Back to Journals » Cancer Management and Research » Volume 17

Multicenter Development of a Clinical-Molecular Nomogram for Predicting Survival in Lung Cancer Brain Metastasis Patients
Authors Qiu X, Lu Z, Li C, Chen S, Zhou X, Peng Z, Chen L, Zhao WP, Shi J, He J, Xia X, Wang Z
Received 8 May 2025
Accepted for publication 14 August 2025
Published 3 September 2025 Volume 2025:17 Pages 1881—1895
DOI https://doi.org/10.2147/CMAR.S538752
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Chien-Feng Li
Xiansheng Qiu,1,2,* Zhenwei Lu,1,2,* Chongfei Li,1,2 Sifang Chen,2 Xiaoping Zhou,1,3 Zhizhu Peng,4 Li Chen,1 Wen peng Zhao,2 JingJing Shi,2 Jiawei He,2 Xuewei Xia,5,* Zhanxiang Wang1,*
1The School of Clinical Medicine, Fujian Medical University, Fuzhou, Fujian, People’s Republic of China; 2The First Hospital Affiliated of Xiamen University, Xiamen, Fujian, People’s Republic of China; 3Ganzhou People’s Hospital, Ganzhou, Jiangxi, People’s Republic of China; 4Guangxi Second People’s Hospital, Guangxi Zhuang Autonomous Region, People’s Republic of China; 5The First Hospital Affiliated of Guilin Medical University, Guilin, Guangxi Zhuang Autonomous Region, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xuewei Xia, Department of Neurosurgery, Affiliated Hospital of Guilin Medical University, No. 15 Lequn Road, Guilin, Guangxi, 541001, People’s Republic of China, Tel +86-773-2800672, Fax +86-773-2812650, Email [email protected] Zhanxiang Wang, The School of Clinical Medicineh, Fujian Medical University, The First Hospital Affiliated of Xiamen University, Xiamen, Fujian, People’s Republic of China, Tel/Fax +86-0592-2139715, Email [email protected]
Background: Lung cancer brain metastasis (LCBM) accounts for 40– 50% of intracranial malignancies, with emerging evidence of alternative metastatic pathways circumventing the blood-brain barrier. Existing prognostic models lack validation in Asian populations and molecular stratification. This multicenter study aimed to develop a clinical nomogram integrating clinicopathological and molecular determinants for personalized LCBM management.
Methods: Retrospective analysis of 522 surgically treated LCBM patients (2015– 2021) from four Chinese institutions was conducted. Patients were randomized 7:3 into training (n=365) and validation (n=157) cohorts. Multivariate Cox regression identified independent prognostic factors, which were incorporated into a nomogram predicting 6-/12-/18-month overall survival (OS). Model performance was assessed via time-dependent ROC curves (AUC), calibration plots, and decision curve analysis (DCA).
Results: The median OS after neurosurgery was 9 months (range: 4– 18 months), with 6-, 12-, and 18-month survival rates of 86.2%, 46.7%, and 17.2%, respectively. Independent predictive factors included brain metastasis size ≥ 5 cm, Leptomeningeal metastasis(LM), EGFR mutation with TKI treatment, and extracranial metastases. The nomogram demonstrated robust discriminative ability and calibration. EGFR-mutant patients receiving postoperative TKIs showed significantly prolonged survival attributable to enhanced blood-brain barrier permeability. Finally, the authors developed a web-based dynamic nomogram for LCBM patients to facilitate clinical implementation.
Conclusion: This study establishes a validated prognostic model integrating tumor burden, EGFR mutation status, and metastatic patterns. It demonstrates that EGFR-guided TKI therapy and bone metastasis surveillance critically influence LCBM outcomes. The nomogram provides a quantifiable framework for risk-adapted therapeutic decisions, advancing precision oncology in neuro-oncology practice.
Keywords: nomogram, overall survival, lung cancer brain metastases, cranial metastases, surgery
Introduction
Lung cancer (LC), as the leading cause of global cancer morbidity and mortality, poses a significant public health threat in China with approximately 1.06 million new cases annually and a mortality rate of 28.5 per 100,000.1,2 Approximately 40–50% of LC patients develop brain metastases during disease progression, with its incidence surpassing gliomas to become the most prevalent type of intracranial malignancy.3,4 The mechanisms underlying lung cancer brain metastasis (LCBM) formation include the classical hematogenous dissemination route (intracranial vascular invasion by cancer cells) and novel metastatic patterns revealed through breakthrough research: tumor cells may migrate along the peri-vascular spaces of vertebral vessels,5,6 penetrating the leptomeninges via cranial emissary veins to infiltrate brain parenchyma. This pathway completely circumvents blood-brain barrier(BBB) defense mechanisms.7 Notably, the bone metastatic pattern, as a newly identified LCBM pathway, demonstrates insufficient clinical translatability evidence thus far.
In recent years, innovations in targeted/immunotherapy have significantly extended median survival in advanced LC. Evidence-based medicine findings demonstrate that LCBM prognosis is strongly associated with driver gene status.8 While patients with epidermal growth factor receptor (EGFR)-mutated non-small cell lung cancer (NSCLC) exhibit 27–35% prolonged survival compared to wild-type counterparts, their risk of brain metastasis increases 2–3-fold.9–11 However, the underlying pathophysiological mechanisms of this paradoxical association between genotype and metastatic risk remain incompletely elucidated.
Additionally, the quantitative associations between features such as brain metastasis volume (>3cm), Leptomeningeal metastasis(LM), neurological dysfunction, and extracranial multi-organ metastases with survival outcomes still require validation through large-scale studies. While existing prognostic models based on Recursive Partitioning Analysis (RPA) classification and Graded Prognostic Assessment (GPA) scores provide clinical references,12,13 their generalizability within Asian populations with LCBM has not yet been sufficiently validated.
This study, utilizing multi-center clinical data from socioeconomically diverse regions including Fujian, Jiangxi, and Guangxi, systematically investigated prognostic variables in postoperative LCBM patients, with particular focus on elucidating the mechanistic impacts of EGFR mutation status, bone metastatic patterns, and clinicopathological characteristics. By developing a clinicopathological nomogram model with clinically significant predictive efficacy, it provides robust evidence-based evidence to inform precision medicine practices and stratified clinical trial management.
Materials and Methods
Patient Selection
This retrospective analysis examined 1158 LCBM surgical cases from January 2015 to January 2021, ultimately enrolling 522 eligible patients (Figure 1). The cohort comprised cases from four institutions: The First Affiliated Hospital of Xiamen University (128), Ganzhou People’s Hospital (261), Guilin Medical University Affiliated Hospital (90), and Guangxi Second People’s Hospital (43). Participants were randomized 7:3 into training (n=365) and validation (n=157) cohorts. Conducted per China’s Clinical Practice Guideline for Lung Cancer Brain Metastases,14 the study followed surgical recommendations throughout, with operative indications including: 1) Single lesion in anatomically resectable locations (eg, non-eloquent cortex); 2) Significant mass effect (perilesional edema >30 mL) or obstructive hydrocephalus; 3) Acute intracranial pressure decompensation (tumor hemorrhage, impending herniation); 4) Diagnostic histopathological confirmation. All data underwent consensus review by neurosurgical, radiological, and pathological specialists.
