Back to Journals » Journal of Inflammation Research » Volume 19
Mental Health Disorders in Pediatric Inflammatory Bowel Disease: Epidemiology, Mechanisms, and Interventions
Authors Liu Y, Hu Y, Zheng J, Wu Z
Received 8 January 2026
Accepted for publication 15 May 2026
Published 22 May 2026 Volume 2026:19 594782
DOI https://doi.org/10.2147/JIR.S594782
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Alberto Caminero
Yu Liu,1,* Yibing Hu,2,* Jiajing Zheng,1 Zhifei Wu1
1Department of Pediatrics, Beilun District People’s Hospital, Ningbo, Zhejiang, 315800, People’s Republic of China; 2Department of Gastroenterology, Affiliated Jinhua Hospital, Zhejiang University School of Medicine, Jinhua, Zhejiang, 321000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yu Liu, Department of Pediatrics, Beilun District People’s Hospital, No. 1288 of Lushan Road, Beilun District, Ningbo, Zhejiang, 315800, People’s Republic of China, Email [email protected]
Abstract: This review aims to synthesize current evidence on the association between pediatric inflammatory bowel disease (IBD) and mental health disorders, with a focus on epidemiology, underlying pathophysiological mechanisms, and advances in screening and intervention strategies. Pediatric IBD is increasingly recognized as a condition with substantial psychological as well as gastrointestinal burden. Children and adolescents with IBD have a markedly higher prevalence of mental health disorders than the general population, most commonly depression, anxiety, and sleep disorders, with risk appearing particularly higher in adolescents and in those with Crohn’s disease. Based on psychiatric evaluations, the prevalence of mental disorders in this population ranges from 42% to 73%. Accumulating evidence suggests a complex, bidirectional relationship between intestinal inflammation and mental health, mediated through interacting mechanisms that include gene–environment interactions, dysregulation of the gut–brain axis, immune imbalance, and medication-related effects. Although several validated screening tools for anxiety and depression have been introduced into clinical practice, mental health disorders in pediatric IBD remain frequently underrecognized and undertreated. Psychological interventions, family-centered care models, and pharmacologic treatments show potential benefit, but evidence in pediatric populations is limited and largely extrapolated from adult studies. Greater clinical awareness, routine mental health screening, and integrated multidisciplinary care interventions are essential to improve outcomes. Future large-scale, multi-center, and longitudinal studies are needed to clarify underlying mechanisms and optimize prevention and treatment strategies. Unlike previous reviews that often combine adult and pediatric populations, this review specifically focuses on pediatric-onset IBD and provides a dedicated synthesis of mental health comorbidities in children and adolescents.
Keywords: inflammatory bowel disease, children, mental health disorders, depression, anxiety
Introduction
Inflammatory bowel disease (IBD), encompassing Crohn’s disease (CD) and ulcerative colitis (UC), is a chronic immune-mediated disorder characterized by relapsing inflammation of the gastrointestinal tract.1,2 The global burden of IBD has steadily increased over recent decades in both developed and developing countries, with more than 7 million individuals currently affected worldwide. Pediatric-onset IBD represents a substantial and clinically important subgroup, as up to 25% of patients are diagnosed before the age of 18.3,4 The etiology of IBD remains unclear and may involve complex interactions among genetic susceptibility, environmental exposures, intestinal flora imbalance, and dysregulated immune responses.5 Currently, there is no curative therapy, and management strategies are primarily aimed at inducing and maintaining remission by controlling inflammation. Despite advances in pharmacologic treatment, many children fail to achieve sustained remission or experience frequent relapses.6 Pediatric patients commonly present with abdominal pain, diarrhea, rectal bleeding, weight loss, and impaired linear growth, and frequently require biologic agents, surgery, or hospitalization during childhood or adolescence.7,8 Recent global estimates indicate a rising trend in the incidence of pediatric-onset IBD, accompanied by an increasing recognition of its psychiatric burden. These trends underscore the urgent need for a dedicated review focused on this vulnerable population.
Compared with other chronic diseases, pediatric IBD has an earlier onset and follows a lifelong course. Its relapsing and unpredictable symptoms, including frequent toileting and vomiting, impose a substantial psychosocial burden during critical periods of psychological development.9 Mental health disorders are especially prevalent during active disease, including emotional and mood disorders, psychotic disorders, and neurodevelopmental disorders.10 Children with IBD have higher rates of suicidal ideation and are more susceptible to depression, anxiety, and eating disorders than their peers.11,12 Psychological comorbidities are closely associated with disease severity and markedly impair the quality of life, yet they remain frequently underrecognized and undertreated. Clinical research focusing on mental health in pediatric IBD is still limited.13,14 Studies based on psychiatric evaluations report a high prevalence of mental disorders in pediatric IBD (42%–73%), whereas registry-based studies report substantially lower rates (5%–19%), suggesting considerable underdiagnosis in clinical practice.15 In addition, children with preexisting psychological disorders have a significantly higher risk of developing IBD, suggesting a bidirectional relationship between IBD and mental health, although the underlying mechanisms remain unclear.16 A prospective longitudinal study of newly diagnosed pediatric IBD patients showed that once intestinal inflammation was initially controlled, mental health status rather than intestinal inflammation markers emerged as the strongest determinant of overall health outcomes, underscoring the central role of mental health in this population.17
This review aims to clarify the complex and bidirectional relationship between IBD and mental health disorders in children, with particular emphasis on their dynamic interactions. We synthesize current evidence on the underlying pathological and physiological mechanisms linking IBD with psychiatric comorbidities and summarize current intervention strategies for managing mental health problems in pediatric IBD. By moving beyond a purely gastroenterological perspective, this review seeks to encourage pediatric IBD clinicians to place greater emphasis on mental health assessment and care, thereby facilitating earlier recognition and treatment, reducing overall disease burden, and providing a reference for future research on the integration of gastrointestinal and mental health management in pediatric IBD. Existing reviews on mental health in IBD have largely combined adult and pediatric populations, focused primarily on gastrointestinal outcomes, or lacked a dedicated synthesis of psychiatric comorbidities specifically in children and adolescents. Unlike previous reviews, this narrative review specifically examines pediatric-onset IBD and provides a dedicated synthesis of mental health comorbidities in children and adolescents. Figures 1–3 present a conceptual framework of the review’s key domains (epidemiological characteristics, pathophysiological mechanisms, and intervention strategies) to improve reader orientation. By translating current evidence into practical recommendations, this review aims to help bridge the gap between gastroenterology and mental health care in pediatric practice.
