")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 18
Minimal Effects of Cariprazine on Prolactin Levels in Bipolar Disorder and Schizophrenia
Authors Culpepper L , Vieta E , Kelly DL, Patel MD, Szatmári B, Hankinson A, Earley WR
Received 13 November 2021
Accepted for publication 12 April 2022
Published 12 May 2022 Volume 2022:18 Pages 995—1011
DOI https://doi.org/10.2147/NDT.S348143
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Roger Pinder
Larry Culpepper,1 Eduard Vieta,2 Deanna L Kelly,3 Mehul D Patel,4 Balázs Szatmári,5 Arlene Hankinson,4 Willie R Earley4
1Boston University School of Medicine, Boston, MA, USA; 2Hospital Clinic, Institute of Neuroscience, University of Barcelona, IDIBAPS, CIBERSAM, Barcelona, Catalonia, Spain; 3Maryland Psychiatric Research Center, University of Maryland School of Medicine, Baltimore, MD, USA; 4AbbVie, Madison, NJ, USA; 5Gedeon Richter Plc., Budapest, Hungary
Correspondence: Larry Culpepper, Boston University School of Medicine, 90 Sylvia Lane, Westport, MA, 02790-1406, USA, Tel +1 617 414-6225, Email [email protected]
Background: Many medications used to treat schizophrenia and bipolar I disorder are linked to hyperprolactinemia. The effects of cariprazine, a dopamine D3/D2 receptor partial agonist, on prolactin levels in patients with schizophrenia or bipolar I disorder were evaluated.
Methods: Effects on prolactin were evaluated using pooled data from randomized, double-blind, placebo-controlled studies in patients with schizophrenia (4 studies; 6-week duration; cariprazine 1.5– 3 mg/d, 4.5– 6 mg/d, and 9– 12 mg/d), bipolar mania (3 studies; 3-week duration; cariprazine 3– 6 and 9– 12 mg/d), and bipolar depression (3 studies; 6- to 8-week duration; cariprazine 1.5 and 3 mg/d). Long-term effects were analyzed using open-label studies in patients with schizophrenia (2 studies; 48-week duration) and patients with bipolar mania (1 study; 16-week duration). Change in prolactin levels (ng/mL) from baseline to study endpoint was evaluated in subsets of sex and prior medication use.
Results: In patients with schizophrenia (male, n = 1377; female, n = 558), median prolactin changes were − 1.2 for males and − 7.4 for females on placebo, and ranged from − 4.2 to − 3.6 for males and − 12.4 to +0.2 for females in the cariprazine-treatment groups. In patients with bipolar mania (male, n = 570; female, n = 395), median prolactin changes were − 0.2 for males and − 1.1 for females on placebo and ranged from − 2.1 to − 3.0 for males and 0 to +1.8 for females in the cariprazine-treatment groups. Median decreases were also seen in the long-term studies of schizophrenia (range, − 14.6 to − 2.0) and bipolar mania (range, − 0.8 to +1.9). In patients with bipolar depression (male, n = 485; female, n = 780), median prolactin changes were +0.3 for males and +0.7 for females on placebo and ranged from +0.4 to +0.5 for males and +3.0 to +3.1 for females in the cariprazine-treatment groups.
Conclusion: Treatment with cariprazine for schizophrenia or bipolar I disorder was associated with minimal effects on prolactin levels.
Keywords: dopamine, serotonin, mania, depression, prolactin
Introduction
Schizophrenia and bipolar disorder are severe, chronic, and heterogeneous disorders that impact the health, social, and economic well-being of patients, families, caregivers, and society. Pharmacotherapy can treat and manage these disorders; however, many drugs used in the treatment of schizophrenia and bipolar disorder act as antagonists at dopamine D2 receptors, a mechanism that has been linked to hyperprolactinemia (elevated prolactin levels).1,2
Prolactin is a peptide hormone secreted by the pituitary gland based on a circadian pattern (eg, prolactin levels peak overnight and are approximately 1.5- to 2-fold higher than those during the day).3 The secretion of prolactin is regulated through dopaminergic transmission, as stimulation of dopamine D2 receptors on lactotroph cells inhibits gene transcription, synthesis, and release of prolactin and lactotroph proliferation.4 In healthy adults, prolactin levels are generally less than 25 ng/mL;5 however, there is evidence that normal prolactin levels in men are likely lower (approximately 20 ng/mL),6 which may be due to the differences in physiology between males and females. In females, the main function of prolactin is the induction of lactation and maintenance of breast milk production; prolactin also plays a role in breast enlargement during pregnancy, inhibition of hypothalamic gonadotrophin-releasing hormone (GnRH), and maintenance of ovarian function and progesterone secretion. Prolactin is naturally elevated in pregnant and lactating women, where levels can increase up to 10- to 20-fold compared with normal levels.7 In males, the biological role of prolactin is limited; its effects are indirectly related to its regulation of GnRH, which in turn affects spermatogenesis and testosterone levels.8 Similarly, in developing adolescents, prolactin can indirectly affect sexual development. As such, prolactin at biological concentrations plays an important role in human physiology and accumulating evidence suggests that it plays a role in modulating the immune system.9
Medication-induced hyperprolactinemia has been estimated to affect up to 70% of patients on pharmacotherapy for schizophrenia or bipolar disorder, although to varying degrees of severity.4,10,11 Prevalence of hyperprolactinemia in an unselected, normal adult population is believed to be low, at around 0.4%;8 further, unmedicated patients with schizophrenia are generally found to have normal prolactin levels.1 Rates and degrees of prolactin elevation differ widely between the dopamine and serotonin receptor modulators (ie, atypical antipsychotics) used to treat schizophrenia and bipolar disorder, and as a class, these drugs almost all cause prolactin elevation, though many newer agents elevate prolactin to a lesser extent.4 For example, risperidone, paliperidone (primary active metabolite of risperidone), and amisulpride are also known to be “prolactin-elevating”, while aripiprazole, brexpiprazole, cariprazine, and quetiapine are believed to be “prolactin-sparing” or pose little to no risk of hyperprolactinemia.12 Others, such as asenapine, clozapine, iloperidone, lurasidone, olanzapine, and ziprasidone, are believed to pose some risk but do not elevate prolactin to levels as high as those induced by risperidone and certain other drugs. While there is no algorithm that can predict if a certain patient will develop hyperprolactinemia, certain risk factors have been identified, such as adolescence, high-dose treatment with dopamine D2 receptor antagonists, specific dopamine D2 receptor gene variants, female sex, and the reproductive age of females.4,10,13,14
Elevated levels of prolactin can occur within hours after oral administration of dopamine D2 receptor antagonists.15 Sexual and reproductive side effects of hyperprolactinemia associated with dopamine D2 receptor antagonists can lead to infertility, menstrual irregularities (eg, oligomenorrhea, amenorrhea), galactorrhea, and vaginal dryness in women and decreased libido, impotence, infertility, gynecomastia, and erectile dysfunction in men,1 although symptoms in men are often more subtle.8 In addition, significant bone loss, likely as a consequence of changes in estrogen in females and testosterone levels in males, can occur.1,8 Normal development in adolescents can also be affected as elevated prolactin levels can delay puberty in addition to the above side effects.16 These adverse events (AEs) can lead to treatment nonadherence, and this is an important consideration because all-cause nonadherence or partial adherence rates have been reported to be as high as 50% in patients with schizophrenia,17,18 and up to 60% in patients with bipolar disorder.19 These side effects are very undesirable, and drug-induced hyperprolactinemia is mitigated by either reducing the dose, which can reduce efficacy, or adding or switching to a prolactin-sparing drug.20 A few studies have reported on the reduction of elevated prolactin levels or reversal of hyperprolactinemia-related side effects after switching to medications not known to elevate prolactin levels.21,22 Furthermore, one study reported that the adjunctive use of aripiprazole was associated with a decrease in prolactin levels to the normal range and a reduction in prolactin-related adverse effects in women with psychosis. These studies underscore the need for prolactin-neutral pharmacotherapy (ie, medications that result in prolactin levels within the normal range).
Cariprazine, an oral dopamine D3-preferring D3/D2 receptor partial agonist and serotonin 5-HT1A receptor partial agonist, is approved for the treatment of adults with schizophrenia (1.5–6 mg/d) and manic/mixed (3–6 mg/d) or depressive episodes (1.5–3 mg/d) associated with bipolar I disorder. The objective of this pooled, post hoc study was to evaluate the effect of cariprazine on prolactin levels by sex and prior medication status in patients with schizophrenia or bipolar I disorder.