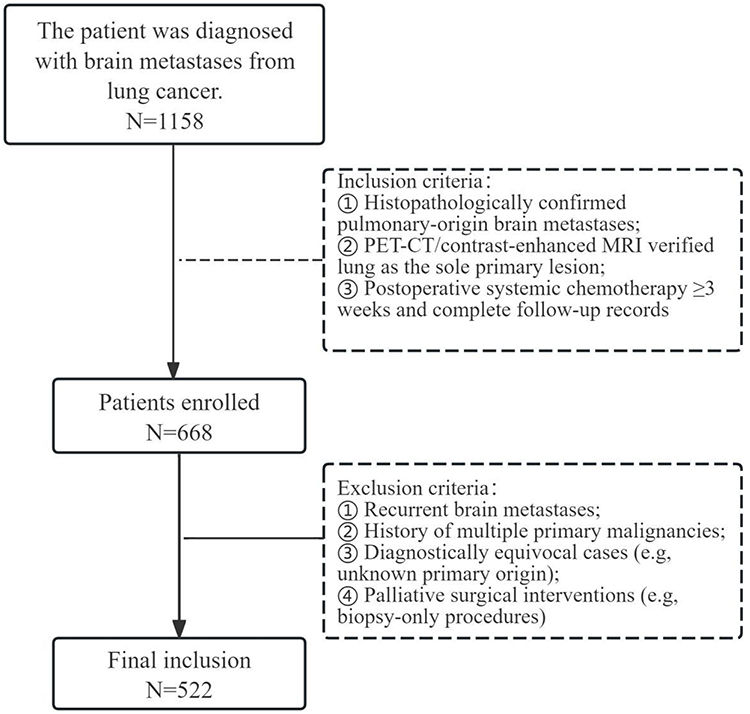 |
Figure 1 Flow chart for patient selection. |
This study conducted a systematic review of 1158 surgically managed LCBM cases from healthcare institutions across four provinces between January 2015 and January 2021, ultimately enrolling 522 rigorously screened surgical patients meeting inclusion criteria (Figure 1). The cohort comprised four regional medical centers: The First Affiliated Hospital of Xiamen University (n=128), Ganzhou People’s Hospital (n=261), Guilin Medical University Affiliated Hospital (90), and Guangxi Second People’s Hospital (43), with cases randomly allocated in a 7:3 ratio to model training (n=365) and internal validation cohorts (n=157). The protocol strictly adhered to the Chinese Clinical Practice Guideline for Brain Metastases of Lung Cancer,14 with surgical indications for LCBM defined as: ① Solitary lesion with anatomically favorable location for gross total resection (eg, non-eloquent cortical areas); ② Significant mass effect (peritumoral edema volume >30mL) or obstructive hydrocephalus; ③ Acute intracranial pressure decompensation (tumor apoplexy/pre-herniation status); ④ Surgical intervention for histopathological diagnostic confirmation.
Inclusion Criteria
- Histopathologically confirmed pulmonary-origin brain metastases;
- PET-CT/contrast-enhanced MRI verified lung as the sole primary lesion;
- Postoperative systemic chemotherapy ≥3 weeks and complete follow-up records
Exclusion Criteria
- Recurrent brain metastases;
- History of multiple primary malignancies;
- Diagnostically equivocal cases (eg, unknown primary origin);
- Palliative surgical interventions (eg, biopsy-only procedures)
Ethical Statement
This study received approval from the Institutional Review Board of The First Affiliated Hospital of Xiamen University(XMYY-2022KY076). In accordance with national regulations for retrospective observational studies using fully anonymized data, the requirement for informed consent was formally waived. All procedures strictly adhered to the ethical principles of the Declaration of Helsinki.
Data Collection and Variables Definitions
Collected patient data included: gender, age, presenting symptoms, histological subtype, skull invasion, LM, tumor number, tumor size (The maximum diameter of the tumor on CT or MRI scans), extracranial metastases, EGFR mutation status, survival data, and cause of death.
Overall survival (OS) was defined as the duration from craniotomy diagnosis to death or last follow-up, with the final follow-up date being December 31, 2024.
Survival Data Analysis, Nomogram Construction and Evaluation
All data were organized and analyzed using Microsoft Excel (version 2016), SPSS (version 25.0), and R (version 4.4). All patients were randomly divided into training and validation sets at a 7:3 ratio and classified using R software. We then used the training set to identify independent prognostic factors associated with OS and construct a prognostic nomogram, while the validation set was used to verify the nomogram’s performance. Details are as follows:
(1) Screening of influencing factors: Using overall survival (OS) of brain metastasis patients as the dependent variable, potential predictors with statistical significance (P<0.10) were first screened via univariate Cox regression analysis, incorporating clinically observed features with potential prognostic value to form an initial variable pool. Risk variables identified by univariate Cox regression (P<0.1) were further analyzed using multivariate Cox regression to determine independent prognostic factors associated with OS in LCBM patients.
(2) Nomogram development: A visual predictive tool was constructed based on the final Cox model parameters. Through linear transformation, the regression coefficients of each independent prognostic variable were mapped to a 0–100-point scoring scale. The total score for individual patients was obtained by summing the corresponding points for each variable. This total score could then be converted into predicted probabilities of 6-month, 12-month, and 18-month survival, enabling individualized prognostic assessment.
(3) Model validation system: Model performance was evaluated using a multidimensional approach:
① Discriminative ability: Time-dependent receiver operating characteristic (ROC) curve analysis was performed to calculate the area under the curve (AUC), assessing sensitivity and specificity for 6-, 12-, and 18-month survival predictions.
② Calibration: Bootstrap resampling (1000 repetitions) was used to generate calibration curves, evaluating the agreement between predicted survival rates and actual Kaplan-Meier estimates.
③ Clinical utility: Decision curve analysis (DCA) quantified the model’s net benefit across different threshold probabilities.
④ Internal validation: Bootstrap resampling was applied to calculate the corrected mean AUC and its 95% confidence interval, assessing the degree of model overfitting.
Results
Patient Characteristics
According to our inclusion criteria, a total of 522 patients were enrolled, including 372 males (71.26%) and 150 females (28.74%). The median age at BM surgery was 61 years (range: 31–81 years). Histopathological subtypes included: adenocarcinoma (42.91%), squamous cell carcinoma (22.8%), large cell carcinoma (19.92%), and small cell carcinoma (14.37%). In addition to brain tissue involvement, 72 cases (13.79%) presented with skull invasion and 84 cases (16.09%) had LM. Detailed demographic and clinicopathological characteristics are summarized in Table 1 below.