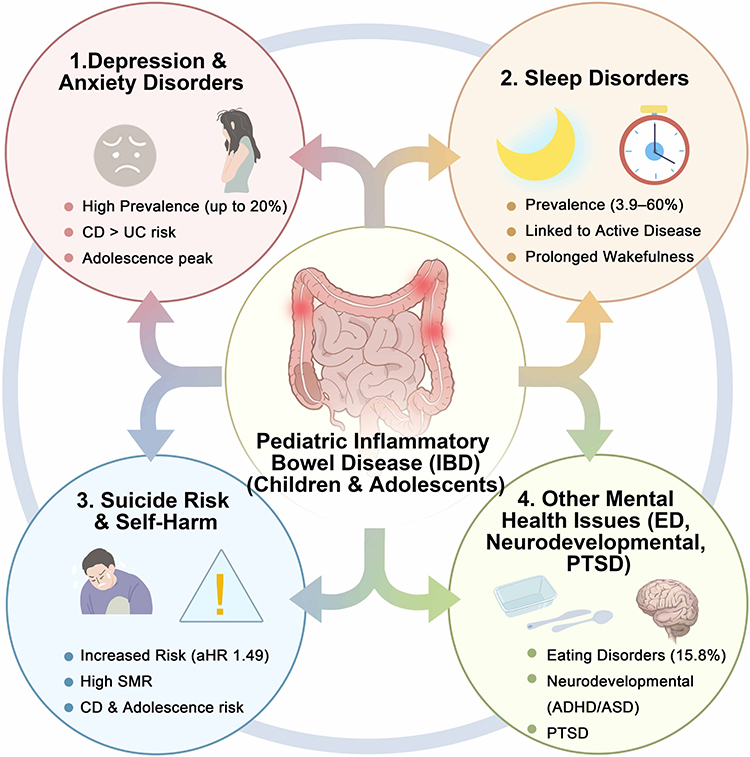 |
Figure 1 Epidemiological characteristics and mechanisms of mental health comorbidities in pediatric IBD. |
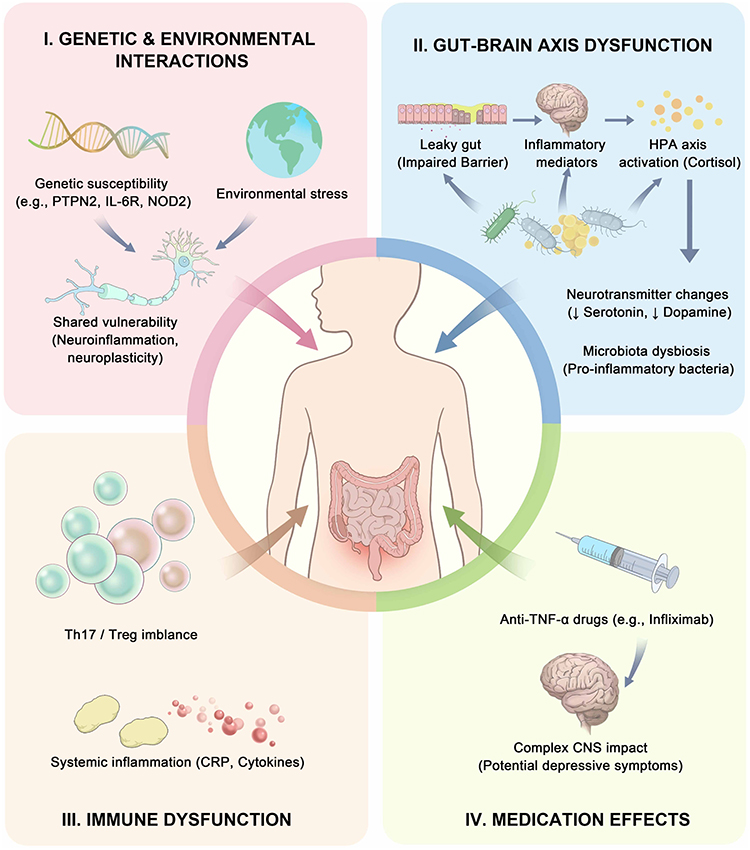 |
Figure 2 Pathophysiological mechanisms of co-morbid mental health disorders in pediatric IBD. |
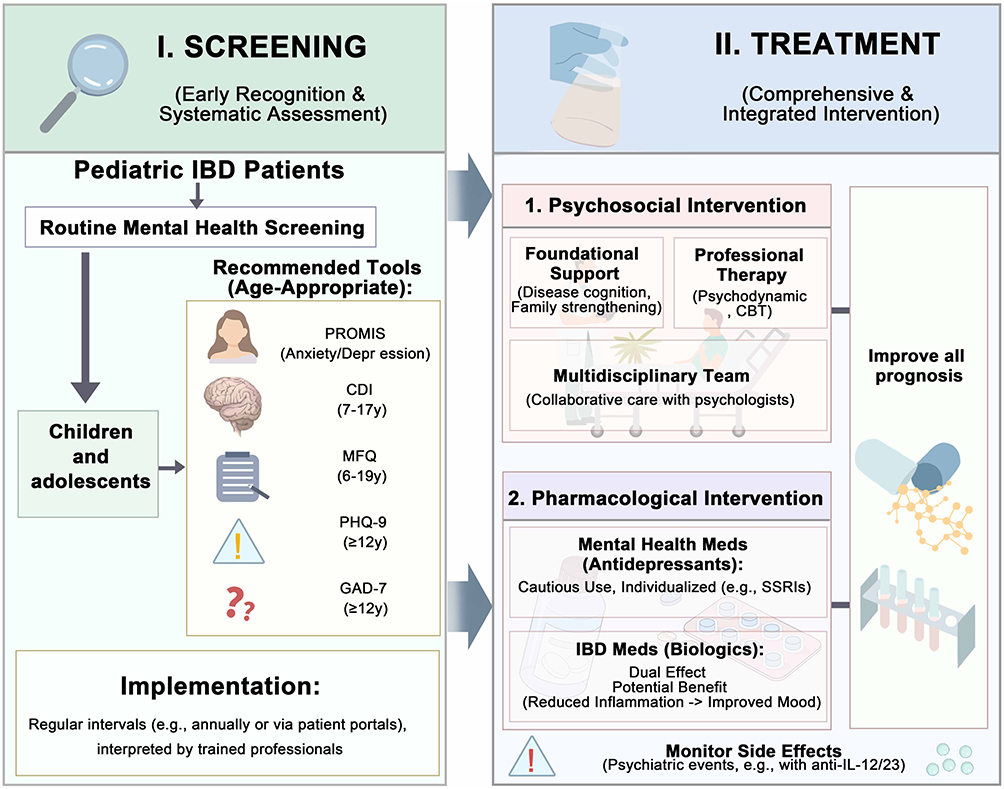 |
Figure 3 Interventions for pediatric IBD comorbid with mental health disorders. |
Epidemiological Characteristics of Mental Health Disorders in Pediatric IBD
Depression and Anxiety
Depression and anxiety are the most common mental health disorders observed in patients with IBD.18,19 Depressive disorders are characterized by persistent sad, empty, or irritable mood accompanied by cognitive and somatic symptoms that impair daily functioning, whereas anxiety encompasses a spectrum of emotional disorders marked by excessive fear and worry. In adult IBD populations, depression and anxiety are independent risk factors for disease onset and are significantly associated with increased relapse rates and overall disease burden.20–22 Children and adolescents are at a critical stage of physical and psychological development, and the diagnosis of a chronic disease may have profound effects on their mental health.23 Questionnaire-based studies indicate that up to 20% of pediatric patients report clinically significant symptoms of anxiety or depression.24
Emerging evidence suggests that mental health risk may vary by IBD type. A systematic review including both adult and pediatric populations reported no significant overall increase in anxiety risk among pediatric IBD patients (hazard ratio [HR] 1.47, 95% CI 0.66–3.27), but a markedly elevated risk in children with Crohn’s disease (HR 2.21, 95% CI 1.98–2.47). The risk of depression in pediatric IBD was also significantly increased (HR 1.6, 95% CI 1.4–1.7). However, only two studies specifically examined pediatric patients, limiting statistical power and generalizability.16 Consistent with these findings, another cohort study showed that children with CD had a higher risk of developing depression (adjusted HR [aHR] 1.41; 95% CI, 1.15–1.74; P = 0.001) and anxiety (aHR, 1.39; 95% CI, 1.11–1.74; P = 0.004), whereas these associations were less pronounced in UC.25 In contrast, a nationwide Danish cohort study demonstrated an increased risk of anxiety disorders in patients diagnosed before age 18 with either CD (incidence rate ratio [IRR] 1.58, 95% CI 1.33–1.86) or UC (IRR 1.39, 95% CI 1.19–1.64).26 Collectively, these findings indicate that childhood- or adolescent-onset IBD, irrespective of subtype, is associated with a sustained elevation in mental health risk.
Age at disease onset is an important modifier of mental health risk in pediatric IBD. A recent UK cohort study examining the incidence of mental health disorders in children and young adults with IBD reported that depression was the most common psychiatric condition (6.5% vs 4.7% in controls), followed by anxiety (5.1% vs. 3.9% in controls). After adjustment for confounders, IBD was associated with an increased risk of any mental disorder (aHR 1.28, 95% CI 1.12–1.46, P < 0.001), including depression (aHR 1.34, 95% CI, 1.16–1.56; P < 0.001) and anxiety (aHR 1.25, 95% CI, 1.06–1.48; P = 0.007). Subgroup analyses demonstrated the highest risk of new-onset mental health disorders among patients aged 12–17 years compared with those aged 5–11 years and 18–25 years (aHR 1.39; 95% CI, 1.14–1.70). In both the IBD and control cohorts, cumulative incidence of depression increased with age, reaching 6.3% versus 4.8% by age 18, and 20.6% versus 15.4% by age 25. These findings indicate that children and adolescents with IBD, particularly adolescents and those with CD, represent a high-risk population for mental health disorders. The limitations of this study included the absence of detailed data on disease activity, treatment adherence, family psychiatric history, and academic performance, as well as reliance on primary care coding, which may result in underdiagnosis or misclassification.25 However, a systematic review of children and adolescents aged 6 to 18 years with IBD reported a lower prevalence of anxiety and depressive symptoms (approximately 15–16%) compared with adults with IBD (approximately 21–35%) and with pediatric patients affected by other chronic diseases, such as diabetes and asthma (approximately 27–33%). This discrepancy may reflect age-related increases in psychiatric risk and the cumulative burden of disease-related complications over time. However, this review was dominated by two large studies (n = 2144 and n = 2733), whereas other studies enrolled fewer than 150 participants, raising concerns about selection bias. In addition, nearly 70% of the studies were conducted in North America, limiting cultural generalizability. Heterogeneity in assessment tools and diagnostic criteria for anxiety and depression further reduces the comparability and reliability of the pooled estimates.14
Disease activity is a key determinant of mental health outcomes in IBD and is strongly associated with anxiety and depressive symptoms. Studies in both adult and pediatric populations have consistently reported higher rates of anxiety and depression during active disease than during remission.20,27 A case–control study of 52 adolescents with IBD patients and matched healthy controls found that despite 82.7% of patients being in clinical remission, adolescents with IBD still exhibited a broad spectrum of psychological symptoms, particularly depression (P < 0.001). However, the single-center design and small sample size limited statistical power, highlighting the need for multicenter studies, especially those including patients with active disease.28
Sex-based differences in mental health outcomes among children with IBD remain unclear. Most studies report no significant association between sex and the prevalence of mental health issues in pediatric IBD,14 and several analyses have found no clear relationship between sex and depressive symptoms.29,30 However, some evidence suggests that female pediatric patients may experience more depressive symptoms (r = 0.21, P < 0.01) and anxiety (R2 = 0.05, P = 0.02).31,32 Family and psychosocial factors may also influence mental health risk. A nationwide German study found no significant association between family structure (single-parent vs. two-parent households) and mental health diagnoses (P = 0.06), whereas having one to two siblings was associated with a reduced risk of mental health issues (P = 0.03) and anxiety (P = 0.005). However, the cross-sectional study design and the use of non-validated questionnaires may have introduced sampling bias.33 Additional factors linked to depressive and anxiety symptoms include greater abdominal pain severity, pharmacological treatment, particularly corticosteroid use, negative illness perceptions, and internalizing symptom patterns characterized by mutual reinforcement of depression and anxiety.34 Anxiety has also been associated with increased surgical risk, poorer treatment compliance, and reduced quality of life in pediatric IBD.35,36 Overall, further well-designed studies are needed to clarify the relationship between pediatric IBD and depression and anxiety.