Methods
This post hoc study investigated the short- and long-term effects of cariprazine on prolactin levels in patients with schizophrenia or bipolar I disorder. Phase II/III studies from the clinical development program of cariprazine for schizophrenia, bipolar mania, and bipolar depression were included in the analysis. All participants provided written informed consent after receiving a complete description of the studies. All component studies were conducted in compliance with the International Conference on Harmonisation Guidances on General Considerations for Clinical Trials and Good Clinical Practice, and the Declaration of Helsinki. These studies were also approved by institutional review boards or ethics committees, and government agencies. Since our study is a pooled analysis of data from previously published studies, additional ethical approval was not required.
Study Designs
Schizophrenia
Detailed methods of studies in patients with schizophrenia have been previously published; the included studies were as follows: 4 phase II/III randomized, double-blind, placebo-controlled studies (RGH-MD-03, −04, −05, and −16; Supporting Information Table 1),23–26 2 long-term (48-week), open-label extension studies (RGH-MD-11 and MD-17),27,28 and 1 relapse prevention study (RGH-MD-06).29,30 The treatment period in the 4 acute studies was 6 weeks. In the long-term studies (RGH-MD-11, −17, and −06), the length of cariprazine treatment was substantial (Supporting Information Table 2). For RGH-MD-11 and −17, some of the patients were on cariprazine for over a year (up to 54 weeks of treatment) since the lead-in studies (RGH-MD-04, −05, and −16) had 6 weeks of treatment. For RGH-MD-06, patients were first stabilized on open-label cariprazine treatment for up to 20 weeks, and if patients met stabilization criteria, then patients were randomized to either continue cariprazine treatment or switched to placebo for up to an additional 72 weeks of double-blind treatment. All of these studies required patients to discontinue previous medications for schizophrenia (or other psychiatric disorders) and had a washout/screening period of up to 7 days. This is important to note as some patients were receiving prolactin-elevating medications prior to study enrollment; however, the effects of these drugs are likely short term as most of the common oral prolactin-elevating medications (eg, risperidone, paliperidone) have elimination half-lives that are less than 24 hours.
Bipolar Mania
Detailed methods of studies in patients with bipolar mania have been previously published; the included studies were as follows: 3 phase II/III randomized, double-blind, placebo-controlled, 3-week studies (RGH-MD-31, −32, and −33; Supporting Information Table 1)31–33 and 1 long-term safety study (RGH-MD-36)34 where patients were on open-label cariprazine treatment for a maximum of 16 weeks (Supporting Information Table 2). Similar to the schizophrenia studies, all bipolar mania studies required patients to discontinue previous medications for bipolar disorder (or other psychiatric disorders) and had a washout/screening period of up to 4 to 7 days.
Bipolar Depression
Detailed methods of the 3 phase II/III randomized, double-blind, placebo-controlled studies in patients with bipolar depression (RGH-MD-53, −54, and −56; Supporting Information Table 1) have been previously published;35–37 all 3 studies had a pre-specified endpoint at 6 weeks, although RGH-MD-53 and −54 had 6 weeks of treatment and RGH-MD-56 had 8 weeks of treatment. A smaller, Phase II cariprazine study of patients with bipolar depression (RGH-MD-52) was not included in this bipolar depression analysis due to the inclusion of patients with bipolar II disorder in addition to those with bipolar I disorder. In contrast, studies RGH-MD-53, −54, and −56 enrolled patients with bipolar I disorder only. Data from the 0.75 mg/d dose group, present only in RGH-MD-56, was excluded. Like the schizophrenia and bipolar mania studies, all bipolar depression studies also required patients to discontinue previous medication for bipolar disorder (or other psychiatric disorders) and had a washout/screening period of 7 to 14 days.
Post Hoc Analyses
Data were pooled for studies within each patient population (schizophrenia, bipolar mania, and bipolar depression). Pooling within each indication was done to provide a more stable and representative estimate for each patient population (and for subgroups) than individual studies. For the schizophrenia and bipolar mania analyses, in order to assess the effects of cariprazine dose, groups were analyzed by modal daily dose (most frequent dose) due to the inclusion of flexible-dose studies; for bipolar depression, the pooled groups were based on randomized dose since all 3 studies had fixed dosing. The treatment groups were placebo, cariprazine 1.5–3 mg/d, 4.5–6 mg/d, or 9–12 mg/d, risperidone 4 mg/d, or aripiprazole 10 mg/d for the schizophrenia studies; placebo, cariprazine 3–6 mg/d, or cariprazine 9–12 mg/d for the bipolar mania studies; and placebo, cariprazine 1.5, or cariprazine 3 mg/d for the bipolar depression studies. In addition to the pooling of data within each indication, studies were also pooled across all 3 indications (combined groups from the schizophrenia, bipolar mania, and/or bipolar depression studies) to provide an overall estimate of prolactin changes for the acute and long-term studies. For these analyses, cariprazine doses were also pooled (1.5–6 [the recommended dose range] and 9–12 mg/d).
Patients included in this analysis were part of the safety population (eg, took at least 1 dose of the study medication) and also had a baseline and a postbaseline prolactin serum value. In all studies, a central laboratory was used to evaluate all serum prolactin samples, which were collected, processed, and stored according to the instructions provided by the laboratory. Further, the normal reference range for each study was determined by the laboratory and presented in Supporting Information Table 1. Samples were obtained at approximately the same time for each patient. Postbaseline prolactin levels were also blinded.
Baseline was defined as the first assessment after the screening/washout period but before initiation of study medication. For the acute studies, descriptive statistics for change in prolactin levels from baseline to endpoint (defined as the last available double-blind assessment) were evaluated and presented as median and mean with standard deviation (SD). Due to differences in physiology, results for male and female patients were analyzed separately. Prolactin levels over time were presented using observed case data; change in prolactin levels from baseline to endpoint (defined as last available assessment) for the open-label studies were also presented as median and mean with SD. Additional analyses were conducted to determine the percentage of patients in each treatment group who shifted from having prolactin levels in the normal range at baseline to greater than 2 times (2X) the upper limit of normal (ULN) and 4 times (4X) ULN at endpoint. Additionally, the percentage of patients that had prolactin levels in the >ULN range at baseline but shifted to the normal range at endpoint were also tabulated. The cutoff points of 2X and 4X ULN, which generally correspond to >50 (moderate hyperprolactinemia) or >100 ng/mL (severe hyperprolactinemia), were used to determine clinical relevance of prolactin elevation.6 Changes in prolactin levels were also evaluated in subgroups based on medication use prior to the start of the study. The 4 prior medication subgroups were based on their prolactin-elevating potential (no prior medications, low risk, moderate risk, and high risk; see footnote in Table 2 for the list of medications).4 Potentially prolactin-related treatment-emergent adverse events (TEAEs) were summarized and analyzed descriptively.
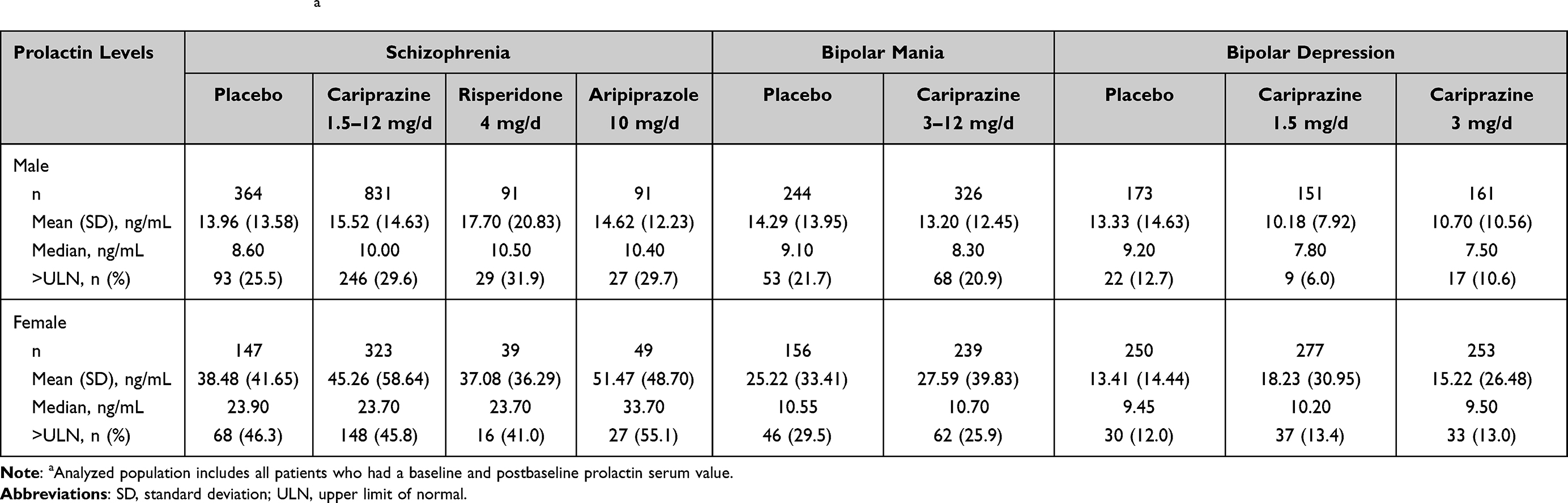 |
Table 1 Prolactin Levels at Baselinea |
Results
Demographic and Baseline Characteristics
Demographic information for the schizophrenia,23–26 bipolar mania,31–33 and bipolar depression35–37 studies has been previously published and is briefly summarized in Supporting Information Table 3. The mean age was approximately 38 years in the schizophrenia studies, 40 years in the bipolar mania studies, and 43 years in the bipolar depression studies. Across all studies, a notable proportion of patients were white (40% in the schizophrenia studies, >45% in the bipolar mania studies, and ~75% in the bipolar depression studies). In the schizophrenia and bipolar mania studies, most patients were male (~72% and 60%, respectively), while the majority were female in the bipolar depression studies (>60%).
