Back to Journals » Cancer Management and Research » Volume 18

Multidisciplinary Palliative Care and Its Impact on Symptom Burden and Quality of Life in Advanced Cancer Patients in Ethiopia: A Pre–Post Quasi-Experimental Study
Authors Fentie AM ![]() , Seife E, Ozawa S, Fenta TG
, Seife E, Ozawa S, Fenta TG
Received 14 May 2026
Accepted for publication 2 July 2026
Published 17 July 2026 Volume 2026:18 624631
DOI https://doi.org/10.2147/CMAR.S624631
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Zubing Mei
Video abstract of “Palliative Care in Advanced Cancer Patients in Ethiopia” [624631].
Views: 12
Atalay Mulu Fentie,1,2 Edom Seife,3 Sachiko Ozawa,4 Teferi Gedif Fenta2
1Department of Pharmacology and Clinical Pharmacy, School of Pharmacy, Addis Ababa University, Addis Ababa, Ethiopia; 2Department of Social and Administrative Pharmacy, School of Pharmacy, Addis Ababa University, Addis Ababa, Ethiopia; 3Oncology and Radiotherapy Department, School of Medicine, Addis Ababa University, Addis Ababa, Ethiopia; 4Eshelman School of Pharmacy, The University of North Carolina at Chapel Hill, Chapel Hill, NC, USA
Correspondence: Atalay Mulu Fentie, Email [email protected]
Purpose: This study implemented a multidisciplinary team (MDT) palliative care and assessed its impact on symptom burden and health-related quality of life (HRQoL) among patients with advanced-stage cancer at Tikur Anbessa Specialized Hospital, Addis Ababa, Ethiopia.
Methods: This non-randomized pre–post quasi-experimental study (without a concurrent control group) enrolled 192 adult patients with cancer. The intervention was the introduction of MDT palliative care delivered by palliative-care–trained healthcare professionals. Outcomes were assessed before and after MDT implementation using the African Palliative Outcome Scale (APCA POS), EQ-5D-5L (Ethiopian value set) with EQ-VAS, and EORTC QLQ-C15-PAL. Within-patient changes were evaluated in the matched alive cohort (n=167) using paired-sample t-tests, with effect sizes quantified using Cohen’s d. Factors associated with changes in HRQoL were examined using ANCOVA-of-change linear regression.
Results: All APCA POS domains, except social/communication, improved significantly, and the overall patient score decreased by 3.71 points (Cohen’s d = − 0.662, p< 0.001). The EQ-5D-5L utility index score increased by 0. 0.286 (Cohen’s d=0.668, p< 0.001). The EORTC global HRQoL increased by 14.62 points (Cohen’s d = 0.909, p< 0.001), exceeding the conventional 10-point minimal clinically important difference. In the multivariable model, each one-level reduction in patient-rated pain severity was associated with a 4.22-point gain in HRQoL (p< 0.001), and approximately 31.2% of marginal HRQoL improvement was associated with concurrent pain reduction. Patients with a poor performance status (ECOG 2– 4) showed greater HRQoL improvement than those with a better performance status (β = 2.81, p=0.031).
Conclusion: MDT palliative care was associated with clinically meaningful improvements in symptom burden and HRQoL, with the largest gains observed in patients with the greatest symptom burden at baseline. To maximize the population-level impact, ensuring the integration of MDT palliative care into Ethiopia’s national cancer and palliative care strategies is recommended.
Keywords: cancer, ethiopia, low-income countries, palliative care, multidisciplinary team, symptom burden, quality of life
Introduction
Palliative care is a universally recommended component of care for individuals with serious or life-limiting illnesses. The World Health Organization (WHO) defines palliative care as an approach that improves the quality of life of patients and their families through the prevention and relief of suffering. Effective palliative care requires a broad multidisciplinary team (MDT) approach that includes the family and available community resources to address physical, psychological, social, and spiritual needs and can be implemented even when resources are limited.1 Of the estimated 56.8 million people requiring palliative care each year worldwide, 78% live in low- and middle-income countries (LMICs), yet only 14% of those in need globally and less than 3% in LMIC settings actually receive palliative care. This gap represents one of the largest unmet healthcare needs in the world.2–4
The cancer burden in sub-Saharan Africa is rising rapidly, with most patients presenting at advanced stages, making palliative care an especially urgent need.3 Barriers in LMICs are well described and multidimensional, including weak integration of palliative care into primary healthcare, restrictive opioid policies, limited opioid availability, trained workforce shortages, geographic barriers to tertiary care, limited funding, and persistent cultural and knowledge-related barriers.3–6
The WHO and the World Hospice and Palliative Care Alliance explicitly recommend the MDT model of palliative care delivery, which integrates physicians, nurses, social workers, spiritual care providers, and where available pharmacists and physiotherapists to address the multidimensional nature of suffering that cannot be managed by a single discipline.7,8 The MDT framework operationalizes the concept of “total pain” introduced by Cicely Saunders, which recognizes that suffering from serious illness is physical, psychological, social, and spiritual in nature.9 Within an MDT, each discipline contributes expertise towards a common patient-centered goal: pain and symptom relief, psychological and spiritual support, communication and family engagement, and care coordination. Evidence from high-income countries has consistently demonstrated that MDT-based palliative care is associated with improved patient-reported outcomes, reduced symptom burden, lower healthcare utilization, and improved caregiver well-being.10,11 However, in LMIC settings, implementation has been uneven, and published evaluations of MDT-based palliative care outcomes remain limited, particularly with patient-reported outcome measures.2,12,13
Ethiopia illustrates both challenges and opportunities for palliative care development in LMICs.14,15 A randomized controlled trial of home-based early integrated palliative care in Addis Ababa showed significant improvements in patient-reported outcomes and demonstrated that palliative care can be delivered sustainably in this setting.16 However, other Ethiopians studies have focused on describing the problem qualitatively and quantitatively.17 Hence, the evaluation of hospital-based MDT palliative care using validated patient-reported outcome measures remains a priority (Figure 1).
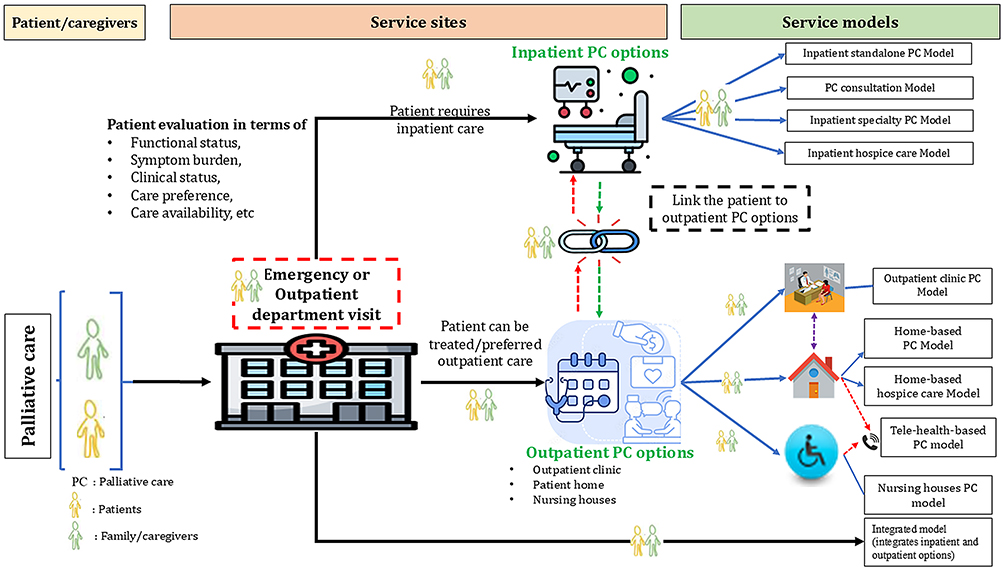 |
Figure 1 Summary of different palliative care (PC) models, showing patient/caregiver entry, service sites (inpatient and outpatient PC options), and the corresponding service-delivery models. Patients enter PC following clinical evaluation (functional status, symptom burden, clinical status, care preference, and care availability) and are directed to inpatient or outpatient or integrated PC options, each linked to its respective service-delivery model. The arrows indicate the direction and type of patient flow between service sites and models: • Solid blue arrows denote referral or branching of a patient to a specific service-delivery model. • Purple dashed bidirectional arrows indicate that outpatient PC may be delivered either at the outpatient clinic or at the patient’s home; that is, the patient may attend the clinic or clinic staff may provide the service at home. • Teal dashed arrows represent tele-health–based PC, in which the patient or family caregiver receives consultation via phone call or other tele-based platforms. • Red dashed arrows (outpatient → inpatient) indicate escalation of care: when a patient is critical and requires admission, the outpatient PC unit links or admits the patient to the inpatient PC ward. • Green dashed arrows (inpatient → outpatient) indicate step-down of care: when a patient is clinically improved or stable, the inpatient PC unit links the patient to the outpatient unit for outpatient follow-up. |
Methods
Study Setting
This study was conducted at TASH, the largest tertiary teaching and referral hospital in Ethiopia, located in Addis Ababa. TASH has approximately 800 operational beds and provides inpatient and outpatient services to more than 500,000 patients annually. It serves as the national referral center for cancer care and hosts the country’s largest oncology and radiotherapy units. Annually, more than 15,000 cancer patients are diagnosed and treated across the adult, pediatric, and Amistegna wings of the hospital, of which approximately 70% are adults, 30% are pediatric patients, and more than two-thirds of patients are diagnosed with advanced-stage disease.18,19 The hospital has eight dedicated inpatient beds for palliative and end-of-life care, and outpatient palliative care clinics are conducted twice weekly. The TASH has integrated palliative care within its oncology department and established both short- and long-term training programs. It has also served as a site for the American Society of Clinical Oncology (ASCO) International Cancer Corps, a capacity-building initiative supporting cancer care in LMICs through which many of these interventions have been supported.