Sleep Disorders
Sleep disorders encompass impairments across multiple dimensions of sleep health, including sleep behavior, satisfaction, duration, efficiency, and daytime sleepiness.37 Evidence from adult IBD populations indicates that poor sleep quality can exacerbate inflammation, potentially worsening disease prognosis.38 Given that pediatric IBD often has a more aggressive course and broader intestinal involvement, understanding sleep health in this population is particularly important. A recent retrospective cohort study from the United Kingdom examined sleep outcomes in individuals aged 5–25 years and found that patients with IBD and comorbid mental health disorders had a significantly higher risk of developing sleep disorders (aHR = 1.63, 95% CI 1.02–2.62). Although sleep risk was not analyzed separately for those younger than 18 years, and the pediatric sample was relatively small (n = 40), an increasing trend in sleep disorder risk was still observed in children with IBD.39 Overall, the incidence of sleep disorders in pediatric IBD (3.9%) was significantly higher than that in controls (2.6%), making sleep disorders the third most common mental health condition in this population after depression and anxiety. After adjustment for age, sex, socioeconomic status, and race, pediatric IBD was independently associated with sleep disorders (aHR 1.40, 95% CI: 1.15–1.71; P = 0.001). Importantly, elevated risk may persist for up to 10 years following IBD diagnosis. Sleep disorders frequently coexist with depression and anxiety. However, the observational study design precludes causal inferences, and the absence of detailed data on sleep disorder type, severity, and treatment, represents an important limitation of the current evidence.25
A systematic review of 28 studies, including 3905 participants, reported that 53%–60% of children with IBD experienced clinically significant sleep disturbances. However, the overall prevalence of sleep disorders in pediatric IBD was not consistently higher than that observed in healthy children. Most included studies identified a positive correlation between disease activity and sleep disorders, particularly in CD, characterized by prolonged nocturnal awakenings and reduced deep sleep duration. Parent-reported nighttime awakenings were also significantly correlated with disease activity. However, interpretation of these findings is limited by methodological heterogeneity, as only nine studies used validated sleep assessment instruments, while 15 relied on single sleep items or subscales. In addition, most studies were cross-sectional and involved small sample sizes.40
A cross-sectional study of 53 children with IBD found that 67.9% of parents and 60% of adolescents identified sleep disturbances. Notably, over half of patients continued to experience sleep disturbances during remission (53.12%). By disease type, sleep disorders appeared more severe in UC than in CD. Across multiple self-reported sleep scales, including the Pittsburgh Sleep Quality Index (PSQI, P = 0.03), Pediatric Daytime Sleepiness Scale (PDSS, P = 0.05), and Adolescent Sleep–Wake Scale (ASWS, P = 0.04), patients with UC reported more severe sleep disturbances than CD patients. Importantly, sleep quality was significantly associated with disease activity in both CD (P = 0.002) and UC (P = 0.04). However, interpretation is limited by the small sample size, particularly in the UC group (n = 12), necessitating confirmation in larger cohorts.41 These findings are supported by a larger study from Turkey, which reported sleep disorders in 49% of pediatric IBD patients, with a higher prevalence in UC (59.2%) than in CD (40.1%). Patients with UC exhibited later sleep onset times (P = 0.008). Disease activity was identified as an independent predictor of sleep disorders in both CD (odds ratio [OR] 1.165, P = 0.018) and UC (OR 1.247, P = 0.013). However, the retrospective study design and single-center setting limit the generalizability of findings.42 Further large, multicenter, well-designed studies are needed to obtain more robust evidence. It should be noted, however, that most studies in this field are limited by small sample sizes, single-center designs, and cross-sectional methodology. These limitations constrain the generalizability of prevalence estimates and preclude definitive conclusions regarding causality.
Suicide and Self-Harm
Suicide is defined as death resulting from intentional self-inflicted injury with the intent to die, whereas self-harm refers to deliberate injury without suicidal intent.43 Several studies have examined the association between adult-onset IBD (≥18 years) and suicide risk.44 Adult IBD patients have an overall higher risk of suicide (HR 1.2, 95% CI 1.1–1.4), with a particularly higher risk in CD (HR = 1.5, P = 0.0001).45 However, there is a paucity of studies focusing on pediatric IBD.
Evidence suggests that suicide-related behaviors may be more prevalent in pediatric IBD than in other chronic childhood conditions. Compared with adolescents with juvenile idiopathic arthritis, adolescents with IBD have a higher prevalence of at least one mental health disorder (30% vs. 15.8%). In this cohort, 18% of adolescents with IBD reported suicidal ideation, 6% reported self-harm behaviors, and 2% reported suicide attempts.46 In addition, female patients had a higher prevalence of mental health problems (35% vs. 21%). However, the single-center retrospective study limits the generalizability of the findings.
Population-based data from the United Kingdom further indicate an increased risk of self-harm in children and young people with IBD (aHR 1.49, 95% CI 1.00–2.21, P = 0.05). Although the risk of parasuicide (suicide-like behavior) did not reach statistical significance, event rates were consistently higher than in controls, suggesting a potentially elevated suicide-related risk in this population. Subgroup analyses identified adolescents aged 12–17 years, males, and patients with CD as higher-risk groups.25 A prior systematic review reported particularly elevated suicide risk among patients with childhood-onset IBD, young adults with IBD, and those with a short disease duration, with the highest risk observed in childhood-onset disease. Contributing factors may include limited psychological maturity, disease-related stigma, the vulnerability of adolescence to mental health issues, and decreased treatment adherence during transition from pediatric to adult care.47 Consistent with this, a study of 6,689 patients with childhood-onset IBD reported a standardized mortality ratio (SMR) for suicide of 3.8 (95% CI 2.2–6.0).48 Another large cohort study, including 6,464 pediatric patients, found an increased risk of suicide attempts (HR 1.4, 95% CI 1.2–1.7), with a higher incidence in IBD patients than in the general population (1.6 vs. 1.2 per 1,000 person-years). Risk was significantly higher in CD (HR 1.5, 95% CI 1.1–2.0) but not in UC (HR 1.2, 95% CI 0.9–1.6).49
In adult IBD outpatients, depression severity has been identified as the strongest predictor of suicidal ideation, whereas disease activity and inflammatory markers show no significant association; use of low-dose tricyclic antidepressants has also been linked to increased risk.50 Whether these findings apply to pediatric populations remains unclear. Overall, suicide and self-harm in children and adolescents with IBD remain underrecognized, highlighting the need for systematic psychological assessment and targeted mental health support in this vulnerable population.
Other Mental Health Issues
Adolescents with IBD have a markedly higher risk of eating disorders (EDs). A study comparing adolescents aged 13–18 years with IBD and those with restrictive eating disorders (REDs), including anorexia nervosa and avoidant or restrictive food intake disorder, found that 15.8% of adolescents with IBD screened positive for ED risk, substantially higher than the prevalence in the general adolescent population (approximately 2.7%). Adolescents with IBD at high risk for EDs demonstrated psychological profiles that closely overlapped with those of patients with diagnosed REDs, suggesting shared underlying mechanisms. Female sex (OR 0.133) and longer disease duration (OR 1.055) were identified as risk factors for ED in adolescents with IBD.51 However, the relatively small sample size and possible exclusion of more complex cases may have introduced selection bias.