Baseline prolactin levels for patients enrolled in the randomized, double-blind, placebo-controlled, short-term studies are summarized in Table 1. Median prolactin levels at baseline were within the normal range (see Supporting Information Table 1), although baseline prolactin levels were above the ULN for at least 10% of patients across all studies (34% of patients with schizophrenia, 24% of patients with bipolar mania, and 12% of patients with bipolar depression).
Prior use of medications for the treatment of schizophrenia or bipolar disorder within 28 days of treatment initiation is presented in Table 2. In the schizophrenia and bipolar mania studies, most patients had some prior medication use compared with no prior medication use. In the bipolar depression studies, most patients did not have prior medication use. Furthermore, the distribution of patients in each prior medication subgroup was similar between treatment groups within each patient population.
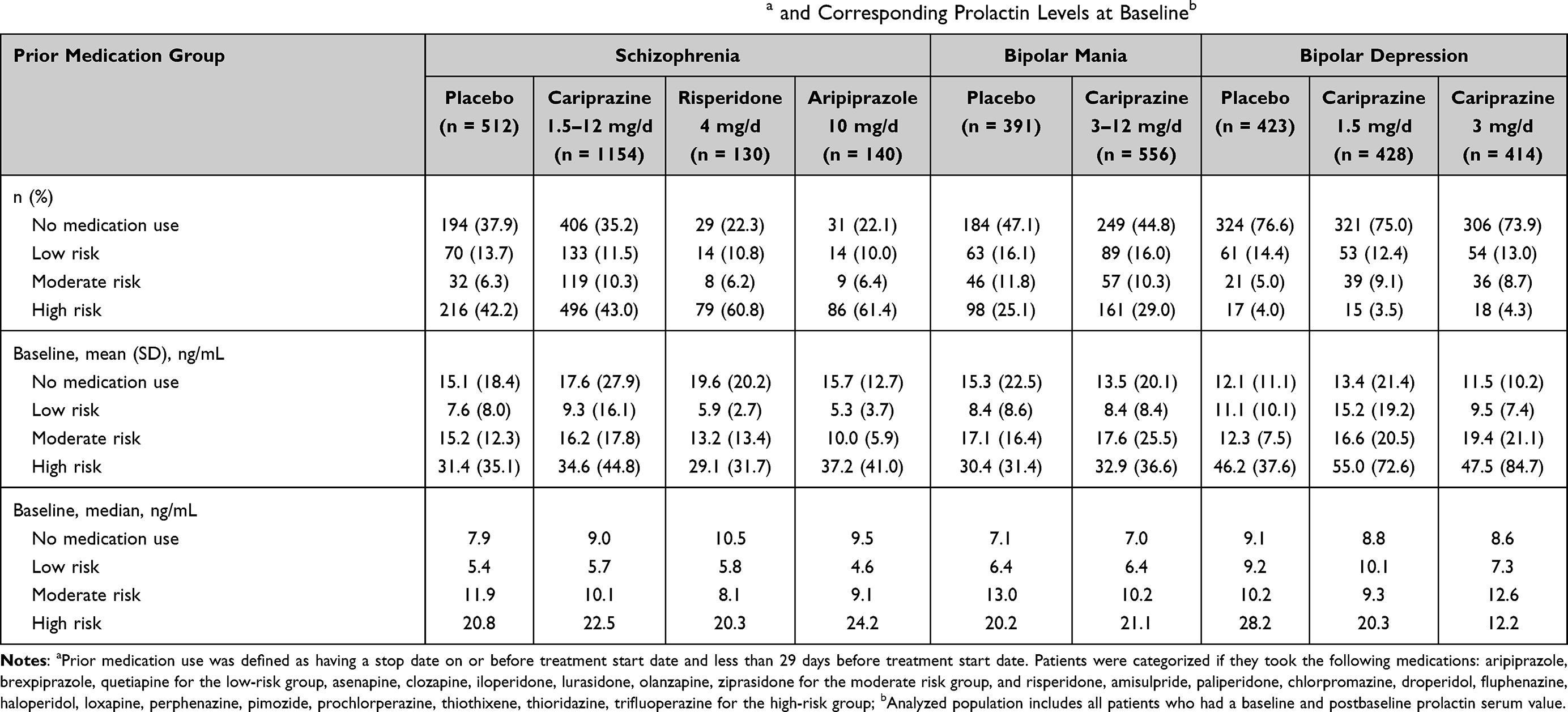 |
Table 2 Number of Patients Available for Analysis in Each Prior Medication Use Groupa and Corresponding Prolactin Levels at Baselineb |
Randomized, Double-Blind, Placebo-Controlled Short-Term Studies
All patients included in the analysis had baseline and endpoint prolactin levels. For the acute studies, a total of 1377 male and 558 female patients with schizophrenia, 570 male and 395 female patients with bipolar mania, and 485 male and 780 female patients with bipolar depression were included in the analysis dataset. In the acute studies of schizophrenia, when considering the total sample of all prior medication groups combined, cariprazine treatment decreased the median prolactin levels to within the normal range in both male and female subgroups, regardless of dose (Figure 1A). In patients with bipolar mania and bipolar depression, median changes in prolactin levels were small in all treatment groups of male and female patients (Figures 1B and 1C). For all acute studies, median prolactin levels in the cariprazine studies fell within the normal range at study endpoint. In the schizophrenia studies, the effects of cariprazine were similar to what was seen in the placebo and aripiprazole groups; in contrast, patients on risperidone saw a marked increase in prolactin levels. Further, median changes in prolactin levels were higher for female compared with male patients; this trend is not as striking in the bipolar mania and bipolar depression studies.
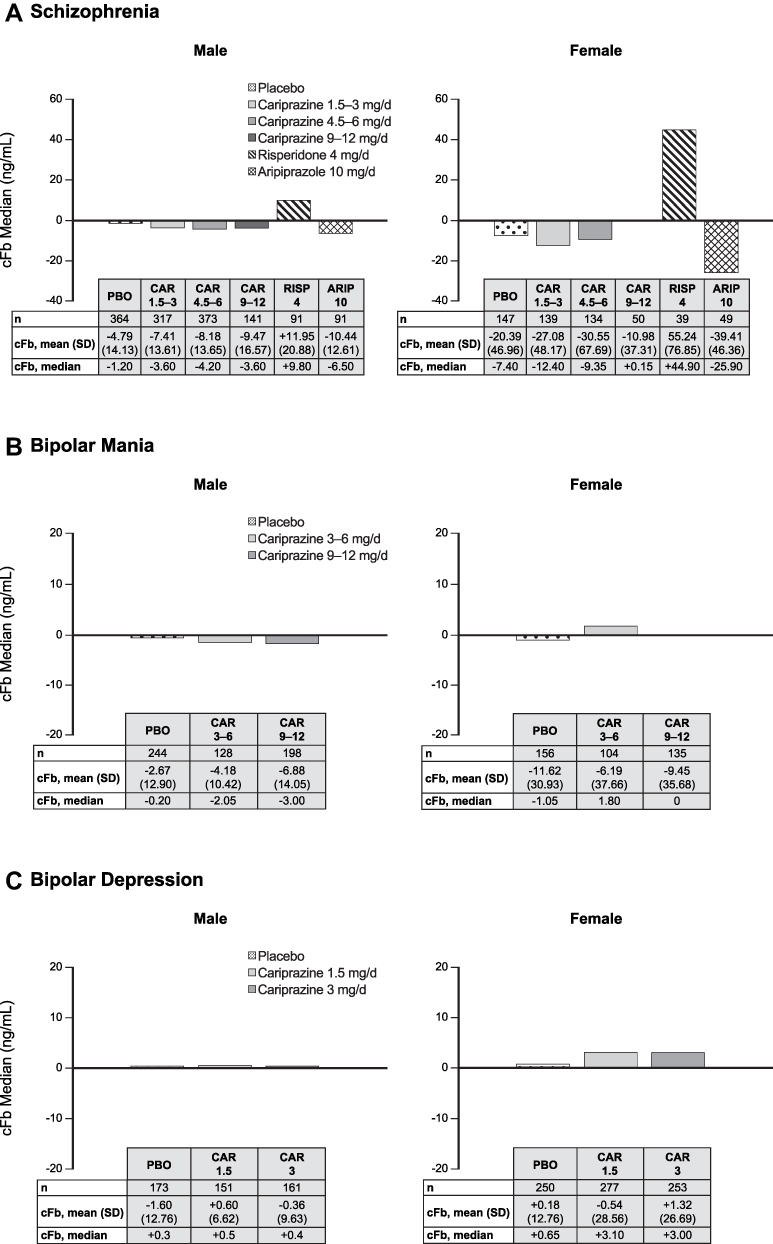 |
Figure 1 Change from baseline prolactin levels in patients with (A) schizophrenia, (B) bipolar mania, or (C) bipolar depression. Abbreviations: ARIP, aripiprazole; CAR, cariprazine; cFb, change from baseline; PBO, placebo; RISP, risperidone; SD, standard deviation. |
When considering the entire pooled population from all of the acute studies of schizophrenia, bipolar mania, and bipolar depression, median changes in prolactin levels from baseline to study endpoint were also minimal, and these changes were similar between the cariprazine (1.5–6 mg/d: median = −0.6; mean = −7.0, SD = 29.9; 9–12 mg/d: median = −2.2; mean = −8.1, SD = 23.3) and placebo groups (median = −0.4; mean = −5.5, SD = 23.0).