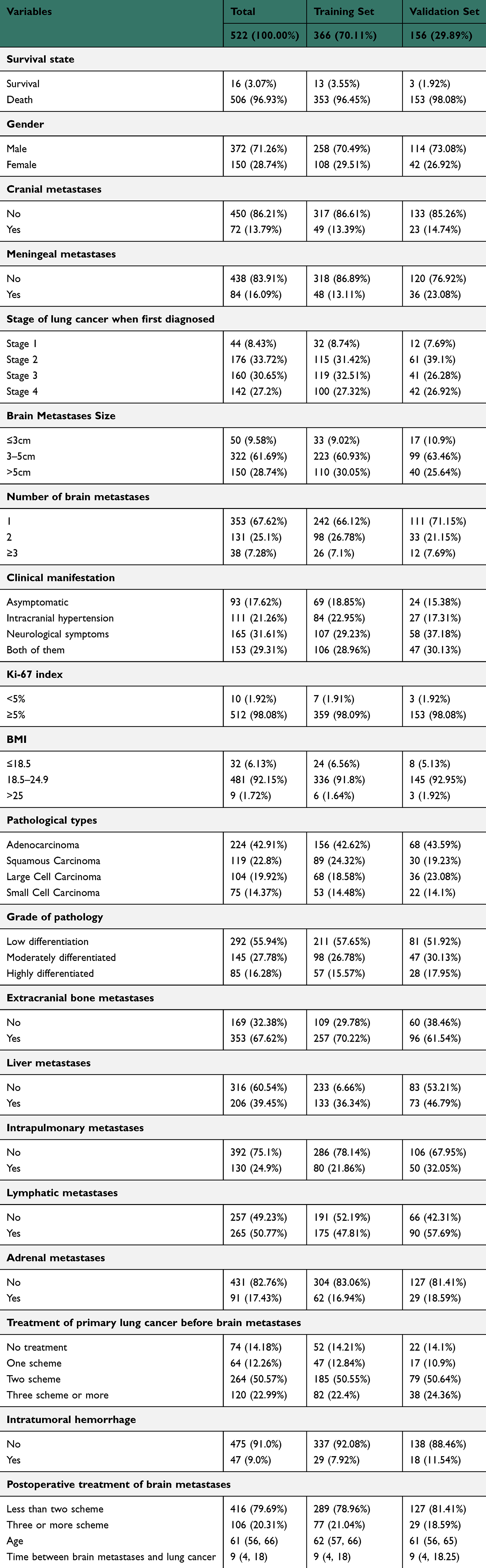 |
Table 1 Baseline Demographic and Clinicopathological Characteristics of OS-Related Variables in Lung Cancer with Brain Metastases |
Survival Analysis
Kaplan-Meier Survival Curves and Associated Parameters
At final follow-up, 16 of the 522 enrolled patients remained alive, with a median overall survival (OS) of 9 months (range: 4–18 months). The survival rates at 6, 12, 18, 24, and 36 months were 86.20%, 46.74%, 17.24%, 9.96%, and 4.21%, respectively (Figure 2A). Significant prognostic factors included tumor size, multiplicity, and anatomical location (Figure 2B–E); histopathological characteristics, intracranial hemorrhage, and clinical manifestations (Figure 2F–I); and extracranial metastasis status with postoperative therapeutic strategies (Figure 2J–N).
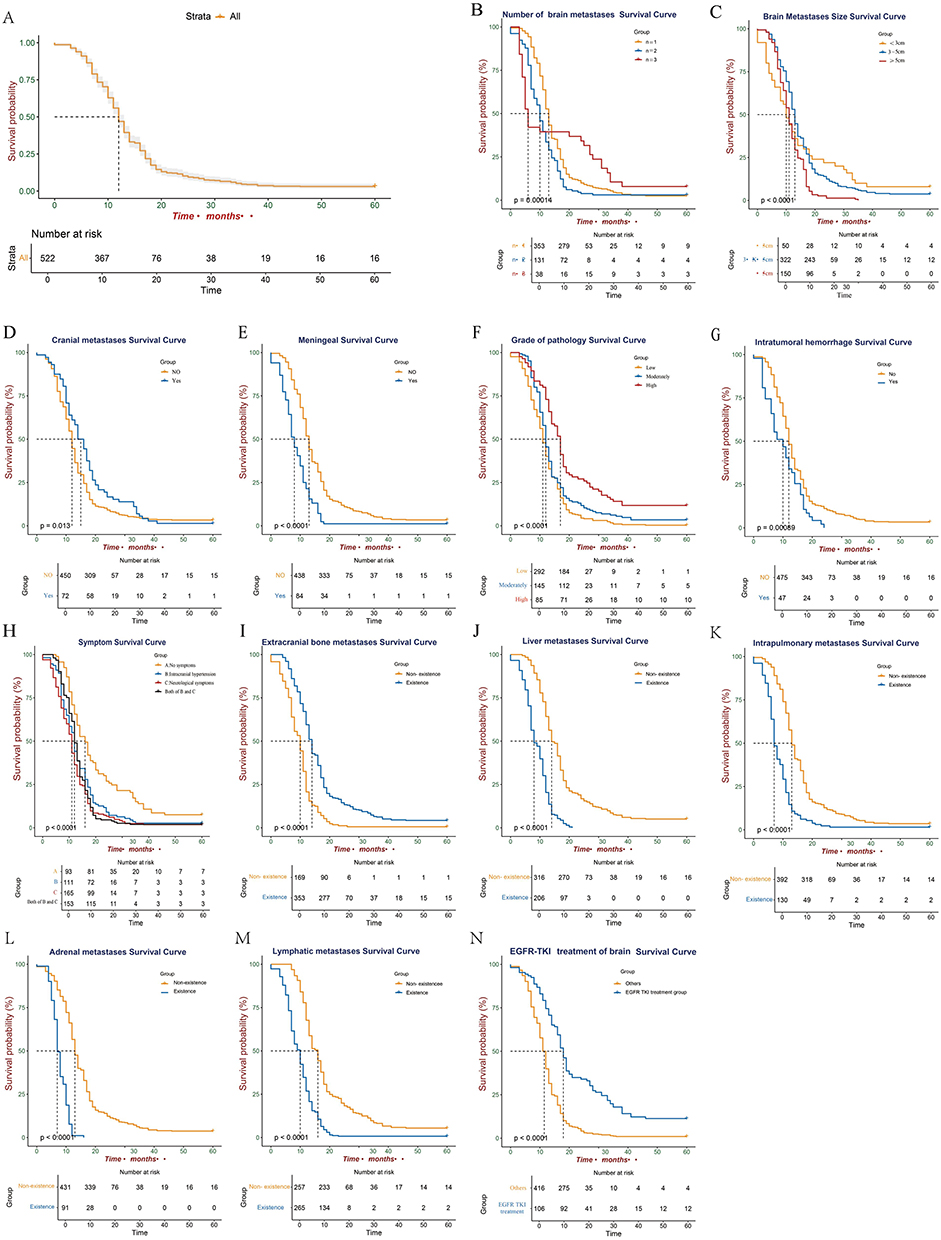 |
Figure 2 Analysis of overall survival-related risk variables in patients with cranial metastases from lung cancer using Kaplan-Meier survival curves. (A) Overall survival curve; (B) Tumor size; (C) Number of tumors; (D) Meningeal metastases; (E) Craniofacial metastases; (F) Type of pathology; (G) Intratumoral hemorrhage; (H) Clinical presentation; (I) Extracranial bone metastases; (J) Contralateral lung metastases; (K) Lymphatic metastases; (L) Hepatic metastases; (M) Adrenal metastases; (N) EGFR-TKI treatment of brainSurvival Curve. |
Univariate and Multivariate Cox Regression Analyses
All patients were included in univariate and multivariate analyses to identify survival predictors. Univariate analysis revealed significantly worse prognosis for patients with LM (HR=2.93, 95% CI: 2.19–3.91, P<0.001) and intratumoral hemorrhage (HR=1.48, 95% CI: 1.03–2.14, P=0.034). Additionally, brain metastasis area >5 cm (HR=2.14, 95% CI: 1.42–3.24, P<0.001), tumor number >3 (HR=0.78, 95% CI: 0.50–1.21, P=0.27), concurrent neurological signs and intracranial hypertension symptoms (HR=2, 95% CI: 1.45–2.74, P<0.001), Small cell lung cancer (SCLC) (HR=2.5, 95% CI: 1.83–3.42, P<0.001), and poorly differentiated adenocarcinoma (HR=0.46, 95% CI: 0.33–0.64, P<0.001) were significantly associated with shorter BMOS. Other variables, including extracranial metastases (bone, liver, lung, lymph nodes, adrenal glands, etc), initial LC diagnosis stage, and whether patients received active treatment after craniotomy, also showed significant correlations with survival (Table 2).