Neurodevelopmental disorders, primarily attention-deficit/hyperactivity disorder (ADHD) and autism spectrum disorder (ASD), have also been reported at higher rates in pediatric IBD. A single-center retrospective study found that 21.4% of children with UC had comorbid neurodevelopmental disorders, significantly exceeding population estimates (8.8%). The prevalence of ASD was particularly elevated at 8.2%, approximately threefold higher than in the general pediatric population. Children with UC and comorbid neurodevelopmental disorders exhibited more extensive endoscopic involvement, with E3–4 disease in 94.6% of cases, compared with 78.2% in those without comorbidity. Paradoxically, overall endoscopic severity scores were lower in the comorbidity group, suggesting a clinical–endoscopic dissociation that may reflect altered pain perception or communication difficulties, potentially leading to underreporting of symptoms and misestimation of disease activity. Limitations include reliance on medical history and behavioral observation for diagnosis, without standardized neuropsychological assessments. The potential contribution of the gut microbiota to these associations warrants further investigation.52 Consistent with a bidirectional relationship, a systematic review reported that individuals with ASD have an overall 1.66-fold higher risk of subsequently developing IBD, with a stronger association for UC (1.91-fold) than for CD (1.47-fold). These findings emphasize the importance of considering IBD in children with ASD who present with non-specific gastrointestinal symptoms such as abdominal pain, diarrhea, or weight loss.53 Overall, available evidence suggests meaningful interactions between neurodevelopmental abnormalities and IBD, although further large-scale, mechanistic studies are needed. Importantly, evidence on neurodevelopmental comorbidities in pediatric IBD is derived predominantly from small, single-center retrospective studies that often lack standardized neuropsychological assessments.
Although post-traumatic stress disorder (PTSD) is not a predominant psychiatric condition in pediatric IBD, and the absolute number of affected individuals is small, the relative risk is markedly increased. Among children and young adults with IBD, the odds ratio for PTSD is 4.5 (95% CI: 4.21–4.81, P < 0.001), indicating an approximately fourfold higher risk compared with peers without IBD. These findings support the inclusion of PTSD in routine mental health screening for pediatric and young adult IBD patients. However, the retrospective design of this study precludes definitive causal inference.54 A large Swedish cohort study reported a 20% increased risk of ADHD among children with IBD (HR 1.20, 95% CI 1.10–1.40).55 However, a more recent population-based cohort study found no statistically significant increase in ADHD diagnoses in pediatric IBD and suggested a decreasing trend (HR 0.77, 95% CI 0.56–1.06). Compared with matched controls, children with IBD also had a significantly lower likelihood of methylphenidate use (a commonly prescribed medication for ADHD) (HR 0.75, 95% CI 0.58–0.98), a pattern that was particularly pronounced in UC, where both the risk of methylphenidate use and ADHD diagnosis were markedly decreased (HR 0.63, 95% CI 0.43–0.93; HR 0.63, 95% CI 0.39–1.03, respectively). The reduced risk may reflect lifestyle changes following IBD diagnosis, symptom overlap between IBD and ADHD (such as fatigue and poor concentration), or underdiagnosis in this population. As this study was conducted within the Danish healthcare system, caution is warranted when extrapolating these results to other settings.56 A schematic illustration of the epidemiological characteristics and mechanisms of mental health comorbidities in pediatric IBD is presented in Figure 1.
Pathophysiological Mechanisms of Mental Health Disorders Comorbid with Pediatric IBD
Gene–Environment Interactions
Gene–environment interactions play a central role in linking pediatric IBD with mental health disorders. The immune-related gene PTPN2 (protein tyrosine phosphatase non-receptor type 2) regulates T-cell receptor signaling, cytokine pathways, and intestinal epithelial homeostasis, and has been implicated in IBD susceptibility and progression. In PTPN2 knockout mouse models, reduced brain levels of norepinephrine, dopamine, and serotonin have been observed, accompanied by anxiety-like behaviors, suggesting a mechanistic link between PTPN2 dysfunction, intestinal inflammation, and anxiety phenotypes.57,58 Genome-wide association studies (GWAS) have also identified shared genetic risk loci between IBD and depression, including RHOA (Ras homolog family member A). RHOA is a stress response-related gene involved in neuronal dendritic remodeling and regulation of social stress responses and depression-like behaviors.59
Beyond shared susceptibility genes, several inflammation-related genes implicated in IBD, such as IL-6R, P2RX7, NOD2, and IL23R, contribute to immune activation, cytokine signaling, and microbial recognition. These genes also exhibit altered expression in specific brain regions and have been associated with depressive phenotypes, suggesting that inflammatory pathways may serve as a biological bridge between IBD and depression.60
Environmental stressors such as chronic pain, frequent medical visits, and disease-related social restrictions can also cause psychological stress in children with IBD, thereby triggering or exacerbating depression and anxiety.20 In addition, maternal history of mental illness has been associated with an increased risk of emotional disorders in children with UC, highlighting the potential contribution of familial and heritable factors to mental health comorbidity in pediatric IBD.26
Dysregulation of the Gut–Brain Axis
Bidirectional communication between the gastrointestinal tract and the central nervous system, known as the gut-brain axis, plays a critical role in both IBD pathogenesis and the development of mental health disorders. Intestinal inflammation can influence brain function through neural, endocrine, and immune mechanisms, thereby contributing to anxiety, depression, and other psychiatric symptoms.61,62 Chronic intestinal inflammation may disrupt epithelial and vascular barriers, promoting systemic inflammation and neuroimmune signaling. In this context, brain-resident macrophages, particularly microglia, may play a key role in mediating inflammatory effects on the central nervous system.63
Experimental studies in germ-free mice have demonstrated that the gut microbiota regulates the set point of the hypothalamic–pituitary–adrenal (HPA) axis and behavioral stress responses. Conversely, sustained psychological stress can induce HPA axis dysfunction and colonic cortisol deficiency, potentially triggering chronic intestinal inflammation in genetically susceptible hosts.64–67 Clinically, up to 50% of patients with depression exhibit HPA axis overactivation, characterized by persistently elevated cortisol levels, impaired glucocorticoid receptor sensitivity, and weakened negative feedback. These alterations may further compromise intestinal barrier integrity, reshape the gut microbiota, and dysregulate mucosal immune responses, thereby promoting IBD development or exacerbation.67,68
Gut microbiota dysbiosis, typified by an expansion of pro-inflammatory taxa and depletion of anti-inflammatory bacteria, has been observed in both IBD and depression, supporting a shared microbial signature in these conditions.69,70 Clinical interest in microbiota-based interventions has therefore increased. A systematic review reported improvements in depressive and anxiety-like symptoms following fecal microbiota transplantation (FMT) in diverse populations.71 In addition, probiotics such as Lactobacillus and Bifidobacterium have been shown to alleviate depressive symptoms, and fecal microbiota from patients with comorbid IBD and depression can induce both depression-like behaviors and intestinal inflammation in animal models.72,73 Collectively, these findings support the concept of the microbiota–gut–brain axis (MGBA) as a mechanistic link between IBD and neuropsychiatric disorders. The MGBA represents a complex, multi-directional network integrating neural, immune, and endocrine signaling between the gut microbiota, intestine, and brain.74 However, most available evidence is indirect and is derived largely from observational studies or small experimental cohorts. Robust mechanistic and longitudinal studies are still needed to define the precise role of the gut microbiota in the pathogenesis of mental health disorders comorbid with pediatric IBD. Although adult studies have extensively characterized microbiota alterations in IBD-associated depression, pediatric data remain scarce.
Immune Dysregulation
Immune imbalance, particularly increased T helper 17 (Th17) cells and reduced regulatory T (Treg) cells, has been documented in both IBD and depression. In mouse models, probiotic and prebiotic interventions targeting group 3 innate lymphoid cells (ILC3) promote the expansion of Treg cells in the intestinal mucosa and enhance behavioral responses under sustained and recurrent stress. Conversely, disruption of the Th17/Treg equilibrium has been implicated in stress-induced behavioral alterations, suggesting that intestinal immune dysregulation may affect emotional function through central nervous system pathways.75
A study prospectively examined the associations between immune biomarkers, including C-reactive protein (CRP), albumin, and the CRP-to-albumin ratio, and symptoms of anxiety, depression, and insomnia in children with IBD treated at an Italian outpatient clinic between September 2021 and March 2022. The cortisol awakening response showed a positive correlation with anxiety symptoms (ρ = 0.591, P = 0.026), whereas albumin levels showed a negative correlation with both anxiety (ρ = −0.687, P = 0.007) and insomnia (ρ = −0.648, P = 0.012). No significant correlation was observed with depressive symptoms. These findings suggest that albumin and CAR may serve as potential biomarkers of anxiety and sleep disturbance risk in pediatric IBD. However, the small sample size precluded multivariable analyses, limiting interpretability. Larger multicenter, longitudinal studies incorporating repeated assessments and integrated biological, psychological, and social variables are required to validate these associations.76 In-depth comprehension of the interactions among the gastrointestinal tract, immune system, and central nervous system, as well as clarification of disease-specific mechanisms in UC and CD, will be essential for improving the prediction and management of mental health comorbidities in pediatric IBD and other inflammatory disorders.
