Back to Journals » Journal of Hepatocellular Carcinoma » Volume 13
Multicenter Validation of a RAR-Based Nomogram for Predicting Postoperative Progression in HBV-Related Hepatocellular Carcinoma
Authors Dai W, Tan M, Shen W, Huang J, Chen F, Cai D, Chen B, Li D ![]() , Huang H
, Huang H
Received 12 November 2025
Accepted for publication 30 January 2026
Published 26 February 2026 Volume 2026:13 581070
DOI https://doi.org/10.2147/JHC.S581070
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Imam Waked
Wei Dai,1,* Maoqing Tan,2,* Wenlong Shen,2,* Jun Huang,3 Fengsui Chen,2 Danni Cai,1 Baomin Chen,4 Dongliang Li,2 Huifang Huang1
1Central Laboratory, Fujian Medical University Union Hospital, Fuzhou, Fujian, 350001, People’s Republic of China; 2Department of Hepatobiliary Disease, 900th Hospital of PLA Joint Logistics Support Force (Fuzong Clinical Medical College of Fujian Medical University), Fuzhou, Fujian, 350025, People’s Republic of China; 3Department of Clinical Laboratory, Fujian Medical University Union Hospital, Fuzhou, Fujian, 350001, People’s Republic of China; 4Department of Hepatobiliary Surgery, The First Affiliated Hospital of Sun Yat-Sen University, Guangzhou, Guangdong, 510000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Huifang Huang, Central Laboratory, Fujian Medical University Union Hospital, 29 Xinquan Road, Fuzhou, Fujian, 350001, People’s Republic of China, Tel +8613365910318, Email [email protected] Dongliang Li, Department of Hepatobiliary Disease, 900th Hospital of PLA Joint Logistics Support Force (Fuzong Clinical Medical College of Fujian Medical University), Xi Er Huan Bei Road, Fuzhou, Fujian, 350025, People’s Republic of China, Tel +8613665052006, Email [email protected]
Background: The red cell distribution width–to–albumin ratio (RAR) is a biomarker reflecting systemic inflammation and oxidative stress, and has been associated with outcomes in multiple diseases. However, its value for predicting postoperative recurrence or progression in hepatitis B virus–related hepatocellular carcinoma (HBV-HCC) remains undetermined.
Methods: We retrospectively reviewed 1 011 HBV-HCC patients who underwent surgical treatment at three tertiary centres. Patients were divided into training, internal validation and external validation cohorts. The performance of RAR for predicting progression-free survival (PFS) was assessed using receiver operating characteristic (ROC) analysis, and restricted cubic spline (RCS) modelling was used to explore its nonlinear association with progression risk. Independent prognostic factors were identified by multivariate Cox regression and incorporated into a nomogram and an interactive web-based calculator, which were validated in all cohorts.
Results: RAR achieved an area under the ROC curve (AUC) of 0.662 for predicting PFS. RCS analysis revealed a nonlinear increase in progression risk with rising RAR values, with the curve plateauing at higher levels. Multivariate Cox analysis confirmed RAR as an independent predictor of postoperative PFS (hazard ratio [HR] = 4.40; 95% CI, 1.74– 11.12). The nomogram—integrating RAR, tumour size, alpha-fetoprotein, TNM stage and portal vein tumour thrombus (PVTT)—demonstrated Satisfactory discrimination, excellent calibration and consistent net clinical benefit across data sets.
Conclusion: RAR independently predicts postoperative recurrence or progression in HBV-HCC. The RAR-based nomogram offers a practical tool for individualised estimation of PFS, facilitating more precise postoperative risk stratification and management.
Keywords: red cell distribution width–to–albumin ratio, hepatitis B virus–related hepatocellular carcinoma, progression-free survival, nomogram, prognostic model
Introduction
Hepatocellular carcinoma (HCC) ranks among the most prevalent and lethal malignancies globally, with a steadily increasing incidence and mortality rate that poses a significant public health challenge.1,2 In China, chronic hepatitis B virus (HBV) infection remains the leading cause of HCC, accounting for the majority of cases.3 In recent years, substantial progress has been made in both locoregional and systemic therapies, including the development of highly stable radiolipiodol formulations and microenvironment-responsive interventional drug delivery systems, which have broadened the therapeutic landscape for HCC.4–6 Despite these advances, surgical resection continues to represent the cornerstone and the most effective curative option for patients with HBV-related HCC (HBV-HCC). However, even with standardized surgical management, postoperative tumor recurrence and disease progression remain alarmingly frequent and constitute the principal obstacles to achieving durable survival.7 Previous evidence indicates that up to 70% of patients experience recurrence within five years, emphasizing the need for reliable prognostic indicators to identify individuals at high risk of relapse and to optimize follow-up strategies.8,9
Despite continuous progress in HCC prognostic research, many routinely used biomarkers still exhibit substantial limitations. Inflammatory markers such as the neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR) are associated with clinical outcomes, yet their predictive performance is unstable due to the influence of underlying cirrhosis, inconsistency in optimal cut-off values across studies, and population heterogeneity.10–13 Moreover, alpha-fetoprotein (AFP), the most widely used tumor marker, suffers from insufficient sensitivity and specificity. For early-stage tumors (<3 cm), AFP sensitivity can be as low as 25%, and false-positive elevations are common during active hepatitis or alanine aminotransferase (ALT) flares; notably, approximately 40% of HCC patients present with normal AFP levels. These constraints markedly reduce the clinical utility of traditional biomarkers and underscore the urgent need for novel, economical, reproducible, and readily obtainable prognostic indicators.14,15
Increasing evidence highlights the critical role of systemic inflammation and nutritional status in HCC development and progression. Hematologic and biochemical biomarkers have drawn growing attention because they are inexpensive, accessible, and reproducible for routine assessment.16 Red cell distribution width (RDW), a routinely measured parameter representing erythrocyte size heterogeneity, has been linked to systemic inflammation and oxidative stress in malignancies.17,18 Serum albumin (ALB), a classical indicator of hepatic synthetic function and nutritional reserve, also reflects the host’s inflammatory and immune status.19 Previous studies have indicated that inflammatory markers have potential value in predicting postoperative recurrence,20 and the ratio of RDW to ALB (RAR), which integrates both inflammatory and nutritional dimensions, has recently emerged as a novel inflammation-based prognostic marker and has demonstrated prognostic relevance in multiple cancers.21–23
Nevertheless, whether RAR can predict progression-free survival (PFS) in patients with HBV-HCC undergoing surgical treatment remains unclear. PFS, which captures the interval until tumor recurrence or progression, was chosen as the primary endpoint because it directly reflects early postoperative tumor behavior and is less influenced by subsequent treatments or competing events compared with overall survival (OS).24,25 Exploring the prognostic value of RAR for postoperative PFS may therefore help refine risk stratification and facilitate precision management in HBV-HCC.
