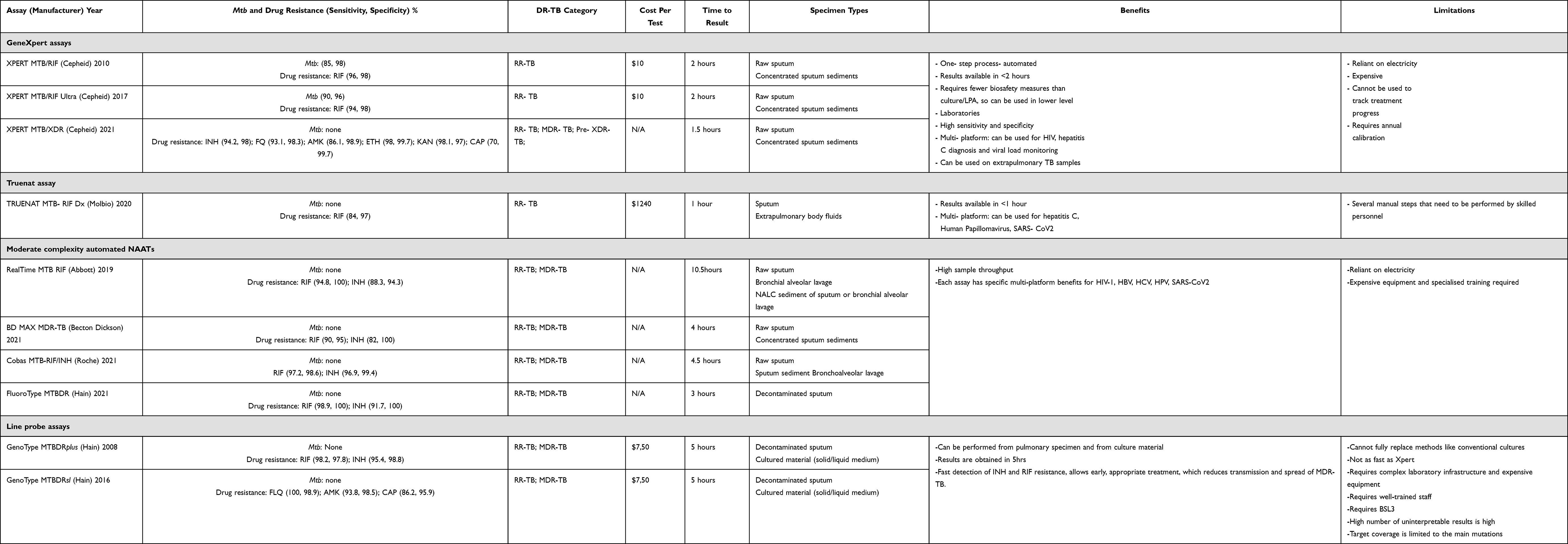 |
Table 2 Performance of WHO-Endorsed Molecular Diagnostics for Drug-Resistant TB Diagnosis and Drug-Susceptibility Testing |
Xpert MTB/RIF, Xpert MTB/RIF Ultra and Xpert MTB/XDR Assays
The Xpert MTB/RIF assay (Cepheid Inc., Sunnyvale, CA, USA) uses semi-quantitative real-time polymerase chain reaction (PCR) to rapidly identify Mtb complex and detect rifampicin (RIF) resistance, a surrogate marker for MDR-TB, by amplifying a fragment containing the 81-base pair hotspot region of the rpoB gene (codons 507–533) that is then hybridised to five molecular beacon probes.26–31 Each probe covers a separate sequence and is labeled with a fluorescent dye.32 Several large-scale trials have assessed the accuracy of Xpert MTB/RIF in pulmonary and extrapulmonary TB.33–39 Compared to standard culture-based DST, sensitivity and specificity for smear-positive samples can reach 100 and 99%, respectively, and 62.6 and 99% for smear-negative samples.6,33,35,40–42 For the detection of RIF resistance in regions with high DR-TB prevalence, the sensitivity and specificity are ~94% and ~97%, respectively.2,6 The time to diagnosis of RIF resistance has been significantly reduced from 2 to 8 weeks (culture and DST) to two hours, enabling rapid initiation of DR-TB treatment.31 Moreover, Xpert MTB/RIF increases the Mtb detection rate (23%) among culture-confirmed cases compared with smear microscopy, with higher accuracy of Mtb detection, limiting the misdiagnosis between Mtb and non-tuberculous mycobacteria.27,35 However, some studies reported false-positive results with Xpert MTB/RIF due to silent mutations [eg, at codon 514 of the rpoB gene]29 and false-negative results because of the inability to detect RIF-resistance conferring mutations outside the rpoB hotspot region.43 In addition, this test does not detect mutations in genes associated with isoniazid (INH) resistance but uses RIF resistance as a proxy for MDR-TB detection.44 Consequently, many INH mono-resistant TB cases are erroneously classified as drug-susceptible.
POC feasibility for Xpert MTB/RIF has been demonstrated in well-resourced clinics primarily because it is semi-automated and requires minimally trained non-technical personnel.45–48 Despite these advancements, several limitations are noteworthy, such as suboptimal sensitivity in special populations (HIV-positive adults, children, patients with extrapulmonary TB),49,50 the need for an uninterrupted power supply, and dependence on mild ambient conditions (15°C–30°C).51 Despite being designed for POC use, the Xpert MTB/RIF assay is predominantly implemented in centralised laboratories.52 Furthermore, despite reducing the time to TB diagnosis, there is no evidence of Xpert MTB/RIF reducing morbidity and mortality among TB patients in high TB/HIV burden settings53–56
The next-generation Xpert MTB/RIF Ultra (Cepheid Inc., Sunnyvale, CA, USA) assay has better Mtb identification and RIF resistance detection capabilities. It has a larger amplification chamber to increase the amount of sputum and two additional targets (IS1081 and IS6110) to identify Mtb.57,58 The bacilli limit of detection (LOD) for Xpert MTB/RIF Ultra is four-fold lower compared to Xpert MTB/RIF, at 15.6 CFU/mL vs 112.6 CFU/mL. The increased sensitivity of Xpert MTB/RIF Ultra is due to additional probes capable of detecting very low concentrations or “traces” of TB, making it more appropriate for use among children and people living with HIV/AIDS who often have paucibacillary or disseminated forms of TB.57 While the sensitivity of the Xpert MTB/RIF Ultra is 5% higher than that of Xpert MTB/RIF, specificity is 3.2% lower.59 Various studies reported a higher incremental sensitivity among paucibacillary forms of TB disease (childhood TB, HIV-associated TB, or extrapulmonary TB).60–62 However, specificity is lower in patients with a previous history of TB, generating false-positive results due to the detection of non-viable Mtb. When Xpert MTB/RIF Ultra probes detect only “traces” of TB - and not more substantial concentrations of TB bacteria – an inconclusive test result is produced.63 Furthermore, false positivity is associated with the recent previous TB, a high cycle threshold (>30), and a chest radiograph without features of active TB.41 Therefore, Xpert MTB/RIF Ultra results should be interpreted carefully, together with a comprehensive clinical history and physical examination2,4 in patients with recent previous TB.
