")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 19
Albumin and Associated Biomarkers in Severe Neuropsychiatric Disorders: Acute-Phase Schizophrenia and Bipolar Disorder
Authors Xu H, Zheng L, Wang L, Gao H, Wei Y, Chen J
Received 29 May 2023
Accepted for publication 17 August 2023
Published 28 September 2023 Volume 2023:19 Pages 2027—2037
DOI https://doi.org/10.2147/NDT.S423399
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Yuping Ning
Haiting Xu,1 Lina Zheng,2 Leilei Wang,1 Huanqin Gao,1 Yanyan Wei,1 Jingxu Chen1
1Psychology and Psychiatric Department, Beijing Hui-Long-Guan Hospital, Peking University, Beijing, People’s Republic of China; 2Psychology and Psychiatric Department, Liaocheng People’s Hospital, Liaocheng, People’s Republic of China
Correspondence: Jingxu Chen, Email [email protected]
Background: Inflammation is relevant to the pathophysiology of severe neuropsychiatric disorders, schizophrenia (SCZ) and bipolar disorders (BD). Multiple pathophysiological biomarkers are valuable for the study of inflammatory processes. This study investigated albumin-related biomarkers in SCZ and BD to explore their roles in disease.
Methods: A total of 5,577 SCZ, 3442 BD-manic (BD-M) and 1405 BD-depression (BD-D) in acute stage and 5000 health controls (HCs) were enrolled. The differences in these biomarker levels among different groups were compared, and the contributing factors for the occurrence of SCZ, BD, and subgroups of BD were analyzed.
Results: Both SCZ and BD exhibit lower prognostic nutritional index (PNI), but higher neutrophil percentage-to-albumin ratio (NPAR) and creatinine–albumin ratio (CRA) compared with HC. Compared with BD-D, BD-M had higher NPAR and platelet-to-albumin ratio (PAR) and lower CRA. In logistic regression, lower prognostic nutritional index (PNI) and higher CRA were associated with both SCZ and BD, while higher NPAR was associated with BD. In the subgroup of BD, higher NPAR, CRA and lower PNI were associated with BD-M; lower PAR, PNI and higher CRA were associated with BD-D.
Conclusion: Our study reaffirmed the role of inflammation in the pathophysiology of SCZ and BD. Diagnostic value has been demonstrated in NPAR, PAR, PNI and CRA for BD and SCZ.
Keywords: schizophrenia, bipolar disorder, inflammation, albumin, neutrophil percentage-to-albumin ratio, platelet to albumin ratio, prognostic nutritional index
Introduction
Schizophrenia and bipolar disorder are severe neuropsychiatric disorders defined by remarkably heterogeneous clinical symptoms and are high global burden diseases because of multiple and persistent functional impairments including dysfunction in thoughts, perceptions, emotions and behaviour,1 which share common features with each other considerably in terms of pathophysiological level and risk genes.2 The etiologies of both schizophrenia and bipolar disorder are yet uncovered completely and precisely, and there still lack of effective biological markers for the diagnosis of both diseases.
Over the last two decades, chronic systemic inflammation and immunity are relevant to the pathophysiology of SCZ3 and BD.4 Previous studies demonstrated that multiple pathophysiological biomarkers, which are easily available by use of routine blood examinations, are valuable for the study of inflammatory processes and immune states in psychiatry.5,6 However, for complicated diseases, like a lot of physical diseases and psychotic illnesses, one single biological marker often could not display satisfactory predictive value, while combined biomarkers can effectively improve the sensitivity of prediction.7 Along with the finding, combinations of biomarkers have become research hot spot recently.
Albumin is a protein with anti-inflammatory effects,8 which are down-regulated in response in the process of inflammation.9 Some biomarkers derived from albumin have been proved prognostic and predictive functions in critically ill patients. As a new biomarker, neutrophil percentage-to-albumin ratio (NPAR) has been reported to reflect inflammatory status10 and might be more effective in reflecting inflammation than albumin, neutrophil percentage, and neutrophil-to-albumin ratio (NLR).11 The platelet-to-albumin ratio (PAR) was first proposed to assess cancer prognostic and considered as a biomarker for inflammatory status,12 which has been shown to be effective in predicting inflammation states of affective disorders in previous study.13 The prognostic nutritional index (PNI) was a biomarker, which was originally used in assessment in malnutritional status and immune state of surgical patients.14 In recent years, studies showed that not only nutrient intake but also inflammation and oxidation stress played a role in malnutrition. A large number of studies have been performed using PNI as prognosis among patients with inflammation-related disease.15 Current evidence in the literature showed that elevated serum creatinine reflects inflammation that alters renal endothelial/vascular function leading to decreased renal function, and worsening kidney function may itself be an inflammation.16 Studies of somatic diseases suggested that creatinine–albumin ratio (CRA) was a new promising and easy-to-measure clinical indicator of prognostic assessment.7 Some studies has conducted to detect neurobiological markers in schizophrenia and bipolar disorder, NLR, MLR and SII index were significantly higher in patients with BD than in healthy controls;17 NLR and neutrophil and platelet counts were found to be higher in the patient with schizophrenia as compared to the healthy control group;18 a functional imbalance in the synthesis of amino acids metabolites causes the appearance of pathophysiologic mechanisms that leads to various neuropsychiatric diseases, such as schizophrenia and bipolar disorder.19 However, as far as we know, there are limited number of existing studies on NPAR, PNI and PAR and no studies on CRA in patients with SCZ and BD. Limited studies have been conducted using these indicators in psychotic disorders. In this study, we propose that NPAR, PAR, PNI and CRA may participate in the occurrence of BD and SCZ and be biomarkers to reflect the inflammation-immune status of acute SCZ and BD.