Accordingly, this multicenter, real-world study systematically evaluated the prognostic impact of RAR in surgically treated HBV-HCC patients and developed a RAR-based nomogram for individualized prediction of postoperative progression risk, aiming to support tailored follow-up and therapeutic decision-making.
Materials and Methods
Study Population
This multicenter retrospective cohort included HBV-HCC patients who underwent surgical treatment between January 2012 and December 2022 at three tertiary hospitals in China. The inclusion criteria were: (1) confirmed HCC diagnosis via contrast-enhanced computed tomography (CT), magnetic resonance imaging (MRI), or histopathological examination; (2) hepatitis B surface antigen (HBsAg) positivity for more than six months; and (3) no prior antitumor therapy before the initial diagnosis. Exclusion criteria included other viral hepatitis, additional cancers, and incomplete clinical information or missing follow-up data. The selection process is illustrated in Figure S1.
A total of 601 eligible patients from the 900th Hospital of PLA Joint Logistics Support Force (900H) were randomly allocated to the training set (n = 421) and the internal validation set (n = 180) in a 7:3 proportion using R software. An additional 410 cases from Fujian Medical University Union Hospital (FJMUUH) and the First Affiliated Hospital of Sun Yat-sen University (FAHSYSU) constituted the external validation cohort. Relevant demographic, clinical, and biochemical variables were retrieved retrospectively from the institutional electronic medical record systems.
PFS was defined as the interval from the date of surgical treatment to the first documented tumor recurrence, radiologic or clinical disease progression, or death from any cause, whichever occurred first. Patients without events at the last follow-up were censored at that date. The study protocol was approved by the institutional review boards of 900H (2022–014), FJMUUH (2023KY225), and FAHSYSU (Ethics approval No. [2024]241). Given the retrospective observational design, informed consent was waived by all committees. Throughout the entire process, patient privacy and data confidentiality were strictly protected. All data were fully anonymized before analysis, and no identifiable information was accessible to the researchers.
Identification of Prognostic Factors and Nomogram Construction
The prognostic capability of RAR for PFS was first examined through receiver operating characteristic (ROC) curve analysis. Nonlinear relationships between RAR levels and progression risk were further explored using restricted cubic spline (RCS) functions. Potential predictors identified in univariable Cox analyses (p < 0.05) were incorporated into a multivariable Cox regression model to isolate independent prognostic factors. These variables were subsequently integrated into a nomogram constructed within the training cohort.
Model performance was verified across the internal and external validation sets. Discriminatory power was quantified by ROC curves at 1, 2, and 3 years, whereas calibration plots were applied to compare predicted versus actual outcomes. The clinical value of the nomogram was further evaluated using decision curve analysis (DCA).
Development of a Web-Based Dynamic Nomogram
An online dynamic nomogram was implemented using the Shiny and DynNom packages in R and deployed on the shinyapps.io platform. Clinicians can input patient-specific clinical variables to obtain real-time individualized PFS predictions along with visualized results.
Statistical Analysis
The normality of continuous variables was examined using the Kolmogorov–Smirnov test. Data following a normal distribution were expressed as the mean ± standard deviation (SD), whereas non-normally distributed data were summarized as the median and interquartile range (IQR). Categorical variables were described as frequencies and percentages. Differences between groups were analyzed using independent Student’s t-tests or Mann–Whitney U-tests for continuous variables and χ2 or Fisher’s exact tests for categorical variables, as appropriate. Only cases with complete baseline and follow-up information were included, so no additional missing-data handling was required. All statistical procedures were conducted using R software (version 4.2.1; R Foundation for Statistical Computing, Vienna, Austria) and SPSS (version 26.0; IBM Corp., Armonk, NY, USA). A two-tailed p < 0.05 was considered statistically significant.
Results
Patient Characteristics
A total of 1011 patients diagnosed with HBV-HCC who underwent surgical treatment were retrospectively analyzed. Among them, 601 patients from the 900H had a median age of 54 years (IQR: 45–62), and 87% were male (522/601). Their median tumor diameter was 7.0 cm (IQR: 3.9–10.9), with median follow-up and PFS times of 52 and 8 months, respectively. The FJMUUH cohort included 310 patients with a median age of 58 years (IQR: 50–66); 85% were male (264/310), with a median tumor size of 5.3 cm (IQR: 3.0–9.3), median follow-up of 17 months, and median PFS of 34 months. The FAHSYSU cohort consisted of 100 patients, 90% male (90/100), with a median age of 54 years (IQR: 45–60) and a median tumor diameter of 6.0 cm (IQR: 3.8–9.1). The median follow-up and PFS durations were 62 and 15 months, respectively. No significant baseline differences were detected between the training and internal validation cohorts (all p > 0.05), as detailed in Table S1, while comprehensive baseline data for each institution are presented in Table 1.