The novel Xpert MTB/XDR assay (Cepheid Inc., Sunnyvale, CA, USA) is also a rapid, cartridge-based assay that is intended to be used as a reflex or follow-up test to any Mtb positive result for the detection of first- and second-line drug-resistance in sputum specimens.64 In specimens where Mtb has been detected, the Xpert MTB/XDR assay can also detect resistance-conferring mutations of INH (target genes: inhA promoter, katG, fabG1, oxyR-aphC intergenic region), fluoroquinolones (FQs) (gyrA and gyrB), ethionamide (ETH) (inhA promoter), and second-line injectable drugs (rrs and eis promoter).65 The Xpert MTB/XDR assay is a fully integrated and automated system utilising the exact sample processing techniques as the Xpert MTB/RIF and Ultra. Additionally, this assay can be run on existing GeneXpert platforms equipped with 10-colour modules. The rapid profiling of extended drug resistance is a fundamental benefit of the Xpert MTB/XDR assay.64 It also has minimal biosafety requirements, offers quick turnaround times and can be operated by health care professionals with limited training. Traditional culture-based DSTs typically take several weeks compared to the Xpert MTB/XDR assay, which produces results in less than 90 minutes.64
Several studies have also reported this assay’s high performance and specificity for detecting resistance to INH and second-line injectable drugs.57,65–67 The first prospective study that assessed the clinical diagnostic accuracy of the Xpert MTB/XDR assay for INH, FQ, ETH, and second-line TB drug resistance conducted in Africa, Europe, and South-East Asia reported a resistance detection sensitivity of 94% for INH, 95% for FQs, 54% for ETH, 73% for amikacin, 86% for kanamycin, and 61% for capreomycin. Specificity for all drugs was greater than 98%.68
While significant specificity and sensitivity data describing the Xpert MTB/XDR assay’s ability to detect DR-TB rapidly exists, shortcomings associated with this assay need to be acknowledged. The assay detects mutations only in “hot spots” of target resistance-conferring genes. Moreover, it cannot detect resistance against newer/repurposed drugs now included in the WHO-approved DR-TB treatment regimen (bedaquiline, delamanid, linezolid, clofazimine, carbapenems, and pyrazinamide). The 18-month cartridge shelf-life and the requirement for annual refitting and recalibration64 of the GeneXpert 10-colour multiplex technology for both new and pre-existing Cepheid GeneXpert Instrument Systems are significant additional limitations, especially in low- and middle-income countries. While the assay is attractive for decentralisation, its optimal placement in different locations needs to be guided by local diagnostic algorithms and local feasibility and cost-effectiveness. Moreover, POC implementation will be limited in high-burden countries due to cost, logistical constraints and poor infrastructure.69
Truenat Assays
In 2020, the WHO also recommended Truenat MTB, MTB Plus, and the RIF-resistance detection reflex assays (Truenat MTB-RIF Dx) (Molbio Diagnostics, India) as initial tests for the detection of TB and RIF resistance in all people being evaluated for pulmonary TB.2 Truenat uses real-time micro-PCR to detect the presence of major mutations (single nucleotide polymorphisms) in the Mtb genome that are known to cause resistance to RIF.70 A large multicentre clinical trial assessed the diagnostic accuracy of the Truenat assays MTB and MTB Plus to diagnose pulmonary TB and the MTB-RIF Dx assay to diagnose RIF resistance in symptomatic adults in India, 24% of whom were sputum culture-positive. Sensitivity and specificity for each assay were as follows: Truenat MTB: 73% (95% CI 67–78%) and 97% (95% CI 96–98); Truenat MTB Plus: 79% (95% CI 74–84) and 96% (95% CI 95–97) and Truenat MTB-RIF Dx: 84% (95% CI 62–94) and 94% (95% CI 90–97).71
The semi-automated Truenat tests are performed using the Trueprep sample preparation device that extracts DNA and the Truelab PCR device that produces a result in under one hour. Unlike the fully automated Xpert tests that simultaneously test for TB and RIF resistance, the Truenat test series requires several manual steps to be performed by trained technical laboratory staff. Trueprep and Truelab instruments are battery-powered, run-up to a full eight-hour day on a single battery charge, and may be operated without air conditioning at temperatures ≤40°C, enabling them to be positioned in microscopy centres.70
Moderate Complexity Automated NAATs
High-throughput molecular tests highlighted in this section are automated, highly sensitive and specific and use the same PCR technology as rapid molecular tests such as Xpert and Truenat. Several manufacturers have developed moderate complexity automated NAATs for detecting TB and resistance to RIF and INH on high throughput platforms in laboratories.72 Currently available high-throughput molecular tests for resistance to RIF and INH include Abbott’s RealTime MTB RIF/INH; BD MAX® MDR-TB, Roche’s Cobas MTB-RIF/INH, and Fluoro-Type (FT) MTBDR.2 Tests belonging to this class are faster and less complex to perform than phenotypic culture-based DSTs and LPA and have the advantage of being automated after the initial sample preparation step. Moderate complexity automated NAATs may be used as an initial test for the detection of TB and resistance to both first-line TB drugs simultaneously (RIF and INH). They offer the potential for the rapid provision of accurate results (important to patients) and for testing efficiency where high volumes of tests are required daily. Hence, these technologies are suited to areas with a high population density and rapid sample referral systems.
Abbott Molecular has two NAATs for TB, one for the detection of Mtb (RealTime MTB-96 samples per run) that targets both the IS6110 genetic element and the PstS1 (Rv0934) gene and the other for the detection of both RIF and INH resistance (RealTime MTB RIF/INH). The RIF and INH resistance tests use eight dye-labelled probes to detect variants in the RIF resistance determining region of the rpoB gene and four probes to detect INH resistance, with two probes each for the katG and inhA genes.6 The sensitivity and specificity of the Abbott RealTime MTB and INH/RIF assays for detection of Mtb and detection of INH resistance were 92.4% (95% CI 83.6–96.9) and 95.4% (95% CI 91.1–97.7) and 84.2% (95% CI 60.4–96.6) and 100% (95% CI 89.7–100), respectively. In the case of RIF resistance, no discrepant results were observed,73 a finding supported by several other studies.74–77
The multiplexed real-time PCR (MAX MDR-TB) (Becton Dickinson) NAAT platform using five-colour detection enables direct detection of Mtb in raw sputum or concentrated sputum sediments. This test satisfies the WHO consolidated guidelines for Mtb diagnostics by providing rapid TB detection using multicopy genomic elements IS6110 and IS1081 together or singly.2 To detect resistance to RIF, the test targets codons 426–452 of the rpoB gene; for detecting resistance to INH, the test targets both the inhA promoter region and the 315 codons of the katG gene.78 A recent diagnostic accuracy study using the BD MAX MDR-TB test found sensitivity and specificity of 90.6% and 98.5%, and 82.5% and 98.9% for detection of Mtb in pulmonary and extrapulmonary samples, respectively. For detecting INH and RIF resistance, sensitivity and specificity were 71.4% and 96.8%, and 100% and 93.9%, respectively.79 Similar reports of the diagnostic accuracy of the BD MAX MDR-TB assay have been reported from a diversity of geographic and TB prevalence settings.79–84 Overall, the BD MAX™ MDR-TB assay is automated and integrated and requires a stable source of electricity; 24 specimens can be tested in one run and the turnaround time from the start of testing to the result is four hours. This platform is expected to be most suitable for use in high throughput central laboratories where minimal operator hands-on time is desirable.