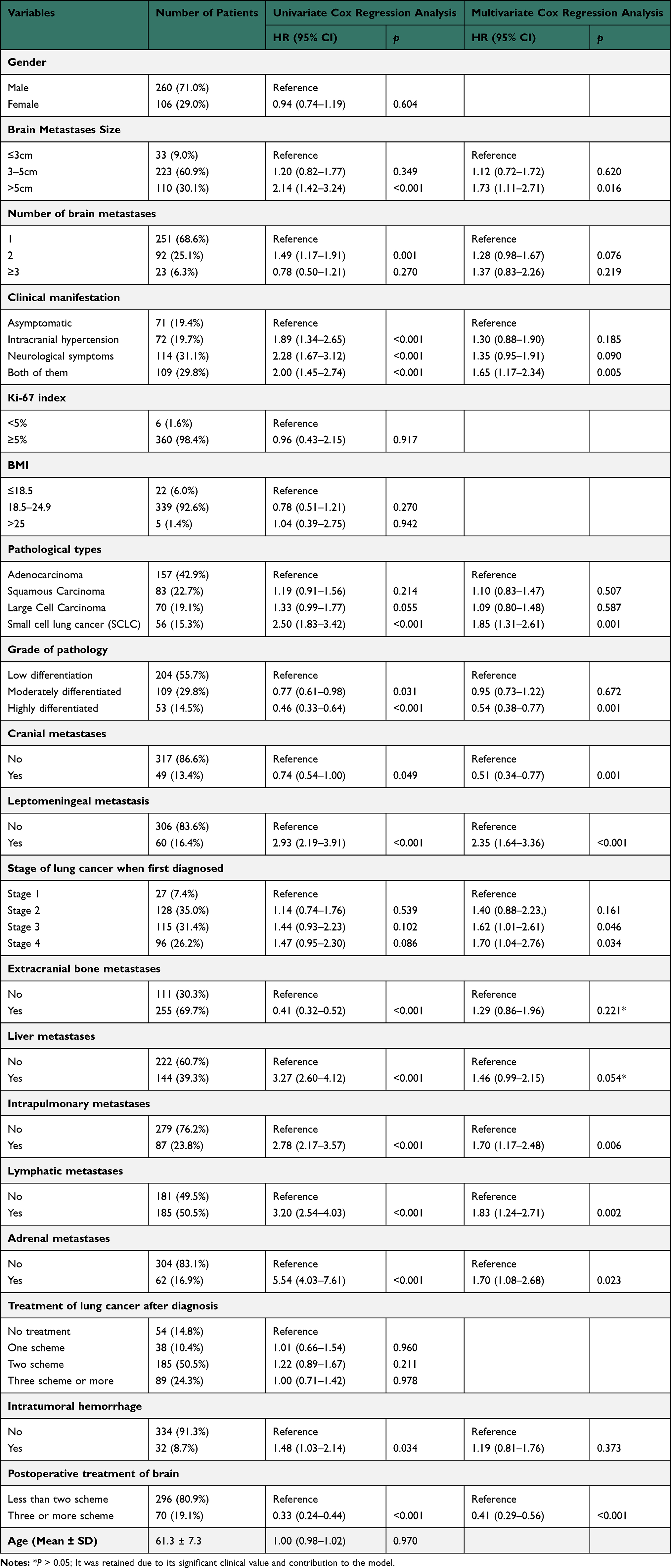 |
Table 2 Univariate and Multivariate Cox Regression Analysis of OS-Related Variables in Lung Cancer Patients with Craniocerebral Metastases |
Further multivariate Cox regression analysis demonstrated that brain metastasis size ≥5 cm, multiple brain metastases, presence of neurological clinical manifestations, preoperative intratumoral hemorrhage, poorly differentiated SCLC, skull metastasis, LM, stage IV LC at initial diagnosis, extracranial metastases (bone, liver, contralateral lung, lymph node, adrenal gland), and EGFR-positive status with TKI treatment were all independent prognostic factors for LCBM patients (Table 2).
Nomogram Development and Validation
The 15 independent prognostic predictors identified from the multivariate Cox regression analysis were integrated to construct a predictive nomogram for quantitatively assessing 6-month, 12-month, and 18-month OS risk in LCBM patients (Figure 3). By assigning weighted scores to each variable and calculating the total points, the nomogram estimated individual mortality probabilities for LCBM patients. All patients were then randomly divided into training (Figure 4A) and validation cohorts (Figure 4B) at a 7:3 ratio. Calibration curves at 6, 12, and 18 months demonstrated close agreement between predicted and observed mortality probabilities in both cohorts, confirming the nomogram’s high predictive accuracy.