Methods
Samples
We carried out a retrospective cross-sectional cohort study in Beijing Hui-Long-Guan hospital, in collaboration with Clinical Medical College of Peking University, China. In the study, we extracted and analyzed research data from electronic medical record database in Beijing Hui-Long-Guan hospital, ie, HIS System in six-year (from March 15th, 2015 to March 15th, 2021) period. The research data was extracted without any information that can be used to identify the patients except illness case numbers. The Hui-Long-Guan Hospital Ethics Committee approved the low-risk observational and retrospective research protocol, the ethical approval number 2021-17-KE.
Eligible data in this study should meet the inclusion criteria as follows: patients diagnosed schizophrenia and bipolar disorder in acute stage who were admitted or hospitalized by two attending psychiatrists based on the International Classification of Diseases-10 (ICD-10) coding from F20.0 to F20.9 and F31.1; 31.2; 31.4; 31.5, respectively; subjects were Han Chinese; age from 18 to 65 years old when blood tested. The exclusion criteria were as follows: 1) comorbid psychiatric disorder, 2) somatic diseases that might affect inflammatory, immune or antioxidant status such as hypertensive disease, diabetes, acute infection, acute or chronic autoimmune disease, 3) pregnancy or lactating female, 4) BMI >29.9 kg/m2 or <18.5 kg/m2, 5) smoking more than 20 cigarettes per day, 6) laboratory test showed hepatopathy or nephropathy, anemia. The health control group was consisted of 5000 healthy individuals recruited from the local community of matching age (18 to 65 years old) and sex with the case group, without family history of mental illness and any somatic disease that may disturb stabilization of homeostasis, including inflammatory, immune or antioxidant status. All subjects were Han Chinese and signed informed written consent. The data in this study were collected only from patients admitted inpatient care unit for the first time. We supposed that the blood samples enrolled in our study reflected the characters in acute phase of the diseases, as the blood test was performed the second day after hospitalized as a part of routine checks. Within the designated time frame, this retrospective case–control study enrolled 5,577 patients with SCZ, 4847 patients with BD (3,442 patients with manic episode and 1,405 patients with depressive episode).
Statistical Analysis
In this study, statistical analysis used SPSS (version 19.0) was used for the statistical analysis. The chi-square test was used to test gender. Continuous variable, age, among multiple independent groups, was compared using one-way analysis of variance (ANOVA). Analysis of covariance (ANCOVA) was performed in the context of the General Linear Model to assess the differences in biomarkers among the different groups. In the ANCOVA analysis process, we consider biomarkers as the dependent variables, and the diagnostic groups were included as fixed factors, while age and sex were included as covariates. Bonferroni-corrected ANCOVA as post hoc analysis was conducted to detect the differences among groups. Binary logistic regression analysis was adopted to investigate the risk factors for SCZ or BD by adjusting gender and age as covariates. Nomogram combined multiple indicators was used to predict the risk of SCZ or BD. Statistical significance threshold was set at P < 0.05.