Medication Effects
Small-scale studies have reported the emergence of neuropsychiatric symptoms within months of initiating TNF-α inhibitor therapy, even as gastrointestinal symptoms improve, suggesting partially shared or interacting pathogenic mechanisms.77,78 Psychiatric adverse effects typically appear within 2–8 weeks after initiation of biologic agents and most commonly include depression, anxiety, irritability, insomnia, suicidal ideation, and manic symptoms. Notably, many affected patients have no prior psychiatric history. However, evidence in pediatric IBD populations remains sparse.
Infliximab, in addition to its association with depression and suicidality in adults, has also been linked to similar effects in adolescents. One case report described a 16-year-old boy with a 2-year history of CD who developed depressive symptoms shortly after starting infliximab and attempted suicide by hanging after the fourth infusion. His psychiatric symptoms resolved with fluoxetine, melatonin, and psychotherapy, and did not recur with subsequent infusions, highlighting the importance of pre-treatment mental health screening, close monitoring during biologic therapy, and timely intervention in adolescents receiving biologic agents.78 Adalimumab has likewise been associated with insomnia, emotional lability, depressed mood, impaired attention, and suicidal ideation in pediatric patients with other inflammatory diseases, indicating that similar risks should be considered in the management of pediatric IBD.79,80 Although TNF-α is considered a key molecule linking inflammation, major depressive disorder, and suicidal behavior, the mechanisms by which pharmacological suppression of endogenous TNF-α may precipitate neuropsychiatric symptoms remain unclear.81 To date, most evidence on medication-related psychiatric effects in IBD derives from adult studies, with limited and heterogeneous pediatric data. Well-designed randomized controlled trials are needed to better define the relationship between the two in pediatric populations. A schematic illustration of the pathophysiological mechanisms of co-morbid mental health disorders in pediatric IBD is presented in Figure 2.
Interventions for Mental Health Disorders in Pediatric IBD
Established and Evidence-Based Approaches
Screening
Children and adolescents with IBD are at an increased risk for anxiety and depression, yet these conditions remain frequently underdetected. Failure to identify mental health disorders can compromise treatment adherence, increase relapse risk, and raise healthcare utilization and costs. A recent consensus statement from the Crohn’s & Colitis Foundation (New York, NY, USA) advocates routine assessment of anxiety and depression in patients with IBD, including children and adolescents, using the Patient-Reported Outcomes Measurement Information System (PROMIS). Several age-appropriate tools are endorsed, including the Child Depression Inventory for children and adolescents aged 7–17 years, the Moods and Feelings Questionnaire for individuals aged 6–19 years, the Patient Health Questionnaire (PHQ-2 and PHQ-9) for those aged 12 years and older, and the Generalized Anxiety Disorder-7 (GAD-7) for anxiety screening in individuals aged 12 years and older. Interpretation of screening results should be performed by appropriately trained professionals.82 In line with these recommendations, some experts advocate integrating depression screening into routine pediatric IBD care. Specifically, annual screening is recommended for all patients aged 12 years and older, using the short form of the Moods and Feelings Questionnaire (MFQ-SF) at age 12 and the PHQ-9 from age 13 onwards.83
The feasibility of implementing Patient-Reported Outcome Measures (PROMs) in pediatric IBD practice has been demonstrated in a real-world outpatient setting. In one study, patients aged 8–18 years and their parents received automated PROMs questionnaires via a patient portal every three months, administered seven days before scheduled visits. The assessments covered anxiety, depression, fatigue, pain, and quality of life. High satisfaction with the patient portal and clinician communication was reported, supporting the practicality of PROMs-based screening. However, the authors noted that questionnaire results required more systematic discussion during clinic visits and suggested that extending the screening interval to six months might further improve patient acceptability.24
Emerging and Experimental Approaches
Treatment
Similar to adults, adolescents with anxiety or depression demonstrate poorer adherence to medical therapy, underscoring the particular challenges of managing mental health comorbidities in pediatric IBD.84 To mitigate the long-term psychological consequences of childhood-onset IBD, disease narrative training has been proposed to help patients develop a more adaptive understanding of their illness, which may help ameliorate depressive symptoms.85 Strengthening family support is also crucial, as family functioning strongly influences treatment adherence and psychological outcomes in affected children and adolescents.86 Psychotherapeutic interventions have shown potential benefits. A prospective randomized trial evaluated short-term psychodynamic psychotherapy combined with standard medical treatment in adolescent and young adults with IBD and found a significant reduction in depressive symptoms compared with standard treatment alone (PHQ-9 score reduction, P = 0.014), although no significant improvement in anxiety was observed (P = 0.288).87 However, interpretation is limited by the small sample size and the absence of inflammatory marker assessment, precluding mechanistic insights. Disease-specific cognitive behavioral approaches, such as primary and secondary control enhancement therapy, have also been proposed for adolescent depression in IBD, but robust evidence supporting their efficacy remains limited.82
A patient- and family-centered multidisciplinary care model has been proposed for pediatric IBD, integrating psychologists into the core care team. In this model, psychologists conduct early and annual screening for depression, anxiety, and quality of life, deliver targeted psychological interventions, and coordinate referrals. Joint consultations involving psychologists and clinicians are recommended to facilitate comprehensive assessment and early intervention.88 Despite its conceptual appeal, this model has not yet been widely implemented in clinical practice.
Pharmacologic management of psychiatric symptoms in pediatric IBD requires particular caution. A case series involving four adolescents reported frequent gastrointestinal adverse effects with fluoxetine during active IBD, leading to treatment discontinuation in three patients, whereas tolerability improved during remission. Mirtazapine and sertraline were better tolerated in some cases. These findings highlight the need to individualize antidepressant selection based on disease activity, symptom profiles, and psychological status, although the small sample size and lack of controls limit generalizability.89
Biologic therapies, which target dysregulated inflammatory cytokines, are now central to pediatric IBD management. However, evidence regarding their effects on mental health outcomes remains limited and is largely extrapolated from adult studies. In adults with active IBD, anti-TNF therapy has been associated with improvements in depressive and anxiety symptoms alongside reduced disease activity.90 However, a randomized, controlled trial in treatment-resistant depression found no overall antidepressant effect of anti-TNF therapy, with benefits confined to patients with high inflammatory burden.91 Anti-α4/β7 integrin therapy has shown comparable and potentially more sustained improvements in mood symptoms in IBD populations.92 Importantly, psychiatric adverse effects have also been reported with biologic agents, with depression ranking among the most common psychiatric events associated with anti-p40 IL-12/IL-23 antibodies and vedolizumab.93 These observations highlight the need for careful mental health monitoring, particularly during the early phases of biologic therapy94 The interventions for pediatric IBD comorbid with mental health disorders are illustrated in Figure 3.
Summary
The incidence of pediatric IBD has shown a progressive increase. Its chronic, relapsing course is closely linked with various mental health disorders. Children and adolescents with IBD are at an elevated risk of developing depression, anxiety, sleep disorders, suicidal and self-harming behaviors, eating disorders, neurodevelopmental disorders (such as ASD), and PTSD. The wide variability in the reported rates of mental comorbidities suggests substantial underdiagnosis. The relationship between pediatric IBD and mental health issues arises from complex, interacting mechanisms involving gene–environment interactions, gut–brain axis dysregulation, immune imbalance, and medication effects. Disease activity, adolescent onset, Crohn’s disease subtype, and biologic therapy, particularly anti-TNF-α agents, may further influence psychiatric risk. Despite increasing recognition, evidence-based strategies for preventing and managing mental comorbidities in pediatric IBD remain limited. Routine mental health screening using validated tools (PROMIS, PHQ-9, and GAD-7) should be integrated into pediatric IBD care, including regular outpatient assessment and at least annual universal screening. Multidisciplinary teams comprising psychologists, gastroenterologists, nurses, and social workers are essential for early identification and coordinated intervention. Future research should prioritize large-scale, prospective, mechanism-oriented studies, including longitudinal pediatric cohorts, randomized controlled trials of psychological and pharmacologic interventions, and validation of pediatric-specific screening tools and biomarkers across multicenter and cross-cultural settings, to clarify causal pathways and optimize prevention and treatment strategies.
Data Sharing Statement
Data sharing is not applicable to this article as no data were created or analysed in this study.
Acknowledgments
We thank Medjaden Inc. for scientific editing of this paper.
Author Contributions
Yu Liu: Conceptualization, Methodology, Project administration, Supervision, Writing - original draft, Writing - review & editing; Yibing Hu: Conceptualization, Data curation, Investigation, Writing - review & editing; Jiajing Zheng: Conceptualization, Data curation, Investigation, Writing - original draft; Zhifei Wu: Data curation, Investigation, Software, Supervision, Visualization, Writing - original draft. All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work. Yu Liu & Yibing Hu contributed equally to the work and share first authorship.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare that they have no competing interests.