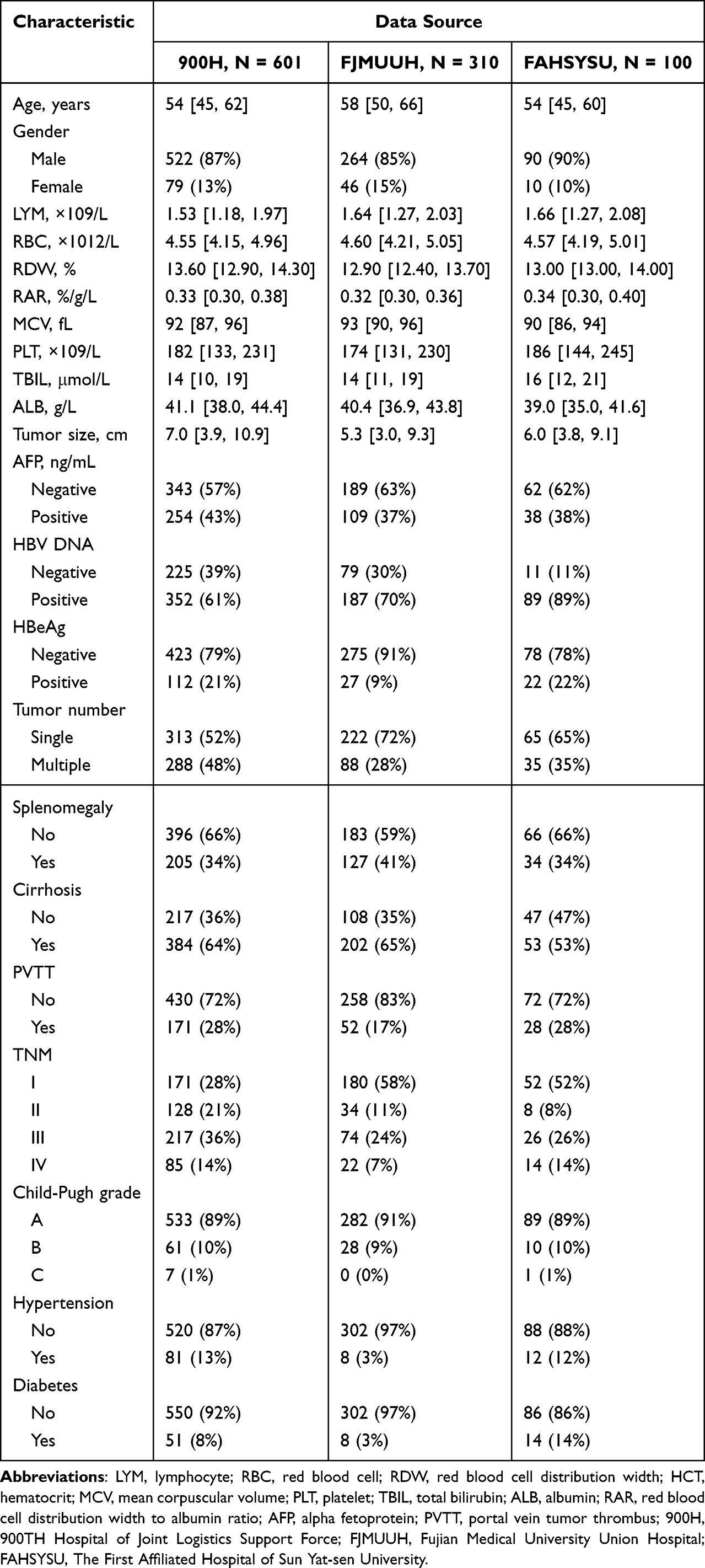 |
Table 1 Clinical Characteristics of the Patients in Three Healthcare Facilities |
Prognostic Value of RAR for Postoperative PFS
ROC curve analysis demonstrated that RAR predicted postoperative PFS with an AUC of 0.662 (95% CI: 0.626–0.697) (Figure 1A). RCS analysis further revealed a nonlinear association between RAR and recurrence or progression risk, showing a gradual increase in risk with higher RAR values, which plateaued at elevated levels (p < 0.001) (Figure 1B).
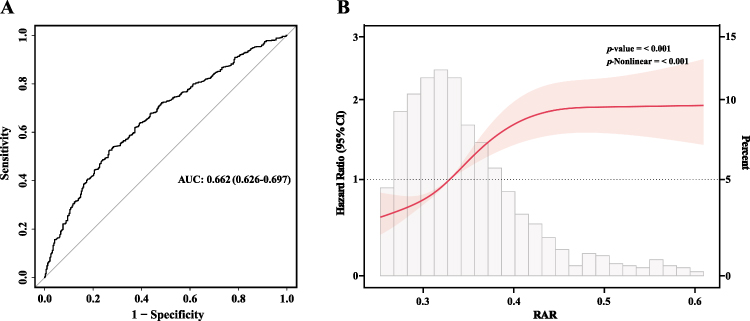 |
Figure 1 ROC and restricted cubic spline analyses of RAR for predicting PFS. (A) Time-dependent ROC curve evaluating the discriminative performance of RAR for PFS; (B) Restricted cubic spline (RCS) curve depicting the nonlinear association between RAR and progression risk. Abbreviations: RAR, red cell distribution width-to-albumin ratio; ROC, receiver operating characteristic; RCS, restricted cubic spline; PFS, progression-free survival. |
Independent Predictors of PFS
In the univariable Cox regression, age, RAR, alpha-fetoprotein (AFP), maximum tumor diameter, portal vein tumour thrombus (PVTT), and TNM stage were all significantly associated with postoperative PFS (all p < 0.05). After multivariable adjustment, RAR remained a strong and independent prognostic indicator (HR = 4.40, 95% CI: 1.74–11.12, p = 0.002). AFP (HR = 1.23, 95% CI: 1.05–1.45, p = 0.011), tumor size (HR = 1.06, 95% CI: 1.04–1.08, p < 0.001), and PVTT (HR = 1.27, 95% CI: 1.03–1.57, p = 0.024) also retained independent significance. The risk of postoperative recurrence increased progressively with advancing TNM stage, with hazard ratios of 1.69 (95% CI: 1.34–2.14) for stage II, 2.20 (95% CI: 1.73–2.79) for stage III, and 4.02 (95% CI: 3.02–5.35) for stage IV (all p < 0.001). These parameters consistently served as independent predictors of postoperative PFS (Table 2).