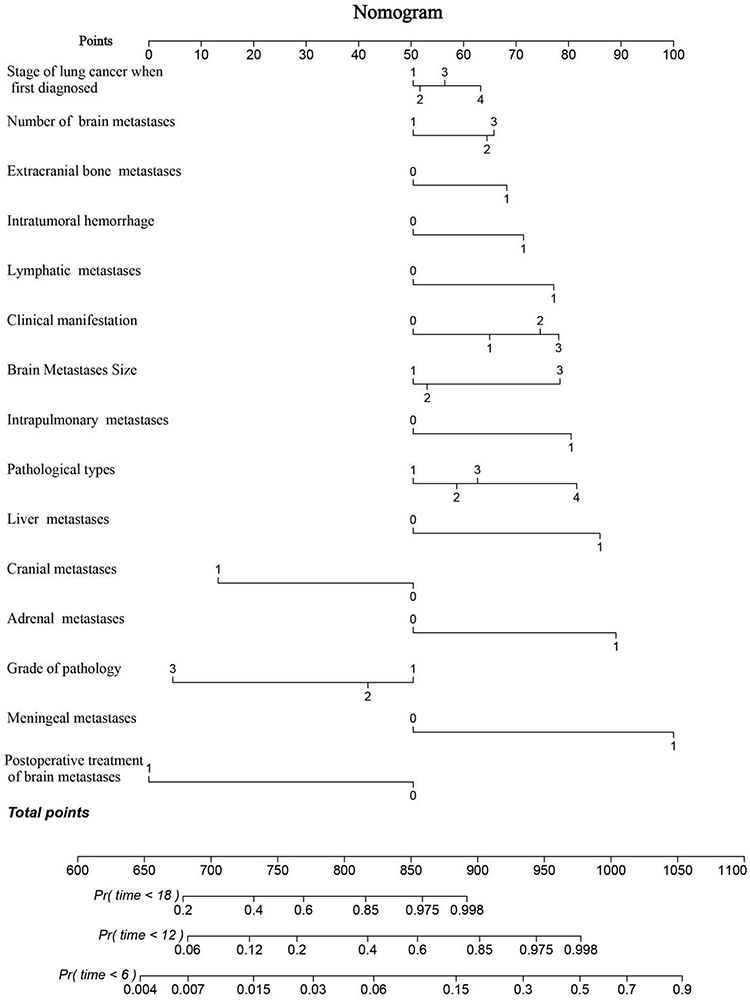 |
Figure 3 The prognostic nomogram predicts the 6, 12, and 18 months probability of OS in patients with LCBM. |
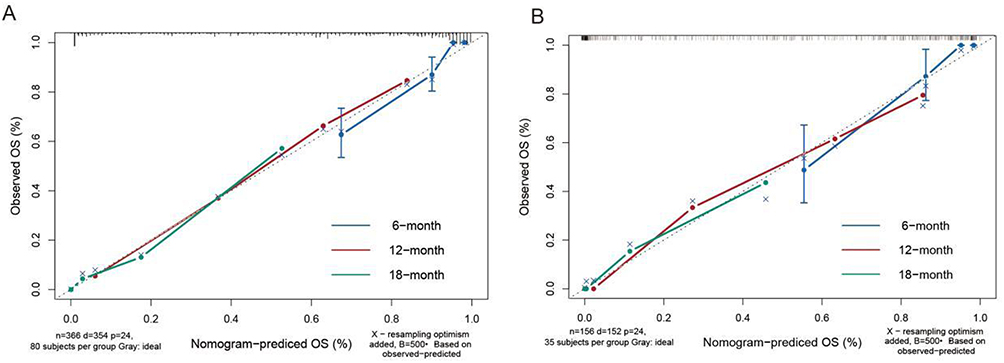 |
Figure 4 Calibration curves for 6, 12 and 18 months prediction in training set (A) and validation set (B). |
In the training cohort, the AUC values for the ROC curves were 0.919 (6-month), 0.872 (12-month), and 0.927 (18-month, Figure 5A), while in the validation cohort the corresponding values were 0.900, 0.851, and 0.873 (Figure 5B), indicating robust discriminative ability of the nomogram. Furthermore, decision curve analysis confirmed that the nomogram serves as an effective clinical tool for evaluating mortality risk in LCBM patients, demonstrating significant clinical utility (Figure 6A and B).
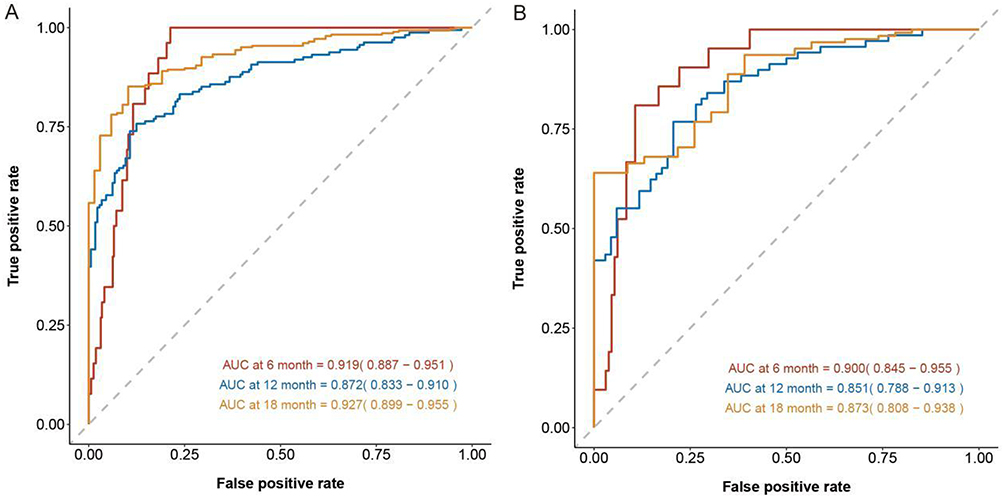 |
Figure 5 Receiver operating characteristic curves for 6 months, 12 months, and 18 months probability of OS in patients with LCBM in the training (A) and validation set (B). |
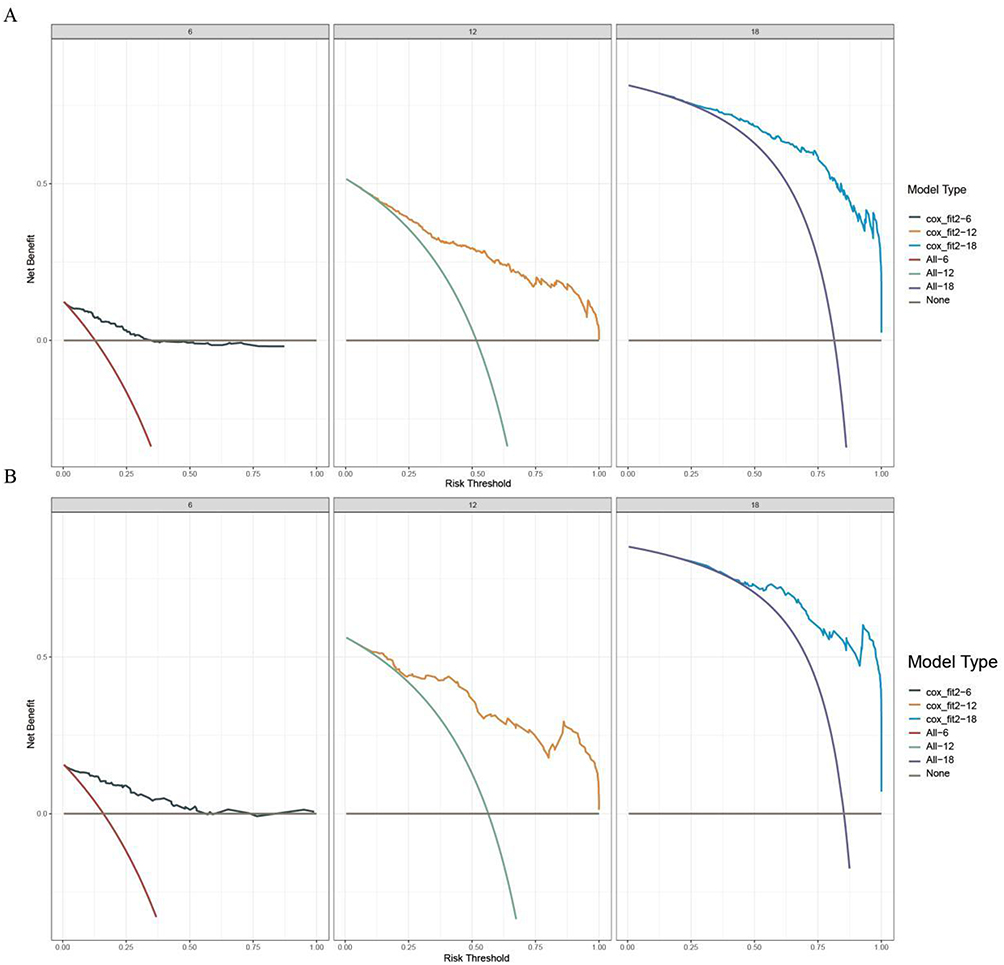 |
Figure 6 Decision curve analysis of the training and validation sets. Decision curve analysis of the nomogram for predicting the 6 months, 12 months and 18 months OS in the training set (A)and the 6 months, 12 months and 18 months OS in the validation set (B) of patients with LCBM. |
Web-Based Dynamic Nomogram
The authors developed a web-based dynamic nomogram to facilitate clinical application and generalization. By accurately inputting information on various independent prognostic factors, it can predict OS in LCBM patients (https://huyiba.shinyapps.io/QiuS/), thereby helping clinicians utilize the nomogram model more effectively.
Discussion
In this study, we investigated the differential clinical characteristics of bone metastasis-predisposing brain metastases and the prognostic impact of EGFR mutation status. To eliminate histological confounding factors, this analysis was restricted to data with histologically confirmed LC as the sole metastatic origin via brain tissue. Notably, bone metastatic tumors demonstrated increased probabilities of skull invasion and meningeal invasion. Concurrently, we followed survival outcomes in EGFR mutation-positive patients and developed a nomogram prediction model through univariate/multivariate analyses to estimate 6-/12-/18-month postoperative overall survival rates.
Recent studies reveal tumor cells can bypass the blood-brain barrier via anatomical conduits7 (eg peri-vascular spaces of vertebral vessels and cranial emissary veins) to directly invade the leptomeninges.15,16 Once breaching the leptomeninges, malignant cells rapidly disseminate through the subarachnoid space and cerebrospinal fluid (CSF) circulation, forming diffuse LM.17 As LM is unresectable, clinical management primarily involves palliative interventions like CSF diversion (eg, Ommaya reservoir chemotherapy) or diagnostic biopsies, yet prognosis remains dismal with a median survival of ~4 months.18–20 Our findings indicate about 70% of skull metastasis patients developed concurrent LM, potentially attributable to skull-leptomeningeal anatomical contiguity: tumor cells synchronously or sequentially colonized skull and leptomeninges via emissary veins before invading adjacent tissues,21,22 corroborating the “bone metastasis and intracranial