References
1. Dolinger M, Torres J, Vermeire S. Crohn’s disease. Lancet. 2024;403(10432):1177–15. doi:10.1016/s0140-6736(23)02586-2
2. Le Berre C, Honap S, Peyrin-Biroulet L. Ulcerative colitis. Lancet. 2023;402:571–584. doi:10.1016/s0140-6736(23)00966-2
3. Hathagoda W, Rajindrajith S, Niriella MA. Challenges in the Management of Inflammatory Bowel Disease in Children: a Narrative Review. Clin Exp Gastroenterol. 2025;18:259–275. doi:10.2147/ceg.S557464
4. Vuijk SA, Camman AE, de Ridder L. Considerations in Paediatric and Adolescent Inflammatory Bowel Disease. J Crohn’s Colitis. 2024;18:ii31–ii45. doi:10.1093/ecco-jcc/jjae087
5. Iliev ID, Ananthakrishnan AN, Guo CJ. Microbiota in inflammatory bowel disease: mechanisms of disease and therapeutic opportunities. Nat Rev Microbiol. 2025;23:509–524. doi:10.1038/s41579-025-01163-0
6. Pikov V. Vagus Nerve Stimulation and Sacral Nerve Stimulation for Inflammatory Bowel Disease: a Systematic Review. J Transl Gastroenterol. 2023;1:94–100. doi:10.14218/jtg.2023.00098
7. Kaplan GG. The global burden of inflammatory bowel disease: from 2025 to 2045. Nat Rev Gastroenterol Hepatol. 2025;22:708–720. doi:10.1038/s41575-025-01097-1
8. Honap S, Jairath V, Danese S, Peyrin-Biroulet L. Navigating the complexities of drug development for inflammatory bowel disease. Nat Rev Drug Discov. 2024;23:546–562. doi:10.1038/s41573-024-00953-0
9. Kuenzig ME, Fung SG, Marderfeld L, et al. Twenty-first Century Trends in the Global Epidemiology of Pediatric-Onset Inflammatory Bowel Disease: systematic Review. Gastroenterology. 2022;162:1147–1159.e1144. doi:10.1053/j.gastro.2021.12.282
10. Sadik A, Dardani C, Pagoni P, et al. Parental inflammatory bowel disease and autism in children. Nat Med. 2022;28:1406–1411. doi:10.1038/s41591-022-01845-9
11. Kammermeier J, Lamb CA, Jones KDJ, et al. Genomic diagnosis and care co-ordination for monogenic inflammatory bowel disease in children and adults: consensus guideline on behalf of the British Society of Gastroenterology and British Society of Paediatric Gastroenterology, Hepatology and Nutrition. Lancet Gastroenterol Hepatol. 2023;8:271–286. doi:10.1016/s2468-1253(22)00337-5
12. Tiles-Sar N, Neuser J, de Sordi D, et al. Psychological interventions for treatment of inflammatory bowel disease. Cochrane Database Syst Rev. 2025;4:Cd006913. doi:10.1002/14651858.CD006913.pub3
13. Marafini I, Longo L, Lavasani DM, et al. High Frequency of Undiagnosed Psychiatric Disorders in Inflammatory Bowel Diseases. J Clin Med. 2020;9:1387. doi:10.3390/jcm9051387
14. Stapersma L, van den Brink G, Szigethy EM, Escher JC, Utens E. Systematic review with meta-analysis: anxiety and depression in children and adolescents with inflammatory bowel disease. Aliment Pharmacol Ther. 2018;48:496–506. doi:10.1111/apt.14865
15. Jansson S, Malham M, Wewer V, Rask CU. Psychiatric comorbidity in childhood onset immune-mediated diseases-A systematic review and meta-analysis. Acta Paediatr. 2022;111:490–499. doi:10.1111/apa.16246
16. Bisgaard TH, Allin KH, Elmahdi R, Jess T. The bidirectional risk of inflammatory bowel disease and anxiety or depression: a systematic review and meta-analysis. Gen Hosp Psychiatry. 2023;83:109–116. doi:10.1016/j.genhosppsych.2023.05.002
17. Mekhael AA, Nabbijohn AN, Mack D, Stintzi A, Cohen JS, McMurtry CM. Psychological well-being is the major determinant of global health in the first year following a diagnosis of inflammatory bowel disease in children. J Psychosom Res. 2025;194:112142. doi:10.1016/j.jpsychores.2025.112142
18. Thapar A, Eyre O, Patel V, Brent D. Depression in young people. Lancet. 2022;400:617–631. doi:10.1016/s0140-6736(22)01012-1
19. Penninx BW, Pine DS, Holmes EA, Reif A. Anxiety disorders. Lancet. 2021;397:914–927. doi:10.1016/s0140-6736(21)00359-7
20. Bisgaard TH, Allin KH, Keefer L, Ananthakrishnan AN, Jess T. Depression and anxiety in inflammatory bowel disease: epidemiology, mechanisms and treatment. Nat Rev Gastroenterol Hepatol. 2022;19:717–726. doi:10.1038/s41575-022-00634-6
21. Barberio B, Zamani M, Black CJ, Savarino EV, Ford AC. Prevalence of symptoms of anxiety and depression in patients with inflammatory bowel disease: a systematic review and meta-analysis. Lancet Gastroenterol Hepatol. 2021;6:359–370. doi:10.1016/s2468-1253(21)00014-5
22. Petracco G, Faimann I, Reichmann F. Inflammatory bowel disease and neuropsychiatric disorders: mechanisms and emerging therapeutics targeting the microbiota-gut-brain axis. Pharmacol Ther. 2025;269:108831. doi:10.1016/j.pharmthera.2025.108831
23. Su S, Lewis TT, Belsky DW, et al. Impact of psychosocial stress in early life on pace of aging in young adulthood. Clin Clin Epigenet. 2025;17:186. doi:10.1186/s13148-025-02002-y
24. van Dalen M, van Gaalen MAC, Favejee MM, et al. Implementing routine medical and mental health screening in children and adolescents with inflammatory bowel disease. J Pediatr Gastroenterol Nutr. 2025;81:43–52. doi:10.1002/jpn3.70039
25. Cooney R, Tang D, Barrett K, Russell RK. Children and Young Adults With Inflammatory Bowel Disease Have an Increased Incidence and Risk of Developing Mental Health Conditions: a UK Population-Based Cohort Study. Inflamm Bowel Dis. 2024;30:1264–1273. doi:10.1093/ibd/izad169
26. Rasmussen J, Hansen ASK, Nørgård BM, et al. Mental Health Disorders in Patients with Inflammatory Bowel Disease Onset in Childhood or Youth - A Nationwide Cohort Study from Denmark. Clin Epidemiol. 2025;17:177–192. doi:10.2147/clep.S491881
27. Fairbrass KM, Gracie DJ, Ford AC. Relative Contribution of Disease Activity and Psychological Health to Prognosis of Inflammatory Bowel Disease During 6.5 Years of Longitudinal Follow-Up. Gastroenterology. 2022;163:190–203.e195. doi:10.1053/j.gastro.2022.03.014
28. Riva A, Arienti G, Zuin G, et al. Psychological symptoms and alexithymia in adolescents with inflammatory bowel diseases: a case-control study. Eur J Gastroenterol Hepatol. 2025;37:917–921. doi:10.1097/meg.0000000000002999
29. Schuman SL, Graef DM, Janicke DM, Gray WN, Hommel KA. An exploration of family problem-solving and affective involvement as moderators between disease severity and depressive symptoms in adolescents with inflammatory bowel disease. J Clin Psychol Med Settings. 2013;20:488–496. doi:10.1007/s10880-013-9368-x
30. Hill R, Lewindon P, Muir R, et al. Quality of life in children with Crohn disease. J Pediatr Gastroenterol Nutr. 2010;51:35–40. doi:10.1097/MPG.0b013e3181c2c0ef
31. Brooks AJ, Norman P, Peach EJ, et al. Prospective Study of Psychological Morbidity and Illness Perceptions in Young People With Inflammatory Bowel Disease. J Crohn’s Colitis. 2019;13:1003–1011. doi:10.1093/ecco-jcc/jjz028
32. Reed-Knight B, van Tilburg MAL, Levy RL, et al. Maladaptive Coping and Depressive Symptoms Partially Explain the Association Between Family Stress and Pain-Related Distress in Youth With IBD. J Pediatr Psychol. 2018;43:94–103. doi:10.1093/jpepsy/jsx082
33. Hieronymi C, Kaul K, de Laffolie J, Brosig B, On Behalf Of Cedata-Gpge A. Family Factors and the Psychological Well-Being of Children and Adolescents with Inflammatory Bowel Disease-An Exploratory Study. Children (Basel). 2025;12:575. doi:10.3390/children12050575
34. Touma N, Varay C, Baeza-Velasco C. Determinants of quality of life and psychosocial adjustment to pediatric inflammatory bowel disease: a systematic review focused on Crohn’s disease. J Psychosom Res. 2021;142:110354. doi:10.1016/j.jpsychores.2020.110354
35. Gray WN, Denson LA, Baldassano RN, Hommel KA. Treatment adherence in adolescents with inflammatory bowel disease: the collective impact of barriers to adherence and anxiety/depressive symptoms. J Pediatr Psychol. 2012;37:282–291. doi:10.1093/jpepsy/jsr092
36. Graff LA, Walker JR, Bernstein CN. Depression and anxiety in inflammatory bowel disease: a review of comorbidity and management. Inflamm Bowel Dis. 2009;15:1105–1118. doi:10.1002/ibd.20873
37. Meltzer LJ, Williamson AA, Mindell JA. Pediatric sleep health: it matters, and so does how we define it. Sleep Med Rev. 2021;57:101425. doi:10.1016/j.smrv.2021.101425
38. Kinnucan JA, Rubin DT, Ali T. Sleep and inflammatory bowel disease: exploring the relationship between sleep disturbances and inflammation. Gastroenterol Hepatol (N Y). 2013;9:718–727.