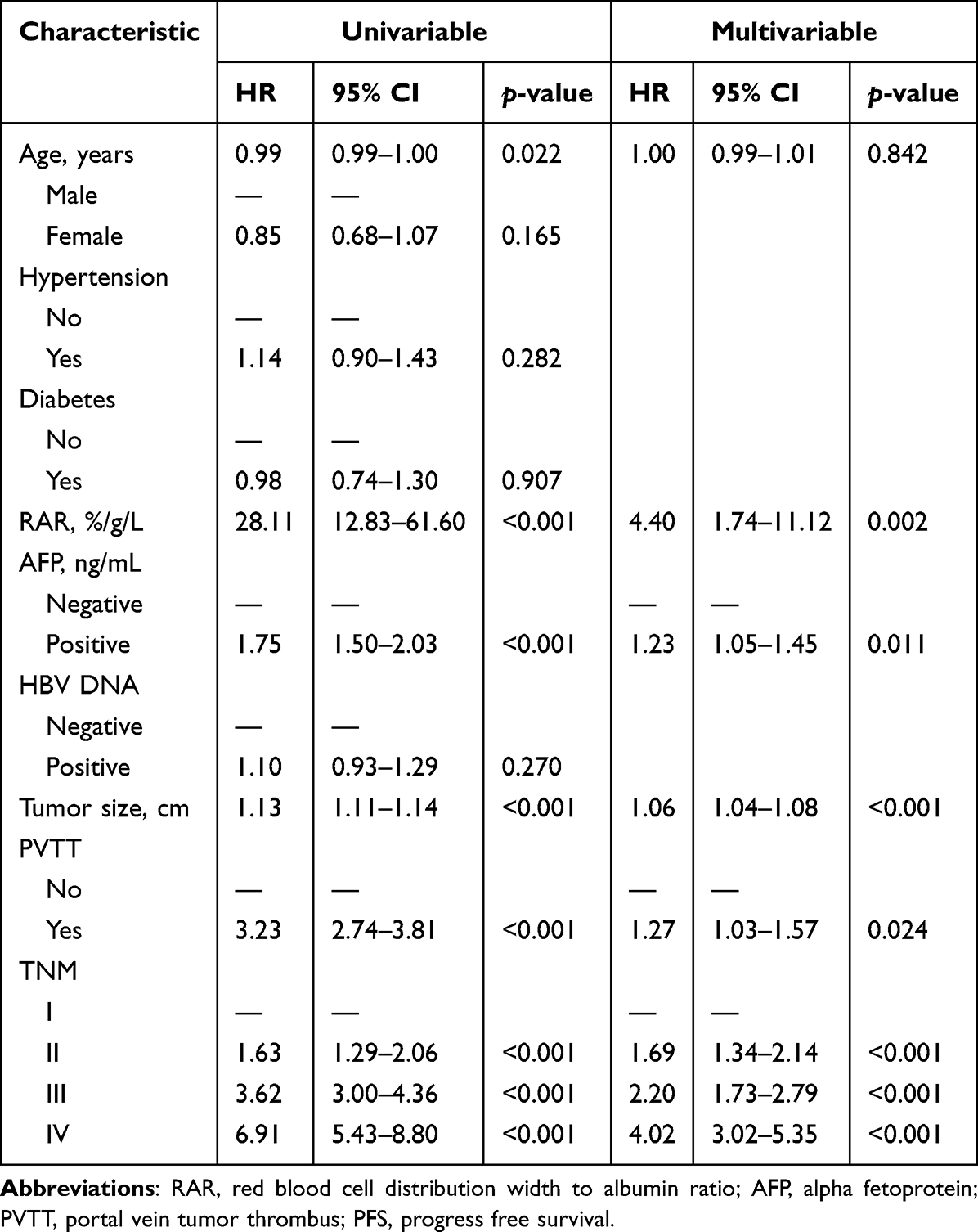 |
Table 2 Univariate and Multivariate Analysis of Factors Associated with PFS |
Nomogram Development and Validation
Independent prognostic factors from the multivariable Cox model—RAR, AFP, maximum tumor diameter, PVTT, and TNM stage—were integrated to build a postoperative nomogram (Figure 2). In the training cohort, discrimination for 1-, 2-, and 3-year PFS was favorable, with AUCs of 78.7% (95% CI: 74.3–83.2%), 81.0% (95% CI: 76.4–85.6%), and 80.9% (95% CI: 75.8–85.9%), respectively (Figure 3A). Performance remained robust in the internal validation cohort, yielding AUCs of 80.9% (95% CI: 74.3–87.5%), 83.9% (95% CI: 77.1–90.7%), and 90.8% (95% CI: 85.5–96.1%) (Figure 3B). External validation showed AUCs of 78.1% (95% CI: 72.9–83.4%), 78.4% (95% CI: 72.9–83.9%), and 75.8% (95% CI: 69.6–82.0%), confirming satisfactory discrimination (Figure 3C). Calibration curves demonstrated close agreement between predicted and observed PFS across cohorts (Figure 4). DCA indicated consistent net clinical benefit across a broad range of threshold probabilities at all evaluated time points (Figure 5).
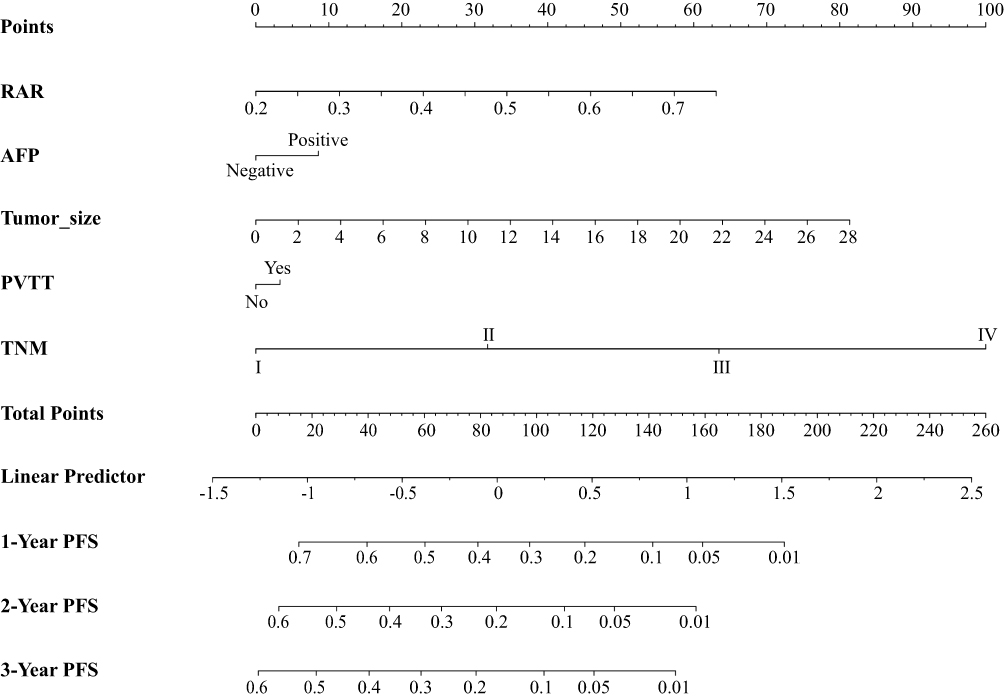 |
Figure 2 Nomogram for predicting progression-free survival in patients with HBV-HCC. Abbreviations: RAR, red cell distribution width-to-albumin ratio; AFP, alpha-fetoprotein; PVTT, portal vein tumor thrombus; PFS, progression-free survival. |
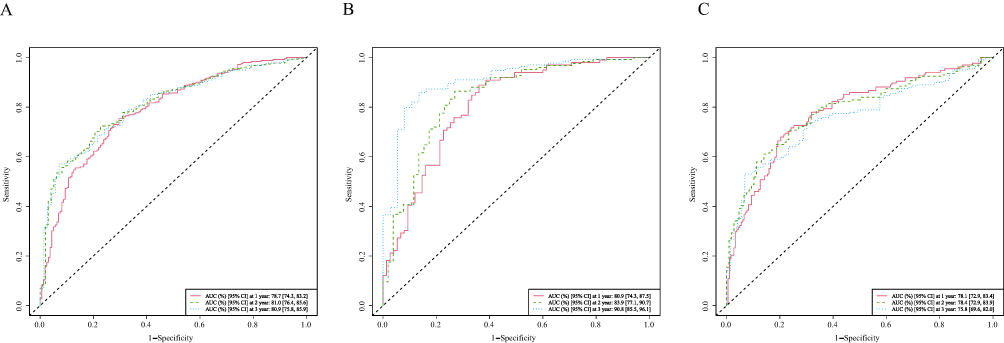 |
