")
Back to Journals » Psychology Research and Behavior Management » Volume 16
The Effect of Mental Health Status and Family Function on Nonsuicidal Self-Injury: A Longitudinal Analysis of Chinese Children and Adolescents
Authors Chen Y, Hu R, Xu X, Hong B, Zhang J, Jia P, Zhao L
Received 11 August 2023
Accepted for publication 23 October 2023
Published 2 November 2023 Volume 2023:16 Pages 4491—4500
DOI https://doi.org/10.2147/PRBM.S429748
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Yuxin Chen,1,2,* Rui Hu,1,* Xinmao Xu,1 Binxue Hong,1 Jinquan Zhang,1 Peng Jia,3,4 Li Zhao1,2,4
1West China School of Public Health and West China Fourth Hospital, Sichuan University, Chengdu, People’s Republic of China; 2China-PUMC C.C. Chen Institute of Health, Sichuan University, Chengdu, People’s Republic of China; 3School of Resource and Environmental Sciences, Wuhan University, Wuhan, People’s Republic of China; 4International Institute of Spatial Lifecourse Health (ISLE), Wuhan University, Wuhan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Li Zhao, Email [email protected]
Background: Nonsuicidal self-injury (NSSI) is an overwhelming social problem in children and adolescents. Focusing on the change of NSSI behavior, including onset, cessation, and maintenance, is crucial to developing effective prevention and intervention strategies. This study explored the effect of mental health status (depressive and anxiety symptoms) and family function on NSSI.
Methods: The study sample comprised 7554 children and adolescents based on the first two rounds of the Chengdu Positive Child Development (CPCD) dataset in China. Depressive and anxiety symptoms measured mental health status. The self-reported questionnaires also assessed NSSI behaviors and family function. The interrelationship between NSSI behaviors, mental health status, and family function was evaluated. Logistic regression and linear regression were performed to examine the interrelationship between mental health status, family function and NSSI behaviors. Sensitivity analysis was performed.
Results: In this study, 2167 (28.69%) participants reported NSSI at baseline and 2101 (27.81%) at follow-up. Depression, anxiety, and family function were salient influential factors in the prevalence, onset, and cessation of NSSI. Parents’ accompaniment showed a significant effect on the prevalence of NSSI.
Conclusion: Depression, anxiety, family function, and parents’ accompaniment are all associated with NSSI behaviors. Strategies targeting mental health status and family function could effectively protect children and adolescents from NSSI behaviors.
Keywords: nonsuicidal self-injury, NSSI, depression, anxiety, family function, children, adolescent
Introduction
Self-injurious behavior includes direct and deliberate destruction of themselves, involving nonsuicidal self-injury (NSSI) and suicide attempts.1,2 While suicide attempts refer to the explicit intention to end one’s life, NSSI is defined as deliberately harming one’s body tissue without the intent to die.3 As NSSI may lead to increased risks of suicide, expected NSSI behavior involves cutting, hitting, scratching, burning oneself, etc.4–6
NSSI is a significant public health concern among children and adolescents.7,8 Since many adolescents reported engagement in NSSI behaviors at some point in their lives, researchers have found that the prevalence of NSSI steadily increases up to age 12, peaks between 14 and 16, and decreases at follow-up.7,9,10 In China, previous research has reported that the prevalence of NSSI among Chinese adolescents is over 20%.11 The early initiation and the high incidence of NSSI behavior are becoming severe societal problems in China.12 Following the robust evidence this study focuses on a critical period of NSSI and is based on Chinese children and adolescents.
While NSSI is a functional approach, previous studies indicate that a history of NSSI is related to a wide range of risk factors, such as depressive and anxiety symptoms, poor family support, and childhood maltreatment.13–15 Negative affect is closely associated with self-harm acts, and mental disorders are proven to be significant predictors of NSSI.16 Wilcox et al demonstrate that the diagnosis of depression predicts past-year NSSI and is associated with lifetime NSSI.17 And the frequency of NSSI behaviors is related to severe anxiety symptoms.18 According to the strong association with NSSI, depressive and anxiety signs were selected to represent participants’ mental health status in this study.
Various intrapersonal and interpersonal factors, including family function and family-related loneliness, directly increase the risk of NSSI behaviors.19–22 Learning how to manage their emotional reactivity was more difficult for people who were through childhood maltreatment, leading to poor problem-solving and communication skills.23 People with psychiatric disorders were more likely to commit NSSI to eliminate or escape challenging or stressful events with affective or social dysregulation.24 Family, especially parents, play a predominant role in protecting children and adolescents from childhood maltreatment. Since the family function and parents’ accompaniment could represent most of one’s subjective family environment, these factors’ relationship with NSSI should be explored.
As the predictive effect of vulnerability factors was studied repeatedly, most studies were focused on the onset and maintenance of NSSI.25,26 However, few studies have longitudinally explored the transformation process of NSSI behaviors, including the onset, maintenance, and cessation of self-harm. Tatnell et al have investigated the association between intrapersonal factors, interpersonal factors, and the change in NSSI behaviors and examined the effect of intrapersonal and interpersonal factors with the utilization of the mediating model.27 Clarifying the potential impacts of various vulnerability factors on the changes in NSSI behaviors is vital to determining effective strategies to protect people from NSSI behaviors and subsequent suicide attempts or implement the intervention in time.
As few studies have been conducted to research the relationship between risk factors and NSSI behaviors among Chinese children and adolescents, it is interesting to fill the research gap. To further research the relationship between various vulnerability factors and the transformation of NSSI behaviors in children and adolescents longitudinally, we hypothesized that participants with more depressive and anxiety symptoms, poorer family function and no parents’ accompaniment might find it easier to start or keep hurting themselves, and hardly cease NSSI during the survey. Moreover, different NSSI groups might lead to varying results of depression, anxiety and family function in participants. The onset, maintenance, and cessation of NSSI behaviors were studied dynamically in our research. Furthermore, the interrelationship between depression, anxiety, family function, parents’ accompaniment and the NSSI groups were explored in the present study.