Results
Comparison Among SCZ, BD and HCs
The total sample included 5577 SCZs, 4847 BDs and 5000 HCs. Chi-square test and ANOVA analysis in the study showed that there were no difference in age and gender among the three groups (F = 1.799, P = 0.165; χ2 = 2.799, P = 0.061) (Table 1).
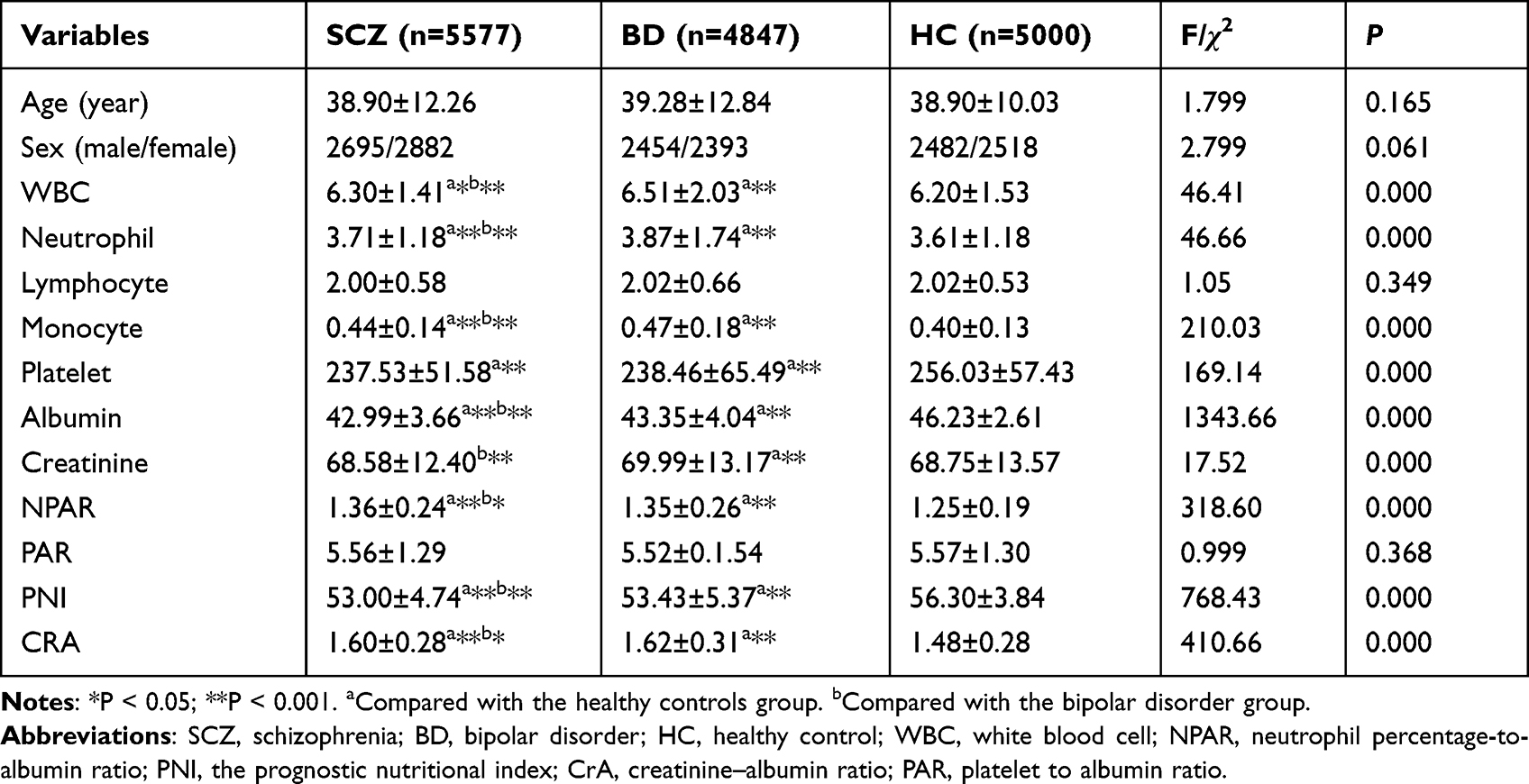 |
Table 1 Comparison of Sociodemographic and Laboratory Variables Among Schizophrenia, BD and Healthy Controls |
ANCOVA of the biomarker ratios which are related with inflammation and calculated from albumin levels displayed that both SCZs and BDs had higher NPAR, CRA (F = 318.60, P = 0.000; F = 410.086, P = 0.000, respectively) and lower PNI (F = 768.43, P = 0.000) compared to the HCs after adjusting for age and sex, and BDs had lower NPAR compared with the SCZ group. PNI and CRA in BDs exhibited higher level than those in the SCZs after adjusting for age and sex (Table 1).
The levels of WBC, neutrophil, monocyte, platelet counts, albumin and creatinine displayed significant differences (P < 0.01) in ANCOVA analysis after adjusting for age and sex among three groups, while there was no difference in the level of lymphocyte. Compared with HCs, the levels of WBC, neutrophil, and monocyte are higher, while levels of platelet counts and albumin are lower in SCZ group (P < 0.001, respectively) in post hoc analysis. No difference was found in lymphocyte and creatinine between SCZ group and HC group; compared with the HCs, BDs have slightly higher levels of WBC, neutrophil, monocyte and creatinine while slightly lower levels of platelet counts and albumin (P < 0.05, respectively). Furthermore, WBC, neutrophil, monocyte, albumin and creatinine differed between SCZ group and BD group after adjustment for age and sex (P < 0.05, respectively) (Table 1).
Comparison Among BD-M, BD-D and HCs
4847 individuals diagnosed of BD and 5000 HCs were included in the research. A total of 3,442 individuals with BD-M and 1,405 individuals with BD-D were included in data analysis. The ANCOVA analysis demonstrated that after controlling age and sex, there were significant differences in levels of blood cell counts, albumin, creatinine, NPAR, PAR, PNI, and CRA (P < 0.05, respectively). Post hoc analysis showed that BD-M group has higher levels of WBC, neutrophil, monocyte and creatinine, NPAR, CRA and lower levels of platelet, albumin and PNI than the HC group (P < 0.001, respectively); results demonstrated in BD-D group were not the same, ie, only the levels of mono, creatinine, NPAR and CRA were higher than HC group, while levels of platelet, albumin, PAR and PNI were lower than HC group (P < 0.001, respectively). Furthermore, there were differences in blood cell counts, albumin, creatinine, NPAR, PAR and CRA between BD-M and BD-D, after adjustment for age and sex (P < 0.05, respectively) (Table 2).