Subgroup analysis of patients by prior medication use showed similar patterns to the pooled male and female subgroups (Figure 2). In all 3 patient populations, there were substantial decreases in median prolactin levels in patients who were taking prolactin-elevating medications (high-risk group) prior to initiation of cariprazine treatment, though the difference was less striking in the bipolar depression studies. In the patients who were not in the high-risk group of all 3 patient populations, cariprazine treatment resulted in minimal changes.
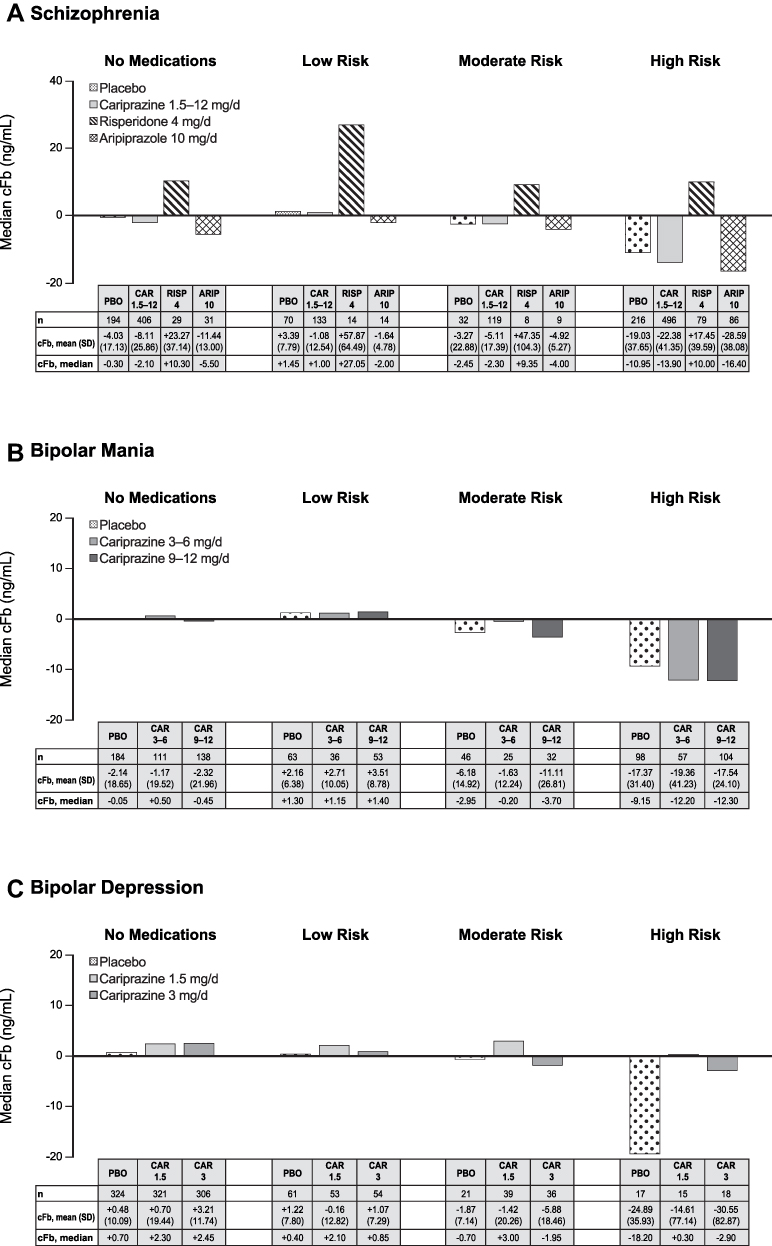 |
Figure 2 Change from baseline prolactin levels grouped by prior medicationa use in patientsb with (A) schizophrenia, (B) bipolar mania, or (C) bipolar depression. aPrior medication use was defined as having a stop date on or before treatment start date and less than 29 days before treatment start date. Patients were categorized if they took the following medications: aripiprazole, brexpiprazole, quetiapine for the low-risk group, asenapine, clozapine, iloperidone, lurasidone, olanzapine, ziprasidone for the moderate risk group, and risperidone, amisulpride, paliperidone, chlorpromazine, droperidol, fluphenazine, haloperidol, loxapine, perphenazine, pimozide, prochlorperazine, thiothixene, thioridazine, trifluoperazine for the high-risk group; bAnalyzed population includes all patients who had a baseline and postbaseline prolactin serum value. Abbreviations: cFb, change from baseline; LS, least squares. |
Across both the schizophrenia and bipolar disorder populations, very few patients on placebo (0–6.3%) or cariprazine (all <3%) shifted from having normal prolactin levels at baseline to levels of >2X or 4X ULN. In contrast, in the risperidone-treatment group, 19.4% of male patients and 60.9% of female patients shifted from normal prolactin levels at baseline to >2X ULN and 30.4% of female patients shifted to levels >4X ULN. Aripiprazole treatment did not lead to any shifts to >2X or >4X ULN. Among patients with elevated prolactin levels (>ULN) at baseline, the majority of patients on cariprazine treatment had their prolactin levels return to normal. In contrast, with risperidone treatment, no female patients and only 13.8% of male patients had prolactin levels return to normal. These results are presented in Supporting Information Tables 4 and 5.
Long-Term Studies
A total of 556 patients from the open-label schizophrenia studies, and a total of 659 patients in the open-label phase and 178 patients in the double-blind phase from the relapse prevention schizophrenia study were included. Based on the open-label studies, the long-term effects of cariprazine on median prolactin levels in patients with schizophrenia were minimal, and there also did not appear to be dose effects on prolactin levels (Figure 3A). There was a slight decrease in median prolactin levels from week 0 to week 24, which may be due to 1 of the 2 studies enrolling new patients, who had recently discontinued from other medications, and both studies enrolling patients from the lead-in studies, one of which had a risperidone-treatment arm.
 |
Figure 3 Time profile of prolactin levels. (A) Schizophrenia: open-label, safety studies (MD-11, −17)a. (B) Bipolar mania: open-label, safety study (MD-36)b.aWeek 48: male, n = 176, female, n = 90; bweek 16: male, n = 75, female, n = 55. Abbreviations: cFb, change from baseline; SD, standard deviation. |
In the relapse prevention study, some patients were on cariprazine treatment (dose range of cariprazine was 3–9 mg/d) for up to 92 weeks; cariprazine resulted in decreased prolactin levels from baseline in the open-label phase and the decreased prolactin levels were maintained during the double-blind treatment period in both the cariprazine and placebo groups. Median prolactin levels at baseline, week 8, and week 20 during the open-label phase were 12.8, 6.3, and 6.3 ng/mL, respectively. At end of double-blind treatment (week 92; placebo, n = 15, cariprazine, n = 19), median prolactin levels were 6.4 ng/mL for the placebo group and 6.3 ng/mL for the cariprazine group; levels were similar at weeks 46 (placebo, n = 40; cariprazine, n = 55), 58 (placebo, n = 30; cariprazine, n = 46), and 74 (placebo, n = 22; cariprazine, n = 34) during the double-blind treatment period (placebo = 6.6, 7.1, 6.0 ng/mL; cariprazine = 7.5, 8.2, 9.7 ng/mL, respectively). In addition, changes from open-label baseline to the end of double-blind treatment in median prolactin levels were similar for both the placebo (−2.1 ng/mL) and cariprazine groups (−1.4 ng/mL).