Roche Cobas MTB-RIF/INH is an automated, qualitative real-time PCR test designed as a reflex test together with cobas® MTB to detect RIF resistance-associated mutations of the rpoB gene and INH resistance-associated mutations in the katG and inhA genes. The test is intended for use on raw sputum, decontaminated sputum, or bronchial alveolar lavage samples, irrespective of smear status.1,2 The LOD for this test is 7.6–8.8 CFU/mL.6 Sensitivity and specificity for RIF vs INH resistance detection was 88.4% and 97.6% vs 76.6% and 100.0%, respectively.85 Similar findings were noted in other comparative studies assessing Cobas MTB-RIF/INH.86,87
The FluoroType MTBDR (FT-MTBDR; Hain Lifescience) is a new in vitro automated molecular-based assay that simultaneously detects Mtb mutations associated with RIF and INH in a single reaction without the need for reflexing.88,89 Decontaminated sputum and culture isolates can be used as sample material. The FluoroType MTBDR test uses asymmetric excess PCR and light on/off probes. The LOD is 20 CFU/mL for the FluoroType MTBDR assay (FluoroType® MDRTB, 2019, Unitaid, 2017). Manual (FluoroLyse) and automated (GenoXtract) options are available for DNA extraction. The FluoroCycler XT for the MTBDR assay is used for amplification and detection. The diagnostic accuracy of FluoroType MTB and MTBDR VER 2.0 assays was assessed in smear-positive and -negative specimens. Sensitivity for detecting Mtb complex in smear-positive and smear-negative specimens were 97.9% and 91.8%, respectively. Sensitivity and specificity for detecting RIF versus INH resistance from smear-positive specimens were 96.9% and 97% versus 98.3% and 97.3%, respectively.90 Other studies also noted similar findings.88,91,92
While accuracy, speed, and capacity to concurrently test large sample volumes are clear advantages of high-throughput molecular tests, their centralised placement is a clear disadvantage due to reduced patient accessibility and shortened result turnaround time. Furthermore, test costs are yet to be made public. Hence, affordability to endemic resource-limited settings remains unknown.93
Line Probe Assays
In 2008, the WHO recommended using LPAs as initial DST for first- and second-line TB drugs instead of liquid culture. LPAs are highly accurate and produce results within five hours compared with the two- to six-week turnaround time required for culture-based DST.1,2 LPA technology is based on reverse hybridisation of DNA on a visually read test strip, targeting DNA sequences associated with resistance to first-line (RIF and INH) and some second-line TB drugs (fluoroquinolones and second-line injectable drugs).94 Current WHO recommended LPAs for initial drug-resistance testing on sputum smear-positive samples include GenoType MTBDRplus and GenoType MTBDRsl (Hain LifeScience GmbH, Germany).2
The GenoType MTBDRplus (First-line Line probe assay; FL-LPA) assay detects Mtb complex and drug resistance by targeting specific mutations in the rifampicin resistance determining region of the rpoB gene (codon 505 to 533), as well as mutations in the isoniazid resistance determining inhA promoter (−16 to −8 nucleotides upstream of inhA) and katG (codon 315), from direct sputum smear-positive samples or indirect culture isolates.95–98 In sputum smear-positive samples, sensitivity and specificity for detecting RIF and INH resistance were 96.7% and 98.8%, and 90.2% and 99.2%, respectively.99–103 The sensitivity and specificity of MTBDRplus to detect RIF on culture isolates were 95.1% (95% CI 92.2% to 98.1%) and 100%, respectively. The sensitivity and specificity to detect INH resistance were 96.1% (93.5% to 98.7%) and 96.1% (90.8% to 100%), respectively.104 The GenoType MTBDRplus enables a rapid result from sputum smear-positive specimens, thereby enabling appropriate treatment; however, the dependence on culture isolates from respiratory tract samples in the case of smear-negative specimens is a major shortcoming of this assay. Furthermore, the MTBDRplus assay, which produces amplicons in an open-tube format, requires an experienced operator, strict adherence to standard operating procedures with a minimum of three separate rooms for DNA extraction, and multiple procedures to minimise the risk of amplicon cross-contamination. These assays also require experienced readers to interpret the hybridised bands, although this can be semi-automated at additional expense.91
The Genotype® MTBDRsl assay (Second Line –Line probe assay; SL-LPA) version 2.0, released in 2015, detects mutations associated with FQ and SLID resistance. The MTBDRsl assay includes the quinolone resistance-determining regions of the gyrA gene (codon 85 to 96) and the gyrB (codon 536 to 541) gene, as well as the SLID resistance-determining regions of the rrs gene (position 1401, 1402 and 1484) and the eis gene (from −37 to −2 nucleotides upstream). The assay procedure can be performed directly using a processed sputum sample or indirectly using DNA isolated and amplified from Mtb culture. MTBDRsl has a pooled sensitivity and specificity of 86.2% and 98.6%, respectively, for detecting FQ resistance by direct testing, and pooled sensitivity and specificity of 87.0% and 99.5%, respectively, for the detection of SLID resistance.105 Several other studies assessed the diagnostic accuracy of the Genotype® MTBDRsl assay and reported similar findings.104,106–108
In summary, LPAs are rapid, simple, easy to perform and straightforward to interpret (generated manually or automatically). Limitations to using LPAs include the need for complex laboratory infrastructure, including expensive equipment ordinarily available in reference laboratories only.2 Furthermore, the high number of indeterminate results and restriction of LPA target coverage to common high-confidence mutations only present additional limitations.
Impediments to the Rollout of Rapid Molecular Assays
The WHO recommends universal access to new rapid molecular TB diagnostic technologies to reduce the high TB morbidity and mortality rates. Underdiagnosis of TB remains a problem, with only two-thirds of those who develop TB currently being detected and only half of these cases being bacteriologically confirmed.2 The main reasons for these gaps are inadequate diagnostic capacity and an overreliance on chest radiography and/or sputum smear microscopy as diagnostic tools.22 Patients with HIV-associated TB, sputum smear-negative TB, and drug-resistant TB are the most disadvantaged by the failure of microscopy as a primary diagnostic tool.109 The diagnosis of HIV-associated and drug-resistant TB is expensive, complex, slow and technically challenging, relying on conventional culture and drug susceptibility testing.110 The long delay (up to several weeks) required to obtain results has devastating consequences for patients who go undiagnosed (and therefore untreated or suboptimally treated), are diagnosed too late, or are lost to follow-up before treatment can be initiated.111 Therefore, detecting more TB cases early and rapidly identifying drug resistance is essential for improving individual patient care and interrupting transmission in the community. This requires universal access to modern tools and innovative strategies.2,111,112 However, significant economic challenges impede the development and implementation of new diagnostics.