Materials and Methods
Participants
The study sample was from the Chengdu Positive Child Development (CPCD) survey. Using a random cluster sampling procedure, the dynamic cohort was designed to investigate associations among students’ sociodemographic, physical and psychological characteristics, family environment, lifestyle behaviors, academic performance, and health status. The survey was conducted in five primary and middle schools in Chengdu, China. Between 23 December 2019 and 13 January 2020, 8825 students aged 6–16 were recruited in the cohort study, while the follow-up survey of 7985 students responded was conducted between 16 June and 8 July 2020. Overall, 10,371 students have been invited to participate in the survey. The invited participants included all students and their parents from selected schools. During the data collection, two well-trained research assistants were present in each classroom to give the exact instructions and ensure participants completed the questionnaires independently. The average data collection session for each participant was about 10 min, and participants should return questionnaires to the researcher immediately after completion. The research team would keep all the data confidential without revealing any personal information in the research output. This research is being carried out in conformity with the Helsinki Declaration’s principles, and written informed consent was obtained from the study participants legal guardians. Prior to the start of the study, all programs were ethically authorized by Sichuan University’s Ethics Committee to ensure that the study adhered to national and international human research standard (Grant No. K2020025). The published cohort profile revealed more details about the CPCD study.28
This study focused on the NSSI behaviors that occurred in children and adolescents in two waves. It was hypothesized that the self-harm behaviors were associated with depression, anxiety, family function, and parents’ accompaniment. Furthermore, the predictive effect of follow-up NSSI was explored among the included study scales’ scores at baseline. According to the study hypothesis, the sample of this study consisted of 7554 (3847 males and 3694 females, 48.90% female participants) children and adolescents who completed the integrated questionnaire at baseline and follow-up. The age range of the enrolled respondents was 7–20 years old (M=11.80, SD=2.14).
The study subject who did not self-injure through the cohort study was designed as the control group (n=4505), while those who reported NSSI at both baseline and follow-up were defined as the maintaining group (n=1219). Participants who engaged in NSSI at baseline but reported no history at follow-up were considered the cessation group (n=948). In contrast, individuals with no history at baseline but reported the episode at follow-up were the onset group (n=882).
Outcome Variable
NSSI, which was the predominant variable in this study, was measured by the Deliberate Self-Harm Inventory (DSHI) which includes 9 questions, such as “Did you hurt yourself by means on purpose?” and the frequency was provided on a 4-point Likert scale (Never, 1 time, 2 times, and ≥3 times).29 The precondition for the definition of self-harm behavior is without the intention to die, and those self-injurious behaviors include cutting, burning, scratching, biting, and punching. Qualified test-retest reliability and validity were verified with an alpha coefficient average of 0.755 previously.30 For the current sample, Cronbach’s alpha=0.856.
To measure depressive symptoms in children and adolescents, the Center for Epidemiological Studies Depression Scale for Children (CES-DC) was used to obtain estimates of symptom prevalence and screen psychiatric disorders in the past two weeks.31 The scale consists of 20 items on a 4-point Likert scale (1=<1 day, Rarely or None of the Time, 2=1~2 days, Some or Little of the Time, 3= 3~4 days, Moderately or Much of the time, 4= 5~7 days, Most or Almost All the Time). The reliability and validity were examined and showed an overall alpha coefficient of 0.89 in a previous study.32 This sample had Cronbach’s α=0.885.
While childhood anxiety disorders were defined in the Diagnostic and Statistical Manual of Mental Disorders (DSM), the Screen for Child Anxiety-Related Emotional Disorders (SCARED) was devised to measure DSM-defined anxiety disorder symptoms.33,34 The questionnaire records anxiety-related feelings in the recent two weeks on a 3-point Likert scale (0=Never, 1=Sometimes, 2=Often). Good internal consistency and discriminant validity have been demonstrated before35 and in the current sample (α=0.950).
With specific reference to Chinese culture, The Chinese Family Assessment Instrument (C-FAI) was appropriate for assessing Chinese family functioning.36 Questions in the questionnaire, for example, “the family members support each other” and “there are frictions between family members”, were presented to explore the feelings of offspring toward their parents and the whole family, including both positive and negative sides. Each statement is scored on a 5-point Likert scale (1=strongly similar, 5=strongly dissimilar). The factorial invariance of the instrument was examined in terms of factor pattern, factor loadings, and intercepts by the constructor. Excellent internal consistency was demonstrated previously.37 The sample showed strong internal character with Cronbach’s α=0.938.
Additionally, one specific question, “Fill in the blank with your family who live with you recently”, was designed to ensure whether participants have their parents’ accompaniment. The multiple-choice question has 9 choices, including father, mother, paternal grandfather, paternal grandmother, maternal grandfather, maternal grandmother, stepfather, stepmother, and others (fill in the blank). It was possible to assess if participants were accompanied by their parents for some time. In the categorization process, the stepfather was equivalent to the father, and so was the stepmother. The question was incorporated in this study and participants were divided into 4 different groups (accompanied by both parents, accompanied by father, accompanied by mother, and without parents’ accompaniment) by the responses.
Statistical Analysis
The descriptive statistical analysis was conducted at first. To assess differences across time within and between the four defined groups, doubly multivariate analyses of variance were performed after we confirmed that the variables conform to a normal distribution. As the existence of variation in group size, we selected Pillai’s trace to report, and the Bonferroni correction was used for post hoc comparisons.38 Furthermore, Spearman correlation analyses were used to examine the relationship between age and the DSHI, CES-DC, SCARED, and C-FAI scores, which were presented as one correlation matrix. Three logistic analyses were performed to explore the predictive effect of selective scales on NSSI, controlling for gender and age. The independent variables were the baseline results of CES-DC, SCARED, C-FAI, and the parents’ accompaniment question. The logistic analyses were used to establish the relationship between the independent variables and the presence of NSSI (who reported any history of NSSI behaviors during the survey), the onset of NSSI, and the cessation of NSSI, respectively. Additionally, linear regression analyses were utilized reversely to evaluate the interrelationship between NSSI groups and the three scales. Sensitivity analysis was performed by entering the follow-up values in the logistic and linear regression. The significance of the results was set at α=0.05 for all statistical analyses. The collected data was analyzed using SPSS version 26.0.