Figure 3 Time-dependent ROC curves of the nomogram for predicting PFS. (A) Time-dependent ROC curves for 1-, 2-, and 3-year PFS in the training cohort; (B) Time-dependent ROC curves for 1-, 2-, and 3-year PFS in the internal validation cohort; (C) Time-dependent ROC curves for 1-, 2-, and 3-year PFS in the external validation cohort. Abbreviations: AUC, area under the curve; PFS, progression-free survival. Abbreviations: AUC, area under the curve; PFS, progression-free survival. |
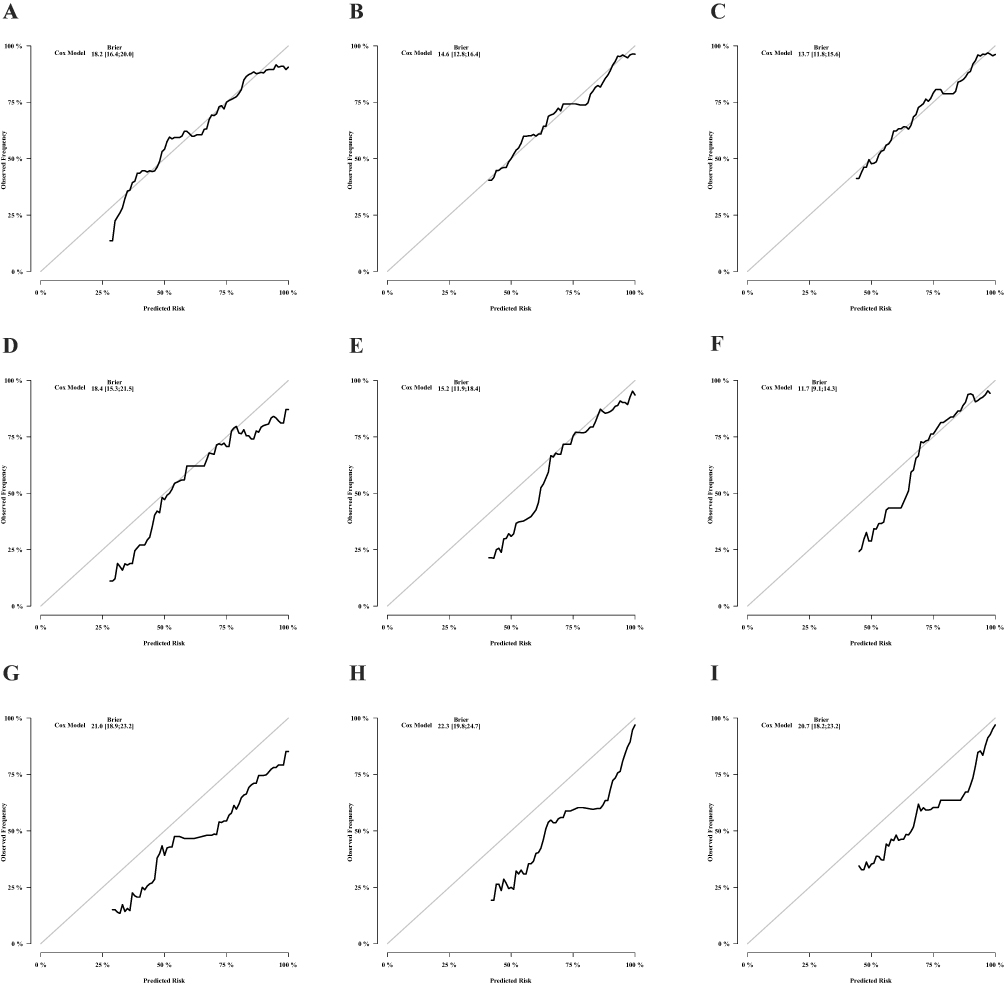 |
Figure 4 Calibration curves of the nomogram for predicting PFS. (A–C) Calibration curves for 1-, 2-, and 3-year PFS in the training cohort; (D–F) Calibration curves for 1-, 2-, and 3-year PFS in the internal validation cohort; (G–I) Calibration curves for 1-, 2-, and 3-year PFS in the external validation cohort. Abbreviations: PFS, progression-free survival. |
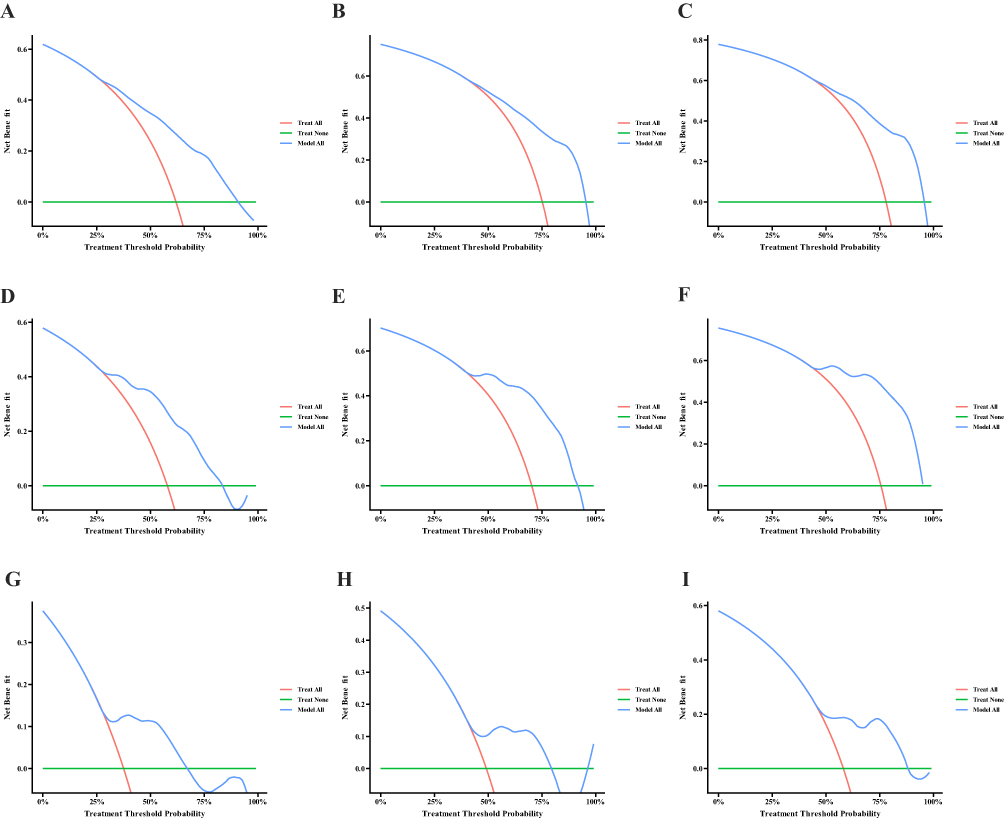 |
Figure 5 Decision curve analysis (DCA) of the nomogram for clinical utility. (A–C) DCA for 1-, 2-, and 3-year PFS in the training cohort; (D–F) DCA for 1-, 2-, and 3-year PFS in the internal validation cohort; (G–I) DCA for 1-, 2-, and 3-year PFS in the external validation cohort. Abbreviations: DCA, decision curve analysis; PFS, progression-free survival. |
Deployment of the Web-Based Dynamic Nomogram
To enhance accessibility, the RAR-based nomogram was implemented as an online interactive tool (available at: https://fmuuhrar.shinyapps.io/dynnomapp/). Clinicians can input patient-specific variables to obtain individualized 1-, 2-, and 3-year PFS probabilities in real time, facilitating the integration of the model into clinical decision-making.