Developer, Policy, and Programmatic Perspectives
The lack of well-defined target product profiles (TPP) remains an ongoing challenge from the test developer’s perspective.113 Prioritisation of test features may differ significantly based on the setting and local disease burden. Considerations in each setting may include the level of automation or integration with multiplexed platforms, test throughput, result reporting requirements, position within a diagnostic algorithm (eg, screening of asymptomatic vs symptomatic patients), location within health systems (POC vs peripheral or centralised laboratory), target populations (HIV-infected, inpatients vs outpatients, adult vs paediatric), target conditions (eg, latent TB vs sub-clinical TB vs active TB; pulmonary vs extrapulmonary TB), drug-resistance profiles (which drugs should be evaluated in a changing treatment landscape) and the availability of well-characterised biological samples.113,114 The absence of a validated global biomarker that detects active TB disease poses another challenge, impeding the development of a “one size fits all” TB test.115
Many TB endemic settings incorporate molecular tests in their TB diagnostic algorithm. A significant challenge for incorporating rapid molecular assays from a policy perspective is the lack of data assessing the impact of new TB diagnostic tools on patient outcomes.116 To produce estimates of effectiveness for economic evaluation, studies must also assess clinical outcomes through longitudinal follow-up, which increases study costs and duration, and is rarely measured as part of diagnostic test accuracy studies.114 Furthermore, the performance and impact of implementing new tests within existing diagnostic algorithms are impeded by limited data, and cost-effectiveness studies may be highly context-dependent and may not translate into an “affordable” test.114
There is uncertainty if TB diagnostic programmes can afford recurring investments as multiple TB diagnostic tools emerge into the market. Furthermore, studies assessing TB diagnostic accuracy may only provide limited data on various programmatic considerations such as simplicity, affordability, ability to be used at the bedside, personnel training, required infrastructure and quality assurance.114 To improve existing TB diagnostic tools or to incorporate new adjunctive diagnostics, policymakers and programme implementers need to consider the following favourable characteristics: more efficient, lower cost, reduced sample processing time and reagent costs, shorter time to a result, minimum training and skill-level requirements, while offering the same or better diagnostic accuracy for detection of prevalent DR-TB resistance profiles as the existing programmatic test/s.
Conclusion
The global rollout of WHO-endorsed molecular assays has improved the detection of DR-TB cases. Despite this progress, there is no reliable and rapid POC test for diagnosing DR-TB. To bridge this gap, rapid molecular diagnostic tests for DR-TB detection should be accurate, inexpensive, performed on an easily accessible sample, detect prevalent circulating drug-resistant strains and provide results within a short turnaround time to enable timely treatment initiation, reduce pre-treatment loss to follow-up, and shorten the time to an optimal treatment regimen. Each of the assays included in this review demonstrates their own strengths and weaknesses, and their selection for programmatic implementation will depend heavily on the available skills and resources, the capacity and distribution of laboratory infrastructure, the positioning of the assay within the programmatic algorithm, and the epidemiology and evolution of the local DR-TB epidemic.
Funding
Authors partly supported by the South African Medical Research Council and by the European and Developing Countries Clinical Trials Partnership (TMA2018SF-2476 and RIA2019IR-2888).
Disclosure
The authors declare that the research was conducted without any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. World Health Organisation. Global tuberculosis report 2021; 2021.
2. World Health Organization. WHO Consolidated Guidelines on Tuberculosis: Module 3: Diagnosis–Rapid Diagnostics for Tuberculosis Detection. World Health Organization; 2021.
3. Bulterys MA, Wagner B, Redard-Jacot M, et al. Point-of-care urine LAM tests for tuberculosis diagnosis: a status update. J Clin Med. 2020;9(1):111. doi:10.3390/jcm9010111
4. García-Basteiro AL, DiNardo A, Saavedra B, et al. Point of care diagnostics for tuberculosis. Pulmonology. 2018;24(2):73–85. doi:10.1016/j.rppnen.2017.12.002
5. Dheda K, Ruhwald M, Theron G, Peter J, Yam WC. Point‐of‐care diagnosis of tuberculosis: past, present and future. Respirology. 2013;18(2):217–232. doi:10.1111/resp.12022
6. Branigan D. AN ACTIVIST’S. GUIDE to “Tuberculosis Diagnostic Tools”. New York, NY, USA: Treatment Action Group; 2020.
7. Schito M, Peter TF, Cavanaugh S, et al. Opportunities and challenges for cost-efficient implementation of new point-of-care diagnostics for HIV and tuberculosis. J Infect Dis. 2012;205(suppl_2):S169–S180. doi:10.1093/infdis/jis044
8. Ryu YJ. Diagnosis of pulmonary tuberculosis: recent advances and diagnostic algorithms. Tuberc Respir Dis. 2015;78(2):64–71. doi:10.4046/trd.2015.78.2.64
9. Harries A. Tuberculosis and human immunodeficiency virus infection in developing countries. Lancet. 1990;335:387–390. doi:10.1016/0140-6736(90)90216-R
10. Peter JG, Theron G, Muchinga TE, Govender U, Dheda K, Goletti D. The diagnostic accuracy of urine-based Xpert MTB/RIF in HIV-infected hospitalized patients who are smear-negative or sputum scarce. PLoS One. 2012;7(7):e39966. doi:10.1371/journal.pone.0039966
11. Peter JG, Theron G, van Zyl-Smit R, et al. Diagnostic accuracy of a urine lipoarabinomannan strip-test for TB detection in HIV-infected hospitalised patients. Eur Respir J. 2012;40(5):1211–1220. doi:10.1183/09031936.00201711
12. Paris L, Magni R, Zaidi F, et al. Urine lipoarabinomannan glycan in HIV-negative patients with pulmonary tuberculosis correlates with disease severity. Sci Transl Med. 2017;9(420). doi:10.1126/scitranslmed.aal2807
13. Cannas A, Goletti D, Girardi E, et al. Mycobacterium tuberculosis DNA detection in soluble fraction of urine from pulmonary tuberculosis patients. Int J Tuberc Lung Dis. 2008;12(2):146–151.