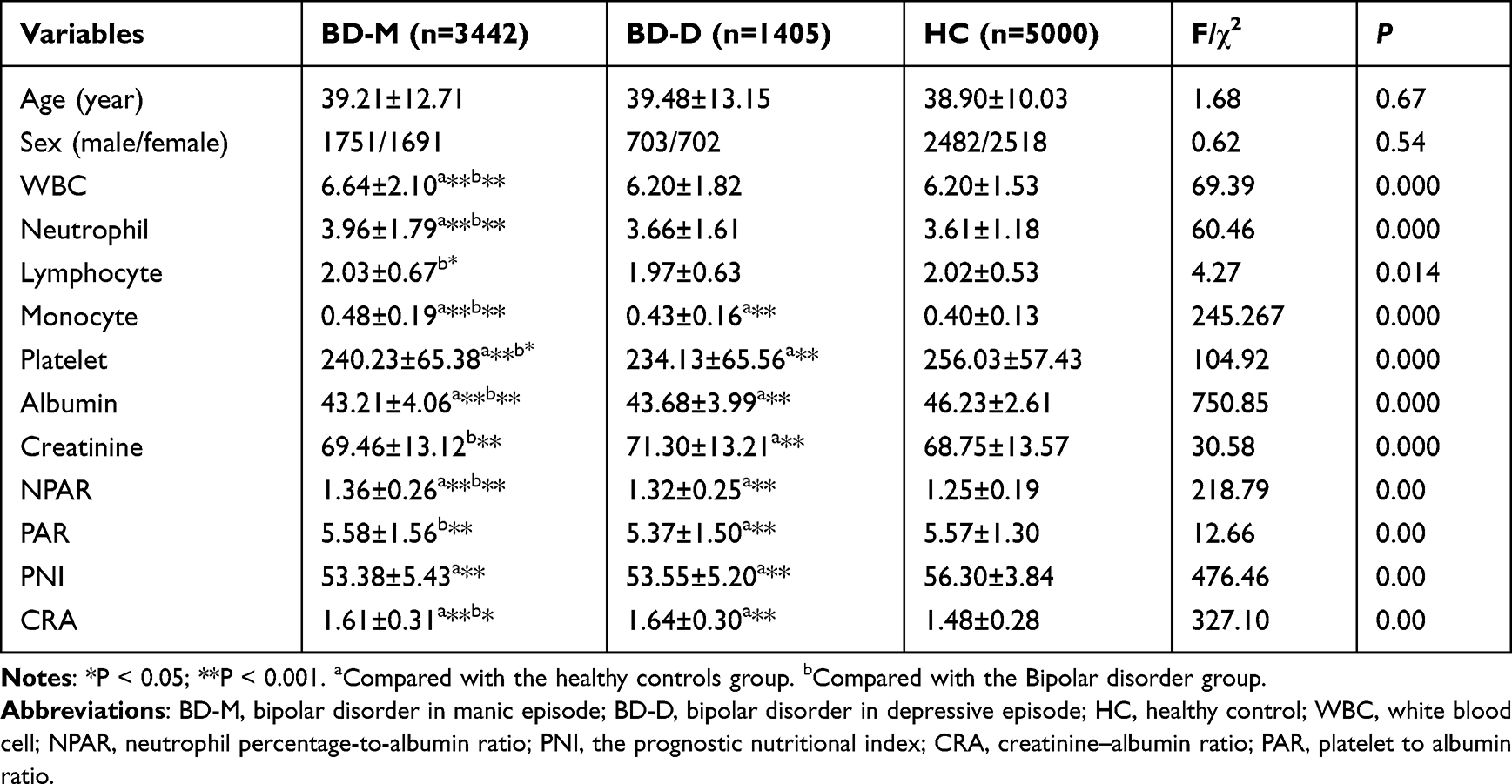 |
Table 2 Comparison of Sociodemographic and Laboratory Variables Among BD-Depression, BD-Manic and Healthy Controls |
Comparison Among BD-D, BD-M and SCZ
There were no differences in age and male/female ratio among SCZ group, BD-D group and BD-M group (F = 1.473, P = 0.229; χ2 = 2.898, P = 0.055, respectively). In the ANCOVA analysis, after adjusting for age and sex, significant differences were found in the levels of blood cell counts, albumin, creatinine, NPAR, PAR, PNI, and CRA (p < 0.05, respectively) among SCZ group, BD-D group and BD-M group. Post hoc analysis displayed that the levels of WBC, neutrophil and monocyte are higher, while levels of platelet, albumin and PNI are lower in BD-M group than SCZ group (P < 0.001, respectively); differently, the blood cell counts exhibit similar levels between BD-D group and SCZ group. In BD-D group, only the levels of creatinine, NPAR and CRA were higher than SCZ group, while levels of albumin, PAR and PNI were lower than SCZ group (P < 0.001, respectively) (Table 3).
 |
Table 3 Comparison of Sociodemographic and Laboratory Variables Among BD-D, BD-M and SCZ |
Logistic Regression
This study aimed to explore whether these albumin-based biomarkers could be the contributing factors for SCZ, BD, BD-M or BD-D. Disease status and control were adopted as dependent variables in the stepwise logistic regression model. The potential predictive values of albumin-based markers including NPAR, PAR, PNI and CRA, which were shown to be different between the control group and the acute disease status group, were assessed in the model (Table 4).
 |
Table 4 The Potential Predictive Values of Albumin-Based Markers in Logistic Regression Between the Control Group and the Acute Disease Status Group |
In binary logistic regression model of occurrence of acute SCZ, the result showed age (β = −0.016, P = 0.000), sex (β = −0.120, P = 0.035), PNI (β = −0.183, P = 0.000) and CRA (β = 1.657, P = 0.000) were independent influencing factors. We performed nomogram that combined multiple indicators to predict the risk of acute schizophrenia (Figure 1).
 |
Figure 1 Risk factors of SCZ nomogram. (Code of sex, 1: male, 2: female) (To use the nomogram, an individual patient’s value is located on each variable axis, and a line is drawn upward to determine the number of points received for each variable value. The sum of these numbers is located on the Total Points axis, and a line is drawn downward to the Risk of SCZ axes to determine the SCZ risk). Abbreviation: SCZ, schizophrenia. |
In binary logistic regression model of occurrence of acute BD group, the result showed age (β = −0.011, P = 0.000), sex (β = −0.235, P = 0.000), NPAR (β = 0.370, P = 0.004), PNI (β = −0.118, P = 0.000) and CRA (β = 1.849, P = 0.000) were independent influencing factors. We performed nomogram that combined multiple indicators to predict the risk of acute BD (Figure 2).