39. Cooney R, Barrett K, Russell RK. Impact of mental health comorbidity in children and young adults with inflammatory bowel disease: a UK population-based cohort study. BMJ Open. 2024;14:e080408. doi:10.1136/bmjopen-2023-080408
40. Moorman EL, Koskela-Staples NC, Janicke DM. A Systematic Review of Sleep Disturbances in Pediatric Inflammatory Bowel Disease. J Pediatr Psychol. 2023;48:267–282. doi:10.1093/jpepsy/jsac088
41. Jarasvaraparn C, Zlomke K, Vann NC, Wang B, Crissinger KD, Gremse DA. The Relationship Between Sleep Disturbance and Disease Activity in Pediatric Patients With Inflammatory Bowel Disease. J Pediatr Gastroenterol Nutr. 2019;68:237–243. doi:10.1097/mpg.0000000000002156
42. Gundogdu D, Urgancı N, Usta M. Relationship between disease activity index and sleep disorders in children with inflammatory bowel diseases. Eur J Pediatr. 2023;182:4095–4102. doi:10.1007/s00431-023-05081-2
43. Barry MJ, Nicholson WK, Silverstein M, et al. Screening for Depression and Suicide Risk in Adults: US Preventive Services Task Force Recommendation Statement. JAMA. 2023;329:2057–2067. doi:10.1001/jama.2023.9297
44. Gradus JL, Qin P, Lincoln AK, et al. Inflammatory bowel disease and completed suicide in Danish adults. Inflamm Bowel Dis. 2010;16:2158–2161. doi:10.1002/ibd.21298
45. Ludvigsson JF, Olén O, Larsson H, et al. Association Between Inflammatory Bowel Disease and Psychiatric Morbidity and Suicide: a Swedish Nationwide Population-Based Cohort Study With Sibling Comparisons. J Crohn’s Colitis. 2021;15:1824–1836. doi:10.1093/ecco-jcc/jjab039
46. Beaudoin K, Lo J, Mewhinney E, et al. Silent Struggles: uncovering Mental Health Burdens in Adolescents with Inflammatory Bowel Disease and Juvenile Idiopathic Arthritis-A Retrospective Chart Review. Children. 2025;12:995. doi:10.3390/children12080995
47. Xiong Q, Tang F, Li Y, et al. Association of inflammatory bowel disease with suicidal ideation, suicide attempts, and suicide: a systematic review and meta-analysis. J Psychosom Res. 2022;160:110983. doi:10.1016/j.jpsychores.2022.110983
48. Malham M, Jakobsen C, Paerregaard A, Virta LJ, Kolho KL, Wewer V. The incidence of cancer and mortality in paediatric onset inflammatory bowel disease in Denmark and Finland during a 23-year period: a population-based study. Aliment Pharmacol Ther. 2019;50:33–39. doi:10.1111/apt.15258
49. Butwicka A, Olén O, Larsson H, et al. Association of Childhood-Onset Inflammatory Bowel Disease With Risk of Psychiatric Disorders and Suicide Attempt. JAMA Pediatr. 2019;173:969–978. doi:10.1001/jamapediatrics.2019.2662
50. Hashash JG, Vachon A, Ramos Rivers C, et al. Predictors of Suicidal Ideation Among IBD Outpatients. J Clin Gastroenterol. 2019;53:e41–e45. doi:10.1097/mcg.0000000000001094
51. Riva A, Arienti G, Zuin G, et al. “Inside the Gut-Brain Axis”: psychological Profiles of Adolescents with Inflammatory Bowel Diseases and with Restrictive Eating Disorders. Nutrients. 2025;17:1706. doi:10.3390/nu17101706
52. Nakamura A, Jimbo K, Suzuki M, et al. Impact of Psychosocial and Neurodevelopmental Disorders on Pediatric Ulcerative Colitis: a Single-Center, Retrospective, Observational Study. Inflamm Bowel Dis. 2025;31:2495–2502. doi:10.1093/ibd/izaf034
53. Kim JY, Choi MJ, Ha S, et al. Association between autism spectrum disorder and inflammatory bowel disease: a systematic review and meta-analysis. Autism Res. 2022;15:340–352. doi:10.1002/aur.2656
54. Thavamani A, Umapathi KK, Khatana J, Gulati R. Burden of Psychiatric Disorders among Pediatric and Young Adults with Inflammatory Bowel Disease: a Population-Based Analysis. Pediatr Gastroenterol Hepatol Nutr. 2019;22:527–535. doi:10.5223/pghn.2019.22.6.527
55. Walker JR, Ediger JP, Graff LA, et al. The Manitoba IBD cohort study: a population-based study of the prevalence of lifetime and 12-month anxiety and mood disorders. Am J Gastroenterol. 2008;103:1989–1997. doi:10.1111/j.1572-0241.2008.01980.x
56. Kappel RK, Bisgaard TH, Poulsen G, Jess T. Risk of Anxiety, Depression, and Attention-Deficit/Hyperactivity Disorder in Pediatric Patients With Inflammatory Bowel Disease: a Population-Based Cohort Study. Clin Transl Gastroenterol. 2024;15:e00657. doi:10.14309/ctg.0000000000000657
57. Yang BZ, Han S, Kranzler HR, Farrer LA, Gelernter J. A genomewide linkage scan of cocaine dependence and major depressive episode in two populations. Neuropsychopharmacology. 2011;36:2422–2430. doi:10.1038/npp.2011.122
58. Nishimura T, Kubosaki A, Ito Y, Notkins AL. Disturbances in the secretion of neurotransmitters in IA-2/IA-2beta null mice: changes in behavior, learning and lifespan. Neuroscience. 2009;159:427–437. doi:10.1016/j.neuroscience.2009.01.022
59. Lasconi C, Pahl MC, Cousminer DL, et al. Variant-to-Gene-Mapping Analyses Reveal a Role for the Hypothalamus in Genetic Susceptibility to Inflammatory Bowel Disease. Cell Mol Gastroenterol Hepatol. 2021;11:667–682. doi:10.1016/j.jcmgh.2020.10.004
60. Pinakhina D, Yermakovich D, Vergasova E, et al. GWAS of depression in 4,520 individuals from the Russian population highlights the role of MAGI2 (S-SCAM) in the gut-brain axis. Front Genet. 2022;13:972196. doi:10.3389/fgene.2022.972196
61. Ge L, Liu S, Li S, et al. Psychological stress in inflammatory bowel disease: psychoneuroimmunological insights into bidirectional gut-brain communications. Front Immunol. 2022;13:1016578. doi:10.3389/fimmu.2022.1016578
62. Skonieczna-żydecka K, Marlicz W, Misera A, Koulaouzidis A, Łoniewski I. Microbiome-The Missing Link in the Gut-Brain Axis: focus on Its Role in Gastrointestinal and Mental Health. J Clin Med. 2018;7:521. doi:10.3390/jcm7120521
63. Masanetz RK, Winkler J, Winner B, Günther C, Süß P. The Gut-Immune-Brain Axis: an Important Route for Neuropsychiatric Morbidity in Inflammatory Bowel Disease. Int J Mol Sci. 2022;23:1111. doi:10.3390/ijms231911111
64. Wu WL, Adame MD, Liou CW, et al. Microbiota regulate social behaviour via stress response neurons in the brain. Nature. 2021;595:409–414. doi:10.1038/s41586-021-03669-y
65. Karin O, Raz M, Tendler A, et al. A new model for the HPA axis explains dysregulation of stress hormones on the timescale of weeks. Mol Syst Biol. 2020;16:e9510. doi:10.15252/msb.20209510
66. Bitton A, Dobkin PL, Edwardes MD, et al. Predicting relapse in Crohn’s disease: a biopsychosocial model. Gut. 2008;57:1386–1392. doi:10.1136/gut.2007.134817
67. Iob E, Kirschbaum C, Steptoe A. Persistent depressive symptoms, HPA-axis hyperactivity, and inflammation: the role of cognitive-affective and somatic symptoms. Mol Psychiatry. 2020;25:1130–1140. doi:10.1038/s41380-019-0501-6
68. Reber SO. Stress and animal models of inflammatory bowel disease--an update on the role of the hypothalamo-pituitary-adrenal axis. Psychoneuroendocrinology. 2012;37:1–19. doi:10.1016/j.psyneuen.2011.05.014
69. Qiu P, Ishimoto T, Fu L, Zhang J, Zhang Z, Liu Y. The Gut Microbiota in Inflammatory Bowel Disease. Front Cell Infect Microbiol. 2022;12:733992. doi:10.3389/fcimb.2022.733992