Discussion
This study is the first to establish the independent prognostic value of RAR for postoperative PFS in patients with HBV-related HCC and to construct a validated nomogram based on this marker for individualized risk assessment. The findings indicate that RAR may serve as a practical tool to guide postoperative surveillance and clinical decision-making.
Higher RAR values were consistently associated with unfavorable PFS outcomes. Elevated RAR likely represents a systemic milieu dominated by inflammation and oxidative stress, which promotes residual tumor cell persistence and immune escape.26,27 RDW reflects variability in erythrocyte volume and is a sensitive marker of inflammatory and oxidative injury. Persistent inflammation disrupts erythropoiesis and damages erythrocyte membrane integrity, thereby increasing RDW, while oxidative stress amplifies this disturbance.18,28 Meanwhile, serum albumin reflects not only hepatic synthetic capacity but also nutritional reserves and antioxidant potential.29 By integrating RDW and albumin, RAR captures multiple physiological dimensions, offering a comprehensive assessment of systemic inflammation, oxidative stress, and nutritional status. Elevation of RAR may therefore indicate disrupted metabolic and immune homeostasis, contributing to a microenvironment conducive to tumor recurrence and progression.
In addition to RAR, the nomogram further incorporated AFP, maximum tumor diameter, portal vein tumor thrombus (PVTT), and TNM stage to enhance predictive accuracy. Elevated serum alpha-fetoprotein (AFP) levels are commonly indicative of more biologically aggressive hepatocellular carcinoma, characterized by poorer cellular differentiation, increased incidence of microvascular invasion, greater tumor burden, and unfavorable survival outcomes.30–32 In addition, tumors exceeding 5 cm in diameter are associated with significantly worse prognosis in hepatocellular carcinoma, as larger tumors tend to harbor more aggressive pathology, higher rates of vascular invasion and early recurrence.33–35 The presence of portal vein tumor thrombus (PVTT) denotes advanced-stage disease and is frequently correlated with a median survival of fewer than four months.36 Moreover, higher TNM stages generally reflect enhanced tumor invasiveness and a greater propensity for metastasis. Incorporating these clinical variables alongside RAR enables the nomogram to capture the comprehensive disease burden and postoperative progression risk with improved precision.
Compared with conventional inflammation- or nutrition-related indices such as NLR, PLR, or PNI, RAR offers distinct advantages in clinical application. Traditional markers mainly capture immune cell ratios or nutritional status, but do not fully reflect liver functional reserve or oxidative stress.11,37,38 RAR, by contrast, integrates these physiological dimensions, providing a more holistic overview of systemic metabolic state. Furthermore, the continuous relationship between RAR and PFS was confirmed through ROC and restricted cubic spline analyses, avoiding information loss from arbitrary categorization and enhancing predictive precision and stability.
Beyond traditional markers, emerging HCC prognostic biomarkers such as AFP-L3, DCP/PIVKA-II, circulating tumor DNA (ctDNA), and specific microRNA panels also provide valuable information on tumor biology or residual disease.39–41 However, their clinical application is often limited by cost, accessibility, or technical complexity. In contrast, RAR, derived from routine blood tests, represents a low-cost, convenient, and readily available alternative that reflects host systemic condition rather than tumor-specific features alone, offering an additional dimension for postoperative risk stratification. Clinically, the RAR-based nomogram provides individualized predictions of PFS, which can inform follow-up intensity and adjuvant therapy decisions. High-risk patients may benefit from more frequent imaging or closer monitoring of liver function and tumor markers, whereas low-risk patients can adhere to standard surveillance schedules. The availability of an online dynamic nomogram allows real-time calculation of PFS probabilities, supporting risk-adapted, evidence-based postoperative management.
Several limitations should be considered. First, incomplete follow-up data in some patients may have led to underestimation of progression events. Second, the retrospective design introduces inherent selection bias, limiting the generalizability of the results, which warrants validation in prospective studies. Third, only baseline RAR was assessed, precluding longitudinal evaluation of temporal changes. Future multicenter, prospective studies with large cohorts and longitudinal monitoring of inflammatory and oxidative biomarkers are needed to further elucidate the biological and clinical significance of RAR in HCC recurrence and progression.
Conclusions
RAR is an accessible and cost-effective laboratory indicator derived from routine testing and independently predicts postoperative tumor progression risk in patients with HBV-HCC. The RAR-based nomogram demonstrates robust predictive performance and provides an effective tool for individualized postoperative risk assessment. Owing to its simplicity and ease of implementation, this model may be incorporated into postoperative surveillance workflows to support risk-adapted clinical management. Prospective studies are needed to further validate its clinical utility and elucidate the biological mechanisms linking RAR to tumor progression.