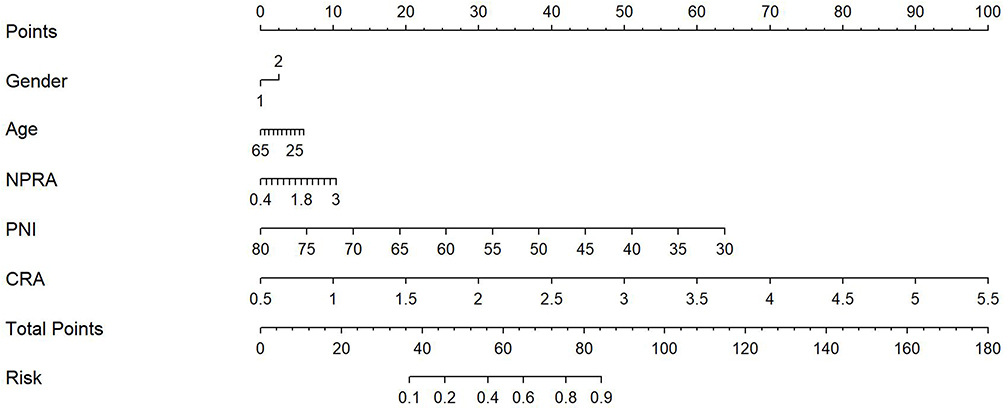 |
Figure 2 Risk factors of BD nomogram. (Code of sex, 1: male, 2: female) (To use the nomogram, an individual patient’s value is located on each variable axis, and a line is drawn upward to determine the number of points received for each variable value. The sum of these numbers is located on the Total Points axis, and a line is drawn downward to the Risk of BD axes to determine the BD risk). Abbreviation: BD, bipolar disorder. |
In binary logistic regression model of occurrence of acute BD-M group the result showed age (β = −0.013, P = 0.000), sex (β = −0.168, P = 0.009), NPAR (β = 0.596, P = 0.004), PNI (β = −0.122, P = 0.000) and CRA (β = 1.669, P = 0.000) were independent influencing factors. We performed nomogram that combined multiple indicators to predict the risk of acute BD-M (Figure 3).
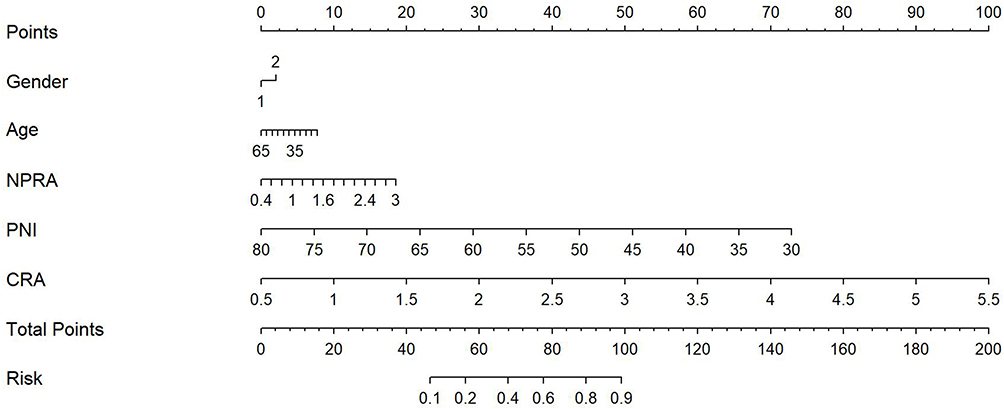 |
Figure 3 Risk factors of BD-M nomogram. (Code of sex, 1: male, 2: female) (To use the nomogram, an individual patient’s value is located on each variable axis, and a line is drawn upward to determine the number of points received for each variable value. The sum of these numbers is located on the Total Points axis, and a line is drawn downward to the Risk of BD-M axes to determine the BD-M risk). Abbreviation: BD-M, bipolar disorder manic episode. |
In binary logistic regression model of occurrence of acute BD-D group the result showed age (β = −0.009, P = 0.000), sex (β = −0.387, P = 0.005), PAR (β = −0.126, P = 0.000), PNI (β = −0.148, P = 0.000) and CRA (β = 2.031, P = 0.000) were independent influencing factors. We performed nomogram that combined multiple indicators to predict the risk of acute BD-D (Figure 4).