Study Design and Period
A pre-post quasi-experimental study design was used to evaluate the impact of an MDT palliative care intervention guided by an integrated palliative care model (Figure 1). The integrated palliative care model embeds palliative care across the continuum of care through coordinated multidisciplinary services delivered alongside disease-directed treatment. Each participant served as their own control, with outcomes measured before (baseline) and approximately four weeks after the introduction of MDT services (post-intervention). The MDT structure at TASH was formally established in November 2024. To allow the MDT, training program, symptom-based protocol, and referral pathways to mature into routine practice, the study evaluation and patient recruitment began approximately six months later between May 2025 and February 2026, with post-intervention follow-up assessments completed by March 31, 2026. This delay between MDT launch and study recruitment was deliberate, ensuring that the intervention being evaluated reflected an established and stable model of care rather than a newly launched program and that observed outcomes could not be attributed to early implementation enthusiasm or transient start-up effects.
Context Before the Intervention
Palliative care services at TASH were fragmented and delivered without a formal multidisciplinary structure. Outpatient palliative care was provided by a single general practitioner with six months of short-term palliative care training, while inpatient palliative care was delivered by family physicians in the emergency ward, where four beds were designated for palliative care patients. The emergency ward environment was overcrowded with acutely ill emergency patients, limiting opportunities for private, patient-centered, and family centered communication. Baseline assessment revealed inconsistent symptom management, the absence of standardized symptom management protocols, limited cross-disciplinary coordination, and restricted access to specialist palliative care input or structured community-based follow-up.6
Palliative Care Context During Intervention
An integrated, symptom-guided MDT palliative care intervention was implemented according to the WHO multidisciplinary framework for palliative care delivery and comprised four core components: (1) stakeholder engagement and governance, (2) workforce capacity building, (3) symptom-based palliative care protocol-guided treatment, and (4) patient and family support with community-based palliative care linkage.20,21
Stakeholder Engagement and Governance
A stakeholder mapping exercise identified the clinical and administrative units directly and indirectly involved in palliative care. A multidisciplinary working group was established with representation from oncology, family medicine, nursing, public health, emergency medicine, neurology, psychiatry, pharmacy, and a community-based palliative care provider, Hospice, Ethiopia.16,22 Following consultative meetings, a concept note was endorsed by hospital management, leading to institutional support, including the allocation of a dedicated ward with more beds for palliative care, advanced palliative care training for healthcare professionals, and the recruitment of two additional general practitioners. Sustained advocacy with the Ministry of Health, the Ethiopian Food and Drug Authority, and the Ethiopian Pharmaceutical Supply Service (EPSS) improved access to essential palliative care medicines, although regulatory constraints prevented hospital-level preparation of oral morphine solution. Advocacy with EPSS secured the availability of sustained-release morphine 30 mg tablets and then locally manufactured oral morphine solution (20 mg/5 mL of 125 mL bottle).
Workforce Capacity Building
Capacity building was implemented as a core component of the intervention. Foundational multidisciplinary training was provided to physicians, nurses, psychologists, pharmacists, and social workers, complemented by an institutional awareness campaign conducted under the American Cancer Society Hospital Pain-Free Initiative. Training was provided and scaled up through a partnership with the ASCO, which supported seven sequential, context-adapted training sessions delivered through a blended learning approach combining virtual and in-person sessions, classroom instruction, and bedside experiential learning with real case presentations. The training content covered core palliative care principles, symptom assessment and management, pain control, communication skills, psychosocial and spiritual support, and multidisciplinary team coordination. For long-term sustainability, the working group developed symptom-based continuing professional development training material (15 continuing educational units), which was formally accredited by the College of Health Sciences CPD Center and can also be used to expand training coverage.
Symptom-Based Palliative Care Protocol
A context-adapted palliative care protocol was also developed by the working group, informed by the baseline symptom burden assessment (manuscript under review in the ASCO Journal of Clinical Oncology) and based on the availability of medicines and services in the Ethiopian setting. The protocol was endorsed by the senior leadership of the College of Health Sciences and was approved by the Hospital Drug and Therapeutics Committee for institutional adoption. It provides standardized, evidence-based guidance for the assessment and management of common palliative care symptoms such as pain, dyspnea, nausea and vomiting, constipation, fatigue, anxiety, and depression with explicit treatment algorithms, medication recommendations, and referral criteria. Using this protocol, patients received integrated palliative care comprising systematic symptom assessment, individualized care planning, multidisciplinary case discussions, medication optimization, and structured patient and family counselling.
Patient and Family Support and Community Linkage
Targeted support mechanisms address financial hardship, with assistance mobilized from charitable organizations and philanthropic individuals to reduce out-of-pocket costs. In the absence of formal chaplaincy services at TASH, spiritual care is addressed through structured counselling and referral to patients’ respective religious leaders, reflecting the role of faith traditions in Ethiopian palliative care. To ensure continuity of care beyond the hospital, patients who required ongoing supportive and palliative care after discharge were systematically linked to Hospice Ethiopia and Hope Beyond International, both of which provide home-based palliative care.
Team Composition for the Intervention and Follow-Up
The MDT comprised palliative care-trained physicians (oncologists and family physicians), nurses, social workers, and a clinical pharmacist with additional specialist consultations arranged as clinically indicated. The team convened regularly to coordinate the care plans and review patient progress. The intensity of the MDT intervention over the approximately four-week follow-up period varied by care follow-up type (predominantly inpatient vs outpatient linked with home-based palliative care). Following the structured baseline assessment, admitted patients were reviewed by the MDT three times per week; given a mean inpatient length of stay of 7.78 days, this corresponded to approximately three to four MDT rounds during a typical admission. Patients receiving outpatient palliative care were reviewed in the palliative care clinic every two weeks, and patients linked to home-based palliative care received, in most cases, one or two home visits over the follow-up period. Across all follow-up types, every enrolled patient was discussed in at least one formal multidisciplinary case discussion, and medication and care plans were reviewed and adjusted at each contact according to the symptom-based protocol. Outcomes were compared between pre- and post-intervention measurements using patient-reported outcome measures, as described in the Introduction section.
A summary of how each WHO-recommended palliative care domain and indicators were addressed before and during the MDT intervention is provided in the Supplementary File 1 (Table S1).
Source and Study Population
The source population comprised adult patients diagnosed with advanced-stage cancer and receiving care at TASH inpatient and outpatient clinics during the study period. The study population consisted of adult patients who met the following eligibility criteria. Patients were included if they were: (i) aged 18 years or older; (ii) had a confirmed diagnosis of cancer based on histopathological or cytological examination; (iii) able and willing to provide written informed consent; and (iv) had at least one indication for palliative care. Indications for palliative care included patients with (a) advanced disease, defined as stage III–IV or relapsed/refractory solid tumors, or hematologic malignancies classified as advanced, relapsed, or refractory according to the applicable disease-specific staging or prognostic criteria, as confirmed from the medical record; (b) uncontrolled symptoms were defined as a baseline APCA POS pain or any other-symptom item score of ≥3 (on the 0–5 scale); and (c) complex psychosocial needs were defined as documented financial hardship, absence of a primary caregiver, or clinically significant psychological distress identified during the structured baseline assessment. Patients were excluded if they were: (i) unable to communicate meaningfully due to severe cognitive impairment, confusion, or aphasia; (ii) unable or unwilling to provide informed consent; or (iii) already receiving MDT palliative care in another setting at the time of enrolment.
Sample Size and Sampling Procedure
To detect at least a clinically meaningful change in the EORTC QLQ-C15-PAL health related quality of life (HRQoL) score from pre- to post-intervention, a minimum important difference or threshold proposed by Osoba et al (1998) of 5 points on the 0–100 scale was applied for the sample size calculation.23 Assuming a standard deviation (SD) of paired differences of 22 points based on published EORTC reference values in advanced cancer populations, a paired Cohen’s d of 0.23,24 two-sided α = 0.05, and 80% power, a minimum of 152 evaluable participants was required. Allowing for approximately 20% loss to follow-up due to mortality and attrition typical of palliative care populations,25,192 participants were recruited. Eligible cancer patients attending TASH inpatient and outpatient units for palliative care were recruited consecutively until the target sample size was reached.

Where:
n = required number of evaluable participants
Z0⁄2 = 1.96 (critical value for two-sided α = 0.05)
Zβ = 0.84 (critical value for 80% power, 1 − β = 0.80)
δ = 5 (minimum important difference on a 0–100 scale).
σd = 22 (assumed standard deviation of paired differences in EORTC HRQoL) and its equivalent Cohen’s d = 0.23 (5 divided by 22)
Outcome Measures
Three complementary patient-reported outcome measures were used to capture different dimensions of palliative care outcomes.
Symptom Burden and Concerns
The African Palliative Outcome Scale (APCA POS), a 10-item multidimensional tool developed specifically for African palliative care settings and validated across multiple sub-Saharan African countries, was used to measure symptom burden and concerns.26 Each item is scored on a 0–5 Likert scale and addresses five key domains: pain and other symptom burden (items 1–2), psychological distress (item 3, worry), spiritual/existential concerns (items 5–6, life feeling worthwhile and feeling at peace), social and emotional symptoms/communication (items 4 and 7, ability to share feelings and help/advice for family), and family caregiver concerns (items 8–10, information received, confidence in caring, and family worry).
Health Related Quality of Life (HRQoL)
HRQoL was measured using the EQ-5D-5L, a generic preference-based instrument developed by the EuroQol Group.27 The instrument comprised five dimensions: (1) mobility, (2) self-care, (3) usual activities, (4) pain/discomfort, and (5) anxiety/depression, each rated on five severity levels (1 = no problems to 5 = extreme problems). A visual analog scale (EQ-VAS) measured self-rated current health from 0 (worst imaginable) to 100 (best imaginable health). In addition, the EORTC QLQ-C15-PAL, a 15-item palliative care–specific HRQoL instrument derived from the EORTC QLQ-C30, was translated into Amharic and validated following the standard EORTC translation procedure. This included two independent forward translations by professional bilingual translators with oncology and qualitative research experience (AMF), followed by blind back-translation by a bilingual palliative care trained oncology expert (ES) unfamiliar with the original instrument.