invasion” pathway as an alternative to classical hematogenous spread.7 Histopathological analysis showed skull metastases exclusively originated from NSCLC (adenocarcinoma 39%, squamous cell carcinoma 18.7%, large cell carcinoma 9%), while SCLC was absent—likely due to its indolent skull metastatic behavior (prolonged latency from primary LC to skull metastasis) and rapid intracranial progression once intracranially seeded,23,24 precluding surgical candidacy.25,26 These findings suggest skull metastasis may serve as a sentinel marker for impending LM,27 though the preventive value of early interventions (eg, metastatic lesion resection) requires validation through prospective studies.28
Beyond inherent tumor characteristics, postoperative pharmacotherapy sensitivity significantly impacts survival outcomes in LCBM patients.29,30 Current postoperative management of brain metastases remains understudied, with most approaches extrapolating metastatic potential from primary lung cancer histopathology and imaging features—a paradigm overlooking brain-specific pathological attributes.30–32 This study exclusively analyzed LCBM histopathological profiles, emphasizing the unique prognostic and therapeutic implications of EGFR signaling axis activation. Within the ASCO-SNO-ASTRO guideline-endorsed multidisciplinary framework (surgery, systemic therapy, radiotherapy),33 EGFR mutation-positive patients demonstrated superior OS following pharmacotherapy, attributable to: ① Potential transient modulation of local BBB integrity post-surgery, which may facilitate exposure of residual tumor cells to systemically administered EGFR-TKIs with inherent CNS activity (eg, osimertinib);34–36 ② postoperative molecular profiling identifying T790M secondary mutations in 21% of EGFR-mutant patients,37 enabling timely TKI resistance management via third-generation TKI escalation;38 ③ reduced radiation necrosis incidence with TKI combination therapy despite EGFR-mutant patients’ heightened neurocognitive vulnerability to whole-brain radiotherapy.39,40 Our findings validate that EGFR status-guided TKI therapy significantly improves objective response rates and prolongs OS, providing critical evidence for establishing a “pathological confirmation-molecular subtyping-targeted priority” comprehensive LCBM management protocol.
In contrast to most previous prediction models based on presumptive radiological diagnosis (without pathological confirmation), this study utilized a rigorously screened cohort of lung cancer brain metastasis (LCBM) patients who underwent surgical resection with pathological confirmation. We systematically characterized their clinical features and identified maximum tumor diameter, number of metastatic lesions, intratumoral hemorrhage, and extracranial lymphatic invasion as independent prognostic determinants. The nomogram model integrating these variables demonstrated excellent performance in predicting 6/12/18-month overall survival (OS) (sensitivity: 82–91%; specificity: 76–88%), validated by ROC curves, calibration curves, and decision curve analysis (DCA). Its core advantage lies in pathological confirmation eliminating imaging misdiagnosis risks, ensuring cohort homogeneity and data authenticity, thereby significantly enhancing model reliability and accuracy while outperforming comparable studies.