14. Oreskovic A, Panpradist N, Marangu D, et al. Diagnosing pulmonary tuberculosis by using sequence-specific purification of urine cell-free DNA. J Clin Microbiol. 2021;59(8):e0007421. doi:10.1128/JCM.00074-21
15. Atherton RR, Cresswell FV, Ellis J, et al. Detection of Mycobacterium tuberculosis in urine by Xpert MTB/RIF Ultra: a useful adjunctive diagnostic tool in HIV-associated tuberculosis. Int J Infect Dis. 2018;75:92–94. doi:10.1016/j.ijid.2018.07.007
16. Horváth I, Hunt J, Barnes PJ, et al. Exhaled breath condensate: methodological recommendations and unresolved questions. Eur Respir J. 2005;26(3):523–548. doi:10.1183/09031936.05.00029705
17. Chen D, Bryden NA, Bryden WA, et al. Non-volatile organic compounds in exhaled breath particles correspond to active tuberculosis. Sci Rep. 2022;12(1):7919. doi:10.1038/s41598-022-12018-6
18. Chen D, Bryden WA, Wood R. Detection of tuberculosis by the analysis of exhaled breath particles with high-resolution mass spectrometry. Sci Rep. 2020;10(1):7647. doi:10.1038/s41598-020-64637-6
19. Zijenah LS. The world health organization recommended TB diagnostic tools. Tuberculosis. 2018;2:71–90.
20. Hobby GL, Holman AP, Iseman MD, Jones JM. Enumeration of tubercle bacilli in sputum of patients with pulmonary tuberculosis. Antimicrob Agents Chemother. 1973;4(2):94–104. doi:10.1128/AAC.4.2.94
21. Cudahy P, Shenoi SV. Diagnostics for pulmonary tuberculosis. Postgrad Med J. 2016;92(1086):187–193. doi:10.1136/postgradmedj-2015-133278
22. Harries AD, Kumar A. Challenges and progress with diagnosing pulmonary tuberculosis in low-and middle-income countries. Diagnostics. 2018;8(4):78. doi:10.3390/diagnostics8040078
23. Cruciani M, Scarparo C, Malena M, Bosco O, Serpelloni G, Mengoli C. Meta-analysis of BACTEC MGIT 960 and BACTEC 460 TB, with or without solid media, for detection of mycobacteria. J Clin Microbiol. 2004;42(5):2321–2325. doi:10.1128/JCM.42.5.2321-2325.2004
24. Ardito F, Posteraro B, Sanguinetti M, Zanetti S, Fadda G. Evaluation of BACTEC Mycobacteria Growth Indicator Tube (MGIT 960) automated system for drug susceptibility testing of Mycobacterium tuberculosis. J Clin Microbiol. 2001;39(12):4440–4444. doi:10.1128/JCM.39.12.4440-4444.2001
25. Schön T, Miotto P, Köser CU, Viveiros M, Böttger E, Cambau E. Mycobacterium tuberculosis drug-resistance testing: challenges, recent developments and perspectives. Clin Microbiol Infect. 2017;23(3):154–160. doi:10.1016/j.cmi.2016.10.022
26. Campbell EA, Korzheva N, Mustaev A, et al. Structural mechanism for rifampicin inhibition of bacterial RNA polymerase. Cell. 2001;104(6):901–912. doi:10.1016/S0092-8674(01)00286-0
27. Steingart KR, Sohn H, Schiller I, et al. Xpert® MTB/RIF assay for pulmonary tuberculosis and rifampicin resistance in adults. Cochrane Database Syst Rev. 2013;(1). doi:10.1002/14651858.CD009593.pub2
28. Wang S, Zhao B, Song Y, et al. Molecular characterization of the rpoB gene mutations of Mycobacterium tuberculosis isolated from China. J Tuberc Res. 2013;01(01):1–8. doi:10.4236/jtr.2013.11001
29. Bunsow E, Ruiz-Serrano MJ, Roa PL, Kestler M, Viedma DG, Bouza E. Evaluation of GeneXpert MTB/RIF for the detection of Mycobacterium tuberculosis and resistance to rifampin in clinical specimens. J Infect. 2014;68(4):338–343. doi:10.1016/j.jinf.2013.11.012
30. Ochang EA, Udoh UA, Emanghe UE, et al. Evaluation of rifampicin resistance and 81-bp rifampicin resistant determinant region of rpoB gene mutations of Mycobacterium tuberculosis detected with XpertMTB/Rif in Cross River State, Nigeria. Int J Mycobacteriol. 2016;5(5):145. doi:10.1016/j.ijmyco.2016.09.007
31. Ramasamy P, Sounderrajan V, Harshavardhan S, Harshavardhan S. Current perceptions on advanced molecular diagnostics for drug-resistant Mycobacterium tuberculosis. Biomed Pharmacol J. 2021;14(3):1249–1257. doi:10.13005/bpj/2226
32. Nguyen TNA, Berre A-L, Bañuls A-L, Nguyen TVA. Molecular diagnosis of drug-resistant tuberculosis; a literature review. Front Microbiol. 2019;10:794. doi:10.3389/fmicb.2019.00794
33. Lee H, Seong M, Park S, et al. Diagnostic accuracy of Xpert® MTB/RIF on bronchoscopy specimens in patients with suspected pulmonary tuberculosis. Int J Tuberc Lung Dis. 2013;17(7):917–921. doi:10.5588/ijtld.12.0885
34. Scott LE, Beylis N, Nicol M, et al. Diagnostic accuracy of Xpert MTB/RIF for extrapulmonary tuberculosis specimens: establishing a laboratory testing algorithm for South Africa. J Clin Microbiol. 2014;52(6):1818–1823. doi:10.1128/JCM.03553-13
35. Sharma SK, Kohli M, Yadav RN, et al. Evaluating the diagnostic accuracy of Xpert MTB/RIF assay in pulmonary tuberculosis. PLoS One. 2015;10(10):e0141011. doi:10.1371/journal.pone.0141011
36. Allahyartorkaman M, Mirsaeidi M, Hamzehloo G, Amini S, Zakiloo M, Nasiri MJ. Low diagnostic accuracy of Xpert MTB/RIF assay for extrapulmonary tuberculosis: a multicenter surveillance. Sci Rep. 2019;9(1):1–6. doi:10.1038/s41598-019-55112-y
37. Bahr NC, Nuwagira E, Evans EE, et al. Diagnostic accuracy of Xpert MTB/RIF Ultra for tuberculous meningitis in HIV-infected adults: a prospective cohort study. Lancet Infect Dis. 2018;18(1):68–75. doi:10.1016/S1473-3099(17)30474-7
38. Mekkaoui L, Hallin M, Mouchet F, et al. Performance of Xpert MTB/RIF Ultra for diagnosis of pulmonary and extra-pulmonary tuberculosis, one year of use in a multi-centric hospital laboratory in Brussels, Belgium. PLoS One. 2021;16(4):e0249734. doi:10.1371/journal.pone.0249734
39. Nicol MP, Workman L, Prins M, et al. Accuracy of Xpert MTB/RIF Ultra for the diagnosis of pulmonary tuberculosis in children. Pediatr Infect Dis J. 2018;37(10):e261–e3. doi:10.1097/INF.0000000000001960