The psychometric properties of the Amharic version EORTC QLQ-C15-PAL were evaluated using a baseline sample (N = 192) and included assessments of acceptability (item completion rates and floor/ceiling effects), internal consistency (Cronbach’s alpha), convergent validity (Spearman correlations with EQ-VAS), known-group validity (comparisons by ECOG performance status), and structural validity (exploratory factor analysis using principal axis factoring with Promax rotation). Detailed methods, a priori hypotheses, and full validation results are provided in the Supplementary File 2 (Tables S2–S7).
Pain Management Index (PMI)
The PMI was computed to quantify the adequacy of the analgesic treatment. Pain intensity was categorized into four levels based on a Numeric Rating Scale: 0 (no pain), 1 (mild pain), 2 (moderate pain), and 3 (severe pain). Analgesic potency was similarly categorized on a 0–3 scale (0 = no analgesic, 1 = non-opioid, 2 = weak opioid, and 3 = strong opioid). PMI was computed as analgesic potency minus pain severity; scores ≥0 were classified as adequate analgesia and negative scores as inadequate analgesia.
Patient Satisfaction with Palliative Care
Patient satisfaction was assessed post-intervention using a structured 10 item-questionnaire, FAMCARE-10, covering five domains: information giving, availability of providers, physical/symptom care, coordination and continuity of care, and family involvement.28
Data Collection and Technique
Data were collected using structured questionnaires administered through face-to-face interviews with trained data collectors (two general practitioners, two nurses, and one clinical pharmacist). Data collectors received two-day training on the study protocol, questionnaire administration, and ethical considerations. The data collectors were dedicated study staff who were not members of the MDT delivering the intervention. To further reduce the risk of social desirability bias, patients were explicitly informed at consent that their responses were confidential, were used only for research, and would not affect the care they received, and the interviewers were trained to administer the patient-reported outcome measures in a neutral, non-leading manner. Residual social desirability and Hawthorne effects cannot be fully excluded and are acknowledged in the Limitations. Baseline data were collected at study enrolment, prior to initiation of MDT services, and included sociodemographic, clinical, and treatment-related characteristics; symptom burden using APCA POS; and HRQoL using EQ-5D-5L/EQ-VAS and EORTC QLQ-C15-PAL. Follow-up data were collected approximately four weeks after MDT initiation based on their nearest appointment period using the same instruments and the satisfaction questionnaire. Clinical information, such as cancer type and treatment received, was also extracted from their respective medical records after obtaining their informed consent. The supportive-care elements summarized as “Yes/No”; eg, psychological support, spiritual care, financial/social support, physiotherapy, and wound care) were not based on patient self-report. A “Yes” was recorded only when the relevant intervention was documented in the patient’s medical record or MDT care plan as having been delivered by the responsible professional (for example, a counselling session recorded by a social worker, a referral to a religious/spiritual-care provider, or a documented physiotherapy or wound-care episode). Pharmacological items were verified against the medication record. Thus, all indicators reflect documented service delivery rather than patient perception. The mortality status and reasons for loss to follow-up were also documented.
Data Quality Assurance
Several measures were implemented to ensure the data quality. First, the Amharic translation of all patient-reported outcome measures underwent a rigorous forward–backward translation and cultural adaptation process, with cognitive debriefing to confirm comprehensibility. Second, the data collectors received standardized training on instrument administration, informed consent, and ethical conduct. Third, a pre-test was conducted on 10 patients prior to the main study to identify and address challenges with questionnaire administration, timing, and comprehension. Findings from the pre-test were used to refine the data collection procedures. Fourth, the questionnaires were checked for completeness and consistency immediately after administration; any missing or inconsistent data were resolved through clarification with the respondent when possible. Fifth, double data entry with range and consistency checks were performed to minimize data entry errors. Finally, the PI (AMF) supervised data collection throughout the study period, with regular reviews in person meetings, phone call follow-ups, and discussions to address any emerging issues.
Data Analysis
Complete and cleaned data were entered and analyzed using IBM SPSS Statistics version 27 (IBM Corp., Armonk, NY, USA). Baseline sociodemographic and clinical characteristics were summarized using frequencies and percentages for categorical variables and means with standard deviations or medians with interquartile ranges for continuous variables as appropriate. Changes in WHO-aligned palliative care management practices before and after MDT intervention were evaluated using McNemar’s test for paired categorical data.
For symptom burden and concerns, items 4–9 of the APCA POS were reverse-scored prior to analysis so that, for all items, lower scores indicated better status. Composite scores were calculated as sums within each domain, with the patient total score (items 1–7, range 0–35) and total POS score (items 1–10, range 0–50). EQ-5D index utility values ranged from <0 (worse than death) to 1 (full health). These values were derived by applying the Ethiopian health state value developed by Welie et al,2020,29 which provides country-relevant preference weights anchored at 1 (full health) and 0 (dead), with negative values possible for states considered worse than death. Utility values below zero were retained on their original scale for analysis, in line with the EuroQol Group guidance.24 The EORTC QLQ-C15-PAL scores were linearly transformed to a 0–100 scale according to the EORTC scoring manual, with higher scores on functional scales and global quality of life indicating better status and higher scores on symptom scales indicating greater symptom burden.30 The EQ-5D-5L utility index was analyzed using the intention-to-treat approach (N = 192), with deceased participants (n = 21) assigned a post-intervention utility of 0 per QALY convention and participants who left against medical advice (LAMA) (n = 4) assigned baseline-carried-forward values.31 All other measures were analyzed using complete-case data (n=167, excluding those who died and were left against medical advice). For outcomes other than the EQ-5D-5L utility index (APCA POS, EQ-VAS, EORTC QLQ-C15-PAL, and the regression analyses), item-level missing data within the matched alive cohort were zero, and therefore, no imputation was required. Patients who died (n = 21) or left against medical advice (LAMA) (n = 4) before the follow-up assessment did not contribute post-intervention values and were excluded from these complete-case analyses. Their systematically worse baseline characteristics are presented separately (Figure 2) and are discussed as a potential source of attrition (survivorship) bias. The patient satisfaction domain scores were transformed to a scale of 0–100. The overall satisfaction score is calculated as the mean domain score. Those who responded to items satisfied or very satisfied were classified as “satisfied” whereas those who responded as “not satisfied” where categorized as “dissatisfied.”
 |
Figure 2 Pre–post multidisciplinary team (MDT) palliative care outcomes for symptom burden (APCA POS patient total), health-related quality of life (EQ-5D-5L utility, Ethiopian value set), and overall quality of life (EORTC QLQ-C15-PAL item 15). Error bars on group means show 95% confidence intervals of the mean (not standard deviations). Annotation boxes summarize the paired t-test results between Pre-MDT and Post-MDT in the matched alive cohort (n=167). The Died/LAMA bar shows baseline (pre-intervention) values only and is not part of the paired test. Abbreviations: APCA POS, African Palliative Care Association Palliative Outcome Scale; EORTC, European Organization for Research and Treatment of Cancer; LAMA, left against medical advice; MDT, multidisciplinary team; QoL, quality of life. |
Changes in all multidimensional patient-reported outcomes (APCA POS, EQ-5D-5L utility, EQ-VAS, and EORTC QLQ-C15-PAL) were assessed using matched paired-sample t-tests with 95% CI for the mean difference (Δ). The “Δ” was calculated as post (MDT intervention) minus pre-intervention. Effect sizes were calculated as Cohen’s d for matched paired samples, defined as the “Δ” divided by the standard deviation (SD) of paired differences. For the APCA POS scales, EQ-5D-5L dimension scores, and EORTC QLQ-C15-PAL symptom scales, lower values indicate better status, so negative “Δ” and Cohen’s d indicate improvement. For the EQ-5D-5L utility index, EQ-VAS, EORTC functional scales and global HRQoL, higher values indicate better status, so positive “Δ” and Cohen’s d indicate improvement. Effect sizes (Cohen’s d) were interpreted using conventional benchmarks: values <|0.2| trivial, |0.2| to <|0.5| small, |0.5| to <|0.8| moderate, and ≥|0.8| large, and signs (− or +) indicated either worsening or improvement.
Factors associated with changes in HRQoL (ΔHRQoL = post-MDT minus pre-MDT EORTC global HRQoL score) were examined using multiple linear regression in an ANCOVA-of-change framework, estimated using ordinary least squares (OLS), on the matched alive cohort (n = 167 with complete covariate data). The outcome (ΔHRQoL) was modelled as a function of within-patient change in pain severity (Δpain= post-MDT pain-pre-MDT pain), baseline (pre-MDT) HRQoL score (to adjust for regression-to-the-mean per Vickers and Altman recommendation,32 and baseline characteristics (age, sex, education, employment, ECOG performance status, and cancer type). Candidate predictors were screened using univariate regression with a permissive entry threshold of p<0.25 to avoid premature exclusion of clinically important variables.33 The final model was checked for fit and influential observations.
To explore how much of the HRQoL improvement was related to concurrent pain reduction versus other MDT-related changes (psychosocial support, symptom management for non-pain symptoms, care coordination, etc)., an exploratory decomposition of the cross-sectional association was computed as the product of the mean within-patient pain change (Mean Δpain = (1/167) × Σ (post pain_i − pre pain_i) and main effect (the Δpain beta-coefficient from the primary model). Because pain and HRQoL were assessed concurrently at the same follow-up, no temporal ordering between the proposed mediator (pain reduction) and the outcome (HRQoL) could be established; this quantity is therefore interpreted as the proportion of the HRQoL change that is statistically associated with concurrent pain change, and not as a formal causal mediation effect.
The final model was checked for model fit, multicollinearity, and normality (Shapiro–Wilk and Q-Q plots). A concordant sensitivity analysis using a long-form linear mixed-effects model (359 complete observations: 192 observations in the pre-intervention period and 167 observations excluding died and LAMA patients in post-intervention) with random patient intercept was performed to confirm robustness to the modelling framework. Statistical significance was set at p<0.05.