In the bipolar mania safety study, 228 male and 168 female patients were included. Long-term effects of cariprazine on median prolactin levels in patients with bipolar mania were minimal and did not substantially change over the course of the 16-week cariprazine treatment, and there also did not appear to be overall dose effects (Figure 3B). Since the bipolar mania study enrolled new patients, there was an overall slight decrease in median prolactin levels within 1 week of open-label treatment, which may be due to the recent discontinuation of other medications.
When pooled across the long-term studies in schizophrenia and bipolar mania where all patients received open-label cariprazine treatment, median changes in prolactin levels from baseline to study endpoint were small for the recommended dose range (1.5–6 mg/d: median = −2.2; mean = −11.3, SD = 36.0). Further, higher doses of cariprazine did not lead to larger changes in prolactin levels (9–12 mg/d: median = −1.8; mean = −8.8, SD = 24.6).
Prolactin-Related TEAEs
In the acute schizophrenia, bipolar mania, and bipolar depression studies, potentially prolactin-related TEAEs occurred infrequently in all treatment groups, with no AE > 2% in any cariprazine group (Table 3 for schizophrenia and Table 4 for bipolar disorder). For the schizophrenia and bipolar depression studies, all TEAEs in the cariprazine-treatment groups were mild or moderate in severity. In the bipolar mania studies, there were 2 severe TEAEs (erectile dysfunction = 1; ejaculation disorder = 1); both were also in the 9–12 mg/d cariprazine group, which is outside of the recommended dose range for bipolar mania (3–6 mg/d).
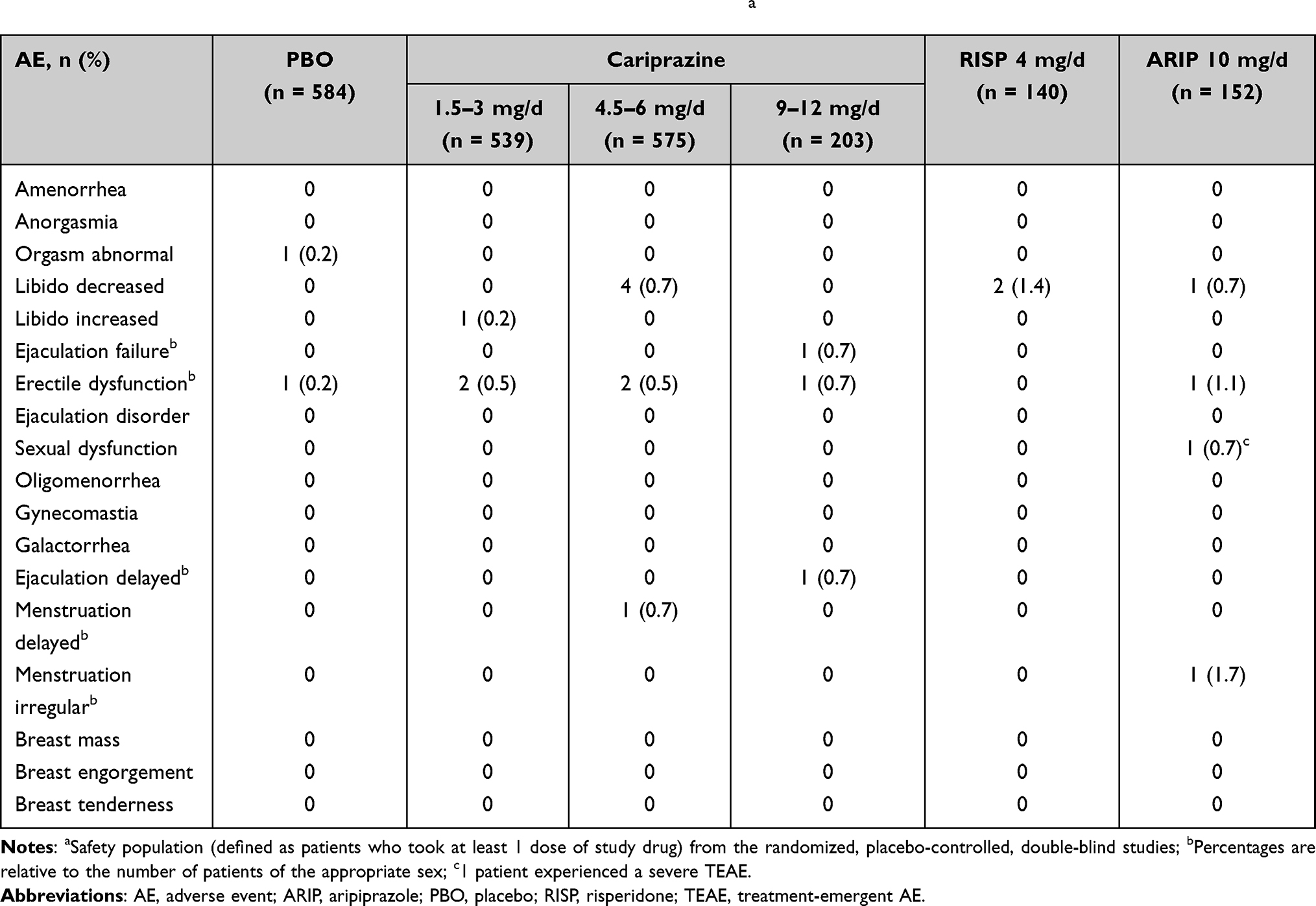 |
Table 3 Potentially Prolactin-Related TEAEs in Patients with Schizophreniaa |
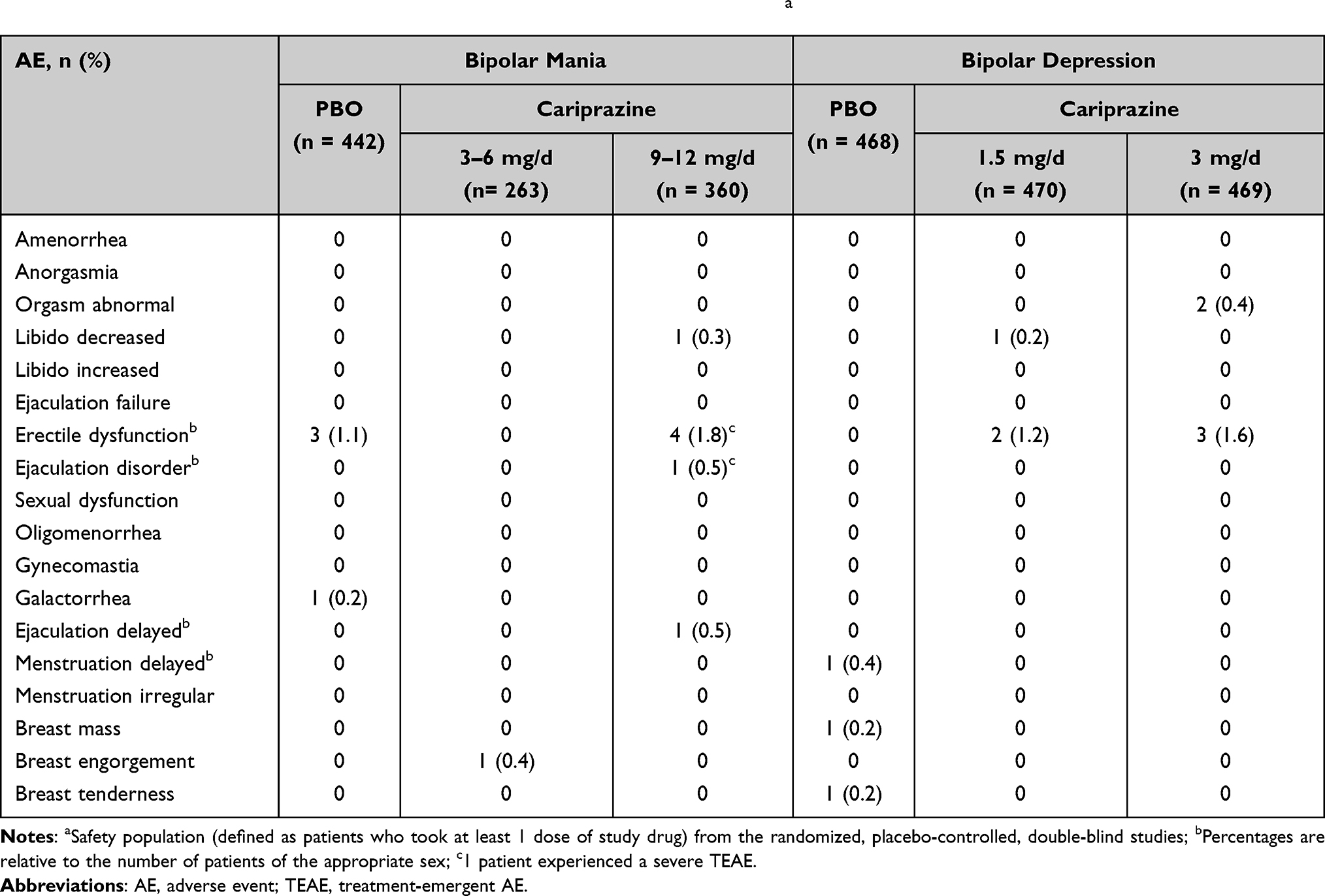 |
Table 4 Potentially Prolactin-Related TEAEs in Patients with Bipolar Disordera |
Discussion
Hyperprolactinemia occurs when prolactin, a hormone involved in sexual and reproductive function, becomes elevated. Drug-induced hyperprolactinemia is a common adverse effect that is associated with medications used to treat schizophrenia and bipolar disorder.38 As many medications that treat schizophrenia and bipolar disorder are known to increase prolactin levels, there is an unmet need for effective prolactin-neutral medications. The current study assessed the effects of cariprazine, a dopamine D3-preferring D3/D2 receptor partial agonist, on prolactin levels in patients with schizophrenia or bipolar I disorder. In patients with schizophrenia, cariprazine treatment was associated with decreases from baseline in prolactin levels. Subgroup analyses suggested that the largest decreases in prolactin following cariprazine treatment were observed in patients who were previously taking medications with a high risk of elevating prolactin, suggesting that cariprazine treatment was associated with normalization of prolactin levels in these patients. Prolactin changes following cariprazine treatment were smaller in patients who received no prior medication or medications with lower risk of elevating prolactin. In general, changes in prolactin were much smaller in patients with bipolar mania and patients with bipolar depression, but trends were similar to those observed in the schizophrenia studies as the largest decreases in prolactin were also observed in patients previously taking medications at high risk of elevating prolactin. There did not appear to be dose-related differences in prolactin changes with respect to cariprazine. Changes in prolactin were generally greater in females than males across all treatment groups; however, this finding is not surprising as prolactin levels are generally higher in females compared with males due to normal physiological differences. In long-term studies, prolactin decreased to normal levels following cariprazine treatment, which was maintained over time for patients with schizophrenia or bipolar mania. In addition, the duration of cariprazine exposure did not seem to affect the prolactin change from baseline, which is supported by the analysis of the acute versus long-term studies pooled across all indications. These findings indicate that there was no overall increase in mean or median prolactin levels as a result of acute or long-term cariprazine treatment. Very few patients on cariprazine treatment experienced potentially prolactin-related sexual and reproductive TEAEs. Furthermore, higher doses of cariprazine (>6 mg/d, above the recommended clinical dose range) did not result in greater incidences of AEs compared to lower doses. These findings suggest that cariprazine may be a prolactin-neutral pharmacotherapy option in patients with schizophrenia, bipolar mania, or bipolar depression.
While it is not exactly clear what drug properties cause hyperprolactinemia, there are mechanisms that have gained traction as potential explanations.4,20,39 One such mechanism is dopamine D2 antagonism. Dopamine exerts an inhibitory action on prolactin secretion; thus, dopaminergic inhibition increases prolactin release, as corroborated by the fact that most medications used to treat schizophrenia and bipolar disorder exhibit antagonism activity at dopamine D2 receptors and are associated with elevations in prolactin. Medication effects on prolactin levels can differ based on mechanism of action, and hyperprolactinemia is generally more likely to be associated with certain potent dopamine D2 receptor antagonists, such as risperidone, than dopamine D2 receptor partial agonists, such as aripiprazole. The prolactin-neutral effects of cariprazine may be due to its pharmacological properties as a partial agonist (and not an antagonist) at dopamine D2 receptors.