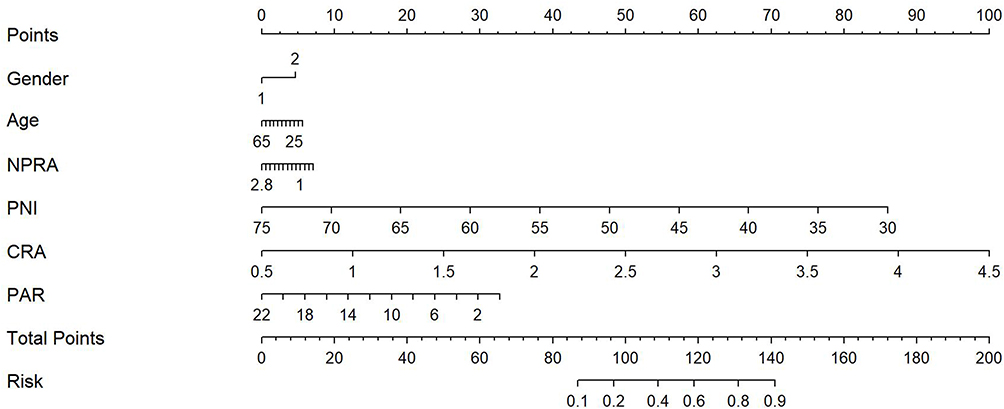 |
Figure 4 Risk factors of BD-D nomogram. (Code of sex, 1: male, 2: female) (To use the nomogram, an individual patient’s value is located on each variable axis, and a line is drawn upward to determine the number of points received for each variable value. The sum of these numbers is located on the Total Points axis, and a line is drawn downward to the Risk of BD-D axes to determine the BD-D risk). Abbreviation: BD-M, bipolar disorder manic episode. |
Discussion
This was a large-scale research, as far as we known, which was the first time explored albumin and related biomarkers, including NPAR, PAR, PNI and CRA, in schizophrenia and bipolar disorder patients at acute stage. Furthermore, the data of manic episode and depressive episode were analyzed separately. Our study showed that both SCZ and BD patients exhibited lower albumin and PNI, but higher NPAR and CRA compared with health controls. Compared with SCZ, BD had lower NPAR and higher PNI and CRA. Both BD-M and BD-D had higher NPAR, CRA and lower PNI than health controls, as well as lower PNI than SCZ. However, in BD-D, the level of PAR was lower than both health control and SCZ and the levels of NPAR and CRA were higher than SCZ. Compared with BD-D, BD-M had higher levels of NPAR and PAR and lower level of CRA. In multiple logistic regression, lower PNI and higher CRA were found to be strongly associated with both SCZ and BD, while higher levels of NPAR were associated with BD. In subgroup of BD, higher levels of NPAR, CRA and lower level of PNI were significantly associated with BD-M; lower levels of PAR, PNI and higher level of CRA were associated with BD-D.
There were some reasons why we have chosen these parameters calculated from albumin: first, unlike other inflammatory markers, albumin has a long half-life and can be easily obtained in daily clinical work in a real-life setting;6 second, these parameters were easily obtained from blood screening and have been proven effective in reflecting inflammatory processes and immune states in physical illness.
NPAR is a newly exploited predictor related with systemic inflammation stage in somatic diseases, such as cancer and stroke.11 Increased neutrophil percentage and decreased albumin levels have been demonstrated in patients with SCZ5,20 and BD.21,22 Along with the above observation, we found that NPAR, the combination of albumin and neutrophil percentage, displayed a valuable prediction of occurrence of BD, especially BD-M. Platelet played an important role in inflammatory response.23 Studies have demonstrated that a series of inflammatory conditions, including cancer progression,12 atherosclerosis24 and the pathophysiology of COVID-19,25 can be mediated by platelets. Platelet albumin ratio (PAR) is a combined indicator of inflammation and nutritional status and has been shown to be a useful and potentially prognostic biomarker for various cancers.12 There was limited data about PAR and psychotic disorders. In our team’s early work, we found that the BD-D patients had the lowest PAR among major depression disorders, BD-M and BD-D patients.13 The present study had found PAR levels in BD-D patients are also lower than those of SCZ patients, hence PAR could be a protective factor for BD-D which is contrary to the findings in other inflammation diseases.26 The reason could be related to the fact that platelet can regulate 5-HT23 which plays a key role in depression episode.27 PNI calculated peripheral blood lymphocyte count and albumin concentration as an indicator of the inflammatory response28 and linked nutritional status to immune response for patients.29 To our knowledge, this is the first study to detect PNI in acute psychotic disorders. We found both schizophrenia patients and BD patients have lower PNI than health control, and schizophrenia has the lowest PNI among schizophrenia, BD manic and depressive episodes, while PNI could play a protective role in both SCZ and BD patients. Further research should pay attention to PNI to back up these results. Creatinine is not only a metabolite of creatine phosphate as an energy storage but also had distinct effects for systemic inflammatory response7 and capacity to contribute to the total antioxidant.30 Previous study31 showed no difference in creatine levels among major depression disorder, BD-M and BD-D, which have been evaluated only in small single-center series. In the present study, we found BD-D has higher creatinine level than BD-M, SCZ and health controls, and the results were similar among the creatine levels of BD-M, SCZ and HCs. The inconsistency of results could be due to differences in the population studied and sample sizes of these studies. Studies of digestive diseases,7 suggested that creatinine-albumin ratio (CRA) was a negative prognostic factor with worse disease specific survival. Our results displayed that both BD and SCZ groups had higher levels of CRA than HC group, and both BD-D and BD-M had higher levels of CRA than HC group. Compared to the patients with SCZ and BD-M, the BD-D patients had higher CRA level. Our findings were not consistent with previous studies32,33 in that hypo(manic) phases of BD was associated with more obvious changes in inflammatory process than BD-D, but supports another point of view that heterogeneity existed between BD-D and BD-M.31 We speculate that there exist different inflammation mechanisms in BD-M and BD-D. CRA was showed to be a risk factor for the occurrence of BD and SCZ in the logistic regression analysis. However, limited studies were carried out on the association of the CAR with psychiatry diseases, and we speculated that elevated CRA may reflect the level of system inflammation as a peripheral sign and marker. Thus far, the mechanisms underlying BD and SCZ are shown to be complex and still not completely elucidated. And it is possible that inflammation and immune are only partial contributing factors of occurrence of SCZ and BD, which may explain why our study found these serum markers had minor relevance in logistic regression. This study can also reflect clinical phenomena more truly and facilitates an entry point in clinical application that combined biomarkers and model of biological markers can effectively improve the sensitivity of prediction.