Clinically meaningful EQ-5D-5L utility changes were interpreted against a published minimum important difference of approximately 0.03 on the 0–1 utility scale,34 and for the APCA POS patient total score against the minimum important difference of 3 points established by Harding et el, 2010.26
Ethical Considerations
Ethical approval was obtained from the Institutional Review Board (IRB) of the College of Health Sciences, Addis Ababa University (protocol number 054/23/SoP). The study was conducted in accordance with the Declaration of Helsinki and the local Ethiopian research ethics guidelines. Written informed consent was obtained from each participant prior to enrolment. For participants who were unable to read or write, verbal informed consent was obtained in the presence of a witness and thumb-printed consent was recorded. The confidentiality of participant information was strictly maintained, and questionnaires were coded with unique study identifiers. Personal identifying information was stored separately from clinical and outcome data, and access to the study database was restricted to the PI (AMF). Participants were informed that they could withdraw from the study at any time without impacting their clinical care. No financial incentives were provided for participation.
Results
Patient Characteristics
The mean (±SD) age was 46.3 ± 9.6 years. The majority were females (121, 63.0%) and most patients were married (127, 66.1%). Slightly over half resided outside Addis Ababa (101, 52.6%); among them, 37 (36.6%) reported no close family in the city. Regarding education, the majority had no formal education 40 (20.8%) or diploma or higher (41, 21.4%). Gynecological cancers were the most frequent (44, 22.9%), followed by gastrointestinal (42, 21.9%) and breast cancers (32, 16.7%). Comorbidities were reported in 50 patients (26.0%), with the majority having hypertension (23, 46.0%), HIV/AIDS (15, 30.0%), and deep vein thrombosis (14, 28.0%). Nearly half (n=98) of the patients had recurrent disease at recruitment, and (144, 75.0%) had an ECOG score of 2–4. Most patients’ sources of financing for care were community-based health insurance (140, 72.9%). In total, 21 (10.9%) patients died at the end of the month follow-up period and four left against medical advice (Table 1).
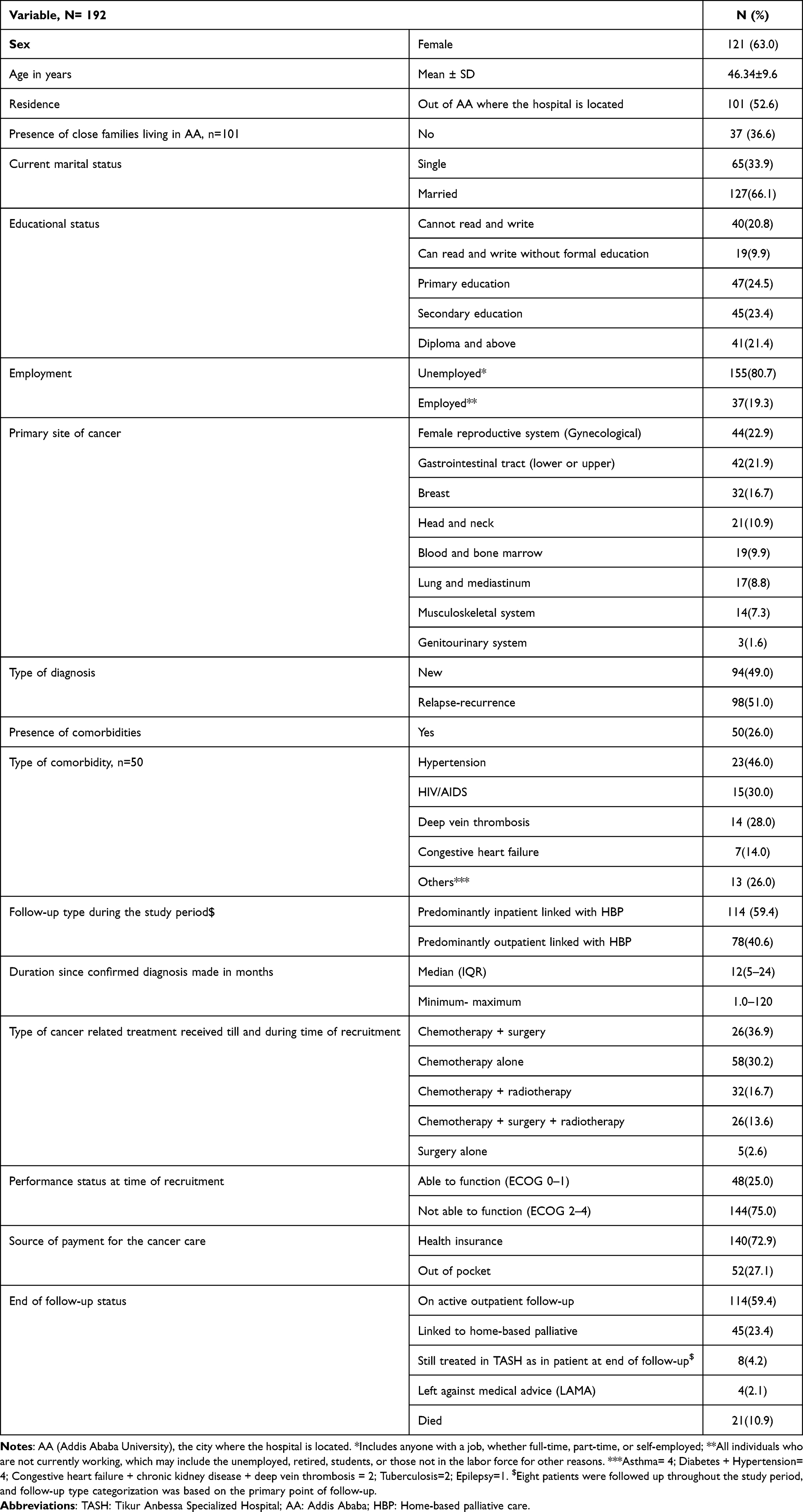 |
Table 1 Demographics, Clinical and Cancer-Related Treatment Characteristics |
Symptom-Based Management Before and After MDT Intervention
Implementation of MDT was associated with significant improvements in pain management and other palliative care delivery WHO domains. The proportion of patients reporting severe pain decreased markedly from 49.7% at baseline to 9.6% post-intervention, whereas those reporting mild or no pain increased substantially (p<0.001). Significant changes were observed in pain management practices (p<0.001), including a reduction in the number of patients receiving no analgesics and increased use of strong opioids (19.8%–44.3%) and adjuvant medications (1.8%–11.4%). The Provision of other palliative care interventions improved substantially across multiple domains, particularly psychological support (1.6%–43.7%) and spiritual care (4.7%–78.4%) (p<0.001). The PMI showed significant improvement, with adequate pain management increasing from 38.3% to 96.5% (p<0.001). Similarly, patient-reported pain relief improved significantly (p<0.001), with complete pain relief increasing from 5.4% to 58.7% (Table 2).
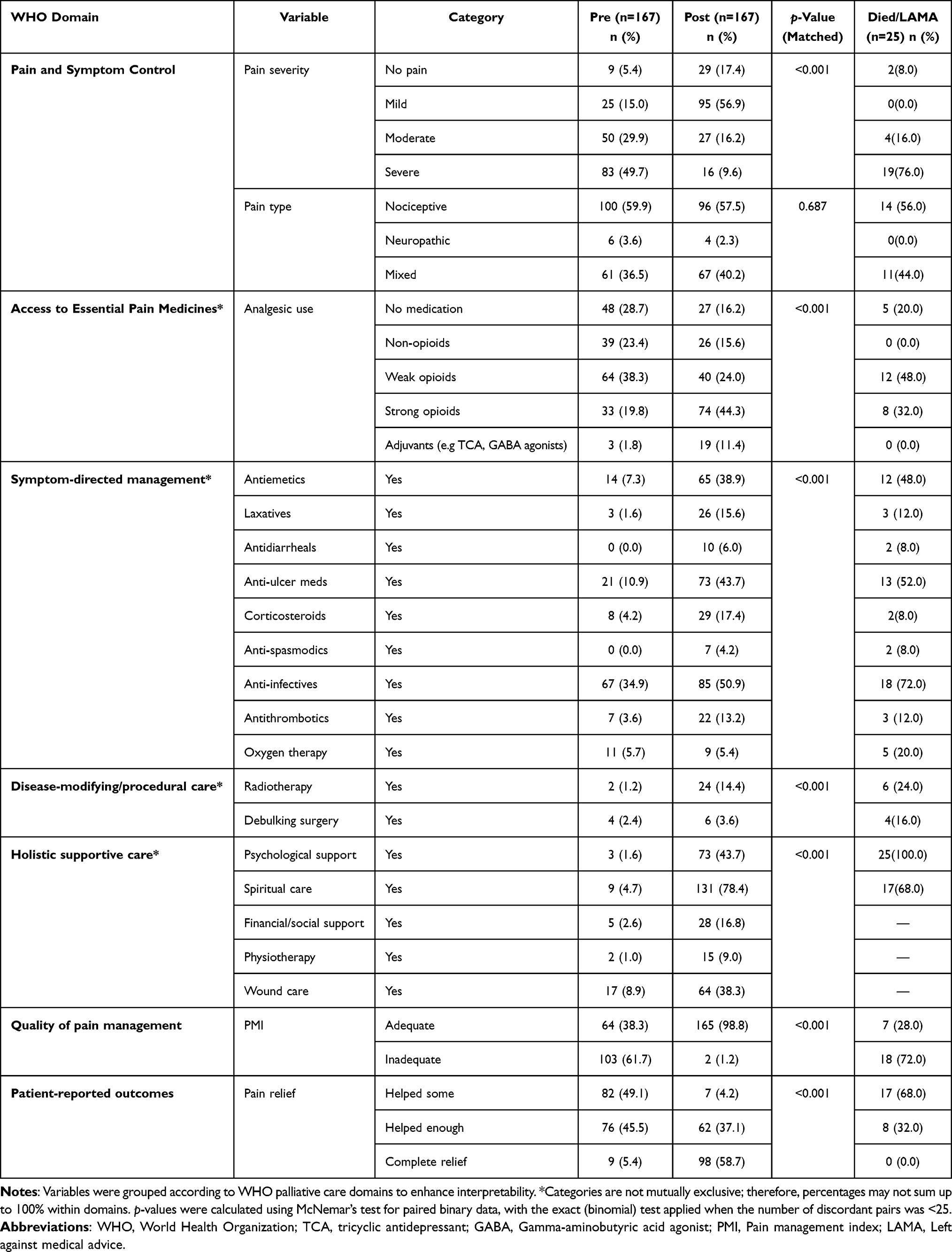 |
Table 2 Pain Characteristics and Palliative Care Interventions Before and After MDT Implementation Aligned with WHO Palliative Care Indicators |
Changes in Symptom Burden and Concerns Following MDT Intervention
All APCA POS domains showed statistically significant improvements from pre- to post-intervention, except for social/communication concerns. The largest effect was observed for physical symptom burden, which decreased by a mean difference (Δ) of 2.41 points on the 0–10 scale (p<0.001), corresponding to a large effect size (Cohen’s d=−0.974). Psychological distress decreased by 0.41 points on a 0–5 scale (p<0.001; d=−0.267, small effect), while spiritual/existential concerns decreased by 0.60 points on a 0–10 scale (p=0.003; d=−0.233, small effect). Social/communication concerns showed no significant change (Δ:−0.33, p=0.149; d=−0.112), suggesting that the intervention did not measurably affect this dimension of patient experience. Overall, the patient total score (items 1–7) decreased by 3.71 points (p<0.001; d=−0.662, medium effect), and overall score combining patient and family carer items (items 1–10) decreased by 4.54 points (p<0.001; d =−0.653, medium effect). The Died/LAMA cohort (n=25) had systematically worse pre-intervention scores across all domains, particularly the physical symptom burden (7.40 vs 5.28; ≈40% higher than the matched alive cohort) and total POS score (26.76 vs 23.56) (Table 3 and Figure 2).