Results
Demographic Profile of Study Participants
Of 7554 children and adolescents who engaged in this survey, 2167 (28.69%) participants reported NSSI at baseline and 2101 (27.81%) at follow-up. The gender difference was discovered through the survey; females had a higher rate of NSSI at baseline (χ²(2)=6.83, p=0.03) and follow-up (χ²(2)=31.33, p<0.01), and it was controlled in all following analyses to address the imbalance. At baseline, three kinds of NSSI behaviors occurred most frequently. A total of 1115 students (14.8%) had bitten themselves, 864 (11.4%) had cut themselves, and 822 (10.9%) reported blood or scars on their bodies caused by self-cutting. Similarly, most students conducted the same three self-harm behaviors at follow-up. 1141 participants (15.1%) bit themselves, 1035 (13.7%) cut themselves, and 936 (12.4%) cut themselves and caused blood or scarring. According to the mean score of each item in the CES-DC, a lot of students have reported that they often/always feel like they were worse than others (57.8% at baseline), and lots of students often/always refuse to believe anything good would happen to them (69.6% at baseline). Many participants declare they dislike being with anyone unfamiliar (53.9% at baseline) in SCARED. Additionally, many students reported friction between family members (35.8% at baseline) and parents’ marriage problems (34.5% at baseline) in C-FAI.
Comparison Across Time Within and Between NSSI Groups
Based on the normal distribution that the variables fit, incorporating the quantitative variables of CES-DC, SCARED and C-FAI, the main effect of NSSI groups was observed (V=0.27, F (9, 22,650) =250.76, p<0.01, η²=0.09), and the effect of time was discovered (V=0.01, F (3, 7548) =28.64, p<0.01, η²=0.01). Meanwhile, there was a significant effect of interaction (V=0.06, F (9, 22,650) =52.81, p<0.01, η²=0.02).
For CES-DC, a significant interactive effect was reported (F (3, 7550) =97.70, p<0.01, η²=0.04). The interactive effect of SCARED was shown (F (3, 7550) =118.20, p<0.01, η²=0.05), while the result of C-FAI was presented (F (3, 7550) =37.26, p<0.01, η²=0.02). By group, the mean and standard deviation of variables of interest at baseline and follow-up and the results of doubly multivariate analyses were presented in Table 1. The intercorrelations of included variables were depicted with significant correlations in Table 2.
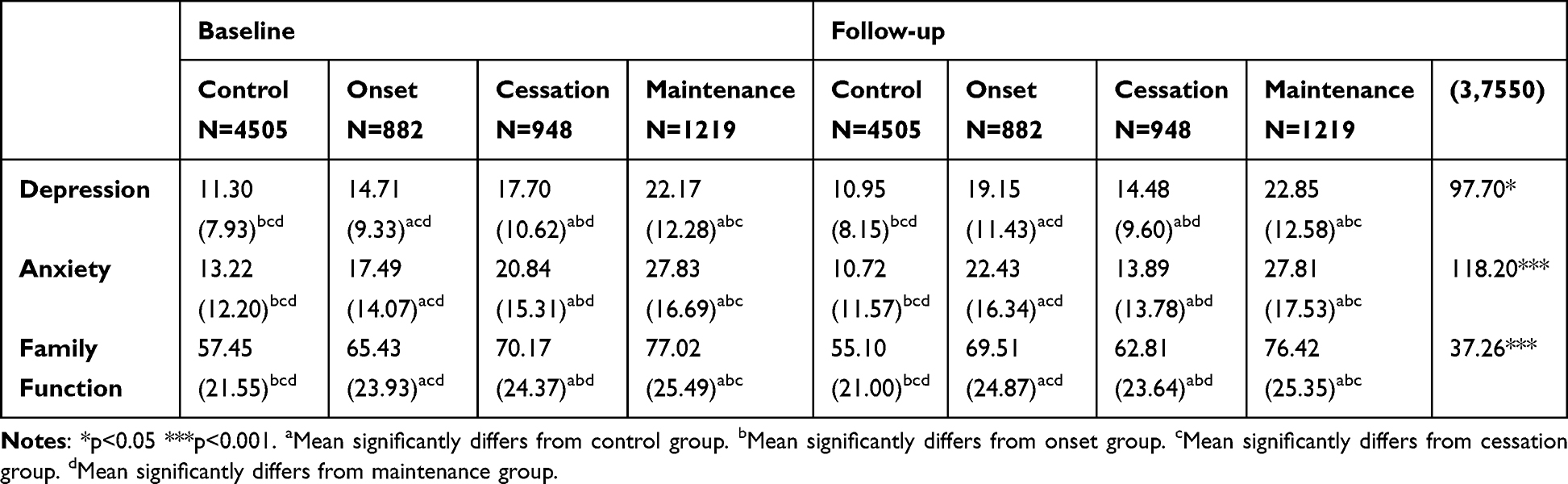 |