Abbreviations
HCC, Hepatocellular Carcinoma; HBV, Hepatitis B Virus; PFS, progression-free survival; TNM, Tumor Node Metastasis; RDW, Red Blood Cell Distribution Width; ALB, Albumin; RAR, RDW to ALB Ratio; TBIL, Total Bilirubin; LYMs, Lymphocytes; PVTT, Portal Vein Tumor Thrombosis; HR, Hazard Ratio; CI, Confidence Interval; IQR, Interquartile Range; ROC, receiver operating characteristic; AUC, area under curve; AFP, alpha fetoprotein; DCA, decision curve analysis.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are not publicly available due to containing information that could compromise research participant privacy but are available from the corresponding author (Prof. Huifang Huang) on reasonable request and with permission of the local Institutional Review Board.
Ethics Approval and Informed Consent
This study was conducted in accordance with the ethical standards outlined in the Declaration of Helsinki. Ethical approval was obtained from the institutional review boards of the 900th Hospital (No. 2022-014), Fujian Medical University Union Hospital (No. 2023KY225), and the First Affiliated Hospital of Sun Yat-sen University (No. [2024]241).
Acknowledgments
The authors sincerely thank the individuals who took part in this research and the clinical teams who contributed to data collection and patient care.
Author Contributions
Wei Dai, Maoqing Tan, and Wenlong Shen should be considered co-first authors. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was financially supported by Fujian Provincial Government-Funded Project of the Construction of High-Level Laboratory of China (Min201704; H.H.).
Disclosure
The authors declare that there are no competing interests related to this work.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–12. doi:10.3322/caac.21660
2. Llovet JM, Kelley RK, Villanueva A, et al. Hepatocellular carcinoma. Nat Rev Dis Primers. 2021;7(1):6. doi:10.1038/s41572-020-00240-3
3. Chen W, Zheng R, Baade PD, et al. Cancer statistics in China, 2015. CA Cancer J Clin. 2016;66(2):115–132. doi:10.3322/caac.21338
4. Gao X, Cheng H, Teng M, et al. Optimizing interventional therapy: a homogeneous lipiodol formulation of Tirapazamine and Sorafenib responsive to post-embolization microenvironment. J Controlled Release. 2025;379:879–889. doi:10.1016/j.jconrel.2025.01.074
5. Peng Y, Liu H, Liang X, et al. Self-assembling chemodrug fiber-hydrogel for transarterial chemoembolization and radiotherapy-enhanced antitumor immunity. J Controlled Release. 2025;380:1–16. doi:10.1016/j.jconrel.2025.01.088
6. Chen H, Xiong Y, Teng M, et al. A preclinical and first-in-human study of superstable homogeneous radiolipiodol for revolutionizing interventional diagnosis and treatment of hepatocellular carcinoma. Acta Pharmaceutica Sinica B. 2025;15(10):5022–5035. doi:10.1016/j.apsb.2025.02.021
7. Forner A, Reig M, Bruix J. Hepatocellular carcinoma. Lancet. 2018;391(10127):1301–1314. doi:10.1016/s0140-6736(18)30010-2
8. Imamura H, Matsuyama Y, Tanaka E, et al. Risk factors contributing to early and late phase intrahepatic recurrence of hepatocellular carcinoma after hepatectomy. J Hepatol. 2003;38(2):200–207. doi:10.1016/s0168-8278(02)00360-4
9. Bruix J, Sherman M. Management of hepatocellular carcinoma: an update. Hepatology. 2011;53(3):1020–1022. doi:10.1002/hep.24199
10. Lin S, Hu S, Ran Y, Wu F. Neutrophil-to-lymphocyte ratio predicts prognosis of patients with hepatocellular carcinoma: a systematic review and meta-analysis. Transl Cancer Res. 2021;10(4):1667–1678. doi:10.21037/tcr-20-3237
11. Xu C, Wu F, Du L, Dong Y, Lin S. Significant association between high neutrophil-lymphocyte ratio and poor prognosis in patients with hepatocellular carcinoma: a systematic review and meta-analysis. Front Immunol. 2023;14:1211399. doi:10.3389/fimmu.2023.1211399
12. Li D-Z, Guo J, Song Q-K, Hu X-J, Bao X-L, Lu J. Prognostic prediction of the platelet-to-lymphocyte ratio in hepatocellular carcinoma: a systematic review and meta-analysis. Transl Cancer Res. 2022;11(11):4037–4050. doi:10.21037/tcr-22-1197
13. Rocco A, Sgamato C, Pelizzaro F, et al. Systemic inflammatory response markers improve the discrimination for prognostic model in hepatocellular carcinoma. Hepatol Int. 2025;19(4):915–928. doi:10.1007/s12072-025-10806-6
14. Hu J, Wang N, Yang Y, et al. Diagnostic value of alpha-fetoprotein combined with neutrophil-to-lymphocyte ratio for hepatocellular carcinoma. BMC Gastroenterol. 2018;18(1):186. doi:10.1186/s12876-018-0908-6
15. Chan YT, Zhang C, Wu J, et al. Biomarkers for diagnosis and therapeutic options in hepatocellular carcinoma. Mol Cancer. 2024;23(1):189. doi:10.1186/s12943-024-02101-z
16. McMillan DC. The systemic inflammation-based Glasgow Prognostic Score: a decade of experience in patients with cancer. Cancer Treat Rev. 2013;39(5):534–540. doi:10.1016/j.ctrv.2012.08.003
17. Hu L, Li M, Ding Y, et al. Prognostic value of RDW in cancers: a systematic review and meta-analysis. Oncotarget. 2017;8(9):16027–16035. doi:10.18632/oncotarget.13784
18. Salvagno GL, Sanchis-Gomar F, Picanza A, Lippi G. Red blood cell distribution width: a simple parameter with multiple clinical applications. Crit Rev Clin Lab Sci. 2015;52(2):86–105. doi:10.3109/10408363.2014.992064
19. Wiedermann CJ. Hypoalbuminemia as Surrogate and Culprit of Infections. Int J Mol Sci. 2021;22(9). doi:10.3390/ijms22094496
20. Zheng Z, Guan R, Zou Y, et al. Nomogram based on inflammatory biomarkers to predict the recurrence of hepatocellular carcinoma-A multicentre experience. J Inflamm Res. 2022;15:5089–5102. doi:10.2147/jir.S378099
21. Lu C, Long J, Liu H, et al. Red blood cell distribution width-to-albumin ratio is associated with all-cause mortality in cancer patients. J Clin Lab Anal. 2022;36(5):e24423. doi:10.1002/jcla.24423