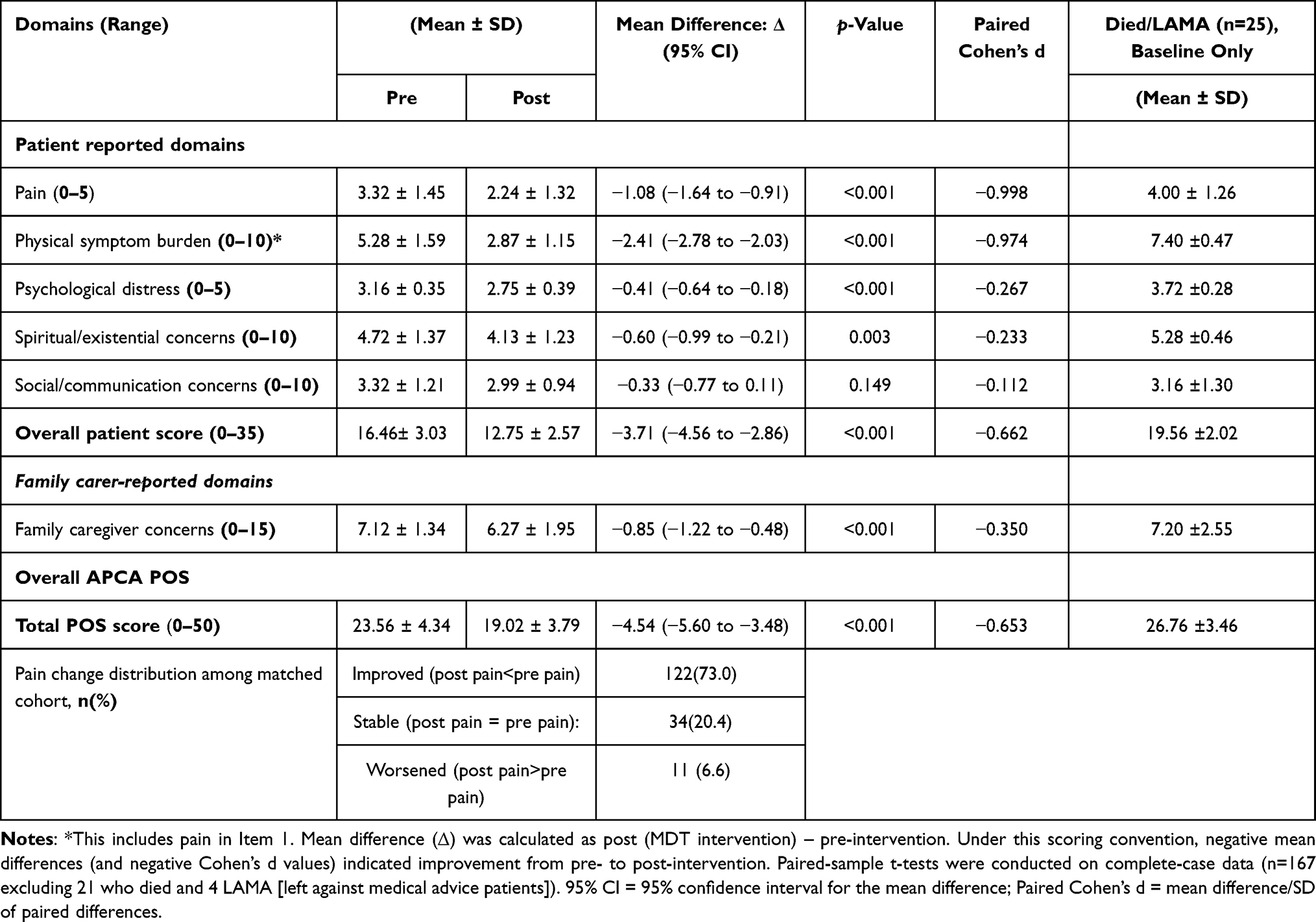 |
Table 3 Comparison of Symptom Burden and Concerns Before and After MDT Intervention |
Changes in Health-Related Quality of Life Following MDT Intervention
All five EQ-5D-5L dimensions showed statistically significant improvements from pre- to post-intervention. Anxiety/depression showed the largest reduction (Δ:−0.91 levels, p< 0.001; Cohen’s d=−0.663, medium-large effect), followed by pain/discomfort (Δ:−0.75, p<0.001; d=−0.606), and mobility (Δ:−0.63, p< 0.001; d=−0.584). The mean EQ-5D-5L utility index “Δ” increased significantly from 0.372 pre-intervention to 0.658 post-intervention (Δ:0.286, p<0.001; d=0.668, medium-large effect). Self-rated health on the EQ-VAS improved by a mean of 9.51 points (p<0.001; d=0.862, large effect). Similarly, the EORTC QLQ-C15-PAL functional and symptom scales showed significant improvement (p<0.001). The single-item EORTC global quality of life measure also increased by 14.62 points (p<0.001; d=0.909, large effect) and exceeded the conventional 10-point minimal clinically important difference for EORTC global HRQoL. The Died/LAMA cohort (n=25) had systematically worse pre-intervention scores than the matched alive cohort across all measured domains (Figure 2 and Table 4).
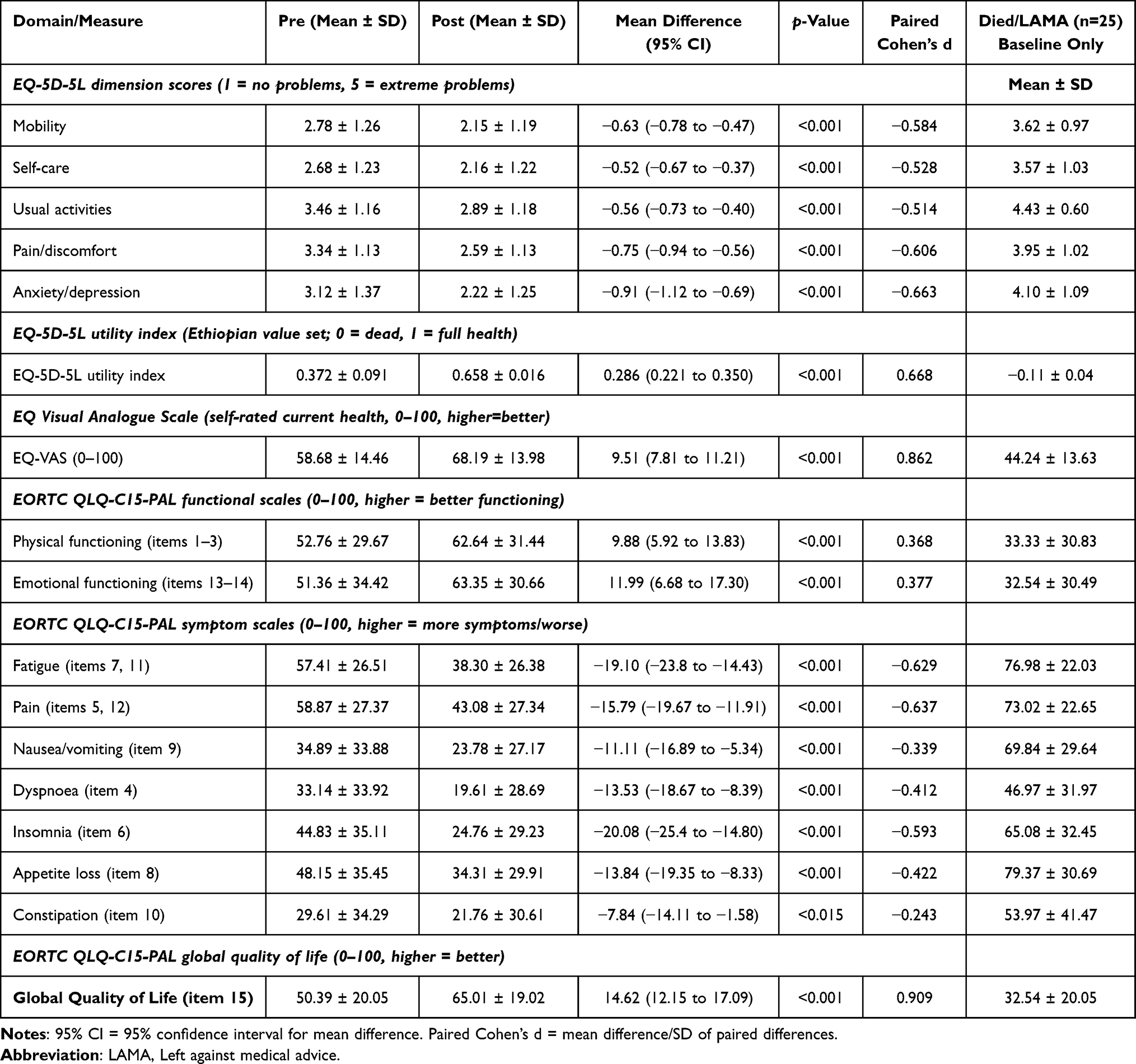 |
Table 4 Pre- and Post-Intervention Comparison of Health-Related Quality of Life Patients |
Factors Affecting Health Related Quality of Life
Of the candidate predictors, only four variables retained statistical significance in the multivariable linear regression: Δpain, baseline HRQoL, ECOG performance status, and treatment for lower or upper gastrointestinal cancer. Overall, the model explained 48.6% of the patient-to-patient variation in HRQoL (R2 = 0.486).