Table 1 Mean (Standard Deviation) of Variables of Interest at Baseline and Follow-Up, by Group |
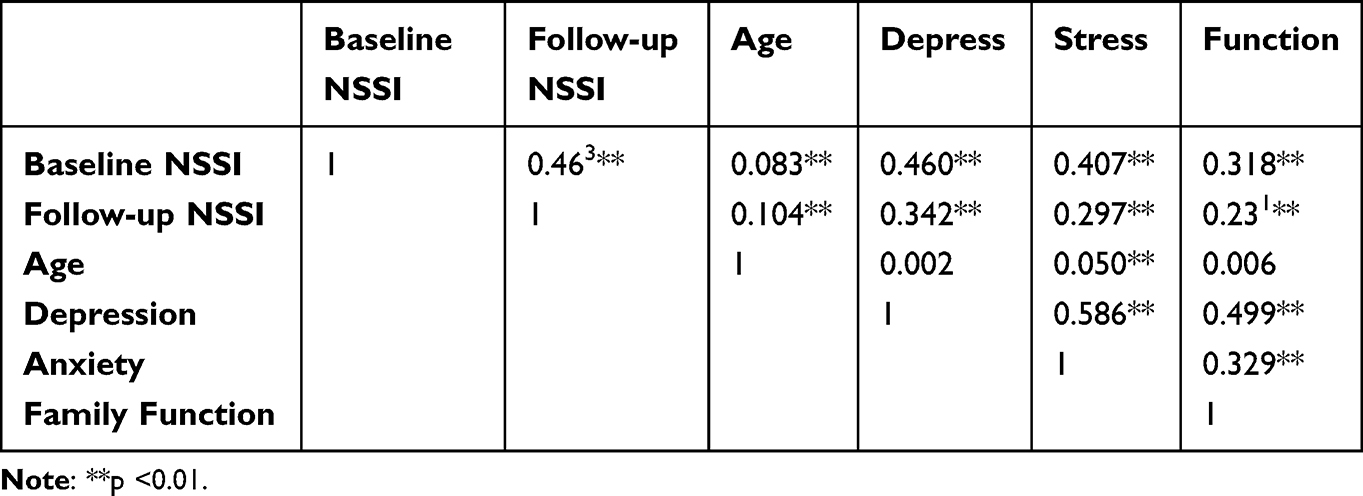 |
Table 2 Correlation Matrix |
In the post-hoc tests, individuals who chose to start NSSI during the research period had higher rates of depression and anxiety syndrome including a worse family environment. Contrastingly, children and adolescents who ceased to hurt themselves reported better psychological status and family function. Most significantly, the maintenance group scored higher on the three scales than the control group. All the comparisons have statistical significance with p<0.01.
Across two survey rounds, the estimated marginal means of depression, anxiety, and family function significantly increased in the onset group. On the opposite, the values of the cessation group decreased during the period.
Logistic Regression Analysis Revealing Effect on NSSI
One logistic regression was conducted to evaluate the related factors to the prevalence of NSSI during the two-wave survey. The outcome variable was binary, distinguishing participants without any history of NSSI (the control group) from those who reported NSSI through the survey (the maintenance group, onset group, and cessation group). In terms of results, poor psychological status and frequent family conflict indicate the occurrence of self-injury. While depression (OR = 1.05 [95% CI: 1.04–1.06]) and anxiety (OR = 1.02 [95% CI: 1.02–1.03]) symptoms were positively associated with NSSI, poor family environment (OR = 1.01 [95% CI: 1.01–1.02]) has qualified association with NSSI. Specifically, whether parents had accompanied their kids (OR = 1.34 [95% CI: 1.15–1.56]) has a robust connection with NSSI, as Table 3 shows.
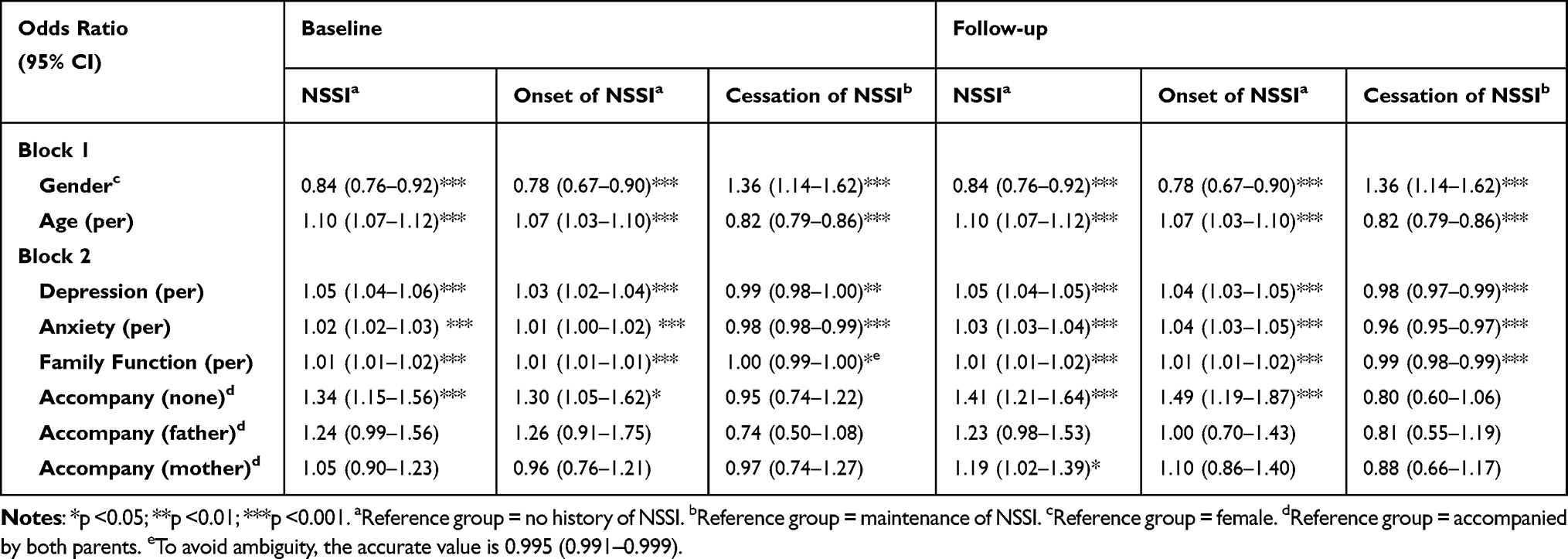 |
Table 3 Logistic Regressions for Primary Analysis (Baseline) and Sensitivity Analysis (Follow-Up) |
The second logistic regression explored the differences between participants who begin NSSI at follow-up (the onset group) and those who never hurt themselves during the survey (the control group). Children and adolescents who got higher scores in the depression (OR = 1.03 [95% CI: 1.02–1.04]) and anxiety (OR = 1.01 [95% CI: 1.00–1.02]) questionnaires were more likely to develop NSSI. Negative family estimation (OR = 1.01 [95% CI: 1.01–1.01]) was associated with self-injury, while parent companion has an insignificant effect.