40. Moure R, Martín R, Alcaide F. Effectiveness of an integrated real-time PCR method for detection of the Mycobacterium tuberculosis complex in smear-negative extrapulmonary samples in an area of low tuberculosis prevalence. J Clin Microbiol. 2012;50(2):513–515. doi:10.1128/JCM.06467-11
41. Rasheed W, Rao NA, Adel H, Baig MS, Adil SO. Diagnostic accuracy of Xpert MTB/RIF in sputum smear-negative pulmonary tuberculosis. Cureus. 2019;11(8):e5391. doi:10.7759/cureus.5391
42. Khadka P, Thapaliya J, Basnet RB, Ghimire GR, Amatya J, Rijal BP. Diagnosis of tuberculosis from smear-negative presumptive TB cases using Xpert MTB/Rif assay: a cross-sectional study from Nepal. BMC Infect Dis. 2019;19(1):1090. doi:10.1186/s12879-019-4728-2
43. Sanchez-Padilla E, Merker M, Beckert P, et al. Detection of drug-resistant tuberculosis by Xpert MTB/RIF in Swaziland. N Engl J Med. 2015;372(12):1181–1182. doi:10.1056/NEJMc1413930
44. Manson AL, Cohen KA, Abeel T, et al. Genomic analysis of globally diverse Mycobacterium tuberculosis strains provides insights into the emergence and spread of multidrug resistance. Nat Genet. 2017;49(3):395–402. doi:10.1038/ng.3767
45. Clouse K, Page-Shipp L, Dansey H, et al. Implementation of Xpert MTB/RIF for routine point-of-care diagnosis of tuberculosis at the primary care level. South Afr Med J. 2012;102(10):805–807. doi:10.7196/SAMJ.5851
46. Hanrahan C, Clouse K, Bassett J, et al. The patient impact of point-of-care vs. laboratory placement of Xpert® MTB/RIF. Int J Tuberc Lung Dis. 2015;19(7):811–816. doi:10.5588/ijtld.15.0013
47. Hanrahan CF, Selibas K, Deery CB, et al. Time to treatment and patient outcomes among TB suspects screened by a single point-of-care xpert MTB/RIF at a primary care clinic in Johannesburg, South Africa. PLoS One. 2013;8(6):e65421. doi:10.1371/journal.pone.0065421
48. Theron G, Zijenah L, Chanda D, et al. Feasibility, accuracy, and clinical effect of point-of-care Xpert MTB/RIF testing for tuberculosis in primary-care settings in Africa: a multicentre, randomised, controlled trial. Lancet. 2014;383(9915):424–435. doi:10.1016/S0140-6736(13)62073-5
49. Detjen AK, DiNardo AR, Leyden J, et al. Xpert MTB/RIF assay for the diagnosis of pulmonary tuberculosis in children: a systematic review and meta-analysis. Lancet Respir Med. 2015;3(6):451–461. doi:10.1016/S2213-2600(15)00095-8
50. Marcy O, Ung V, Goyet S, et al. Performance of Xpert MTB/RIF and alternative specimen collection methods for the diagnosis of tuberculosis in HIV-infected children. Clin Infect Dis. 2016;62(9):1161–1168. doi:10.1093/cid/ciw036
51. Schnippel K, Meyer‐Rath G, Long L, et al. Scaling up Xpert MTB/RIF technology: the costs of laboratory‐vs. clinic‐based roll‐out in South Africa. Trop Med Int Health. 2012;17(9):1142–1151. doi:10.1111/j.1365-3156.2012.03028.x
52. Theron G. Point‐of‐care technologies for the diagnosis of active tuberculosis. Mol Microbiol. 2016;556–579. doi:10.1128/9781555819071.ch40
53. Churchyard GJ, Stevens WS, Mametja LD, et al. Xpert MTB/RIF versus sputum microscopy as the initial diagnostic test for tuberculosis: a cluster-randomised trial embedded in South African roll-out of Xpert MTB/RIF. Lancet Global Health. 2015;3(8):e450–e457. doi:10.1016/S2214-109X(15)00100-X
54. Cox HS, Mbhele S, Mohess N, et al. Impact of Xpert MTB/RIF for TB diagnosis in a primary care clinic with high TB and HIV prevalence in South Africa: a pragmatic randomised trial. PLoS Med. 2014;11(11):e1001760. doi:10.1371/journal.pmed.1001760
55. Theron G, Peter J, Calligaro G, et al. Determinants of PCR performance (Xpert MTB/RIF), including bacterial load and inhibition, for TB diagnosis using specimens from different body compartments. Sci Rep. 2014;4(1):1–10.
56. Theron G, Peter J, Dowdy D, Langley I, Squire SB, Dheda K. Do high rates of empirical treatment undermine the potential effect of new diagnostic tests for tuberculosis in high-burden settings? Lancet Infect Dis. 2014;14(6):527–532. doi:10.1016/S1473-3099(13)70360-8
57. Chakravorty S, Simmons AM, Rowneki M, et al. The new Xpert MTB/RIF Ultra: improving detection of Mycobacterium tuberculosis and resistance to rifampin in an assay suitable for point-of-care testing. mBio. 2017;8(4):e00812–e00817. doi:10.1128/mBio.00812-17
58. Perez-Risco D, Rodriguez-Temporal D, Valledor-Sanchez I, Alcaide F, Land GA. Evaluation of the Xpert MTB/RIF Ultra assay for direct detection of Mycobacterium tuberculosis complex in smear-negative extrapulmonary samples. J Clin Microbiol. 2018;56(9):e00659–18. doi:10.1128/JCM.00659-18
59. Dorman SE, Schumacher SG, Alland D, et al. Xpert MTB/RIF Ultra for detection of Mycobacterium tuberculosis and rifampicin resistance: a prospective multicentre diagnostic accuracy study. Lancet Infect Dis. 2018;18(1):76–84. doi:10.1016/S1473-3099(17)30691-6
60. Kohli M, Schiller I, Dendukuri N, et al. Xpert MTB/RIF Ultra and Xpert MTB/RIF assays for extrapulmonary tuberculosis and rifampicin resistance in adults. Cochrane Database Syst Rev. 2021;(1). doi:10.1002/14651858.CD012768.pub3
61. Sabi I, Rachow A, Mapamba D, et al. Xpert MTB/RIF Ultra assay for the diagnosis of pulmonary tuberculosis in children: a multicentre comparative accuracy study. J Infect. 2018;77(4):321–327. doi:10.1016/j.jinf.2018.07.002
62. Wang G, Wang S, Jiang G, et al. Xpert MTB/RIF Ultra improved the diagnosis of paucibacillary tuberculosis: a prospective cohort study. J Infect. 2019;78(4):311–316. doi:10.1016/j.jinf.2019.02.010
63. Mishra H, Reeve BW, Palmer Z, et al. Xpert MTB/RIF Ultra and Xpert MTB/RIF for diagnosis of tuberculosis in an HIV-endemic setting with a high burden of previous tuberculosis: a two-cohort diagnostic accuracy study. Lancet Respir Med. 2020;8(4):368–382. doi:10.1016/S2213-2600(19)30370-4