ΔHRQoL = 28.31 − 4.22 Δpain − 0.86 baseline_HRQoL + 2.81 ECOG2-4 + 4.86 GI_ca + (other non-significant predictors in the model, see (Table 5).
 |
Table 5 Factors Affecting Health Related Quality of Life of Patients with Cancer Treated with Integrated Palliative Care Model (n=167) |
In the model, each one-point pain severity reduction on the scale for the patient was associated with a +4.22-point HRQoL gain (β: −4.22; 95% CI: −5.47, −0.97, p=0.005). In an exploratory cross-sectional decomposition, approximately 31.2% of the marginal +14.62-point HRQoL improvement (Table 4) was statistically associated with concurrent pain reduction, while the remaining 68.8% (~+10.06 points) HRQoL benefits was associated with non-pain factors such as psychological support, family communication, non-pain symptom management, and continuity of care provided by the MDT. Patients with a lower baseline HRQoL had larger gains (β:− 0.86, 95% CI: −1.09, −0.24, p<0.001). Among other clinical characteristics, patients diagnosed and treated for lower and upper gastrointestinal cancer (β = +4.84, p=0.003) and baseline performance status (ECOG 2–4) (β = 2.81, p=0.031) were independently associated with greater HRQoL improvement (Table 5).
Satisfaction and Associated Factors
Post-intervention, the mean overall satisfaction score was 64.1 (SD 18.6) on the 0–100 transformed scale, with a median of 65.0 (IQR: 50.0–75.0). Using the pre-specified cut-off point, 135 of 168 respondents (80.4%) were classified as satisfied with MDT palliative care services. Patients who received adequate analgesic treatment (PMI ≥ 0) reported a substantially higher overall satisfaction score than those with inadequate analgesic use (64.7 ±18.5 vs 44.0±15.6; p=0.014). Overall satisfaction did not differ significantly between outpatients (66.0±16.3) and inpatients (62.6±20.2); p =0.237, although the proportion of patients classified as satisfied was higher among outpatients (87.5% vs 75.0%). At the domain level, outpatients reported significantly higher satisfaction with family involvement in care decisions (73.6 vs 64.1, p=0.049) (Table 6).
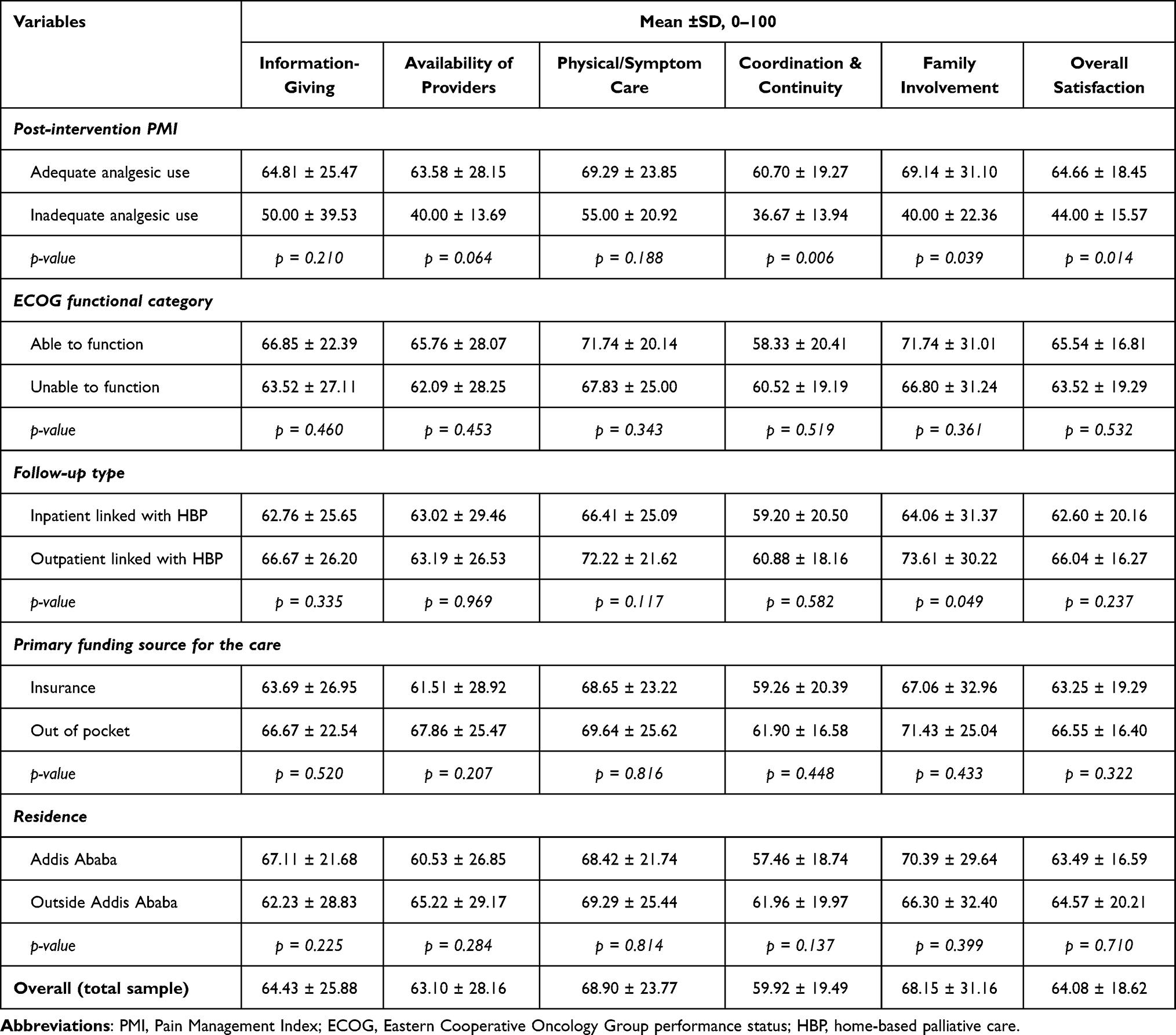 |
Table 6 Satisfaction with Palliative Care and Associated Factors Towards MDT Palliative Care in TASH |
Discussion
The WHO recognizes palliative care as an essential component of comprehensive cancer care and universal health coverage as well as a basic human right.1,35 Consequently, the WHO and World Health Assembly Resolution WHA67.19 advocate integrated MDT palliative care models to improve symptom management, communication, and continuity of care.16,36 Despite these recommendations, implementation remains uneven globally and is particularly limited across sub-Saharan Africa, including Ethiopia, where access to structured hospital-based palliative care services remains scarce.14 In this context, our study provides important evidence of the effectiveness of an MDT palliative care model in a tertiary cancer care setting.
Our MDT palliative care intervention produced a clinically meaningful reduction in symptom burden and patient concerns, with the total APCA POS score decreasing by 4.54 points, exceeding the established minimal clinically important difference (MCID) of three points for the instrument.26 This finding is consistent with evidence from sub-Saharan Africa showing that structured palliative care services can achieve meaningful symptom relief even in resource-constrained settings.37 According to an integrated outpatient-home-based palliative care study in Ethiopia, Reid et al similarly reported significant improvements in pain control and symptom management following the intervention.16 The observed reduction likely reflects the effectiveness of core MDT components, including comprehensive symptom assessment, severity-matched multimodal analgesia, and coordinated care, consistent with Cicely Saunders’ total pain framework.9
The MDT intervention produced significant improvements across all HRQoL measures, including the EORTC QLQ-C15-PAL Global HRQoL (Cohen’s d = 0.909), EQ-VAS (Cohen’s d = 0.862), and EQ-5D-5L utility index using the Ethiopian value set (Cohen’s d = 0.668). Consistent improvement across these complementary instruments provides strong evidence of clinically meaningful benefit26,29,30 and aligns with multiple clinical trials in high income and LMIC settings.10,16,38 The baseline Global HRQoL (50.39) was substantially lower than the 65–75 typically reported in high-income settings,10,38 likely reflecting late-stage presentation, limited prior access to palliative care, poor opioid availability, and inadequate pain assessment and management. By improving access to coordinated symptom management and analgesia, the MDT intervention addressed these gaps, creating greater scope for improvement. These findings suggest that MDT palliative care models developed in high-income settings are not only transferable to LMICs but may yield even greater absolute benefits in resource-constrained contexts.8,11,36
The matched-cohort pre–post improvement of +14.62 points (Table 4) in the EORTC Global HRQoL exceeded the conventional 10-point minimum clinically important difference and was greater than improvements reported in major MDT palliative care trials, including ENABLE II (+4.6 points over 13 months)39 and the NCLC trial (+6.5 points at 12 weeks).10 The larger effect observed in our study likely reflects the high baseline symptom burden of the cohort, with most patients having poor functional status (ECOG 2–4) and severe pain, together with the within-patient comparison design. These findings support scaling MDT palliative care in resource-constrained settings, where palliative care infrastructure remains limited.