The third logistic regression was analyzed to assess the difference between individuals who ceased NSSI at follow-up (the cessation group) and those who kept hurting themselves during the study (the maintenance group). As a result, less anxiety (OR = 0.98 [95% CI: 0.98–0.99]) had a reliable association with NSSI cessation. Meanwhile, little depressive symptoms (OR = 0.99 [95% CI: 0.98–1.00]) and positive family function (OR = 1.00 [95% CI: 0.99–1.00]) were capable of indicating the suspension of self-injury behavior.
The sensitivity analysis further investigated the association between independent variables and NSSI groups in the three logistic regressions, using the follow-up scores of depression, anxiety, family function and parental accompaniment. Compared to the primary analysis, similar results were demonstrated in Table 3. The results indicated that the intercorrelation was stable across time.
Linear Regression Analysis Evaluating the Opposite Directional Relationship
Three linear regressions have been conducted to evaluate the effect of different NSSI groups on variables. As the control group of NSSI was a control, we transformed the NSSI group, which is a categorical variable, into dummy variables. We assessed the effect on depression, anxiety and family function separately. Like the logistic regression analyses, all the linear regression has reported great model fit and significant association between variables. In the three regressions on dependent variables, the maintenance group showed the most potent effect on depression (β=11.08, p<0.001), anxiety (β=14.44, p<0.001) and family function(β=20.11, p<0.001), which is rational. The regression in follow-up values also reported significant results. The results are presented in Table 4.
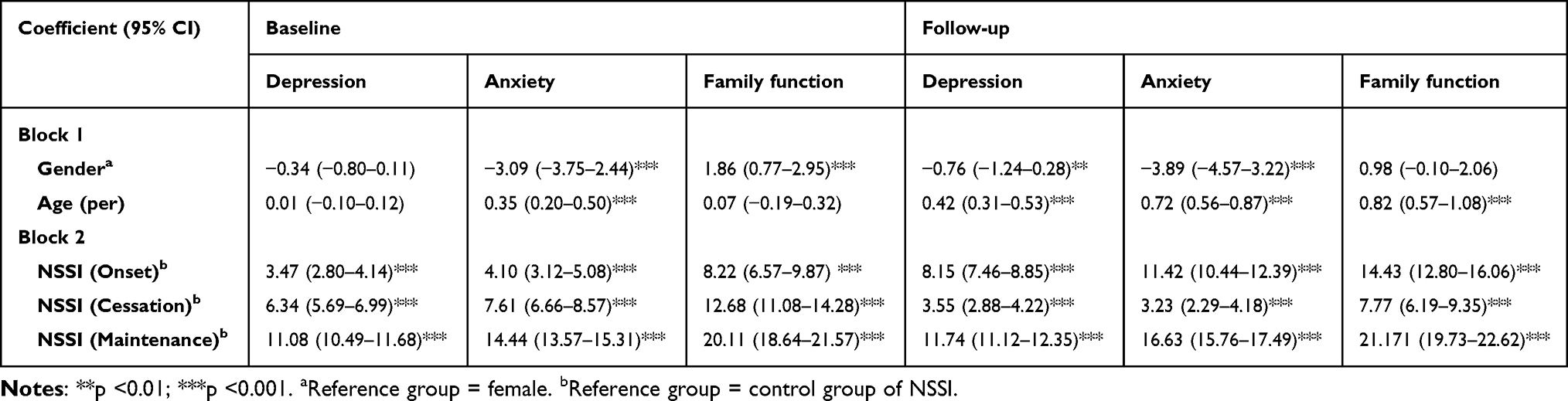 |
Table 4 Linear Regression for Primary Analysis (Baseline) and Sensitivity Analysis (Follow-Up) |
Discussion
The results support our contentions that poorer mental status (more depressive and anxiety symptoms) and worse family environment (poor family function and without parents’ accompaniment) are positively associated with the onset and maintenance of NSSI and negatively related to NSSI cessation. Additionally, the result of logistic regression demonstrated that being accompanied by both parents could reduce the prevalence of NSSI.
While depression and anxiety were labeled as the symbol of the mental health status of children and adolescents, typically, they were salient influential factors in all the regressions. Participants with more anxiety or depression symptoms were more likely to engage in NSSI. Reciprocally, compared with the NSSI control group, participants who conducted or maintained NSSI behaviors during the survey tended to have more depressive and anxiety symptoms, and students who ceased to hurt themselves would own better mental health. Our results have been confirmed in other studies on NSSI. Depression, which means more negative emotions for individuals, could lead to the conduction of NSSI due to the deficit of emotion regulation.39–41 Similarly, anxiety has been proven to have a strong connection with NSSI and even suicide attempts.42,43 This significant interrelationship might be explained by the fact that NSSI was treated as a coping strategy to regulate unwanted and/or intolerable disgust.44 Additionally, in our study, worse mental health status means less probability of NSSI cessation, leading to the fact that students with mental illnesses are inclined to maintain self-harm behaviors.
Consistent with the theoretical hypotheses that invalidating family environments increases vulnerability toward self-destructive behavior, poor family function and family-related loneliness are reciprocally associated with NSSI in children and adolescents.45 On the one hand, poor family function often indicates the occurrence of child maltreatment and leads to the presence of NSSI.46–48 Self-injuries were more impulsive and aggressive, which means they might decide without a second thought, like releasing stress by hurting themselves.18 On the other hand, the emotional bond between parents and offspring and the family-based social support were constructed based on parents’ accompaniment. These vulnerability factors indicated NSSI in children and adolescents.18,49,50 Specifically, few researchers have explored the direct effect of parents’ accompaniment, which existed as a significant influential factor of NSSI prevalence in our study.