Furthermore, a web-based dynamic nomogram (https://huyiba.shinyapps.io/QiuS/) was implemented to optimize clinical translation. By inputting key prognostic parameters, clinicians can obtain quantitative OS predictions.
Limitation
The retrospective design of this study has inherent limitations: 1) Case selection bias (The exclusive focus on post-neurosurgical cohorts limits generalizability to non-operative LCBM populations); 2) Due to the insufficient sample size of the ALK-positive subgroup (n=29), it was not included in the study cohort separately, which may reduce the statistical power and requires subsequent large-sample verification. 3) Temporal therapeutic heterogeneity: Prolonged enrollment periods (2015.01–2021.01) introduced confounding through evolving EGFR-TKI generational use (1st/2nd/3rd gen agents), requiring time-stratified efficacy analyses. 4) Unmeasured prognostic variables: Absence of perioperative volumetric analysis (eg residual tumor burden quantification) and treatment fidelity metrics (eg chemotherapy cycle completion rates) may constrain model precision, (5) Competing risk consideration: While non-cancer deaths were infrequent (11.1%), future studies could incorporate Fine-Gray models for comprehensive risk quantification.
Conclusion
This study systematically analyzed the clinical heterogeneity and molecular regulatory mechanism of LCBM, revealed the anatomical association between bone metastasis and meningeal metastasis and the core role of the EGFR signaling axis in prognostic stratification. Meanwhile, the nomogram model constructed by integrating multiple parameters (maximum cross-sectional area of brain metastasis foci, intratumbral hemorrhage, etc) demonstrated excellent predictive efficacy and could quantitatively guide individualized treatment decisions.
Acknowledgments
This work was supported by Xiamen Cell Therapy Center (Grant No. 3502Z20214001).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Qiu H, Cao S, Xu R. Cancer incidence, mortality, and burden in China: a time-trend analysis and comparison with the United States and United Kingdom based on the global epidemiological data released in 2020. Cancer Commun. 2021;41(10):1037–1048. doi:10.1002/cac2.12197
2. Han B, Zheng R, Zeng H, et al. Cancer incidence and mortality in China, 2022. J Natl Cancer Cent. 2024;4(1):47–53. doi:10.1016/j.jncc.2024.01.006
3. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
4. Suzuki T, Deguchi S, Matsushima K, et al. Brain metastasis of non-small cell lung cancer after disease-free survival of 5 years: case series and comprehensive literature review. World Neurosurg. 2024;186:e353–e359. doi:10.1016/j.wneu.2024.03.139
5. Boire A, Brastianos PK, Garzia L, Valiente M. Brain metastasis. Nat Rev Cancer. 2020;20(1):4–11. doi:10.1038/s41568-019-0220-y
6. Achrol AS, Rennert RC, Anders C, et al. Brain metastases. Nat Rev Dis Primers. 2019;5(1):5. doi:10.1038/s41572-018-0055-y
7. Whiteley AE, Ma D, Wang L, et al. Breast cancer exploits neural signaling pathways for bone-to-meninges metastasis. Science. 2024;384(6702):eadh5548. doi:10.1126/science.adh5548
8. Tang T, Huang X, Zhang G, Hong Z, Bai X, Liang T. Advantages of targeting the tumor immune microenvironment over blocking immune checkpoint in cancer immunotherapy. Signal Transduct Target Ther. 2021;6(1):72. doi:10.1038/s41392-020-00449-4
9. Chong CR, Jänne PA. The quest to overcome resistance to EGFR-targeted therapies in cancer. Nat Med. 2013;19(11):1389–1400. doi:10.1038/nm.3388
10. Harrison PT, Vyse S, Huang PH. Rare epidermal growth factor receptor (EGFR) mutations in non-small cell lung cancer. Semin Cancer Biol. 2020;61:167–179. doi:10.1016/j.semcancer.2019.09.015
11. Sigismund S, Avanzato D, Lanzetti L. Emerging functions of the EGFR in cancer. Mol Oncol. 2018;12(1):3–20. doi:10.1002/1878-0261.12155
12. Sperduto PW, Mesko S, Li J, et al. Survival in patients with brain metastases: summary report on the updated diagnosis-specific graded prognostic assessment and definition of the eligibility quotient. J Clin Oncol. 2020;38(32):3773–3784. doi:10.1200/JCO.20.01255
13. Oliver DE, Yu HM, Ahmed KA. The lung graded prognostic assessment: continued evolution of brain metastases prognostication. Int J Radiat Oncol Biol Phys. 2022;114(1):75–77. doi:10.1016/j.ijrobp.2022.05.045
14. Chinese Association for Clinical Oncologists, Medical Oncology Branch of Chinese International Exchange and Promotion Association for Medical and Healthcare. [Clinical practice guideline for brain metastases of lung cancer in China (2021 version)]. Zhonghua Zhong Liu Za Zhi. 2021;43(3):269–281. Polish. doi:10.3760/cma.j.cn112152-20210104-00009
15. Lamba N, Wen PY, Aizer AA. Epidemiology of brain metastases and leptomeningeal disease. Neuro Oncol. 2021;23(9):1447–1456. doi:10.1093/neuonc/noab101
16. Ozcan G, Singh M, Vredenburgh JJ. Leptomeningeal metastasis from non-small cell lung cancer and current landscape of treatments. Clin Cancer Res. 2023;29(1):11–29. doi:10.1158/1078-0432.CCR-22-1585
17. Cheng H, Perez-Soler R. Leptomeningeal metastases in non-small-cell lung cancer. Lancet Oncol. 2018;19(1):e43–e55. doi:10.1016/S1470-2045(17)30689-7
18. Zheng MM, Tu HY, Yang JJ, et al. Clinical outcomes of non-small cell lung cancer patients with leptomeningeal metastases after immune checkpoint inhibitor treatments. Eur J Cancer. 2021;150:23–30. doi:10.1016/j.ejca.2021.03.037
19. Nanjo S, Hata A, Okuda C, et al. Standard-dose osimertinib for refractory leptomeningeal metastases in T790M-positive EGFR-mutant non-small cell lung cancer. Br J Cancer. 2018;118(1):32–37. doi:10.1038/bjc.2017.394
20. Le Rhun E, Preusser M, van den Bent M, Andratschke N, Weller M. How we treat patients with leptomeningeal metastases. ESMO Open. 2019;4(Suppl 2):e000507. doi:10.1136/esmoopen-2019-000507