In our study, pain reduction was an independent predictor of improved HRQoL (β= −4.22; p=0.005), and concurrent pain reduction was statistically associated with approximately 31.2% of the observed HRQoL improvement, while the remaining 68.8% was associated with non-pain factors, including psychological support, family communication, spiritual care, and management of other distressing symptoms such as fatigue, nausea, dyspnea, insomnia, and appetite loss, all of which improved significantly in the MDT intervention.10,36,39 Nonetheless, the finding highlights that MDT palliative care extends beyond pain management alone and suggesting that scale-up efforts should invest not only in analgesic access but also in counselling, family support, and broader symptom management.4,6
After adjusting for pain change and baseline HRQoL, patients with poorer performance status (ECOG 2–4) experienced greater HRQoL improvement than those with better functional status (β = 2.81, p = 0.031). The negative association with baseline HRQoL (β = −0.86, p<0.001) further indicated that patients with lower initial HRQoL had greater scope for improvement. These findings suggest that MDT palliative care provides the greatest benefit to patients with the highest symptom burden and poorest functioning, consistent with evidence from supportive care and rehabilitation interventions, and support the prioritizing severe-pain and low-functioning patients for early MDT case review in resource-constrained settings such as Ethiopia.40
Overall, these findings support the scalability of WHO-recommended MDT palliative care as a feasible and high-value model for oncology care in LMICs. The greatest improvements were observed among patients with the highest baseline symptom burden and poorest functional status, supporting the use of simple, locally feasible triage criteria, such as an APCA POS pain/symptom score ≥3 or an ECOG performance status of 2–4, to prioritize patients for early MDT review where specialist resources are limited.
Consistent with Saunders’ total pain concept,9 the observation that most of the HRQoL improvement was associated with factors beyond pain underscores the value of MDT care that integrates effective symptom management with psychological, social, spiritual, and family support.
Several implementation lessons from this study may be relevant to other LMIC settings seeking to establish MDT structures and deliver the four core components. These include securing institutional and ministerial leadership support before launch; providing accredited blended (virtual and bedside) training to develop a skilled workforce; embedding context-adapted symptom-management protocols aligned with local medicine availability and approved by the institutional drug and therapeutics committee; and engaging medicines regulators and supply agencies early to overcome barriers to opioid access and formulation availability. Linkage with community- and home-based palliative care services, together with social and financial support mechanisms, can further sustain continuity of care beyond the hospital setting.12,41
At the policy level, the magnitude and consistency of benefit observed across three validated outcome measures support integrating MDT palliative care into Ethiopia’s national cancer control plan, palliative care strategic plan, and universal health coverage benefit package, including sustainable financing for essential palliative medicines and workforce development. For research, adequately powered controlled or stepped-wedge studies with longer follow-up are needed to confirm the durability of benefit, establish temporal relationships among key outcomes (including the pain-HRQoL pathway), evaluate generalizability across multiple sites, and determine cost-effectiveness to inform resource allocation decisions.16,42 This study has the following strengths: First, to our knowledge, this is the first prospective evaluation of an integrated MDT palliative care intervention spanning both inpatient and outpatient services in Ethiopia, conducted at the National Referral Oncology Center. Second, the use of three validated instruments, APCA POS, EORTC QLQ-C15-PAL, and EQ-5D-5L, provided convergent evidence across palliative care–specific, multidimensional, and preference-based HRQoL domains. Third, the EQ-5D-5L utilities were derived using the Ethiopian value set,29 ensuring locally relevant preference weighting. Fourth, the matched-cohort change-on-change OLS approach, with baseline HRQoL adjustment and multiple prespecified pain specifications, strengthened the robustness of the estimates. Finally, this study also validated the Amharic EORTC QLQ-C15-PAL, demonstrating good-to-excellent psychometric performance (KMO = 0.84), strong internal consistency, convergent validity with EQ-VAS, and a factor structure consistent with established physical, emotional, and symptom domains. This study also had several limitations that should be considered when interpreting the findings. First, the single-arm pre–post quasi-experimental design lacked a concurrent control group and therefore cannot fully exclude regression-to-the-mean, secular trends or other background changes in care, as alternative explanations for the observed improvements, although the consistent improvements across three independent outcome measures and the seven-month interval between MDT establishment and recruitment reduce this concern. Second, because the outcomes were patient-reported and assessed before and after a known intervention, repeated assessments and awareness of observations may have introduced Hawthorne or social desirability effects, to mitigate this, data collectors were independent of the MDT delivering care and were not involved in the clinical management of participants, although such bias cannot be entirely excluded. Third, the follow-up was limited to approximately four weeks and therefore captured only short-term outcomes, leaving the durability of benefit uncertain. Fourth, attrition due to death and loss to follow-up was modest but likely informative, as sicker patients were less likely to complete follow-up; however, intention-to-treat analyses produced consistent findings, suggesting conservative survivorship (attrition) bias against the intervention effect. Fifth, the study was conducted at a single tertiary referral hospital, which may limit the generalizability of the findings to primary or secondary level settings, although TASH serves a nationally diverse oncology population. Sixth, residual confounding from unmeasured factors, such as social support, family involvement, and psychological resilience, cannot be excluded. Finally, the decomposition attributing part of the HRQoL improvement to pain reduction should be interpreted with caution. Pain and HRQoL were measured concurrently at the same four-week assessment, so no temporal sequence between the proposed mediator (pain reduction) and the outcome (HRQoL improvement) could be established. The decomposition therefore reflects a cross-sectional statistical association rather than formal causal mediation, and the proportions reported (approximately 31% pain-related and 69% non-pain-related) should be regarded as exploratory and hypothesis-generating; a design with the mediator and outcome measured at separate time points would be required to test causal mediation.
Conclusions
The implementation of an MDT palliative care approach at a tertiary hospital in Ethiopia resulted in statistically and clinically significant improvements in symptom burden, patient concerns, HRQoL, and satisfaction among cancer patients. Improvements were consistently demonstrated across three validated outcome measures: the APCA POS, the newly validated Amharic EORTC QLQ-C15-PAL, and the EQ-5D-5L, using the Ethiopian value set. The greatest benefits were observed in patients with a higher baseline symptom burden, particularly those with severe pain and poor functional status.
Data Sharing Statement
The de-identified data that support the findings of this study are available from the corresponding author upon reasonable request, subject to approval by the College of Health Sciences IRB, and in compliance with applicable Ethiopian data protection regulations.
Acknowledgments
The authors thank the patients and families who participated in this study and the clinical staff of the Oncology Unit and Family Medicine at TASH for their dedication to patient care, particularly the core members of the MDT palliative care team and data collectors. We gratefully acknowledge the Mayo Clinic for covering the article processing charge. As an ASCO International Cancer Corps (ICC) partner site, TASH benefited from capacity-building activities that informed this intervention, including in-person training of local clinical staff and visiting expert faculty; we thank the ASCO ICC leadership, faculty mentors, and program staff for their sustained partnership and technical support. We also thank Hospice Ethiopia and Hope Beyond for providing home-based palliative care services and technical support, and the Night patient support group for offering vital psychosocial support to patients in need. The symptom-based palliative care protocol was developed independently by the multidisciplinary working group based on WHO essential medicines for palliative care, Ethiopian national guidelines, and local medicine availability. No Pfizer-manufactured products were preferentially recommended or used, and all analgesic and adjuvant medications were selected according to generic, guideline-based criteria; thus, the drug-selection process was fully independent of the funder.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study data collection, symptom-based protocol, training material development, and related costs were supported by Pfizer Global Medical Grants (#76384195), which focused on strengthening broader palliative care services at TASH. Although this work was supported by Pfizer Global Medical Grants, the funder had no role in study design, implementation, data analysis, manuscript preparation, or the selection of medicines.
Disclosure
The authors declare no competing interests in this work.
References
1. World Health Organization. Palliative Care. Geneva: WHO; 2020. Available from: https://www.who.int/news-room/fact-sheets/detail/palliative-care.
2. Abu-Odah H, Molassiotis A, Liu J. Challenges on the provision of palliative care for patients with cancer in low- And middle-income countries: a systematic review of reviews. BMC Palliat Care. 2020;19(1):1–20. doi:10.1186/s12904-020-00558-5
3. Knaul FM, Farmer PE, Krakauer EL, et al. The Lancet Commissions Alleviating the access abyss in palliative care and pain relief an imperative of universal health coverage. Lancet. 2018;391(10128):1391–1454. doi:10.1016/S0140-6736(17)32513-8
4. Poudel A, Kc B, Shrestha S, Nissen L. Access to palliative care: discrepancy among low-income and high-income countries. J Glob Health. 2019;9(2):020309. doi:10.7189/jogh.09.020309
5. Negasa EH, Human SP, Roro AG. Challenges in Palliative Care Provision in Ethiopia: an Exploratory Qualitative Study. J Pain Res. 2023;16:3405–3415. doi:10.2147/JPR.S415866
6. Fentie AM, Seife E, Ozawa S, Fenta TG. Experience and satisfaction towards palliative care in an Ethiopian tertiary care setting: a mixed methods study of patients with cancer and caregivers. PLOS Glob Public Heal. 2026;6(4):e0005754. doi:10.1371/journal.pgph.0005754
7. World Health Organization. Palliative Care Palliative Care: NCC Clin Pract Guidel Oncol. 2020; Version 1 (Version 1.2020 — February 7, 2020). 2020:68–69
8. World Health Organization. Integrating Palliative Care and Symptom Relief Into Primary Health Care: A WHO Guide for Planners, Implementers and Managers. Licence: CC BY-NC-SA 3.0 IGO. Geneva: World Health Organization; 2018.