22. Tan M, You R, Cai D, et al. The red cell distribution width to albumin ratio: a novel prognostic indicator in Hepatitis B virus-related hepatocellular carcinoma. Int J Med Sci. 2025;22(2):441–450. doi:10.7150/ijms.103125
23. Tan M, Liu Y, Dai W, et al. RAR-based prognostic model for predicting overall survival in hepatitis B virus-related hepatocellular carcinoma: a multicenter study. J Inflamm Res. 2025;18:9159–9170. doi:10.2147/jir.S527420
24. Paoletti X, Oba K, Bang YJ, et al. Progression-free survival as a surrogate for overall survival in advanced/recurrent gastric cancer trials: a meta-analysis. J Natl Cancer Inst. 2013;105(21):1667–1670. doi:10.1093/jnci/djt269
25. Blumenthal GM, Karuri SW, Zhang H, et al. Overall response rate, progression-free survival, and overall survival with targeted and standard therapies in advanced non-small-cell lung cancer: US Food and Drug Administration trial-level and patient-level analyses. J Clin Oncol. 2015;33(9):1008–1014. doi:10.1200/jco.2014.59.0489
26. Wang M, Xiao Y, Miao J, et al. Oxidative stress and inflammation: drivers of tumorigenesis and therapeutic opportunities. Antioxidants. 2025;14(6). doi:10.3390/antiox14060735
27. Zhou NJ, Bao WQ, Zhang CF, et al. Immunometabolism and oxidative stress: roles and therapeutic strategies in cancer and aging. Npj Aging. 2025;11(1):59. doi:10.1038/s41514-025-00250-z
28. Mohanty JG, Nagababu E, Rifkind JM. Red blood cell oxidative stress impairs oxygen delivery and induces red blood cell aging. Front Physiol. 2014;5:84. doi:10.3389/fphys.2014.00084
29. Gupta D, Lis CG. Pretreatment serum albumin as a predictor of cancer survival: a systematic review of the epidemiological literature. Nutr J. 2010;9:69. doi:10.1186/1475-2891-9-69
30. Agopian VG, Harlander-Locke MP, Markovic D, et al. Evaluation of patients with hepatocellular carcinomas that do not produce α-fetoprotein. JAMA Surg. 2017;152(1):55–64. doi:10.1001/jamasurg.2016.3310
31. Montal R, Andreu-Oller C, Bassaganyas L, et al. Molecular portrait of high alpha-fetoprotein in hepatocellular carcinoma: implications for biomarker-driven clinical trials. Br J Cancer. 2019;121(4):340–343. doi:10.1038/s41416-019-0513-7
32. Lee WC. Value of alpha-fetoprotein in hepatocellular carcinoma. Translat Gastroenterol Hepatol. 2021;6:52. doi:10.21037/tgh.2019.12.19
33. Dai CY, Lin CY, Tsai PC, et al. Impact of tumor size on the prognosis of hepatocellular carcinoma in patients who underwent liver resection. J Chin Med Assoc. 2018;81(2):155–163. doi:10.1016/j.jcma.2017.06.018
34. Liang BY, Gu J, Xiong M, et al. Tumor size may influence the prognosis of solitary hepatocellular carcinoma patients with cirrhosis and without macrovascular invasion after hepatectomy. Sci Rep. 2021;11(1):16343. doi:10.1038/s41598-021-95835-5
35. Shehta A, Elsabbagh AM, Medhat M, et al. Impact of tumor size on the outcomes of hepatic resection for hepatocellular carcinoma: a retrospective study. BMC Surg. 2024;24(1):7. doi:10.1186/s12893-023-02296-w
36. Minagawa M, Makuuchi M. Treatment of hepatocellular carcinoma accompanied by portal vein tumor thrombus. World J Gastroenterol. 2006;12(47):7561–7567. doi:10.3748/wjg.v12.i47.7561
37. Ma W, Zhang P, Qi J, et al. Prognostic value of platelet to lymphocyte ratio in hepatocellular carcinoma: a meta-analysis. Sci Rep. 2016;6:35378. doi:10.1038/srep35378
38. Wang Z, Wang J, Wang P. The prognostic value of prognostic nutritional index in hepatocellular carcinoma patients: a meta-analysis of observational studies. PLoS One. 2018;13(10):e0202987. doi:10.1371/journal.pone.0202987
39. Li K, Mathew B, Saldanha E, et al. New insights into biomarkers and risk stratification to predict hepatocellular cancer. Mol Med. 2025;31(1):152. doi:10.1186/s10020-025-01194-6
40. Sharma R, Alharbi SN, Ellum K, et al. Deep sequencing of circulating tumour DNA as a biomarker of clinical outcome to transarterial chemoembolisation in hepatocellular carcinoma. NPJ Precision Oncol. 2025;9(1):214. doi:10.1038/s41698-025-00961-2
41. Alemayehu E, Fasil A, Ebrahim H, et al. Circulating microRNAs as promising diagnostic biomarkers for hepatocellular carcinoma: a systematic review and meta-analysis. Front Mol Biosci. 2024;11:1353547. doi:10.3389/fmolb.2024.1353547
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Exploring Prognosis, Tumor Microenvironment and Tumor Immune Infiltration in Hepatocellular Carcinoma Based on ATF/CREB Transcription Factor Family Gene-Related Model
Shen H, Gu X, Li H, Tang M, Li X, Zhang Y, Su F, Wang Z
Journal of Hepatocellular Carcinoma 2023, 10:327-345
Published Date: 27 February 2023
Novel Prognostic Nomogram to Predict Progression-Free Survival of Patients with Hepatocellular Carcinoma After Transarterial Chemoembolization
Xi D, Xu M, Han M, Guan Q, Guo Q, Yan F, Yao J, Ning Q
Journal of Hepatocellular Carcinoma 2023, 10:909-920
Published Date: 16 June 2023
Development and Validation of a Prediction Model for Hepatitis B Virus-Related Hepatocellular Carcinoma Patients Receiving Postoperative Adjuvant Transarterial Chemoembolization
Tu X, Zhang J, Li M, Lu F, Wang T, Gong W, Xiang B
Journal of Hepatocellular Carcinoma 2023, 10:1881-1895
Published Date: 24 October 2023
Development and Validation of Nomograms to Predict the Overall Survival and Progression-Free Survival in Patients with Advanced Unresectable Intrahepatic Cholangiocarcinoma
Xian F, Song X, Bie J, Xu G
Cancer Management and Research 2024, 16:1835-1849
Published Date: 18 December 2024
Prognostic Significance of Circulating Immune Subset Counts in Nasopharyngeal Carcinoma
Xie H, Zhang L, Chen L, Zhou W, Zhang L, Su Y, Li B, Ding P, Xiao Y, Lu T, Gong X, Li J
ImmunoTargets and Therapy 2025, 14:577-587
Published Date: 17 June 2025