70. Jiang H, Ling Z, Zhang Y, et al. Altered fecal microbiota composition in patients with major depressive disorder. Brain Behav Immun. 2015;48:186–194. doi:10.1016/j.bbi.2015.03.016
71. Chinna Meyyappan A, Forth E, Wallace CJK, Milev R. Effect of fecal microbiota transplant on symptoms of psychiatric disorders: a systematic review. BMC Psychiatry. 2020;20:299. doi:10.1186/s12888-020-02654-5
72. Koh A, Bäckhed F. From Association to Causality: the Role of the Gut Microbiota and Its Functional Products on Host Metabolism. Mol Cell. 2020;78:584–596. doi:10.1016/j.molcel.2020.03.005
73. Khan R, Roy N, Ali H, Naeem M. Fecal Microbiota Transplants for Inflammatory Bowel Disease Treatment: synthetic- and Engineered Communities-Based Microbiota Transplants Are the Future. Gastroenterol Res Pract. 2022;2022:9999925. doi:10.1155/2022/9999925
74. Tian CM, Yang MF, Kong C, et al. Microbiome-Gut-Brain Axis: implications for the Links Between Inflammatory Bowel Disease and Neuropsychiatric Disorders. J Inflamm Res. 2025;18:13183–13212. doi:10.2147/jir.S514838
75. Westfall S, Caracci F, Estill M, Frolinger T, Shen L, Pasinetti GM. Chronic Stress-Induced Depression and Anxiety Priming Modulated by Gut-Brain-Axis Immunity. Front Immunol. 2021;12:670500. doi:10.3389/fimmu.2021.670500
76. Ballesio A, Santamaria T, Furio S, et al. Associations between immune biomarkers and symptoms of anxiety, depression, and insomnia in paediatric inflammatory bowel disease: a preliminary longitudinal analysis. Physiol Behav. 2024;278:114510. doi:10.1016/j.physbeh.2024.114510
77. McGregor L, Saunders SA, Hunter JA, Murphy E. Acute psychosis in three patients receiving anti-tumour necrosis factor-alpha therapy. Rheumatology. 2008;47:1254–1255. doi:10.1093/rheumatology/ken212
78. Afzal NA, Ozzard A, Keady S, Thomson M, Murch S, Heuschkel R. Infliximab delays but does not avoid the need for surgery in treatment-resistant pediatric Crohn’ disease. Dig Dis Sci. 2007;52:3329–3333. doi:10.1007/s10620-007-8102-1
79. Guo Y, Li J, Hu R, et al. Adalimumab-induced manic episode in an adolescent with juvenile idiopathic arthritis. BMC Psychiatry. 2024;24:596. doi:10.1186/s12888-024-06037-y
80. Jafri F, Sammut A. A rare case of suicidal ideation related to Adalimumab use. Open Access Rheumatol. 2018;10:113–115. doi:10.2147/oarrr.S168559
81. Wang Q, Roy B, Turecki G, Shelton RC, Dwivedi Y. Role of Complex Epigenetic Switching in Tumor Necrosis Factor-α Upregulation in the Prefrontal Cortex of Suicide Subjects. Am J Psychiatry. 2018;175:262–274. doi:10.1176/appi.ajp.2017.16070759
82. Hinnant L, Rios Villacorta N, Chen E, et al. Consensus Statement on Managing Anxiety and Depression in Individuals with Inflammatory Bowel Disease. Inflamm Bowel Dis. 2025;31:1248–1255. doi:10.1093/ibd/izae151
83. Mackner LM, Whitaker BN, Maddux MH, et al. Depression Screening in Pediatric Inflammatory Bowel Disease Clinics: recommendations and a Toolkit for Implementation. J Pediatr Gastroenterol Nutr. 2020;70:42–47. doi:10.1097/mpg.0000000000002499
84. Spekhorst LM, Hummel TZ, Benninga MA, van Rheenen PF, Kindermann A. Adherence to Oral Maintenance Treatment in Adolescents With Inflammatory Bowel Disease. J Pediatr Gastroenterol Nutr. 2016;62:264–270. doi:10.1097/mpg.0000000000000924
85. Scheier MF, Carver CS. Optimism, coping, and health: assessment and implications of generalized outcome expectancies. Health Psychol. 1985;4:219–247. doi:10.1037//0278-6133.4.3.219
86. Feldman ECH, Durkin LK, Greenley RN. Family Support is Associated with Fewer Adherence Barriers and Greater Intent to Adhere to Oral Medications in Pediatric IBD. J Pediatr Nurs. 2021;60:58–64. doi:10.1016/j.pedn.2021.01.026
87. Milo F, Imondi C, D’Amore C, et al. Short-term Psychodynamic Psychotherapy in Addition to Standard Medical Therapy Increases Clinical Remission in Adolescents and Young Adults with Inflammatory Bowel Disease: a Randomised Controlled Trial. J Crohn’s Colitis. 2024;18:256–263. doi:10.1093/ecco-jcc/jjad145
88. Michel HK, Boyle B, David J, et al. The Pediatric Inflammatory Bowel Disease Medical Home: a Proposed Model. Inflamm Bowel Dis. 2022;28:1420–1429. doi:10.1093/ibd/izab238
89. Kochetkova L, You D, Yeung STA, Mahmood D. Tolerability of Antidepressants in Adolescents With Inflammatory Bowel Disease: a Small Case Series. J Paediatr Child Health. 2025;61:1932–1934. doi:10.1111/jpc.70203
90. Uzzan S, Azab AN. Anti-TNF-α Compounds as a Treatment for Depression. Molecules. 2021. doi:10.3390/molecules26082368
91. Raison CL, Rutherford RE, Woolwine BJ, et al. A randomized controlled trial of the tumor necrosis factor antagonist infliximab for treatment-resistant depression: the role of baseline inflammatory biomarkers. JAMA Psychiatry. 2013;70:31–41. doi:10.1001/2013.jamapsychiatry.4
92. Stevens BW, Borren NZ, Velonias G, et al. Vedolizumab Therapy Is Associated with an Improvement in Sleep Quality and Mood in Inflammatory Bowel Diseases. Dig Dis Sci. 2017;62:197–206. doi:10.1007/s10620-016-4356-2
93. Sandborn WJ, Feagan BG, Fedorak RN, et al. A randomized trial of Ustekinumab, a human interleukin-12/23 monoclonal antibody, in patients with moderate-to-severe Crohn’s disease. Gastroenterology. 2008;135:1130–1141. doi:10.1053/j.gastro.2008.07.014
94. Shayowitz M, Bressler M, Ricardo AP, Grudnikoff E. Infliximab-induced Depression and Suicidal Behavior in Adolescent with Crohn’s Disease: case Report and Review of Literature. Pediatr Qual Saf. 2019;4:e229. doi:10.1097/pq9.0000000000000229
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Subjective Sleep Disruption and Mood Disorders are Associated with the Risk of Chronic Pain in Patients with Obstructive Sleep Apnea
Liu L, Li X, Xue P, Wu M, Zeng S, Dai Y, Zhou J
Nature and Science of Sleep 2022, 14:2023-2032
Published Date: 7 November 2022
Correlation Analysis Between Disease Activity and Anxiety, Depression, Sleep Disturbance, and Quality of Life in Patients with Inflammatory Bowel Disease
Yu R, Liu C, Zhang J, Li J, Tian S, Ding F, Liu Z, Wang T, Liu Z, Jiang C, Shi J, Wu K, Dong W
Nature and Science of Sleep 2023, 15:407-421
Published Date: 26 May 2023
The Effect of Mental Health Status and Family Function on Nonsuicidal Self-Injury: A Longitudinal Analysis of Chinese Children and Adolescents
Chen Y, Hu R, Xu X, Hong B, Zhang J, Jia P, Zhao L
Psychology Research and Behavior Management 2023, 16:4491-4500
Published Date: 2 November 2023
AI Technology panic—is AI Dependence Bad for Mental Health? A Cross-Lagged Panel Model and the Mediating Roles of Motivations for AI Use Among Adolescents
Huang S, Lai X, Ke L, Li Y, Wang H, Zhao X, Dai X, Wang Y
Psychology Research and Behavior Management 2024, 17:1087-1102
Published Date: 12 March 2024
Mushrooms, Microdosing, and Mental Illness: The Effect of Psilocybin on Neurotransmitters, Neuroinflammation, and Neuroplasticity
Kinderlehrer DA
Neuropsychiatric Disease and Treatment 2025, 21:141-155
Published Date: 29 January 2025