The present study was a real-world research aimed to take the advantage of a large size database of patient medical information, the finding of which had potential for clinical transformation. However, there are still some limitations that need to be considered and caution should be taken when interpreting the findings of our study. First, as a retrospective study, certain clinical information is absent, such as course of disease, first episode of psychosis, BMI of subjects, and the severity of the disease. Second, due to the nature of cross-sectional study, the conclusion lacks of causal relationships between albumin-related parameters (NPAR, PAR, PNI and CRA) and BD or SCZ. Third, since information on dietary supplementation and pharmacotherapy is unreliable and fragmented, we could not assess whether albumin-related parameters (NPAR, PAR, PNI and CRA) might be at-least partly explained by these confounding factors.
Conclusions
In the present study, the albumin-related ratios, including the NAPR, PAR, PNI and CRA, were found to exhibit different levels in both BD and SCZ compared to in HCs. PNI could be a protective factor, and CRA could be a risk factor for both SCZ and BD. In BD-D, PAR could only be explained to a limited extent by inflammation but can reflect to a larger extent the critical role of platelets in the occurrence of the disease. Compared to the patients with BD-M, the BD-D subgroup had higher CRA level, suggesting that inflammatory changes are not more significant during manic episodes of BD than during depressive phases. Higher levels of NPAR, CRA and lower level of PNI were significantly linked to BD-M; lower levels of PAR, PNI and higher level of CRA were associated with BD-D, which support the previous literature which demonstrated heterogeneity existed between BD-D and BD-M, especially in the process of inflammation. The present research reaffirmed the role of systemic inflammation in the pathophysiology of SCZ and BD; along with the findings of our present study, more attention should be paid to NPAR, PAR, PNI and CRA to detect the mechanisms of inflammation in BD and SCZ, and heterogeneity in different episodes of BD, which could help find new ways of preventing BD and SCZ. Moreover, diagnostic value has been demonstrated in NPAR, PAR, PNI and CRA for BD and SCZ, and more detailed studies are needed to investigate on this point to help fill in gaps in the field of diagnostic biomarkers for BD and SCZ.
Abbreviations
SCZ, schizophrenia; BD, bipolar disorders; BD-M, BD-manic; BD-D, BD-depression; HCs, health controls; NPAR, neutrophil percentage-to-albumin ratio; CRA, creatinine–albumin ratio; PAR platelet-to-albumin ratio; PNI, prognostic nutritional index.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
The experimental protocol was established, according to the ethical guidelines of the Helsinki Declaration and was approved by the Human Ethics Committee of Hui-Long-Guan Hospital, no.2021-17-KE. Written informed consent was obtained from individuals or guardian participants.
Acknowledgments
The authors thank all of the participants for their commitment to this study. The authors report no financial relationship with commercial interests.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was supported by Scientific Foundation of Beijing Huilongguan Hospital, No LY202204, Beijing Hospitals Authority Clinical medicine Development of special funding, code XMLX202150; Beijing Municipal Hospital Scientific Research and Cultivation Program, PX2022079, and Capital’s Funds for Health Improvement and Research (2022-4-2134).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Dickerson F, Severance E, Yolken R. The microbiome, immunity, and schizophrenia and bipolar disorder. Brain Behav Immun. 2017;62:46–52. doi:10.1016/j.bbi.2016.12.010
2. Bowie CR, Best MW, Depp C, et al. Cognitive and functional deficits in bipolar disorder and schizophrenia as a function of the presence and history of psychosis. Bipolar Disord. 2018;20(7):604–613. doi:10.1111/bdi.12654
3. Morris G, Berk M, Walder K, O’Neil A, Maes M, Puri BK. The lipid paradox in neuroprogressive disorders: causes and consequences. Neurosci Biobehav Rev. 2021;128:35–57.
4. Jones BDM, Daskalakis ZJ, Carvalho AF, et al. Inflammation as a treatment target in mood disorders: review. BJPsych Open. 2020;6(4):e60.
5. Xu H, Wei Y, Zheng L, et al. Relation between unconjugated bilirubin and peripheral biomarkers of inflammation derived from complete blood counts in patients with acute stage of Schizophrenia. Front Psychiatry. 2022;13:843985.
6. Balcioglu YH, Kirlioglu SS. C-Reactive protein/albumin and neutrophil/albumin ratios as novel inflammatory markers in patients with Schizophrenia. Psychiatry Investig. 2020;17(9):902–910.
7. Zhao Z, Yu Y, Xie R, et al. Prognostic value of the creatinine-albumin ratio in acute pancreatitis debridement. BMC Surg. 2020;20(1):322.
8. Pisoschi AM, Pop A. The role of antioxidants in the chemistry of oxidative stress: a review. Eur J Med Chem. 2015;97:55–74.
9. Ritchie RF, Palomaki GE, Neveux LM, Navolotskaia O, Ledue TB, Craig WY. Reference distributions for the negative acute-phase serum proteins, albumin, transferrin and transthyretin: a practical, simple and clinically relevant approach in a large cohort. J Clin Lab Anal. 1999;13(6):273–279.