64. Cepheid. Xpert MTB-XDR English Package Insert 302–351. 4 Rev A; 2020.
65. Cao Y, Parmar H, Gaur RL, et al. Xpert MTB/XDR: a 10-color reflex assay suitable for point-of-care settings to detect isoniazid, fluoroquinolone, and second-line-injectable-drug resistance directly from Mycobacterium tuberculosis-positive sputum. J Clin Microbiol. 2021;59(3):e02314–e02320. doi:10.1128/JCM.02314-20
66. Georghiou SB, Penn-Nicholson A, de Vos M, et al. Analytical performance of the Xpert MTB/XDR® assay for tuberculosis and expanded resistance detection. Diagn Microbiol Infect Dis. 2021;101(1):115397. doi:10.1016/j.diagmicrobio.2021.115397
67. Xie YL, Chakravorty S, Armstrong DT, et al. Evaluation of a rapid molecular drug-susceptibility test for tuberculosis. N Engl J Med. 2017;377(11):1043–1054. doi:10.1056/NEJMoa1614915
68. Penn-Nicholson A, Georghiou SB, Ciobanu N, et al. Clinical evaluation of the Xpert MTB/XDR assay for rapid detection of isoniazid, fluoroquinolone, ethionamide and second-line drug resistance: a cross-sectional multicentre diagnostic accuracy study. medRxiv. 2021. doi:10.1101/2021.05.06.21256505
69. Bainomugisa A, Gilpin C, Coulter C, Marais BJ. New xpert MTB/XDR: added value and future in the field. Eur Respiratory Soc. 2020;56(5):2003616. doi:10.1183/13993003.03616-2020
70. Truenat. MTB-RIF Dx English Package Insert; 2018.
71. Penn-Nicholson A, Gomathi SN, Ugarte-Gil C, et al. A prospective multicentre diagnostic accuracy study for the Truenat tuberculosis assays. Eur Respir J. 2021;58(5):2100526. doi:10.1183/13993003.00526-2021
72. Kohli M, MacLean E, Pai M, Denkinger CM. Web Annex 4.8. Moderate complexity automated NAATs: diagnostic accuracy for TB detection and detection of resistance to rifampicin and isoniazid. A systematic review and meta-analysis. WHO consolidated guidelines on tuberculosis Module 3: diagnosis–rapid diagnostics for tuberculosis detection; 2021:181.
73. Araya BT, Ali KE, Geleta DA, Tekele SG, Tulu KD, Quinn F. Performance of the Abbott RealTime MTB and RIF/INH resistance assays for the detection of Mycobacterium tuberculosis and resistance markers in sputum specimens. PLoS One. 2021;16(5):e0251602. doi:10.1371/journal.pone.0251602
74. David A, Singh L, Da Silva P, Scott L, Stevens W. The performance of the Abbott real time MTB RIF/INH compared to the MTBDRplus V2 for the identification of MDR-TB among isolates. Infect Drug Resist. 2020;13:3301. doi:10.2147/IDR.S247524
75. Kostera J, Leckie G, Abravaya K, Wang H. Performance of the Abbott RealTime MTB RIF/INH resistance assay when used to test Mycobacterium tuberculosis specimens from Bangladesh. Infect Drug Resist. 2018;11:695. doi:10.2147/IDR.S158953
76. Scott L, David A, Noble L, et al. Performance of the Abbott RealTi me MTB and MTB RIF/INH assays in a setting of high tuberculosis and HIV coinfection in South Africa. J Clin Microbiol. 2017;55(8):2491–2501. doi:10.1128/JCM.00289-17
77. Wang M-G, Xue M, Wu S-Q, et al. Abbott RealTime MTB and MTB RIF/INH assays for the diagnosis of tuberculosis and rifampicin/isoniazid resistance. Infect Genet Evol. 2019;71:54–59. doi:10.1016/j.meegid.2019.03.012
78. Dickinson B. BD MAX™ multi drug resistant tuberculosis (MDR-TB) assay. Pack insert; 2020.
79. Sağiroğlu P, Atalay MA. Evaluation of the performance of the BD MAX MDR-TB test in the diagnosis of Mycobacterium tuberculosis complex in extrapulmonary and pulmonary samples. Expert Rev Mol Diagn. 2021;21(12):1361–1367. doi:10.1080/14737159.2021.1997594
80. Shah M, Paradis S, Betz J, et al. Multicenter study of the accuracy of the BD MAX™ MDR-TB assay for detection of Mycobacterium tuberculosis complex and mutations associated with resistance to rifampin and isoniazid. Clin Infect Dis. 2019;71(5):1161–1167.
81. Ciesielczuk H, Kouvas N, North N, Buchanan R, Tiberi S. Evaluation of the BD MAX™ MDR-TB assay in a real-world setting for the diagnosis of pulmonary and extra-pulmonary TB. Eur J Clin Microbiol Infect Dis. 2020;39(7):1321–1327. doi:10.1007/s10096-020-03847-2
82. Beutler M, Plesnik S, Mihalic M, et al. A pre-clinical validation plan to evaluate analytical sensitivities of molecular diagnostics such as BD MAX MDR-TB, Xpert MTB/Rif Ultra and FluoroType MTB. PLoS One. 2020;15(1):e0227215. doi:10.1371/journal.pone.0227215
83. Hofmann-Thiel S, Plesnik S, Mihalic M, et al. Clinical evaluation of BD MAX MDR-TB assay for direct detection of Mycobacterium tuberculosis complex and resistance markers. J Mol Diagn. 2020;22(10):1280–1286. doi:10.1016/j.jmoldx.2020.06.013
84. Gotuzzo E, King B, Dorman SE, et al. Multicenter study of the accuracy of the BD MAX MDR-TB assay for detection of Mycobacterium tuberculosis complex and mutations associated with resistance to rifampin and isoniazid. Clin Infect Dis. 2019. doi:10.1093/cid/ciz932
85. Nadarajan D, Hillemann D, Kamara R, et al. Evaluation of the Roche cobas MTB and MTB-RIF/INH assays in samples from Germany and Sierra Leone. J Clin Microbiol. 2021;59(5):e02983–20. doi:10.1128/JCM.02983-20
86. Scott L, David A, Govender L, et al. Performance of the Roche cobas MTB assay for the molecular diagnosis of pulmonary tuberculosis in a high HIV burden setting. J Mol Diagn. 2020;22(10):1225–1237. doi:10.1016/j.jmoldx.2020.06.018
87. de Vos M, Scott L, David A, et al. Comparative analytical evaluation of four centralized platforms for the detection of Mycobacterium tuberculosis complex and resistance to rifampicin and isoniazid. J Clin Microbiol. 2021;59(3):e02168–20. doi:10.1128/JCM.02168-20
88. Haasis C, Rupp J, Andres S, et al. Validation of the FluoroType® MTBDR assay using respiratory and lymph node samples. Tuberculosis. 2018;113:76–80. doi:10.1016/j.tube.2018.09.004
89. Svensson E, Folkvardsen DB, Rasmussen EM, Lillebaek T. Detection of Mycobacterium tuberculosis complex in pulmonary and extrapulmonary samples with the FluoroType MTBDR assay. Clin Microbiol Infect. 2021;27(10):
90. Dippenaar A, Derendinger B, Dolby T, et al. Diagnostic accuracy of the FluoroType MTB and MTBDR VER 2.0 assays for the centralised high throughput detection of Mycobacterium tuberculosis complex DNA and isoniazid and rifampicin resistance. Clin Microbiol Infect. 2021;27(9):