The idea that lesser effects are caused by partial agonism versus full antagonism is supported by the results of this study. RGH-MD-16 included a risperidone-treatment arm, and in this study, mean prolactin changes for cariprazine and risperidone trended in different directions,26 indicating that cariprazine does not elevate prolactin levels compared with risperidone, a known prolactin-elevating drug. The different effects of cariprazine and risperidone, in addition to their dopamine receptor pharmacology, may also be due to differences in their ability to penetrate the blood-brain barrier (BBB; eg, drugs that have difficulty crossing the BBB are more likely to elevate prolactin levels). Prolactin secretion is regulated through dopaminergic transmission in the tuberoinfundibular pathway, which connects the pituitary gland (outside of the BBB) to the hypothalamus (inside of BBB, except the median eminence); as such, strong antagonist activity at dopamine D2 receptors at the pituitary gland could increase prolactin secretion. This hypothesis is consistent with data from a recent PET study that found a positive correlation between prolactin serum levels and dopamine D2 receptor occupancy at the pituitary.40 Cariprazine should readily cross the BBB; in a preclinical study, the ratio of brain to plasma cariprazine levels was 7.6, suggesting that over 80% of the drug is in the brain.41 Conversely, risperidone has a lower brain-to-plasma ratio, which may be due to its involvement with P-glycoprotein, an efflux transporter that can limit the access of drugs to the brain.42 Therefore, at therapeutic doses, risperidone and its active metabolite paliperidone (9-OH risperidone) likely accumulate at the pituitary gland, which may explain its propensity to induce hyperprolactinemia. Given that cariprazine is a partial agonist and can readily cross the BBB, there may be advantages for cariprazine over risperidone in treating patients who are at risk of developing hyperprolactinemia.
The hypothesis that partial agonism has lesser effects on prolactin elevation is also supported by results from study RGH-MD-04, which included an aripiprazole-treatment arm. Mean prolactin changes for the cariprazine and aripiprazole groups were similar with the 6 mg/d dose group having near identical changes to that of aripiprazole (cariprazine 3 mg/d = −15.9 ng/mL; cariprazine 6 mg/d = −20.6 ng/mL; aripiprazole = −20.6 ng/mL),24 which supports the lack of prolactin elevation with cariprazine. These results also corroborate a previously published meta-analysis, which found that aripiprazole and cariprazine had smaller increases in prolactin levels versus placebo compared with other medications in patients with schizophrenia.43 The similarities on prolactin between cariprazine and aripiprazole are likely due to neither agent exhibiting potent D2 receptor antagonist activity but instead displaying partial agonist activity at dopamine D2 receptors. Further, brexpiprazole, another dopamine D2 receptor partial agonist, also has minimal effects on prolactin levels in patients with schizophrenia,44 although its effect on prolactin levels was ranked less favorably than aripiprazole and cariprazine.43 Based on this observation, cariprazine appears to have a similar prolactin profile compared to aripiprazole, which has been used to reduce prolactin levels either by switching medication or as an adjunctive treatment.20,45
The effect of cariprazine treatment on median prolactin levels differed between patient populations, with moderate-to-small decreases in prolactin observed in patients with schizophrenia and bipolar mania and small-to-no changes in patients with bipolar depression. In addition, the magnitude of change was 2- to 3-times as large in patients with schizophrenia than in patients with bipolar mania. The most likely contributing factor was that baseline prolactin levels were the highest in patients with schizophrenia, as patients with schizophrenia were more likely to be receiving prolactin-elevating medications prior to study entry than patients with bipolar disorder. As such, patients who were treated with cariprazine had a much more pronounced normalization effect in the schizophrenia studies and, to a lesser extent, in the bipolar mania studies than those in the bipolar depression studies. This observation is supported by the analyses evaluating shifts in prolactin—nearly one third of patients with schizophrenia had elevated prolactin levels at baseline, compared with one quarter for bipolar mania and one eighth for bipolar depression. Regardless of disorder, the majority of patients who had elevated prolactin levels at baseline ended up with levels in the normal range after cariprazine treatment, and the percentage of patients in the placebo and cariprazine groups were also similar, indicating the potential for cariprazine to normalize elevated prolactin levels. Further, of patients who began the study with normal prolactin levels, very few patients exhibited hyperprolactinemia (greater than 2X or 4X ULN) after treatment with cariprazine in the acute studies, suggesting that cariprazine generally does not result in increases in prolactin. The subgroup analyses grouped by prior medication use also showed this normalization effect, as median changes in prolactin levels from baseline were greater in patients who were on prolactin-elevating medications prior to enrollment. This suggests that decreases in prolactin were likely driven by a subgroup of patients who were previously on prolactin-elevating medications, providing further support for cariprazine as a prolactin-neutral option for patients with schizophrenia or bipolar I disorder.
The results of this post hoc study should be interpreted within its limitations. First, the included studies were not designed to prospectively analyze the effects of prolactin as a result of cariprazine treatment. Second, baseline prolactin levels may be confounded by previous medication use, and while the studies had a washout period, the length of which differed between studies, it is possible that some patients had elevated prolactin levels at baseline. We attempted to take this into account by stratifying by prior medication use. Third, the frequency of sampling varied between studies, and serial sampling was not done to gauge whether the changed levels were at steady state or when the elevation (or decrease) occurred. Lastly, sample collection, depending on the time of day samples were taken, could also be a potential limitation of these results as the circadian rhythm of prolactin release may influence prolactin levels.