10. Chen Z, Xie D, Li Y, et al. Neutrophil albumin ratio is associated with all-cause mortality in stroke patients: a retrospective Database Study. Int J Gen Med. 2022;15:1–9. doi:10.2147/IJGM.S323114
11. Zhang H, Wu T, Tian X, Lyu P, Wang J, Cao Y. High neutrophil percentage-to-albumin ratio can predict occurrence of stroke-associated infection. Front Neurol. 2021;12:705790. doi:10.3389/fneur.2021.705790
12. Guo M, Sun T, Zhao Z, Ming L. Preoperative platelet to albumin ratio predicts outcome of patients with non-small-cell lung cancer. Ann Thorac Cardiovasc Surg. 2021;27(2):84–90. doi:10.5761/atcs.oa.20-00090
13. Wei Y, Feng J, Ma J, et al. Characteristics of platelet-associated parameters and their predictive values in Chinese patients with affective disorders. BMC Psychiatry. 2022;22(1):150. doi:10.1186/s12888-022-03775-9
14. Tsai M-T, Chang T-H, Wu B-J. Prognostic impact of nutritional risk assessment in patients with chronic schizophrenia. Schizophr Res. 2018;192:137–141. doi:10.1016/j.schres.2017.04.011
15. Basta G, Chatzianagnostou K, Paradossi U, et al. The prognostic impact of objective nutritional indices in elderly patients with ST-elevation myocardial infarction undergoing primary coronary intervention. Int J Cardiol. 2016;221:987–992. doi:10.1016/j.ijcard.2016.07.039
16. Stuveling EM, Hillege HL, Bakker SJ, Gans RO, De Jong PE, De Zeeuw D. C-reactive protein is associated with renal function abnormalities in a non-diabetic population. Kidney Int. 2003;63(2):654–661. doi:10.1046/j.1523-1755.2003.00762.x
17. Dadouli K, Janho MB, Hatziefthimiou A, et al. Neutrophil-to-lymphocyte, monocyte-to-lymphocyte, platelet-to-lymphocyte ratio and systemic immune-inflammatory index in different states of bipolar disorder. Brain Sci. 2022;12(8):1034. doi:10.3390/brainsci12081034
18. Gercek HG, Citir BG, Bukulme A. Neutrophil-to-lymphocyte and platelet-to-lymphocyte ratios as inflammation markers for early-onset schizophrenia. Bratisl Lek Listy. 2023;124(7):503–507. doi:10.4149/BLL_2023_077
19. Davidson M, Rashidi N, Nurgali K, Apostolopoulos V. The role of tryptophan metabolites in neuropsychiatric disorders. Int J Mol Sci. 2022;23(17):9968. doi:10.3390/ijms23179968
20. Chen S, Xia HS, Zhu F, et al. Association between decreased serum albumin levels and depressive symptoms in patients with schizophrenia in a Chinese Han population: a pilot study. Psychiatry Res. 2018;270:438–442. doi:10.1016/j.psychres.2018.10.012
21. Dargel AA, Volant S, Brietzke E, et al. Allostatic load, emotional hyper-reactivity, and functioning in individuals with bipolar disorder. Bipolar Disord. 2020;22(7):711–721. doi:10.1111/bdi.12927
22. Ozdin S, Usta MB. A comparison of inflammatory markers in manic and euthymic states of bipolar disorder. Nord J Psychiatry. 2021;75(2):124–129. doi:10.1080/08039488.2020.1807048
23. Pogorzelska K, Kretowska A, Krawczuk-Rybak M, Sawicka-Zukowska M. Characteristics of platelet indices and their prognostic significance in selected medical condition - a systematic review. Adv Med Sci. 2020;65(2):310–315. doi:10.1016/j.advms.2020.05.002
24. Custodio-Chable SJ, Lezama RA, Reyes-Maldonado E. Platelet activation as a trigger factor for inflammation and atherosclerosis. Cir Cir. 2020;88(2):233–243. doi:10.24875/CIRU.19000725
25. Manne BK, Denorme F, Middleton EA, et al. Platelet gene expression and function in patients with COVID-19. Blood. 2020;136(11):1317–1329. doi:10.1182/blood.2020007214
26. Tan J, Song G, Wang S, et al. Platelet-to-albumin ratio: a novel iga nephropathy prognosis predictor. Front Immunol. 2022;13:842362. doi:10.3389/fimmu.2022.842362
27. Izzi B, Tirozzi A, Cerletti C, et al. Beyond haemostasis and thrombosis: platelets in depression and its co-morbidities. Int J Mol Sci. 2020;21(22):8817. doi:10.3390/ijms21228817
28. Wang D, Hu X, Xiao L, et al. Prognostic nutritional index and systemic immune-inflammation index predict the prognosis of patients with HCC. J Gastrointest Surg. 2021;25(2):421–427. doi:10.1007/s11605-019-04492-7
29. Onodera T, Goseki N, Kosaki G. [Prognostic nutritional index in gastrointestinal surgery of malnourished cancer patients]. Nihon Geka Gakkai Zasshi. Japanese. 1984;85(9):1001–1005.
30. Nyasavajjala SM, Phillips BE, Lund JN, Williams JP. Creatinine and myoglobin are poor predictors of anaerobic threshold in colorectal cancer and health. J Cachexia Sarcopenia Muscle. 2015;6(2):125–131.
31. Bartoli F, Crocamo C, Dakanalis A, et al. Purinergic system dysfunctions in subjects with bipolar disorder: a comparative cross-sectional study. Compr Psychiatry. 2017;73:1–6.
32. Fusar-Poli L, Natale A, Amerio A, et al. Neutrophil-to-Lymphocyte, platelet-to-lymphocyte and monocyte-to-lymphocyte ratio in bipolar disorder. Brain Sci. 2021;11(1):58.
33. Mazza MG, Tringali AGM, Rossetti A, Botti RE, Clerici M. Cross-sectional study of neutrophil-lymphocyte, platelet-lymphocyte and monocyte-lymphocyte ratios in mood disorders. Gen Hosp Psychiatry. 2019;58:7–12.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.