Unexpectedly, some of our analysis results presented a contradictive outcome. First, although quite a few publications have demonstrated that gender difference does not exist in the prevalence of NSSI, girls reported higher NSSI prevalence than boys in our sample.51 This finding could be explained by the higher social stress on female students, like exaggerated social comparisons of physical appearance and body image. Girls are more sensitive to interpersonal relationships and more inclined to hide negative emotions.52 While age plays a moderate role, gender difference deserves more attention.37,53 Second, while previous research claims that the quality of the relationship with the mother was an essential factor associated with the presence of NSSI, the result of this study contradicts the claim.48 The result of logistic regressions showed that whether a separate father or mother accompanied students did not significantly predict the occurrence of NSSI. Only the accompaniment by both parents could reduce the risk of NSSI in children and adolescents. As the parent-child separation might form long-term deficits in perceptions of control and helplessness towards challenging situations among children and adolescents, participants without parents’ accompaniment might be poor at emotion regulation and then engage in NSSI behavior, which is a functional approach.54
We used a random cluster sampling method to choose the five primary and middle schools in Chengdu city, and all the students in the extracted schools were included in this survey, so the large sample size and religious sampling method could agree with the robust representativeness of children and adolescents in China. Therefore, the suggestions which are proposed in this study should apply to most children and adolescents in China. Although the bi-directional effect has been validated in our research, clinical efforts should be focused on preventing students from starting NSSI behaviors. Students without any history of NSSI deserve to pay more attention to their’ mental health and organize courses to release stress. While students severe with mental health issues were found, corresponding measures should be adopted, such as placing psychiatrists for those with severe mental issues and having teachers educate those with minor psychological problems. Based on schools’ schedules, regular questionnaire surveys and home visits are essential to know the family environment of students and then arrange reasonable parent meetings to improve the parent-child relationship. For intervention strategies, face-to-face psychological surgery would help those who conducted self-hurting, and their parents should have positive child growth courses. Exploring and healing the inside of students is the essence of NSSI treatment. Additionally, although parents’ accompaniment did not significantly affect onset and cessation groups, prevention and intervention strategies should not be neglected.
The limitations of our study are noteworthy and necessary to be improved in further research. Firstly, based on the existing survey we did, the study did not include all the potential risk factors reported in the previous study and confounding factors except for gender and age. We only chose the most salient characteristics among the various scales. To further explore the influential effect of NSSI, other related factors, like family financial situation and parents’ education level, should be employed in future research. Secondly, we relied solely on students’ self-report results, which might be subject to recall bias, social desirability, and single-rater bias. For example, even though the CES-D scale is a validated instrument, it is limited to depressive symptoms screening and it is difficult to make a depression diagnosis through the assistance of mental health professionals. The views of guardians and students might differ in family function.55 Also, whether participants have parents’ accompaniment may not represent the parent-child relationship, as remote communication devices are developed today. However, it is a meaningful question on the side of family construction and could be utilized to observe students’ family environments. Future studies should try to solve the problems using more reasonable and sensible assessment tools. Thirdly, applying our study results to different populations, like clinical patients, should be cautious, as we conducted the research among school students in the city. Fourthly, while the scales could only assess the recent status of participants limited to a short time, the six-month gap between the two waves might weaken the association we validated. The potential differences in results at different time points could cause bias, and future research should not neglect this problem. Finally, while this study only utilized two waves of data due to the survey limitation, future studies should try to build a more extended cohort study to verify the influential effects over time.
Conclusion
Our study demonstrated the relationship between mental health status, family environment, and NSSI behaviors among children and adolescents. More depressive and anxiety symptoms, poor family function, and fewer parents’ accompaniment were closely associated with the prevalence of NSSI behaviors. To protect students from NSSI behaviors, more strategies could focus on preventing students from depressive and anxiety symptoms and developing their family function; also, getting children and adolescents more accompaniment from their parents would help. Psychological courses and surgery for students, followed by home visits and parents’ education would assist in protecting children and adolescents from NSSI.
Data Sharing Statement
Available data that support this study could be provided by the corresponding author upon reasonable request.
Acknowledgments
Yuxin Chen and Rui Hu are co-first authors for this study. We thank all participants especially Prof. Daniel T.L. Shek who made this study possible.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by the National Natural Science Foundation of China (Grant No. 82273748).
Disclosure
The authors declare that the research was conducted without any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Linehan MM. Behavioral treatments of suicidal behaviors. Definitional obfuscation and treatment outcomes. Ann N Y Acad Sci. 1997;836:302–328. doi:10.1111/j.1749-6632.1997.tb52367.x
2. O’Carroll PW, Berman AL, Maris RW, Moscicki EK, Tanney BL, Silverman MM. Beyond the tower of babel: a nomenclature for suicidology. Suicide Life Threat Behav. 1996;26(3):237–252. doi:10.1111/j.1943-278X.1996.tb00609.x
3. Nock MK, Joiner TE, Gordon KH, Lloyd-Richardson E, Prinstein MJ. Non-suicidal self-injury among adolescents: diagnostic correlates and relation to suicide attempts. Psychiatry Res. 2006;144(1):65–72. doi:10.1016/j.psychres.2006.05.010
4. Lloyd-Richardson EE, Perrine N, Dierker L, Kelley ML. Characteristics and functions of non-suicidal self-injury in a community sample of adolescents. Psychol Med. 2007;37(8):1183–1192. doi:10.1017/s003329170700027x
5. Swannell S, Martin G, Hazell P, Harrison J, Taylor A. Australian national epidemiological study of self injury (Anessi); 2008.