9. Clark D. `Total pain’, disciplinary power and the body in the work of Cicely Saunders, 1958–1967. Soc Sci Med. 1999;49(6):727–736. doi:10.1016/S0277-9536(99)00098-2
10. Temel JS, Greer JA, Muzikansky A, et al. Early Palliative Care for Patients with Metastatic Non–Small-Cell Lung Cancer. N Engl J Med. 2010;363(8):733–742. doi:10.1056/NEJMoa1000678
11. Smith TJ, Temin S, Alesi ER, et al. American Society of Clinical Oncology Provisional Clinical Opinion: the Integration of Palliative Care Into Standard Oncology Care. J Clin Oncol. 2012;30(8):880–887. doi:10.1200/JCO.2011.38.5161
12. Peeler A, Afolabi O, Adcock M, et al. Primary palliative care in low- and middle-income countries: a systematic review and thematic synthesis of the evidence for models and outcomes. Palliat Med. 2024;38(8):776–789. doi:10.1177/02692163241248324
13. Maresova P, Hruška J, Randlova K, Rezny L, Carrillo-de-la-Peña MT, Kuca K. Systematic Review of the Cost-Effectiveness of Home-Based Palliative Care Interventions in Patients with Cancer: a Critical Analysis. Cancer Manag Res. 2024;16:1155–1174. doi:10.2147/CMAR.S472649
14. Heller LD. Palliative Care in Sub-Saharan Africa: a Narrative Review. J Palliat Care. 2024;27(8):1083–1089.
15. Sadiq FU, Yeh YL, Liao HE, Pranata MAE, Patnaik S, Shih YH. The benefits, barriers, and specific needs of palliative care for adults with cancer in sub-Saharan Africa: a systematic review. Glob Health Action. 2025;18(1). doi:10.1080/16549716.2025.2485742
16. Reid E, Abathun E, Diribi J, et al. Early integrated palliative care in patients newly diagnosed with cancer in Ethiopia: a randomised controlled trial and cost–consequence analysis. Lancet Glob Heal. 2022;10:S13. doi:10.1016/S2214-109X(22)00142-5
17. Abdulwehab S, Kedir F. Barriers and facilitators to palliative care service utilization in Ethiopia: a qualitative systematic review, 2025. PLoS One. 2025;20(8):e0328222. doi:10.1371/journal.pone.0328222
18. Zewdie A, Kassie TD, Anagaw TF, et al. Advanced-stage breast cancer diagnosis and its determinants in Ethiopia: a systematic review and meta-analysis. BMC Womens Health. 2024;24(1):284. doi:10.1186/s12905-024-03133-9
19. Haileselassie W, Mulugeta T, Tigeneh W, Kaba M, Labisso WL. The Situation of Cancer Treatment in Ethiopia: challenges and Opportunities. J Cancer Prev. 2019;24(1):33–42. doi:10.15430/JCP.2019.24.1.33
20. Callaway MV, Connor SR, Foley KM. World Health Organization Public Health Model: a Roadmap for Palliative Care Development. J Pain Symptom Manage. 2018;55(2S):S6–13. doi:10.1016/j.jpainsymman.2017.03.030
21. Mathews J, Hannon B, Zimmermann C. Models of Integration of Specialized Palliative Care with Oncology. Curr Treat Options Oncol. 2021;22(5). doi:10.1007/s11864-021-00836-1
22. Mamo Y, Habte A, W/Giorgis N, et al. The evolution of hospice and palliative care in Ethiopia: from historic milestones to future directions. Ethiop J Heal Dev. 2020;34(4):310–312.
23. Osoba D, Rodrigues G, Myles J, Zee B, Pater J. Interpreting the significance of changes in health-related quality-of-life scores. J Clin Oncol. 1998;16(1):139–144. doi:10.1200/JCO.1998.16.1.139
24. Scott NW, Fayers PM, Aaronson NK, et al. EORTC QLQ-C30 Reference Values. 2008.
25. Oriani A, Dunleavy L, Sharples P, Perez Algorta G, Preston NJ. Are the MORECare guidelines on reporting of attrition in palliative care research populations appropriate? A systematic review and meta-analysis of randomised controlled trials. BMC Palliat Care. 2020;19(1):6. doi:10.1186/s12904-019-0506-6
26. Harding R, Selman L, Agupio G, et al. Validation of a core outcome measure for palliative care in Africa: the APCA African Palliative Outcome Scale. Health Qual Life Outcomes. 2010;8(10):1–9. doi:10.1186/1477-7525-8-10
27. Herdman M, Gudex C, Lloyd A, et al. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual life Res. 2011;20(10):1727–1736.
28. Ornstein KA, Teresi JA, Ocepek-Welikson K, et al. Use of an Item Bank to Develop Two Short-Form FAMCARE Scales to Measure Family Satisfaction With Care in the Setting of Serious Illness. J Pain Symptom Manage. 2015;49(5):894. doi:10.1016/j.jpainsymman.2014.10.017
29. Welie AG, Gebretekle GB, Stolk E, et al. Valuing Health State: an EQ-5D-5L Value Set for Ethiopians. Value Heal Reg Issues. 2020;22:7–14. doi:10.1016/j.vhri.2019.08.475
30. Groenvold M, Petersen MA, Aaronson NK, et al. The development of the EORTC QLQ-C15-PAL: a shortened questionnaire for cancer patients in palliative care. Eur J Cancer. 2006;42(1):55–64. doi:10.1016/j.ejca.2005.06.022
31. Wichmann AB, Goltstein LCMJ, Obihara NJ, et al. QALY-time: experts’ view on the use of the quality-adjusted LIFE year in COST-effectiveness analysis in palliative care. BMC Health Serv Res. 2020;20(1):659. doi:10.1186/s12913-020-05521-x
32. Vickers AJ, Altman DG. Statistics notes: analysing controlled trials with baseline and follow up measurements. BMJ. 2001;323(7321):1123–1124. doi:10.1136/bmj.323.7321.1123
33. Bursac Z, Gauss CH, Williams DK, Hosmer DW. Purposeful selection of variables in logistic regression. Source Code Biol Med. 2008;3:17. doi:10.1186/1751-0473-3-17
34. Bourke S, Bennett B, Oluboyede Y, et al. Estimating the minimally important difference for the EQ-5D-5L and EORTC QLQ-C30 in cancer. Health Qual Life Outcomes. 2024;22(1):81. doi:10.1186/s12955-024-02294-3
35. The International Association for Hospice and Palliative Care (IAHPC). IAHPC List of Essential Medicines for Palliative Care; 2023. Available from: https://iahpc.org/uploads/2011/8/iahpc-essential-meds-en.pdf.
36. Ferrell BR, Temel JS, Temin S, et al. Integration of Palliative Care Into Standard Oncology Care: American Society of Clinical Oncology Clinical Practice Guideline Update. J Clin Oncol. 2017;35(1):96–112. doi:10.1200/JCO.2016.70.1474
37. Merriman A, Mwebesa E, Zirimenya L. Improving access to palliative care for patients with cancer in Africa: 25 years of Hospice Africa. Ecancermedicalscience. 2019;13:946. doi:10.3332/ecancer.2019.946
38. Zimmermann C, Swami N, Krzyzanowska M, et al. Early palliative care for patients with advanced cancer: a cluster-randomised controlled trial. Lancet. 2014;383(9930):1721–1730. doi:10.1016/S0140-6736(13)62416-2
39. Bakitas M, Lyons KD, Hegel MT, et al. Effects of a palliative care intervention on clinical outcomes in patients with advanced cancer: the Project ENABLE II randomized controlled trial. JAMA. 2009;302(7):741–749. doi:10.1001/jama.2009.1198
40. Mishra SI, Scherer RW, Geigle PM, et al. Exercise interventions on health-related quality of life for cancer survivors. Cochrane Database Syst Rev. 2012;2012(8):CD007566. doi:10.1002/14651858.CD007566.pub2
41. Hamdan Alshehri H, Olausson S, Öhlén J, Wolf A. Factors influencing the integration of a palliative approach in intensive care units: a systematic mixed-methods review. BMC Palliat Care. 2020;19(1). doi:10.1186/s12904-020-00616-y
42. Johansson T, Diggle MFJ, Finucane A, et al. Defining and measuring unmet palliative care needs among people with life-limiting illness: a scoping review of international evidence. Palliat Med. 2026;40(4):448–471. doi:10.1177/02692163261416279
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Socioeconomic Disparity Trends in End-of-Life Care for Cancer and Non-Cancer Patients: Are We Closing the Gap?
Vestergaard AHS, Christiansen CF, Neergaard MA, Valentin JB, Johnsen SP
Clinical Epidemiology 2022, 14:653-664
Published Date: 4 May 2022
The Burden of Metastatic Cancer–Induced Bone Pain: A Narrative Review
Colosia A, Njue A, Bajwa Z, Dragon E, Robinson RL, Sheffield KM, Thakkar S, Richiemer SH
Journal of Pain Research 2022, 15:3399-3412
Published Date: 25 October 2022
The Prevalence of Cancer Patients Requiring Palliative Care and Its Associated Factors at St. Paul Hospital, Addis Ababa, Ethiopia: A Cross-Sectional Study
Amare N, Gintamo B, Tukeni KN, Gebremichael EH, Abera EG
Risk Management and Healthcare Policy 2023, 16:1203-1214
Published Date: 28 June 2023
Neurofibromatosis Type 1: Optimizing Management with a Multidisciplinary Approach
Lalvani S, Brown RM
Journal of Multidisciplinary Healthcare 2024, 17:1803-1817
Published Date: 23 April 2024
Systematic Review of the Cost-Effectiveness of Home-Based Palliative Care Interventions in Patients with Cancer: A Critical Analysis
Maresova P, Hruška J, Randlova K, Rezny L, Carrillo-de-la-Peña MT, Kuca K
Cancer Management and Research 2024, 16:1155-1174
Published Date: 6 September 2024