In post hoc analyses of patients with schizophrenia or bipolar I disorder with a current depressive or manic/mixed episode, median prolactin changes were generally similar for placebo and cariprazine treatment in both male and female subgroups undergoing short-term treatment. Further, the early decreases in prolactin levels due to cariprazine treatment were also maintained long term; median prolactin levels were in the normal range throughout the long-term studies. Sexual and reproductive TEAEs that are potentially related to prolactin occurred infrequently for all treatment groups. These results suggest that cariprazine is a prolactin-neutral agent in male or female patients with schizophrenia or bipolar I disorder and that it is associated with minimal prolactin-related adverse effects. As such, cariprazine may be a useful treatment choice for patients with schizophrenia or bipolar I disorder who are concerned about elevated prolactin levels or sexual or reproductive side effects.
Abbreviations
5-HT, 5-hydroxytryptamine; AEs, adverse events; ARIP, aripiprazole; BBB, blood-brain barrier; BMI, body mass index; CAR, cariprazine; cFb, change from baseline; GnRH, gonadotrophin-releasing hormone; LS, least squares; PBO, placebo; PET, positron emission tomography; RISP, risperidone; SD, standard deviation; TEAEs, treatment-emergent adverse events; ULN, upper limit of normal.
Clinical Trials Registration
NCT00404573, NCT01104766, NCT01104779, NCT00694707, NCT01104792, NCT00839852, NCT01412060, NCT00488618, NCT01058096, NCT01058668, NCT01059539, NCT02670538. NCT02670551, NCT01396447
Data Sharing Statement
The datasets generated for this article are available on request to the corresponding author.
Ethics Approval and Consent to Participate
All studies were conducted in compliance with the International Conference on Harmonisation Guidances on General Considerations for Clinical Trials and Good Clinical Practice, and the Declaration of Helsinki. These studies were also approved by institutional review boards or ethics committees and government agencies. In addition, all participants provided written informed consent after receiving a complete description of the studies.
Acknowledgments
Writing and editorial assistance were provided by Katharine Fang, PhD, of Prescott Medical Communications Group (Chicago, IL), which was funded by AbbVie. The authors would like to thank Thais Moreira, PhD, PharmD, for her contributions to this analysis. Statistical analysis support was provided by Qing Dong and Lei Luo, of AbbVie (Madison, NJ). All authors met the ICMJE authorship criteria. Neither honoraria nor payments were made for authorship.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval for the version to be published, and agree to be accountable for all aspects of the work.
Funding
This study was funded by AbbVie, Inc.
Disclosure
L. Culpepper has served as an advisor or consultant for Acadia Pharmaceuticals, Allergan Pharmaceuticals, Eisai Pharmaceuticals, Merck & Co., Takeda, Supernus Pharmaceuticals; owns stock in M-3 Information, LLC, and has received royalties from UpToDate and Oxford University Press in addition to receiving payment from Physicians Postgraduate Press as Editor-in-Chief of the Primary Care Companion for CNS Diseases. E. Vieta has received grants and served as consultant, advisor, or speaker for: AB Biotics, Abbott, Alexza, Almirall, Allergan, Angelini, AstraZeneca, Bristol Myers Squibb, Casen Recordati, Cephalon, Dainippon Sumitomo Pharma, Elan, Eli Lilly, Ferrer, Forest Research Institute, Galenica, Gedeon Richter, GH Research, GlaxoSmithKline, Janssen Cilag, Jazz, Johnson and Johnson, Lundbeck, Merck, Novartis, Organon, Otsuka, Pfizer, Raffo, Roche, Sage, Sanofi Aventis, Servier, Schering Plough, Shire, the Spanish Ministry of Science and Innovation, the Seventh European Framework Programme, the Stanley Medical Research Institute, Sunovion, Takeda, Teva, United BioSource Corporation, and Wyeth. D.L. Kelly serves as a consultant to Alkermes, Sunovion, and Lyndra Therapeutics. B. Szatmári is an employee of Gedeon Richter Plc. and has a patent EP 2925324 B1 issued to Gedeon Richter Plc. A. Hankinson and W.R. Earley were employees of AbbVie at the time of the study and may hold stock. W.R. Earley is also a shareholder of AstraZeneca and Eli Lilly. M.D. Patel was an employee of AbbVie at the time of the study and may hold stock. The authors report no other conflicts of interest in this work.
References
1. Haddad PM, Wieck A. Antipsychotic-induced hyperprolactinaemia: mechanisms, clinical features and management. Drugs. 2004;64(20):2291–2314. doi:10.2165/00003495-200464200-00003
2. Goodnick PJ, Rodriguez L, Santana O. Antipsychotics: impact on prolactin levels. Expert Opin Pharmacother. 2002;3(10):1381–1391. doi:10.1517/14656566.3.10.1381
3. Egli M, Leeners B, Kruger TH. Prolactin secretion patterns: basic mechanisms and clinical implications for reproduction. Reproduction. 2010;140(5):643–654. doi:10.1530/REP-10-0033
4. Peuskens J, Pani L, Detraux J, et al. The effects of novel and newly approved antipsychotics on serum prolactin levels: a comprehensive review. CNS Drugs. 2014;28(5):421–453. doi:10.1007/s40263-014-0157-3
5. Kelly DL, Wehring HJ, Earl AK, et al. Treating symptomatic hyperprolactinemia in women with schizophrenia: presentation of the ongoing DAAMSEL clinical trial (Dopamine partial Agonist, Aripiprazole, for the Management of Symptomatic ELevated prolactin). BMC Psychiatry. 2013;13(1):214. doi:10.1186/1471-244X-13-214
6. Montejo AL, Arango C, Bernardo M, et al. Multidisciplinary consensus on the therapeutic recommendations for iatrogenic hyperprolactinemia secondary to antipsychotics. Front Neuroendocrinol. 2017;45:25–34. doi:10.1016/j.yfrne.2017.02.003
7. Hill PD, Chatterton RT
8. Saleem M, Martin H, Coates P. Prolactin biology and laboratory measurement: an update on physiology and current analytical issues. Clin Biochem Rev. 2018;39(1):3–16.