6. Whitlock J, Muehlenkamp J, Eckenrode J, et al. Nonsuicidal self-injury as a gateway to suicide in young adults. J Adoles Health. 2013;52(4):486–492. doi:10.1016/j.jadohealth.2012.09.010
7. Plener PL, Schumacher TS, Munz LM, Groschwitz RC. The longitudinal course of non-suicidal self-injury and deliberate self-harm: a systematic review of the literature. Borderline Personal Disord Emot Dysregul. 2015;2:2. doi:10.1186/s40479-014-0024-3
8. Barrocas AL, Hankin BL, Young JF, Abela JR. Rates of nonsuicidal self-injury in youth: age, sex, and behavioral methods in a community sample. Pediatrics. 2012;130(1):39–45. doi:10.1542/peds.2011-2094
9. Muehlenkamp JJ, Claes L, Havertape L, Plener PL. International prevalence of adolescent non-suicidal self-injury and deliberate self-harm. Child Adolesc Psychiatry Ment Health. 2012;6:10. doi:10.1186/1753-2000-6-10
10. Taliaferro LA, Muehlenkamp JJ. Risk factors associated with self-injurious behavior among a national sample of undergraduate college students. J Am Coll Health. 2015;63(1):40–48. doi:10.1080/07448481.2014.953166
11. Lang J, Yao Y. Prevalence of nonsuicidal self-injury in Chinese middle school and high school students: a meta-analysis. Medicine. 2018;97(42):e12916. doi:10.1097/md.0000000000012916
12. Xu H, Jiang Z, Li S, et al. Differences in influencing factors between non-suicidal self-injury and suicide attempts in Chinese adolescents: the role of gender. Front Psychiatry. 2022;13:870864. doi:10.3389/fpsyt.2022.870864
13. Cox LJ, Stanley BH, Melhem NM, et al. A longitudinal study of nonsuicidal self-injury in offspring at high risk for mood disorder. J Clin Psychiatry. 2012;73(6):821–828. doi:10.4088/JCP.11m07250
14. Nock MK. Why do people hurt themselves? New insights into the nature and functions of self-injury. Curr Dir Psychol Sci. 2009;18(2):78–83. doi:10.1111/j.1467-8721.2009.01613.x
15. Garisch JA, Wilson MS. Prevalence, correlates, and prospective predictors of non-suicidal self-injury among New Zealand adolescents: cross-sectional and longitudinal survey data. Child Adolesc Psychiatry Ment Health. 2015;9(28). doi:10.1186/s13034-015-0055-6
16. Hepp J, Carpenter RW, Störkel LM, Schmitz SE, Schmahl C, Niedtfeld I. A systematic review of daily life studies on non-suicidal self-injury based on the four-function model. Clin Psychol Rev. 2020;82:101888. doi:10.1016/j.cpr.2020.101888
17. Wilcox HC, Arria AM, Caldeira KM, Vincent KB, Pinchevsky GM, O’Grady KE. Longitudinal predictors of past-year non-suicidal self-injury and motives among college students. Psychol Med. 2012;42(4):717–726. doi:10.1017/s0033291711001814
18. Di Pierro R, Sarno I, Perego S, Gallucci M, Madeddu F. Adolescent nonsuicidal self-injury: the effects of personality traits, family relationships and maltreatment on the presence and severity of behaviours. Eur Child Adolesc Psychiatry. 2012;21(9):511–520. doi:10.1007/s00787-012-0289-2
19. Plener PL, Libal G, Keller F, Fegert JM, Muehlenkamp JJ. An international comparison of adolescent non-suicidal self-injury (Nssi) and suicide attempts: Germany and the USA. Psychol Med. 2009;39(9):1549–1558. doi:10.1017/s0033291708005114
20. Giletta M, Scholte RH, Engels RC, Ciairano S, Prinstein MJ. Adolescent non-suicidal self-injury: a cross-national study of community samples from Italy, the Netherlands and the United States. Psychiatry Res. 2012;197(1–2):66–72. doi:10.1016/j.psychres.2012.02.009
21. Tang WC, Lin MP, You J, Wu JY, Chen KC. Prevalence and psychosocial risk factors of nonsuicidal self-injury among adolescents during the covid-19 outbreak. Curr Psychol. 2021;1–10. doi:10.1007/s12144-021-01931-0
22. Nock MK, Mendes WB. Physiological Arousal, distress tolerance, and social problem-solving deficits among adolescent self-injurers. J Consult Clin Psychol. 2008;76(1):28–38. doi:10.1037/0022-006x.76.1.28
23. Kaufman J, Charney D. Effects of early stress on brain structure and function: implications for understanding the relationship between child maltreatment and depression. Dev Psychopathol. 2001;13(3):451–471. doi:10.1017/s0954579401003030
24. Nock MK, Prinstein MJ. A functional approach to the assessment of self-mutilative behavior. J Consult Clin Psychol. 2004;72(5):885–890. doi:10.1037/0022-006x.72.5.885
25. Hankin BL, Abela JR. Nonsuicidal self-injury in adolescence: prospective rates and risk factors in a 2½ year longitudinal study. Psychiatry Res. 2011;186(1):65–70. doi:10.1016/j.psychres.2010.07.056
26. Serafini G, Canepa G, Adavastro G, et al. The relationship between childhood maltreatment and non-suicidal self-injury: a systematic review. Front Psychiatry. 2017;8:149. doi:10.3389/fpsyt.2017.00149
27. Tatnell R, Kelada L, Hasking P, Martin G. Longitudinal analysis of adolescent nssi: the role of intrapersonal and interpersonal factors. J Abnorm Child Psychol. 2014;42(6):885–896. doi:10.1007/s10802-013-9837-6
28. Zhao L, Shek DTL, Zou K, Lei Y, Jia P. Cohort profile: Chengdu positive child development (Cpcd) survey. Int J Epidemiol. 2022;51(3):e95–e107. doi:10.1093/ije/dyab237
29. Gratz KL. Measurement of deliberate self-harm: preliminary data on the deliberate self-harm inventory. J Psychopathol Behav Assess. 2001;23(4):253–263. doi:10.1037/t04163-000
30. Bjärehed J, Lundh LG. Deliberate self-harm in 14-year-old adolescents: how frequent is it, and how is it associated with psychopathology, relationship variables, and styles of emotional regulation? Cogn Behav Ther. 2008;37(1):26–37. doi:10.1080/16506070701778951