21. Pinho-Ribeiro FA, Deng L, Neel DV, et al. Bacteria hijack a meningeal neuroimmune axis to facilitate brain invasion. Nature. 2023;615(7952):472–481. doi:10.1038/s41586-023-05753-x
22. Kurokawa R, Kurokawa M, Isshiki S, et al. Dural and leptomeningeal diseases: anatomy, causes, and neuroimaging findings. Radiographics. 2023;43(9):e230039. doi:10.1148/rg.230039
23. Chiang CL, Yang HC, Liao YT, et al. Treatment and survival of patients with small cell lung cancer and brain metastasis. J Neurooncol. 2023;165(2):343–351. doi:10.1007/s11060-023-04512-2
24. Stokes M, Berfeld N, Gayle A, Descoteaux A, Rohrmoser O, Franks A. A systematic literature review of real-world treatment outcomes of small cell lung cancer. Medicine. 2022;101(26):e29783. doi:10.1097/MD.0000000000029783
25. Semenova EA, Nagel R, Berns A. Origins, genetic landscape, and emerging therapies of small cell lung cancer. Genes Dev. 2015;29(14):1447–1462. doi:10.1101/gad.263145.115
26. Zhu Y, Cui Y, Zheng X, Zhao Y, Sun G. Small-cell lung cancer brain metastasis: from molecular mechanisms to diagnosis and treatment. Biochim Biophys Acta Mol Basis Dis. 2022;1868(12):166557. doi:10.1016/j.bbadis.2022.166557
27. Louarn N, Dauta A, Lechapt-Zalcman E, Kauv P, Itti E. Meningeal metastasis relapse with focal involvement of cranial bone flap: a case resolved by 18F-DOPA PET/MRI. Clin Nucl Med. 2019;44(4):e315–e317. doi:10.1097/RLU.0000000000002492
28. Hong YW, Lin JD, Yu MC, Hsu CC, Lin YS. Outcomes and prognostic factors in thyroid cancer patients with cranial metastases: a retrospective cohort study of 4,683 patients. Int J Surg. 2018;55:182–187. doi:10.1016/j.ijsu.2018.06.001
29. Suh JH, Kotecha R, Chao ST, Ahluwalia MS, Sahgal A, Chang EL. Current approaches to the management of brain metastases. Nat Rev Clin Oncol. 2020;17(5):279–299. doi:10.1038/s41571-019-0320-3
30. Nie Y, Ying B, Lu Z, Sun T, Sun G. Predicting survival and prognosis of postoperative breast cancer brain metastasis: a population-based retrospective analysis. Chin Med J. 2023;136(14):1699–1707. doi:10.1097/CM9.0000000000002674
31. Wang Y, Xu H, Sa Q, et al. Development of graded prognostic assessment for breast Cancer brain metastasis incorporating extracranial metastatic features: a retrospective analysis of 284 patients. BMC Cancer. 2024;24(1):1262. doi:10.1186/s12885-024-12983-3
32. Karimi E, Yu MW, Maritan SM, et al. Single-cell spatial immune landscapes of primary and metastatic brain tumours. Nature. 2023;614(7948):555–563. doi:10.1038/s41586-022-05680-3
33. Vogelbaum MA, Brown PD, Messersmith H, et al. Treatment for Brain Metastases: ASCO-SNO-ASTRO Guideline. J Clin Oncol. 2022;40(5):492–516. doi:10.1200/JCO.21.02314
34. Liu Y, Liu J, Wu X, Jiang E. Risk factors for central nervous system infections after craniotomy. J Multidiscip Healthc. 2024;17:3637–3648. doi:10.2147/JMDH.S476125
35. Colclough N, Chen K, Johnström P, et al. Preclinical comparison of the blood-brain barrier permeability of osimertinib with other EGFR TKIs. Clin Cancer Res. 2021;27(1):189–201. doi:10.1158/1078-0432.CCR-19-1871
36. Ballard P, Yates JW, Yang Z, et al. Preclinical comparison of osimertinib with other EGFR-TKIs in EGFR-mutant NSCLC brain metastases models, and early evidence of clinical brain metastases activity. Clin Cancer Res. 2016;22(20):5130–5140. doi:10.1158/1078-0432.CCR-16-0399
37. Yun CH, Mengwasser KE, Toms AV, et al. The T790M mutation in EGFR kinase causes drug resistance by increasing the affinity for ATP. Proc Natl Acad Sci U S A. 2008;105(6):2070–2075. doi:10.1073/pnas.0709662105
38. Remon J, Steuer CE, Ramalingam SS, Felip E. Osimertinib and other third-generation EGFR TKI in EGFR-mutant NSCLC patients. Ann Oncol. 2018;29(suppl_1):i20–i27. doi:10.1093/annonc/mdx704
39. O’Kane GM, Su J, Tse BC, et al. The impact of brain metastases and associated neurocognitive aspects on health utility scores in EGFR mutated and ALK rearranged NSCLC: a real world evidence analysis. Oncologist. 2019;24(7):e501–e509. doi:10.1634/theoncologist.2018-0544
40. Wrona A, Dziadziuszko R, Jassem J. Management of brain metastases in non-small cell lung cancer in the era of tyrosine kinase inhibitors. Cancer Treat Rev. 2018;71:59–67. doi:10.1016/j.ctrv.2018.10.011
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Evaluation of Lactate Dehydrogenase and Alkaline Phosphatase as Predictive Biomarkers in the Prognosis of Hepatocellular Carcinoma and Development of a New Nomogram
Su K, Huang W, Li X, Xu K, Gu T, Liu Y, Song J, Qian K, Xu Y, Zeng H, Yang Y, Guo L, Han Y
Journal of Hepatocellular Carcinoma 2023, 10:69-79
Published Date: 14 January 2023
Prognostic Value of Body Composition and Systemic Inflammatory Markers in Patients with Locally Advanced Cervical Cancer Following Chemoradiotherapy
Guo H, Feng S, Li Z, Yin Y, Lin X, Yuan L, Sheng X, Li D
Journal of Inflammation Research 2023, 16:5145-5156
Published Date: 10 November 2023
Clinical Implications of Naples Prognostic Score for Patients with Resected Cholangiocarcinoma: A Real-World Experience
Xu B, Zhu J, Wang R, Pang X, Wang X, Lian J, Lu H
Journal of Inflammation Research 2024, 17:655-667
Published Date: 2 February 2024
A Nomogram Model Based on the Inflammation-Immunity-Nutrition Score (IINS) and Classic Clinical Indicators for Predicting Prognosis in Extranodal Natural Killer/T-Cell Lymphoma
He Y, Luo Z, Chen H, Ping L, Huang C, Gao Y, Huang H
Journal of Inflammation Research 2024, 17:2089-2102
Published Date: 4 April 2024
A Novel Inflammation-Marker-Based Prognostic Model for Advanced Pulmonary Lymphoepithelioma-Like Carcinoma
Chen X, Liu T, Mo S, Yang Y, Chen X, Hong S, Zhou T, Chen G, Zhang Y, Ma Y, Ma Y, Zhang L, Zhao Y
Journal of Inflammation Research 2025, 18:2433-2445
Published Date: 20 February 2025