9. Freeman ME, Kanyicska B, Lerant A, et al. Prolactin: structure, function, and regulation of secretion. Physiol Rev. 2000;80(4):1523–1631. doi:10.1152/physrev.2000.80.4.1523
10. Ajmal A, Joffe H, Nachtigall LB. Psychotropic-induced hyperprolactinemia: a clinical review. Psychosomatics. 2014;55(1):29–36. doi:10.1016/j.psym.2013.08.008
11. Montgomery J, Winterbottom E, Jessani M, et al. Prevalence of hyperprolactinemia in schizophrenia: association with typical and atypical antipsychotic treatment. J Clin Psychiatry. 2004;65(11):1491–1498. doi:10.4088/JCP.v65n1108
12. Solmi M, Murru A, Pacchiarotti I, et al. Safety, tolerability, and risks associated with first- and second-generation antipsychotics: a state-of-the-art clinical review. Ther Clin Risk Manag. 2017;13:757–777. doi:10.2147/TCRM.S117321
13. Bostwick JR, Guthrie SK, Ellingrod VL. Antipsychotic-induced hyperprolactinemia. Pharmacotherapy. 2009;29(1):64–73. doi:10.1592/phco.29.1.64
14. Calarge CA, Ellingrod VL, Acion L, et al. Variants of the dopamine D2 receptor gene and risperidone-induced hyperprolactinemia in children and adolescents. Pharmacogenet Genomics. 2009;19(5):373–382. doi:10.1097/FPC.0b013e328329a60f
15. Turrone P, Kapur S, Seeman MV, et al. Elevation of prolactin levels by atypical antipsychotics. Am J Psychiatry. 2002;159(1):133–135. doi:10.1176/appi.ajp.159.1.133
16. Matalliotakis M, Koliarakis I, Matalliotaki C, et al. Clinical manifestations, evaluation and management of hyperprolactinemia in adolescent and young girls: a brief review. Acta Biomed. 2019;90(1):149–157. doi:10.23750/abm.v90i1.8142
17. Dolder CR, Lacro JP, Dunn LB, et al. Antipsychotic medication adherence: is there a difference between typical and atypical agents? Am J Psychiatry. 2002;159(1):103–108. doi:10.1176/appi.ajp.159.1.103
18. Velligan DI, Wang M, Diamond P, et al. Relationships among subjective and objective measures of adherence to oral antipsychotic medications. Psychiatr Serv. 2007;58(9):1187–1192. doi:10.1176/ps.2007.58.9.1187
19. Gaudiano BA, Weinstock LM, Miller IW. Improving treatment adherence in bipolar disorder: a review of current psychosocial treatment efficacy and recommendations for future treatment development. Behav Modif. 2008;32(3):267–301. doi:10.1177/0145445507309023
20. Tewksbury A, Olander A. Management of antipsychotic-induced hyperprolactinemia. Ment Health Clin. 2016;6(4):185–190. doi:10.9740/mhc.2016.07.185
21. Mattingly GW, Haddad PM, Tocco M, et al. Switching to Lurasidone following 12 months of treatment with Risperidone: results of a 6-month, open-label study. BMC Psychiatry. 2020;20(1):199. doi:10.1186/s12888-020-02523-1
22. Byerly MJ, Marcus RN, Tran QV, et al. Effects of aripiprazole on prolactin levels in subjects with schizophrenia during cross-titration with risperidone or olanzapine: analysis of a randomized, open-label study. Schizophr Res. 2009;107(2–3):218–222. doi:10.1016/j.schres.2008.09.019
23. Durgam S, Litman RE, Papadakis K, et al. Cariprazine in the treatment of schizophrenia: a proof-of-concept trial. Int Clin Psychopharmacol. 2016;31(2):61–68. doi:10.1097/YIC.0000000000000110
24. Durgam S, Cutler AJ, Lu K, et al. Cariprazine in acute exacerbation of schizophrenia: a fixed-dose, Phase 3, randomized, double-blind, placebo- and active-controlled trial. J Clin Psychiatry. 2015;76(12):e1574–1582. doi:10.4088/JCP.15m09997
25. Kane JM, Zukin S, Wang Y, et al. Efficacy and safety of cariprazine in acute exacerbation of schizophrenia: results from an international, Phase III clinical trial. J Clin Psychopharmacol. 2015;35(4):367–373. doi:10.1097/JCP.0000000000000346
26. Durgam S, Starace A, Li D, et al. An evaluation of the safety and efficacy of cariprazine in patients with acute exacerbation of schizophrenia: a Phase II, randomized clinical trial. Schizophr Res. 2014;152(2–3):450–457. doi:10.1016/j.schres.2013.11.041
27. Cutler AJ, Durgam S, Wang Y, et al. Evaluation of the long-term safety and tolerability of cariprazine in patients with schizophrenia: results from a 1-year open-label study. CNS Spectr. 2018;23(1):39–50. doi:10.1017/S1092852917000220
28. Durgam S, Greenberg WM, Li D, et al. Safety and tolerability of cariprazine in the long-term treatment of schizophrenia: results from a 48-week, single-arm, open-label extension study. Psychopharmacology. 2017;234(2):199–209. doi:10.1007/s00213-016-4450-3
29. Durgam S, Earley W, Li R, et al. Long-term cariprazine treatment for the prevention of relapse in patients with schizophrenia: a randomized, double-blind, placebo-controlled trial. Schizophr Res. 2016;176(2–3):264–271. doi:10.1016/j.schres.2016.06.030
30. Earley W, Guo H, Luchini R. Modified cariprazine relapse prevention clinical trial results. Schizophr Res. 2018;199:452–453. doi:10.1016/j.schres.2018.04.016
31. Durgam S, Starace A, Li D, et al. The efficacy and tolerability of cariprazine in acute mania associated with bipolar I disorder: a phase II trial. Bipolar Disord. 2015;17(1):63–75. doi:10.1111/bdi.12238
32. Sachs GS, Greenberg WM, Starace A, et al. Cariprazine in the treatment of acute mania in bipolar I disorder: a double-blind, placebo-controlled, phase III trial. J Affect Disord. 2015;174:296–302. doi:10.1016/j.jad.2014.11.018
33. Calabrese JR, Keck PE
34. Ketter TA, Sachs GS, Durgam S, et al. The safety and tolerability of cariprazine in patients with manic or mixed episodes associated with bipolar I disorder: a 16-week open-label study. J Affect Disord. 2018;225:350–356. doi:10.1016/j.jad.2017.08.040
35. Earley WR, Burgess MV, Khan B, et al. Efficacy and safety of cariprazine in bipolar I depression: a double-blind, placebo-controlled phase 3 study. Bipolar Disord. 2019;22(4):372–384. doi:10.1111/bdi.12852
36. Earley W, Burgess MV, Rekeda L, et al. Cariprazine treatment of bipolar depression: a randomized double-blind placebo-controlled phase 3 study. Am J Psychiatry. 2019;176(6):439–448. doi:10.1176/appi.ajp.2018.18070824
37. Durgam S, Earley W, Lipschitz A, et al. An 8-week randomized, double-blind, placebo-Controlled evaluation of the safety and efficacy of cariprazine in patients with bipolar I depression. Am J Psychiatry. 2016;173(3):271–281. doi:10.1176/appi.ajp.2015.15020164
38. Pacchiarotti I, Murru A, Kotzalidis GD, et al. Hyperprolactinemia and medications for bipolar disorder: systematic review of a neglected issue in clinical practice. Eur Neuropsychopharmacol. 2015;25(8):1045–1059. doi:10.1016/j.euroneuro.2015.04.007
39. Torre DL, Falorni A. Pharmacological causes of hyperprolactinemia. Ther Clin Risk Manag. 2007;3(5):929–951.
40. Arakawa R, Okumura M, Ito H, et al. Positron emission tomography measurement of dopamine D(2) receptor occupancy in the pituitary and cerebral cortex: relation to antipsychotic-induced hyperprolactinemia. J Clin Psychiatry. 2010;71(9):1131–1137. doi:10.4088/JCP.08m04307yel
41. Gyertyan I, Kiss B, Saghy K, et al. Cariprazine (RGH-188), a potent D3/D2 dopamine receptor partial agonist, binds to dopamine D3 receptors in vivo and shows antipsychotic-like and procognitive effects in rodents. Neurochem Int. 2011;59(6):925–935. doi:10.1016/j.neuint.2011.07.002
42. Wang JS, Ruan Y, Taylor RM, et al. The brain entry of risperidone and 9-hydroxyrisperidone is greatly limited by P-glycoprotein. Int J Neuropsychopharmacol. 2004;7(4):415–419. doi:10.1017/S1461145704004390
43. Leucht S, Leucht C, Huhn M, et al. Sixty years of placebo-controlled antipsychotic drug trials in acute schizophrenia: systematic review, bayesian meta-analysis, and meta-regression of efficacy predictors. Am J Psychiatry. 2017;174(10):927–942. doi:10.1176/appi.ajp.2017.16121358
44. Ivkovic J, Lindsten A, George V, et al. Effect of brexpiprazole on prolactin. J Clin Psychopharmacol. 2019;39(1):13–19. doi:10.1097/JCP.0000000000000979
45. Zheng W, Cai DB, Yang XH, et al. Adjunctive aripiprazole for antipsychotic-related hyperprolactinaemia in patients with first-episode schizophrenia: a meta-analysis. Gen Psychiatr. 2019;32(5):e100091. doi:10.1136/gpsych-2019-100091
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Anhedonia in Depression and Schizophrenia: Brain Reward and Aversion Circuits
Liang S, Wu Y, Hanxiaoran L, Greenshaw AJ, Li T
Neuropsychiatric Disease and Treatment 2022, 18:1385-1396
Published Date: 7 July 2022
Switching Clozapine to Cariprazine in Three Patients with Persistent Symptoms of Schizophrenia: A Case Series
Duque-Yemail JD, Avila JC
Neuropsychiatric Disease and Treatment 2022, 18:1433-1440
Published Date: 13 July 2022
Seasonal Effects on Hospitalizations Due to Mood and Psychotic Disorders: A Nationwide 31-Year Register Study
Törmälehto S, Svirskis T, Partonen T, Isometsä E, Pirkola S, Virtanen M, Sund R
Clinical Epidemiology 2022, 14:1177-1191
Published Date: 21 October 2022
Albumin and Associated Biomarkers in Severe Neuropsychiatric Disorders: Acute-Phase Schizophrenia and Bipolar Disorder
Xu H, Zheng L, Wang L, Gao H, Wei Y, Chen J
Neuropsychiatric Disease and Treatment 2023, 19:2027-2037
Published Date: 28 September 2023
Neurogenetics and Epigenetics of Loneliness
Bowirrat A, Elman I, Dennen CA, Gondré-Lewis MC, Cadet JL, Khalsa J, Baron D, Soni D, Gold MS, McLaughlin TJ, Bagchi D, Braverman ER, Ceccanti M, Thanos PK, Modestino EJ, Sunder K, Jafari N, Zeine F, Badgaiyan RD, Barh D, Makale M, Murphy KT, Blum K
Psychology Research and Behavior Management 2023, 16:4839-4857
Published Date: 29 November 2023