31. Faulstich ME, Carey MP, Ruggiero L, Enyart P, Gresham F. Assessment of depression in childhood and adolescence: an evaluation of the center for epidemiological studies depression scale for children (Ces-Dc). Am J Psychiatry. 1986;143(8):1024–1027. doi:10.1176/ajp.143.8.1024
32. Fendrich M, Weissman MM, Warner V. Screening for depressive disorder in children and adolescents: validating the center for epidemiologic studies depression scale for children. Am J Epidemiol. 1990;131(3):538–551. doi:10.1093/oxfordjournals.aje.a115529
33. Birmaher B, Khetarpal S, Brent D, et al. The screen for child anxiety related emotional disorders (scared): scale construction and psychometric characteristics. J Am Acad Child Adolesc Psychiatry. 1997;36(4):545–553. doi:10.1097/00004583-199704000-00018
34. Edition F. Diagnostic and statistical manual of mental disorders. Am Psychiatric Assoc. 2013;21(21):591–643. doi:10.1176/appi.books.9780890425787
35. Birmaher B, Brent DA, Chiappetta L, Bridge J, Monga S, Baugher M. Psychometric properties of the screen for child anxiety related emotional disorders (Scared): a replication study. J Am Acad Child Adolesc Psychiatry. 1999;38(10):1230–1236. doi:10.1097/00004583-199910000-00011
36. Shek DT, Ma CM. The Chinese family assessment instrument (C-Fai) hierarchical confirmatory factor analyses and factorial invariance. Res Soc Work Pract. 2010;20(1):112–123. doi:10.1177/1049731509355145
37. Law BM, Shek DT. Self-harm and suicide attempts among young Chinese adolescents in hong kong: prevalence, correlates, and changes. J Pediatr Adolesc Gynecol. 2013;26(3 Suppl):S26–32. doi:10.1016/j.jpag.2013.03.012
38. Tabachnick BG, Fidell LS, Ullman JB. Using Multivariate Statistics. Boston, MA: Pearson; 2007.
39. Klonsky ED, Muehlenkamp JJ. Self-injury: a research review for the practitioner. J Clin Psychol. 2007;63(11):1045–1056. doi:10.1002/jclp.20412
40. Fliege H, Lee JR, Grimm A, Klapp BF. Risk factors and correlates of deliberate self-harm behavior: a systematic review. J Psychosom Res. 2009;66(6):477–493. doi:10.1016/j.jpsychores.2008.10.013
41. Clapham R, Brausch A. Emotion regulation deficits across the spectrum of self-harm. Death Stud. 2022;46(10):2477–2484. doi:10.1080/07481187.2021.1972366
42. Chartrand H, Sareen J, Toews M, Bolton JM. Suicide attempts versus nonsuicidal self-injury among individuals with anxiety disorders in a nationally representative sample. Depress Anxiety. 2012;29(3):172–179. doi:10.1002/da.20882
43. Kokaliari ED, Roy AW, Koutra K. A cross-sectional study comparing predictors of non-suicidal self-injury among college students in the United States and Greece. Int J Cult Ment Health. 2017;10(1):50–61. doi:10.1080/17542863.2016.1259339
44. Hu Z, Yu H, Zou J, Zhang Y, Lu Z, Hu M. Relationship among self-injury, experiential avoidance, cognitive fusion, anxiety, and depression in Chinese adolescent patients with nonsuicidal self-injury. Brain Behav. 2021;11(12):e2419. doi:10.1002/brb3.2419
45. Martin J, Bureau J-F, Cloutier P, Lafontaine M-F. A comparison of invalidating family environment characteristics between university students engaging in self-injurious thoughts & actions and non-self-injuring university students. J Youth Adol. 2011;40(11):1477–1488. doi:10.1007/s10964-011-9643-9
46. Zhang H, Han T, Ma S, et al. Association of child maltreatment and bullying victimization among Chinese adolescents: the mediating role of family function, resilience, and anxiety. J Affect Disord. 2022;299:12–21. doi:10.1016/j.jad.2021.11.053
47. Yates TM, Carlson EA, Egeland B. A prospective study of child maltreatment and self-injurious behavior in a community sample. Dev Psychopathol. 2008;20(2):651–671. doi:10.1017/s0954579408000321
48. Whitlock J, Eckenrode J, Silverman D. Self-injurious behaviors in a college population. Pediatrics. 2006;117(6):1939–1948. doi:10.1542/peds.2005-2543
49. Gratz KL. Risk factors for and functions of deliberate self-harm: an empirical and conceptual review. Clin Psychol. 2003;10(2):192.
50. Muehlenkamp J, Brausch A, Quigley K, Whitlock J. Interpersonal features and functions of nonsuicidal self-injury. Suicide Life Threat Behav. 2013;43(1):67–80. doi:10.1111/j.1943-278X.2012.00128.x
51. Lim KS, Wong CH, McIntyre RS, et al. Global lifetime and 12-month prevalence of suicidal behavior, deliberate self-harm and non-suicidal self-injury in children and adolescents between 1989 and 2018: a meta-analysis. Int J Environ Res Public Health. 2019;16(22):4581. doi:10.3390/ijerph16224581
52. Hawton K, Rodham K, Evans E. By Their Young Hand: Deliberate Self-Harm and Suicidal Ideas in Adolescents. Jessica Kingsley Publishers; 2006.
53. Shek DT, Tang V. Adolescent suicide in hong kong during 1980–2000. Int J Adolesc Med Health. 2003;15(3):245–265. doi:10.1515/ijamh.2003.15.3.245
54. Rudolph KD, Kurlakowsky KD, Conley CS. Developmental and social–contextual origins of depressive control-related beliefs and behavior. Cognit Ther Res. 2001;25(4):447–475. doi:10.1023/A:1005538704056
55. Baetens I, Claes L, Martin G, et al. Is nonsuicidal self-injury associated with parenting and family factors? J Early Adolesc. 2014;34(3):387–405. doi:10.1177/0272431613494006
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.