91. de Vos M, Derendinger B, Dolby T, et al. Diagnostic accuracy and utility of FluoroType MTBDR, a new molecular assay for multidrug-resistant tuberculosis. J Clin Microbiol. 2018;56(9):e00531–18. doi:10.1128/JCM.00531-18
92. Hillemann D, Haasis C, Andres S, Behn T, Kranzer K, Land GA. Validation of the FluoroType MTBDR assay for detection of rifampin and isoniazid resistance in Mycobacterium tuberculosis complex isolates. J Clin Microbiol. 2018;56(6):e00072–18. doi:10.1128/JCM.00072-18
93. MacLean E, Kohli M, Weber SF, et al. Advances in molecular diagnosis of tuberculosis. J Clin Microbiol. 2020;58(10):e01582–19. doi:10.1128/JCM.01582-19
94. Mäkinen J, Marttila HJ, Marjamäki M, Viljanen MK, Soini H. Comparison of two commercially available DNA line probe assays for detection of multidrug-resistant Mycobacterium tuberculosis. J Clin Microbiol. 2006;44(2):350–352. doi:10.1128/JCM.44.2.350-352.2006
95. Bang D, Bengård Andersen AS, Thomsen VØ. Rapid genotypic detection of rifampin-and isoniazid-resistant Mycobacterium tuberculosis directly in clinical specimens. J Clin Microbiol. 2006;44(7):2605–2608. doi:10.1128/JCM.00752-06
96. Gamboa F, Cardona P, Manterola J, et al. Evaluation of a commercial probe assay for detection of rifampin resistance in Mycobacterium tuberculosis directly from respiratory and nonrespiratory clinical samples. Eur J Clin Microbiol Infect Dis. 1998;17(3):189–192. doi:10.1007/BF01691116
97. Hillemann D, Weizenegger M, Kubica T, Richter E, Niemann S. Use of the genotype MTBDR assay for rapid detection of rifampin and isoniazid resistance in Mycobacterium tuberculosis complex isolates. J Clin Microbiol. 2005;43(8):3699–3703. doi:10.1128/JCM.43.8.3699-3703.2005
98. Tortoli E, Marcelli F. Use of the INNO LiPA Rif. TB for detection of Mycobacterium tuberculosis DNA directly in clinical specimens and for simultaneous determination of rifampin susceptibility. Eur J Clin Microbiol Infect Dis. 2007;26(1):51–55. doi:10.1007/s10096-006-0240-x
99. Bai Y, Wang Y, Shao C, Hao Y, GenoType JY, Chatterji D. MTBDR plus assay for rapid detection of multidrug resistance in Mycobacterium tuberculosis: a meta-analysis. PLoS One. 2016;11(3):e0150321. doi:10.1371/journal.pone.0150321
100. Nathavitharana RR, Hillemann D, Schumacher SG, et al. Multicenter noninferiority evaluation of Hain GenoType MTBDR plus version 2 and Nipro NTM+ MDRTB line probe assays for detection of rifampin and isoniazid resistance. J Clin Microbiol. 2016;54(6):1624–1630. doi:10.1128/JCM.00251-16
101. Dantas NGT, Suffys PN, Carvalho WDS, et al. Correlation between the BACTEC MGIT 960 culture system with Genotype MTBDRplus and TB-SPRINT in multidrug resistant Mycobacterium tuberculosis clinical isolates from Brazil. Mem Inst Oswaldo Cruz. 2017;112:769–774. doi:10.1590/0074-02760170062
102. Meaza A, Kebede A, Yaregal Z, et al. Evaluation of genotype MTBDR plus VER 2.0 line probe assay for the detection of MDR-TB in smear positive and negative sputum samples. BMC Infect Dis. 2017;17(1):1–8. doi:10.1186/s12879-017-2389-6
103. Dorman SE, Chihota VN, Lewis JJ, et al. Genotype MTBDRplus for direct detection of Mycobacterium tuberculosis and drug resistance in strains from gold miners in South Africa. J Clin Microbiol. 2012;50(4):1189–1194. doi:10.1128/JCM.05723-11
104. Tomasicchio M, Theron G, Pietersen E, et al. The diagnostic accuracy of the MTBDRplus and MTBDRsl assays for drug-resistant TB detection when performed on sputum and culture isolates. Sci Rep. 2016;6:17850. doi:10.1038/srep17850
105. World Health Organization. The use of molecular line probe assays for the detection of resistance to second-line anti-tuberculosis drugs: policy guidance. World Health Organization; 2016. Report No.: 9241516135.
106. Javed H, Bakuła Z, Pleń M, et al. Evaluation of genotype MTBDRplus and MTBDRsl assays for rapid detection of drug resistance in extensively drug-resistant Mycobacterium tuberculosis isolates in Pakistan. Front Microbiol. 2018;9:2265. doi:10.3389/fmicb.2018.02265
107. Kiet VS, Lan NTN, An DD, et al. Evaluation of the MTBDRsl test for detection of second-line-drug resistance in Mycobacterium tuberculosis. J Clin Microbiol. 2010;48(8):2934–2939. doi:10.1128/JCM.00201-10
108. Theron G, Peter J, Richardson M, Warren R, Dheda K, Steingart KR. GenoType ® MTBDR sl assay for resistance to second-line anti-tuberculosis drugs. Cochrane Database Syst Rev. 2016;2016(9). doi:10.1002/14651858.CD010705.pub3
109. Weyer K, Mirzayev F, Migliori GB, et al. Rapid molecular TB diagnosis: evidence, policy making and global implementation of Xpert MTB/RIF. Eur Respir J. 2013;42(1):252–271. doi:10.1183/09031936.00157212
110. Parsons LM, Somoskövi Á, Gutierrez C, et al. Laboratory diagnosis of tuberculosis in resource-poor countries: challenges and opportunities. Clin Microbiol Rev. 2011;24(2):314–350. doi:10.1128/CMR.00059-10
111. Raviglione M, Marais B, Floyd K, et al. Scaling up interventions to achieve global tuberculosis control: progress and new developments. Lancet. 2012;379(9829):1902–1913. doi:10.1016/S0140-6736(12)60727-2
112. Matteelli A, Centis R, D’Ambrosio L, Migliori G. Multidrug-resistant tuberculosis today. SciELO Public Health. 2012;90:78.
113. World Health Organization. Development of a Target Product Profile (TPP) and a framework for evaluation for a test for predicting progression from tuberculosis infection to active disease 2017 WHO collaborating centre for the evaluation of new diagnostic technologies. Geneva, Switzerland: World Health Organization; 2017.
114. Hanrahan CF, Shah M. Economic challenges associated with tuberculosis diagnostic development. Expert Rev Pharmacoecon Outcomes Res. 2014;14(4):499–510. doi:10.1586/14737167.2014.914438
115. Goletti D, Petruccioli E, Joosten SA, Ottenhoff TH. Tuberculosis biomarkers: from diagnosis to protection. Infect Dis Rep. 2016;8(2):24–32. doi:10.4081/idr.2016.6568
116. Lessells RJ, Cooke GS, Newell M-L, Godfrey-Faussett P. Evaluation of tuberculosis diagnostics: establishing an evidence base around the public health impact. J Infect Dis. 2011;204(suppl_4):S1187–S95. doi:10.1093/infdis/jir412
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.